Correção cirúrgica da persistência do canal arterial em crianças de ...

Persistência do Canal Arterial - Casuísticade uma Unidade de Cuidados Intensivos
Neonatais [64]HELENA ANDRADE, CARLA LOUREIRO, JOAQUIM TIAGO, RAQUEL HENRIQUES, ANTÓNIO MARINHO DA SILVA, DINA RODRIGUES,
ANTÓNIO SÁ E MELO, ROSA RAMALHO ALVES
Serviço de Neonatologia e Unidade de Cardiologia Pediátrica dos Hospitais da Universidade de Coimbra, Coimbra, Portugal
Rev Port Cardiol 2008; 27 (7-8): 877-885
ARTIGOS ORIGINAIS
877
RESUMO
Objectivo: O estudo, realizado na Unidade deCuidados Intensivos do Recém-Nascido
(UCIRN) da Maternidade Dr. Daniel de Matos,avaliou a incidência da Persistência do Canal
Arterial (PCA), a evolução clínica dos Recém--Nascidos (RN) afectados, o tratamento
prescrito, bem como a morbilidade emortalidade associadas.
Métodos: Analisaram-se retrospectivamente osprocessos clínicos dos RN internados na
UCIRN entre Janeiro de 2001 a Dezembro de2005.
Resultados: Em 69 RN foi diagnosticado PCA(4,6% do total de RN internados). A medianada idade gestacional (IG) foi de 28 semanas e
do peso de nascimento (PN) de 1100 gramas. Odiagnóstico de PCA foi estabelecido, em
média, entre o 5º e o 6º dia de vida. Dos 53 RNcom critérios para encerramento, 49 fizeramindometacina (taxa de sucesso de 88%); em
seis foi posteriormente necessárioencerramento cirúrgico. Trinta e oito RNapresentaram co-morbilidade associada.
Faleceram oito RN.Discussão: Neste estudo, os resultados
encontrados estão de acordo com a literatura.Em IG inferiores às 30 semanas e/ou PN
abaixo dos 1500g, a necessidade de tratamentopara encerramento do canal arterial é superiorà das IG/PN superiores, sendo necessário uma
atitude mais interventiva, com indometacinapré-sintomática em esquema longo. Os
resultados obtidos neste trabalho permitiram--nos concluir ser necessário contemplar a
ecocardiografia como meio de rastreio da PCAa todos os RN abaixo das 30 semanas ou com
PN inferior aos 1500g. Pretendemos, num
ABSTRACT
Patent Ductus Arteriosus - NeonatalIntensive Care Unit Registry
Objectives: This study took place at theNeonatal Intensive Care Unit (NICU) of the DrDaniel de Matos Maternity Hospital andevaluated the incidence of patent ductusarteriosus (PDA), the clinical evolution of thenewborns affected, the treatment prescribed,and associated morbidity and mortality.Methods: We carried out a retrospectivemedical chart review of newborns admitted tothe NICU between January 2001 andDecember 2005.Results: PDA was found in 69 newborns.Median gestational age (GA) was 28 weeks andbirth weight (BW) 1100 grams. The diagnosisof PDA was established, on average, betweenthe fifth and sixth day of life. Of the 53newborns with criteria for closure, 49 hadindomethacin therapy, with a success rate of88%; surgical ligation was subsequentlynecessary in six of these. Thirty-eightnewborns presented associated comorbidities,and eight died.Conclusions: The results obtained in this studyare in agreement with the literature. In caseswith GA of less than 30 weeks and/or BWbelow 1500g, the need for treatment for PDAclosure is greater than in cases with higherGA/BW, and a more aggressive approach isrequired, with presymptomatic prolongedindomethacin. The results obtained in thiswork led us to conclude that echocardiographyshould be performed to screen for PDA in allnewborns of less than 30 weeks or with BWbelow 1500g. We intend in the near future to
Recebido para publicação: Janeiro 2008 • Aceite para publicação: Maio de 2008Received for publication: January 2008 • Accepted for publication: May 2008

INTRODUÇÃO E OBJECTIVOS
Ocanal arterial (CA) une o ramo esquerdoda artéria pulmonar com a aorta
descendente (1). Na vida fetal 90% do débitodo ventrículo direito é canalizado para o CA (2),mantendo-se patente devido aos altos níveis deprostaglandinas, quer circulantes quer locais(principalmente a PGE (2), o prostanoide commaior potência relaxante do CA) (3-7).
Em recém-nascidos (RN) de termo o CAgeralmente encerra entre as primeiras horas e o 3ºdia de vida (8), sendo a sua persistência poucofrequente e raramente sintomática (3,5,6,9-11).
A persistência do canal arterial (PCA) é, noentanto, um problema comum em prematuros (6),originando mais frequentemente um shuntesquerdo-direito significativo e um aumento dodébito do ventrículo esquerdo. Assim, obser-vam-se efeitos tanto a nível pulmonar, comaumento do fluxo pulmonar, como a nívelsistémico, com redução do débito devido aofluxo diastólico retrógrado (“diastolic steal”) (3,5,9).
O objectivo deste estudo foi avaliar aincidência da PCA na Unidade de CuidadosIntensivos do Recém-Nascido (UCIRN) doServiço de Neonatologia dos HospitaisUniversidade de Coimbra, assim como aevolução clínica destes RN, o tratamentoefectuado e a morbilidade e mortalidadeassociadas.
MATERIAL E MÉTODOS
Foi feita a análise retrospectiva do processoclínico dos RN internados na UCIRN, no períodode Janeiro de 2001 a Dezembro de 2005 (cincoanos), aos quais foi estabelecido clinica eecograficamente, o diagnóstico de PCA. Foram
INTRODUCTION AND OBJECTIVES
The ductus arteriosus (DA) connects the leftpulmonary artery and the descending aorta (1);
in the fetus, 90% of right ventricular output ischanneled through it (2). The DA can remain opendue to high levels of circulating and localprostaglandins, particularly PGE2, the prostanoidwith the strongest relaxation effect on the DA (3-7).
In full-term newborns, the DA usually closeswithin hours or up to three days after birth (8);failure to close is uncommon and rarely causessymptoms (3, 5, 6, 9-11).
Patent ductus arteriosus (PDA) is however acommon problem in preterm infants (6), frequentlycausing a significant left-to-right shunt andincreased left ventricular output. This in turnincreases pulmonary flow and, at the systemiclevel, reduces cardiac output due to diastolicsteal (3, 5, 9).
The objective of this study was to evaluate theincidence of PDA at the Neonatal Intensive CareUnit (NICU) of the Neonatology Department ofCoimbra University Hospitals, as well as theclinical evolution of the newborns affected, thetreatment prescribed and associated morbidityand mortality.
METHODS
We carried out a retrospective medical chartreview of the newborns admitted to the NICU overa five-year period (January 2001 and December2005) with a clinical and echocardiographicdiagnosis of PDA. The following parameters wereanalyzed: maternal age, gestational age (GA),prenatal administration of corticosteroids, type ofbirth, birth weight (BW) and gender. Clinicalevolution was assessed based on need for878
Rev Port CardiolVol. 27 Julho/Agosto 08 / July/August 08
futuro breve, responder à questão que nos ficoucom este estudo: poderá um diagnóstico mais
precoce conduzir a uma melhoria deresultados?
Palavras-Chave
Recém-nascido; Persistência do canal arterial; Indometacina;
Morbilidade; Mortalidade
answer a question that emerged from thisstudy: will earlier diagnosis lead to improvedoutcomes?
Key words
Newborn; Patent ductus arteriosus; Indomethacin; Morbidity;
Mortality

avaliados os seguintes aspectos: idade materna,idade gestacional (IG), administração decorticoides pré-natais, o tipo de parto, o peso aonascimento (PN) e o sexo. A evolução clínica foiavaliada em função da necessidade de ventilaçãomecânica, assim como pela morbilidadeassociada e mortalidade. Avaliámos também asopções terapêuticas e a sua taxa de sucesso.
Os sinais clínicos valorizados foram apresença de sopro sistólico ou contínuo nobordo esternal esquerdo/dorso, tensão arterialdivergente ou dependência de ventilaçãomecânica.
Uma vez estabelecido o diagnóstico de PCA, otratamento obedeceu ao protocolo de tratamentoda UCIRN: indometacina precedida de restriçãohídrica, em esquema longo de 0,1 mg/kg/dia, seisdoses (RN com menos de catorze dias de vida) ouesquema curto de 0,2 mg/kg/dose, de 12-12horas, três doses (RN com catorze ou mais dias devida) (12).
Os resultados foram apresentados sob aforma de percentagem, mediana (variáveisdiscretas) e média ± erro padrão da média(variáveis contínuas).
Para o estudo estatístico foi utilizado oprograma SAS, versão 8.01, para Windows.Usou-se o teste exacto de Fisher e o teste de χ2
com correção de Yates. As decisões estatísticasobedeceram a um limiar de significância deα=0,05 considerando-se as diferenças ousignificativas (P<0,05), ou bastante significativas(P<0,01), ou muito significativas (P<0,001).
RESULTADOS
No período em causa, estiveram internados naUCIRN 1503 RN, dos quais 69 tiveramdiagnóstico de PCA, o que corresponde a umaincidência de 46 por cada mil RN internados.
Os 69 RN correspondem a 64 grávidas. Amédia da idade materna foi de 30 anos, variandoentre 18 e 42 anos. Catorze grávidas registaramhipertensão arterial, das quais oito com pré-eclâmpsia e uma com eclâmpsia e três comdiabetes gestacional controlada com medidasalimentares. Registou-se uma corioamniotite eseis sépsis clínicas.
Oito RN apresentaram ecografias fetaisalteradas, dos quais cinco por restrição docrescimento intra-uterino (RCIU) e três com
mechanical ventilation, and associated morbidityand mortality. We also analyzed treatment optionsand their success rates.
Clinical symptoms included systolic orcontinuous murmur at the left sternal borderradiating to the back, divergent blood pressureand dependence on mechanical ventilation.
Once the diagnosis of PDA was made,treatment followed the NICU treatment protocol:after fluid restriction, prolonged indomethacintherapy of 0.1 mg/kg/day in six doses in infantsaged under 14 days, or short therapy of 0.2mg/kg, every 12 hours in three doses in thoseaged 14 days or more (12).
The results are presented as percentages andmedians for discrete variables, and means ±standard error for continuous variables.
SAS for Windows version 8.01 was used forthe statistical analysis, together with Fisher’sexact test and the chi-square test with the Yatescorrection. The significance level was set atα=0.05, with differences being consideredsignificant for p<0.05, very significant forp<0.01, and highly significant for p<0.001.
RESULTS
In the period under study, 1503 newbornswere admitted to the NICU, of whom 69 werediagnosed with PDA, an incidence of 46 for every1000 admitted.
The 69 newborns were the result of 64pregnancies. Mean maternal age was 30, rangingbetween 18 and 42 years. Fourteen mothers hadhypertension during pregnancy, of whom eighthad pre-eclampsia and one eclampsia, and threehad gestational diabetes controlled through diet.There was one case of chorioamnionitis and sixcases of clinical sepsis.
Eight newborns presented abnormalities onfetal ultrasound, five due to intrauterine growthretardation and three with oligamnios. Fetalechocardiography was performed in five (three forgestational diabetes, one for fetal ascites and theother for fetal arrhythmia), which was normal inall cases.
Of the 59 newborns with GA of less than 34weeks, corticosteroids were administered in allbut eight. In most cases, duration of rupture ofmembranes was less than 12 hours, and 61% ofdeliveries were by Cesarean section. 879
HELENA ANDRADE, at alRev Port Cardiol 2008; 27: 877-85

oligoâmnios. Cinco realizaram ecocardiografiafetal (três por diabetes gestacional, um por ascitefetal e outro por arritmia fetal), sendo em todosconsiderada normal.
Dos 59 RN com IG inferior a 34 semanas,em apenas oito não foi administrada qualquerdose de corticoide. Na maioria dos casosregistou-se uma rotura de membranas inferior a12 horas. Em 61% dos casos o parto foi porcesariana.
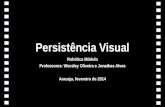
A média da IG foi de 29 semanas (± 3,8semanas) e a mediana foi de 28 semanas(variando entre 24 e 41 semanas). Sessenta equatro RN (93%) eram prematuros (IG inferior a37 semanas completas) (Gráfico 1). A média doPN foi de 1345 g (± 845 g) e a mediana foi de1100 g (variando entre 500 e 4670 g). Sessenta edois (90%) eram RN de baixo peso (PN inferior a2500 g) e 52 eram RN de muito baixo peso(RNMBP), isto é, PN inferior a 1500 g. Como noperíodo em causa estiveram internados 316RNMBP, pode-se dizer que 16,5% tiveram odiagnóstico de PCA. Oito RN eram RCIU.
Quarenta (58%) RN eram do sexo feminino e29 do sexo masculino, o que representa umarelação masculino/feminino de 1/1,4.
Quarenta e três RN foram reanimados nasala de partos e 47 necessitaram de intubaçãoe ventilação mecânica na UCIRN.
O diagnóstico de PCA foi estabelecido,em média, entre o 5º e o 6º dia de vida, porecocardiografia.
Vinte e nove RN tinham cardiopatia e/oualterações cardíacas associadas, nomeadamente
Mean GA was 29±3.8 weeks and the medianwas 28 weeks (24-41). Sixty-four newborns (93%)were preterm (GA less than 37 full weeks) (Figure1). Mean BW was 1345±845 g, and the medianwas 1100 g (500-4670). Sixty-two (90%) had lowBW (below 2500 g), and 52 had very low BW(below 1500 g). Of the 316 infants with very lowBW admitted during the study period, 16.5% hada diagnosis of PDA. Eight newborns hadintrauterine growth retardation.
Forty (58%) of the newborns were girls and 29boys, a male/female ratio of 1/1.4.
Forty-three required resuscitation in thedelivery room and 47 needed intubation andmechanical ventilation in the NICU.
The diagnosis of PDA was established byechocardiography, between the fifth and sixth dayof life on average.
Twenty-nine infants had heart disease and/orassociated cardiac anomalies, includingventricular septal defect (four), atrial septaldefect or patent foramen ovale (fourteen),pulmonary hypertension (eight), and poorventricular function (eight).
Fifty-two had clinical and echocardiographiccriteria for DA closure. Of these, three hadabsolute contraindication for indomethacintherapy, and so only 49 underwentpharmacological closure. Thirty had prolongedtherapy, 10 short therapy and four had twocycles (prolonged followed by short). Five didnot complete the therapy - in three closure wasdetected on reassessment, and two died. Closurewas confirmed by echocardiography in all cases.
880
Rev Port CardiolVol. 27 Julho/Agosto 08 / July/August 08
0
2
4
6
8
10
12
24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 >40
Idade gestacional (semanas)Gestational age (weeks)
Nº
de r
ecém
-nas
cido
sN
umbe
r of
new
born
s
Gráfico 1. Distribuição doscasos por idade gestacional.
Figure 1. Distribution of casesby gestational age

Comunicação Interventrícular (quatro),Comunicação Interauricular / Foramen OvalePatente (catorze), Hipertensão Pulmonar (oito) oumá função ventricular (oito).
Cinquenta e dois RN apresentavam critérios(clínicos e ecográficos) para realização deencerramento do CA. Destes, três tinhamcontra-indicação absoluta para o uso deindometacina, pelo que apenas 49 foramsubmetidos a encerramento farmacológico: 30fizeram ciclo longo, 10 ciclo curto e quatrofizeram dois ciclos (ciclo longo seguido de ciclocurto). Cinco não completaram o ciclo, três por tersido detectado encerramento numa reavaliaçãointercalar e dois por falecimento. O encerramentodo CA foi sempre confirmado por ecocardiografia.
Houve necessidade de seis RN seremsubmetidos a encerramento cirúrgico, porinsucesso do tratamento com indometacina.Nenhum RN foi submetido a cirurgia comotratamento de primeira linha. A cirurgia foirealizada, em média, ao 28º dia de vida. Quatrodestes RN estavam dependentes do ventilador àdata da intervenção.
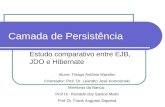
No quadro I está apresentada a média dosquadrados mínimos da idade gestacional e dospesos, de acordo com o tratamento realizado.
Para a avaliação da co-morbilidade foramanalisados os seguintes parâmetros: sépsis (comhemocultura positiva) 34 RN, doença demembrana hialina 27 RN, displasia bronco-pulmonar (DBP) quatro RN, insuficiência renalaguda dez RN (apenas quatro durante otratamento com indometacina, sem obrigar asuspender tratamento e todas elas reversíveis),hemorragia intra-ventricular (HIV) grave (grauIII-IV) seis RN e enterocolite necrotizante (NEC)três RN.
Faleceram oito RN (11,6%), tendo cincorealizado indometacina e três com contra-
Six infants required surgical ligation afterunsuccessful indomethacin therapy. In no casewas surgical closure the first-line treatment. Onaverage, surgery was performed at 28 days of life;in four cases, the infant was dependent onmechanical ventilation at the time of theintervention.
Table I shows the minimum mean squares ofgestational age and birth weight according to thetreatment prescribed.
The following comorbidities were analyzed:sepsis, with positive blood culture, in 34 infants,hyaline membrane disease in 27, broncho-pulmonary dysplasia (BPD) in four, acute renalfailure in ten (only four during indomethacintherapy, which did not need to be suspended, andreversible in all cases), severe intraventricularhemorrhage (IVH) (grade III-IV) in six, andnecrotizing enterocolitis (NEC) in three.
Eight infants died (11.6%), of whom five hadhad indomethacin and three had absolutecontraindication for this therapy. All had very lowbirth weight (mean 857±279 g) and were verypremature (mean GA 26.4 weeks, maximum 28weeks).
Analysis of follow-up was possible in 49(80%) of the 61 surviving infants, age at lastassessment ranging between eight and 28months. Forty of them (82%) had normalpsychomotor and cognitive development; threehad cerebral palsy, all of whom were born veryprematurely with very low BW.
DISCUSSION
The incidence of PDA in the NICU was 4.6%of the total admitted and 16.5% of those of verylow birth weight. Published series show that theincidence of PDA is higher the lower the GA andBW (4, 6, 8, 13), and can reach 80% if BW is below 881
HELENA ANDRADE, at alRev Port Cardiol 2008; 27: 877-85
Terapêutica
Sem tratamento
I.Gest. (*)27,6
27,7
33
Médica
Cirúrgica
P.N. (*)1039
980
2237
Quadro I. Média dos quadrados mínimos da idadegestacional e do peso de nascimento, de acordo com otratamento realizado.
I. Gest. - Idade Gestacional (em semanas)P.N. - Peso de Nascimento (em gramas)* - Média dos quadrados mínimos
Treatment
No treatment
Gestational age(weeks) (*)
27,6
27,7
33
Medical
Surgical
Birth weight(g) (*)1039
980
2237
Table I. Minimum mean squares of gestational age andbirth weight by treatment option
* Minimum mean square

indicação absoluta para tal. Todos eram RNMBP(média de PN de 857g ± 279g) e grandesprematuros (média da IG de 26,4 semanas,máximo de 28 semanas).
Foi possível avaliar o follow-up de 49 (80%)dos 61 RN sobreviventes, com idade na últimaavaliação variando entre oito e 28 meses.Quarenta (82%) são crianças normais,nomeadamente em termos psico-motores ecognitivos; registam-se três paralisias cerebrais,em RNMBP grandes prematuros.
DISCUSSÃO
A incidência da PCA na UCIRN foi de 4,6%no total de RN internados e de 16,5% nos RNde muito baixo peso. Séries publicadas revelamuma incidência da PCA maior quanto menor é aIG e o PN (4,6,8,13), principalmente se abaixo das1000g, onde pode atingir os 80% (8,14). O provávelsub-diagnóstico pode prender-se, em grandemedida, com o facto de não se realizar na UCIRNecocardiograma de rotina para rastreio da PCAsilenciosa.
Alguns autores propõem uma avaliaçãoecocardiográfia de rotina a todos os RNprematuros abaixo das 30 semanas, quer peloimpacto negativo da PCA neste grupo, quer pelotardar da clínica (5,15). Segundo Evans et al (16),confiar nos sinais clínicos resulta num atraso dodiagnóstico da PCA.
A média da idade materna está de acordo coma população geral da maternidade.
Tal com descrito na literatura (excepto nacasuística de Baptista et al (14)), predominou o sexofeminino.
Tanto o tipo de tratamento como a altura idealpara o iniciar ainda são controversos, nãohavendo consenso na literatura, quer nacionalquer internacional (2,4,9). Na nossa amostra odiagnóstico foi estabelecido entre o 5º e o 6º diade vida, o que está de acordo com a literatura,quando se fala em diagnóstico baseado naclínica (3,5,16). Já Pham et al (13) refere o facto de CAlargos poderem apresentar sopros discretos oumesmo não apresentar qualquer sopro, pelo que énecessário cuidado quando se opta pelaabordagem de tratar CA sintomáticos.
Os RN que não necessitaram de tratamentorevelaram IG e PN significativamente superioràqueles que necessitaram de tratamento
1000 g (8, 14). The fact that it is probablyunderdiagnosed may be due in large part to thefact that routine echocardiography is notperformed in the NICU to screen for silent PDA.
Some authors suggest routine echocardio-graphic assessment in all preterm infants under30 weeks, given the negative impact of PDA inthis group and that clinical symptoms may onlyappear later (5, 15). According to Evans et al. (16),relying on clinical signs results in delay indiagnosing PDA.
Mean maternal age in our study was similar tothe general maternity hospital population.
As in other studies in the literature (exceptthat of Baptista et al. (14)), there was a higherproportion of female infants in our population.
The type and timing of treatment is still thesubject of debate, with no consensus in thePortuguese or international literature (2, 4, 9). In oursample, the diagnosis was established betweenthe fifth and sixth day of life, which is inagreement with the literature for diagnosis basedon clinical signs (3, 5, 16). Pham et al. (13) point out thata large ductus arteriosus may present only a slightmurmur or none at all, and opting for a strategy ofonly treating symptomatic PDA should beregarded with caution.
The newborns who did not require treatmenthad significantly higher GA and BW than thosewho did (p<0.001), but there were no significantdifferences in these parameters in terms of type oftreatment (Table II). Our results clearly show thatin infants of low GA, particularly less than 30weeks, and/or BW below 1500 g, the need fortreatment for PDA closure is greater than in thosewith higher GA/BW. This indicates that an earlierassessment than usual and a more aggressive(presymptomatic) approach may be necessary,with a view to preventing complications
882
Rev Port CardiolVol. 27 Julho/Agosto 08 / July/August 08
Treatment
No treatmentSig. (‡)
Gestational age(weeks) (†)
27,6
27,7
33*
b
b
a
Medical
Surgical
Birth weight(g) (†)1039
980
2237*
Table II. Statistical analysis of the effect of gestational ageand birth weight on type of treatment.
Sig.: level of significance; *: p=0.001 by Fisher’s exact test; †: Minimum meansquares; ‡: In each column, values followed by the same letter did not differsignificantly (level of significance >0.05) by MDS

(P<0,001); o tipo de tratamento não apresentoudiferenças significativas nestes parâmetros(Quadro II). Estes resultados são clarosindicadores que em IG baixas, principalmenteinferiores às 30 semanas e/ou PN abaixo dos1500g, a necessidade de tratamento paraencerramento do CA é superior à das IG/PNsuperiores, levando a pensar ser necessáriouma avaliação mais precoce do que o habitual euma atitude mais interventiva (pré-sintomática),com a perspectiva de evitar complicações(nomeadamente DBP, necessidade de ventilaçãomecânica e NEC) (3,5,6,9,14,15).
A favor desta atitude está também um estudoque refere que, mesmo nos RN com IG<27s,quando se verifica uma constrição precocepobre do CA, este tem maior probabilidade depersistir patente. Já quando se verifica uma boaconstrição precoce, o CA raramente se mantémaberto (5).
A taxa de sucesso com a indometacina foielevada (88%), o que é semelhante ao encontradona literatura (4-6,8,13). Na revisão que efectuamos,preconiza-se actualmente o ciclo longo emdetrimento do curto, pela sua eficácia semelhantee menos efeitos secundários (3-5,13,17).
A necessidade de encerramento cirúrgicoprendeu-se com a falência do tratamentomédico/evolução clínica desfavorável e foi,em média, aos 28 dias de vida. Tal como descritona literatura, a opção cirúrgica na nossa unidadeé de segunda linha (14), o mais precocementepossível após falência do tratamento médico. Noentanto pensamos que deverá ser mais precoce,tal como é referido por Jaillard et al (18): alaqueação cirúrgica antes das 3 semanas de vida,
(particularly DBP, need for mechanicalventilation and NEC) (3, 5, 6, 9, 14, 15).
In support of this approach, another studyreports that even in newborns with a GA of <27weeks, poor early ductal constriction indicates agreater likelihood that it will remain patent, whilein infants with good early constriction, it rarelyremains open (5).
The success rate of indomethacin washigh (88%), similar to that reported in theliterature (4-6, 8, 13). From our chart review, prolongedrather than short therapy is now recommended,since it has similar efficacy and fewer secondaryeffects (3-5, 13, 17).
Surgical closure was required in cases ofunsuccessful medical treatment or unfavorableclinical evolution, and was performed, onaverage, at 28 days of life. As described in theliterature, surgery is the second-line treatment inour unit (14), and is performed as soon as possibleafter failure of the medical option. Nevertheless,we believe it should be performed even earlier, asindicated by Jaillard et al. (18); surgical ligationwithin three weeks of birth enables more rapidreduction in ventilatory parameters, earlier fulloral feeding and better weight gain at a correctedage of 36 weeks.
In PDA, a large volume of blood isdiverted from the systemic to the pulmonarycirculation, the reduction in systemic cardiacoutput (ductal steal) being proportional to thediameter of the DA (5). The negative effects ofPDA on the systemic circulation includepulmonary hemorrhage (3), IVH, NEC, and renaldysfunction (7, 11). Early PDA closure preventsdeterioration of pulmonary function and appearsto reduce the incidence of NEC (19).
Comorbidities (particularly chronic lungdisease and IVH (3)), mortality and follow-up inour series were similar to those reported in otherstudies (14).
The results obtained in this work led us toconclude that, in view of the probableunderdiagnosis of PDA, a new protocol shouldbe implemented in our unit, in whichechocardiography is performed to screen forPDA in all newborns of less than 30 weeks orwith BW below 1500 g. We also feel thatfollowing earlier diagnosis, a more aggressiveapproach is required, with presymptomaticprolonged indomethacin therapy.
We intend in the near future to answer a 883
HELENA ANDRADE, at alRev Port Cardiol 2008; 27: 877-85
Terapêutica
Sem tratamentoSig. (‡)
I.Gest. (†)27,6
27,7
33*
b
b
a
Médica
Cirúrgica
P.N. (†)1039
980
2237*
Quadro II. Análise estatística do efeito da idadegestacional e do peso de nascimento no tipo de tratamentonecessário.
Sig. - nível de significância* - significativo ao nível de 0,001 pelo teste de Fisher.† - Média dos quadrados mínimos‡ - Em cada coluna, valores seguidos da mesma letra não diferemsignificativamente ao nível de 0,05 pelo teste da MDS.
b
b
a

quando comparado com a efectuada poste-riormente, permite redução mais rápida deparâmetros ventilatórios, alimentação oral totalmais precoce e melhor ganho ponderal às 36semanas de idade corrigida.
Através do CA grandes volumes de sanguesão desviados da circulação sistémica para acirculação pulmonar, havendo relação entre odiâmetro do canal e o baixo débito cardíacosistémico (“ductal steel”) (5). Os efeitos negativosdo CA na circulação sistémica podem-se traduzirem hemorragia pulmonar (3), HIV, NEC, disfunçãorenal (7,11). O encerramento precoce do CA previnea deterioração da função pulmonar e parecediminuir a incidência de NEC (19).
A co-morbilidade (nomeadamente doençapulmonar crónica e HIV (3)), mortalidade e ofollow-up na nossa série foram idênticos àsdescritas noutras séries (14).
Os resultados obtidos através deste trabalhopermitiram-nos concluir, tendo em conta oprovável sub-diagnóstico da PCA, ser necessárioa implementação de novo protocolo de actuaçãona Unidade, contemplando a ecocardiografiacomo meio de rastreio da PCA a todos os RNabaixo das 30 semanas ou com PN inferior aos1500g. Também achamos importante, noseguimento de um diagnóstico mais precoce, umaactuação mais agressiva, com indometacina pré-sintomática em esquema longo.
Pretendemos, num futuro breve, responder àquestão que nos ficou com este estudo: poderá umdiagnóstico mais precoce conduzir a umamelhoria de resultados?
AGRADECIMENTOS
Um agradecimento especial ao Eng. JoséViana Andrade pelo apoio na elaboração do textoe ao Dr. Fernando Delgado pela dedicadacolaboração na análise estatística dos dados.
question that emerged from this study: will earlierdiagnosis lead to improved outcomes?
ACKNOWLEDGEMENTS
We would like to extend our special thanks toJosé Viana Andrade for his help in preparing thetext and to Dr. Fernando Delgado for his valuablecontribution to statistical analysis of the data.
Pedidos de separatas para:
Address for reprints:
HELENA ANDRADE
Unidade de Cardiologia Pediátrica
Hospitais da Universidade de Coimbra
Praceta Prof. Mota Pinto
3000-075 Coimbra, Portugal
Tel. 351.239400400 - Fax 351.239837081
E-mail: [email protected]
884
Rev Port CardiolVol. 27 Julho/Agosto 08 / July/August 08

885
HELENA ANDRADE, at alRev Port Cardiol 2008; 27: 877-85
1. Ellis H. Anatomy of fetal circulation. Anaesthesia andIntensive Care Medicine 2005; 6(3): 73.
2. Markham M. Patent Ductus Arteriosus in the PrematureInfant: a clinical dilemma. Newborn and Infant NursingReviews 2006; 6(3): 151-157.
3. Evans N. Current controversies in the diagnosis andtreatment of patent ductus arteriosus in preterm infants.Advances in Neonatal Care 2003; 3(4): 168-177.
4. Wyllie J. Treatment of patent ductus arteriosus. SeminNeonatol 2003; 8: 425-432.
5. Evans N. Patent ductus arteriosus in the neonate. CurrentPaediatrics 2005; 15: 381-389.
6. Overmeire B, Chemtob S. The pharmacologic closure of thepatent ductus arteriosus. Seminars in Fetal & NeonatalMedicine 2005; 10: 177-184.
7. Miyague NI. Persistência do canal arterial em recém-nascidosprematuros. J Pediatr 2005; 81: 429-430.
8. Afiune JY, Singer JM, Leone CR. Evolução ecocardiográficasde recém-nascidos com persistência do canal arterial. J Pediatr2005; 81: 454-460.
9. Knight D. The treatment of patent ductus arteriosus inpreterm infants. A review and overview of randomized trials.Semin Neonatol 2001; 6: 63-73.
10. Skinner J. Diagnosis of patent ductus arteriosus. SeminNeonatol 2001; 6: 49-61.
11. Artman M, Mahony L, Teitel DF. Patent Ductus Arteriosus.In: Artman M, Mahony L, Teitel DF, eds. Neonatal Cardiology.McGraw-Hill, 2002; 113-115.
12. Negrão F, Afonso E. Persistência do Canal Arterial. In:Protocolos de Neonatologia, Maternidade Dr. Daniel de Matos,Hospitais da Universidade de Coimbra, 1996; 4.
13. Pham J, Carlos M. Current Treatment Strategies ofSymptomatic Patent Ductus Arteriosus. PediatricPharmacology 2002; 16(6): 306-310.
14. Baptista M J, Correia-Pinto J, Areias J C, Guimarães H.Canal arterial patente em cuidados intensivos neonatais. RevPort Cardiol 1999; 18(12): 1095-1100.
15. Evans N. The neonate and ductus arteriosus: importance,diagnosis and practical management. Current Paediatrics 1995;5: 114-117.
16. Evans N, Malcolm G, Osborn D, Kluckow M. Diagnosis ofPatent Ductus Arteriosus in Preterm Infants. NeoReviews 2004;5(3): 86-97.
17. Tammela O, Ojala R, Iivainen T, et al. Short versusProlonged Indomethacin Therapy for Patent Ductus Arteriosusin Preterm Infants. J Pediatr 1999; 134(5): 552-557.
18. Jaillard S, Larrue B, Rakza T, Magnenant E, WarembourgH, Storme L. Consequences of Delayed Surgical Closure ofPatent Ductus Arteriosus in Very Premature Infants. AnnThorac Surg 2006; 81: 231-235.
19. Clyman RI, Chorne N. Patent Ductus Arteriosus: Evidencefor and against Treatment. J Pediatr 2007; 150: 216-219.
BIBLIOGRAFIA / REFERENCES
3º Congresso Português de Hipertensão International Meeting on Hypertension
Hotel Tivoli Marina Vilamoura, Algarve12 a 15 de Fevereiro de 2009
Presidente do Congresso: Luís Martins
Presidente da Comissão Organizadora: Paula Alcântara
www.sphta.org.pt