BEM Biokim Harly PhD (2)
23
Endocrine Disorders Endocrine Disorders Harliansyah,Ph.D Harliansyah,Ph.D Dept Biochemistry, FK-UY Dept Biochemistry, FK-UY
-
Upload
affandi-akbar -
Category
Documents
-
view
236 -
download
0
Transcript of BEM Biokim Harly PhD (2)

Endocrine DisordersEndocrine Disorders
Harliansyah,Ph.DHarliansyah,Ph.DDept Biochemistry, FK-UYDept Biochemistry, FK-UY

Abnormalities of endocrine glands Abnormalities of endocrine glands generally fall into one of the generally fall into one of the
several categories;several categories; 1. Hypersecretion1. Hypersecretion - Excess activity of a specific hormone- Excess activity of a specific hormone - May be due to overproduction of a hormone due to - May be due to overproduction of a hormone due to
abnormal abnormal glandular function, glandular hypertrophy/ glandular function, glandular hypertrophy/
hyperplasia or thehyperplasia or the presence of tumors that secrete hormone.presence of tumors that secrete hormone.
2. Hyposecretion2. Hyposecretion - Reduced activity of a specific hormone- Reduced activity of a specific hormone - May be due to atrophy of glandular tissue or damage - May be due to atrophy of glandular tissue or damage
from autoimmune attack, infection or neeoplasia. from autoimmune attack, infection or neeoplasia.

3. Altered responsiveness of a tissue to a specific hormone
-. Tissue no longer responds to a specific hormone -. May involve down regulation of receptors or altered receptor/ secondary messenger function -. Circulating levels of hormone may be normal or even elevated ( Type II DM)
Metabolic syndromeMetabolic syndrome



The metabolic syndrome is identified by The metabolic syndrome is identified by the presence of three or more of these the presence of three or more of these
components:components: Central obesity as measured by waist Central obesity as measured by waist
circumference:circumference:Men — Greater than 40 inches (102 cm)Men — Greater than 40 inches (102 cm)
Women — Greater than 35 inches (88 cm)Women — Greater than 35 inches (88 cm) Fasting blood triglycerides greater than or equal to Fasting blood triglycerides greater than or equal to
1.7 mmol/L1.7 mmol/L Blood HDL cholesterol:Blood HDL cholesterol:
Men — Less than 1.03 mmol/LMen — Less than 1.03 mmol/LWomen — Less than 1.2 mmol/LWomen — Less than 1.2 mmol/L
Blood pressure greater than or equal to 130/85 Blood pressure greater than or equal to 130/85 mmHgmmHg
Fasting glucose greater than or equal to 6.1 mmol/LFasting glucose greater than or equal to 6.1 mmol/L

The Metabolic Syndrome:The Metabolic Syndrome:SignificanceSignificance
Body SizeBody Size BMIBMI
Central AdiposityCentral Adiposity
GlucoseGlucoseMetabolismMetabolism
Uric AcidUric AcidMetabolismMetabolism DyslipidemiaDyslipidemia Hemodynamic Novel Risk
Factors
CORONARY HEART DISEASECORONARY HEART DISEASE
Insulin ResistanceInsulin Resistance
HyperinsulinemiaHyperinsulinemia++
TGTG PP lipemiaPP lipemia HDL-CHDL-C
Small, dense LDLSmall, dense LDL
± ± GlucoseGlucoseintoleranceintolerance
Uric acidUric acid Urinary Urinary
uricuricacid clearanceacid clearance
SNS activitySNS activity Na retentionNa retentionHypertensionHypertension
CRPCRP PAI-1PAI-1
FibrinogenFibrinogen

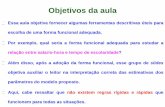
There are three types of hormonal control pathways
Pathway Example
Stimulus Low bloodglucose
Receptorprotein
Pancreassecretesglucagon ( )
Endocrinecell Blood
vessel
LiverTarget
effectors
Response
Pathway Example
Stimulus Suckling
Sensoryneuron
Hypothalamus/posterior pituitary
Neurosecretorycell
Bloodvessel
Posterior pituitarysecretes oxytocin( )
Targeteffectors
Smooth musclein breast
Response Milk release
Pathway Example
Stimulus Hypothalamicneurohormonereleased inresponse toneural andhormonalsignals
Sensoryneuron
Hypothalamussecretes prolactin-releasinghormone ( )
Neurosecretorycell
Bloodvessel
Anteriorpituitarysecretesprolactin ( )Endocrine
cellBloodvessel
Targeteffectors
Response
Mammary glands
Milk production
(c) Simple neuroendocrine pathway
(b) Simple neurohormone pathway
(a) Simple endocrine pathway
Hypothalamus
Glycogenbreakdown,glucose releaseinto blood





Glucos
e Ra
TG
Normal Insulin Normal Insulin FunctionFunction
Insulin InsulinInsulin
Glucose
InsulinInsulin
Insulin
InsulinInsulin
Insulin
Insulin InsulinInsulin
GlucoseGlucose
GlucoseGlucose
GlucoseGlucoseGlucose
Glucose

Normal Insulin ActionNormal Insulin Action
Increase in glucose uptake by Increase in glucose uptake by muscle, liver, and fatmuscle, liver, and fat
Decrease glucose output by the Decrease glucose output by the liverliver
Increase TG storage, decreased Increase TG storage, decreased TG breakdownTG breakdown
Net Result:

Insulin ResistanceInsulin Resistance
Increased insulin production to Increased insulin production to force glucose uptakeforce glucose uptake
Decreased inhibition of glucose Decreased inhibition of glucose rate of appearance from the liverrate of appearance from the liver
Decreased inhibition of TG Decreased inhibition of TG breakdown FFA in blood.breakdown FFA in blood.
Net Result:

TGTGCholesterolCholesterolLDLLDLHDLHDLInsulin (hyperinsulinemia)Insulin (hyperinsulinemia)Post-prandial glucosePost-prandial glucose
Consequences of Prolonged Consequences of Prolonged HyperinsulinemiaHyperinsulinemia

Consequences of Prolonged Consequences of Prolonged Hyperinsulinemia….Hyperinsulinemia….
Prolonged high levels of insulin:Prolonged high levels of insulin: glucose continues to enter cells, but glucose continues to enter cells, but
stored in liver and fat cells and less stored in liver and fat cells and less glucose for immediate fuelglucose for immediate fuel
hunger returns quickly and eating hunger returns quickly and eating increases resulting in weight gain increases resulting in weight gain






Thanks you