Centro de Investigação em Atividade Física, Saúde e Lazer · programa de exercícios que foram...
150
UNIVERSIDADE DO PORTO FACULDADE DE DESPORTO Centro de Investigação em Atividade Física, Saúde e Lazer Efeitos de um programa de exercícios na sintomatologia lombar e qualidade de vida em operários A presente dissertação foi escrita para a obtenção do título de Doutor no âmbito do curso de Doutoramento em Atividade Física e Saúde, da Faculdade de Desporto, nos termos do artigo 81º do Decreto de Lei 74/2006. Orientadores: Prof. Doutor José Carlos Ribeiro Prof. Doutor Pedro Moreira Cristina Teresa Torrão de Carvalho Mesquita Porto, Setembro, 2011
Transcript of Centro de Investigação em Atividade Física, Saúde e Lazer · programa de exercícios que foram...

UNIVERSIDADE DO PORTO
FACULDADE DE DESPORTO
Centro de Investigação em Atividade Física, Saúde e Lazer
Efeitos de um programa de exercícios na sintomatologia lombar e qualidade de vida em
operários
A presente dissertação foi escrita para a obtenção do título de Doutor no âmbito do curso de Doutoramento em Atividade Física e Saúde, da Faculdade de Desporto, nos termos do artigo 81º do Decreto de Lei 74/2006. Orientadores: Prof. Doutor José Carlos Ribeiro
Prof. Doutor Pedro Moreira
Cristina Teresa Torrão de Carvalho Mesquita Porto, Setembro, 2011

II
Ficha de catalogação
Mesquita, C.T.T.C. (2011). Efeitos de um programa de exercícios na sintomatologia lombar e qualidade de vida em operários. Porto: C.T.T.C. Mesquita. Dissertação de Doutoramento em Actividade Física e Saúde apresentada na Faculdade de Desporto da Universidade do Porto
PALAVRAS-CHAVE: DOR LOMBAR, OPERÁRIOS, FORÇA E RESISTÊNCIA
MUSCULAR, EXERCICIO ESPECIFICO.

III
Deus não escolhe os capacitados, capacita os escolhidos
Fazer ou não fazer algo só depende de nossa vontade e perseverança
Albert Einstein
Acredita em Ti Mesmo
O homem converte-se aos poucos naquilo que acredita poder vir a ser. Se me
repetir incessantemente a mim mesmo que sou incapaz de fazer determinada
coisa, é possível que isso acabe finalmente por se tornar verdade. Pelo
contrário, se acreditar que a posso fazer, acabarei garantidamente por adquirir
a capacidade para a fazer, ainda que não a tenha num primeiro momento.
Mohandas Gandhi, in 'The Words of Gandhi'


V
O trabalho da candidata foi financiado pela bolsa de doutoramento PROTEC do
Instituto Politécnico do Porto e da Fundação para a Ciência e Tecnologia
(SFRH/BD/50183/2009).
Trabalho efectuado em colaboração com o Centro de Investigação em
Atividade Física, Saúde e Lazer (CIAFEL) da Faculdade de Desporto da
Universidade do Porto.


VII
Agradecimentos
Agradeço aos meus orientadores, Prof. Doutor José Carlos Ribeiro e Prof.
Doutor Pedro Moreira pela sua competência científica e pelo apoio prestado na
realização deste trabalho.
À coordenadora da área científica da Fisioterapia da Escola Superior de
Tecnologia da Saúde do Porto, Prof. Doutora Cristina Melo que sempre apoiou
os docentes que estavam e estão a realizar doutoramento mantendo as suas
funções profissionais.
A todos os indivíduos que fizeram parte deste estudo sem os quais teria sido
impossível a realização deste trabalho, os meus sinceros agradecimentos,
assim como, aos Departamentos Médico, de Recursos Humanos e de Higiene
e Saúde Ambiental da empresa.
Aos colegas que ajudaram na recolha de dados, implementação e controle do
programa de exercícios que foram a Bárbara, César, Irene, Joana, Mariana e
Vera.
Um especial e profundo agradecimento às amigas e colegas que me ajudaram
na revisão dos artigos e da tese e que desde o inicio até ao final me apoiaram
dando força, ânimo para manter a perseverança e nunca “pensar” em desistir,
não cito nomes pois elas sabem quem são…
Aos meus pais que foram e sempre serão os pilares da minha existência e
exemplos de coragem, determinação e moralidade.
Aos meus irmãos e queridos sobrinhos que souberam compreender as minhas
ausências.
Aos amigos e família que sempre me apoiaram em todos os meus projectos
pessoais e profissionais, o meu bem-haja.
Ao Rui pelo esforço, paciência, compreensão e amor demonstrado ao longo
desta jornada, o meu muito obrigada.


IX
Índice Geral
Agradecimentos VII
Índice Geral IX
Índice de Figuras XI
Índice de Tabelas XII
Resumo XIII
Abstract XV
Lista de Abreviaturas XVII
Introdução 1
Revisão da literatura 7
Objetivos 17
Material e Métodos 19
Instrumentos 20
Procedimentos 23
Capitulo 1 25
Introduction 28
Methods 29
Results 30
Discussion 31
Conclusion 32
References 32
Capitulo 2 35
Introduction 37
Methods 39
Results 41

X
Discussion 43
Conclusion 45
References 45
Capitulo 3 51
Introduction 54
Methods 55
Results 59
Discussion 60
Acknowledgements 63
References 63
Capitulo 4 69
Introduction 72
Methods 74
Results 77
Discussion 80
Conclusion 83
Acknowledgements 83
Discussão 87
Conclusões 97
Bibliografia Geral 101
Anexos XIX

XI
Índice de Figuras
Figura 1 21
Figura 2 21
Figura 3 22
Figura 4 22

XII
Índice de Tabelas
Capitulo 1
Tabela 1 31
Tabela 2 31
Capitulo 2
Tabela 1 40
Tabela 2 42
Tabela 3 43
Tabela 4 43
Capitulo 3
Tabela 1 57
Tabela 2 60
Capitulo 4
Tabela 1 75
Tabela 2 78
Tabela 3 78
Tabela 4 79
Tabela 5 80

XIII
RESUMO
As lesões músculo-esqueléticas estão entre as doenças mais referidas pelos trabalhadores europeus. Um Inquérito Europeu sobre Condições de Trabalho (2005) revelou que 20% dos trabalhadores queixavam-se de problemas e dores musculares nas costas. Os distúrbios lombares foram identificados como um risco elevado em muitas indústrias, devido à incidência e prevalência de lombalgia ocupacional elevadas sendo um dos fatores de limitação do sistema locomotor.Cada vez se torna mais pertinente prevenir estas disfunções e reduzir a sintomatologia músculo-esquelética (SME). Também, quanto mais alta for a perceção que os indivíduos têm da sua qualidade de vida (QV) resultará numa melhor funcionalidade e num melhor desempenho profissional.
Esta tese foi constituída por quatro estudos, o estudo I, foi a adaptação para a população portuguesa de um instrumento válido e fiável que avalie a SME, tendo-se optado pelo standardized Nordic musculoskeletal questionnaire
(NMQ); o estudo II, analisou a SME existentes no início e após 11 e 21 meses de intervenção; o estudo III, foi a avaliação da força e resistência dos extensores e flexores lombares; e o estudo IV, verificou a percepção da QV relacionada com a saúde durante todo o período de intervenção.
A versão em português do NMQ mostrou ser válida revelando bons coeficientes de fiabilidade (estudo I). No estudo II, pode-se concluir que um programa de exercícios específicos melhorou a SME na região lombar durante os 21 meses, nas variáveis: "problemas nos últimos 12 meses", "limitações nos últimos 12 meses" e "problemas nos últimos 7 dias". Houve melhorias significativas na força muscular e resistência dos extensores, medidos 11 meses após o início da intervenção; ao comparar os dois grupos, as principais diferenças foram verificadas nos flexores lombares e força de extensores (estudo III). Relativamente à QV verificou-se que um programa de exercícios específicos, a longo prazo, modificou positivamente a perceção dos indivíduos em relação à sua saúde.
Palavras-chave : saúde ocupacional, NMQ, fiabilidade, validade, operários, sintomas músculo-esqueléticos, força e resistência muscular, exercícios específicos, qualidade de vida, SF-36.


XV
ABSTRACT
Musculoskeletal disorders are among the most widespread illnesses reported by European workers. According to European Working Conditions Survey (2005), about 20% of EU workers complain of back problems and muscular pains. In fact, low back pain (LBP) constitutes the major cause of work absence, as it is one of the causes of limitation of the locomotor system. LBP are especially high in manual work industries. The importance of prevention and decrease the musculoskeletal symptomatology and improved quality of life (QoL), resulting in better professional performance and functionality is well Know.
This thesis comprises four studies, study I, the adaption to the Portuguese population of an instrument to assess musculoskeletal symptoms, the standardized Nordic musculoskeletal questionnaire (NMQ); study II, that
measures the musculoskeletal symptomatology (MSS) changes after 21months intervention; study III, to assess the strength and resistance of the extensors and flexors of the trunk; and the study IV to verify the perception of health related QoL throughout the intervention period.
The Portuguese version of NMQ seems to be valid revealing good coefficients of reliability (study I).In the study (II), it can be concluded that a specific exercise program improved MSS in the low back region throughout the 21 months, in all variables: “troubles in the last 12 months”, “limitations in the last 12 months” and “troubles in the last 7 days”. There were significant improvements in extensor muscle strength and resistance, measured 11 months after following the exercise program (study III). In the long term, a low back specific exercise program modified positively the QoL of workers (study IV). After 21 months of following the exercise program, the dimensions physical functioning, role-physical, bodily pain, social functioning, role-emotional and mental health have improved significantly.
Keywords: occupational health, NMQ, reliability, validity, workers, musculoskeletal symptoms, muscle strength and resistance, specific exercises, QoL, SF-36.


XVII
Lista de Abreviaturas
cm Centímetros
EU European Union
ICC Intraclass Correlation Coefficient
IMC Índice de massa corporal
Kg Quilograma
Kgf Quilograma força
LBP Low back pain
LME Lesões músculo-esqueléticas
M1 Momento 1
M2 Momento 2
M3 Momento 3
MSD Musculoskeletal disorders
MSS Musculoskeletal symptomatology
MSS Musculoskeletal symptoms
NMQ Standardized Nordic musculoskeletal questionnaire
OMS Organização Mundial de Saúde
QNM Questionário Nórdico músculo-esquelético
QoL Quality of life
QV Qualidade de vida
Sf-36 – v2 Short Form Health Survey – versão 2
SME Sintomatologia músculo-esquelética
VAS Visual Analogue Scale


1
Introdução
A Organização Mundial de Saúde (OMS) caracterizou as lesões relacionadas com o trabalho como doenças multifatoriais, devido aos diferentes fatores de risco envolvidos, tais como de organização do trabalho, alterações físicas, psicossociais e socioculturais, assim como ergonómicas, contribuindo para a causa destes problemas (WHO, 1985). Uma das principais controvérsias em volta da sintomatologia músculo-esquelética relacionada com o trabalho é a sua natureza multifatorial. Alguns centros de estudo não estão de acordo na relação entre os fatores de risco múltiplos e individuais no desenvolvimento desta doença (WHO, 1985). Contudo, os distúrbios músculo-esqueléticos são cada vez mais frequentes, tornando-se assim num dos principais problemas dos países industrializados (Airaksinen et al., 2006; Bigos et al., 2009; Borenstein, 2000). Representam uma das principais causas de morbilidade e têm sido descritos, como sendo os sintomas mais habituais de dor severa prolongada e de incapacidade física na população ativa (Airaksinen et al., 2006; Bigos et al., 2009; IJzelenberg & Burdorf, 2004; Meerdinga, IJzelenberga,
Koopmanschapb, Severensc, & Burdorfa, 2005; Rulgulies & Krause, 2005).
Afetam muitos trabalhadores, refletindo um enorme impacto na produtividade, com consequências económicas substanciais e inerentes repercussões no bem-estar social e económico dos trabalhadores, assim como das suas famílias (Airaksinen et al., 2006;Bigos et al., 2009; Butler & Johnson, 2011; Gundewall, Lilequist, & Hansson, 1993; Juul-Kristensen & Jensen, 2005). São vários os estudos que consideram que nas últimas décadas tem havido um aumento de disfunções músculo-esqueléticas (Harrington, 1994; IJzelenberg & Burdorf, 2004; Kuorinka, Alaranta, & Erich, 1995; Morken et al., 2003; Tveito,
Hysing, & Eriksen, 2004).
A European Foundation for the Improvement of Living and Working Conditions (Giaccone, 2007), destaca que Portugal é o terceiro país na UE no
qual os trabalhadores mais faltam devido a lesões músculo-esqueléticas. Em 2001, o National Institute for Occupational Safety and Health baseando-se em
diversas publicações construiu um modelo conceptual para as lesões músculo-esqueléticas. Neste modelo foram determinados possíveis efeitos resultantes da aplicação de cargas. Podem ser de origem externa ou forças internas resultantes dos efeitos dinâmicos e gravitacionais. Estas cargas aplicadas criam respostas internas dos tecidos muscular, ligamentar e nas superfícies articulares. Conforme a dimensão da carga e dos fatores individuais,

2
organizacionais ou sociais, os resultados podem desencadear efeitos de adaptação (aumentos na força, resistência e aptidão física ou serem prejudiciais (tais como dor ou mesmo lesões estruturais nos tendões, nervos, músculos, articulações ou tecidos de suporte), que podem resultar em sintomas dolorosos, disfunção ou incapacidade (Byrns, Reeder, Jin, & Pachis, 2004; Keyserling, Sudarsan, Martin, Haig, & Armstrong, 2005; Roffey, Wai, Bishop,
Kwon, & Dagenais, 2010; Wai, Roffey, Bishop, Kwon, & Dagenais, 2010).
Os trabalhadores são, muitas vezes, sujeitos a movimentos repetitivos e vibratórios, ao levantamento e transporte de pesos, a posturas incorretas por períodos de tempo prolongados e por vezes a longas horas de trabalho (Ala-Mursula, Vahtera, Pentti, & Kivimäki, 2004; Akbar Alipour, Mostafa Ghaffari, Batoul Shariati, Irene Jensen, & Eva Vingard, 2008; Dembe, Erickson, Delbos, & Banks, 2005; Dovrat & Katz-Leurer, 2007; Guo, 2002; Hussain, 2004; Häkkänen, Viikari-Juntura, & Martikainen, 2001; Jansen, Morgenstern, & Burdorf, 2004; Juul-Kristensen & Jensen, 2005; Shimizu, Horie, Nagata, & Marui, 2004; Tveito et al., 2004). Estes fatores colocam os tecidos moles em tensão, surgindo, progressivamente, as lesões músculo-esqueléticas (Bonde et
al., 2005; Jansen et al., 2004; Kuorinka & Patry, 1995).
A sintomatologia músculo-esquelética pode ainda surgir ou ser exacerbada se o trabalho desenvolvido implicar a exposição a temperaturas baixas. Alguns autores, Piedrahíta, Punnett, & Shahnavaz (2004) verificaram uma elevada prevalência de sintomatologia músculo-esquelética (SME) nos trabalhadores de áreas muito frias (2ºC), especialmente na região lombar, pescoço e ombros. Outros autores, referem que o frio diminui a performance muscular, levando, progressivamente, a um aumento de tensão e posterior fadiga precoce (Dovrat & Katz-Leurer, 2007). Por outro lado, a carga psicossocial a que o operário é sujeito, acrescida de um fraco suporte social e baixa satisfação profissional desenvolvem um mecanismo de stress que leva
ao aumento do tónus muscular e à ativação dos recetores da dor potenciando a dor músculo-esquelética (Besler & Can, 2003; Bonde et al., 2005; Cherry,
Meyer, Chen, Holt, & McDonald, 2001; Hoogendoorn et al., 2002)
Segundo a European Foundation for the Improvement of Living and Working Conditions (Giaccone, 2007), as lesões músculo-esqueléticas mais
frequentes nos trabalhadores da EU são a lombalgia (25%) e as dores musculares generalizadas (23%). Os distúrbios músculo-esqueléticos podem ser mensuráveis através da sintomatologia referida por parte dos operários, sendo considerado como sintomatologia a presença de dor, sofrimento ou

3
desconforto. Afeta todas as regiões anatómicas, tanto da coluna vertebral como dos membros superiores ou inferiores (Enthoven, Skargren, Carstensen, & Oberg, 2006; Juul-Kristensen & Jensen, 2005; Kuorinka et al., 1987; Punnett &Wegman, 2004). No entanto, é a lombalgia a condição que implica maior morbilidade e incapacidade, compreendendo custos financeiros consideráveis afetando 58 a 84% dos adultos ativos (Airaksinen et al., 2006; Alexopoulos, Burdorf, & Kalokerinou, 2003; Alexopoulos, Tanagra, Konstantinou, & Burdorf, 2006; Alipour, Ghaffari, Shariati, Jensen, &Vingard, 2008; Bongers, Ijmker, van den Heuvel, & Blatter, 2006; Deyo et al., 1998; Dunn, Jordan, & Croft, 2006; Dunning et al., 2010).
A lombalgia pode restringir a função com consequências pessoais, interpessoais e sociais, como perda de independência, e incapacidade em executar diversas atividades na vida social, podendo interferir ainda com atividades básicas como estar de pé, caminhar e vestir-se, diminuindo a qualidade de vida, assim como as muitas atividades relacionadas com o desempenho profissional (Ceran & Özcan, 2006; Hilfiker et al., 2007; Loisel,
2005; van Tulder, Malmivaara, & Koes, 2007).
A estabilidade e os movimentos permitidos à coluna lombar são determinados pelas estruturas osteoligamentares e musculares do tronco, desempenhando os músculos, ainda, um importante papel protetor sobre as estruturas passivas da coluna vertebral. Quando estas estruturas, por qualquer motivo, se encontram enfraquecidas, os segmentos lombares ficam suscetíveis a lesão (Arokoski, Valta, Airaksinen, & Kankaanpää, 2001; Stevens et al., 2006). Para além dos fatores físicos, diversos estudos comprovam que os fatores psicossociais inerentes ao emprego, como autoridade para decisão, exigência psicológica do trabalho, apoio de supervisores, insatisfação e insegurança do emprego contribuem para o decréscimo do estado de saúde dos trabalhadores (Arnold, Witzeman, Swank, McElroy & Keck Jr, 2000; Edwards, Van Laar, Easton, & Kinman, 2009; Ferreira, 2000b; Moffett, Torgerson, Bell-Syer, Jackson, & Llewlyn-Phillips, 1999). Este tipo de fatores parece potenciar a progressão da dor e incapacidade ao longo do tempo, enquanto os fatores físicos estão mais relacionados com a fase aguda do problema (Lamers, Meerding, Severens, & Brouwer, 2005; Tavafian, Jamshidi,
Mohammad, & Montazeri, 2007).
As convicções que o indivíduo tem acerca da sua dor, levam a que tenha medo do movimento/nova lesão, redução da função e da atividade e consequente exacerbação para uma incapacidade crónica (Urquhart et al.,

4
2008; Vlaeyen, Kole-Snijders, Boeren, & van Eek, 1995). O indivíduo perceciona então uma menor qualidade de vida, que segundo a OMS condiciona a perceção do indivíduo a sua condição de vida, dentro do contexto de cultura e valores em que se insere, das suas metas, expetativas e padrões sociais (Brox et al., 2008; Claiborne, Vandenburgh, Krause& Leung, 2002). De acordo com uma revisão sistemática, van Tulder et al., (2007) de facto as lesões músculo-esqueléticas estão associadas a uma diminuição da qualidade
de vida.
Nas últimas décadas, o exercício tem sido relatado como uma mais-valia no tratamento da dor lombar, parecendo auxiliar pacientes com lombalgia crónica no retomar das atividades normais no seu emprego (Rainville et al., 2004). A realização de programas de prevenção de lesões, (Salinas et al., 2002), como a promoção para a saúde e a realização de exercício físico, têm como objetivo reduzir os possíveis fatores de risco (Eriksen et al., 2002), contribuindo para a redução dos custos diretos com as lesões, bem como para
o aumento da produtividade e qualidade de vida (Salinas et al., 2002).
Os programas de exercício têm provado ser mais eficazes na prevenção e tratamento da dor lombar do que as terapias convencionais, resultando numa redução de sintomatologia dolorosa e maior funcionalidade, diminuindo o absentismo por dor lombar (Moffett et al., 1999). Numa recente revisão os autores encontraram uma forte evidência entre os programas de exercício e a prevenção de problemas lombares (Bigos et al., 2009). Num outro estudo verificaram que existe suporte para que se possa afirmar que os programas de exercício melhoram a flexibilidade e força muscular ao nível do ráquis (Rainville et al., 2004). Contudo, ainda persiste uma certa controvérsia relativamente aos efeitos do exercício, Daltroy et al., (1997) não verificaram efeitos positivos na sua intervenção em trabalhadores industriais. Por outro lado, num estudo mais recente, Brox et al., (2008) verificaram que os programas de exercício eram efetivos na redução de dor e funcionalidade, mas apenas a curto prazo, e IJzelenberg, Meerding, & Burdorf (2007) não verificaram melhoras significativas com o seu programa. Estes resultados poderão ser devidos a problemas de comunicação ou à insatisfação e altas expectativas criadas (Goldby, Moore,
Doust, & Trew, 2006; Sherman, Cherkin, Erro, Miglioretti, & Deyo, 2005).
Um programa de exercícios bem estruturado deverá levar à diminuição de sintomatologia, diminuição de dor e aumento de força que permita aos indivíduos realizarem as suas tarefas com menor esforço, resultando numa melhoria da qualidade de vida (Airaksinen et al., 2006; Arnold, Witzeman,

5
Swank, McElroy& Keck Jr, 2000; Carroll & Whyte, 2003; Lang, Liebig, Kastner, Neundörfer& Heuschmann, 2003; Moffet, 1999).
Apesar de as guidelines europeias não recomendarem o tipo e intensidade do exercício, estas preconizam que os programas deverão ser realizados tendo em conta as tarefas e movimentos repetidos que os indivíduos realizam durante o seu trabalho (Airaksinen et al., 2006; Burton et al., 2006). Os trabalhadores deverão receber instruções de como se efetuam os exercícios, devendo-se reforçar a ideia de que os fatores físicos, sociais e mentais são os alicerces da qualidade de vida (Airaksinen et al., 2006; Burton
et al., 2006).
Assim, com este trabalho pretendeu-se avaliar os efeitos de um programa de exercícios específicos em indivíduos operadores de armazém da indústria alimentar durante 21meses.
O programa de intervenção considerou a sintomatologia músculo-esquelética, força e resistência dos músculos da região lombar e a qualidade
vida.
Uma vez que são vários os objetivos deste trabalho, optou-se por apresentar uma breve revisão bibliográfica, os objetivos e os métodos, seguida de quatro capítulos com os diversos estudos resultantes. Segue-se uma
discussão geral e por fim as principais conclusões.


7
Revisão da literatura
Lesões músculo-esqueléticas
Desde o início do século XVIII, as lesões músculo-esqueléticas (LME) foram reconhecidas como tendo por base fatores etiológicos e ocupacionais. No entanto, só a partir da década de 1970 é que os fatores ocupacionais foram estudados utilizando métodos epidemiológicos, e os estudos que relacionavam o trabalho com esses fatores começaram a aparecer regularmente na literatura científica internacional. Desde então, a evidência resultante do desenvolvimento de mais de seis mil artigos científicos publicados apenas abordam a importância da ergonomia no local de trabalho (Bernard, 1997). No entanto, a relação entre as lesões músculo-esqueléticas relacionadas com o trabalho e diversos fatores, continua a ser um assunto de debate (Bernard, 1997). O mesmo tipo de controvérsia tem sido tema de estudo no âmbito de outras patologias, nomeadamente os problemas pulmonares e o cancro, ambos com causas multifatoriais (Bernard, 1997).
Com o mercado cada vez mais competitivo, hoje em dia a produtividade é a palavra de ordem, e as empresas procuram diferentes estratégias para sobreviver a esta nova realidade (Tuomi, Vanhala, Nykyri, & Janhonen, 2004). Algumas seguem a estratégia da melhoria da qualidade, modificando-se na sua produtividade e na sua estrutura organizacional. Porém, as dificuldades encontradas na implementação de uma melhor qualidade, devem-se sobretudo, à escassez de recursos humanos especializados em que as máquinas são indispensáveis e o homem é considerado apenas mais um elemento do sistema de produção, tendo este que se adaptar às mudanças do processo, muitas vezes inadequado às suas características individuais (Costa, 2003). Na maioria dos postos de trabalho cada sujeito desempenha as suas atividades específicas limitadas por um determinado período de tempo, quase sempre reduzido, induzindo os trabalhadores a desempenhar as suas funções no tempo devido, mesmo quando isso coloque em risco a sua saúde (Costa, 2003). Este tipo de convicção leva muitas vezes a incapacidades e limitações funcionais nas atividades de vida diária, bem como profissional, restringindo a participação do indivíduo na sociedade (Meijsen & Knibbe, 2007; van
Nieuwenhuyse et al., 2006)
Num contexto de trabalho, observa-se que as desordens músculo-esqueléticas, nomeadamente ao nível lombar, cervical e membros superiores,

8
são um problema de saúde com impacto importante (Bongers, Ijmker, van den Heuvel& Blatter, 2006; Klussmann, Gebhardt, Liebers, & Rieger, 2008), que conduz a custos elevados em cuidados de saúde, salários perdidos devido a períodos de baixa laboral e redução da produtividade (Côté, Cassidy, Carroll, &
Kristman, 2004; Szabo, 2001).
As desordens músculo-esqueléticas são consideradas um problema multifatorial já com identificação de principais fatores de risco: físicos, psicossociais e individuais. A nível físico, a realização de tarefas que exijam níveis elevados de força, o grande número de repetições de um determinado movimento, a vibração e as posturas incorretas foram os principais fatores responsáveis pelo surgimento de sintomatologia músculo-esquelética nesta área (Alexopoulos, Tanagra, Konstantunou, & Burdof, 2006; Bongers et al.,
2006; Goldsheyder, Nordin, Weiner, & Hiebert, 2002).
Dentro dos fatores psicossociais, estudos realizados em contexto empresarial revelam que estes se prendem com fatores como: os altos grau de exigência no local de trabalho, o baixo apoio social recebido, assim como o insuficiente apoio entre colegas, pouca autonomia relativamente às tarefas e horários atribuídos, o elevado stress psicológico e também a baixa satisfação (Lotters, Franche, Hogg-Johnson, Burdorf, & Pole, 2006; McClelland & McCubbin, 2008; Nahit et al., 2003). Os sintomas depressivos, a perceção de baixa condição física e de saúde, foram considerados preditores significativos de maior número de dias de baixa médica e, parecem constituir fatores de risco importantes para incapacidade laboral prolongada (Alexopoulos et al., 2006; Arnold et al., 2000; Lotters et al., 2006).
Numa revisão sistemática, May (2010) identificou a osteoartrite e a dor lombar crónica como os dois problemas músculo-esqueléticos mais prevalentes na população em geral. Esta caracteriza-se pela elevada frequência, estando associada a elevados custos para a sociedade, diretos e indiretos. Estes resultados epidemiológicos proporcionam uma imagem da realidade que justifica a utilização de estratégias de autogestão a fim de minimizar estes problemas (Airaksinen et al., 2006; Bigos et al., 2009; Bongers et al., 2006; Gundewall, Liljeqvist, & Hansson, 1993; Kent & Keating, 2005; Porter & Gyi, 2002; Trainor & Wiesel, 2002). Como definição de autogestão entenda-se uma ligação entre profissionais de saúde e indivíduos com necessidades nesse sentido, bem como atividades de promoção da saúde independente (May, 2010). Estratégias de autogestão independentes, como o exercício e a automedicação, são praticadas por indivíduos na população em geral sendo o

9
exercício uma estratégia eficaz na gestão de dor lombar crónica e osteoartrite, sem que no entanto não esteja claro o que é “o exercício ideal”. Contudo, o exercício, suportado pelo aconselhamento e educação, deve estar no cerne das estratégias de autogestão para dor lombar crónica (Brox et al., 2008; Burton et al., 2006; Cancelliere, Cassidy, Ammendolia, & Côté, 2011; Giaccone, 2007; Holmstrom & Ahlborg, 2005; May, 2010; May & Rosedale, 2009; Moses, Heestand, Doyle, & O'Sullivan, 2006; T. H. Tveito, M. Hysing, & H. R. Eriksen,
2004; van Oostrom et al., 2009).
Lombalgia (etiologia, fisiopatologia)
A etiologia da dor lombar é muitas vezes atribuída às tarefas e condições de trabalho (Bigos et al., 2009). A combinação do profundo esforço físico e de intensidade, posturas incorretas, exposição aos condicionamentos ambientais e a tempo de recuperação insuficiente contribuem para o aumento de lombalgias, tanto de repetição como o aparecimento de situações agudas (Arokoski et al., 1999; Borenstein, 2000; Goldsheyder et al., 2002; Piedrahíta et
al., 2004).
Chaffin e Park (1973) verificaram que a sintomatologia lombar, incluindo lesões, foi três vezes mais prevalente nos trabalhadores que apresentavam um nível de força inferior ao necessário para a execução das suas tarefas laborais. Na maioria dos casos, é difícil identificar uma causa anátomo-patológica específica para a origem da lombalgia (Fritz, Erhard, & Hagen, 1998; Hicks, Fritz, Delitto, & McGill, 2005; O'Sullivan et al., 2006). Segundo Fritz (1998) os indivíduos com diagnósticos de lombalgia sem etiologia específica são
usualmente incluídos no grupo das lombalgias de origem mecânica.
A lombalgia de origem mecânica é um termo que descreve a dor lombar resultante do esforço físico e que é aliviada com o repouso. Deve-se, geralmente, a disfunções na musculatura posterior do tronco, tendões e ligamentos e pode ser agravada em atividades como levantar pesos, permanecer em posições estáticas prolongadas, tanto na posição de pé como sentada. Indivíduos com este tipo de lombalgia referem sentir um “peso” e uma sensação dolorosa que piora ao final do dia em decorrência de atividades e esforço físico (Cholewicki & McGill, 1996; Imamura, Kaziyama, & Imamura, 2001). A estabilidade dada à coluna vertebral durante a realização dos mais variados movimentos no quotidiano é garantida, principalmente, pelo sistema muscular (Lee et al., 1999; Norris, 1995; O'Sullivan, 2000; Richardson, Jull,

10
Toppenberg, & Comerford, 1992). Quando este falha, ou se encontra enfraquecido, há um aumento da sobrecarga sobre as articulações e ligamentos espinhais (Hodges, 1999). Assim, será mais provável que ocorra uma lesão a nível da coluna lombar (Richardson et al., 1992). Krajcarski et al. (1999) verificaram que a pré-ativação dos músculos extensores do tronco podem servir para reduzir a deslocação do disco intervertebral aquando do movimento de flexão rápido e em carga. A diminuição da força e da resistência dos músculos do tronco surge como um factor de risco primário na ocorrência da lombalgia (Critchley, 2002). Vários estudos verificaram que indivíduos com disfunção da coluna lombar apresentam, na maior parte dos casos, uma diminuição significativa da força e da resistência dos músculos estabilizadores da coluna, comparativamente a indivíduos saudáveis (Arokoski, Valta, Kankaanpää, & Airaksinen, 2004; Costa & Palma, 2005; Gonçalves & Barbosa, 2005; Ismaeil, Hosseini, Salavati, Farahini, & Arab, 2005; Moffroid, 1997; Sung, 2003; Udermann, Mayer, Graves, &Murray, 2003). Os músculos extensores e flexores do tronco são importantes estabilizadores da coluna vertebral, contudo os músculos profundos com inserções nas apófises vertebrais lombares proporcionam uma maior estabilidade intersegmentar, pelo que os músculos multífidos e o transverso abdominal (via fáscia toracolombar) parecem desempenhar o papel principal na estabilização da coluna lombar (Arokoski et al., 2004; Costa & Palma, 2005; Critchley, 2002). De facto, não só a força muscular mas também a resistência parecem estar relacionadas com o aparecimento de dor na região lombar (Arokoski et al., 1999; Arokoski, Valta, Airaksinen, & Kankaanpaa, 2001; Hodges, 1999; Maher et al., 2005; Nourbakhsh & Arab, 2002; O'Sullivan et al., 2006; Roussel et al., 2006; Yang, Marras, & Best, 2011). Os investigadores atribuem a diminuição da resistência dos extensores do tronco encontrada em doentes com lombalgia, a vários fatores, tais como: alto nível metabólico do músculo resultante de tensão prolongada; grande proporção de fibras do tipo II nos músculos para-espinhais, especialmente os multífidos; descondicionamento físico; desequilíbrio na coordenação muscular e inadequada distribuição da força muscular extensora (Arokoski et al., 1999; Arokoski et al., 2001; Hodges, 1999; Maher et al., 2005; Nourbakhsh & Arab, 2002; O'Sullivan et al., 2006; Roussel et al., 2006; Yang et
al., 2011).
Segundo Trainor (2002) o rácio de força entre extensores/flexores do tronco deveria ser de 1.3/1. Estudos têm revelado que pacientes com lombalgia têm este rácio alterado comparativamente à população normal (Lee et al., 1999) verificando-se uma relação de 1.2/1 a 1.5/1 em indivíduos assintomáticos

11
(propensos à aquisição da doença) e de 1.0/1 em alguns casos de indivíduos com lombalgia crónica (Costa, 2003). A falta de suporte dado pela musculatura extensora do tronco pode ocorrer devido à fraqueza muscular, associada,
muitas vezes ao sedentarismo.
Num estudo realizado com o objetivo de investigar a associação entre dezassete fatores mecânicos e a ocorrência de dor lombar concluiu-se que, a diminuição da força e resistência musculares do tronco, estavam associados à ocorrência de lombalgia; os fatores estruturais como a lordose lombar, tilt
pélvico, discrepância no tamanho dos membros, comprimento dos abdominais, isquiotibiais e iliopsoas não estavam relacionados com a ocorrência de dor lombar (Nourbakhsh & Arab, 2002). Alguns estudos concluíram que os músculos mais envolvidos na estabilização da coluna lombar são os oblíquos do abdómen e o transverso abdominal em co-ativação com o eretor da espinha (Richardson, Jull, Toppenberg, & Comerford, 1992; Trainor & Wiesel, 2002). Os músculos abdominais oblíquos, especialmente os oblíquos externos, rapidamente aumentam os níveis de ativação em resposta ao movimento rápido. Quando os níveis de pré-ativação são baixos o tronco fica rígido exercendo-se forças compressivas no disco e estruturas moles adjacentes. Algumas lesões ocorrem devido a erros de controlo motor (Krajcarski, Potvin, & Chiang, 1999). Estes são eventos aleatórios, mas são mais prováveis em pessoas com um sistema de controlo motor pobre (Brereton & McGill, 1999). Assim, uma lesão na região lombar pode ocorrer mesmo numa tarefa simples se não houver aviso de sobrecarga.
A resistência é importante porque com tarefas repetitivas os músculos entram em fadiga (McGill, Childs, &Liebenson, 1999). McGill, Sharratt, &Seguin (1995) observaram que as pessoas têm diferentes capacidades em suportar uma carga nas mãos e respirar "arduamente".Vários autores acreditam que uma condição física pobre associada à fraqueza, quer dos músculos abdominais quer dos extensores do tronco, são fatores importantes no desenvolvimento e persistência de lombalgia (Besler & Can, 2003; Rantanen, Airaksinen, & Penttinen, 1994). Outros autores vão mais longe e salientam mesmo o importante papel da musculatura extensora na prevenção de lombalgia (Arokoski et al., 2001; Arokoski, Valta, Kankaanpaa, & Airaksinen, 2004; Hodges & Richardson, 1998; Peltonen et al., 1998; Rissanen et al., 2002; Roussel et al., 2006). Alguns estudos sugerem que indivíduos que possuem músculos fortes, principalmente os extensores lombares, sofrem menos desta patologia (Besler & Can, 2003; Ng, Richardson, Kippers, & Parnianpour, 1998).

12
Por outro lado, outros autores afirmam que o enfraquecimento dos músculos do tronco não está relacionado com a incidência de dor lombar (Johannsen et al.,
1995; Mostardi, Noe, Kovacik, & Porterfield, 1992).
A realização de movimentos repetitivos, ou aquisição de certas posturas viciosas, como é o caso da maioria dos indivíduos, pode levar a um maior desenvolvimento de determinados músculos em detrimento de outros, gerando
desequilíbrios musculares (Comerford & Mottram, 2001; Rissanen et al., 2002).
Potvin & O’Brien (1998) constataram que a fadiga é resultado de uma mudança nos padrões de recrutamento dos músculos do tronco, estes, que atuam como estabilizadores, durante um movimento prolongado de rotação e flexão, passam a funcionar como antagonistas, exigindo mais força e mais rapidamente entram em fadiga. A postura sentada leva à inatividade que pode ser prejudicial (Bernard, 1997; Besler & Can, 2003). A falta de movimento leva a um acúmulo de metabolitos, que provavelmente aceleram a degeneração dos discos e aumentam a probabilidade de estrangulamento do disco (Bigos et al., 2009; Brereton & McGill, 1999; Dunn, Jordan, & Croft, 2006). As posturas de condutores de máquinas, também podem levar a problemas músculo-esqueléticos na região cervical, lombar, ombros e membros superiores. No local de trabalho, em pé e sentado são as duas formas básicas de posturas (Fathallah, Marras, & Parnianpour, 1997; Gagnon & Smyth, 1992). Essas posturas têm vantagens específicas e desvantagens para a mobilidade, exercícios de força, consumo de energia, sistema circulatório, coordenação e controle de movimento (Friedrich, Karnzl, Heller, Kirtley, & Cermak, 2000; Marras, Lavende, Fergunson, Splittstoesser, & Yang, 2010). A estabilidade e os movimentos permitidos à coluna lombar são determinados pelas estruturas osteo-ligamentares e musculares do tronco, desempenhando o músculo, ainda, um importante papel protetor sobre as estruturas passivas da coluna vertebral. Quando estas estruturas, por qualquer motivo, se encontram enfraquecidas, os segmentos lombares ficam suscetíveis a lesão (Arokoski et al., 2001; Stevens et al., 2006). Muitas vezes, a dificuldade em manter dupla tarefa, pode ser importante para a compreensão de que os músculos necessários para evitar deformações na coluna estão permanentemente a ser requisitados para a ventilação, podendo comprometer a elasticidade pulmonar (McGill, Sharratt, &
Seguin, 1995).

13
Qualidade de vida
Sendo a região lombar uma importante zona de suporte e de transferência de forças, as alterações acompanhadas de dor terão impacto na qualidade de vida do indivíduo, pela diminuição da função física e deterioração da saúde no geral. A presença da dor quer seja pontual ou constante, induz no indivíduo uma situação de desconforto, comprometendo as atividades da vida diária, reduzindo a sua participação nas atividades sociais e lúdicas, nas atividades familiares e ainda na atividade laboral, com todas as consequências que daí
advêm (Claiborne et al., 2002; Galukande, Muwazi, & Mugi, 2005).
A perceção que o indivíduo tem acerca da dor, leva a que reduza os movimentos pela antecipação da dor ou eventual lesão. Esta condição leva à redução da função e da atividade, e consequentemente à exacerbação da incapacidade, com evolução desta para uma condição crónica (Urquhart et al., 2008; Vlaeyen et al., 1995). Este ciclo induz uma menor qualidade de vida, que segundo a OMS resulta da perceção do indivíduo sobre a sua condição de vida, dentro do contexto de cultura e valores em que se insere, e das suas metas, expetativas e padrões sociais (Brox et al., 2008; Claiborne et al., 2002). Esta evidência foi reforçada por uma recente revisão realizada por van Tulder et al. (2007), onde referem que de facto as lesões músculo-esqueléticas estão associadas a uma diminuição da qualidade de vida.
Para além dos fatores físicos, diversos estudos comprovam que os fatores psicossociais inerentes ao trabalho, como autoridade para decisão, exigência psicológica do trabalho, apoio de supervisores, insatisfação e insegurança do emprego têm também o seu contributo para o decréscimo do estado de saúde dos trabalhadores (Arnold et al., 2000; Edwards et al., 2009; Ferreira, 2000b; Moffett et al., 1999). Este tipo de fatores parece potenciar a progressão da dor e incapacidade ao longo do tempo, estando os fatores físicos mais relacionados com a fase aguda do problema (Lamers et al., 2005; Tavafian et al., 2007).
A saúde relacionada com a qualidade de vida é uma vertente multidisciplinar que mede a capacidade de um indivíduo face às diferentes funções, emoções do seu quotidiano e ao impacto da dor nas suas atividades diárias (Claiborne et al., 2002). A satisfação do indivíduo, isto é, a avaliação do mesmo relativamente aos seus cuidados de saúde de acordo com as expetativas iniciais, é uma forma subjetiva importante de medida do estado de saúde. A redução dos sintomas subjetivos leva a um aumento da qualidade de

14
vida e do bem-estar, condições essenciais para o conceito de saúde (Hemingway, Stafforf, Stansfeld, Shipley, & Marmot, 1997; Lang, Liebig, Kastner, Neundörfer, & Heuschmann, 2003; Sculco, Paup, Fernhall, & Sculco,
2001).
O exercício aumenta a qualidade de vida, resultando num aumento da funcionalidade e performance dos indivíduos (Airaksinen et al., 2006; Claiborne, Vandenburgh, Krause, & Leung, 2002). Percebe-se assim a importância da reabilitação quer dos extensores quer dos abdominais do tronco quando se fala em alcançar a máxima performance possível (Essendrop, Maul,
Läubli, Riihimäki, & Schibye, 2002).
Importância dos programas de exercício físico
O comportamento natural do ser humano é mudar a postura muitas vezes. Mesmo durante o sono, há uma necessidade de ajustes de postura. Nenhuma posição deve ser mantida por um longo período de tempo sem desconforto considerável. Embora possa vir a ser um problema, a prevenção é, de longe, o tratamento de escolha. Os efeitos combinados da comunidade médica, trabalhadores e administradores são necessários para causar algum impacto sobre este problema (Keyserling, Martin, Sudarsan, Haig, & Armstrong, 2005; Pope, Goh, & Magnusson, 2002; Poppel, Hooftman, & Koes, 2004). De facto vários são os estudos que demonstram melhorias nas escalas globais de dor, assim como nas estratégias de lidar com síndromes lombares (Andersen et al., 2010; Bigos et al., 2009; Borenstein, 2000; Brox et al., 2008; Byrne, Doody, & Hurley, 2006; Carroll, Rick, Pilgrim, Cameron, & Hillage, 2010; Ceran & Ozcan, 2006; Costa & Palma, 2005; Denis, St-Vincent, Imbeau, Jette, & Nastasia, 2008; Descarreaux, Normand, Laurencelle, & Dugas, 2002; Gerr et al., 2005; Hildebrandt & Neufer, 2000; Hlobil et al., 2005; Holmstrom & Ahlborg, 2005; Johannsen et al., 1995; Kaser et al., 2001; Lee et al., 1999; Maher, 2000; McGill, Childs, & Liebenson, 1999; Moffroid, 1997; Moseley, 2002; Rainville, Hartigan, Jouve, & Martinez, 2004; Rainville, Hartigan, Martinez, et al., 2004; Stevens et al., 2006; Tuncel, 2006; Tveito & Eriksen, 2009; Tveito et al., 2004;
Udermann, Mayer, Graves, & Murray, 2003).
Foram realizados vários estudos onde se verificou que os indivíduos na presença de dor subaguda respondem restringindo a atividade física para se protegerem da dor e de possíveis lesões ao nível da coluna, sendo esta, uma reação de medo normal em pacientes sintomáticos (Brox, Storheim, Holm,

15
Friis, & Reikeras, 2005). Todo este processo vai condicionar a qualidade de vida do indivíduo ao impedi-lo de realizar as suas tarefas e atividades diárias, sociais e laborais da forma habitual, devido a uma consequente diminuição da
funcionalidade (Rainville et al., 2004).
A prevenção/tratamento através de classes de exercícios tem evidenciado resultados mais eficientes relativamente ao tratamento conservador, apresentando não só redução da dor ao nível lombar e da incapacidade, mas também menores custos, com menor necessidade de recorrer aos serviços de saúde e menor absentismo laboral por dor lombar (Merkesdal & Mau, 2005). Tudo isto se traduz em aumento de qualidade de vida para o indivíduo, proporcionando-lhe através do exercício o aumento do seu desempenho a nível profissional, melhorando também a sua funcionalidade (Claiborne et al., 2002). Pelo que um programa de exercícios bem estruturados leva, a longo prazo, a uma redução da dor lombar (Merkesdal & Mau, 2005). Estes mesmos programas de exercícios específicos para a região lombar têm-se demonstrado eficazes na diminuição da dor, reduzindo assim o desempenho necessário exigido pelas atividades diárias, assim como na incapacidade (Lang et al., 2003), induzindo assim uma melhoria significativa da qualidade de vida nos indivíduos (Merkesdal & Mau, 2005; van Poppel, Hooftman, & Koes, 2004).
Morken et al. (2003) verificaram que mais de um terço dos sintomas músculo-esqueléticos relacionados com o trabalho podia ser evitado. Uma das formas seria um programa de intervenção para a lombalgia através do exercício físico (Airaksinen et al., 2006; Maher et al., 2005; Tveito et al., 2004). Alguns estudos relatam que uma elevada satisfação por parte do indivíduo, no que se refere à sua saúde ocupacional, pode estar relacionada com uma melhor compreensão e adesão ao tratamento (NORA, 2001; Rainville et al.,
2004).
Alguns empregadores têm vindo a implementar medidas para reduzir a carga de trabalho aos seus colaboradores na tentativa de reduzir a incidência de sintomatologia dolorosa e doenças relacionadas com o trabalho de forma a reduzir o absentismo, assim como os custos decorrentes. Para além dessas medidas têm feito ajustes ergonómicos no local de trabalho que podem consistir em programas educativos de educação ou formação. Este tipo de intervenção consiste no ensino de manuseamento e levantamento de cargas, incluindo a prescrição de suportes lombares e programas de exercícios
(Airaksinen et al., 2006; Brox et al., 2008; van Poppel et al., 2004).


17
Objetivos
Os objetivos deste estudo foram avaliar os efeitos de um programa de exercícios específicos a médio e longo prazo, em operários de um armazém de distribuição da indústria alimentar. Para que se pudesse concretizar estes
objetivos foi necessário:
� Adaptar para a população portuguesa um instrumento que avaliasse a sintomatologia músculo-esquelética tendo-se optado pelo standardized
Nordic musculoskeletal questionnaire;
� Analisar a sintomatologia músculo-esquelética ao nível das regiões do pescoço, ombros, cotovelos, mãos/punhos, torácica, lombar,
ancas/coxas, joelhos e pés/tornozelos, durante 21 meses;
� Medir a força máxima e resistência dos flexores e extensores lombares,
durante 11 meses;
� Avaliar a perceção da saúde relacionada com a qualidade de vida nas dimensões Função Física, Desempenho Físico, Dor Física, Saúde em Geral, Vitalidade, Função Social, Desempenho Emocional e Saúde
mental, durante 21 meses.


19
Material e Métodos
Amostra
A população utilizada neste estudo incluiu 557 trabalhadores do sexo masculino de um armazém de uma empresa de distribuição de alimentos na cidade do Porto. Todos os trabalhadores, do sexo masculino, estavam envolvidos em uma rotina de tarefas sobrecarga e / ou movimentos repetitivos e eles trabalharam sob baixas temperaturas (entre 0 º e 4 º C) durante todas as estações do ano. De acordo com as normas da empresa, todos os trabalhadores usavam roupas de proteção para o frio (blusão, luvas e botas) e cintas de apoio lombar. Os critérios de seleção foram enviados para a empresa (equipa de Medicina do Trabalho e equipa de recursos humanos).
A empresa apresentou uma lista de trabalhadores elegíveis organizados em ordem alfabética de 249 trabalhadores, correspondendo a 45% da população. Aleatoriamente dividiu-se em dois grupos (125 no grupo intervenção e 124 no grupo controlo). De seguida foi solicitado aos trabalhadores que se voluntariassem para participar no estudo, tendo que dar um consentimento por escrito. Os voluntários foram 112 para o grupo intervenção e 117 para o grupo controlo; no início do estudo a amostra foi de
n=229 equivalente a 41% da população.
Incluíram-se os indivíduos que preenchessem os seguintes critérios: um contrato para três ou mais anos e que realizassem o mesmo tipo de tarefa (montagem e desmontagem de paletes). Excluíram-se os indivíduos que: a) eram obrigados a rodar postos de trabalho; b) absentismo no último ano devido a dor nas costas; c) tivessem dor forte nas costas (VAS ≥ 5) no último ano; d) tivessem realizado tratamento (conservador ou cirúrgico) à região lombar durante o último ano, e) se existisse qualquer tipo de patologia diagnosticada
que impedisse a prática exercício físico (Sculco et al., 2001).
Da primeira para a segunda avaliação houve uma perda total de 37,5% dos indivíduos, 29.4% no grupo de intervenção e 44,4% no grupo controlo, assim no momento 2 ficaram 151 trabalhadores dos quais 79 no grupo de intervenção e 72 no de controlo. Do segundo para o terceiro momento de avaliação houve uma perda de 34,2% dos indivíduos, 38,5% do grupo
intervenção e 39,2% do grupo controlo.

20
Desde o primeiro ao terceiro momentos de avaliação, as perdas nos grupos de intervenção e controlo foram de 57% e 60%, respetivamente. Depois
de 21 meses a amostra ficou reduzida a aproximadamente 17% da população.
Estas perdas foram de trabalhadores que deixaram a empresa, a mudanças do local de trabalho, não responderem aos questionários e,
nalgumas situações, à falta de motivação para continuar no estudo.
A Tabela 1 mostra os valores de média, desvio padrão, mínimo e máximo para a idade (anos), altura (cm), peso (kg) e índice de massa corporal (IMC) dos trabalhadores incluídos em grupos intervenção e controlo no
Momento 1, antes da intervenção.
Tabela 1: Valores de média, desvio padrão, mínimo e máximo de idade (anos), altura (cm), peso (kg) e IMC dos trabalhadores dos grupos de intervenção e de controlo.
Instrumentos
Questionário de Saúde Geral
Este questionário teve como objetivo fazer a caraterização dos indivíduos, quanto às variáveis demográficas, assim como em relação a alguns hábitos dos indivíduos (Anexo 1).
Questionário Nórdico Músculo Esquelético
Para avaliar a sintomatologia músculo-esquelética dos indivíduos usou-se o Questionário Nórdico músculo-esquelético validado para a população
n=229
Grupo de Intervenção
n=112
Grupo de controlo
n=117
média±dp min Max média±dp min Max
Idade (anos) 34.41±8.36 20 49 33.05±10.19 18 56
Altura (cm) 173.0±0.07 160.0 188.0 178.0±0.09 159.0 188.0
Peso (kg) 76.54±10.44 55 95 81.07±16.84 60 110
IMC (kg/m 2) 25.57 21.48 26.91 25.58 23.81 31.16

21
portuguesa (Mesquita, Ribeiro, & Moreira, 2010). A primeira parte do QNM consiste em questões de escolha dicotómica (Sim ou Não) acerca da ocorrência de sintomas em nove regiões anatómicas. Cada operário deve relatar a ocorrência de SME tendo em consideração os 12 meses e os 7 dias anteriores ao dia do preenchimento do questionário, bem como, relatar se nos últimos 12 meses sentiu alguma limitação nas atividades funcionais pessoais e
ocupacionais (Anexo 2).
Dinamómetro Eletrónico
Para a mensuração da força máxima isométrica foi utilizado o dinamómetro eletrónico isométrico (Globus Ergometer, Globus, Codigné, Italy) para a medição da força máxima isométrica dos grupos musculares flexor e extensor do tronco. É um instrumento de fácil instalação e manuseamento que avalia a força em quilograma força (Kgf) e da resistência, em segundos (Seg). O dinamómetro eletrónico isométrico apresenta uma elevada fiabilidade inter-sessão ICC=0.94 e inter-observador ICC=0.98 (Dankaerts, O'Sullivan, Burnett,
Straker, & Danneels, 2004).
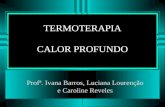
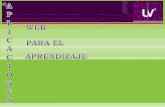
Foram utilizados mosquetões e uma banda de suporte adjacente ao dinamómetro (Fig.1, 2 3 4) para a realização dos testes e, ainda, um
cronómetro Swatch® para controlar os períodos de repouso.
Figura. 1 Figura. 2

22
Figura. 3 Figura. 4
Short Form Health Survey – versão 2 (Sf-36 – v2)
Para a avaliação da qualidade de vida foi utilizado o questionário de auto preenchimento validado para a população portuguesa (Ferreira, 2000a, 2000b). Este é um questionário genérico de estado de saúde desenhado para avaliar o impacto da doença sobre a qualidade de vida (Ware & Sherbourne, 1992). O SF-36 mede o estado de saúde segundo oito dimensões: Função Física (10 itens), Desempenho Físico (4itens), Dor Física (2itens), Saúde em Geral (5itens), Vitalidade (4itens), Função Social (2itens), Desempenho Emocional
(3itens) e Saúde Mental (5itens).
A avaliação da limitação da Função Física é quantificada pela capacidade do indivíduo executar tarefas leves (tomar banho, vestir-se sozinho, caminhar), tarefas moderadas (levantar ou pegar em sacos de mercearia, subir um lanço de escadas) ou tarefas mais violentas como desportos radicais. Para a avaliação do Desempenho Físico e Emocional a medição é realizada em detrimento da quantidade e tipo de trabalho executado, da limitação das tarefas executadas habitualmente e da necessidade de redução do tempo de trabalho.

23
Relativamente à Função Social do indivíduo, são cotadas a quantidade e a qualidade das atividades sociais realizadas e o impacto da limitação física e emocional sobre essas mesmas atividades. A dor corporal é classificada segundo a intensidade e o incómodo que causa e ainda a forma como intervém nas atividades do paciente. Quanto à Saúde Geral, esta é avaliada através de uma escala que descreve o estado de saúde da pessoa relativamente à condição atual, a resistência à doença e ainda a aparência saudável. A Vitalidade permite captar as diferenças de bem-estar, tendo em conta os níveis de energia e de fadiga. A avaliação da Saúde Mental corresponde às questões dirigidas para a ansiedade, depressão, controlo comportamental e emocional
assim como bem-estar psicológico.
Este questionário apresenta 10 questões com várias alíneas, cada uma com uma cotação que traduz a quantidade de cada dimensão. Cada alínea foi traduzida numericamente e o posterior somatório traduz um resultado que varia entre “0”, que corresponde à pior qualidade de vida e “100”, que corresponde à
melhor qualidade de vida possível (Anexo 3).
Procedimentos
Inicialmente, foram realizadas várias visitas às instalações do armazém para conhecer o tipo de tarefas executadas pelos trabalhadores, fotografar e filmar as diferentes atividades realizadas ao longo de um dia de trabalho. Perceber quais os principais problemas dos indivíduos, pedindo a sua colaboração no futuro projeto, dando sugestões. Após a avaliação dos riscos e gestos mais repetidos, foi criado um programa de exercícios (Anexo 4).
Este programa incluiu oito exercícios de fácil execução para promover alongamento e fortalecimento dos tecidos moles responsáveis pela estabilidade da coluna vertebral, especialmente a estabilidade lombar. O programa de exercícios salientou mais o fortalecimento dos extensores lombares e foi criado para ser executado diariamente com duração entre cinco a nove minutos, no início do tempo de trabalho e preferencialmente no posto de trabalho.
Para motivar os trabalhadores a aderir ao programa e segui-lo, houve várias sessões de formação e cartazes que ilustravam o programa de exercícios. Paralelamente um grupo de fisioterapeutas esteve presente diariamente nas primeiras duas semanas, no início de cada turno de trabalho (07h30, 15h30 e 23h30). Após os 15 dias, as visitas passaram a ser em dias alternados durante mais duas semanas. Nas quatro semanas seguintes passou-se a fazer as visitas duas e uma vez por semana. No final das oito

24
semanas passou-se a fazer visitas quinzenais durante todo o período em que se realizou o estudo.
Estas visitas visaram a educação na realização dos exercícios, correção de eventuais erros de execução e responder a dúvidas e perguntas dos trabalhadores quanto ao programa de exercícios e à sua saúde em geral. A eficácia do programa foi avaliada em três momentos: antes da aplicação do programa de exercícios (M1), após 11 meses (M2) e no final, após 21 meses (M3).
O grupo controlo participou nos pré e pós testes. Após a conclusão da intervenção foi-lhes oferecido o mesmo programa de intervenção. O estudo foi realizado entre Fevereiro de 2005 e Março de 2007.
O estudo foi realizado com autorização da empresa, e de acordo com o protocolo entre as instituições envolvidas. Todos os participantes forneceram consentimento informado antes de entrar no estudo, de acordo com a Declaração de Helsínquia.
O estudo foi aprovado pela Comissão de Ética da Escola Superior de Tecnologia da Saúde do Instituto Politécnico do Porto.

Capitulo 1
Portuguese Version of the Standardized Nordic
musculoskeletal questionnaire: cross cultural and r eliability


27

28

29

30

31

32

33


Capitulo 2
An exercise program decreases low back symptoms of workers
(SUBMETIDO PARA PUBLICAÇÃO NO Scandinavian Journal of Work, Environment & Health)


37
ABSTRACT
Background
Musculoskeletal symptoms are associated with pain, problems and functional limitations.
Specific exercise can improve daily life activities and well-being, resulting in better professional
performance and functionality.
Aim
The purpose of this study was to evaluate the effect of following a 21-month exercise program
on the musculoskeletal symptoms of warehouse workers.
Methods
The population included 557 warehouse male workers from a food distribution company in
Oporto/Portugal. Upon application of the selection criteria, 249 workers were deemed eligible,
which were randomised in two groups (125 in the intervention group and 124 in the control
group). Then, subjects were asked to volunteer for the study, being the sample formed by 229
workers (112 in the intervention group and 117 in the control group). All subjects completed the
Portuguese version of the Nordic Musculoskeletal Questionnaire at baseline (M1) and at 11(M2)
and 22(M3) months of follow-up. The exercises were executed in the company facilities once a
day for eight minutes. Data were analysed using SPSS® 17.0 for Windows®.
Results
The most common symptom, with higher proportion across all points of assessment, was the
low back region, followed by the neck, in both groups before intervention. In the intervention
group, improvements were statistically significant in the low back, in the variable “troubles in the
last 12 months”, at M1/M2 (p=0.000) and M1/M3 (p=0.000); in the variable “limitations in the last
12 months”, at M1/M2 (p=0.001) and M1/M3 (p=0.000); and in the variable “troubles in the last 7
days”, at M1/M3 (p=0.01). In the control group there were statistically significant differences at
M1/M3 (p=0.029), although these differences resulted from increased symptoms.
Conclusion
It can be concluded that the implementation of a 21-month low back specific exercise program
decreased low back pain symptoms of warehouse workers.
Keywords: occupational health, musculoskeletal symptoms, specific exercises, Nordic
questionnaire.
INTRODUCTION
Musculoskeletal disorders (MSD) are very common and can even be considered as one
of the main problems in industrialised countries (1).In fact, they represent the most common
cause of chronic incapacity (2, 3). The National Institute for Occupational Safety and Health
defined musculoskeletal symptoms (MSS) as a group of conditions involving the nerves,
tendons, muscles, and supporting structures such as inter vertebral discs (4). Pain is workers’

38
most reported problem and one of the most common causes of work absence (5, 6). According
to (7) low back pain (LBP) (25%) and muscle pain (23%) account for the two major MSD
affectingEUworkers. LBP is the major cause of morbidity and disability, involving considerable
financial costs and affecting 58%-84% of the working population (4, 5,8-15).
Punnett et al. (2005) have verified that about 37% of LBP is associated with exposure to
risk factors (16). Moreover, LBP is considered to depend from different aspects, resulting from
the interaction of physiological, psychological and social factors (17). The physical ergonomic
features of work are frequently mentioned as risk factors for the occurrence of LBP, including
heavy work, repetitive motion patterns, lifting of carrying heavy weight or other forceful manual
tasks, asymmetric body postures (either dynamic or static); movements with trunk flexion or
torsion, forced or involving accumulated compressive forces on vertebral discs, vibration (both
segmental and whole-body), low temperatures, excessive weight on tendons, joints and
muscles, insufficient recovery time of musculoskeletal structures and activity intensity (18-24).
Kasai considered lumbar stability to be a potential cause for LBP (25). The risk of developing
LBP is particularly high when the working environment involves exposure to one or more of
these risk factors.
Low back disorders in warehouses or distribution centres have been identified as an
area of elevated risk in many industries (26), as the incidence and prevalence of occupational
LBP are especially high in manual work industries (26, 27).Common tasks involving manual
work in distribution centres are the assembly and disassembly of pallets, and also the transfer
and stacking of material (boxes or bags) in pallets, which require repetitive movements with
trunk flexion and torsion (28-30). According to Mazloum (2006) weight lifting contributes more to
LBP than any other occupational risk factors (31). Working in wrong postures demands
adequate trunk muscle flexibility and strength (32). In fact, reduced vertebral muscle flexibility
and trunk extension strength are generally associated with LBP and sciatic pain (33-35). MSD
can be measured considering the symptoms reported by workers, such as pain, ache or
discomfort (36-38), affecting all anatomic regions, both spine and extremities (39, 40).
The prevention of LBP and the associated disability is the best attitude to be adopted by
all economic agents and work-related health professionals (1,18, 39-42). Specific exercises
have been shown to prevent and reduce work-related MSD, such as LBP, and the associated
costs (29, 43-48). These exercises aim to restore trunk muscle normal function and have been
shown to be efficient in reducing disability and in increasing performance in individuals with mild
disability (29, 49). These can be important arguments for the implementation of exercise
programs in the work place. These programs include specific exercises which are performed in
the work place to improve workers’ general health and the conditions regarding work activities
and tasks. They promote stretching of shortened muscles and improve motor coordination and
interpersonal relations. Soukup (2001) considered specific exercise to be a common
physiotherapy approach in the prevention of LBP (50).

39
The aim of this study was to evaluate the effects of a specific exercise program
executed before work in the MSS of warehouse workers. Specifically, it aimed to check if a
specific exercise program could decrease MSS in warehouse workers.
METHODS
Subjects
The population used in this study included 557 warehouse urban male workers from a food
distribution company in Oporto/Portugal. All workers were involved in a routine of overcharge
tasks and/or repetitive movements and they worked under low temperatures (between 0º and
4ºC) during all seasons of the year. According to the company norms, all workers wore cold
protective clothing, gloves, boots and lumbar support belts. After informing the clinical physician
and human resources staff on the criteria that would have to be taken into account for subject
selection, the company has provided us with an alphabetically organised list of 249 eligible
workers, corresponding to 45% of the population. The sample was randomised in two groups
(125 in the intervention group and 124 in the control group). Then, subjects were asked to
volunteer to participate in the study under written consent. The sample included 112 volunteers
for the intervention group and 117 for the control group. At baseline the sample was n=229,
corresponding to 41% of the population.
Workers were deemed eligible if they met the following criteria: a) they had a contract
for three or more years; b) they performed the same task type (assembly and disassembly of
pallets). On the other hand, it excluded individuals who: a) were required to rotate work
positions; b) were absent from work because of back pain; c) had severe back pain (VAS ≥ 5) in
the last year; d) had undergo treatment (conservative or surgical) to LBP for the last year; and
e) had been diagnosed with any kind of pathology which could prevent them from participating
in the prescribed exercises (51).
From the first to the second assessment there was a total loss of 37.5% of the subjects,
30% from the intervention group and 44.4% from the control group. From the second to the third
assessment there was a total loss of 34.2% of the individuals, 38.5% from the intervention
group, and 29.2% from the control group. From the first to the third assessment, losses in the
intervention group and in the control group were 57% and 60%, respectively. After 21 months
the sample was reduced to approximately 17% of population. These losses resulted from
workers leaving the company, changing workplace, losing motivation to continue in the study or
not answering the questionnaire.
Table 1 shows values for mean, standard deviation, minimum and maximum for age
(years), height (cm), weight (kg) and body mass index (BMI) of workers included in the
intervention group and in the control group.

40
Table 1: Values for mean, standard deviation, minimum and maximum of age (years), height (cm), weight (Kg) and BMI
of workers included in the intervention group and in the control group.
n=229
Intervention group
n=112
Control group
n=117
mean±sd Min Max mean±sd Min Max
Age
(years) 34.41±8.36 20 49 33.05±10.19 18 56
Height
(cm) 173.0±0.07 160 188 178.0±0.09 159 188
Weight
(Kg) 76.54±10.44 55 95 81.07±16.84 60 110
BMI
Kg/m 2 25.57 21.48 26.91 25.58 23.81 31.16
Instruments
The Portuguese version of the Nordic musculoskeletal questionnaire (NMQ) was used
to evaluate MSS of subjects. This questionnaire has a Kuder-Richardson reliability of 0,855 and
a test-retest reliability in the Cohen’s kappa coefficient test between 0,677 and 1 (52). The NMQ
consists of 27 binary choice questions (yes or no). The questionnaire has three questions
correlating to nine anatomic regions (neck, shoulders, wrists/hands, upper back, low back,
hips/thighs, knees, ankles/feet), addressing three variables: in the first, subjects are asked if
they felt any troubles or pain in the last 12 months; the second variable questions if subjects felt
any work-related limitation in their daily activities in the last 12 months”; the third addresses
troubles or pain felt in the last 7 days. According to the original author of the questionnaire, for
“troubles” we must understand pain, discomfort or aching (36). For a clear identification of
corporal areas, the questionnaire also includes a picture of the human form with nine body
areas shaded and defined (36).
Procedures
The exercise program was implemented in several stages. In a first moment, visits to the
warehouse facilities allowed to know the type of tasks executed by workers and the most
common injuries. Upon evaluation of risks and most repeated gestures, an adequate exercise
program was created. This program included nine easily-executed exercises to promote
stretching and strengthening of soft tissues responsible for spinal stability, especially lumbar
stability. This program was applied, with exercises being executed daily, at the beginning of the
working time, in the company facilities and lasting approximately eight minutes. To motivate
workers to adhere to the program and follow it, there were several training sessions and posters
illustrating the exercise program to execute were distributed in the company facilities.
Facilitators of the program included physiotherapists, who visited the warehouse facilities
each 15 days to correct possible execution errors or to answer doubts and questions from
workers as to the exercise program. The program efficacy was assessed at three moments – at

41
baseline (M1), 11 months after study entry (M2), and 21 months after intervention (M3) – by
application of the NMQ.
The control group participated in the pre- and post-program tests. At the end of the
study this group was offered the possibility of executing the same exercises which were
implemented in the intervention group.
The study was conducted between February 2005 and March 2007, with authorisation
by the company, and according to a protocol between the institutions involved. All participants
provided written informed consent before entering the study. All procedures were in accordance
with the Helsinki Declaration. The study design was approved by the ethics committee of Escola
Superior de Tecnologia da Saúde do Porto, in Portugal.
Statistics
Exploratory data analysis and sample characterisation were performed using descriptive
statistics.
The Q Cochran’s test was used at the different points of assessment to analyse if the
exercise program influenced the intervention group during the study. When values obtained with
this test were below the significance level, the McNemar test was used to check in which
moment (M1-M2; M2-M3; M1-M3) there were statistically significant differences.
The Chi-square test was used to check if there was any association between the
exercise program and the intervention and control groups.
The level of significance was set at 0.05, with 95% confidence intervals. Statistical
analysis was conducted using SPSS® 17.0 for Windows®.
RESULTS
The baseline (M1) symptoms’ proportions were identical in both groups, without
statistical significant differences in any of the variables. The most common symptom, with
higher proportion across all points of assessment, was the low back region, followed by the
neck, in both groups (table 2).As to the intervention group, there was a general reduction in
MSS during the study, in all variables:” troubles in the last 12 months”, “limitations in the last 12
months” and “troubles in the last 7 days”. There was a clear decrease in low back symptoms.
However, there was an increase in symptoms associated with knees and a moderate increase
in symptoms in the neck region, especially in the last 12 months. In the control group there was
a general increase in symptoms, especially in the low back region, where this increase was
higher. Symptoms in the neck also increased significantly, especially in the last 12 months.

42
Table 2 : Proportion of symptoms in the intervention group and in the control group across all points
of assessment (M1, M2, M3) in all regions of the NMQ.
Intervention group
Control group
Troubles in the last 12 months
Limitation in the last 12
months
Troubles in the last 7 days
Regions
Troubles in the last 12 months
Limitation in the last 12 months
Troubles in the last 7 days
M1 M2 M3 M1 M2 M3 M1 M2 M3 M1 M2 M3 M1 M2 M3 M1 M2 M3
% % % % % %
8.3 10.2 19.6 3.1 5.1 4.3 5.3 6.8 5.7 Neck 9.7 8.2 24.2 7.3 6.0 4.8 7.3 6.0 4.8
4.2 6.8 2.2 3.1 3.4 2.2 1.0 3.4 2.2 Shoulders 0.8 2.4 3.2 0.8 3.6 1.6 0.8 3.6 0.0
2.0 0.0 2.2 2.0 0.0 0.0 2.0 0.0 2.2 Elbows 0.8 1.2 3.2 0.8 1.2 0.0 0.0 0.0 0.0
9.4 8.5 8.7 6.3 6.8 0.0 6.3 8.5 4.3 Wrists/Hands 5.6 3.6 8.0 5.7 6.9 4.8 4.9 3.6 3.2
3.1 3.4 2.2 2.1 1.7 0.0 1.0 1.7 0.0 UpperBack 2.4 6.0 7.8 0.8 2.4 3.1 1.6 4.8 4.6
29.0 14.5 10.9 20.0 7.9 6.5 14.6 14.5 6.5 LowBack 24.0 32.1 46.9 12.1 17.9 17.5 23.4 25.0 21.9
7.3 1.7 0.0 4.2 1.7 0.0 2.1 1.7 0.0 Hips/Thighs 4.8 7.2 4.8 2.4 4.8 3.2 4.0 3.6 4.8
5.2 13.6 8.7 4.2 6.8 2.2 3.1 10.2 2.2 Knees 5.6 7.2 9.5 2.4 2.4 3.1 4.0 2.4 6.3
2.1 6.8 0.0 1.0 5.1 2.1 2.1 6.8 0.0 Ankles/Feet 3.2 1.2 4.8 3.2 1.2 0.0 1.6 1.2 1.6
The Cochran’s Q test to independent samples used across all assessments for all
regions (knees, shoulders, elbows, wrists/hands, upper back, low back, hips/thighs and
ankles/feet) only showed statistically significant results for the low back region in the three
variables: “troubles in the last 12 months” (p=0.000); “limitations in the last 12 months”
(p=0.000) and “troubles in the last 7 days” (p=0.030), in the intervention group. In the control
group, the same test was used for the three assessments and for all regions, being results
statistically significant for the low back region, for the variable “troubles in the last 7 days”
(p=0.039). Subsequently, the McNemar test was used to verify in which moment there were
statistically significant differences (table 3).Results have shown statistically significant
differences in the variable ‘troubles in the last 12 months’ for the intervention group at M1/M2
(p=0.000), and M1/M3 (p=0.000). As to the variable ‘limitations in the last 12 months’,
differences in the intervention group were statistically significant at M1/M2 (p=0.001) and M1/M3
(p=0.000). In the variable 'troubles in the last 7 days', in the intervention group, there were
statistically significant differences at M1/M3 (p=0.01), whereas in the control group there were
statistically significant differences at M1/M3 (p=0.029), although these differences resulted from
increased symptoms, which did not occur in the intervention group.

43
Table 3 : McNemar test proof values for both groups across all points of assessment.
The chi-square test was used to verify the association between the exercise program
and symptoms in the different regions (neck, shoulders, elbows, wrists/hands, upper back, low
back, hips/thighs, knees and ankles/feet), but the results obtained did not show statistical
evidence that there is a relation between symptoms and the specific exercise program, either in
the intervention group or in the control group, at baseline (table 4). However, results in table 4
show that in the intervention group there is some dependency in two of the variables for the low
back region. The variable “troubles in the last 12 months”, at M2 (p=0.019) and M3 (p=0.000);
and in the variable ‘troubles in the last 7 days’ at the final assessment (p=0.033).
Table 4 : Chi-square test proof values for both groups across all points of assessment.
Intervention group Region
Control group
M1 M2 M3 M1 M2 M3
p p p Low back p p p
NS 0.019 0.000 Troubles in the last 12 months
NS NS NS
NS NS NS Limitations in the last 12 months
NS NS NS
NS NS 0.033 Troubles in the last
7 days NS NS NS
DISCUSSION
At baseline, the sample was homogeneous, without significant differences as to weight,
height and BMI. The greatest proportion of problems reported was from the low back, as a
result of the type of tasks executed by workers participating in this study: prepare and
disassemble pallets, make picking, drive pallet trucks standing with body turned to the right,
typical tasks executed in warehouses. These results are consistent with other studies (19, 28,
42, 48, 53,54). Increased flexion with trunk rotation, combined with repetitive tasks, provoke
posterior soft-tissue stretch and tension, leading to MSD. These effects stimulate
mechanoreceptors, causing fatigue and discomfort in the low back area. Several authors have
Intervention group Region
Control group
M1-M2 M2-M3 M1-M3 M1-M2 M2-M3 M1-M3
p p p Low back P p p
0.000 NS 0.000 Troubles in the last 12 months NS NS NS
0.001 NS 0.000 Limitations in the last 12 months NS NS NS
NS NS 0.010 Troubles in the
last 7 days NS NS 0.029

44
suggested that noniceptive pain is generated by ischemic muscle tension (20, 30, 53,55-57).
Nevertheless, although the low back is the most affected region, symptoms have decreased
during this study, being differences statistically significant between M1 and M2 and between M2
and M3. These results are similar to the ones obtained in Moffett, where a specific exercise
program led to improved condition in individuals with LBP (55). From M2 to M3 there was no
statistical evidence of a decrease in MSS in the low back region, probably as a result of
increased anxiety motivated by changes in the company direction and in working shifts, which
have caused workers some discomfort. According to Feyer, dissatisfaction has been associated
with self-reported symptoms (57). Harkness defends that work-related stress and psychosocial
conditions, such as dissatisfaction and relationship with supervisors and colleagues, are
associated with work-related MSD (58).
With a decrease in reported LBP symptoms in the last 12 months, there was also a
decrease in reported situations of symptoms in shoulders and wrists/hands and an increase of
symptoms affecting the neck. This can result from incorrect delimitation of body regions by
subjects and the possibility that they can be identifying pain in the wrong area. Other possible
explanation is that the pain felt in the shoulder and wrists/hands regions was in fact a result of
cervical irradiating pain, which became centralised as a benefit of executing the exercise
program, which included specific exercises for these body regions (57).
The greatest proportion of problems reported as provoking higher limitation to personal
and work-related activities in the last 12 months in the control group was the low back, which
shows that besides being the most frequent symptom, LBP was also the most incapacitating.
These results are consistent with several studies which refer that LBP is the major cause of
pain, diminished work capabilities, limitation, resulting in work-absenteeism, substantial health-
care related expenses and productivity losses (10, 16, 31, 42, 53, 59-63). In the intervention
group there was a decrease in reported limitations due to MSS, being differences statistically
significant from M1 to M3, with individuals with LBP showing increased functional capacity
following participation in the exercise program, similarly to other studies (22, 33, 43, 64-66).
Moseley (2002), Waddel and Burton (2001), Arokoski (2004) and O’Sullivan (2006) refer that
following a specific exercise program reduces LBP intensity and improves functional disability in
sub-acute and chronic low back patients. In Kasai, a strengthening exercise program, designed
to increase low back flexibility, has contributed to improve subjects’ functional ability (67).
According to Friedrich, full benefits can only be realised if the exercises are performed regularly
and consistently (68). In fact, exercise effects on functional ability only persist if they are
executed for long periods (69).
Throughout the 21-month follow-up there were no statistically significant differences in
any variable in the regions neck, shoulders, elbows, wrists/hands, upper back, thighs/hips,
knees and ankles/feet, although the proportion of neck-related symptoms must be taken into
account when designing new exercise programs. Together with the low back, the neck is a
transition region where instability problems can occur, with pain and functional limitation. As to

45
MSS pain intensity in the different regions, there were no statistically significant differences to
conclude that there were any changes throughout the study.
A limitation of this study was the impossibility of controlling subjects’ tasks, resting time,
presence of a second subject, eating habits and leisure and sports activities executed by
subjects in non-working time. Other limitation was the high number of losses, which can lead to
errors in the results obtained. However, these limitations are difficult to control in real life
situations, although the whole team has been always interested and paying attention to
motivate subjects to participate and to understand the importance of this study.
As MSD are a major work-related problem, with high disability and reduction of quality
of life, with individuals experiencing pain daily, efforts should be directed towards prevention of
this situation. As such, we suggest carrying out more and longer experimental studies, which
implement prevention strategies, including ergonomic studies which help reducing these
problems.
CONCLUSION
It can be concluded that a specific exercise program improved MSS in the low back
region throughout the 21 months, in all variables: “troubles in the last 12 months”, “limitations in
the last 12 months” and “troubles in the last 7 days”.
References
1. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al.
Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur
Spine J. 2006 Mar;15 Suppl 2:S192-300.
2. Liira JP, Shannon HS, Chambers LW, Haines TA. Long-term back problems and physical
work exposures in the 1990 Ontario Health Survey. Am J Public Health. 1996 Mar;86(3):382-7.
3. Herbert RD, Maher CG, Moseley AM, Sherrington C. Effective physiotherapy. BMJ.
2001 Oct 6;323(7316):788-90.
4. Dovrat E, Katz-Leurer M. Cold exposure and low back pain in store workers in Israel.
Am J Ind Med. 2007 Aug;50(8):626-31.
5. W IJ, Burdorf A. Impact of musculoskeletal co-morbidity of neck and upper extremities
on healthcare utilisation and sickness absence for low back pain. Occup Environ Med. 2004
Oct;61(10):806-10.
6. van Poppel MN, Hooftman WE, Koes BW. An update of a systematic review of
controlled clinical trials on the primary prevention of back pain at the workplace. Occup Med
(Lond). 2004 Aug;54(5):345-52.
7. Giaccone M. Annual review of working conditions in the EU 2006-2007. Luxembourg:
The European Foundation for the Improvement of Living and Working Conditions2007.
8. Bernard BP. A Critical Review of Epidemiologic Evidence for Work-Related
Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back. Columbia-Cincinnati:
National Institute for Occupational Safety and Health1997.
9. van Vuuren BJ, Becker PJ, van Heerden HJ, Zinzen E, Meeusen R. Lower back problems
and occupational risk factors in a South African steel industry. Am J Ind Med. 2005
May;47(5):451-7.

46
10. Van Nieuwenhuyse A, Somville PR, Crombez G, Burdorf A, Verbeke G, Johannik K, et al.
The role of physical workload and pain related fear in the development of low back pain in
young workers: evidence from the BelCoBack Study; results after one year of follow up. Occup
Environ Med. 2006 Jan;63(1):45-52.
11. Steenstra IA, Anema JR, Bongers PM, de Vet HC, van Mechelen W. Cost effectiveness
of a multi-stage return to work program for workers on sick leave due to low back pain, design
of a population based controlled trial [ISRCTN60233560]. BMC Musculoskelet Disord. 2003 Nov
21;4:26.
12. Morken T, Riise T, Moen B, Bergum O, Hauge SH, Holien S, et al. Frequent
musculoskeletal symptoms and reduced health-related quality of life among industrial
workers. Occup Med (Lond). 2002 Mar;52(2):91-8.
13. Jansen JP, Morgenstern H, Burdorf A. Dose-response relations between occupational
exposures to physical and psychosocial factors and the risk of low back pain. Occup Environ
Med. 2004 Dec;61(12):972-9.
14. Hoogendoorn WE, Bongers PM, de Vet HC, Ariens GA, van Mechelen W, Bouter LM.
High physical work load and low job satisfaction increase the risk of sickness absence due to
low back pain: results of a prospective cohort study. Occup Environ Med. 2002 May;59(5):323-
8.
15. Guo HR. Working hours spent on repeated activities and prevalence of back pain.
Occup Environ Med. 2002 Oct;59(10):680-8.
16. Punnett L, Pruss-Utun A, Nelson DI, Fingerhut MA, Leigh J, Tak S, et al. Estimating the
global burden of low back pain attributable to combined occupational exposures. Am J Ind
Med. 2005 Dec;48(6):459-69.
17. Kent PM, Keating JL. The epidemiology of low back pain in primary care. Chiropr
Osteopat. 2005 Jul 26;13:13.
18. Rugulies R, Krause N. Job strain, iso-strain, and the incidence of low back and neck
injuries. A 7.5-year prospective study of San Francisco transit operators. Soc Sci Med. 2005
Jul;61(1):27-39.
19. Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic
evidence and the debate. J Electromyogr Kinesiol. 2004 Feb;14(1):13-23.
20. Kaser L, Mannion AF, Rhyner A, Weber E, Dvorak J, Muntener M. Active therapy for
chronic low back pain: part 2. Effects on paraspinal muscle cross-sectional area, fiber type size,
and distribution. Spine (Phila Pa 1976). 2001 Apr 15;26(8):909-19.
21. Hlobil H, Uegaki K, Staal JB, de Bruyne MC, Smid T, van Mechelen W. Substantial sick-
leave costs savings due to a graded activity intervention for workers with non-specific sub-
acute low back pain. Eur Spine J. 2007 Jul;16(7):919-24.
22. Waddell G, Burton AK. Occupational health guidelines for the management of low back
pain at work: evidence review. Occup Med (Lond). 2001 Mar;51(2):124-35.
23. Lurie-Luke E, Neubauer G, Lindl C, Breitkreutz H, Fischer P, Hitzeroth S. An exploratory
workplace study to investigate the perceived value of continuous low-level heatwrap therapy
in manual workers. Occup Med (Lond). 2003 May;53(3):173-8.
24. Levangie PK. Association of low back pain with self-reported risk factors among
patients seeking physical therapy services. Phys Ther. 1999 Aug;79(8):757-66.
25. Kasai Y, Morishita K, Kawakita E, Kondo T, Uchida A. A new evaluation method for
lumbar spinal instability: passive lumbar extension test. Phys Ther. 2006 Dec;86(12):1661-7.
26. Marras WS, Granata KP, Davis KG, Allread WG, Jorgensen MJ. Effects of box features
on spine loading during warehouse order selecting. Ergonomics. 1999 Jul;42(7):980-96.
27. Renkawitz T, Boluki D, Grifka J. The association of low back pain, neuromuscular
imbalance, and trunk extension strength in athletes. Spine J. 2006 Nov-Dec;6(6):673-83.

47
28. Alexopoulos EC, Stathi IC, Charizani F. Prevalence of musculoskeletal disorders in
dentists. BMC Musculoskelet Disord. 2004 Jun 9;5:16.
29. Bigos SJ, Holland J, Holland C, Webster JS, Battie M, Malmgren JA. High-quality
controlled trials on preventing episodes of back problems: systematic literature review in
working-age adults. Spine J. 2009 Feb;9(2):147-68.
30. Marras WS, Lavender SA, Ferguson SA, Splittstoesser RE, Yang G. Quantitative dynamic
measures of physical exposure predict low back functional impairment. Spine (Phila Pa 1976).
2010 Apr 15;35(8):914-23.
31. Mazloum A, Nozad H, Kumashiro M. Occupational low back pain among workers in
some small-sized factories in Ardabil, Iran. Ind Health. 2006 Jan;44(1):135-9.
32. Shinozaki T, Yano E, Murata K. Intervention for prevention of low back pain in Japanese
forklift workers. Am J Ind Med. 2001 Aug;40(2):141-4.
33. Kuukkanen T, Malkia E. Effects of a three-month therapeutic exercise programme on
flexibility in subjects with low back pain. Physiother Res Int. 2000;5(1):46-61.
34. Hilfiker R, Bachmann LM, Heitz CA, Lorenz T, Joronen H, Klipstein A. Value of predictive
instruments to determine persisting restriction of function in patients with subacute non-
specific low back pain. Systematic review. Eur Spine J. 2007 Nov;16(11):1755-75.
35. Ceran F, Ozcan A. The relationship of the Functional Rating Index with disability, pain,
and quality of life in patients with low back pain. Med Sci Monit. 2006 Oct;12(10):CR435-9.
36. Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sorensen F, Andersson G, et al.
Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon.
1987 Sep;18(3):233-7.
37. Kuorinka I, Cote MM, Baril R, Geoffrion R, Giguere D, Dalzell MA, et al. Participation in
workplace design with reference to low back pain: a case for the improvement of the police
patrol car. Ergonomics. 1994 Jul;37(7):1131-6.
38. Forcier L, Lapointe C, Lortie M, Buckle P, Kuorinka I, Lemaire J, et al. Supermarket
workers: their work and their health, particularly their self-reported musculoskeletal problems
and compensable injuries. Work. 2008;30(4):493-510.
39. Piedrahita H. Costs of work-related musculoskeletal disorders (MSDs) in developing
countries: Colombia case. Int J Occup Saf Ergon. 2006;12(4):379-86.
40. Hussain T. Musculoskeletal symptoms among truck assembly workers. Occup Med
(Lond). 2004 Dec;54(8):506-12.
41. Burton AK, Balague F, Cardon G, Eriksen HR, Henrotin Y, Lahad A, et al. Chapter 2.
European guidelines for prevention in low back pain : November 2004. Eur Spine J. 2006
Mar;15 Suppl 2:S136-68.
42. Alexopoulos EC, Tanagra D, Konstantinou E, Burdorf A. Musculoskeletal disorders in
shipyard industry: prevalence, health care use, and absenteeism. BMC Musculoskelet Disord.
2006;7:88.
43. Moseley L. Combined physiotherapy and education is efficacious for chronic low back
pain. Aust J Physiother. 2002;48(4):297-302.
44. Mannion AF, Taimela S, Muntener M, Dvorak J. Active therapy for chronic low back
pain part 1. Effects on back muscle activation, fatigability, and strength. Spine (Phila Pa 1976).
2001 Apr 15;26(8):897-908.
45. Holmstrom E, Ahlborg B. Morning warming-up exercise--effects on musculoskeletal
fitness in construction workers. Appl Ergon. 2005 Jul;36(4):513-9.
46. Hildebrandt VH, Bongers PM, Dul J, van Dijk FJ, Kemper HC. The relationship between
leisure time, physical activities and musculoskeletal symptoms and disability in worker
populations. Int Arch Occup Environ Health. 2000 Nov;73(8):507-18.
47. Comerford MJ, Mottram SL. Functional stability re-training: principles and strategies
for managing mechanical dysfunction. Man Ther. 2001 Feb;6(1):3-14.

48
48. Bergman S. Management of musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007
Feb;21(1):153-66.
49. Besler A, Can F. Correlation between pain, trunk muscle strength, and functional state
in low back pain. The Pain Clinic. 2003;15(4):415-9.
50. Soukup MG, Lonn J, Glomsrod B, Bo K, Larsen S. Exercises and education as secondary
prevention for recurrent low back pain. Physiother Res Int. 2001;6(1):27-39.
51. Sculco AD, Paup DC, Fernhall B, Sculco MJ. Effects of aerobic exercise on low back pain
patients in treatment. Spine J. 2001 Mar-Apr;1(2):95-101.
52. Mesquita CC, Ribeiro JC, Moreira P. Portuguese version of the standardized Nordic
musculoskeletal questionnaire: cross cultural and reliability. J Public Health. 2010;18(5):461–6.
53. Keyserling WM, Sudarsan SP, Martin BJ, Haig AJ, Armstrong TJ. Effects of low back
disability status on lower back discomfort during sustained and cyclical trunk flexion.
Ergonomics. 2005 Feb 22;48(3):219-33.
54. Alipour A, Ghaffari M, Shariati B, Jensen I, Vingard E. Occupational neck and shoulder
pain among automobile manufacturing workers in Iran. Am J Ind Med. 2008 May;51(5):372-9.
55. Moffett JK, Torgerson D, Bell-Syer S, Jackson D, Llewlyn-Phillips H, Farrin A, et al.
Randomised controlled trial of exercise for low back pain: clinical outcomes, costs, and
preferences. BMJ. 1999 Jul 31;319(7205):279-83.
56. Marras WS, Granta KP, Davis KG. Variability in spine loading model performance. Clin
Biomech (Bristol, Avon). 1999 Oct;14(8):505-14.
57. Feyer AM, Herbison P, Williamson AM, de Silva I, Mandryk J, Hendrie L, et al. The role
of physical and psychological factors in occupational low back pain: a prospective cohort study.
Occup Environ Med. 2000 Feb;57(2):116-20.
58. Harkness EF, Macfarlane GJ, Nahit ES, Silman AJ, McBeth J. Risk factors for new-onset
low back pain amongst cohorts of newly employed workers. Rheumatology (Oxford). 2003
Aug;42(8):959-68.
59. Wynne-Jones G, Dunn KM, Main CJ. The impact of low back pain on work: a study in
primary care consulters. Eur J Pain. 2008 Feb;12(2):180-8.
60. Tveito TH, Hysing M, Eriksen HR. Low back pain interventions at the workplace: a
systematic literature review. Occup Med (Lond). 2004 Jan;54(1):3-13.
61. Tveito TH, Eriksen HR. Integrated health programme: a workplace randomized
controlled trial. J Adv Nurs. 2009 Jan;65(1):110-9.
62. Levangie PK. The association between static pelvic asymmetry and low back pain.
Spine (Phila Pa 1976). 1999 Jun 15;24(12):1234-42.
63. Hlobil H, Staal JB, Twisk J, Koke A, Ariens G, Smid T, et al. The effects of a graded
activity intervention for low back pain in occupational health on sick leave, functional status
and pain: 12-month results of a randomized controlled trial. J Occup Rehabil. 2005
Dec;15(4):569-80.
64. Rainville J, Hartigan C, Martinez E, Limke J, Jouve C, Finno M. Exercise as a treatment
for chronic low back pain. Spine J. 2004 Jan-Feb;4(1):106-15.
65. O'Sullivan PB, Mitchell T, Bulich P, Waller R, Holte J. The relationship beween posture
and back muscle endurance in industrial workers with flexion-related low back pain. Man Ther.
2006 Nov;11(4):264-71.
66. Arokoski JP, Valta T, Kankaanpaa M, Airaksinen O. Activation of lumbar paraspinal and
abdominal muscles during therapeutic exercises in chronic low back pain patients. Arch Phys
Med Rehabil. 2004 May;85(5):823-32.
67. Kasai R. Current Trends in Exercise Management for Chronic Low Back Pain:
Comparison between Strengthening Exercise and Spinal Segmental Stabilization exercise.
Journal of Physical Therapy Science. 2006;18:97-105.

49
68. Friedrich M, Gittler G, Arendasy M, Friedrich KM. Long-term effect of a combined
exercise and motivational program on the level of disability of patients with chronic low back
pain. Spine (Phila Pa 1976). 2005 May 1;30(9):995-1000.
69. Peate WF, Bates G, Lunda K, Francis S, Bellamy K. Core strength: a new model for injury
prediction and prevention. J Occup Med Toxicol. 2007;2:3.


Capitulo 3
Effect of a specific exercise program on strength a nd resistance levels of lumbar muscles of warehouse wo rkers.
(EM PUBLICAÇÃO NO International Journal of Occupational Medicine and Environmental Health)


53
Abstract
Low back pain is one of the major causes of limitation of the locomotor system and one of the most common reasons for searching medical assistance. Different studies have come to the conclusion that patients with low back pain present more weakness in trunk extensor and flexor muscles. Several lines of evidence have shown the importance of implementing exercise programmes specifically directed to workers.
The aim of this study was to verify the influence of a specific exercise program on strength and resistance levels of lumbar flexors and extensors in warehouse
workers.
Study Design
The population used in this randomized controlled trial included 557 warehouse male workers from a food distribution company in Oporto/Portugal. Upon application of the selection criteria, 98 workers were deemed eligible, which were randomized in two groups: 57 were assigned to the intervention group and 41 to the control group. The intervention included 9 easily-executed exercises to promote stretching and strengthening of lumbar region, being executed daily, at the beginning of the working time, in the company facilities and lasting 8’. Trunk muscles´ voluntary strength and resistance were measured using an isometric electronic dynamometer (Globus Ergometer, Globus, Codigné, Italy) at baseline and eleven months after implementing the exercise program. Data were analysed using SPSS®, version 17.0.
After implementation of the exercise program, in the intervention group, all variables increase, significant differences were observed in muscle strength and resistance values (p=0.014 and p=0.006, respectively), as well as in the ratio extensors/flexors (p=0.037). In the control group, all variables decrease being statistically significant decrease of trunk flexors strength level (p=0.009).
The results of this study suggest that a specific exercise intervention program can increase trunk extensors strength and resistance.
Key words strength, resistance, trunk muscles, exercise

54
Introduction
Low back pain (LBP) is the main cause of incapacity in industrialized countries
[1-6]. Epidemiological studies relate the incidence of LBP in approximately 60%
of industrial workers throughout their lives [7]. In fact, LBP constitutes the major
cause of work absence, as it is one of the causes of limitation of the locomotor
system, and one of the most common reasons for searching medical
assistance. As a consequence, LBP is responsible for a growth in social costs
and a reduction in productivity and in the ability to perform everyday tasks. This,
in turn, results in employee replacement by other workers and originates
temporary or even definitive retirement [8-10]
It is generally accepted that prolonged, static sitting postures, such as those
adopted during driving, are more likely to aggravate a preexisting LBP condition
or instigate the development of a new one [11, 12]. In fact, adopting a poor
posture, combined with the effects of vibration and prolonged driving times,
have been identified as sources of increased risk of low back injuries ranging
from disk herniations to general musculoskeletal strains and sprains [13-15].
De Carvalho et al. (2010) have shown that in automobile sitting, with no
lumbar support, the lumbar spine flattens completely in sitting and yet maintains
near standing levels of intervertebral joint angles at L5/S1 [16]. This situation is
highly suggestive of large strains at the posterior aspect of the intervertebral
disks at L4/L5. This is not surprising, as this segment is often referred to as one
of the most common levels of lumbar disk herniation. Generally this is due to
abnormalities in the posterior muscles, tendons and ligaments of the trunk and it
can be attributed to various physical activities, such as lifting weight and
remaining in a standing or sitting position for long periods [17, 18, 19].
The musculoskeletal system, above all, guarantees stability to the spine
in everyday tasks [20, 21]. When it is weakened, spinal joints and ligaments can
became overloaded, increasing the probability of injury incidents at the lumbar
spine. Muscle weakness proceeds from disuse, remaining in certain positions
for long periods or even from tiredness caused by repetitive gestures, resulting
in an excessive transfer of load to the spine structures, causing pain [17, 20, 22-
24]. There is also evidence suggesting that muscle weakness is one of the risk

55
factors for LBP [25-30]. The importance of rehabilitating the trunk muscles to
maintain the lumbar lordosis is clear, as it seems to have a protective effect on
the structures of the spine in different postures. Taking these considerations
into account, more relevance has been given to implement the exercise
program specifically directed to workers, not only to decrease LBP [31-34] but
also to prevent it [30, 33, 35-37].
Systematically reviewing the literature of all interventions performed in
workplaces, Tveito et al. verified that physical exercise has a documented effect
on lumbar pain prevention, muscle strength and resistance [34]. On the other
hand, van Poppel et al. concluded that there is very limited evidence as to the
benefits of applying an exercise program [38]. The aim of this study was to
verify the influence of an 11-month specific exercise program on the strength
and resistance levels of lumbar flexors and extensors in warehouse workers.
Methods
Study Design
This study was a randomized controlled trial.
Sample
The population used in this study included 557 warehouse male workers
from a food distribution company in Oporto/Portugal. All workers were involved
in a routine of overcharge tasks and/or repetitive movements and they worked
under low temperatures [between 0º and 4ºC) during all seasons of the year.
According to the company norms, all workers wore cold protective clothing,
gloves, boots and lumbar support belts.
After informing the clinical physician and human resources staff on the
criteria that would have to be taken into account for subject selection, the
company has provided us with an alphabetically organized list of 143 eligible
workers, corresponding to 25% of the population. The sample was randomized
in two groups (72 in the intervention group and 71 in the control group). Then,
subjects were asked to volunteer to participate in the study under written

56
consent. The sample included 57 volunteers for the intervention group and 41
for the control group. At baseline the sample was n=98, corresponding to 17%
of the population.
This study included all male workers who did not oppose to being
measured as to their maximal isometric strength and resistance of trunk flexors
and extensors and who completed the exercise program. Subjects were
excluded if they met at least one of these criteria: a) presented a clinically
diagnosed pathology which prevented them from executing the exercises or the
strength and resistance tests [39]; b) had been submitted to abdominal or
lumbar-pelvic surgery [26, 40]; c) suffered any musculoskeletal injury or chronic
illness [40]; d) were taking any medication which could influence the viscous
elastic properties of soft tissue [41]; e) were taking pain killers or AINS [41]; f)
had been under back pain treatment for the last year[20]; g) were unable to
maintain a correct posture during measurement of muscle strength and
resistance[21]; h) reported LBP [39, 42, 43]; or i) practiced regular physical
exercise [44].
There were 26 losses at the end of the research: 15 (26.32%) from the
intervention group and 11 (26.83%) from the control group, being the sample at
the end of the program reduced to 72 workers, 42 in the intervention group and
30 in the control group. These losses resulted from workers leaving the
company, changing workplace or giving up from participating in the study before
the end of the program.
Individual characteristics of the sample for age, weight, height and Body
Mass Index (BMI) are presented in table 1.

57
Table 1.Sample characteristics
Instruments
An isometric electronic dynamometer (Globus Ergometer, Globus, Codigné,
Italy) was used to measure resistance (in seconds) and maximal isometric
strength (in Kgf) of trunk flexors and extensors. According to Robinson et al, the
Intraclass Correlation Coefficient (ICC) of this instrument is 0.93, in the test-
retest for the maximal isometric strength, 0.93 in the Pearson Correlation
Coefficient and 0.85 in the test-retest for the isometric resistance [45]. Generic
health status survey questionnaires were used to select and characterize the
sample.
Procedures
The exercise program was implemented in several stages. In a first moment,
visits to the warehouse facilities allowed to know the type of tasks executed by
workers and the most common injuries. Upon evaluation of risks and most
repeated gestures, an adequate exercise program was created. This program
included nine easily-executed exercises to promote stretching and
strengthening of soft tissues responsible for spinal stability, especially lumbar
stability. This program was applied, with exercises being executed daily, at the
beginning of the working time, in the company facilities and lasting
approximately eight minutes (appendix 1). To motivate workers to adhere to the
program and follow it, there were several training sessions and posters
Sample
N=98
Intervention group
(n=57)
Control group
(n=41)
Mean±sd Minimum Maximum Mean±sd Minimum Maximum
Age (years) 33.5±8.17 20 49 27.4±6.25± 20 45
Weight (kg) 77.0±11.10 56.00 104.00 78.1±14.65 57.00 110.00
Height (cm) 175±7.4 161 194 175±9.3 150 187
BMI (kg/m2) 25.2±2.05 21.6 27.6 25.6±1.69 25.3 31.5

58
illustrating the exercise program to execute were distributed in the company
facilities.
Facilitators of the program included physiotherapists, who visited the
warehouse facilities each 15 days to correct possible execution errors or to
answer doubts and questions from workers as to the exercise program. The
program efficacy was evaluated in two moments – at baseline and 11 months
following participation in the program.
All evaluations were preceded by a 5 minute warming up, which involved some
callisthenic exercises [46-49]. Then individuals were positioned in the test
position. For this, an 8 cm wide band was placed around the subjects’
shoulders, just below the medial end of the clavicles and horizontally connected
with the dynamometer by a steel cable [28, 50]. To increase stability, pelvic
supports were placed by the fourth and fifth lumbar vertebrae and on the inferior
third of the thighs. Individuals were asked to stand on a nonslip surface, with
their back positioned against a pelvic supporting board as trunk flexors strength
was measured and their front against the board as trunk extensors strength was
evaluated [28, 50, 51]. A short training in the test position, which consisted of 3
submaximal contractions for flexion or extension of the trunk, depending on the
test, was performed prior to measurements. This warming up period allowed
subjects to get used to the equipment, learning how to use it.
After a rest of 1 minute, individuals were encouraged to produce their maximal
strength for flexion or extension of the trunk. Then, in the same position,
resistance tests were made at 60% of their maximum voluntary contraction,
both for trunk flexors and the extensors [52, 53]. During the execution of muscle
contractions, verbal encouragement was constantly given, in order to stimulate
both the maximal strength and period of time in which the individuals endured
the resistance test. The interval between strength and resistance tests was 15
minutes [54].
The control group participated in the pre- and post-program tests. At the end of
the study this group was offered the possibility of executing the same exercises
which were implemented in the intervention group.

59
The study was conducted between February 2005 and March 2007, with
authorization by the company, and according to a protocol between the
institutions involved. All participants provided written informed consent before
entering the study. All procedures were in accordance with the Helsinki
Declaration. The study design was approved by the ethics committee of Escola
Superior de Tecnologia da Saúde do Porto, in Portugal.
Statistics
Descriptive and inferential statistics were used for results analysis. The
student’s t test for independent samples was used to analyze differences
between mean values in both groups. To analyze differences between mean
values in each group before and after the exercise program, the student’s t test
for paired samples was used. The level of significance was set at 5%. Statistical
analysis was conducted using SPSS® 17.0 for Windows®.
Results
Results in table 2 illustrate an increase in all variables after implementation of
the exercise program during 11 months, in the intervention group, being results
statistically significant for trunk extensors strength (p=0.014), trunk extensors
resistance (p=0.006) and the ratio between trunk extensors/flexors strength
(p=0.037).
In the control group there was a statistically significant decrease of trunk flexors
strength level (p=0.009). Both the increase in flexors’ resistance and the
decrease in extensors’ strength and resistance were not statistically significant.
As to the ratio between trunk extensors/flexors strength in the control group,
there was a decrease, but without statistical significance.

60
Table 2.Statistical results of the student’s t test for paired samples between moments 1 and 2: proof value
to the intervention group and the control group.
Intervention Control
Variables Moment 1 Moment 2 P value Moment 1 Moment 2 P value
SFle (Kgf) 72.07 ± 14.33 73.39 ± 14.42 0.257 63.49 ± 20.94 58.81 ± 18.40 0.002
RFle (Sec) 42.43 ± 15.58 44.31 ± 15.89 0.259 42.71 ± 19.45 45.17 ± 17.06 0.464
SExt (Kgf) 79.48 ± 15.94 83.29 ± 13.73 0.014 65.74 ± 18.42 61.90 ± 20.10 0.069
RExt (Sec) 51.57 ± 17.60 58.69 ± 15.38 0.006 62.41± 18.46 61.79± 18.97 0.859
Ratio 1.10 ± 0.25 1.16 ± 0,21 0.037 1.12 ± 0,30 1.08 ± 0.27 0.312
SFle – Trunk flexors strength; RFle – Trunk flexors resistance; SExt – Trunk extensors strength; RExt –
Trunk extensors resistance; Ratio between trunk extensors/flexors strength
Discussion
Several studies have documented the association between chronic LBP
and decreased muscle performance [13-15, 20, 27, 50]. In this study, we have
used isometric tests to evaluate lumbar muscles’ resistance and strength levels,
as they are quite easy to teach and perform, which allows applying them to a
great number of subjects. Besides, according to Brown and Weir, the isometric
strength test provides predictive information about occupational injuries
associated with dynamic activities. Furthermore, the isometric strength test has
been shown to be more reliable. However, one should not forget that the
isometric contraction occurs at a certain specific angle that can be slightly
associated with strength values in other joints positions [46]. Despite all these
arguments, disagreement arises as to the isometric test capacity to predict
dynamic performance. Taking this into account, it would be important to carry
out new studies to quantify strength and resistance dynamics.
All strength and resistance measurements were taken with individuals in
a standing position as, according to Rantanen et al [50] and Rantanen and
NyKvist [51] in this position there is a decrease in the compressive strength
upon the lumbar column, generated by the psoas muscle. Only male workers
have been included in this study, as, according to Ebben and Jensen, there are
differences of strength between genders [55].

61
Although several studies address exercise programs very similar to ours
as to intensity and duration and in the methods adopted to measure muscle
strength and resistance, none of them included all these aspects. Strength and
resistance levels of lumbar extensors have improved after the exercise
programme. These results are consistent with those obtained in the studies of
Mannion et al. and Gundewall et al., which have used a specific exercise
program, executed twice a week, with a duration between 10 and 20 minutes
[39, 56]. Moffroid also verified improvement in trunk extensors strength and
resistance levels after following an exercise program for 6 weeks [57]. However,
this program only included exercises for the lumbar extensors. Koumantakies et
al. observed an increase in strength, not only at the extensors but also at the
lumbar flexors, after implementing a 15 minutes exercise program, applied
specifically to the lumbar region [52]. In a study by Holmstrom and Ahlborg, the
lack of improvement concerning trunk muscle strength and the small increase in
lumbar extensor muscle resistance were not seen as significant [44]. These
results were probably due to the fact that the exercise program adopted global
callisthenic exercises only for 3 months and, according to Cohen and Narrow,
with these conditions improvements in strength and resistance are only shown
after 6 to 8 months of exercise [58]. even affirms that, in spite of the exercise
showing improvements in the trunk muscles’ resistance, intervention
programmes lasting for many months are most effective in improving physical
performance [57]. Although in the intervention group there were no statistically
significant differences in trunk flexors’ strength levels after implementing the
exercise program (although it has increased), in the control group there was a
statistically significant decrease in the strength of these muscles. These
changes were in decrease way, which can show the importance of the applied
programme in preventing atrophy of the trunk flexors. The decrease in strength
values in the control group could be explained by the constant use of lumbar
support belts, which, in the long run, promotes abdominal muscle weakness
[59]. Nevertheless, the influence of lumbar support belts in muscle strength is
still a very controversial issue and, because of that, it should be considered in
future studies. The increased strength and resistance verified in the intervention
group can also be justified by the decrease in pain perception and by
psychological improvement during the programme [39, 52].

62
Analysing the results, statistically significant differences were verified
between groups as to trunk extensors muscle strength. The increase of
registered strength in the intervention group, when compared to the control
group, is consistent with the studies of Mannion et al., which have used the
same methodology for the same measurement of strength and with an intensity
and duration of exercises very similar to the present study [39].
According to Trainor and Wiesel the ratio between trunk
extensors/flexors strength is 1.3/1 [60]. Studies have revealed that patients with
back pain have this ratio altered comparing to the normal population and that a
relation of 1.2/1 to 1.5/1 can be verified in individuals without symptoms (but
likely to get LBP) and of 1.0 in same cases of individuals with back pain [20,
61]. The results of this study have shown a significant increasing change in the
initial ratio (intervention group) of 1.09/1 to 1.15/1 eleven months after following
the exercise program. This change can be seen as having a protective nature
as, according to Lee et al., (1999) the increase in the extensors/flexors strength
ratio has revealed a biggest solidity in preventing future episodes of back pain
[20]. There were also ratio changes when comparing the intervention group with
the control group (intervention group ratio - control group ratio). There are no
experimental studies which evaluate changes in the strength ratio following an
intervention, which calls to the importance of new studies to analyse this
question in more detail.
This study allowed to evaluate the efficiency of a specific exercise
program in warehouse workers. There were significant improvements in
extensor muscle strength and resistance, measured eleven months after
following the exercise program. When comparing both groups, the main
differences were verified in lumbar flexors and extensors strength.
Acknowledgements
This study was supported by a grant from Fundação para a Ciência e
Tecnologia and Instituto Politécnico do Porto (SFRH/BD/50183/2009).
The authors thank all participants in this study for their time and interest.

63
References
1.Rissanen A, Heliovaara M, Alaranta H, Taimela S, Malkia E, Knekt P, et al. Does good trunk extensor performance protect against back-related work disability? J Rehabil Med. 2002;34(2):62-6. Epub 2002/05/22. PubMed PMID: 12019581.
2.Piedrahita H, Oksa J, Malm C, Rintamaki H. Health problems related to working in extreme cold conditions indoors. Int J Circumpolar Health. 2008;67(2-3):279-87. Epub 2008/09/05. doi: 34 [pii]. PubMed PMID: 18767348.
3.Lahiri S, Markkanen P, Levenstein C. The cost effectiveness of occupational health interventions: preventing occupational back pain. Am J Ind Med. 2005;48(6):515-29. Epub 2005/11/22. doi: 10.1002/ajim.20193. PubMed PMID: 16299706.
4.Kent PM, Keating JL. The epidemiology of low back pain in primary care. Chiropr Osteopat. 2005;13:13. Epub 2005/07/28. doi: 1746-1340-13-13 [pii]
10.1186/1746-1340-13-13. PubMed PMID: 16045795; PubMed Central PMCID: PMC1208926.
5.Galukande M, Muwazi S, Mugisa BD.Disability associated with low back pain in Mulago Hospital, Kampala Uganda. Afr Health Sci. 2006;6(3):173-6. Epub 2006/12/05. doi: 10.5555/afhs.2006.6.3.173. PubMed PMID: 17140341; PubMed Central PMCID: PMC1831887.
6.Brox JI, Storheim K, Holm I, Friis A, Reikeras O. Disability, pain, psychological factors and physical performance in healthy controls, patients with sub-acute and chronic low back pain: a case-control study. J Rehabil Med. 2005;37(2):95-9. Epub 2005/03/25. doi: JCAG4RFENCLN278Y [pii]
10.1080/16501970410017738. PubMed PMID: 15788344.
7.O'Sullivan PB, Mitchell T, Bulich P, Waller R, Holte J. The relationship beween posture and back muscle endurance in industrial workers with flexion-related low back pain. Man Ther. 2006;11(4):264-71. Epub 2005/06/15. doi: S1356-689X(05)00043-3 [pii]
10.1016/j.math.2005.04.004. PubMed PMID: 15953751.
8.W IJ, Burdorf A. Impact of musculoskeletal co-morbidity of neck and upper extremities on healthcare utilisation and sickness absence for low back pain. Occup Environ Med. 2004;61(10):806-10. Epub 2004/09/21. doi: 10.1136/oem.2003.011635

64
61/10/806 [pii]. PubMed PMID: 15377765; PubMed Central PMCID: PMC1740669.
9.van Vuuren BJ, Becker PJ, van Heerden HJ, Zinzen E, Meeusen R. Lower back problems and occupational risk factors in a South African steel industry. Am J Ind Med. 2005;47(5):451-7. Epub 2005/04/14. doi: 10.1002/ajim.20164. PubMed PMID: 15828071.
10.Piedrahita H. Costs of work-related musculoskeletal disorders (MSDs) in developing countries: Colombia case. Int J Occup Saf Ergon. 2006;12(4):379-86. Epub 2006/12/13. PubMed PMID: 17156613.
11.Battié MC, Videman T, Gibbons LE, Manninen H, Gill K, Pope M, et al. Occupational driving and lumbar disc degeneration:a case control study. Lancet. 2002:1369-74.
12.Lis AM, Black KM, Korn H, Nordin M. Association between sitting and occupational LBP. Spine J. 2007:283-98.
13.Bovenzi M, Zadini A. Self-reported low back symptoms in urban bus drivers exposed to whole body vibration. Spine. 1992:1948-59.
14.Porter JM, Gyi DE. The prevalence of musculoskeletal troubles among car drivers. Occu Med. 2002:4-12.
15.Wilder DG, Woodworth BB, Frymoyer JM, Pope MH. Vibration and the human spine. Spine. 1982:243-54.
16.De Carvalho DE, Soave D, Ross K, Callaghan JP. Lumbar Spine and Pelvic Posture Between Standing and Sitting: A Radiologic Investigation Including Reliability and Repeatability of the Lumbar Lordosis Measure. J Manipulative Physiol Ther. 2010:48-55.
17.Imamura ST, Kaziyama HD, Imamura M. Lombalgia. Dor músculo-esquelética. São Paulo: Revista Brasileira de Medicina; 2001. p. 375-90.
18.Juul-Kristensen B, Jensen C. Self-reported workplace related ergonomic conditions as prognostic factors for musculoskeletal symptoms: the "BIT" follow up study on office workers. Occu Environ Med. 2005:188-94.
19.Vuuren BJ, Becker PJ, Heerden HJ, Zinzen E, Meeusen R. Lower Back Problems and Occupational Risk Factors in a South African Steel Industry. Ame J Ind Med. 2005:451-7.
20.Lee J, Hoshino Y, Nakamura K, Kariya Y, Saita K, Ito K. Trunk muscle weakness as a risk factor for Low Back Pain: a 5-year prospective study. Spine. 1999:54-7.

65
21.Norris CM. Spinal Stabilisation:3. Stabilisation Mechanisms of the Lumbar SpineStabilization Mechanisms of the Lumbar Spine. Physiotherapy. 1995;81(2):72-9.
22.Comerford MJ, Mottram SL. Movement and stability dysfunction-contemporary developments. Man Ther. 2001:15-26.
23.Richardson C, Jull G, Toppenberg R, Comerford M. Techniques for active lumbar stabilisation for spinal protection: A pilot study. Aust J Phys 1992;38(2):105-12.
24.Sbriccoli P, Yousuf K, Kupershtein I, Solomonow M, Zhou B, Zhu MP, et al. Static load repetition is a risk factor in the development of lumbar cumulative musculoskeletal disorder. Spine. 2004:2643-53.
25.Arokoski JP, Kankaanpaa M, Valta T, Juvoren I, Partanen J, Taimela S, et al. Back and extensor muscle function during therapeutic exercises. Arch Phys Ther Rehab. 1999:842-50.
26.Besler A, Can F. Correlation between pain, trunk muscle strength, and functional state in low back pain. The Pain Clinic. 2003;15(4):415-9. Epub 2003-12-01. doi: DOI: 10.1163/156856903770196791.
27.Hodges PW. Is there a role for transverses abdominis in lumbo-pelvic stability? Man Ther. 1999:74-86.
28.Peltonen JE, Taimela S, Erkintalo M, Salminen JJ, Oksanen A, Kujala UM. Back extensor and psoas muscle cross-sectional area, prior physical training, and trunk muscle strength – a longitudinal study in adolescent girls. Eur J Appl Physiol. 1998:66-71.
29.Rissanen A, Heliövaara M, Alaranta H, Taimela S, Mälkiä E, Knekt P. Does good trunk extensor performance project against back-related work disability? J Rehabil Med. 2002:62-6.
30.Roussel N, Truijen S, Breugelmans S, Claes I, Stassijns G. Reliability of the assessment of lumbar range of motion and maximal isometric strength. Arch Phys Med Rehabil. 2006:576-82.
31.Byrne K, Doody C, Hurley D. Exercise therapy for low back pain: A small-scale exploratory survey of current physiotherapy practice in the Republic of Ireland acute hospital setting. Man Ther. 2006:272-8.
32.Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary Development of a Clinical Prediction Rule for Determining Which Patients With Low Back Pain Will Respond to a Stabilization Exercise Program. Arch Phys Med Rehabil. 2005:1753-62.

66
33.Punnett L, Prüss-Ustün A, Nelson DI, Fingerhut MA, Leigh J, Tak S, et al. Estimating the global burden of low back pain attributable to combined occupational exposures. Am J Ind Med. 2005:459-69.
34.Tveito T, Hysing M, Eriksen H. Low back pain interventions at the workplace: a systemic literature review. Occu Med. 2004:3-13.
35.Lahiri S, Gold J, Levenstein C. Estimation of Net-Costs for Prevention of Occupational Low Back Pain: Three Case Studies From the US. Am J Ind Med. 2005:530-41.
36.Moffett J, Carr J, Howarth E. High fear-avoiders of physical activity benefit from an exercise program for patients with back pain. Spine. 2004:1167-73.
37.Scannell JP, McGill SM. Lumbar posture-should it, and can it, be modified? A study of passive tissue stiffness and lumbar position during activities of daily living. Phys Ther. 2003:907-17.
38.van Poppel MN, Hooftman WE, Koes BW. An update of a systematic review of controlled clinical trials on the primary prevention of back pain at the workplace. Occu Med. 2004:345-52.
39.Mannion AF, Taimela S, Müntener M, Dvorak J. Active Therapy for Chronic Low Back Pain. Part 1. Effects on Back Muscle Activation, Fatigability, and Strength. Spine. 2001:897-908.
40.O'Sullivan P, Mitchell T, Bulich P, Waller R, Holte J, J H. The relationship between posture and back muscle endurance in industrial workers with flexion-related low back pain. Manual Therapy. 2006:264-71.
41.Braggins S. Back Care-A Clinical Aproach. Londres: Churchill Livingstone; 2000.
42.Oddsson LI, De Luca CJ. Activation imbalances in lumbar spine muscles in the presence of chronic low back pain. J Appl Physiol. 2003:1410-20.
43.O'Sullivan P, Mitchell T, Bulich P, Waller R, Holte J. The relationship between posture and back muscle endurance in industrial workers with flexion-related low back pain. Man Ther. 2006:264-71.
44.Holmström E, Ahlborg B. Morning warming-up exercise effects on musculoskeletal fitness in construction workers. Appl Ergonomic. 2005:513-9.
45.Robinson ME, Greene AF, O'Connor P, Graves JE, Millan MM. Reliability of Lumbar Isometric Torque in Patients with Chronic Low Back Pain. Physical Therapy. 1992:186-90.

67
46.Brown LE, Weir JP. ASEP Procedures Recommendation I: Accurate Assessment Of Muscular Strength And Power. Journal of Exercise Physiology online [Internet]. 2001; 4(3):[1-21 pp.].
47.Douris P, Chinan A, Gomez M, Steffens D, Weiss S. Fitness levels of middle aged martial art practitioners. J Sports Med. 2004:143-7.
48.Pettersen J, Hölmich P. Evidence based prevention of hamstring injuries in sport. J Sports Med. 2005:319-23.
49.Remaud A, Cornu C, Guével A. A Methodologic Approach for the Comparison Between Dynamic Contractions: Influences on the Neuromuscular System. J Ath Train. 2005:281-7.
50.Rantanen P, Airaksinen O, Penttinen E. Paradoxical variation of strength determinants with different rotation axes in trunk flexion and extension strength tests. Eur J Appl Physiol. 1994:322-6.
51.Rantanen P, Nykvist F. Optimal sagital motion axis for trunk extension and flexion tests in chronic low back trouble. Clin Biomech. 2000:665-71.
52.Koumantakis GA, Watson PJ, Oldham JA. Supplementation of general endurance exercise with stabilisation training versus general exercise only Physiological and functional outcomes of a randomised controlled trial of patients with recurrent low back pain. Clin Biomechanics. 2005:474-82.
53.McCarthy CJ, Callaghan MJ, Oldham JA. The reliability of isometric strength and fatigue measures in patients with knee osteoarthritis. Man Ther. 2008 May:159-64.
54.Ebrahimi I, Hosseini GR, Salavati M, Farahini H, Arab AM. Clinical trunk muscle endurance tests in subjects with and without low back pain. Medicine Journal of Islamic Republic of Iran. 2005;19(2):95-101.
55.Ebben WP, Jensen RI. Strength Training For Women: Debunking Myths That Block Opportunity. Phys Sports Med. 1998:86-97.
56.Gundewall B, Lilequist M, Hansson T. Primary prevention of back symptoms and absence from work. Spine. 1993:587-94.
57.Moffroid MT. Endurance of trunk muscles in persons with chronic low back pain: Assessment, performance, training. J Rehabil Res Dev. 1997:440-7.
58.Cohen NB, Narrow CM. Effective treatment of back pain. J Am Chirop Assoc. 1999:33-4.
59.Quinn E. The Proper Use of Belts During Weight Training. Sports Med. 2003:72-8.

68
60.Trainor TJ, Wiesel SW. Epidemiology of Back Pain in the Athlete. Clin Sports Med. 2002:93-103.

Capitulo 4
Effect of an exercise program on the quality of lif e of warehouse workers (EM PUBLICAÇÃO NO Applied Research in Quality of Life)


71
ABSTRACT
Background
Low back problems are associated with decreased quality of life. Specific
exercises can improve quality of life, resulting in better professional
performance and functionality.
Aim
The purpose of this study was to evaluate the effect of following a 21-month
exercise program on the quality of life of warehouse workers.
Methods
The population included 557 male warehouse workers from a food distribution
company in Oporto, Portugal. Upon application of the selection criteria, 249
workers were deemed eligible, which were randomized into two groups (125 in
the intervention group and 124 in the control group). Then, subjects were asked
to volunteer for the study, the sample being formed by 229 workers (112 in the
intervention group and 117 in the control group). All subjects completed the SF-
36 questionnaire prior to beginning the program and on the 11th and 21st months
following it. The exercises were executed in the company facilities once a day
for eight minutes. Data were analyzed using SPSS® 17.0 for Windows®.
Results
After 11 months of following the exercise program, there was an increase in all
scores for the experimental group, with statistically significant differences in the
dimensions physical functioning (0.019), bodily pain (0.010), general health
(0.004), and role-physical (0.037). The results obtained at the end of the study
(21 months) showed significant improvements in the dimensions physical
functioning (p=0.002), role-physical (p=0.007), bodily pain (p=0.001), social
functioning (p=0.015), role-emotional (p=0.011), and mental health (p=0.001). In
the control group all dimensions showed a decrease in mean scores.
Conclusion
It can be concluded that the implementation of a low back specific exercise
program has changed positively the quality of life of warehouse workers.
Keywords: occupational health, workers, quality of life, SF-36, specific
exercises.

72
INTRODUCTION
Health and well-being at work are the main focuses that the European
Working Conditions Observatory will advocate to the next years (Giaccone,
2007). Musculoskeletal disorders are among the most widespread illnesses
reported by European workers. According to the fourth European Working
Conditions Survey, carried out in 2005, about 20% of EU15 workers complain of
back problems and muscular pains (Giaccone, 2007). Low back pain (LBP) is
considered one of the major causes of disability (Deyo et al., 1998). After an
initial episode of LBP, 44% to 78% of people suffer a relapse of pain and 26%-
37% have a relapse of work absence. There is little scientific evidence on the
prevalence of chronic non-specific LBP: best estimates suggest that the
prevalence is approximately 23%; 11%12% population is disabled by LBP and
specific causes are unknown (Airaksinen et al., 2006).
It is well-known that the low back region is an important area for support
and transfer of force activities (van Tulder, Malmivaara, & Koes, 2007). In fact,
LBP is a common reason for reduced participation in social and leisure
activities, as well as in professional tasks (Brox, Storheim, Holm, Friis, &
Reikeras, 2005; Galukande, Muwazi, & Mugisa, 2005). Different studies have
reported that chronic LPB, besides being an economic burden to companies, is
a serious public health problem, being more costly than cancer treatment
(Steenstra, Anema, Bongers, de Vet, & van Mechelen, 2003). In fact,
musculoskeletal problems are assumed to be associated with decreased quality
of life (QoL). In specific working populations, the prevalence of musculoskeletal
disorders can be as high as 22%40%, according to a review by van Tulder et
al., (2007).
Exercise programs have proved more efficient than conventional
therapies in the prevention and treatment of LBP, resulting not only in the
reduction of pain and disability but also in lower costs, decreased healthcare
needs, and reduced absenteeism from work (Moffett, Torgerson, Bell-Syer,
Jackson, & Llewlyn-Phillips, 1999). In systematic literature reviews, Bigos et al.,
(2009) present strong evidence that exercise programs are effective in
preventing episodes of back problems. In another study, Rainville et al., (2004)
recognized that there is evidence supporting the use of exercise as a

73
therapeutic tool to improve impairments in back flexibility and strength. In fact,
several studies have observed improvements in global pain ratings and in
behavioral and cognitive aspects of back pain syndromes. Exercise programs
have been shown to promote improved QoL, resulting in better professional
performance and functionality (Airaksinen et al., 2006; Claiborne, Vandenburgh,
Krause, & Leung, 2002).
Interventional preventive measures have been tested in randomized
controlled trials, but results have been controversial. Daltroy et al., (1997) found
that back schools are not an effective intervention of industrial low back injury.
On the other hand, Brox et al., (2008) also noted that back schools were
effective in reducing pain and disability in the short-term, but not in the long-
term. Ijzelenberg, Meerding & Burdorf (2007) did not observe significant
differences in worksite prevention programs for LBP. Probably the lack of
communication with a professional might introduce negative expectations and
dissatisfaction (Goldby, Moore, Doust, & Trew, 2006; Sherman, Cherkin, Erro,
Miglioretti, & Deyo, 2005).
A well-structured exercise program can lead to long-term improvements
for back pain sufferers, (Norris, 1995) diminishing pain, disability, and the effort
required to execute daily activities (Lang, Liebig, Kastner, Neundörfer, &
Heuschmann, 2003) and resulting in improvements in health-related QoL
(Airaksinen et al., 2006; Arnold, Witzeman, Swank, McElroy, & Keck, 2000;
Carroll & Whyte, 2003). According to European guidelines for prevention of LBP
(Burton et al., 2006), physical exercise is recommended for prevention of LBP,
for prevention of recurrence of LBP, and for prevention of recurrence of sick
leave due to LBP (Level C).
As there is no recommendation for the type and intensity of exercise, the
exercise program used in this study was designed specifically for this population
after carefully analyzing all movements and tasks that workers performed
throughout the working day. This study intends to contribute a deeper
knowledge about the relation between exercise programs performed in the
workplace and health-related QoL, taking into account cost benefit, as well as
the characteristicsof the company and itsemployees. Workers received
instructions on the type of exercises they would perform, as well as training

74
activities, which reinforced the idea that physical, social, and mental well-being
are the foundations of QoL (Burton et al., 2006).
The purpose of this study is to evaluate the effect of following a long-term
specific exercise program on health-related QoL of warehouse workers. This
assessment was made by analyzing if the exercise, performed on a daily basis,
improved dimensions of physical functioning, physical role limitations, bodily
pain, social functioning, emotional role limitations, and mental health after 11
and 21 months of following the exercise program.
METHODS
Subjects
The population used in this study included 557 urban, male warehouse
workers from a food distribution company in Oporto, Portugal. All workers were
involved in a routine of overcharge tasks and/or repetitive movements and
worked in low temperatures (between 0º and 4ºC) during all seasons of the
year. According to the company norms, all workers wore cold protective
clothing, gloves, boots, and lumbar support belts.
After informing the clinical physician and human resources staff on the criteria
that would have to be taken into account for subject selection, the company
provided us with an alphabetically organized list of 249 eligible workers,
corresponding to 45% of the population. The sample was randomized into two
groups (125 in the intervention group and 124 in the control group). Then,
subjects were asked to volunteer to participate in the study and give
underwritten consent. The sample included 112 volunteers for the intervention
group and 117 for the control group. At baseline, the sample was n=229,
corresponding to 41% of the population.
Workers were deemed eligible if they met the following criteria: a) they
had a contract for three or more years; and b) they performed the same task
type (assembly and disassembly of pallets. On the other hand, it excluded
individuals who: a) were required to rotate work positions; b) were absent from
work because of back pain; c) had severe back pain (VAS ≥ 5) in the last year;
d) had undergone treatment (conservative or surgical) for LBP in the last year;

75
and e) had been diagnosed with any kind of pathology, which could prevent
them from participating in the prescribed exercises (Sculco, Paup, Fernhall, &
Sculco, 2001).
From the first evaluation moment to the second, there was a total loss of
37.5% of the subjects, 30% from the intervention group and 44.4% from the
control group. From the second to the third evaluation moment there was a total
loss of 34.2% of the individuals, 38.5% from the intervention group, and 29.2%
from the control group. From the first to the third evaluation moment, losses in
the intervention group and in the control group were 57% and 60%,
respectively. After 21 months the sample was reduced to approximately 17% of
the population. These losses resulted from workers leaving the company,
changing workplace, losing motivation to continue in the study, or not answering
the questionnaire.
Table 1 shows values for mean, standard deviation, minimum and
maximum for age (years), height (cm), weight (kg), and body mass index (BMI)
of workers included in the intervention group and in the control group.
Table 1: Values for mean, standard deviation, minimum and maximum of age (years), height (cm), weight
(Kg), and BMI of workers included in the intervention group and in the control group.
n=229 Intervention group
n=112 Control group
n=117 mean±sd min max mean±sd min max
Age (years) 34.41±8.36 20 49 33.05±10.19 18 56
Height (cm) 173.0±0.07 160.0 188.0 178.0±0.09 159.0 188.0
Weight (Kg) 76.54±10.44 55 95 81.07±16.84 60 110
BMI (Kg/m2) 25.57 21.48 26.91 25.58 23.81 31.16
Instrumentation
Health-related QoL was measured using the Short Form Health Survey
(SF-36) self-administered questionnaire, which is a generic health status survey
questionnaire designed to assess the impact of illness on a patient’s QoL (Ware
& Sherbourne, 1992). The SF-36 was translated for the Portuguese population
by Ferreira and yields an 8-dimension profile (Ferreira, 2000a): physical
functioning, role limitations due to physical problems, bodily pain, vitality,
general health perceptions, social functioning, role limitations due to emotional
problems, and mental health. The SF-36 reports the patients' perceived QoL
using scores ranging from zero to 100, zero being the worst score and 100 the

76
best score. The SF-36 has been extensively used in studies addressing patients
with chronic back disorders (Picavet & Hoeymans, 2004). The validity and
reliability of the Portuguese translation of the SF-36 is well documented
(Ferreira, 2000b).
Procedures
The exercise program was implemented in several stages. In the first
evaluation, visits to the warehouse facilities allowed investigation of the types of
tasks executed by workers and the most common injuries. Upon evaluation of
the risks and most repeated gestures, an adequate exercise program was
created. This program included nine easily executed exercises to promote
stretching and strengthening of the soft tissues responsible for spinal stability,
especially lumbar stability. This program was applied, with exercises being
executed daily in the company facilities at the beginning of work and lasting
approximately eight minutes. To motivate workers to adhere to the program and
follow it, there were several training sessions, and posters illustrating the
exercise program were distributed in the company facilities.
Facilitators of the program included physiotherapists, who visited the
warehouse facilities every 15 days to correct possible execution errors or to
answer doubts and questions from workers about the exercise program. The
program efficacy was evaluated in three moments—prior to (M1), at 11 months
(M2), and at 21 months (M3) following participation in the program—by
application of the SF-36 questionnaire.
The control group participated in the pre- and post-program tests. At the
end of the study this group was offered the possibility of executing the same
exercises that were implemented in the intervention group.
The study was conducted between February 2005 and March 2007 with
authorization by the company and according to a protocol between the
institutions involved. All participants provided written, informed consent before
entering the study. All procedures were in accordance with the Helsinki
Declaration. The study design was approved by the ethics committee of Escola
Superior de Tecnologia da Saúde do Porto, in Portugal.

77
Statistics
Exploratory data analysis and sample characterization were performed
using descriptive statistics. Therefore, to check the existence of statistically
significant differences between the data analyzed, before and after
implementing the exercise program, the repeated measures test and the
Friedman ANOVA test were used. The student’s t test for paired samples was
used to analyze differences between mean values in both groups. To analyze
differences between mean values in both groups at the different moments, the
student’s t test for independent samples was used. The level of significance
was set at 0.05, with 95% confidence intervals. Statistical analysis was
conducted using SPSS® 17.0 for Windows®.
RESULTS
Results in table 2 indicate that at baseline, workers in both groups had a
good perception of their QoL. Mean scores of the SF-36 are generally near or
above 80%. However, the analysis does not show statistically significant
differences between groups. It can be observed that the physical functioning
dimension obtained the best mean scores throughout the study in the
intervention group, while both groups showed lower scores in the general health
dimension. The bodily pain dimension obtained the lowest score in the control
group while in the intervention group the worst score obtained was in the vitality
dimension (table 2).
After 11 months of follow-up, groups showed statistically significant
differences in the dimensions physical functioning (0.002), role-physical (0.006),
and bodily pain (0.000) (table 2). At the end of the exercise program, all
dimensions showed increased scores in the intervention group, with the
exception of general health, which obtained a lower score. The control group
obtained the best mean values in the dimensions role-emotional and role-
physical, while lower scores were obtained for the dimensions bodily pain,
vitality, and general health. Nevertheless, it can be observed that mean values,
in all dimensions, decreased throughout the 21-month period in the control
group.

78
Table 2: Values obtained for the 8 dimensions of SF-36 in the form of means and standard deviations, in the intervention group and in the control groups at the three evaluation moments; proof values obtained in the student’s t test for independent samples, between the intervention and control groups, in each evaluation moment.
**P<0.01 and ***P<0.001
When analyzing subjects’ health-related QoL, results have shown that
there were significant differences between the three evaluation moments in
almost all variables, both in the intervention and control groups, as reported in
table 3.
Table 3: Differences between the three evaluation moments in the intervention group and in the control group obtained using the Friedman ANOVA test.
Variables
Intervention group
(P value)
Control group
(P value)
Physical functioning * **
Role-physical * NS
Bodily pain ** NS◊
General health NS *◊
Vitality NS ***
Social functioning * *
Role-emotional * NS
Mental health ** **
*P<0.05, **P<0.01, and ***P<0.001 ◊ Repeated Measures test
In the second evaluation moment (after 11 months of follow-up) there
was an increase in all dimensions for the intervention group, although only
scores for dimensions physical functioning (0.019), bodily pain (0.010), general
health (0.004), and role-physical (0.037) are significant, whereas in the control
group all dimensions showed a decrease in mean scores, with scores in
dimensions physical functioning (0.049) and role-physical (0.006) being the
ones with statistical significance (table 4).
Variables
M1 M2 M3
Intervention group
mean ± sd
Control group
mean ±sd
p value
Intervention group
mean ± sd
Control group
mean ± sd
p value
Intervention group
mean ± sd
Control group
mean ± sd
p value
Physical functioning 91.02±11.325 90.25±11.209 NS 94.22±9.595 88.11±12.0 20 ** 97.50±5.028 84.15±15.481
***
Role-physical 89.00±15.867 88.38±14.539 NS 92.00±12.974 85.28±14. 616 ** 97.01±7.423 85.00±15.608
***
Bodily pain 74.51±22.158 69.22±21.484 NS 82.74±19.108 66.84±21. 251 *** 89.67±15.001 61.79±20.741
***
General health 70.63±13.535 73.04±15.944 NS 76.20±14.364 71.44±16. 531 NS 73.37±11.521 64.84±15.416
**
Vitality 69.11±20.261 74.17±20.798 NS 74.17±17.309 71.82±19. 367 NS 76.04±16.237 63.23±18.866
**
Social functioning 85.30±19.609 85.73±17.669 NS 87.99±16.538 83.91±17. 468 NS 94.39±11.492 78.05±18.68
9 ***
Role-emotional 89.12±15.103 90.10±14.189 NS 93.93±12.555 90.55±13. 018 NS 96.39±8.234 89.18±13.12
5 **
Mental health 78.30±17.470 78.70±18.597 NS 80.44±17.486 81.22±16. 014 NS 89.28±11.097 76.86±19.08
1 ***

79
From the beginning of the study to the end, after 21 months, all
dimensions of the SF-36 have increased in the intervention group, with
differences being statistically significant, except for dimensions general health
and vitality. In the control group, mean values decreased, with scores obtained
in dimensions role-emotional and mental health being not statistically
significant.
Table 4: Values for mean, standard deviation of SF-36 and proof values obtained in the student’s t test for paired samples in the intervention group and in the control group between the first (1st) and second (2nd) and the first (1st) and third (3rd) moments of evaluation.
Variables
Intervention Group Control Group
M2 M1 M3 M2 M1 M3
mean ± sd pvalue mean ± sd pvalue mean ± sd mean ± sd pvalue mean ± sd Pvalue mean ± sd
Physical functioning 94.22±9.595 * 91.02±11.325 ** 97.50±5.028 88.11±12.020 * 90.25±11.209 ** 84.15±15.481
Role-physical 92.00±12.974 NS 89.00±15.867 ** 97.01±7.423 85.28±14.616 ** 88.38±14.539 ** 85.00±15.608
Bodily pain 82.74±19.708 * 74.51±22.158 ** 89.67±15.001 66.84±21.251 NS 69.22±21.484 ** 61.79±20.741
General health 76.20±14.364 ** 70.63±13.535 NS 73.37±11.521 71.44±16.531 NS 73.04±15.944 ** 64.84±15.416
Vitality 74.17±17.309 NS 69.11±20.261 NS 76.04±16.237 71.82±19.367 NS 74.17±20.798 ** 63.23±18.866
Social functioning 87.99±16.538 NS 85.30±19.609 * 94.39±11.492 83.91±17.468 NS 85.73±17.669 ** 78.05±18.689
Role-emotional 93.93±12.555 * 89.12±15.103 * 96.39±8.234 90.55±13.018 NS 90.10±14.189 NS 89.18±1 3.125
Mental health 80.44±17.486 NS 78.30±17.470 * 89.28±11.097 81.22±16.014 ** 78.70±18.597 NS 76.86±19.081
*P<0.05, **P<0.01, and ***P<0.001
From the second to the third moment of evaluation (11th to 21st months),
the intervention group showed statistically significant differences in the
dimension mental health (0.009), whereas in the control group there was a
statistically significant decrease in all dimensions, except for role-physical (table
5).
Table 5: Values for mean, standard deviation of SF-36 and proof values obtained in the student’s t test for paired samples in the intervention group and in the control group between the second (2nd) and third (3rd) moments of evaluation.
Variables Intervention Group Control Group
M2 mean ± sd
M3 mean ± sd p value M2
mean ± sd M3
mean ± sd p value
Physical functioning 94.22±9.595 97.50±5.028 NS 88.11±12.020 84.15±15.48 1 **
Role-physical 92.00±12.974 97.01±7.423 NS 85.28±14.616 85.00±15.6 08 NS
Bodily pain 82.74±19.708 89.67±15.001 NS 66.84±21.251 61.79±20. 741 **
General health 76.20±14.364 73.37±11.521 NS 71.44±16.531 64.84±15. 416 **
Vitality 74.17±17.309 76.04±16.237 NS 71.82±19.367 63.23±18. 866 **
Social functioning 87.99±16.538 94.39±11.492 NS 83.91±17.468 78.05±18. 689 **
Role-emotional 93.93±12.555 96.39±8.234 NS 90.55±13.018 89.18±13.1 25 *
Mental health 80.44±17.486 89.28±11.097 ** 81.22±16.014 76.86±19.081 *
*P<0.05, **P<0.01, and ***P<0.001

80
DISCUSSION
The sample included young male workers (mean age 33-34), with a BMI close
to overweight. Although there is no evidence showing increased weight as a
cause of LBP, several epidemiologic studies showed that there can be a
modest positive association between BMI and LBP (Borenstein, 2000). In fact,
several studies have demonstrated the importance of low back exercise for
spine stabilization, providing better functionality and a consequently better QoL
(Airaksinen et al., 2006; Descarreaux, Normand, Laurencelle, & Dugas, 2002;
Tuncel, Iossifova, Ravelo, Daraiseh, & Salem, 2006; Tuzun, 2007).
In this study, an analysis of the SF-36 dimensions throughout the 21-
month period shows the efficacy of an exercise program, as mean scores
obtained in all dimensions have increased, with results in dimensions physical
functioning, role-physical, bodily pain, social functioning, role-emotional, and
mental health being statistically significant. These results are in accordance with
the results of another study in which the subjective effects of exercise on the
participants’ health and well-being were significantly better in the intervention
group than in the control group (Tveito & Eriksen, 2009). A similar situation
occurred in other studies, where the intervention group tended to have a higher
median baseline physical functioning and bodily pain score on the SF-36
(Santos, Bredemeier, Rosa, Amantéa, & Xavier, 2011).
In the first 11 months of intervention, only three dimensions showed
significant improvement (physical functioning, role limitations physical and
bodily pain) although all of them tended to improve. These results are
consistent with other studies, which have also used pain-specific exercises and
obtained similar results on health-related QoL (Bendix & Bendix, 1997; Carroll &
Whyte, 2003; Walsh & Radcliffe, 2002). In the control group there was a
significant decrease in the dimensions physical functioning and role limitations
physical and a decreasing tendency in the scores of the remaining dimensions.
One possible explanation could be the fact that workers have to execute heavy
tasks all the time and they do not have good motor control. Also, we cannot
forget that 55% of the population suffers episodes of severe back pain every
year. These kinds of factors influence QoL.

81
From the second to the third moment of evaluation there were no
statistically significant differences that showed exercise efficacy on health-
related QoL, with the exception of the dimension mental health in the
intervention group. In the control group there was a steep decrease with
significant differences in all dimensions, except in the dimension role-physical.
A possible explanation for this occurrence could be the fact that during this
period there were changes imposed by the company in terms of working times,
shift work, and increased workload, which could have led to dissatisfaction and
changes in family and social activities. In a large study, Butler & Johnson (2011)
found that workers’ satisfaction with the effectiveness of their health care is
influenced more by reduced perceptions of pain and increased physical
functionality than by the “bedside manner” of health care professionals. In other
words, differences in the type of care provided are important in the early stages
of episodes of back pain but disappear at the 12-month mark. The dominant
influences at 12 months become the workers’ perceptions of the manner in
which they have been treated by the employer. Several studies suggest that
socio-economic and psycho-social factors can negatively affect attitudes and
behaviors (Buchbinder, Jolley, & Wyatt, 2001; Walsh & Radcliffe, 2002)
At the final evaluation (21 months), the intervention group showed
statistically significant differences in all dimensions, except in mental health and
vitality, showing that a specific exercise program can be efficient in increasing
functionality and health-related QoL. These results are consistent with the ones
obtained by Merkesdal & Mau (2005), which have shown that following an
exercise program is efficient in improving daily activities, social relations, and
functional capacity and in diminishing pain, thus contributing to an overall
increase in QoL (Walsh & Radcliffe, 2002). In the intervention group, the
dimension bodily pain improved significantly between evaluation moments, with
individuals feeling less pain, which shows that physical exercise is a good
therapeutic resource in preventing and treating LBP, as it improves weakness
and low isometric resistance of lumbar extensors associated with pain (Pengel,
Herbert, Maher, & Refshauge, 2003). Bendix & Bendix (1997) and Claiborne et
al., (2002) mention that increased activity leads to decreased pain levels and to
better physical performance. This is consistent with the findings obtained in the

82
present study, which show significant improvement in the control group and a
significant decrease in the intervention group at the end of the study.
Improvements in physical function and performance may also result from
the subjects' awareness of the risks they face and their attempt to compensate
these risks with physical exercise. This results in improved physical condition,
increased functionality, and decreased pain, which is in accordance with the
study of Salo et al., (2010), who had similar results in a study applied to women.
At baseline, 55% of the individuals had severe lower back problems, which
reduced the sample to less than half. In the second year, losses were a little
higher than in the first, which could be explained by the fact that during this
period the company demanded more production and changed some
intermediate managers, changes not very well understood by workers.
However, in the study by Santos et al., (2011) there was a loss of 28% of the
sample after nine months of intervention and in the study by Butler & Johnson
(2011) the loss rate was 58% in one year.
Another strong reason for losses throughout the program was the novelty
to do exercise in the company, and also the fact that this was seen as an extra
obligation to the intervention group. Moreover, subjects in the control group did
not seem to understand the importance of their role, despite all the information
and motivation actions taken. The study nature could have also been a
limitation, as it was not possible to control the individuals outside the workplace.
Some factors, such as having more than one job, insufficient rest, holidays, and
non-existence of other entertainment activities, although workplace-
independent, can negatively affect the physical and psychological status of
individuals, as seen in the subjects of this study. The ideal would be to find the
best balance between the costs and benefits for both individuals and companies
(Giaccone, 2007).
This study provides valuable information because it is the first
longitudinal study based on a representative sample of warehouse workers.
Because of the relative insufficiency of evidence on the effectiveness of specific
exercise programs to workers, future trials are needed. In this context, training
institutions and professional organizations should provide continuing education
in pain assessment and management concerning QoL to health professionals at
all levels.

83
CONCLUSIONS
In the long term, a low back specific exercise program positively modified
the quality of life of warehouse workers. After 21 months of following the
exercise program, the dimensions physical functioning, role-physical, bodily
pain, social functioning, role-emotional, and mental health have improved
significantly.
Acknowledgements
This study was supported by a grant from Fundação para a Ciência e
Tecnologia and Instituto Politécnico do Porto (SFRH/BD/50183/2009).
The authors thank all participants in this study for their time and interest.
References
Airaksinen, O., Brox, J. I., Cedraschi, C., Hildebrandt, J., Klaber-Moffett, J., Kovacs, F., . . . Zanoli, G. (2006). Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J, 15 Suppl 2, S192-300. doi: 10.1007/s00586-006-1072-1
Arnold, L. M., Witzeman, K. A., Swank, M. L., McElroy, S. L., & Keck, P. E., Jr. (2000). Health-related quality of life using the SF-36 in patients with bipolar disorder compared with patients with chronic back pain and the general population. J Affect Disord, 57(1-3), 235-239. doi: S0165032799000427 [pii]
Bendix, T., & Bendix, A. F. (1997). [Back pain school]. Ugeskr Laeger, 159(35), 5224-5226.
Bigos, S. J., Holland, J., Holland, C., Webster, J. S., Battie, M., & Malmgren, J. A. (2009). High-quality controlled trials on preventing episodes of back problems: systematic literature review in working-age adults. Spine J, 9, 147–168.
Borenstein, D. G. (2000). Epidemiology, etiology, diagnostic evaluation, and treatment of low back pain. Curr Opin Rheumatol, 12(2), 143-149.
Brox, J. I., Storheim, K., Grotle, M., Tveito, T. H., Indahl, A., & Eriksen, H. R. (2008). Systematic review of back schools, brief education, and fear-avoidance training for chronic low back pain. Spine J, 8, 948–958.
Brox, J. I., Storheim, K., Holm, I., Friis, A., & Reikeras, O. (2005). Disability, pain, psychological factors and physical performance in healthy controls, patients with sub-acute and chronic low back pain: a case-control study. J Rehabil Med, 37(2), 95-99. doi: JCAG4RFENCLN278Y [pii]10.1080/16501970410017738

84
Buchbinder, R., Jolley, D., & Wyatt, M. (2001). Population based intervention to change back pain beliefs and disability:three part evaluation. BMJ, 322, 1516-1520.
Burton, A. K., Balague, F., Cardon, G., Eriksen, H. R., Henrotin, Y., Lahad, A., . . . van der Beek, A. J. (2006). Chapter 2. European guidelines for prevention in low back pain : November 2004. Eur Spine J, 15 Suppl 2, S136-168. doi: 10.1007/s00586-006-1070-3
Butler, R. J., & Johnson, W. G. (2011). Loss reduction through worker satisfaction: the case of workers’ compensation. Risk Management and Insurance Review, 14(1), 1-26. doi: DOI: 10.1111/j.1540-6296.2010.01188.x
Carroll, L. J., & Whyte, A. (2003). Predicting chronic back pain sufferers intention to exercise. British J Ther Rehab, 10, 53-58.
Claiborne, N., Vandenburgh, H., Krause, T. M., & Leung, P. (2002). Measuring quality of life changes in individuals with chronic low back conditions: a back education program evaluation. Evaluation and program planning, 25, 61-70.
Daltroy, L. H., Iversen, M. D., Larson, M. G., Lew, R., Wright, E., Ryan, J., . . . Liang, M. H. (1997). A controlled trial of an educational program to prevent low back injuries. New Eng J Medicine, 337, 322-328.
Descarreaux, M., Normand, M. C., Laurencelle, L., & Dugas, C. (2002). Evaluation of a specific home exercise program for low back pain. J Manip Phys Ther, 25, 497-503.
Deyo, R. A., Battie, M., Beurskens, A. J., Bombardier, C., Croft, P., Koes, B., . . . Waddell, G. (1998). Outcome Measures for Low Back Pain Research: A Proposal for Standardized Use. Spine, 23, 2003-2013.
Ferreira, P. L. (2000a). Criação da versão portuguesa do MOS SF-36.Parte I : adaptação cultural e linguística. Acta Médica Portuguesa, 55-66.
Ferreira, P. L. (2000b). Criação da versão portuguesa do MOS SF-36. Parte II : testes de validação. Acta Médica Portuguesa, 13, 119-127.
Galukande, M., Muwazi, S., & Mugisa, D. B. (2005). Aetiology of low back pain in Mulago Hospital, Uganda. Afr Health Sci, 5(2), 164-167.
Giaccone, M. (2007). Annual review of working conditions in the EU 2006-2007 European Foundation for the Improvement of Living and Working Conditions. Luxembourg: Office for Official Publications of the European Communities.
Goldby, L. J., Moore, A. P., Doust, J., & Trew, M. E. (2006). A randomized controlled trial investigating the efficiency of musculoskeletal physiotherapy on chronic low back disorder. Spine, 31, 1083–1093.
IJzelenberg, H., Meerding, W. J., & Burdorf, A. (2007). Effectiveness of a back pain prevention program: a cluster randomized controlled trial in an occupational setting. Spine, 32, 711-719.
Lang, E., Liebig, K., Kastner, S., Neundörfer, B., & Heuschmann, P. (2003). Multidisciplinary rehabilitation versus usual care for chronic low back pain in the community: effects on quality of life. Spine J, 4, 270-276.
Merkesdal, S., & Mau, W. (2005). Prediction of costs-of-illness in patients with low back pain undergoing orthopedic outpatient rehabilitation. Int J Rehabil Res, 28(2), 119-126. doi: 00004356-200506000-00004 [pii]

85
Moffett, J. K., Torgerson, D., Bell-Syer, S., Jackson, D., & Llewlyn-Phillips, H. (1999). Randomised controlled trial of exercise for low back pain: clinical outcomes, costs, and preferences. BMJ, 319, 279-283.
Norris, C. M. (1995). Spinal Stabilisation:3. Stabilisation Mechanisms of the Lumbar SpineStabilization Mechanisms of the Lumbar Spine. Physiotherapy, 81, 72-79.
Pengel, L. H., Herbert, R. D., Maher, C. G., & Refshauge. (2003). Acute low back pain: systematic review of its prognosis. BMJ, 327, 327-323.
Picavet, H. S., & Hoeymans, N. (2004). Health related quality of life in multiple musculoskeletal diseases: SF-36 and EQ-5D in the DMC3 study. Ann Rheum Dis, 63(6), 723-729. doi: 10.1136/ard.2003.01076963/6/723 [pii]
Rainville, J., Hartigan, C., Martinez, E., Limke, J., Jouve, C., & Finno, M. (2004). Exercise as a treatment for chronic low back pain. Spine J, 4, 106-115.
Salo, P. K., Hakkinen, A. H., Kautiainen, H., & Ylinen, J. J. (2010). Effect of neck strength training on healthrelated quality of life in females with chronic neck pain: a randomized controlled 1-year follow-up study 8:48. Health Qual Life Outcomes, 8.
Santos, A. C., Bredemeier, M., Rosa, K. F., Amantéa, V. A., & Xavier, R. M. (2011). Impact on the Quality of Life of an Educational Program for the Prevention of Work-Related Musculoskeletal Disorders: a randomized controlled trial. BMC Public Health, 11.
Sculco, A. D., Paup, D. C., Fernhall, B., & Sculco, M. J. (2001). Effects of aerobic exercise on low back pain patients in treatment. Spine J, 1(2), 95-101. doi: S1529-9430(01)00026-2 [pii]
Sherman, K. J., Cherkin, D. C., Erro, J., Miglioretti, D. L., & Deyo, R. A. (2005). Comparing yoga, exercise, and a self-care book for chronic low back pain:a randomized, controlled trial. Ann Intern Med, 143, 849–856.
Steenstra, I. A., Anema, J. R., Bongers, P. M., de Vet, H. C., & van Mechelen, W. (2003). Cost effectiveness of a multi-stage return to work program for workers on sick leave due to low back pain, design of a population based controlled trial [ISRCTN60233560]. BMC Musculoskelet Disord, 4, 26. doi: 10.1186/1471-2474-4-261471-2474-4-26 [pii]
Tuncel, S., Iossifova, Y., Ravelo, E., Daraiseh, N., & Salem, S. (2006). Effectiveness of controlled workplace interventions in reducing lower back disorders. Theo Issues in Erg Sci, 7, 211-225.
Tuzun, E. H. (2007). Quality of life in chronic musculoskeletal pain. Best Prat & Res Clin Rheum, 21, 567-579.
Tveito, T. H., & Eriksen, H. R. (2009). Integrated health programme: a workplace randomized controlled trial. J Adv Nurs, 65(1), 110-119. doi: JAN4846 [pii]10.1111/j.1365-2648.2008.04846.x
van Tulder, M., Malmivaara, A., & Koes, B. (2007). Repetitive strain injury. Lancet, 369, 1815-1822.
Walsh, D. A., & Radcliffe, J. C. (2002). Pain beliefs and perceived physical disability of patients with chronic low back pain. Pain, 97, 23-31.
Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care, 30(6), 473-483.

Discussão


88
Discussão
Relativamente às caraterísticas da amostra, os grupos mostraram-se
homogéneos no início do estudo não existindo diferenças estaticamente
significativas quanto ao peso, altura e Índice de Massa Corporal (IMC).
Contudo, o IMC da amostra mostrou estar próximo da classificação de excesso
de peso.Apesar de não se ter encontrado evidência que prove que o excesso
de peso seja causa de problemas vertebrais, nomeadamente da região lombar,
vários estudos mostram a existência de correlação moderada entre o IMC e dor
lombar (Borenstein, 2000).
Na amostra, incluíram-se apenas indivíduos do sexo masculino,
principalmente devido às características da força e resistência serem diferentes
entre sexos (Ebben & Jensen, 1998) e também porque as mulheres que
trabalhavam neste armazém tinham tarefas específicas, tais como limpezas e
não realizavam o mesmo tipo de tarefas dos homens.
Neste trabalho utilizou-se para a avaliação da sintomatologia a versão
portuguesa do standardized Nordic musculoskeletal questionnaire (Mesquita et
al., 2010).
As adaptações culturais e linguísticas dos questionários envolvem
processos de tradução e de retroversão para a língua original, assim como a
análise das propriedades psicométricas. Neste estudo estes processos
desenvolveram-se sem dificuldades e estiveram de acordo com as normas do
Medical Outcomes Trust (1997) e do European Group on Health Outcomes
(ERGHO). A validade de conteúdo foi obtida durante o processo de tradução e
retroversão, o qual foi constituído por um painel de juízes: pessoas comuns,
dois tradutores oficiais, um deles bilingue e fisioterapeutas. Este painel tem
como objetivos verificar incongruências ou redundâncias em cada item do
questionário (Beaton & Schemitsch, 2003). A validade de critério foi testada
com o Oswestry disability índex (ODI) tendo-se obtido uma correlação
moderada e positiva para as regiões torácica e lombar, na variável, últimos 7
dias e para a região lombar, variável, limitações em atividades nos últimos 12
meses. Não se conseguiu mais nenhuma correlação, porém ODI mede o

89
impacto de disfunção apenas para a dor lombar, tendo sido uma das limitações
deste estudo. Contudo o ODI foi o questionário que se encontrou em Portugal,
que reunia mais semelhanças com o NQM.
Quanto aos resultados da fiabilidade, estes foram muito bons tendo os
índices de correlação variado entre 0.7 e 1. Estes resultados estão de acordo
com a versão original que foi entre 0.8 e 1(Kuorinka et al., 1987) e com um
trabalho realizado por Palmer, Smith, Kellingray, & Cooper (1999) que
encontrou índices do coeficiente de Kappa igual a 1. Na versão portuguesa
para a população brasileira os coeficientes de correlação para a fiabilidade
também variaram entre 0.63 e 1 (de Barros & Alexandre, 2003). Numa recente
investigação, na Austrália, Dawson, Steele, Hodges, & Stewart, (2010), os
coeficientes de correlação foram de k/kmax=0.71-0.96 e k/kmax=0.76-1.
Relativamente à consistência interna o coeficiente de correlação, Kuder-
Richardson foi de 0.855 indicando ser muito bom (Carmines & Zeller, 1991).
Infelizmente não foi possível comparar este resultado com outros porque nos
estudos consultados não constavam resultados sobre consistência interna.
Cada vez mais se torna imprescindível a existência de instrumentos
validos e fiáveis para que se possa comparar os resultados obtidos a nível
nacional e internacional (MacDermid, Walton, & Law, 2009; Pynsent, 2001).
No início do estudo, antes da intervenção do programa de exercícios
específicos, momento 1 (M1) não se verificaram diferenças estatisticamente
significativas que mostrassem a existência de diferenças entre o grupo de
intervenção e o de controlo ao nível da sintomatologia músculo-esquelética e
da perceção da qualidade de vida. Na generalidade, pode dizer-se que os
grupos de intervenção e de controlo eram homogéneos. Relativamente às
diferenças entre grupos, manhã, tarde e noite, também não se verificaram
diferenças estatisticamente significativas.
Relativamente aosresultados do NMQ, em M1, mostraram que a região
corporal em que os operários relataram maior proporção de sintomas foi a
região lombar, em ambos os grupos. Este facto pode serdevido ao tipo de
tarefas realizadas pelos indivíduos deste estudo: fazer e desfazer paletes, fazer
picking, manobrar empilhadoras em pé, em rotação vertebral quer para a direita

90
quer para a esquerda, manobrar empilhadoras em posição de sentado, tarefas
típicas dos trabalhadores que operam em grandes armazéns.
Estesresultadosestão em concordância com outrosestudos nos quais se
encontraram resultados semelhantes (Alexopoulos, Stathi, & Charizani, 2004;
Alexopoulos et al., 2006; Alipour et al., 2008; Bergman, 2007; Keyserling et al.,
2005; Punnett &Wegman, 2004).
Ao analisar os níveis de força e resistência muscular antes da
implementação do programa de exercícios verificou-se que os grupos de
intervenção e controlo apresentavam valores diferentes e, em algumas
variáveis, força e resistência dos extensores, eram estatisticamente
significativos. Não se encontra explicação para este facto, contudo é de
salientar que o valor do rácio entre a força dos extensores e flexores é de 1.1/1
para o grupo de intervenção e de 1.03/1 para o grupo de controlo. Estes
valores de rácio são relevantes pois, segundo Trainor & Wiesel (2002), os
valores ideais deveriam ser de 1.3/1,pois abaixo deste rácio existe o risco de
lesão na região lombar. Estes valores complementam a sintomatologia
apresentada pelos indivíduos. Estes resultados poderãoser devido ao tipo de
tarefas efetuadas pelos trabalhadores que exigem aumento da flexão com
rotação do tronco, provocando alongamento e tensão dos tecidos moles da
região posterior, podendo levar a problemas músculo-esqueléticos. Estes
efeitos estimulam os mecanorreceptores causando fadiga e desconforto na
região lombar, sendo que a tensão muscular com isquemia têm sido propostas
como originadoras de dor nociceptiva (Feyer et al., 2000; Kaser et al., 2001;
Keyserling et al., 2005; Marras, Granta, & Davis, 1999; Marras, Lavender,
Ferguson, Splittstoesser, & Yang, 2010; Moffett et al., 1999). A reforçar este
facto são os scores apresentados pelo SF-36, que apesar de no geral estarem
muito bons, as dimensões Dor Física e Saúde em Geral apresentam os valores
mais baixos, influenciando a qualidade de vida.
No segundo momento de avaliaçãoverificaram-se melhorias
significativas, na sintomatologia da região lombar em duas das variáveis,
sintomatologia e limitações nos últimos 12 meses. No entanto, em quase todas
as regiões, a sintomatologia no grupo de intervenção diminui sem que as
diferenças fossem estatisticamente significativas. No grupo de controlo a

91
sintomatologia aumentou, principalmente na região lombar, embora as
diferenças não fossem significativas. Entre M2 e M3 não se verificaram
diferenças estatisticamente significativas em nenhum dos grupos, contudo a
tendência anterior manteve-se, o grupo de intervenção a reduzir as queixas e o
grupo de controlo a aumentar. As diferenças estatisticamente significativas
verificaram-se em M1-M3 na região lombar, no grupo de intervenção,
mostrando um aumento da capacidade funcional, em indivíduos com lombalgia,
após um programa de exercícios específicos para a região lombar como
também é referido em diversos estudos (Arokoski et al., 2004; Kuukkanen &
Malkia, 2000; Moseley, 2002; O'Sullivan, Mitchell, Bulich, Waller, & Holte, 2006;
Rainville, Hartigan, Martinez, et al., 2004; Waddell & Burton, 2001). Estes
referem queos programas de exercício específicos podem reduzir a intensidade
da dor lombar e aliviar a incapacidade funcional naqueles que sofrem de dor
lombar subaguda e crónica. Kasai (2006) utilizando um programa de exercícios
de alongamento, desenhados para aumentar a flexibilidade da região lombar,
também obteve aumentos significativos na capacidade funcional dos
indivíduos. Segundo Friedrich, Gittler, Arendasy, & Friedrich (2005) os
benefícios apenas podem ser atingidos se os exercícios forem realizados
regular e consistentemente. Os efeitos dos exercícios na capacidade funcional
subsistem apenas quando os indivíduos continuam o exercício por um longo
período de tempo (Peate, Bates, Lunda, Francis, & Bellamy, 2007).
Ao longo dos 21 meses deste estudo nas regiões do pescoço, ombros,
cotovelos, mãos/punhos, torácica, ancas/coxas, joelhos e pés/tornozelos, não
se verificaram diferenças estatisticamente significativas em nenhuma das
variáveis embora a proporção de sintomatologia ao nível da região do pescoço
seja preocupante e deva ser tida em conta nos próximos programas de
exercício, pois, tal como a região lombar, ela é também uma região de
transição onde pode vir a existir problemas de instabilidade e
consequentemente dor e limitações funcionais.Relativamente à intensidade da
dor devido a SME nas diversas regiões não se verificaram diferenças
estatisticamente significativas para afirmar que se verificaram alterações ao
longo do estudo.

92
Quanto à força e resistência muscular os resultados neste estudo
mostraram que houve aumentos significativos nos extensores, tal como no
estudo de (Moffroid, 1997), apesar de este ter sido um programa de seis
semanas e apenas contemplou fortalecimento dos extensores. Nos flexores, a
força e resistência aumentaram mas as diferenças não foram significativas.
Estes resultados estão mais de acordo com os de (Koumantakis, Watson, &
Oldham, 2005), que após um programa de 15 minutos que era específico para
a região lombar também obtiveram resultados de aumento de força, tanto dos
extensores como dos flexores. O mesmo tipo de resultados foi obtido em
diversos trabalhos, apesar de serem de características diferentes, pois alguns
decorriam apenas duas vezes por semana com uma duração de 15 a 20
minutos (Gundewall, Lilequist, & Hansson, 1993; Mannion, Taimela, Müntener,
& Dvorak, 2001).
Quanto ao rácio alguns autores preconizam que o ideal seria entre 1.2/1
e 1.5/1, pois foram os valores encontrados em população assintomática e 1.1/1
em algumas situações de indivíduos com dor lombar (Lee et al., 1999; Vital,
Melo, Nascimento, & Roque, 2007). Os valores de rácio extensores/flexores,
neste estudo, em M2, foram de 1.16/1 para o grupo de intervenção tendo esta
diferença sido estatisticamente significativa e de 1.08/1 para o grupo de
controlo. Este último rácio aumentou ligeiramente, mas não foi devido ao
aumento da força dos extensores e sim devido a um decréscimo significativo
da força dos flexores. De acordo com os autores acima referenciados, pensa-
se que os indivíduosdeste estudo, estão em risco de ocorrência de lesões
lombares porque ambos os grupos apresentaram rácios abaixo de 1.2/1. O
acentuado decréscimo de força dos flexores poderá ser devido ao uso
continuado dos cintos lombares (Quinn, 2003). Este autor preconiza que
quando existe uma utilização continuada destes cintos de suporte há uma
promoção de fraqueza dos músculos abdominais. Num outro estudo,
transversal, sobre o uso de cintos lombares, Darren & London (2007)
verificaram que o uso dos cintos aumentava a dor lombar, contudo este estudo
foi realizado em condutores de táxi e os autores são cautelosos nas suas
conclusões, porque não tinham um grupo de controlo randomizado e era muito
pequeno relativamente ao experimental.

93
Teria sido interessante verificar-se como estes resultados da força e
resistência evoluiriam em M3, após os 21 meses de intervenção, mas tal não
foi possível devido a avaria do instrumento de medição (Ergometer) e da sua
reparação ter demorado alguns meses. Esta foi a grande limitação deste
estudo porque apenas existem resultados para 11 meses e não para 21 meses,
tal como seria de esperar.
Quanto á perceção da qualidade de vida, em M2, apenas três
dimensões mostraram melhorias significativas, a função física, o desempenho
físico e a dor corporal; todavia, verificou-se uma tendência geral de subida em
todos os scores do SF-36. Estes resultados são semelhantes aos obtidos em
outros estudos sobre qualidade de vida e programas de exercício (Bendix &
Bendix, 1997; Carroll & Whyte, 2003; Walsh & Radcliffe, 2002). Entre M2-M3
não existiram melhorias significativas, exceto na dimensão saúde mental. No
final do programa, o grupo de intervenção melhorou significativamente em
quase todos os scores do Sf-36, exceto na saúde em geral e vitalidade que as
diferenças dos resultados não foram significativas, notando-se, no entanto, um
aumento dos resultados. Estes mostraram que o programa de exercício físico
específico para a região lombar foi positivo para os indivíduos do grupo de
intervenção, que melhoraram a sua qualidade de vida ao longo dos 21 meses.
Tal é consistente com outros estudos que verificaram que o exercício melhora
as relações sociais, atividades da vida diária e na capacidade funcional,
diminuindo a dor e contribuindo assim para um aumento da qualidade de vida
(Merkesdal & Mau, 2005; Pengel, Herbert, Maher, & Refshauge, 2003; Walsh &
Radcliffe, 2002). Os resultados obtidos através do SF-36, que dão a perceção
da qualidade de vida que o indivíduo tem de si mesmo, estão de acordo com os
resultados do NMQ em que se verificou uma diminuição da dor lombar e
consequentemente das limitações nas atividades do dia-a-dia, estando de
acordo com a maioria da literatura que tem vindo a preconizar a importância do
exercício específico realizado no posto de trabalho como forma de prevenção e
de evitar lesões na coluna na lombar (Bendix, Bendix, Lund, Kirkbak, &
Ostenfeld, 1997; Claiborne et al., 2002; Harkness, Macfarlane, Nahit, Silman, &
McBeth, 2003; Santos, Bredemeier, Rosa, Amantea, & Xavier, 2011; Tveito &
Eriksen, 2009).

94
No momento 1, antes da intervenção, verificou-se que 55% da
população já tinham tido problemas severos de lombalgias, em que estiveram
ausentes no último ano mais de um mês e 10% destes já tinham sido
intervencionados cirurgicamente à coluna vertebral. Dos 45% da população
que cumpria os critérios de inclusão e no momento da primeira avaliação
aproximadamente 30% da população referiu dor lombar e a faixa etária foi de
33 anos em média, ou seja, estes números são um pouco alarmantes e pela
literatura revista não existe uma relação de causalidade (Roffey et al., 2010;
Wai et al., 2010) mas sabe-se que a única forma de tentar prevenir e tratar as
lesões músculo-esqueléticas são através de programas de intervenção
específicos para as populações em risco (Airaksinen et al., 2006; Descarreaux
et al., 2002; Tuncel, 2006; Tuzun, 2007).
A generalidade dos estudos de investigação apresenta um conjunto de
limitações associado. Este projeto apresenta igualmente algumas limitações,
nomeadamente o elevado número de perdas, podendo levar à não ocorrência
de alguns resultados esperados, ou à inexistência de resultados significativos,
fruto de algumas dessas limitações. Porém, este tipo de limitações são de difícil
controlo em situações reais, embora toda a equipa de trabalho tenha estado
sempre atenta e empenhada na motivação dos indivíduos para a participação e
importância deste estudo. Todavia, as perdas deste estudo são relativamente
semelhantes às perdas de 28% referidas por Santos et al. (2011) ao fim de
nove meses de intervenção e das de Butler & Johnson (2011), que reportaram
perdas de 58% da amostra ao fim de um ano de intervenção. Eventualmente,
uma outra razão para a desistência do programa, e dos controlos, foi o facto
dealguns indivíduos considerarem que como o programa era executado dentro
e no horário da empresa, os exercícios eram considerados mais uma obrigação
e tarefa por parte da empresa do que um benefício ou vantagem para os
trabalhadores.
Outra limitação foi o não controlo das tarefas, das horas de descanso, da
presença ou não de um segundo emprego, dos hábitos alimentares e das
atividades recreativas ou desportivas dos operários dos dois grupos fora das
horas laborais.

95
Este estudo afigura-se relevante, visto ter sido experimental e de longa
duração, o que permitiu ter acesso a dados concretos acerca dos trabalhadores
portugueses e das suas reais necessidades e problemas. Uma vez que os
distúrbios músculo-esqueléticos são um problema cada vez mais comum entre
a população trabalhadora, causando elevados níveis de incapacidade nos
indivíduos e consequentemente redução da qualidade de vida, passando os
indivíduos a ter que lidar diariamente com a dor, sugere-se que sejam
efetuados mais estudos experimentais de longa duração sobre estratégias
preventivas, englobando também estudos ergonómicos de modo a diminuir
todas estas sequelas. Seria também importante testar e comparar outro tipo de
programas de atividade física de forma a perceber se existiriam diferenças nos
resultados.

Conclusões


98
Conclusões
A adaptação para a população portuguesa do Standardized Nordic
Musculoskeletal questionnaire evidenciou bons índices de correlação de
fiabilidade e de moderada validade.
O programa de exercícios específicos demonstrou ser eficaz na
diminuição da sintomatologia músculo-esquelética, na região lombar, ao longo
de um período de 21 meses, nas suas três variáveis: sintomatologia nos
últimos 12 meses, limitações nos últimos 12 meses e sintomatologia nos
últimos 7 dias, em trabalhadores de armazém.
Nas outras regiões (pescoço, ombros, cotovelos, mãos/punhos, torácica,
ancas/coxas, joelhos e pés/tornozelos, não se verificaram alterações
significativas da sintomatologia, nas suas três variáveis, com a inserção do
programa de exercícios específicos.
O programa de exercícios específicos aplicado em trabalhadores de
armazém, durante 11 meses, mostrou que a força e resistência dos músculos
extensores lombares aumentaram significativamente. Relativamente à força e
resistência dos flexores aumentou, mas não foi demonstrada evidência
estatística.
Quanto à qualidade de vida dos indivíduos, aos quais se aplicou o
programa de exercícios específicos, esta, evidenciou aumentos significativos
nas dimensões: Função Física, Desempenho Físico, Dor Física, Função Social,
Desempenho Emocional e Saúde Mental.


Bibliografia Geral


102
Bibliografia
Airaksinen, O., Brox, J. I., Cedraschi, C., Hildebrandt, J., Klaber-Moffett, J.,
Kovacs, F., . . . Zanoli, G. (2006). Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J, 15 Suppl 2, S192-300. doi: 10.1007/s00586-006-1072-1
Ala-Mursula, L., Vahtera, J., Pentti, J., & Kivimäki, M. (2004). Effect of
employee worktime control on health: a prospective cohort study. Occup Environ Med, 61, 254-261.
Alexopoulos, E. C., Burdorf, A., & Kalokerinou, A. (2003). Risk factors for
musculoskeletal disorders among nursing personnel in Greek hospitals. Int Arch Occup Environ Health, 76(4), 289-294. doi: 10.1007/s00420-003-0442-9
Alexopoulos, E. C., Stathi, I. C., & Charizani, F. (2004). Prevalence of
musculoskeletal disorders in dentists. BMC Musculoskelet Disord, 5, 16. doi: 10.1186/1471-2474-5-161471-2474-5-16 [pii]
Alexopoulos, E. C., Tanagra, D., Konstantinou, E., & Burdorf, A. (2006).
Musculoskeletal disorders in shipyard industry: prevalence, health care use, and absenteeism. BMC Musculoskelet Disord, 7, 88. doi: 1471-2474-7-88 [pii]10.1186/1471-2474-7-88
Alipour, A., Ghaffari, M., Shariati, B., Jensen, I., & Vingard, E. (2008).
Occupational neck and shoulder pain among automobile manufacturing workers in Iran. Am J Ind Med, 51(5), 372-379. doi: 10.1002/ajim.20562
Andersen, L. L., Christensen, K. B., Holtermann, A., Poulsen, O. M., Sjøgaard,
G., Pedersen, M. T., & Hansen, E. A. (2010). Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: a one-year randomized controlled trial. Man Ther, 15(1), 100-104. doi: S1356-689X(09)00137-4 [pii]10.1016/j.math.2009.08.004
Arnold, L. M., Witzeman, K. A., Swank, M. L., McElroy, S. L., & Keck Jr, P. E.
(2000). Health-related quality of life using the SF-36 in patients with bipolar disorder compared with patients with chronic back pain and the general population. J Affect Disord, 57, 235-239.
Arokoski, J. P., Kankaanpaa, M., Valta, T., Juvonen, I., Partanen, J., Taimela,
S., . . . Airaksinen, O. (1999). Back and hip extensor muscle function during therapeutic exercises. Arch Phys Med Rehabil, 80(7), 842-850. doi: S0003-9993(99)90237-X [pii]
Arokoski, J. P., Valta, T., Airaksinen, O., & Kankaanpaa, M. (2001). Back and
abdominal muscle function during stabilization exercises. Arch Phys Med Rehabil, 82(8), 1089-1098. doi: S0003999301859232 [pii]

103
Arokoski, J. P., Valta, T., Kankaanpaa, M., & Airaksinen, O. (2004). Activation of lumbar paraspinal and abdominal muscles during therapeutic exercises in chronic low back pain patients. Arch Phys Med Rehabil, 85(5), 823-832. doi: S0003999303009420 [pii]
Beaton, D. E., & Schemitsch, E. (2003). Measures of health-related quality of
life and physical function. Clin Orthop Relat Res(413), 90-105. doi: 10.1097/01.blo.0000079772.06654.c8
Bendix, A. F., Bendix, T., Lund, C., Kirkbak, S., & Ostenfeld, F. (1997).
Comparison of three intensive programs for chronic low back pain patients: a prospective, randomized, observer-blinded study with one-year follow-up. Scand J Rehabil Med, 29, 81-89.
Bergman, S. (2007). Management of musculoskeletal pain. Best Pract Res Clin
Rheumatol, 21(1), 153-166. doi: S1521-6942(06)00122-7 [pii]10.1016/j.berh.2006.10.001
Bernard, B. P. (1997). A Critical Review of Epidemiologic Evidence for Work-
Related Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back. Columbia-Cincinnati: National Institute for Occupational Safety and Health.
Besler, A., & Can, F. (2003). Correlation between pain, trunk muscle strength, and functional state in low back pain. The Pain Clinic, 15(4), 415-419. doi: DOI: 10.1163/156856903770196791
Bigos, S. J., Holland, J., Holland, C., Webster, J. S., Battie, M., & Malmgren, J.
A. (2009). High-quality controlled trials on preventing episodes of back problems: systematic literature review in working-age adults. Spine J, 9(2), 147-168. doi: S1529-9430(08)01430-7 [pii] 10.1016/j.spinee.2008.11.001
Bonde, J. P., Mikkelsen, S., Andersen, J. H., Fallentin, N., Bælum, J., & Svendsen SW, S. W. (2005). Understanding work related musculoskeletal pain: does repetitive work cause stress symptoms? Occup Environ Med, 62, 41-48.
Bongers, P. M., Ijmker, S., van den Heuvel, S., & Blatter, B. M. (2006).
Epidemiology of work related neck and upper limb problems: psychosocial and personal risk factors (part I) and effective interventions from a bio behavioural perspective (part II). J Occup Rehabil, 16(3), 279-302. doi: 10.1007/s10926-006-9044-1
Borenstein, D. G. (2000). Epidemiology, etiology, diagnostic evaluation, and
treatment of low back pain. Curr Opin Rheumatol, 12(2), 143-149. Brereton, L., & McGill, S. M. (1999). Effects of physical fatigue and cognitive
challenges on the potential for low back injury. Hum Mov Sci, 18, 839–857.

104
Brox, J. I., Storheim, K., Grotle, M., Tveito, T. H., Indahl, A., & Eriksen, H. R. (2008). Systematic review of back schools, brief education, and fear-avoidance training for chronic low back pain. Spine J, 8(6), 948-958. doi: S1529-9430(07)00700-0 [pii]10.1016/j.spinee.2007.07.389
Brox, J. I., Storheim, K., Holm, I., Friis, A., & Reikeras, O. (2005). Disability,
pain, phychological factors and physical performance in healthy controls, patients with sub-acute and chronic low back pain: a case-control study. Journal of Rehabilitation Medicine, 37 (2), 95-99.
Burton, A. K., Balague, F., Cardon, G., Eriksen, H. R., Henrotin, Y., Lahad, A., .
. . van der Beek, A. J. (2006). Chapter 2. European guidelines for prevention in low back pain : November 2004. Eur Spine J, 15 Suppl 2, S136-168. doi: 10.1007/s00586-006-1070-3
Butler, R. J., & Johnson, W. G. (2011). Loss reduction through worker
satisfaction: the case of workers’ compensation. Risk Management and Insurance Review, 14(1), 1-26. doi: DOI: 10.1111/j.1540-6296.2010.01188.x
Byrne, K., Doody, C., & Hurley, D. A. (2006). Exercise therapy for low back
pain: a small-scale exploratory survey of current physiotherapy practice in the Republic of Ireland acute hospital setting. Man Ther, 11(4),272-278.doi: S1356-89X(05)000731[pii]10.1016/j.math.2005.06.002
Byrns, G., Reeder, G., Jin, G., & Pachis, K. (2004). Risk factors for work-related
low back pain in registered nurses, and potential obstacles in using mechanical lifting devices. J Occup Environ Hyg, 1(1), 11-21. doi: D5FRX11CE212JPYK [pii]10.1080/15459620490249992
Cancelliere, C., Cassidy, J. D., Ammendolia, C., & Côté, P. (2011). Are
workplace health promotion programs effective at improving presenteeism in workers? A systematic review and best evidence synthesis of the literature. BMC Public Health, 11, 395. doi: 1471-2458-11-395 [pii]10.1186/1471-2458-11-395
Carmines, E., & Zeller, R. (1991). Reliability and validity assessment.: Newbury
Park: Sage Publications. Carroll, C., Rick, J., Pilgrim, H., Cameron, J., & Hillage, J. (2010). Workplace
involvement improves return to work rates among employees with back pain on long-term sick leave: a systematic review of the effectiveness and cost-effectiveness of interventions. Disabil Rehabil, 32(8), 607-621. doi: 10.3109/09638280903186301
Carroll, L. J., & Whyte, A. (2003). Predicting chronic back pain sufferers
intention to exercise. British J Ther Rehab, 10, 53-58.

105
Ceran, F., & Ozcan, A. (2006). The relationship of the Functional Rating Index with disability, pain, and quality of life in patients with low back pain. Med Sci Monit, 12(10), CR435-439. doi: 6272 [pii]
Chaffin, D. B., & Park, K. Y. (1973). A longitudinal study of low back pain as
associated with occupational weight lifting factors. Am Ind Hyg Assoc J, 34, 513–525.
Cherry, N. M., Meyer, J. D., Chen, Y., Holt, D. L., & McDonald, J. C. (2001). The
reported incidence of work-related musculoskeletal disease in the UK: Moss 1997-2000. ; 51:. Occup Med, 51, 450-455.
Cholewicki, L., & McGill, S. M. (1996). Mechanical stability of the in vivo lumbar
spine: implications for injury and chronic low backpain. Clin Biomech, 11, 1-15.
Claiborne, N., Vandenburgh, H., Krause, T. M., & Leung, P. (2002). Measuring
quality of life changes in individuals with chronic low back conditions: a back education program evaluation. Evaluation and program planning, 25, 61-70.
Comerford, M. J., & Mottram, S. L. (2001). Functional stability re-training:
principles and strategies for managing mechanical dysfunction. Man Ther, 6(1), 3-14. doi: 10.1054/math.2000.0389S1356-689X(00)90389-8 [pii]
Costa, D., & Palma, A. (2005). O efeito do treinamento contra resistência na
síndrome da dor lombar. Revista Portuguesa de Ciencias do Desporto, 5(2), 224-234.
Costa, G. (2003). Shift work and occupational medicine: an overview. Occup
Med (Lond), 53(2), 83-88. Critchley, D. (2002). Abdominal Muscle Function in Chronic Low Back Pain
Patients. Physiotherapy, 88. Côté, P., Cassidy, D., Carroll, L., & Kristman, V. (2004). The annual incidence
and course of neck pain in the general population: a population-based cohort study. ; : . Pain, 112, 267-273.
Dankaerts, W., O'Sullivan, P. B., Burnett, A. F., Straker, L. M., & Danneels, L. A.
(2004). Reliability of EMG measurements for trunk muscles during maximal and sub-maximal voluntary isometric contractions in healthy controls and CLBP patients. J Electromyogr Kinesiol, 14(3), 333-342. doi: S1050641103001093 [pii]10.1016/j.jelekin.2003.07.001
Darren, M. J., & London, L. (2007). A cross-sectional study of back belt use and
low back pain amongst forklift drivers. International Journal of Industrial Ergonomics, 37(6), 505-513. doi: 10.1016/j.ergon.2007.02.005

106
Dawson, A. P., Steele, E. J., Hodges, P. W., & Stewart, S. (2010). Utility of the Oswestry Disability Index for studies of back pain related disability in nurses: evaluation of psychometric and measurement properties. Int J Nurs Stud, 47(5), 604-607. doi: S0020-7489(09)00349-6 [pii]10.1016/j.ijnurstu.2009.10.013
de Barros, E. N., & Alexandre, N. M. (2003). Cross-cultural adaptation of the
Nordic musculoskeletal questionnaire. Int Nurs Rev, 50(2), 101-108. doi: 188 [pii]
Dembe, A. E., Erickson, J. B., Delbos, R. G., & Banks, S. M. (2005). The impact
of overtime and long work hours on occupational injuries and illnesses: new evidence from the United States. Occup Environ Med, 62, 588-597.
Denis, D., St-Vincent, M., Imbeau, D., Jette, C., & Nastasia, I. (2008).
Intervention practices in musculoskeletal disorder prevention: a critical literature review. Appl Ergon, 39(1), 1-14. doi: S0003-6870(07)00022-1 [pii]10.1016/j.apergo.2007.02.002
Descarreaux, M., Normand, M. C., Laurencelle, L., & Dugas, C. (2002).
Evaluation of a specific home exercise program for low back pain. J Manipulative Physiol Ther, 25(8), 497-503. doi: S0161475402000477 [pii]
Deyo, R. A., Battie, M., Beurskens, A. J., Bombardier, C., Croft, P., Koes, B., . .
. Waddell, G. (1998). Outcome measures for low back pain research. A proposal for standardized use. Spine (Phila Pa 1976), 23(18), 2003-2013.
Dovrat, E., & Katz-Leurer, M. (2007). Cold exposure and low back pain in store
workers in Israel. Am J Ind Med, 50, 626-631. Dunn, K. M., Jordan, K., & Croft, P. R. (2006). Characterizing the course of low
back pain: a latent class analysis. Am J Epidemiol, 163(8), 754-761. doi: kwj100 [pii]10.1093/aje/kwj100
Dunning, K. K., Davis, K. G., Cook, C., Kotowski, S. E., Hamrick, C., Jewell, G.,
& Lockey, J. (2010). Costs by industry and diagnosis among musculoskeletal claims in a state workers compensation system: 1999-2004. Am J Ind Med, 53(3), 276-284. doi: 10.1002/ajim.20774
Ebben, W. P., & Jensen, R. I. (1998). Strength Training For Women: Debunking
Myths That Block Opportunity. Phys Sports Med, 26, 86-97. Edwards, J. A., Van Laar, D., Easton, S., & Kinman, G. (2009). The Work-
related Quality of Life Scale for Higher Education Employees. Qual Higher Educ, 15, 207-219.
Enthoven, P., Skargren, E., Carstensen, J., & Oberg, B. (2006). Predictive
factors for 1-year and 5-year outcome for disability in a working

107
population of patients with low back pain treatedin primary care. Journal of pain.
Eriksen, H., Ihlebæk, C., Mikkelsen, A., Grønningsæter, H., Sandal, G., & Ursin,
H. (2002). Improving subjective health at the worksite: a randomized controlled trial of stress management training, physical exercise and an integrated health programme. Occup Med, 52.
Essendrop, M., Maul, I., Läubli, T., Riihimäki, H., & Schibye, B. (2002).
Measures of low back function: a review of reproducibility studies. Clin Biomech (Bristol, Avon), 17(4), 235-249. doi: S0268003302000220 [pii]
Fathallah, F. A., Marras, W. S., & Parnianpour, M. (1997). The effect of complex
dynamic lifting and lowering characteristics on trunkmuscles recruitment. J Occup Rehabil, 7, 121–138.
Ferreira, P. L. (2000a). [Development of the Portuguese version of MOS SF-36.
Part I. Cultural and linguistic adaptation]. Acta Med Port, 13(1-2), 55-66. Ferreira, P. L. (2000b). [Development of the Portuguese version of MOS SF-36.
Part II --Validation tests]. Acta Med Port, 13(3), 119-127. Feyer, A. M., Herbison, P., Williamson, A. M., de Silva, I., Mandryk, J., Hendrie,
L., & Hely, M. C. (2000). The role of physical and psychological factors in occupational low back pain: a prospective cohort study. Occup Environ Med, 57(2), 116-120.
Friedrich, M., Gittler, G., Arendasy, M., & Friedrich, K. M. (2005). Long-term
effect of a combined exercise and motivational program on the level of disability of patients with chronic low back pain. Spine (Phila Pa 1976), 30(9), 995-1000. doi: 00007632-200505010-00002 [pii]
Friedrich, M., Karnzl, A., Heller, I., Kirtley, C., & Cermak, T. (2000). Spinal
posture during stooped walking under vertical space constraints. Spine, 25, 1118–1125.
Fritz, J. M., Erhard, R. E., & Hagen, B. F. (1998). Segmental Instability of the
Lumbar Spine. Phys Ther, 78, 889-896. Gagnon, M., & Smyth, G. (1992). Biomechanical exploration on dynamic-modes
of lifting. Ergonomics, 35, 329–345. Galukande, M., Muwazi, S., & Mugi, D. B. (2005, Afr Health Sci. 2005 June;
5(2): 164–167.). Aetiology of low back pain in Mulago Hospital, Uganda. Afr Health Sci, 5, 164-167.
Gerr, F., Marcus, M., Monteilh, C., Hannan, L., Ortiz, D., & Kleinbaum, D.
(2005). A randomised controlled trial of postural interventions for prevention of musculoskeletal symptoms among computer users.

108
OccupEnviron Med, 62(7), 478-487. doi: 62/7/478 [pii]10.1136/oem.2004.015792
Giaccone, M. (2007). Annual review of working conditions in the EU 2006-2007
European Foundation for the Improvement of Living and Working Conditions. Luxembourg: Office for Official Publications of the European Communities.
Goldby, L. J., Moore, A. P., Doust, J., & Trew, M. E. (2006). A randomized
controlled trial investigating the efficiency of musculoskeletal physiotherapy on chronic low back disorder. Spine, 31, 1083–1093.
Goldsheyder, D., Nordin, M., Weiner, S. S., & Hiebert, R. (2002).
Musculoskeletal symptom survey among mason tenders. Am J Ind Med, 42, 384-396.
Gonçalves, M., & Barbosa, F. (2005). Análise de parâmetros de força e
resistência dos músculos erectores da espinha lombar durante a realização de exercício isométrico em diferentes níveis de esforço. Rev Bras Med Esporte, 11.
Gundewall, B., Liljeqvist, M., & Hansson, T. (1993). Primary prevention of back
symptoms and absence from work. A prospective randomized study among hospital employees. Spine (Phila Pa 1976), 18(5), 587-594.
Guo,H. R. (2002). Working hours spent on repeated activities and prevalence of
low back pain. Occup Environ Med, 59, 680-688. Harkness, E. F., Macfarlane, G. J., Nahit, E. S., Silman, A. J., & McBeth, J.
(2003). Risk factors for new-onset low back pain amongst cohorts of newly employed workers. Rheumatology (Oxford), 42(8), 959-968. doi: 10.1093/rheumatology/keg265keg265 [pii]
Harrington, J. M. (1994). Improving the Health of People at Work. Ann. Occup.
Hyg., 38(6), 811-813. Hemingway, H., Stafforf, M., Stansfeld, S., Shipley, M., & Marmot, M. (1997). Is
the SF-36 a valid measure of change in population health? Results from the Whitehall II study. BMJ, 315, 1273-1279.
Hicks, G. E., Fritz, J. M., Delitto, A., & McGill, S. M. (2005). Preliminary
Development of a Clinical Prediction Rule for Determining Which Patients With Low Back Pain Will Respond to a Stabilization Exercise Program. Arch Phys Med Rehabil, 86, 1753-1762.
Hildebrandt, A. L., & Neufer, P. D. (2000). Exercise attenuates the fasting-
induced transcriptional activation of metabolic genes in skeletal muscle. Am J Physiol Endocrinol Metab, 278(6), E1078-1086.

109
Hilfiker, R., Bachmann, L. M., Heitz, C. A., Lorenz, T., Joronen, H., & Klipstein, A. (2007). Value of predictive instruments to determine persisting restriction of function in patients with subacute non-specific low back pain. Systematic review. Eur Spine J.
Hlobil, H., Staal, J. B., Twisk, J., Koke, A., Ariens, G., Smid, T., & van
Mechelen, W. (2005). The effects of a graded activity intervention for low back pain in occupational health on sick leave, functional status and pain: 12-month results of a randomized controlled trial. J Occup Rehabil, 15(4), 569-580. doi: 10.1007/s10926-005-8035-y
Hodges, P. W. (1999). Is there a role for transversus abdominis in lumbo-pelvic
stability? Man Ther, 4(2), 74-86. doi: S1356-689X(99)90169-8 [pii] 10.1054/math.1999.0169
Hodges, P. W., & Richardson, C. A. (1998). Delayed postural contraction of
transversus abdominis in low back pain associated with movement of the lower limb. J Spinal Disord, 11(1), 46-56.
Holmstrom, E., & Ahlborg, B. (2005). Morning warming-up exercise--effects on
musculoskeletal fitness in construction workers. Appl Ergon, 36(4), 513-519. doi: S0003-6870(05)00013-X [pii]10.1016/j.apergo.2004.10.015
Hoogendoorn, W. E., Bongers, P. M., Vet, H. C., Ariëns, G. A., Mechelen, W., &
Bouter, L. M. (2002). High physical work load and low job satisfaction increase the risk of sickness absence due to low back pain: results of a prospective cohort study. Occup Environ Med, 59, 323-323.
Hussain, T. (2004, April 26). Musculoskeletal symptoms among truck assembly
workers. Occupational Medicine, 54 (8), 506-512. Häkkänen, M., Viikari-Juntura, E., & Martikainen, R. (2001). Job experience,
work load, and risk of musculoskeletal disorders. Occup Environ Med, 58, 129-135.
IJzelenberg, H., Meerding, W. J., & Burdorf, A. (2007). Effectiveness of a back
pain prevention program: a cluster randomized controlled trial in an occupational setting. Spine, 32, 711-719.
IJzelenberg, W., & Burdorf, A. (2004). Impact of musculoskeletal co-morbidity of
neck and upper extremities on healthcare utilisation and sickness absence for low back pain. Occup Environ Med, 61, 806-810.
Imamura, S. T., Kaziyama, H. D., & Imamura, M. (2001). Lombalgia. Dor
músculo-esquelética (pp. 375-390). S.Paulo: Ed Revista Brasileira de Medicina.
Ismaeil, E., Hosseini, G., Salavati, M., Farahini, H., & Arab, A. (2005). Clinical
Trunk Muscle Endurance Tests in Subjects with and without Low Back Pain. Med J Isl Rep Iran, 19, 95-101.

110
Jansen, J. P., Morgenstern, H., & Burdorf, A. (2004). Dose-response relations between occupational exposures to physical and psychosocial factors and the risk of low back pain. . Occup Environ Med, 61, 972-979.
Johannsen, F., Remvig, L., Kryger, P., Beck, P., Warming, S., Lybeck, K., . . .
Larsen, L. H. (1995). Exercises for chronic low back pain: a clinical trial. J Orthop Sports Phys Ther, 22(2), 52-59.
Juul-Kristensen, B., & Jensen, C. (2005). Self-reported workplace related
ergonomic conditions as prognostic factors for musculoskeletal symptoms: the "BIT" follow up study on office workers. Occupational and Environmental Medicine, 62, 188-194.
Kasai, R. (2006). Current Trends in Exercise Management for Chronic Low
Back Pain: Comparison between Strengthening Exercise and Spinal Segmental Stabilization exercise. Journal of Physical Therapy Science, 18, 97-105.
Kaser, L., Mannion, A. F., Rhyner, A., Weber, E., Dvorak, J., & Muntener, M.
(2001). Active therapy for chronic low back pain: part 2. Effects on paraspinal muscle cross-sectional area, fiber type size, and distribution. Spine (Phila Pa 1976), 26(8), 909-919.
Kent, P. M., & Keating, J. L. (2005). The epidemiology of low back pain in
primary care. Chiropr Osteopat, 13, 13. doi: 1746-1340-13-13 [pii] 10.1186/1746-1340-13-13
Keyserling, W. M., Sudarsan, S. P., Martin, B. J., Haig, A. J., & Armstrong, T. J. (2005). Effects of low back disability status on lower back discomfort during sustained and cyclical trunk flexion. Ergonomics, 48(3), 219-233. doi: GRFTNCY8H53NQRER [pii]10.1080/0014013042000327689
Klussmann, A., Gebhardt, H., Liebers, F., & Rieger, M. (2008). Musculoskeletal
symptoms of the upper extremities and the neck: a cross-sectional study on prevalence and symptom-predicting factors at visual display terminal (VDT) workstations. BMC Musculoskeletal Disorders, 9.
Koumantakis, G. A., Watson, P. J., & Oldham, J. A. (2005). Supplementation of
general endurance exercise with stabilisation training versus general exercise only Physiological and functional outcomes of a randomised controlled trial of patients with recurrent low back pain. Clin Biomechanics, 20, 474-482.
Krajcarski, S. R., Potvin, J. R., & Chiang, J. (1999). The in vivo dynamic
response of the spine to perturbations causing rapid flexion: effects of pre-load and step input magnitude. Clin Biomech (Bristol, Avon), 14(1), 54-62. doi: S0268003398000485 [pii]

111
Kuorinka, I., Alaranta, H., & Erich, I. (1995). Prevention of musculoskeletal disorders at work: Validation and reliability in a multicenter intervention study. International Journal of Industrial Ergonomics, 15, 437-446.
Kuorinka, I., Jonsson, B., Kilbom, A., Vinterberg, H., Biering-Sorensen, F.,
Andersson, G., & Jorgensen, K. (1987). Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon, 18(3), 233-237. doi: 000368708790010X [pii]
Kuorinka, I., & Patry, L. (1995). Participation as a means of promoting
occupational health. International Journal of Industrial Ergonomics, 15, 365-370.
Kuukkanen, T., & Malkia, E. (2000). Effects of a three-month therapeutic
exercise programme on flexibility in subjects with low back pain. Physiother Res Int, 5(1), 46-61.
Lamers, L., Meerding, W., Severens, J., & Brouwer, W. (2005). The relationship
between productivity and health-related quality of life: An empirical exploration in persons with low back pain. Qua Life Res, 14, 805–813.
Lang, E., Liebig, K., Kastner, S., Neundörfer, B., & Heuschmann, P. (2003).
Multidisciplinary rehabilitation versus usual care for chronic low back pain in the community: effects on quality of life. Spine J, 4, 270-276.
Lee,J. H., Hoshino, Y., Nakamura, K., Kariya, Y., Saita, K., & Ito, K. (1999).
Trunk muscle weakness as a risk factor for low back pain. A 5-year prospective study. Spine (Phila Pa 1976), 24(1), 54-57.
Loisel, P. (2005). Prevention of Work Disability Due to Musculoskeletal
Disorders: The Challenge of Implementing Evidence. J Occu Rehab, 4, 507-524.
Lotters, F., Franche, R., Hogg-Johnson, S., Burdorf, & Pole, J. (2006). The
prognostic value of depressive symptoms, fear avoidance, and self-efficacy for duration of lost-time benefits in workers with musculoskeletal disorders. Occup Environ Med, 63, 794-801.
MacDermid, J. C., Walton, D. M., & Law, M. (2009). Critical appraisal of
research evidence for its validity and usefulness. Hand Clin, 25(1), 29-42, v. doi: S0749-0712(08)00103-0 [pii]10.1016/j.hcl.2008.11.003
Maher, C. G. (2000). A systematic review of workplace interventions to prevent
low back pain. Aust J Physiother, 46(4), 259-269. Maher, C. G., Latimer, J., Hodges, P. W., Refshauge, K. M., Moseley, G. L.,
Herbert, R. D., . . . McAuley, J. (2005). The effect of motor control exercise versus placebo in patients with chronic low back pain

112
[ACTRN012605000262606]. BMC Musculoskelet Disord, 6, 54. doi: 1471-2474-6-54 [pii]10.1186/1471-2474-6-54
Mannion, A. F., Taimela, S., Müntener, M., & Dvorak, J. (2001). Active Therapy
for Chronic Low Back Pain. Part 1. Effects on Back Muscle Activation, Fatigability, and Strength. Spine, 26, 897-908.
Marras, W. S., Granta, K. P., & Davis, K. G. (1999). Variability in spine loading
model performance. Clin Biomech (Bristol, Avon), 14(8), 505-514. doi: S0268-0033(98)90090-0 [pii]
Marras, W. S., Lavende, S. A., Fergunson, S. A., Splittstoesser, R. E., & Yang,
G. (2010). Quantitative biomechanical workplace exposure measures: Distribution centers. J Elect Kinesiology 20, 813–822.
Marras, W. S., Lavender, S. A., Ferguson, S. A., Splittstoesser, R. E., & Yang,
G. (2010). Quantitative dynamic measures of physical exposure predict low back functional impairment. Spine (Phila Pa 1976), 35(8), 914-923. doi: 10.1097/BRS.0b013e3181ce1201
May, S. (2010). Self-management of chronic low back pain and osteoarthritis.
Nat Rev Rheumatol, 6(4), 199-209. doi: nrrheum.2010.26 [pii] 10.1038/nrrheum.2010.26
May, S., & Rosedale, R. (2009). Prescriptive Clinical Prediction Rules in Back Pain Research: A Systematic Review. J Man Manip Ther, 17, 36–45.
McClelland, L., & McCubbin, J. (2008). Social influence and pain response in
women and men. J Behav Med, 31, 413-420. McGill, S., Sharratt, M. T., & Seguin, L. P. (1995). Loads on spinal tissues
during simultaneous lifting and ventilatory challenge. Ergon, 38, 1772–1792.
McGill, S. M., Childs, A., & Liebenson, C. (1999). Endurance times for low back
stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil, 80(8), 941-944. doi: S0003-9993(99)90087-4 [pii]
McGill, S. M., Sharratt, M. T., & Seguin, J. P. (1995). Loads on spinal tissues
during simultaneous lifting and ventilatory challenge. Ergonomics, 38(9), 1772-1792. doi: 10.1080/00140139508925226
Medical Outcomes Trust introduces new translation criteria. ( 1997). Medical
Outcomes Trust Bulletin, 5(4), 2-4. Meerdinga, W. J., IJzelenberga, W., Koopmanschapb, M. A., Severensc, J. L.,
& Burdorfa, A. (2005). Health problems lead to considerable productivity loss at work among workers with high physical load jobs. J Clin Epidemiology, 58, 517–523.

113
Meijsen, P., & Knibbe, H. J. (2007). Work-related musculoskeletal disorders of perioperative personnel in the Netherlands. AORN J, 86(2), 193-208. doi: S0001-2092(07)00457-7 [pii]10.1016/j.aorn.2007.07.011
Merkesdal, S., & Mau, W. (2005). Prediction of costs-of-illness in patients with
low back pain undergoing orthopedic outpatient rehabilitation. Int J Rehabil Res, 28(2), 119-126. doi: 00004356-200506000-00004 [pii]
Mesquita, C. C., Ribeiro, J. C., & Moreira, P. (2010). Portuguese version of the
standardized Nordic musculoskeletal questionnaire: cross cultural and reliability. J Public Health, 18(5), 461–466. doi: 10.1007/s10389-010-0331-0
Moffett, J. K., Torgerson, D., Bell-Syer, S., Jackson, D., Llewlyn-Phillips, H.,
Farrin, A., & Barber, J. (1999). Randomised controlled trial of exercise for low back pain: clinical outcomes, costs, and preferences. BMJ, 319(7205), 279-283.
Moffroid, M. T. (1997). Endurance of trunk muscles in persons with chronic low
back pain: Assessment, performance, training. Journal of Rehabilitation Research and Development, 440-447.
Morken, T., Riise, T., Moen, B., Hauge, S. H., Holien, S., Langedrag, A., . . .
Thoppil, V. (2003). Low back pain and widespread pain predict sickness absence among industrial workers. BMC Musculoskelet Disord, 4, 21. doi: 10.1186/1471-2474-4-211471-2474-4-21 [pii]
Moseley, L. (2002). Combined physiotherapy and education is efficacious for
chronic low back pain. Aust J Physiother, 48(4), 297-302. Moses, A. S., Heestand, D. E., Doyle, L. L., & O'Sullivan, P. S. (2006). Impact of
a teaching scholars program. Acad Med, 81(10 Suppl), S87-90. doi: 10.1097/01.ACM.0000236538.29378.e900001888-200610001-00022[pii]
Mostardi, R. A., Noe, D. A., Kovacik, M. W., & Porterfield, J. A. (1992).
Isokinetic lifting strength and occupational injury. A prospective study. Spine (Phila Pa 1976), 17(2), 189-193.
Nahit, E., Hunt, I., Lunt, M., Dunn, G., Silman, A., & Macfarlane, G. (2003).
Effects of psychosocial and individual psychological factors on the onset of musculoskeletal pain: common and site-specific effects. Ann Rheum Dis, 62, 755 – 760.
Ng, J. K., Richardson, C. A., Kippers, V., & Parnianpour, M. (1998).
Relationship between muscle fiber composition and functional capacity of back muscles in healthy subjects and patients with back pain. J Orthop Sports Phys Ther, 27(6), 389-402.

114
NORA,M. D. T. (2001). Research Topics for the Next Decade. Columbia,Cincinnati: National Institute for Occupational Safety and Health.
Norris, C. M. (1995). Stabilization Mechanisms of the Lumbar Spine. Physiotherapy, 81(2), 72-79.
Nourbakhsh, M. R., & Arab, A. M. (2002). Relationship between mechanical
factors and incidence of low back pain. J Orthop Sports Phys Ther, 32(9), 447-460.
O'Sullivan, P. (2000). Lumbar segmental "instability": clinical presentation and
specific stabilizing exercise management. Manual Therapy, 5(1), 2-12. O'Sullivan, P., Dankaerts, W., Burnett, A., Straker, L., Bargon, G., Moloney, N., .
. . Tsang, S. (2006). Lumbopelvic kinematics and trunk muscle activity during sitting on stable and unstable surfaces. J Orthop Sports Phys Ther, 36(1), 19-25.
O'Sullivan, P. B., Mitchell, T., Bulich, P., Waller, R., & Holte, J. (2006). The
relationship beween posture and back muscle endurance in industrial workers with flexion-related low back pain. Man Ther, 11(4), 264-271. doi: S1356-689X(05)00043-3 [pii]10.1016/j.math.2005.04.004
Palmer, K., Smith, G., Kellingray, S., & Cooper, C. (1999). Repeatability and
validity of an upper limb and neck discomfort questionnaire: the utility of the standardized Nordic questionnaire. Occup Med (Lond), 49(3), 171-175.
Peate, W. F., Bates, G., Lunda, K., Francis, S., & Bellamy, K. (2007). Core
strength: a new model for injury prediction and prevention. J Occup Med Toxicol, 2, 3. doi: 1745-6673-2-3 [pii]10.1186/1745-6673-2-3
Peltonen, J. E., Taimela, S., Erkintalo, M., Salminen, J. J., Oksanen, A., &
Kujala, U. M. (1998). Back extensor and psoas muscle cross-sectional area, prior physical training, and trunk muscle strength--a longitudinal study in adolescent girls. Eur J Appl Physiol Occup Physiol, 77(1-2), 66-71.
Pengel, L. H., Herbert, R. D., Maher, C. G., & Refshauge. (2003). Acute low
back pain: systematic review of its prognosis. BMJ, 327, 327-323. Piedrahíta, H., Punnett, L., & Shahnavaz, H. (2004, Junho 15). Musculoskeletal
symptoms in cold exposed and non-cold exposed workers. International Journal of Industrial Ergonomics, 34, 271-278.
Pope,M. H., Goh, K. L., & Magnusson, M. L. (2002). Spine Ergonomics. Annu
Rev Biomed Eng, 4, 49–68. Porter, J. M., & Gyi, D. E. (2002). The prevalence of musculoskeletal troubles
among car drivers. Occup Med (Lond), 52(1), 4-12.

115
Potvin, J. R., & O’Brien, P. R. (1998). Trunk muscle co-contraction increases during fatiguing, isometric, lateral bend exertions—possible implications for spine stability. Spine, 23, 774–780.
Punnett, L., & Wegman, D. H. (2004). Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol, 14(1), 13-23. doi: 10.1016/j.jelekin.2003.09.015S1050641103001251 [pii]
Pynsent, P. B. (2001). Choosing an outcome measure. J Bone Joint Surg Br,
83(6), 792-794. Quinn, E. (2003). The Proper Use of Belts During Weight Training. Sports Med,
72-78. Rainville, J., Hartigan, C., Jouve, C., & Martinez, E. (2004). The influence of
intense exercise-based physical therapy program on back pain anticipated before and induced by physical activities. Spine J, 4(2), 176-183. doi: 10.1016/j.spinee.2003.08.031S1529943003005072 [pii]
Rainville, J., Hartigan, C., Martinez, E., Limke, J., Jouve, C., & Finno, M. (2004).
Exercise as a treatment for chronic low back pain. Spine J, 4(1), 106-115. doi: S1529943003001748 [pii]
Rantanen, P., Airaksinen, O., & Penttinen, E. (1994). Paradoxical variation of
strength determinants with different rotation axes in trunk flexion and extension strength tests. Eur J Appl Physiol Occup Physiol, 68(4), 322-326.
Richardson, C., Jull, G., Toppenberg, R., & Comerford, M. (1992). Techniques for active lumbar stabilisation for spinal protection: A pilot study. Aust J Phys, 38(2), 105-112.
Rissanen, A., Heliovaara, M., Alaranta, H., Taimela, S., Malkia, E., Knekt, P., . .
. Aromaa, A. (2002). Does good trunk extensor performance protect against back-related work disability? J Rehabil Med, 34(2), 62-66.
Roffey, D. M., Wai, E. K., Bishop, P., Kwon, B. K., & Dagenais, S. (2010).
Causal assessment of occupational pushing or pulling and low back pain: results of a systematic review. Spine J, 10(6), 544-553. doi: S1529-9430(10)00217-2 [pii]10.1016/j.spinee.2010.03.025
Roussel, N., Nijs, J., Truijen, S., Breugelmans, S., Claes, I., & Stassijns, G.
(2006). Reliability of the assessment of lumbar range of motion and maximal isometric strength. Arch Phys Med Rehabil, 87(4), 576-582. doi: S0003-9993(06)00045-1 [pii]10.1016/j.apmr.2006.01.007
Rulgulies, R., & Krause, N. (2005). Job strain, isso-strain, and the incidence of
low back and neck injuries. A 7,5-year prospective study of San Francisco transit operators. Social Science & Medicine, 61, 27-39.
Salinas, A. M., Villarreal, E., Nuñez GM, G. M., Garza, M. E., Briones, H., &
Navarro, O. (2002). Health interventions for the metal working industry:

116
which is the most cost-effective? A study from a developing country. Occup Med, 52, 129-135.
Santos, A. C., Bredemeier, M., Rosa, K. F., Amantea, V. A., & Xavier, R. M.
(2011). Impact on the Quality of Life of an Educational Program for the Prevention of Work-Related Musculoskeletal Disorders: a randomized controlled trial. BMC Public Health, 11, 60. doi: 1471-2458-11-60 [pii] 10.1186/1471-2458-11-60
Sculco, A. D., Paup, D. C., Fernhall, B., & Sculco, M. J. (2001, March). Effects of aerobic exercise on low back pain patients in treatment. The Spine Journal, 1 (2), 95-101.
Sherman, K. J., Cherkin, D. C., Erro, J., Miglioretti, D. L., & Deyo, R. A. (2005).
Comparing yoga, exercise, and a self-care book for chronic low back pain:a randomized, controlled trial. Ann Intern Med, 142, 849–856.
Shimizu, T., Horie, S., Nagata, S., & Marui, E. (2004). Relationship between self-reported low productivity and overtime working. . Occup Med, 54, 52-54.
Stevens, V. K., Bouche, K. G., Mahieu, N. N., Coorevits, P. L., Vanderstraeten,
G. G., & Danneels, L. A. (2006). Trunk muscle activity in healthy subjects during bridging stabilization exercises. BMC Musculoskelet Disord, 7, 75. doi: 1471-2474-7-75 [pii]10.1186/1471-2474-7-75
Sung,P. (2003). Multifidi Muscles Median Frequency Before and After Spinal
Stabilization Exercises. Arch Phys Med Rehabil, 84. Szabo,R. M. (2001). Musculoskeletal Disorders and the Workplace: Low Back
and Upper Extremities. Washington DC: National Academy Press. Tavafian, S., Jamshidi, A., Mohammad, K., & Montazeri, A. (2007). Low back
pain education and short term quality of life: a randomized trial. BMC Musculoskeletal Disorders, 8.
Trainor, T. J., & Wiesel, S. W. (2002). Epidemiology of Back Pain in the Athlete.
Clin Sports Med, 21, 93-103. Tuncel, S., Iossifova, Y., Ravelo, E., Daraiseha, N., Salem, S. (2006).
Effectiveness of controlled workplace interventions in reducing lower back disorders. Theoretical Issues in Ergonomics Science, 7(3), 191-209. doi: 10.1080/14639220500090505
Tuomi,K., Vanhala, S., Nykyri, E., & Janhonen, M. (2004). Organizational
practices, work demands and the well-being of employees: a follow-up study in the metal industry and retail trade. Occup Med, 54, 115-121.
Tuzun,E. H. (2007). Quality of life in chronic musculoskeletal pain. Best Pract
Res Clin Rheumatol, 21(3), 567-579. doi: S1521-6942(07)00035-6 [pii] 10.1016/j.berh.2007.03.001

117
Tveito, T. H., & Eriksen, H. R. (2009). Integrated health programme: a workplace randomized controlled trial. J Adv Nurs, 65(1), 110-119. doi: JAN4846 [pii]10.1111/j.1365-2648.2008.04846.x
Tveito, T. H., Hysing, M., & Eriksen, H. R. (2004). Low back pain interventions
at the workplace: a systematic literature review. Occup Med (Lond), 54(1), 3-13.
Udermann, B. E., Mayer, J. M., Graves, J. E., & Murray, S. R. (2003).
Quantitative Assessment of Lumbar Paraspinal Muscle Endurance. J Athl Train, 38(3), 259-262.
Urquhart, D. M., Bell, R. J., Cicuttini, F. M., Cui, J., Forbes, A., & Davis SR, S.
R. (2008). Negative beliefs about low back pain are associated with high pain intensity and high level disability in community-based women. BMC Musculoskeletal Disorders, 9.
van Nieuwenhuyse, A., Somville, P. R., Crombez, G., Burdorf, A., Verbeke, G.,
Johannik, K., . . . Moens, G. F. (2006). The role of physical workload and pain related fear in the development of low back pain in young workers: evidence from the BelCoBack Study; results after one year of follow up. Occup Environ Med, 63(1), 45-52. doi: 63/1/45 [pii]10.1136/oem.2004.015693
van Oostrom, S. H., Driessen, M. T., de Vet, H. C., Franche, R. L., Schonstein,
E., Loisel, P., . . . Anema, J. R. (2009). Workplace interventions for preventing work disability. Cochrane Database Syst Rev(2), CD006955. doi: 10.1002/14651858.CD006955.pub2
van Poppel, M. N., Hooftman, W. E., & Koes, B. W. (2004). An update of a
systematic review of controlled clinical trials on the primary prevention of back pain at the workplace. Occup Med, 54, 345–352.
van Tulder, M., Malmivaara, A., & Koes, B. (2007). Repetitive strain injury.
Lancet, 369, 1815-1822. Vital,E., Melo, M. J., Nascimento, A. I., & Roque, A. L. (2007). A Força Muscular
do Tronco e as Queixas de Raquialgias no Início da Adolescência. Rev Port Fisiot Desp, 1, 4-11.
Vlaeyen, J. W., Kole-Snijders, A. M., Boeren, R. G., & van Eek, H. (1995). Fear
of movement ( re) injury in chronic low back pain and its relation to behavioral performance. Pain, 62, 363-372.
Waddell, G., & Burton, A. K. (2001). Occupational health guidelines for the
management of low back pain at work: evidence review. Occup Med (Lond), 51(2), 124-135.

118
Wai, E. K., Roffey, D. M., Bishop, P., Kwon, B. K., & Dagenais, S. (2010). Causal assessment of occupational bending or twisting and low back pain: results of a systematic review. Spine J, 10(1), 76-88. doi: S1529-9430(09)00273-3 [pii]10.1016/j.spinee.2009.06.005
Walsh, D. A., & Radcliffe, J. C. (2002). Pain beliefs and perceived physical
disability of patients with chronic low back pain. Pain, 97, 23-31. Ware, J. E., & Sherbourne, C. D. (1992). The MOS, 36-Item Short-Form Health
Survey (SF-36): I. Conceptual framework and item selection. Med Care, 30, 473-483.
WHO. (1985). Identification and control ofwork-related diseases. Geneva,
Switzerland: WHO Technical. Yang, G., Marras, W. S., & Best, T. M. (2011). The biochemical response to
biomechanical tissue loading on the low back during physical work exposure. Clin Biomech (Bristol, Avon), 26(5), 431-437. doi: S0268-0033(11)00020-9 [pii]10.1016/j.clinbiomech.2011.01.005


Anexos

Anexo I

XXI
Questionário de Saúde Geral
1. Tem alguma anormalidade anatómica? □Sim □ Não
� Se respondeu sim, diga qual: _______________________________
2. Pratica algum desporto? □Sim □ Não
� Se respondeu sim diga qual a periodicidade: ____________________
3. Possui alguma lesão ou doença crónica do foro neuro-musculo-esquelético? □Sim □
4. Toma alguma medicação específica? □ Sim □ Não
� Se respondeu sim, especifique: _______________________________
5. Realizou alguma cirurgia à zona abdominal ou lombo-pélvica ou devido a dor lombar?
□Sim □ Não
6. Realizou algum tratamento à coluna lombar no último ano? □Sim □ Não
7. Tem história de dor a nível da coluna lombar? □Sim □ Não
8. Neste momento, sente dor a nível da coluna lombar? □ Sim □ Não
� Se respondeu sim, indique com um X qual a sua severidade, tendo em conta que 0
corresponde a “ausência de dor” e 10 a “dor máxima imaginável”.
0 1 2 3 4 5 6 7 8 9 10
Nome: ________________________________________________ Nº Código: _______
Idade: _______ Sexo: □ Masculino □ Feminino
Preencha o questionário com sinceridade,assinale com uma cruz a hipótese mais adequada.
No caso de surgir alguma dúvida no preenchimento do questionário não hesite em esclarecer
com um dos nossoscolaboradores!!!
A informação fornecida jamais servirá para outros fins que nãoesta investigação.

XXII
9. Possui algumadoença a nível do Sistema Respiratório?□ Sim □ Não
� Se respondeu sim, diga qual: _______________________________
10. Possui algumadoença a nível do Sistema Cardiovascular?□ Sim □ Não
� Se respondeu sim, diga qual: _______________________________
11. Possui algumadoença a nível do Sistema Endócrino ou Renal?□ Sim □ Não
� Se respondeu sim, diga qual: _______________________________

XXIII
Anexo 2

Questionário Nórdico Músculo-esquelético
XXIV
Instruções para o preenchimento
• Por favor, responda a cada questão assinalando um “X” na caixa apropriada: �
• Marque apenas um “X” por cada questão.
• Não deixe nenhuma questão em branco, mesmo se não tiver nenhum problema em
qualquer parte do corpo.
• Para responder, considere as regiões do corpo conforme ilustra a figura abaixo.

Questionário Nórdico Músculo-esquelético
XXV
Idade_____Data de nascimento____/___/___Sexo_______ __Data de hoje____/____/_____
Posto de trabalho_________________________________E stado civil__________________
Nome_______________________________________________________________________
Considerando os últimos 12 meses , teve algum problema (tal como dor, desconforto ou dormência ) nas seguintes regiões:
Responda, apenas, se tiver algum problema
Durante os últimos 12 meses teve que evitar as suas actividades normais (trabalho, serviço doméstico ou passatempos) por causa de problemas nas seguintes regiões:
Teve algum problema nos últimos 7 dias, nas seguintes regiões:
1. Pescoço? Não Sim
1 � 2 �
2. Pescoço?
Não Sim
1 � 2 �
3. Pescoço?
Não Sim
1 � 2 �
4.
5. Ombros?
Não Sim
1 � 2 � , no ombro direito
3 � , no ombro
esquerdo
4 � , em ambos
6. Ombros?
Não Sim
1 � 2 � , no ombro direito
3 � , no ombro
esquerdo
4 � , em ambos
7. Ombros?
Não Sim
1 � 2 � , no ombro direito
3 � , no ombro
esquerdo
4 � , em ambos
8.
9. Cotovelo?
Não Sim
1 � 2 � , no cotovelo direito
3� , no cotovelo
10. Cotovelo?
Não Sim
1 � 2 � , no cotovelo direito
3� , no cotovelo
11. Cotovelo?
Não Sim
1� 2� , no cotovelo direito
3� , no cotovelo
12.
Código:

Questionário Nórdico Músculo-esquelético
XXVI
esquerdo
4� , em ambos
esquerdo
4� , em ambos
esquerdo
4� , em ambos
13. Punho/Mãos?
Não Sim
1� 2� , no punho/mãos direitos
3� , no punho/mãos esquerdos
4� , em ambos
14. Punho/Mãos?
Não Sim
1� 2� , no punho/mãos direitos
3� , no punho/mãos esquerdos
4� , em ambos
15. Punho/Mãos?
Não Sim
1� 2� , no punho/mãos direitos
3� , no punho/mãos esquerdos
4� , em ambos
16.
17. Região Torácica?
Não Sim
1 � 2 �
18. Região Torácica?
Não Sim
1 � 2 �
19. Região Torácica?
Não Sim
1 � 2 �
20.
21. Região Lombar?
Não Sim
1 � 2 �
22. Região Lombar?
Não Sim
1 � 2 �
23. Região Lombar?
Não Sim
1 � 2 �
24.
25. Ancas/Coxas?
Não Sim
1 � 2 �
26. Ancas/Coxas?
Não Sim
1 � 2 �
27. Ancas/Coxas?
Não Sim
1 � 2 �
28.
29. Joelhos?
Não Sim
1 � 2 �
30. Joelhos?
Não Sim
1 � 2 �
31. Joelhos?
Não Sim
1 � 2 �
32.
33. Tornozelo/Pés?
Não Sim
1 � 2 �
34. Tornozelo/Pés?
Não Sim
1 � 2 �
35. Tornozelo/Pés?
Não Sim
1 � 2 �
36.

XXVII

XXVIII

XXIX

XXX

XXXI