CESM completa - bbcs.net.br€¦ · Protocolo de desenvolvimento de mamografia com contraste (CESM)...
34
30/05/2016 1 Mamografia 3.0 porque precisamos tanto? Guilherme Rossi Nova Medicina Diagnóstica Cláudio Rossi Cristina R. Longo Guilherme Rossi Paula Soriano CONFLITO DE INTERESSE Protocolo de desenvolvimento de mamografia com contraste (CESM) com apoio GE. Site visiting GE na modalidade. Agradecimentos Faculdade de Medicina de Jundiai Dr. João Bosco Dra. Janaina FMFUABC Dr. Ivo Carelli Dr Paulo Pirozzi Dr. Ricardo Mazzei Dra Izabella Mendes
-
Upload
nguyenngoc -
Category
Documents
-
view
213 -
download
0
Transcript of CESM completa - bbcs.net.br€¦ · Protocolo de desenvolvimento de mamografia com contraste (CESM)...

30/05/2016
1
Mamografia 3.0
porque precisamos tanto?
Guilherme Rossi
Nova Medicina Diagnóstica
Cláudio Rossi Cristina R. Longo Guilherme Rossi Paula Soriano
CONFLITO DE INTERESSE❖ Protocolo de desenvolvimento de mamografia com
contraste (CESM) com apoio GE.❖ Site visiting GE na modalidade.
Agradecimentos
� Faculdade de Medicina de Jundiai❖ Dr. João Bosco❖ Dra. Janaina❖ FMFUABC❖ Dr. Ivo Carelli❖ Dr Paulo Pirozzi❖ Dr. Ricardo Mazzei❖ Dra Izabella Mendes
30/05/2016
2
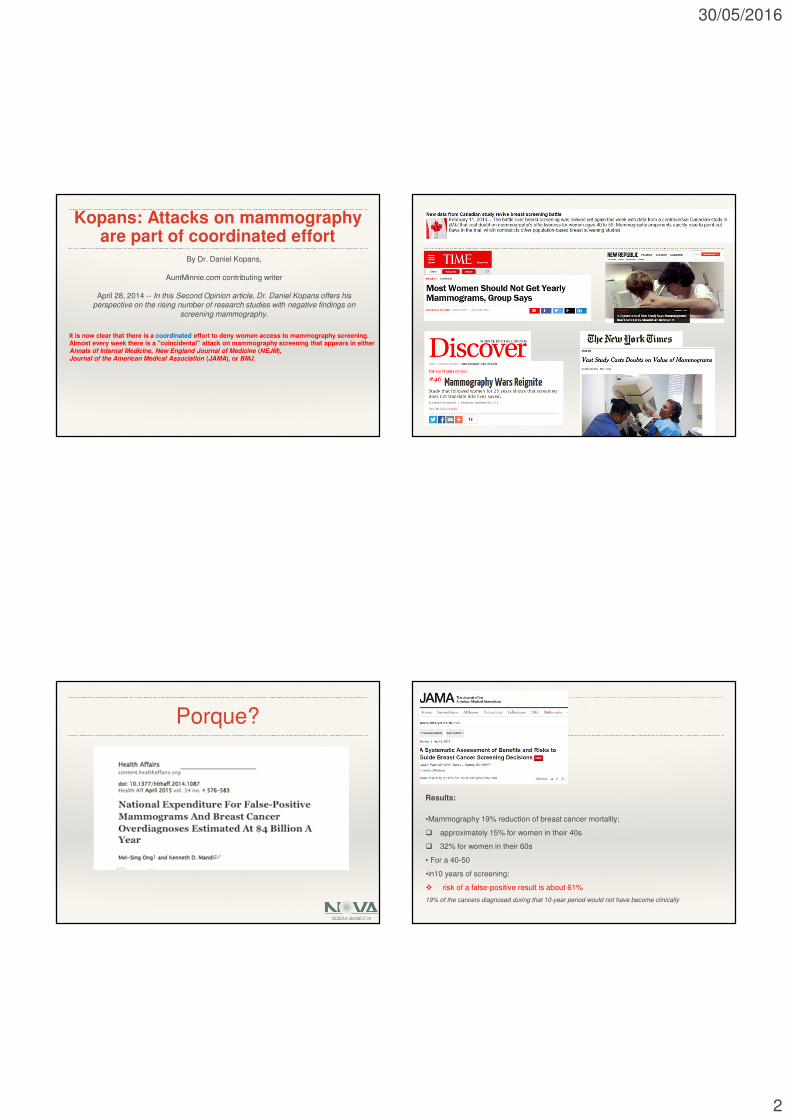
Kopans: Attacks on mammography are part of coordinated effort
By Dr. Daniel Kopans,
AuntMinnie.com contributing writer
April 28, 2014 -- In this Second Opinion article, Dr. Daniel Kopans offers his perspective on the rising number of research studies with negative findings on
screening mammography.
It is now clear that there is a coordinated effort to deny women access to mammography screening. Almost every week there is a "coincidental" attack on mammography screening that appears in either Annals of Internal Medicine, New England Journal of Medicine (NEJM), Journal of the American Medical Association (JAMA), or BMJ.
Porque?
Results:
•Mammography 19% reduction of breast cancer mortality;
� approximately 15% for women in their 40s
� 32% for women in their 60s
• For a 40-50
•in10 years of screening:
� risk of a false-positive result is about 61%
19% of the cancers diagnosed during that 10-year period would not have become clinically

30/05/2016
3
Porque?
False-Positives with Additional Testing and Anxiety.
10% of women will be recalled from each screening examination for further
testing, and only 5 of the 100 women recalled will have cancer;
50% of women screened annually for 10 years in the United States will
experience a false-positive, of whom 7% to 17% will have biopsies;
False-Negatives with False Sense of Security and Potential Delay in Cancer
Diagnosis.
6% to 46% of women with invasive cancer will have negative mammograms,
especially if they are young, have dense breasts, or have mucinous, lobular, or
rapidly growing cancers.
Porque?
Tabár L, Dean PB. Mammographic parenchymal patterns. Riskindicator for breast cancer? JAMA, 247:185-189,1982
Mamas densas Incidência de ca. de mama
Carney PA, et al Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography Ann Intern Med
2003; 138:168-175
Sens Espec
adiposa 87 % 96,9 %
densa 62,9 % 89,1 %
l 329.495 de 40 a 89 anosl 463.372 mamografias de rastreamento
Porque?
100 98,3 93,5 97,3 97
64
98
83
48
64
78
0
20
40
60
80
100
120
1 2 3 4 2-4 Global
Mamografia Ultra-som Mamo+US
Densidade BI-RADS
Sen
sibi
lidad
e (%
)
EVOLUÇÃO
Kolb TM, Lichy J, NewhouseJH. Comparison of the Performance of Screening Mammography, Physical Examination, and Breast US and Evaluation of Factors that Influence Them: An Analysis of
27,825 Patient Evaluations, Radiology 2002; 225:165-1 75
30/05/2016
4
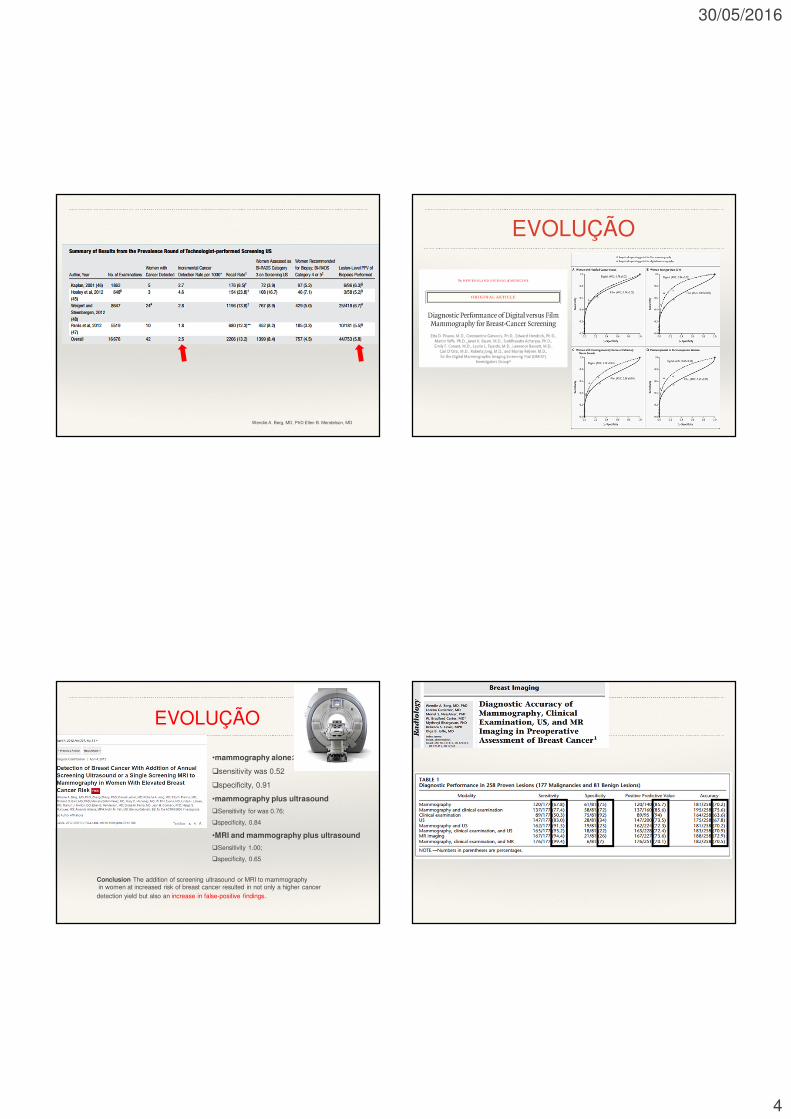
Wendie A. Berg, MD, PhD Ellen B. Mendelson, MD
EVOLUÇÃO
Conclusion The addition of screening ultrasound or MRI to mammographyin women at increased risk of breast cancer resulted in not only a higher cancerdetection yield but also an increase in false-positive findings.
•mammography alone:
�sensitivity was 0.52
�specificity, 0.91
•mammography plus ultrasound
�Sensitivity for was 0.76;
�specificity, 0.84
•MRI and mammography plus ultrasound
�Sensitivity 1.00;
�specificity, 0.65
EVOLUÇÃO

30/05/2016
5
NORUEGA0SLOEstudo
Prospectivo
SUÉCIAMALMO
ITALIATRENTA
EstudoProspectivo
BRASILHSL
BRASILMAMA
IMAGEM
USAROSE
Aumento da detecçãodo câncer de mama 27/40% 45% 34% 16/33% 25% 32%
Tomossíntese x Detecção precoce do câncer
Aumento na taxa de
detecção do câncer 1-4
Aumento na detecção de câncer
invasivo 1-4
Aumento no VPP para reconvocação
4
Redução das taxas de reconvocação 1-4
1. Skaane P et al. Radiology. 2013 Apr;267(1):47-56.2. Ciatto S et al. Lancet Oncol. 2013 Jun;14(7):583-9.
3. Haas BM et al. Radiology. 2013 Dec;269(3):694-700.4. Rose SL et al. AJR Am J Roentgenol. 2013 Jun;200(6):1401-8.
RESUMINDO
RadioGraphics 2015; 35:302–315
REVOLUÇÃO

30/05/2016
6
JCF, 50 anos
Exame físico:Massa palpável na mama esquerda
Mamografia: BI-RADS 2
Cortesia Dr. Felipe Barra

30/05/2016
7
Indicações da CESM❖ Ca. de mama❖ Detecção❖ Mamas densas❖ Alto risco❖ Diagnóstico - Caracterização de lesões❖ Extensão❖ multi-focalidade❖ Contra-lateralidade❖ Ca. Oculto❖ Pós-operatório (margens comprometidas)❖ Monitorar terapia (QT neoadjuvante)
Indicações da CESM
Mamografia e US inconclusivos: ❖ Útil em resolver problemas❖ Possíveis falsos positivos de RM❖ Mamas muito densas❖ Cicatrizes extensas ❖ Pós radioterapia ❖ Mastite x Tumor

30/05/2016
8

30/05/2016
9
CEDM x MMG+USGRastreamento - alto risco
MMG MMG + USG CEDM
Sensibilidade 78% 90% 93%
Especificidade 58% 47% 63%
VPP 70% 69% 76%
VPN 67% 78% 87%
AUC 0,74 0,85 0,91
Dromain C, et al. Eur Radiol. 2010 Sep 14;21(3):565–74.

30/05/2016
10
AAN, 49 anos - Carcinoma ductal invasivo
Mamografia: BI-RADS 5Nódulo mal delimitado na mama esquerda
Ultrassom:Nódulo na mama esquerda

30/05/2016
11
Mamografia com contrasteX
Ressonância Magnética

30/05/2016
12
OUTUBRO DE 2011 OUTUBRO DE 2015
JVR, 74 anosQueixa clínica na mama esquerda há 2 meses
Mamografia: BI-RADS 5Nódulo mal delimitado na mama
Ultrassom:Nódulo na mama esquerda
JVR, 74 anos

30/05/2016
13
JVR, 74 anos JVR, 74 anos
JVR, 74 anos
JVR, 74 anos
30/05/2016
14
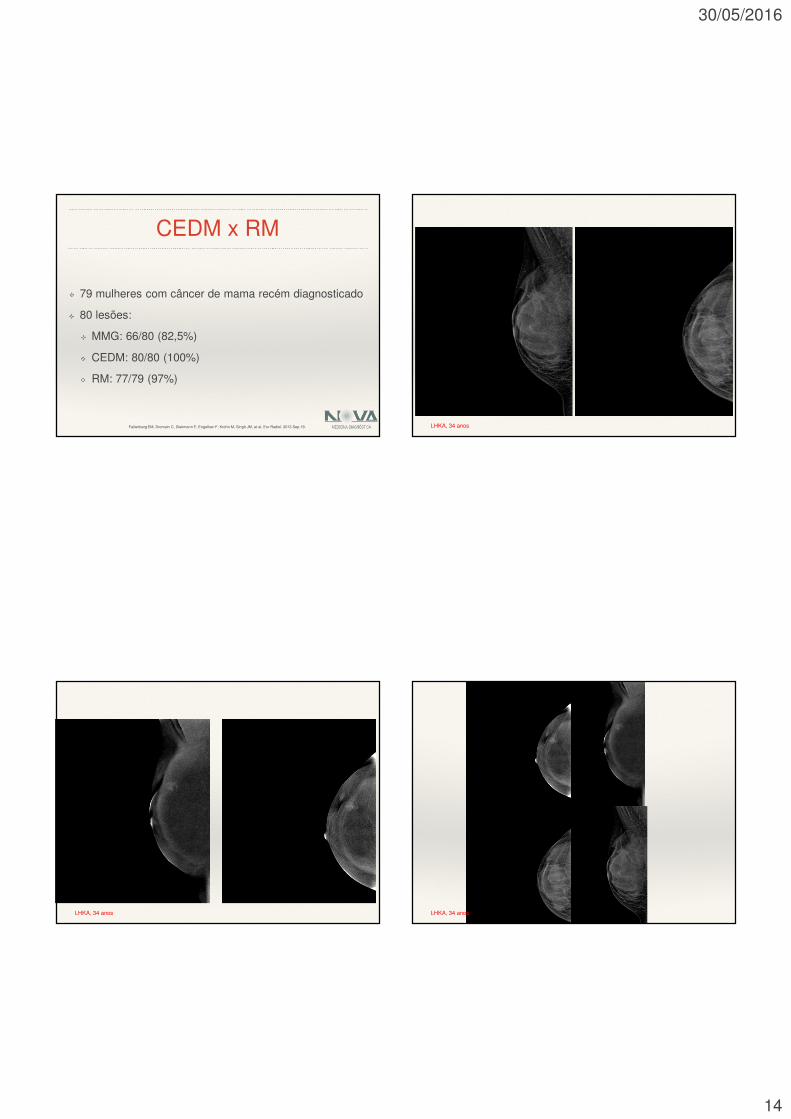
CEDM x RM❖ 79 mulheres com câncer de mama recém diagnosticado❖ 80 lesões:❖ MMG: 66/80 (82,5%)❖ CEDM: 80/80 (100%)❖ RM: 77/79 (97%)
Fallenberg EM, Dromain C, Diekmann F, Engelken F, Krohn M, Singh JM, et al. Eur Radiol. 2013 Sep 19. LHKA, 34 anos
LHKA, 34 anos LHKA, 34 anos

30/05/2016
15
CONTRASTE T2
Diagnóstico:CARCINOMA INVASIVO DE TIPO HISTOLÓGICO NÃO ESPECIAL (ductalinvasivo) COM DIFERENCIAÇÃO APÓCRINA, GRAU 2 HISTOLÓGICO(Nottingham) E GRAU 3 NUCLEAR LHKA, 34 anos
CEDM x RM❖ 52 mulheres (77 lesões)❖ 52 lesões primárias:❖ MMG: 42/52 (81%; 67-90%)❖ CEDM: 50/52 (96%; 87-99%)❖ RM: 50/52 (96%; 87-99%)
Jochelson MS, Dershaw DD, Sung JS, Heerdt AS, Thornton C, Moskowitz CS, et al. Radiology. 2013 Feb 20;266(3):743–51.
CEDM x RM❖ 25 lesões adicionais: ❖ MMG: 7 (28%)❖ CEDM: 14 (56%)❖ RM: 22 (88%)
Jochelson MS, Dershaw DD, Sung JS, Heerdt AS, Thornton C, Moskowitz CS, et al. Radiology. 2013 Feb 20;266(3):743–51.
❖ 13 falsos positivos❖ MMG: 0❖ CEDM: 2❖ RM: 13
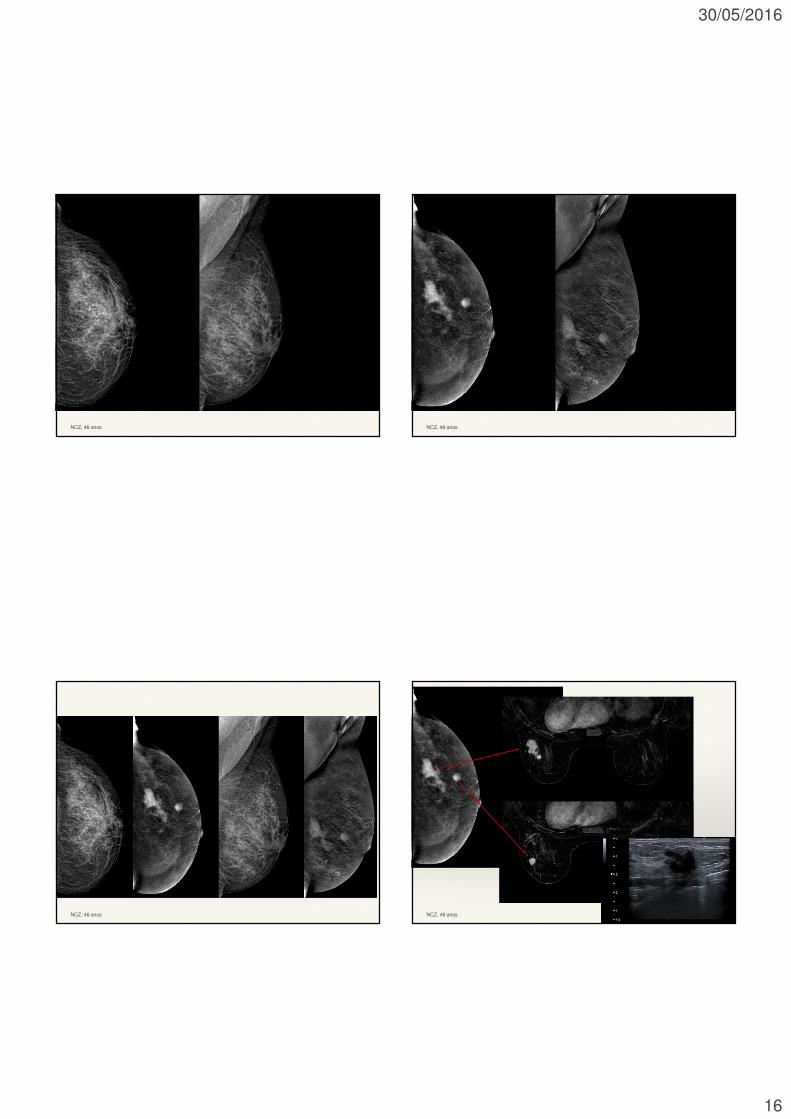
NCZ, 46 anosAntecedentes familiares positivos (2 irmãs com Ca de mama)
Mamografia: BI-RADS 4Ultrassom:
normal
30/05/2016
16
NCZ, 46 anos NCZ, 46 anos
NCZ, 46 anos NCZ, 46 anos

30/05/2016
17
CEDM x RM
n=62 (95) RM Mamografia com contraste
Sensibilidade 95,38% 95,38%
Especificidade 76,66% 95,38%
VPP 89,8% 98,5%
VPN 88,4% 89,3%
Acurácia 89,5% 91,5%
A. Vestito, M. Lorusso, E. Garasto, L. Dicembrino, D. Oreste, A. Ancona. ECR 2014MLRS, 49 anos
MLRS, 49 anos MLRS, 49 anos

30/05/2016
18
Diagnóstico:CARCINOMA INVASIVO DE TIPO HISTOLÓGICO NÃO ESPECIAL (ductalinvasivo) COM DIFERENCIAÇÃO APÓCRINA, GRAU 2 HISTOLÓGICO(Nottingham) E GRAU 3 NUCLEAR· ASSOCIADO A CARCINOMA DUCTAL “IN SITU”, PADRÕES SÓLIDO ECRIBRIFORME, COM DIFERENCIAÇÃO APÓCRINA, GRAU NUCLEAR 3, COMCOMEDONECROSE E MICROCALCIFICAÇÕES· GRADUAÇÃO HISTOLÓGICA:- ESCORE TUBULAR: 3- ESCORE NUCLEAR: 3- ESCORE MITÓTICO: 1· ESTROMA INTRATUMORAL COM:- INTENSA DESMOPLASIA
MLRS, 49 anos
Tamanho lesão
n=80 Média (DP) Mínimo Máximo Dif Patologia
Mamografia 27,31 (22,18) 4 mm 120 mm 14,82 mm
CEDM 31,62 (24,41) 10 mm 120 mm 12,14 mm
RM 27,72 (21,51) 6 mm 110 mm 12,23 mm
Patologia 32,51 (29,02) 8 mm 169 mm -
Fallenberg EM, Dromain C, Diekmann F, Engelken F, Krohn M, Singh JM, et al. Eur Radiol. 2013 Sep 19.
30/05/2016
19
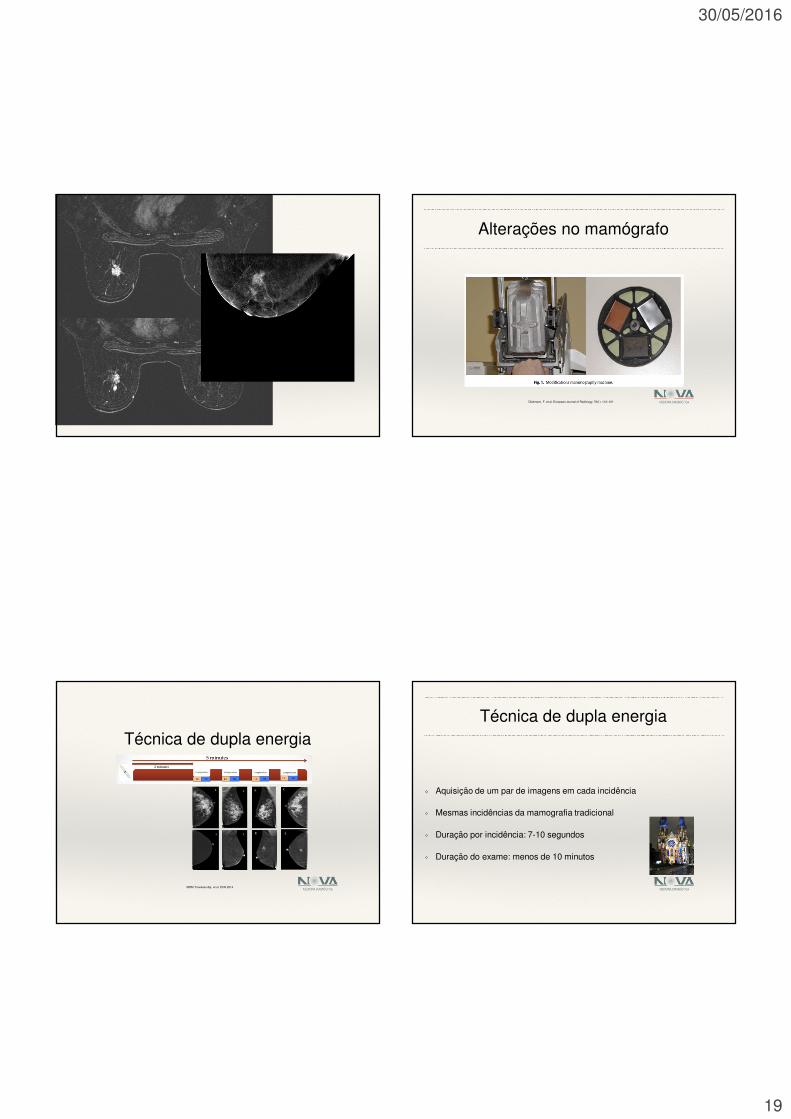
Alterações no mamógrafo
Diekmann, F. et al. European Journal of Radiology, 78(1), 112–121
Técnica de dupla energia
MDM Traviesso Aja, et al. ECR 2014
Técnica de dupla energia❖ Aquisição de um par de imagens em cada incidência❖ Mesmas incidências da mamografia tradicional❖ Duração por incidência: 7-10 segundos❖ Duração do exame: menos de 10 minutos

30/05/2016
20
Técnica de dupla energia❖ Vantagens:❖ Avaliação bilateral❖ Administração do contraste sem compressão mamária❖ Menor susceptibilidade a artefatos de movimento❖ Desvantagem❖ Ausência de curva cinética
Dose de radiação?
Dose Total de Radiação
Barra FR, et al. em publicação

30/05/2016
21
RESUMINDO❖ Como as incidências de baixa energia são similares a mamografia
digital de acordo com inúmeros trabalhos temos de fato:❖ 20 % de incremento de dose por exame
Evaluation of low-energy contrast-enhanced spectral mammography imagesby comparing them to full-field digital mammography using EUREF imagequality criteria.
Conclusion: Low-energy CESM images are non-inferior to FFDM images. From
this perspective FFDM can be omitted in patients with nain patients with an indication for CESM.
Lalji C.U, et al, European Radiology, 2015; 10: 289-298, PMID 5813015.
Contraste❖ Contraste iodado não-iônico❖ Dose: 1,5 ml/kg❖ Concentração: 300mg/ml❖ Fluxo: 3ml/s (30 s)
Qual nossa função❖ Informar da melhor forma possível a comunidade médica e
nossos pacientes sobre a segurança do contraste❖ Tratar de forma clara e objetiva os mitos e verdades❖ Estar capacitado tecnicamente a identificar e solucionar
complicações em qualquer procedimento

30/05/2016
22
Verdade – Avaliação pré-teste❖ Any patient who describes an “allergy” to a food or contrast media
should be questioned further to clarify the type and severity of the
“allergy” or reaction, as these patients could be atopic and at
increased risk for reactions.❖ Most forms of atopy result in a 2 to 3 times likelihood of contrast
reaction compared with non-atopic patients. ❖ However, considering the rarity of severe life-threatening
anaphylaxis, this level of incremental risk remains low and should be
considered in the context of risk versus benefit.
Verdade – Pré-medicação❖ Two frequently used regimens are: ❖ 1. Prednisone – 50 mg by mouth at 13 hours, 7 hours, and 1 hour before contrast media injection, plus Diphenhydramine (Benadryl®) – 50 mg intravenously, intramuscularly, or by mouth 1 hour before contrast medium [12]. or ❖ 2. Methylprednisolone (Medrol®) – 32 mg by mouth 12 hours and 2 hours before contrast media injection. An anti-histamine (as in option 1) can also be added to this regimen injection [34]. ❖ If the patient is unable to take oral medication, 200 mg of hydrocortisone intravenously may be substituted for oral prednisone in the Greenberger protocol [35].
Mito – Pré-teste❖ Pretesting: Preliminary intradermal skin testing with
contrast agents is not predictive of adverse reactions,
may itself be dangerous, and is not recommended [13-
14,32]
Verdade – Esteja preparado❖ Treinamento da equipe❖ Cada um deve saber sua tarefa❖ Tenha tudo na ponta da língua
“ou na parede da sala”

30/05/2016
23
Mito – Nos dias atuais há muitas reações alérgicas graves ao contraste❖ Desconstruindo a memória residual:
Historically, acute adverse events occurred in 5% to 15%
of all patients who received ionic high-osmolality contrast
media (HOCM). Many patients receiving intravascular
HOCM experienced physiologic disturbances (e.g.,
generalized warmth, nausea, or emesis), and this was
often documented as a contrast reaction.
Verdade – Nos dias atuais as reações alérgicas graves são raras❖ nonionic low-osmolality contrast media (LOCM) LOCM are
associated with a very low incidence of acute adverse events,
and the bulk of these are not lifethreatening. ❖ Cochran et al reported an overall acute adverse reaction rate
(allergic-like + physiologic) of 0.2% for nonionic LOCM upon
review of 29,508❖ Wang et al reported an overall acute allergic-like reaction
frequency of 0.6% in 84,928 adult
Verdade – Nos dias atuais as reações alérgicas graves são raras❖ Katayama H et al -Serious acute reactions to IV LOCM are rare,
with an historical rate of approximately four in 10,000 (0.04%) ❖ Katayama H et al - no fatal reactions were attributed to LOCM
despite greater than 170,000 injections❖ A review of U.S. FDA and drug manufacturer data from 1990 to
1994 demonstrated 2.1 fatalities per 1 million contrast-enhanced
studies using LOCM
Iodo x Gadolínio - Alergia❖ Gadolínio : ❖ Reactions resembling an “allergic” response are very unusual and vary in frequency from 0.004% to 0.7%.❖ Severe, life-threatening anaphylactoid or nonallergicanaphylactic reactions are exceedingly rare (0.001% to 0.01%)❖ Iodo:❖ A slightly higher overall frequency of 0.7% (allergic-like + physiologic) ❖ Serious acute reactions to IV LOCM are rare, with an historical rate of approximately four in 10,000 (0.04%)

30/05/2016
24
Verdade – Limitações❖ Miastenia graves❖ Nefropatia crônica❖ Age > 60 ❖ History of renal disease, including: ❖ Dialysis❖ Kidney transplant❖ Single ❖ History of hypertension requiring medical therapy❖ History of diabetes mellitus ❖ Metformin or metformin-containing drug combinations – discontinued at the time of or prior to the procedure, and withheld for 48 hours subsequent
Verdade – Gadolinium e alteração renal❖ Nephrogenic systemic fibrosis (NSF) is a fibrosing
disease❖ In 2006 several groups noted a strong association
between gadolinium-based contrast agent (GBCA)
administration in patients with advanced renal disease
and the development of NSF
DÚVIDA ❖ FDA, Based on the need for additional information, at this time, we are not requiring manufacturers to make changes to the labels of GBCA products.❖ To reduce the potential for gadolinium accumulation, health care professionals should consider limiting GBCA use to clinical circumstances in which the additional information provided by the contrast is necessary.
30/05/2016
25
COMO FAZEMOS❖ Termo de consentimento e informativo
COMO FAZEMOS
COMO FAZEMOS COMO FAZEMOS

30/05/2016
26
COMO FAZEMOS COMO FAZEMOS
Resultados IniciaisNova Medicina Diagnóstica❖ 87 casos de CESM de março ate fevereiro de 2015❖ 24 casos de pacientes de alto risco encaminhadas
para complementação do rastreamento (contra-
indicações a RM)❖ 3 caso CESM positivo❖ 21 exames CESM normais
CAPF, 49 anos
História familiar positiva
Mamografia: BI-RADS 2
❖ Ultrassom: BI-RADS 1

30/05/2016
27
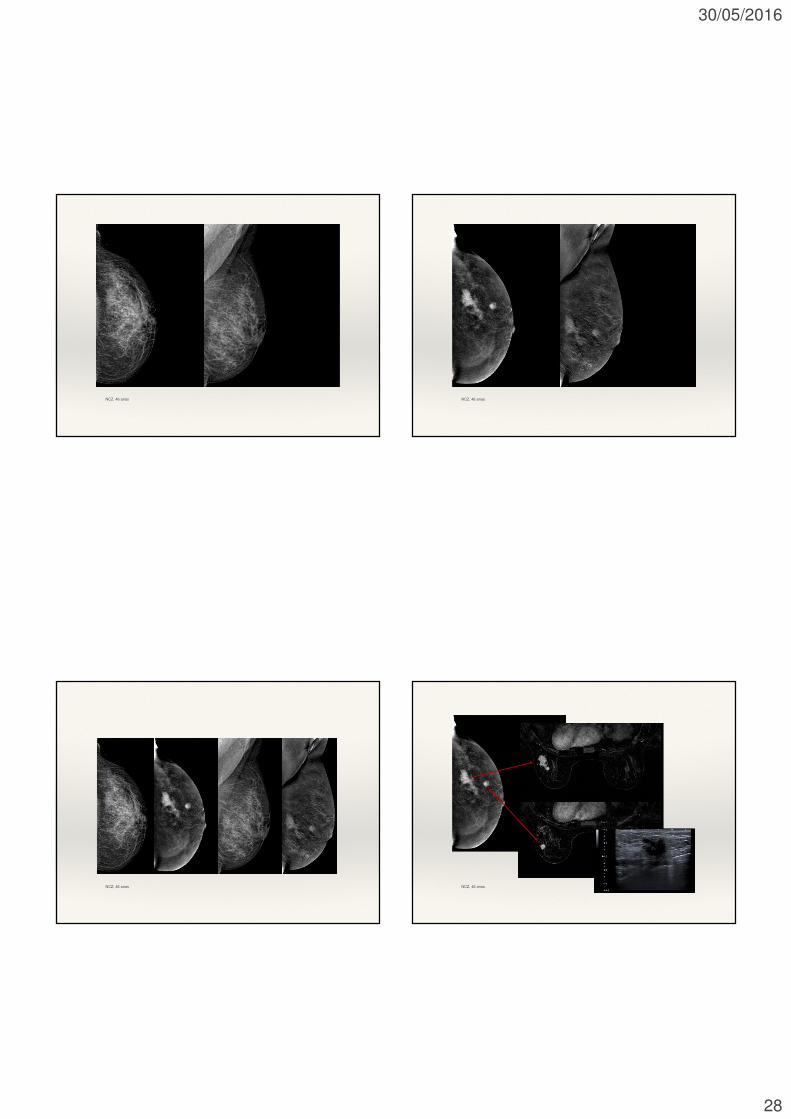
NCZ, 46 anosAntecedentes familiares positivos (2 irmãs com Ca de mama)
Mamografia: BI-RADS 4
❖ Ultrassom externo:❖ normal
30/05/2016
28
NCZ, 46 anos NCZ, 46 anos
NCZ, 46 anos NCZ, 46 anos

30/05/2016
29
Resultados Iniciais❖ 63 casos de exames externos alterados encaminhados para realizarMamografia com contraste e RM ❖ 47 com lesões confirmadas❖ 44 casos de RM x CESM concordantes❖ 1 caso de RM positiva e CESM negativa❖ Lesão profunda, fora do campo da mamografia❖ 2 casos mamografia com contraste superior❖ Calcificações agrupadas
PT, 41 anos
PT, 41 anosRM normal
Realizada mamotomia pelo USG(espessura)
Diagnóstico:CARCINOMA DUCTAL “IN SITU”, GRAU 3 HISTOLÓGICO (Nottingham) GRAU 3 NUCLEAR
PT, 41 anos
LIMITAÇÕES❖ Avaliação das axilas;❖ Avaliação de comprometimento da musculatura peitoral;❖ Lesões profundas (dificuldade de posicionamento);❖ Pacientes com implantes mamários;

30/05/2016
30
ACR, 46 anos
Encaminhada para estadiamento, com Ca invasivo lobular
Na RM a lesão é posterior, medial
Feita nova incidência com 3D, identificando a lesão
Limitação do método: posicionamento
30/05/2016
31
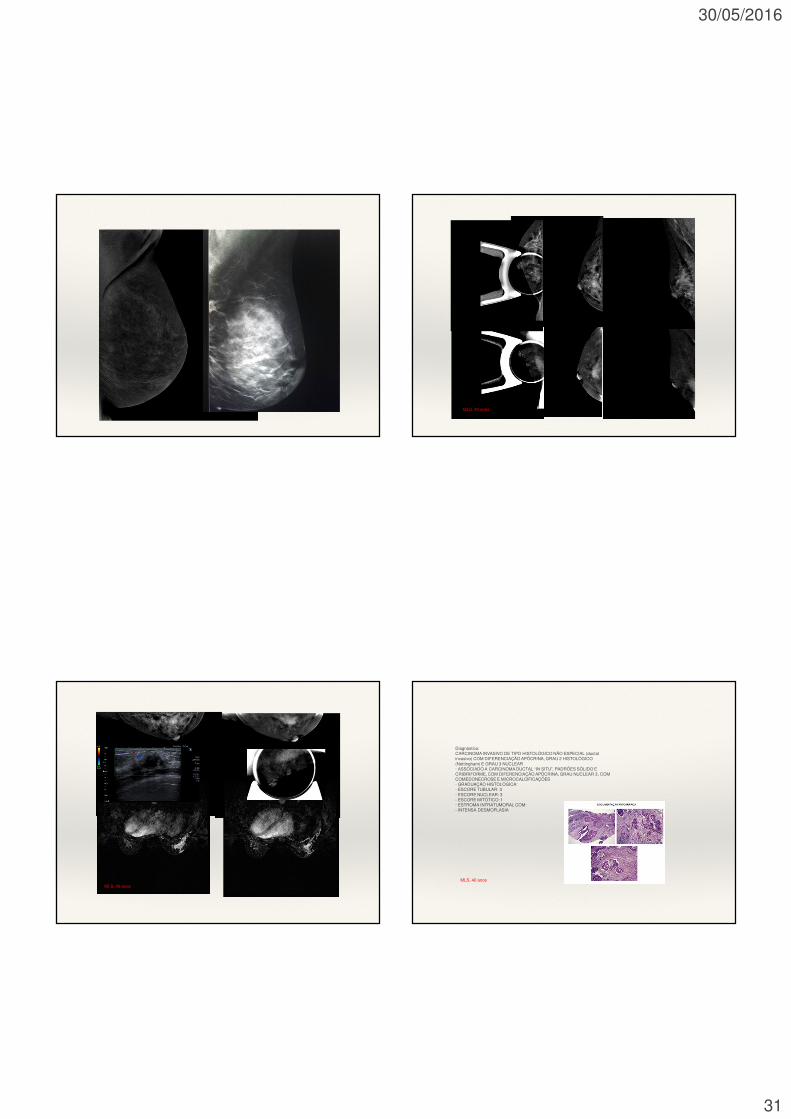
MLS, 40 anos
MLS, 40 anos
Diagnóstico:CARCINOMA INVASIVO DE TIPO HISTOLÓGICO NÃO ESPECIAL (ductalinvasivo) COM DIFERENCIAÇÃO APÓCRINA, GRAU 2 HISTOLÓGICO(Nottingham) E GRAU 3 NUCLEAR· ASSOCIADO A CARCINOMA DUCTAL “IN SITU”, PADRÕES SÓLIDO ECRIBRIFORME, COM DIFERENCIAÇÃO APÓCRINA, GRAU NUCLEAR 3, COMCOMEDONECROSE E MICROCALCIFICAÇÕES· GRADUAÇÃO HISTOLÓGICA:- ESCORE TUBULAR: 3- ESCORE NUCLEAR: 3- ESCORE MITÓTICO: 1· ESTROMA INTRATUMORAL COM:- INTENSA DESMOPLASIA
MLS, 40 anos
30/05/2016
32
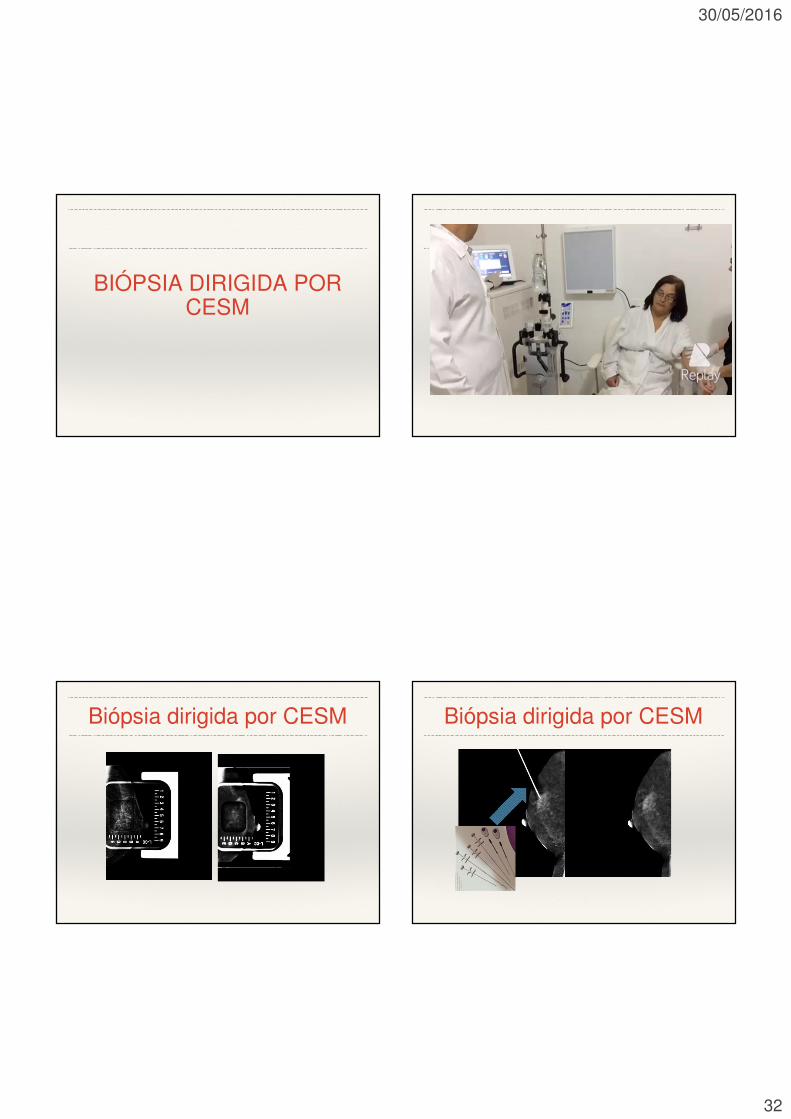
BIÓPSIA DIRIGIDA POR CESM
Biópsia dirigida por CESM Biópsia dirigida por CESM

30/05/2016
33
Biópsia a vácuo após a localização COLÁGENO
CILS
Biópsia dirigida por CESM❖ Tempo de execução do procedimento: 20 minutos❖ 6 minutos na localização e colocação do clip via CESM❖ 2 minutos para troca de sala❖ 12 minutos para a realização da biópsia à vácuo❖ Custo: valor de uma biópsia à vácuo + localização com clip ❖ Lembrando que parte do clip de colágeno fica na lesão
permitindo a localização em até 8 semanas da área
Porque CESM!❖ Rápida execução e leitura❖ Baixo custo❖ Fácil implementação❖ Curva de aprendizado rápida❖ Não operador dependente❖ Reprodutível❖ Disponível

30/05/2016
34
Porque CESM!❖ Avaliação bilateral❖ Baixa dose de radiação (incremento de 20%)❖ Relação sensibilidade x especificidade (97% x 85%)❖ Redução de biópsias (alto VPN 98% aproximado)❖ Redução dos falso positivos❖ Excelente correlação com RM❖ Boa correlação com a histologia
Porque!❖ Baixo índices de artefatos❖ Mesmas indicações que a RM❖ Correlação com mamografia❖ A imagem de baixa energia tem a mesma sensibilidade da mamografia (??)❖ Possível avaliação de calcificações❖ Sempre será mais sensível que a mamografia❖ Possibilidade de biópsias
Limitações / Desvantagens❖Radiação ionizante❖ Padronização da técnica❖Uso de contraste❖ Administração do contraste❖Disponibilidade