DISSO 4.1 (1)
57
A Meta-Analysis of Proton Beam Therapy (PBT) and Intensity-Modulated Radiation Therapy (IMRT) in the Treatment of Prostate Cancer’. Presented to the Faculty of Life Sciences Anglia Ruskin University Cambridge In partial fulfilment of the requirements for the Bachelors (Hons) of Science in Biomedical Sciences By Omar Naveed April 2016 Page 1 of 57
-
Upload
raja-omar-naveed -
Category
Documents
-
view
31 -
download
0
Transcript of DISSO 4.1 (1)

A Meta-Analysis of Proton Beam Therapy (PBT) and Intensity-Modulated Radiation Therapy (IMRT) in the Treatment of Prostate Cancer’.
Presented to the Faculty of Life SciencesAnglia Ruskin University
Cambridge
In partial fulfilment of the requirements forthe Bachelors (Hons) of Science in Biomedical Sciences
ByOmar Naveed
April 2016
Page 1 of 40

I would strongly like to thank Don Keiller, for the guidance, motivation and encouragement
I needed to finish my thesis.
Page 2 of 40

Table of Contents
Introduction .………………………………………………………………………….4
I. Prostate Cancer……………………………………………….……………....4
II. Proton Beam Therapy……………………………………………….………..9
III. Intensity-Modulated radiation therapy …………………………………….13
IV. Null Hypothesis ………………………………………………………………15
V. Alternative hypothesis ………………………….……………………………15
VI. Aim…………………….………………………………………………………15
Methodology………………………………………………………………………….16
I. Data sources………………………………………………………………….16
II. Criteria of selection……………………………………………………..……17
Results …..……………………………………………………………………………19
I. Fox plott…………………..………………………………………………….19
II. t- test……………………………………………….…………………..……...21
III. error bar graph………………………………………………………………21
Discussion…………………………………………….……………………………….23
I. Toxicity of PBT and IMRT…………………………………….……………26
II. Cost of PBT and IMRT………………………………….…………….……..27
III. Cancers Treated with PBT…………………………………….…………….28
IV. Future of PBT ………………………………………………….………….....29
Conclusion……………………………………………………………….…………….29
Acknowledgement……………………………………………………….……………31
References……..……………………………………………………..……………….31
Page 3 of 40

Introduction
Prostate Cancer (PC)Prostate cancer is a prevalent malignant disease in males and a main cause of death in the UK. According to the Cancer Research U.K. they estimated approximately 47,000 new cases of diagnosed patients and >11 thousand deaths annually. This is an overwhelming 130 new cases diagnosed every day. Worldwide prostate cancer has been estimated to occur in approximately 1.11 million men; an estimated 1 in 8 men will be diagnosed with prostate cancer throughout their lifespan. PC also known as adenocarcinoma, or glandular cancer which is characterized by semen-secreting prostate gland cells that are highly sensitive to suffering mutations. Initially, small groups of cancer cells remain confined, these are known as carcinoma in situ and Prostatic intraepithelial neoplasia (PIN), (Costello and Franklin, 2014). The developmental progression of these cancerous cells involve its spread to neighbouring prostate tissue known as the stroma. In addition, the tumour may invade nearby organs including the seminal vesicles or the rectum and enter the bloodstream and lymphatic system affecting other regions in the body such as bones and lymph nodes. This process is known as metastasis (Gundem et al., 2015). Furthermore, prostate differentiation as well as prostate cancer growth and progression are dependent upon androgen receptor (AR) signaling; which is encoded by a single copy gene situated at Xq11.2-q12, (Velcheti et al., 2008). This protein consists of approximately 919 amino acids in length. The length of polyglutamine repeats may vary between 18-22 repeats. However, long repeats (>40) has been largely related with developing prostate cancer (Velcheti et al., 2008).
The role of Z1P1 in prostate cancerStudy by Christudoss et al., (2011), shows that ZIP1 is accountable for the active transport of zinc into prostate cells. The importance of zinc is to
Page 4 of 40

simply help the cell metabolize citrate, an important component of semen. In this process prostate cells typically use enormous amounts of energy (ATP) in order to accomplish this task. Prostate cancer cells generally lack zinc resulting in its growth and spread. The lack of zinc occurs through silencing of the gene that produces the transporter protein ZIP1. ZIP1 is a tumour suppressor gene product for the gene SLC39A1. Furthermore, Costello and Franklin, (2014) shows that downregulation of Z1P1 and decreased zinc are evident in PIN. Recent study by Song and Ho, (2014) shows that Zinc maintains DNA integrity by modulating the expression effects of zinc on the inhibition of terminal oxidation, induction of mitochondrial pathogenesis, and suppression of NFκB activity. In the event of zinc depletion in prostate epithelial cells (PrEC), p53 becomes compromised, hence DNA repair is ineffective, thus leading to compromised DNA integrity.
The role of P13k & Akt in prostate cancer Protein kinase B (Akt), is a downstream effector of phosphatidylinositol 3-kinase (PI3K). It is often implicated in prostate cancer. Study by Gosh et al., (2003) shows that Akt activation is vital for the progression of prostate cancer to an androgen-independent state. In their study they found that Akt phosphorylation is accompanied by the inactivation of ERK, a member of the mitogen activated protein kinase (MAPK) family. Furthermore, PI3k/Akt signaling cascade is involved in transforming growth factor beta/SMAD signaling cascade to ensure prostate cancer cell survival and protection against apoptosis.
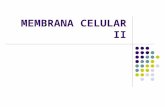
Autophagy Cell Death in prostate cancer cells The mechanism of autophagy in cancer cells are directly mediated by the Beclin1 protein which is encoded by the BECN1 gene (Fig. 1), which in turn modulates the signaling pathways, that autophagy is directly involved (Focaccetti et al., 2015).
Page 5 of 40

Page 6 of 40
Autophagosom Formation
Ambra1Vps34
Atg114LVps15Beclin-1
Atg14L Complex
Autophagosome Maturation
Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1
RubiconBif1
Ambra1Vps34
UVRAGUVRAG Ambra1 Vps34
Vps15 Vps15Beclin-1Beclin-1
Rubicon-UVRAG Complex
UVRAG ComplexFUSION
Lysosome/Endosome
Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34
Atg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LAtg114LVps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1
Atg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L ComplexAtg14L Complex
RubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconRubiconBif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1Bif1
Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34
UVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAGUVRAG Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1Ambra1 Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Vps34Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15 Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Vps15Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1Beclin-1
Rubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG ComplexRubicon-UVRAG Complex
UVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG ComplexUVRAG Complex

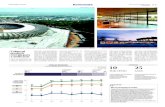
Nuclear factor- κ B (NF- kB) signalling pathway in prostate cancer The NF-κB includes, NF-κB2 p52/p100, NF-κB1 p50/p105, c-Rel, RelA/p65, and RelB; which plays a fundamental role at regulating the expression of genes. For instance, NF-κB cooperates with multiple other signaling molecules and pathways (Fig. 2) (Hoesel and Schmid, 2013).
Page 7 of 40
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
BAFF-R; CD40; BLys
Ras Kinase
HTLV EGF
TCR/BCRTNFR
TLRH2O2Heat Shock
PKCMyD88TAX
TRAF3 EGFRRaIBTRADD/TRAF2
P38
SyK
NIK TBK
CK II
TAK 1
EGFR
IKKα
IKKyIKKαIKKβ
GRB2
NFKBP100/RelB
P50/P65
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
Figure 1. Regulatory function of three Beclin1 containing complexes in different stages of autophagy. There are three class III PI3K complexes that are involved in autophagosome formation and maturation. The Atg14L complex (Beclin1–hVps34–Atg14L) functions in autophagosome formation. The UVRAG complex (Beclin1–hVps34–UVRAG) required for the maturation of autophagosome, while Rubicon–UVRAG complex (Beclin1–hVps34–UVRAG–Rubicon) negatively regulates this process (Self- made adapted form) (Focaccetti et al.,
BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys BAFF-R; CD40; BLys
TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3TRAF3
NIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIKNIK
TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1TAK 1IKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKαIKKα
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβ
IKKyIKKαIKKβNFKB
P100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelBNFKBP100/RelB
P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65P50/P65

NUCLEUS
Page 8 of 40
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
P52/RelB P50/p65
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Proton Beam TherapyEnergised proton particles
Intrinsic Pathway
Extrinsic PathwayCD 95L TRAIL
CD95 Receptor TRAIL Receptor
FADDFADD
Bax
Bid
BCL 2
Caspase 9
Caspase 8 Caspase 8
Cytochrome C
Apaf 1
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
➢ Survival➢ Proliferation➢ Inflammation➢ B-cell maturation
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Figure 2. Activation of NFKB signaling pathway in ccRCC. Signaling and activation directly linked TAK1, IKK and P50/P60. Active NF-κB/Rel complexes are further activated by post-translational modifications (phosphorylation, acetylation, glycosylation) and translocate to the nucleus. Sulforaphane could potentially be used as a therapeutic agent. (Self- made adapted form) (Grivennikov, 2010).
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Proton Beam TherapyEnergised proton particles
Intrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic PathwayIntrinsic Pathway
CD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95LCD 95L TRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAILTRAIL
CD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 ReceptorCD95 Receptor TRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL ReceptorTRAIL Receptor
FADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADDFADD
BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2BCL 2
BaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBaxBax
BidBidBidBidBidBidBidBidBidBidBidBidBidBidBidBidBidBidBidBidBid
Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9Caspase 9
Cytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome CCytochrome C
Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1Apaf 1

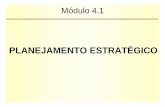
Mitochondrial- inducing cell death via Proton beam therapy
The mitochondrial apoptotic pathways and signal-transducing molecules are characterized by
death receptors including, CD95 (APO-1/Fas), TNF receptor 1 (TNFRI), TNF-related
apoptosis-inducing ligand-receptor 1 (TRAIL-R1) and TRAIL-R2 are largely involved in
killing tumour cells in response to Proton beam therapy (Stanley et al., 2013). It essentially
triggers an increase in CD95L expression, which is mediated by an activation of NFkB and
transcription factor activator proteins (AP-1) (Fulda and Debatin, 2006). Seen in (Fig. 3).
Proton Beam Therapy (PBT)Robert R. Wilson, a professor of physics, who was the designer of the Harvard cyclotron,
first introduced the idea of killing cancer cells by using protons. This idea was then
confirmed by a large scale study on protons by Berkeley Radiation Laboratory (Sugerman and
Livingston, 2014). In 1998, the National Cancer Centre Hospital East (NCCHE) introduced
proton facilities for the application of clinical use in the treatment of prostate cancer (PC)
Page 9 of 40
SMAC/ DIABLO
CASPASE 3 IAP
AIFCAD, ICAD, DFF45
APOPTOSIS
Figure 3. Mitochondrial apoptotic signaling pathways induced Energized Proton beam particles. CD95 (APO-1/Fas) and TNF-related apoptosis-inducing ligand (TRAIL) results in receptor aggregation and recruitment of the adaptor molecule Fas-associated death domain (FADD) and caspase-8. Following recruitment of caspase-8 which essentially leads to the activation of caspase-3 through formation of the Cytochrome C/Apaf-1/caspase-9-containing apoptosome complex. (Self- made adapted) (Fulda and Debatin, 2006).
SMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLOSMAC/ DIABLO
CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3CASPASE 3 IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP IAP
AIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFAIFCAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45CAD, ICAD, DFF45
APOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSISAPOPTOSIS

(Jones, 2016). The proton boost therapy were then employed in 2001 and the trial protocol has
been approved by the institutional review board (Nihei et al., 2005). The highly discussed
and topical concept of proton beam therapy (PBT) for prostate cancer fueled discussion in the
euro-oncological community questioning its superiority to photon therapy regarding local
control, patient survival, better tolerance to side effects and the continuous of the therapy
inquired by patients (Habl and Debus, 2015). Currently, there are ongoing trials for proton
therapy for prostate cancer and emergence of its biological and clinical data (Schiller et al.,
2016).
A proton beam is created by a cyclotron or synchrotron that isolates the proton from a hydrogen particle and speeds it up. The vast mass and vitality provides the increasing speed framework giving protons a particular energy that transport them into a body. Once the protons are in the body, its speed is reduced due to its mass, charge and interactions and eventually come to a stop at a certain depth. This is the point where collaboration mostly occurs with encompassing electrons, causing radiation damage to the target DNA and generating particle ionization. This ability of proton stopping at a particular distance can be controlled based on their energy and the depth of accumulation in the tumour (Fig5b). In contrast, x-rays continue to deposit radiation doses through the target area, damaging nearby healthy tissues and increasing exposure to side effects (Wisenbaugh et al., 2014).
Proton therapy referred to as proton beam therapy (PBT) have been utilised for clinical
purposes for more than 50 years in the treatment of spinal cord, brain, breast, prostate cancers
and noncancerous diseases. There are number of studies which reported the ability of proton
therapy to spare surrounding healthy tissues however, other studies argued and criticised the
cost-effectiveness of such treatment therefore its use on cancer treatment has not been
validated in comparison with photon therapy (Reiazi et al., 2015). Furthermore, small
volumes are treated and the treatment times are low which led to hypothesised high patient
throughput therefore it should not form the basis of medical decision-making.
Traditional radiation therapy uses photons and electrons particles directly at tumours with the
intention of neoplastic tissue eradication whilst adjacent and surrounding normal tissues are
preserved (Levin et al., 2005 and Sugerman and Livingston, 2014). However, radiation dose
Page 10 of 40

delivered poses serious problem such as the concern for the occurrence of second
malignancies within healthy tissues and other various side effects (Jones, 2016). A form of
charged particle therapy, the proton beam radiotherapy has no exit dose benefit and it
function through excellent dose distribution to neoplastic tissue. With this characteristic, it
allows excellent choice of tumour treatment within its vicinity and avoiding affecting the
important organs of the body such as the brain, spinal cord and especially pediatric
malignancies (Levin et al., 2005 and Anon, 2007).
Similarly to a standard x-ray radiation therapy, PBT is a type of external-beam radiation therapy which emits painless radiation through the skin (Main, 2016). The mechanism of radiotherapy (RT) targets the localized PC whilst ensuring
minimum application of possible dose to surrounding tissues such as bladder and rectum,
therefore side effects and toxicities to patients are avoided (Schiller et al., 2016). The intrinsic physical properties of PBT makes its utilization appealing in therapeutic radiation oncology (Blanchard et al. 2012). PBT is an attractive form of therapy due to its physical ability to maintain highly conformal target distribution dose particularly to the tumour while minimizing dose to surrounding normal tissues (Chen, 2011). Also, in comparison to photons, the dose distribution properties of protons are entirely different and the ability to avoid extra-target radiation which is inherent to photons. Due to the heavier mass of proton weighing roughly 1800 times of an electron, it confers particular dosimetric advantages, hence in comparison to photons, heavy particles such as of proton have the ability to stop within target tissue (Wisenbaugh et al., 2014).
Currently, the favorable treatment in radiotherapy for prostate cancer is photon therapy. Due
to no charge and no mass of photons, it can easily travel to the target tissue. Initially, the
photons increases their energy while interacting with the target material electrons (the body),
thus enhancing the effect of the radiation. This results to “dose accumulation effect” which
means that the entrance surface is reached by the peak dose within few centimeters. As the
dose goes further subsequently through the body, the radiation dose drop-offs after energy
deposition until there is no dose delivered to normal tissues beyond the Braggpeak eventually
exiting the body (Diallo et al., 2009, Nihei et al., 2005 and Chen, 2011). Therefore, PBT
provides better option as radiation dose is safely escalated due to reduced scatter and exit
dose in comparison to photons (Chen, 2011). Furthermore, proton beams have a sharp
Page 11 of 40

Bragg peak; with low energy before the peak and almost zero energy after the peak (Nihei et al., 2005). Therefore, in proton beam therapy (PBT), normal tissue around the tumour receives a reduced dose compared to photon radiotherapy, and this is especially beneficial for pediatric tumours or tumours adjacent to normal tissue for which irradiation should be strictly avoided (Mizumoto et al. 2016).
The ‘Bragg peak’ refers to the physical depth dose characteristic of charged particles which
can spread out, shaped and conform the volume and depth of an irregular target (Nihei et al., 2005) (Fig. 4). In addition, recent studies which conducted long term follow up found that PBT has the ability to reduce rate of secondary malignancies (Sethi et al., 2014). The tumour control is similar to photon therapy however, latent toxicity and secondary malignancies is lower due to lower distribution of dose (Mizumoto et al. 2016).
Due to the different field plans, helical techniques and rapid arc, the doses are significantly
smaller (Kosaki et al., 2012). Gastrointestinal (GI) and genitourinary (GU) are the possible
side effects and may potentially increase risk occurrence of secondary malignancies
(Paganetti, 2012) therefore, the photon radiation therapy in terms of its physical characteristic
is seemingly inappropriate in targeting the organs located at a great depth. Studies on
multiple dose escalation demonstrated that by increasing the radiation dose for PC treatment
lead to better biochemical disease-free survival and less clinical failure rates (Chen, 2011).
In addition to the risk of second malignancies developing, this depends on multifactorial
reasons such as dose distribution and volume irradiate as solid cancers are generally found
near or within the primary field of treatment (Diallo et al. 2009). Close distance from the
primary cancer or tissue can also lead to soft tissue and bone sarcoma (Rubino et al. 2005).
On the other hand, Ron et al. (1988) suggested that low doses distributed further outside the
dose field have been linked with the development of second malignancies.
Furthermore, the effect on tumour control with the use of proton therapy is likely similar to
electron or protons however, the dose on significant tissues such as the lung and the heart
may considerably be reduced in order to prevent the future development of very low toxicity
(Gagliardi et al., 1996). A study conducted by Nihei et al. (2005) found that longer
exposure to proton treatment was impractical which may partly due to the development of
second malignancies and complications after the initial treatment. The Radiation
Page 12 of 40

Therapy Oncology Group (RTOG) conducted studies in the evolution of the safety and efficacy of high-dose irradiation for prostate cancer using IMRT or 3D-CRT (Zelefsky et al., 2001 and Michalski et al., 2003). A single proton
beam had different type of doses: no exit dose, a maximal dose at a user-defined depth and
low entrance dose. Therefore, proton beam therapy (PBT) can create 3D conformal dose distribution within defined radiation track length without virtually (Main et al. 2016) emitting extra dose to nearby or surrounding
normal tissues and the probability of cure in comparison to conformal photon radiotherapy (Archambeau et al., 1974).
Figure 4. Beam dose distribution and depth-dose characteristics of proton and photon beams. The example proton beam is of a higher energy than the SOBP for clarity.
Page 13 of 40

Figure 5a and 5b. (a) Dose distribution of dynamic conformal photon therapy. (b) Dose distribution of proton boost therapy. Lateral opposed portals using proton beam can provide good dose coverage to the prostate and reduce the unnecessary irradiated volume of both the ventral and dorsal portion of the body. Isodose lines: orange, 105%; magenta, 100%; yellow, 95%; light green, 90%; light blue, 80%; light purple, 50%; purple, 20%. Red line shows the planning target volume (Nihei et al., 2005).
Intensity-Modulated R adiation Therapy (IMRT)
Intensity-Modulated radiation therapy (IMRT) is a fast past technological advancement in
the treatment of cancer in comparison to current treatment which uses 2D technology.
However, it is more expensive in the method of delivering radiation therapy in order to
minimize toxicity (Beadle et al. 2014). Cancers are treated with radiotherapy that uses
invisible high-energy x-rays and other rays such as electrons. IMRT encompasses various
techniques referred to as “inverse planning” that represents the core change.
Page 14 of 40

It has been 20 years since the first child was treated with IMRT(Paulino,
2016). The utilization of IMRT innovation for the treatment of PC has diffused quickly over the previous decade, and is currently the standard sort of radiation used to treat this cancer(Paulino, 2016). It is also creating
popularity within oncology community as it similarly uses radiation dose like proton beam
therapy in the treatment of cancer. IMRT is a stereotactic radiotherapy which utilities
multiple fields and angles to locate target such as of tumour tissues (Wai, 2015). Due to the
range of clinical concerns and radiobiological surrounding this particular therapy, the
potential for increased dose and daily increase of fraction size to the gross of cancer makes
the administration of the cancer therapy discouraging.
The advancement of conformal radiotherapy technique IMRT is the ability of the radiation
intensity across each radiation to be varied enabling more control over distribution of dose
to the objective range. Also, it specifically allow the conformation of high dose region to
create a concave shape to avoid critical damage to other organs in the body (Chiappiniello
et al, 2016). By controlling and modulating the intensity of radiation beam in multiple small
doses it allows radiation dose of IMRT to conform three-dimensional (3-D) share more
precisely of the tumour tissue. The three-dimensional (3-D) computed tomography (CT) or
MRI images of patients in conjunction with computerized dose calculations aid in the careful
planning in order to determine intensity dose pattern that will be able to successfully
conform to the shape of the tumour tissue and will predict the treatment plan that best
satisfies the constraints (Maddock, 2006). In routine radio therapy, for a six-field 3D conformai plan for malignancy of the prostate every treatment would take roughly thirty minutes, just five or six minutes of which was real radiation introduction. Every treatment utilizing IMRT should be possible within fifteen minutes (Maddock, 2006).
In comparison to conventional radiotherapy techniques, IMRT is more effective as it
administers safe dosage to tumours resulting to lesser side effects. The potential of IMRT to
reduce treatment toxicity are one of its advantages while doses are minimal (Chiappiniello
et al, 2016). In addition, compared to the conventional radiotherapy, IMRT is complex as it
requires longer daily treatment times, safety checks before patient can start initial
treatment and additional planning is needed. In regards to daily treatment, it takes longer as
Page 15 of 40

machine on-time is increased. Therefore, penetration of addition photons through or
scattered by gantry head shielding by patients as total-body dose (Wai, 2015). Typically,
leakage dose is considered of minimal risk. IMRT prevents division and growth of cancers
cells thus, slowing down tumour growth. There are majority of cases where radiation
therapy is able to kill all of the cancer cells therefore eliminating or shrinking tumour cells.
The whole-body exposure is significantly increased in IMRT (Goffman and Glatstein, 2002).
The goal of IMRT is spare normal tissues, however its ability to provide more conformal dose
distributions has allowed increased dose to tumour volumes and accelerated dose delivery.
It has been widely accepted that high-dose areas receive created than 2 Gy per fraction which is the standard with non-IMRT conventional therapies (Nutting et
al., 2011, Eisbruch et al., 2010 and Lee et al., 2009). IMRT has reduced tumour volumes in locally recently developed non–small cell lung cancer, proctitis in prostate cancer, and xerostomia in head and neck cancer (Paulino, 2016).
Lockney et al. (2011) found that latent toxicities were recurring even with the use of IMRT. Three-fourths of the patients developed facial disfigurement, while one-third developed growth hormone deficiency, dental problems, or cataracts. No secondary malignant solid tumours occurred, however one patient developed acute myeloid leukemia and another had myelodysplastic syndrome. It has been reported that IMRT is beneficial in children with other types of tumours. Grade 3 and 4 ototoxicity in medulloblastoma incidence has been reduced from 64% using 2D radiotherapy and 25% with IMRT (Paulino et al., 2010).
Hypothesis:
Null hypothesis H0: Proton Beam therapy (PBT) and Intensity-Modulated radiation therapy (IMRT) are both
equally effective in the treatment of prostate cancer (PC).
Alternative Hypothesis
H1: Proton Beam therapy (PBT) is a better treatment for prostate cancer in comparison to
Intensity-Modulated radiation therapy (IMRT).
Page 16 of 40

Aim: To identify which has greater toxicity and side effects by means of therapy between PBT and IMRT in the treatment of prostate cancer (PC).
MethodologyThis study was performed using meta-analysis which involved an in depth study and analysis
of data from journals and articles in association between the proton beam therapy (PBT) and intensity-modulated radiation therapy (IMRT) in the treatment of prostate cancer.
Data sources
The strategy employed to performed the meta-analysis project is through scientific websites
containing database of peer reviewed journals and articles from certified scientific websites
containing database of
• PubMed
• British Journal of Cancer
• Japanese Journal of Clinical Oncology
• International Journal of Radiation Oncology
• Radiology
• Iranian Journal of Cancer Prevention
• Acta Oncologica
• The British Journal of Radiology
• Cancer Research UK
• Cancer Biology & Therapy
• PLOS One
• Oncogene
• Current Drug Metabolism
• Cell
Page 17 of 40

• Nature
• Current Opinion in Clinical Nutrition and Metabolic Care
• Molecular Cancer
• Science Translational Medicine
• The Ochsner Journal
• La radiologia medica (Radiol Med)
• Health Physics
• The New England Journal of Medicine (NEJM)
• Oxford University Press (Journals)
• The Journal of Clinical Endocrinology & Metabolism
• Journal of the European Society for Medical Oncology
• Journal of the National Cancer Institute
• Journal of Clinical Oncology
• The Journal of Radiation Research
• Systematic Reviews
• Physics in Medicine and Biology
• Radiotherapy & Oncology
• Cancer Medicine
• Cancer
• Reviews in Urology
• Radiation Research
• Wiley Online Library
• The Lancet Oncology
• PharmacoEconomics & Outcomes News
• Journal of Proton Therapy (JPT)
• JAMA
• World Health Organisation (WHO)
Criteria of selection
The method of journal extraction in order to identify the eligibility criteria of articles and
journals is according to the aim of the study. Through the use of inclusion and exclusion, it
Page 18 of 40

helped determine whether the journals containing the information are of great significance
and are vital to achieve the aim that the study has undertaken. It is paramount that each
journals and articles are reliable and credible as this would affect the fate of the results by
adhering to the ‘checklist’ below presented in bullet points. By creating a standardised form
for data collection, it created a structure for the research of journal extraction organised,
straightforward and time efficient. The standardised form that were executed is a tabulated
spreadsheet which contained various segments: authors, publication year, and journal title
and journal website link. Carefully chosen search terms are also used for specificity of
journals and articles such as proton beam therapy (PBT).
By creating a list of how the data or information are selected, it generated a constructed plan
in the selection of suitable materials and data for the project as demonstrated below:
• Journals on cancer in general.
• All the journals on prostate cancer.
• Recent journals within past 10 yrs.
• Journals on Proton Beam Therapy
• Journals on Intensity Modulated Radiation therapy (IMRT)
• Journals with cost of PBT and IMRT
• Journals on cancers treated by PBT
• Journals including countries offering proton therapy
• Journals on toxicity of radiotherapy
• Journals on side effects and risks of PBT and IMRT
• Journals on the efficiency of PBT and IMRT
• Journals linking PBT and/or IMRT in the treatment of prostate cancer.• Journals on the epidemiology of individuals affected by cancer, in particular PC
The search terms included : PBT and/or proton beam therapy, IMRT and/or intensity-modulated radiation therapy, radiotherapy, proton therapy, photon therapy, x-rays,
radiation to cure cancer, prostate cancer, risks of radiation exposure, cancer,
The statistical analysis used was Forest plot and the effect size chosen are relative risk (RR).
The relative risk is chosen as effect size due to the four articles which provided similar RR
values which is easier to calculate and present. The forest plot was chosen to present the data
Page 19 of 40

from the four articles as it provided graphical representation of a meta-analysis including the
list of the authors and date providing detailed and simple presentation of data found. T-test
were also used to compare the effectiveness of PBT and IMRT treatments and whether to
reject or accept the null hypothesis and/or alternative hypothesis. The error bars
are used to indicate uncertainty of the measurement and they provide precise
measurement for reliable and valid data.
Results
Page 20 of 40
Figure 6. A forest plot showing that the treatment Proton Beam therapy is safer therefore, more effective in treating Prostate
Cancer compared to Photon Radiotherapy from four clinical trials from 2012 - 2014. The overall effect estimate is 1.06, therefore
. The boxes from each line represents the effect estimate and weight for each study.
= 73.1%.
Individuals studies by Sheets et al. (2012) and Yu et al. (2012) does not overlap 1, therefore has statistical significance however
the studies by Fang et al. (2014) overlaps 1, therefore therefore no statistical significance.
PBT
IMRT
PBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBTPBT
IMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRTIMRT

Figure 7. T-test of the
effectiveness of PBT and IMRT is used
Page 21 of 40
Figure 9. Shows the four studies used to generate a forest plot (Fig.6) with weight, odds ratio (OR), upper confidence and
patient population value using Evidence Partners which is a Systematic Review and Literature Review Software .

to show similar or different variability between scores. From the result of Levene’s Test for Equality of Variances it shows that p < 0.05 therefore the two treatments have unequal variances or significantly difference. The Sig (2-Tailed) value is 0.463 therefore no statistically significant differences between means of the two
treatments. Therefore, the null hypothesis is rejected as there is no difference in the variances between groups.
Table 1. Comparison of PBT and IMRT on morbidity and disease control in localised PC, patterns of care and early toxicity and two case matched with N value, group value, outcome, standard error (SE) value, variance and weight value in different columns.
Title N group Outcome- Standard error
(SE)
Variance Weight
Intensity-Modulated
Radiation Therapy, Proton
Therapy, or Conformal
Radiation Therapy and
Morbidity and Disease
Control in Localized Prostate
Cancer. 12976 1368 0.105 0.0028 0.001 123082.292
Page 22 of 40
Figure 8a and 8b. Error bar graphs representing mean ±2 SE intervals and the 95% confidence
intervals. The standard error (SE) bars overlap graph 8a and 8b, therefore the difference between the
two means is not statistically significant (P>0.05).
*N = 2, T = -0.899, N = 2, P = 0.163 for IMRT and 0.522 for PBT.
8a 8b

Proton Versus Intensity-
Modulated Radiotherapy for
Prostate Cancer: Patterns of
Care and Early Toxicity 27647 553 0.02 0.001 0.001
1382200.01
6
A case-matched study of
toxicity outcomes after
proton therapy and
intensity-modulated
radiation therapy for
prostate cancer 394 213 0.541 0.037 0.001 728.807
A case-matched study of
toxicity outcomes after
proton therapy and
intensity-modulated
radiation therapy for
prostate cancer 394 181 0.459 0.034 0.001 857.657
Efficacy using PBT & IMRT
P.B.T has a significantly reduced radiation dose drop-off in adjacent tissue. Trofimov et al, (2007) established the delivery dose range to be 68 – 79 GCE (Cobalt Gray Equivalent) for P.B.T in contrast to 35 – 59 GY dose for I.M.R.T. This is further confirmed by the Bragg peak. Based on this evidence and further information presented by (FIGURE?) the N.H.S, should strongly consider the application of this therapy in the U.K.
The 95% CI show no significant trend. However, there is a statistically significant difference in the variability scale between I.M.R.T and P.B.T, meaning that the recurrence rate for I.M.R.T is significantly higher than for P.B.T. This is supported by the clinical trials conducted via the National Association for Proton Therapy, (2014). showing that 97% of patients with prostate cancer displayed no signs of recurrence. This is a significant result which should be highly considered by the N.H.S. Table one highlight key points regarding the treatment of prostate cancer using PBT and IMRT.
Page 23 of 40

Discussion
The result gathered from Figures 6, 7 and 8 showed no statistically difference when
comparing PBT and IMRT treatment for prostate cancer (PC) therefore it agrees with the null
hypothesis (H0) which stated that proton beam therapy (PBT) and intensity-modulated
radiation therapy (IMRT) are both equally effective in the treatment of prostate cancer (PC).
However, Fig. 6 presented that the treatment PBT is favoured by the four studies in
comparison to IMRT. This in effect agrees with the alternative hypothesis which states that
PBT is a better treatment compared to IMRT.
In general, radiation treatment may cause damage to the organs adjacent to the prostate which
can lead to long term urinary and gastrointestinal morbidity, hip fractures and erectile
dysfunction. There are data in the past 10 years which demonstrated that long term risk of
morbidity is directly linked with the radiation dose received by each organ (Michalski et al.,
2010, Roach et al., 2010 and Fiorino et al., 2009). Hence, the development of dose guidelines
for rectum and bowel, bladder and femoral heads which are widely used and standard
operating procedure of radiation treatment (Sheets et al., 2012). In addition, there are no
consistent association found between radiation dose and structure and erectile dysfunction
therefore dose guidelines is not developed (Roach et al., 2010).
The study by Sheets et al. (2012) found no significant difference in PBT and IMRT treated
patients in incontinence diagnoses, hip fractures and erectile dysfunction. There were no
statistically significant difference in the gastrointestinal and other toxicity found between
PRT and IMRT post treatment of 6 or 12 months. Previous studies found that the distribution
of radiation dose is improved in PBT compared with IMRT whereby the amount of bladder
exposed to low and intermediated levels of radiation is reduced (Trofimov et al., 2007 and
Mock et al., 2005). Early toxicity is predicted by the amount of low doses to which the
bladder is exposed to (Karlsdottir et al., 2004). Also, the radiation reduced to the bladder may
be accountable for the temporary improvement in 6 months toxicity with PRT/PBT. In
addition, PBT treated patients have higher chance of being diagnosed of gastrointestinal
related disease and undergo for the disease related procedure. Another recent study also
Page 24 of 40

found higher gastrointestinal morbidity rates in PBT treated patients (Kim et al., 2011)
relative to IMRT patients. Studies by Sheets et al. (2012) and Kim et al. (2011) noted a
statistically significant reduction of gastrointestinal toxicity for patients undergoing IMRT
compared with PBT. This may be due to the higher vulnerability to organ movement of PBT
which can lead to unintended higher dose to the rectum in comparison to IMRT. It is
unknown whether greater image guidance may reduce gastrointestinal morbidity (Sheets et
al., 2012). On the other hand, patients receiving IMRT are less likely to be diagnosed of
gastrointestinal morbidity, hip fracture and less likely
to receive additional cancer therapy, however more
likely to receive diagnosis of erectile dysfunction.
Figure 9. Rates of the probability of additional
treatment in cancer patients months after
treatment of Intensity-Modulated Radiation
Therapy vs Proton Therapy (Sheets et al., 2012).
Furthermore, there is only a small association in the
reduction of genitourinary toxicity at 6 months post-
treatment of patients that received PRT (PBT)
compared to IMRT, however at 12 months no difference were found (Fig. 9). Although
overall, the rates of additional cancer therapy showed no statistical differences between the
two comparative treatments (Fig. 9). In Fig. 6, Fang et al. (2014) found no statistical
difference between PBT and IMRT using the variables late clinical gastrointestinal (GI) and
genitourinary (GU) toxicities in patients with prostate cancer who received PBT versus
IMRT. Although this study measured two particular variables in comparison to the three
studies that were used in the forest plot, Fang et al., (2014) found no GI and GU toxicity by
comparing PBT and IMRT.
The probability of additional treatment of IMRT and PBT is similar after 38 months, however
the probability of additional treatment begins to dramatically increase after 40 months of
IMRT. A high peak of the probability of additional treatment after IMRT occurs within 5
years onwards compared to PBT which remains constant (Fig. 9). Therefore, recurrence of
PC is higher in IMRT than PBT. This is further supported by Fig. 6 which ultimately favored
PBT treatment to IMRT.
Page 25 of 40

Currently, the lack of data regarding on the patterns of use and actual cost of PBT hinders its
development and application. However, PBT slowly disseminating and as a result there are
now nine PRT centers in place in the United states and Table 2. shows countries which
currently provided proton therapy.
The study by Yu, et.al. (2012) has some limitations such as the lack of few patient-reported
outcome data and treatment-related information, no knowledge regarding the radiation dose
and field size where IMRT patients may have received higher radiation dose which could
provide an explanation in the observed increase in 6-month toxicity. It is important that a
longitudinal study regarding comparison of both treatments should take place before
widespread application of PRT/PBT for further justification in the treatment of prostate
cancer (Yu et.al., 2012).
There are new postulated treatments for treating prostate cancer which is convincing such as
minimally invasive prostatectomy and IMRT. However, the lack of data comparing new
against older treatment outcomes proves it difficult for the development of the newer
treatments (Sheets et al., 2012). Despite the high-cost prostate cancer treatment and the high
profile of proton therapy, there have been an increased in the development of building
multiple proton facilities in which direct-to-consumer advertising is likely to lead to a large
increase in its utilization (Schippers et al.,2011 and Institute for Clinical and Economic
Review, 2007).
PBT & IMRT toxicity
The side effects observed were gastro-intestinal(GI) and gastro-urinary(GU) morbidity, erectile
dysfunction, and hip fractures (Sheets, et.al.,2012) (Yu, et.al., 2012) (Fang, et.al., 2014). Both IMRT
and PBT showed these complications. Taking all the variables in consideration, Fang, et al., 2014, test
showed no significant differences of number of patients suffering from acute GI nor GU toxicity with
patients after treated with PBT or IMRT for PC. Fang, et al,. 2014 also proved there is the same risk
of late GI and GU toxicity in patients going through PBT and IMRT, taking all variables in
consideration, PBT did show a minute decline of other complications, the findings on toxicity was
compared with cost from reimbursement per patient and PBT was 1.7 times that of IMRT. (Yu, et.al.,
2012). Sheets et al (2012) results also showed roughly the same number of complications and stated
“The potential advantage of proton therapy compared with IMRT is unclear.”
As aforementioned, the various side effects can immediately appear and some can occur
latent or later in life without the patient’s knowledge. Histologically, radiation-induced
tumour shows differently in comparison to the existing disease. The typical latent stage for a
Page 26 of 40

radiation-associated tumour is several years and cancer patient survivors remain at an
increased risk of developing secondary malignancies even after 30—40 years after initial
radiation treatment Chaturvedi et al. 2007). Minniti et al. (2005) and Kuttesch et al. (1996)
performed an over 25 year follow up and estimated that the cumulative risk of radiation
therapy is 2–11% in patients. There is a possibility of increased risk after ~10 year of other
tumour types such as non-Hodgkin’s lymphoma and acute nonlymphomatic leukemia and
others has even higher risk of more than 20 years after radiation therapy (Foss Abrahamsen et
al. 2002). Therefore, latency stage may not possibly exceed paediatric patients’ life
expectancy in particular. Younger patients are of more increasing concern of developing
second malignancies ((Neglia et al. 2006 and Ron, 2006). An ongoing institutional
retrospective study, The Childhood Cancer Survivor Study presented over 14,000 cases
(Bassal et al. 2006; Ronckers et al. 2006 and Armstrong et al. 2010, 2011). In addition, the
use of photon treatment led to significant side effects such as the high risk of cardiac disease
in women which account to 43% higher than the general population and radiation
pneumonitis (Lundkvist et al., 2005 and Rutqvist et al., 2003).
The dose-response relationship in irradiating prostate cancer have previously been reported
with a higher dose >70 Gy (SI unit of absorbed radiation) had shown potential benefit for
prostate cancer (Perez et al., 1980, Hanks et al., 1988 and Schiller et al., 2016). However,
other studies revealed that conventional radiotherapy techniques drastically increased rectal
complications at >70 Gy (Pilepich et al., 1987, Hanks, 1988 and Schiller et al., 2016). This
type of technique which aim to eradicate prostate cancer pivoted its clinical use to the
development of numerous techniques which became widespread such as intensity-modulated
radiotherapy (IMRT), three-dimensional conformal radiotherapy (3D-CRT), brachytherapy
and charged particle therapy (heavy ion and proton). These different techniques enable
adequate target dose coverage with minimal dose to the normal tissues surrounding the
tumour tissues with improved tumour control with adequate toxicity (Nihei et al., 2005).
Currently, PBT uses three-dimensional conformal techniques (3D-CPT) to deliver the
radiation via passive beam scattering method (Main, 2016). Several institutions have
gradually introduced proton pencil beam scanning (PBS) technique which allows intensity-
modulated proton therapy (IMPT) delivery which potentially improve target conformity and
spare adjacent normal tissues (Clasie et al. 2012). Also, morbidity may be prolonged after
radiation treatment (Slater et al., 1998). PBT have been recognized to have reduced side
effects in comparison with photon therapy. However, it is expensive, higher cost of therapy
facilities and maintenance remain as a concern for its utilization.
Page 27 of 40

Costs of PBT & IMRT
Outpatient setting is the only way of receiving PBT meaning the only way of means of treat-
ment is private institutions located in certain areas for exam and does not involve hospital ad-
mittance. A high capital investment is needed for the construction of a proton facility, and a
large area is needed for the size of the facility (Reza, et.al., 2015). The average cost of a PBT
course not including time spent and commuting cost stands at an average of £90,000 and esti-
mated cost for a IMRT course stands at £10,200 (NHS Private Patient Tariff, 2012; Zelefsky,
et.al., 2006). IMRT is covered by most insurance providers and it should also be noted that
insurance provider may not have PBT covered and if they do, patients will still need to pay a
significant amount. Reiazi et al. (2015) concluded that proton therapy in particular to treat
breast cancer could be cost-effective with appropriate risk groups as targets and is effective in
the reduction of future risk recurrence.
The availability of PBT around the world is minute and in the UK is only 2 locations and the
cost for patients commuting and total time spent, is a disadvantage. Were as IMRT is widely
available in most areas in the United Kingdom. As of February 2016, there are 58 medical
centers that offer PBT worldwide, of which none of them are based in the United Kingdom.
There has been a £250 million investment done on 2 new centers to be established in the
United Kingdom by the government, that are planned to open in 2018 at the Christie Hospital
NHS Foundation Trust in Manchester and University College London Hospitals NHS Foun-
dation Trust.
Table 2: Examples of randomly chosen countries, which have established medical
centers that currently offer proton therapy.
Country Who, Where Start of Treatment
USA, CA J. Slater PTC, Loma Linda 1990
France CPO, Orsay 1991
Japan NCC, Kashiwa 1998
Germany HZB, Berlin 1998
Russia JINR 2, Dubna 1999
Italy CNAO, Pavia 2011
Page 28 of 40

Czech Republic PTC Czech r.s.o., Prague 2012
Cancers Treated with PBT
PBT has shown to be successful in the treatment of prostate cancer but not all cancers can be
treated. Proton therapy is useful for treating tumours that have not spread and for tumours
near important parts of the body, such as the eye, the brain, and the spinal cord. It is also used
for treating children, because it lessens the chance of harming healthy, developing tissue,
such as retinoblastoma and orbital rhabdomyosarcoma.
Proton Beam therapy can be used to treat these cancers:
Central nervous system cancers, including chordoma, chondrosarcoma, and malignant
meningioma. (Suneja G, 2013)(Elnahal SM, 2013)
Eye cancer, including uveal melanoma or choroidal melanoma (Bensoussan E, 2016)
(Sikuade MJ, 2010)
Head and neck cancers, including tongue and paranasal sinus cancer and some
nasopharyngeal cancers (Takayama K, 2016)(Ishikawa H, 2015)
Lung cancer (Parikh RR, 2016) (Ishikawa Y, 2016)
Liver cancer (Muroi H, 2015) (Kim S, 2011)
Spinal and pelvic sarcomas, which are cancers that occur in the soft-tissue and bone
(Soldatos T, 2013)
Noncancerous brain tumors (Verma V, 2016)
Future of Proton beam therapy
The idea that proton beam therapy would revolutionize the treatment of cancer, was firstly
predicted by the American physicist Robert R. Wilson in 1946, who performed extensive
research using proton beam therapy technology. Despite the high costs involved in
developing a proton center and the high costs of treatment using PBT, its efficacy treating
prostate cancer has been highly significant and a major point in further developing the
technology. With the steady rise of prostate cancer worldwide, the need for developing this
technology has been substantially high. Despite its high costs, it has been clear to be
beneficial in the long term in the treatment of cancer, as it has shown to be highly more
effective than the latest photon based therapy the, IMRT. Having said that, PBT is not only
helping in the treatment of patients, improving their 5year survival rate but it is also helping
reshape the economy and the N.H.S. Although theoretically PBT has been seen to cause less
Page 29 of 40

damage to normal tissue surrounding the area of focus. Studies continue to be conducted in
order to evaluate the outcomes between the different modalities, with identification of the
appropriate therapy for different kinds of cancer. Furthermore, the main focus of the N.H.S is
to establish P.B.T as a primary form of treatment for advanced stages of cancer. It has been
speculated to be a standardized form of treatment by 2018.
Conclusion
In conclusion, it is unclear whether proton beam therapy has potential advantage in compari-
son to IMRT. Studies on radiation planning demonstrated that PBT relative to IMRT may
significantly reduce the section of each neighboring organ that receives low radiation doses.
However PBT may be more susceptible to errors related to daily patient positioning, setup
and the movement of the organ during treatment procedure. The relative reimbursement of
new medical technologies needs to be considered carefully so that physicians and hospitals
do not have a financial incentive to adopt a technology before supporting evidence is avail-
able. PBT is very expensive procedure, but evidence does show of its popularity increasing
and new technologies will be introduced to make it less cost effective. PBT and IMRT have
equally shown to work well against prostate cancer, but by reducing the reoccurrence or side
effects because of the therapy, even by a small figure is a step forward for the fight against
cancer. On this basis all governments and private medical centers should invest, for the con-
struction of proton facilities.
Acknowledgement
I would strongly like to thank Don Keiller for the guidance, motivation and encouragement I needed
to finish my thesis.
References
Anon, 2007. Proton beam therapy poor value for prostate cancer. PharmacoEconomics & Outcomes News, &NA;(538), p.9. [Accessed 8 Aug. 2016].
Page 30 of 40

Anon, 2015. Prostate cancer statistics. [online] Cancer Research UK. Available at:
<http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-
cancer-type/prostate-cancer heading-Zero> [Accessed 8 Aug. 2016].
Archambeau JO, Bennett GW, Levine GS, Cowen R, Akanuma A. 1974. Proton radiation
therapy. Radiology;110:445–57.
http://pubs.rsna.org/doi/abs/10.1148/110.2.445[Accessed 8 Aug. 2016].
Armstrong GT, Liu W, Leisenring W, Yasui Y, Hammond S, Bhatia S, Neglia JP, Stovall
M, Srivastava D, Robison LL. Occurrence of multiple subsequent neoplasms in long-term
survivors of childhood cancer: a report from the childhood cancer survivor study. J Clin
Oncol. 2011;29:3056–3064. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3157966/
[Accessed 8 Aug. 2016].
Armstrong GT, Stovall M, Robison LL. Long-term effects of radiation exposure among
adult survivors of childhood cancer: results from the childhood cancer survivor study.
Radiat Res. 2010;174:840–850. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3080029/
[Accessed 8 Aug. 2016].
Bassal M, Mertens AC, Taylor L, Neglia JP, Greffe BS, Hammond S, Ronckers CM,
Friedman DL, Stovall M, Yasui YY, Robison LL, Meadows AT, Kadan-Lottick NS. Risk
of selected subsequent carcinomas in survivors of childhood cancer: a report from the
Childhood Cancer Survivor Study. J Clin Oncol. 2006;24:476–483.
http://jco.ascopubs.org/content/24/3/476.long [Accessed 8 Aug. 2016].
Bensoussan E, e., 2016. Outcomes After Proton Beam Therapy for Large Choroidal
Melanomas in 492 Patients. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/26940166> [Accessed 6 Jul. 2016].
Caroline MainEmail authorView ORCID ID profile, Madhumita Dandapani, Mark
Pritchard, Rachel Dodds, Simon P. Stevens, Nicky Thorp, Roger E. Taylor, Keith
Wheatley, Barry Pizer, Matthew Morrall, Robert Phillips, Martin English, Pamela R.
Kearns, Sophie Wilne and Jayne S. Wilson.
http://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-016-0285-6
[Accessed 8 Aug. 2016].
Chaturvedi AK, Engels EA, Gilbert ES, Chen BE, Storm H, Lynch CF, Hall P, Langmark
F, Pukkala E, Kaijser M, Andersson M, Fosså SD, Joensuu H, Boice JD, Kleinerman RA,
Page 31 of 40

Travis LB.Second cancers among 104,760 survivors of cervical cancer: evaluation of
long-term risk. http://jnci.oxfordjournals.org/cgi/pmidlookup?
view=long&pmid=17971527
Cheng, C., Liu, H. and Lee, S., 2016. Spot scanning with a rapid cycling proton beam: Dose delivery algorithms. Jour Proton Ther, 2(1), p.211.
Chiappiniello, A., Fulcheri, C. and Tarducci, R. (2016). The role of Pinnacle3 scripting in
streamlining IMRT and 3D-CRT treatment planning. Physica Medica, 32, p.11.
Childhood cancer--treatment at a cost. Ron E. J Natl Cancer Inst. 2006 Nov 1;
98(21):1510-1.http://jnci.oxfordjournals.org/content/98/21/1510.long
Clasie, B., Depauw, N., Fransen, M., Gomà, C., Panahandeh, H. R., Seco, J., … Kooy, H.
M. (2012). Golden Beam Data for Proton Pencil Beam Scanning. Physics in Medicine
and Biology, 57(5), 1147–1158. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3387676/
Costello, L. and Franklin, R., 2014. The status of zinc in the development of
hepatocellular cancer. Cancer Biology & Therapy, 15(4), pp.353-360. [Accessed 8 Aug.
2016].
Diallo I, Haddy N, Adjadj E, Samand A, Quiniou E, Chavaudra J, Alziar I, Perret N,
Guérin S, Lefkopoulos D, de Vathaire F. Int J Radiat Oncol Biol Phys. 2009 Jul 1;
74(3):876-83. Abstract only.
http://www.redjournal.org/article/S0360-3016(09)00136-9/abstract
Eisbruch, A., Harris, J., Garden, A. S., Chao, C. K., Straube, W., Harari, P. M., … Ang,
K. K. (2010). Multi-institutional Trial of Accelerated Hypofractionated Intensity-
Modulated Radiation Therapy for Early Stage Oropharyngeal Cancer (RTOG 00-22).
International Journal of Radiation Oncology, Biology, Physics, 76(5), 1333–1338.
http://www.ncbi.nlm.nih.gov/pubmed/19540060
Elnahal SM, e., 2013. Proton beam therapy and accountable care: the challenges ahead. -
PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/23265572> [Accessed 6 Jul. 2016].
Focaccetti, C., Bruno, A., Magnani, E., Bartolini, D., Principi, E., Dallaglio, K., Bucci, E.,
Finzi, G., Sessa, F., Noonan, D. and Albini, A., 2015. Effects of 5-Fluorouracil on
Morphology, Cell Cycle, Proliferation, Apoptosis, Autophagy and ROS Production in
Page 32 of 40

Endothelial Cells and Cardiomyocytes. PLOS One, 10(2), pp.1-5. [Accessed: 8 Aug,
2016]
Foss Abrahamsen A, Andersen A, Nome O, Jacobsen AB, Holte H, Foss Abrahamsen J,
Kvaloy S. Long-term risk of second malignancy after treatment of Hodgkin’s disease: the
influence of treatment, age and follow-up time. Ann Oncol. 2002;13:1786–1791.
http://annonc.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=12419752
Fulda, S. and Debatin, K., 2006. Extrinsic versus intrinsic apoptosis pathways in
anticancer chemotherapy. Oncogene, 25(34), pp.4798-4811. [Accessed: 8 Aug, 2016]
G.E. Hanks, M.D.correspondencePress enter key for correspondence information, K.L.
Martz, M.S., J.J. Diamond, Ph.D., 1988. The effect of dose on local control of prostate
cancer. International Journal of Radiation Oncology. Available
at:<http://www.redjournal.org/article/0360-3016(88)90224-6/abstract>
Gagliardi G1, Lax I, Ottolenghi A, Rutqvist LE. 1996 Long-term cardiac mortality after
radiotherapy of breast cancer--application of the relative seriality model. Br J Radiol.
http://www.ncbi.nlm.nih.gov/pubmed/8983588
Ghosh, P., Malik, S., Bedolla, R. and Kreisberg, J., 2003. Akt in Prostate Cancer: Possible
Role in Androgen-Independence. Current Drug Metabolism, 4(6), pp.487-496. [Accessed
8 Aug. 2016].
Grivennikov, S., Greten, F. and Karin, M., 2010. Immunity, Inflammation, and Cancer.
Cell, 140(6), pp.883-899. [Accessed: 8 Aug, 2016]
Gundem, G., Van Loo, P., Kremeyer, B., Alexandrov, L., Tubio, J., Papaemmanuil, E.,
Brewer, D., Kallio, H., Högnäs, G., Annala, M., Kivinummi, K., Goody, V., Latimer, C.,
O'Meara, S., Dawson, K., Isaacs, W., Emmert-Buck, M., Nykter, M., Foster, C., Kote-
Jarai, Z., Easton, D., Whitaker, H., Neal, D., Cooper, C., Eeles, R., Visakorpi, T.,
Campbell, P., McDermott, U., Wedge, D. and Bova, G., 2015. The evolutionary history
of lethal metastatic prostate cancer. Nature, 520 (7547), pp.353-357. [Accessed 8 Aug.
2016].
Habl G, Debus J. There is evidence for the superiority of protons and heavy ions, pro
radiotherapy in prostate cancer. Abstract only. Med Radiol (2014) 2015:277–89.
http://link.springer.com/chapter/10.1007%2F174_2014_972
Page 33 of 40

Hepatogastroenterology. 1990 Jul;37 Suppl 1:31-5. Neurochemical control of oxyntic cell secretion. Black JW1. http://www.ncbi.nlm.nih.gov/pubmed/1976585
hj5
Ho, E. and Song, Y., 2009. Zinc and prostatic cancer. Current Opinion in Clinical
Nutrition and Metabolic Care, 12(6), pp.640-645. [Accessed 8 Aug. 2016].
Hoesel, B. and Schmid, J., 2013. The complexity of NF-κB signaling in inflammation and
cancer. Molecular Cancer, 12(1), pp.86. [Accessed: April 24, 2016]
Improved survival using intensity-modulated radiation therapy in head and neck cancers:
A SEER-Medicare analysis. Beth M. Beadle MD, PhD,Kai-Ping Liao PhD,Linda S.
Elting DrPH,Thomas A. Buchholz MD,K. Kian Ang MD, PhD, Adam S. Garden MD, B.
Ashleigh Guadagnolo MD, MPH. 2014.
http://onlinelibrary.wiley.com/doi/10.1002/cncr.28372/full
Institute for Clinical and Economic Review. Intensity Modulated Radiation Therapy
(IMRT) for Localized Prostate Cancer. Final Appraisal Document. Boston, MA: Institute
for Clinical and Economic Review; 2007.
Int J Radiat Oncol Biol Phys. 2009 Nov 15;75(4):1084-91. doi:
10.1016/j.ijrobp.2008.12.052. Epub 2009 Mar 26. Risk factors and dose-effect
relationship for mandibular osteoradionecrosis in oral and oropharyngeal cancer patients.
Lee IJ1, Koom WS, Lee CG, Kim YB, Yoo SW, Keum KC, Kim GE, Choi EC, Cha IH.
http://www.ncbi.nlm.nih.gov/pubmed/19327914
Int J Radiat Oncol Biol Phys. 2010 Dec 1;78(5):1445-50. doi: 10.1016/j.ijrobp.2009.09.031. Epub 2010 Mar 16. Ototoxicity after intensity-modulated radiation therapy and cisplatin-based chemotherapy in children with medulloblastoma. Paulino AC1, Lobo M, Teh BS, Okcu MF, South M, Butler EB, Su J, Chintagumpala M. http://www.ncbi.nlm.nih.gov/pubmed/20231075
Intensity-modulated proton beam therapy (IMPT) versus intensity-modulated photon
therapy (IMRT) for patients with oropharynx cancer – A case matched analysis
Intensity-Modulated Radiation Therapy. Thomas E. Goffman and Eli Glatstein. Radiation
Research. Vol. 158, No. 1 (Jul., 2002), pp. 115-117. http://www.jstor.org/stable/3580704?
seq=1#page_scan_tab_contents
Page 34 of 40

Ishikawa H, e., 2016. Proton beam therapy combined with concurrent chemotherapy for
esophageal cancer. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/25750339> [Accessed 7 Jul. 2016].
Ishikawa Y, e., 2016. Dosemetric Parameters Predictive of Rib Fractures after Proton
Beam Therapy for Early-Stage Lung Cancer. - PubMed - NCBI. [online]
Ncbi.nlm.nih.gov. Available at: <http://www.ncbi.nlm.nih.gov/pubmed/27087118>
[Accessed 26 Aug. 2016].
Jones, B., 2016. Proton beam therapy for medulloblastoma. The Lancet Oncology, 17(5), p.e173.
Karlsdottir A, Johannessen DC, Muren LP, Wentzel-Larsen T, Dahl O. Acute morbidity
related to treatment volume during 3D-conformal radiation therapy for prostate cancer.
Radiother Oncol. 2004;71(1):43–53. http://www.thegreenjournal.com/article/S0167-
8140(04)00049-0/abstract
Kim S, e., 2011. Secondary radiation doses of intensity-modulated radiotherapy and
proton beam therapy in patients with lung and liver cancer. - PubMed - NCBI. [online]
Ncbi.nlm.nih.gov. Available at: <http://www.ncbi.nlm.nih.gov/pubmed/21339011>
[Accessed 14 Aug. 2016].
Kim, S., Shen, S., Moore, D. F., Shih, W., Lin, Y., Li, H., … Lu-Yao, G. L. (2011). Late Gastrointestinal Toxicities Following Radiation Therapy for Prostate Cancer. European Urology, 60(5), 908–916. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3185133/
Kuttesch JF Jr, Wexler LH, Marcus RB, Fairclough D, Weaver-McClure L, White M,
Mao L, Delaney TF, Pratt CB, Horowitz ME, Kun LE. J Clin Oncol. 1996 Oct;
14(10):2818-25. http://www.ncbi.nlm.nih.gov/pubmed/8874344/
Levin, W.P., Kooy, H., Loeffler, J.S. and DeLaney, T.F., 2005. Proton beam therapy.
British Journal of Cancer, [online] Available
at:<http://www.nature.com/bjc/journal/v93/n8/full/6602754a.html> [Accessed 22 July
2016].
Liauw, S., Connell, P. and Weichselbaum, R., 2013. New Paradigms and Future
Challenges in Radiation Oncology: An Update of Biological Targets and Technology.
Science Translational Medicine, 5(173), pp.173-174. [Accessed 8 Aug. 2016].
Page 35 of 40

Lundkvist J, Ekman M, Ericsson SR, Jonsson B, Glimelius B. Proton therapy of cancer:
potential clinical advantages and cost-effectiveness. Acta Oncol. 2005;44(8):850–61.
http://www.tandfonline.com/doi/pdf/10.1080/02841860500341157
Maddock, P.G. 2006, "INTENSITY MODULATED RADIATION THERAPY", Medicine and
Health Rhode Island, vol. 89, no. 2, pp. 76-8. http://search.proquest.com/docview/195808173?
accountid=8318&rfr_id=info%3Axri%2Fsid%3Aprimo> [Accessed 11 May 2016].
Michalski JM, Winter K, Purdy JA, Wilder RB, Perez CA, Roach M III, et al. Preliminary
evaluation of low-grade toxicity with conformal radiation therapy for prostate cancer on
RTOG 9406 dose level I and II. Int J Radiat Oncol Biol Phys 2003;56:192–8.
http://www.ncbi.nlm.nih.gov/pubmed/12694838?dopt=Abstract
Michalski, J. M., Gay, H., Jackson, A., Tucker, S. L., & Deasy, J. O. (2010). RADIATION DOSE–VOLUME EFFECTS IN RADIATION-INDUCED RECTAL INJURY. International Journal of Radiation Oncology, Biology, Physics, 76(3 Suppl), S123–S129. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3319467/
Mizumoto, M., Murayama, S., Akimoto, T., Demizu, Y., Fukushima, T., Ishida, Y., …
Sakurai, H. (2016). Proton beam therapy for pediatric malignancies: a retrospective
observational multicenter study in Japan. Cancer Medicine, 5(7), 1519–1525.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4867672/
Mock U, Bogner J, Georg D, Auberger T, Potter R. Comparative treatment planning on
localized prostate carcinoma conformal photon- versus proton-based radiotherapy.
Strahlenther Onkol.. 2005; 181(7):448–
455.http://link.springer.com/article/10.1007%2Fs00066-005-1317-7
Muroi H, e., 2015. Effectiveness of proton beam therapy on liver metastases of
esophageal cancer: report of a case. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov.
Available at: <http://www.ncbi.nlm.nih.gov/pubmed/25594660> [Accessed 14 Aug.
2016].
Neglia JP, Robison LL, Stovall M, Liu Y, Packer RJ, Hammond S, Yasui Y, Kasper CE,
Mertens AC, Donaldson SS, Meadows AT, Inskip PD. New primary neoplasms of the
central nervous system in survivors of childhood cancer: a report from the Childhood
Cancer Survivor Study. J Natl Cancer Inst. 2006;98:1528–1537.
http://jnci.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=17077355
Page 36 of 40

Newhauser, W. D., Giebeler, A., Langen, K. M., Mirkovic, D., & Mohan, R. (2008). Can
megavoltage computed tomography reduce proton range uncertainties in treatment plans for
patients with large metal implants? Physics in Medicine and Biology, 53(9), 2327–2344.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4120878/
Nihei, K., Ogino, T., Ishikura, S., Kawashima, M., Nishimura, H., Arahira S and
Onozawa, M., 2005. Phase II Feasibility Study of High-Dose Radiotherapy for Prostate
Cancer Using Proton Boost Therapy: First Clinical Trial of Proton Beam Therapy for
Prostate Cancer in Japan. Japanese Journal of Clinical Oncology, [online] Available
at:<http://jjco.oxfordjournals.org/content/35/12/745.long> [Accessed 22 July 2016].
Nutting, C. M., Morden, J. P., Harrington, K. J., Urbano, T. G., Bhide, S. A., Clark, C.,
… on behalf of the PARSPORT trial management group. (2011). Parotid-sparing
intensity modulated versus conventional radiotherapy in head and neck cancer
(PARSPORT): a phase 3 multicentre randomised controlled trial. The Lancet Oncology,
12(2), 127–136. http://www.ncbi.nlm.nih.gov/pubmed/21236730
Paganetti, H. (2012). ASSESSMENT OF THE RISK FOR DEVELOPING A SECOND
MALIGNANCY FROM SCATTERED AND SECONDARY RADIATION IN
RADIATION THERAPY. Health Physics, 103(5), 652–
661.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3464436/
Parikh RR, e., 2016. Adjuvant Proton Beam Therapy in the Management of Thymoma: A
Dosimetric Comparison and Acute Toxicities. - PubMed - NCBI. [online]
Ncbi.nlm.nih.gov. Available at: <http://www.ncbi.nlm.nih.gov/pubmed/27372386>
[Accessed 9 Aug. 2016].
Paulino, A., 2016. The promise of intensity modulated radiation therapy. Pediatric Blood &
Cancer, [online] 63(9), pp.1513-1514. Available at:
<http://onlinelibrary.wiley.com/doi/10.1002/pbc.26081/full> [Accessed 11 May 2016].
Perez, C.A., Walz, B.J., Zivnuska, F.R., Pilepich, M., Prasad, K., Bauer, W., 1980.
Irradiation of carcinoma of the prostate localized to the pelvis: Analysis of tumor
response and prognosis. International Journal of Radiation Oncology. Available
at:<http://www.redjournal.org/article/0360-3016(80)90382-X/abstract> [Accessed 22
July 2016].
Page 37 of 40

Phase II Feasibility Study of High-Dose Radiotherapy for Prostate Cancer Using Proton
Boost Therapy: First Clinical Trial of Proton Beam Therapy for Prostate Cancer in Japan
Keiji Nihei, Takashi Ogino, Satoshi Ishikura, Mitsuhiko Kawashima, Hideki Nishimura,
Satoko Arahira and Masakatsu Onozawa. Jpn. J. Clin. Oncol. (December 2005) 35 (12):
745-752.http://jjco.oxfordjournals.org/content/35/12/745.long#F1
Pierre Blanchard, Adam S. Garden, G. Brandon Gunn, David I. Rosenthal, William H.
Morrison, Mike Hernandez, Joseph Crutison, Jack J. Lee, Rong Ye, C. David Fuller,
Abdallah S.R. Mohamed, Kate A. Hutcheson, Emma B. Holliday, Nikhil G. Thaker,
Erich M. Sturgis, Merrill S. Kies, X. Ronald Zhu, Radhe Mohan, Steven J. Frank.
http://www.thegreenjournal.com/article/S0167-8140(16)31136-7/fulltext
Red clover necrotic mosaic virus: Biophysics and Biotechnology. Lockney, Dustin Franzen, Stefan (advisor) 2011http://onlinelibrary.wiley.com/doi/10.1002/pbc.26081/full
Reiazi, R., Norozi, A., & Etedadialiabadi, M., 2015. A Literature Survey on Cost-
Effectiveness of Proton Beam Therapy in the Management of Breast Cancer Patients.
Iranian Journal of Cancer Prevention, 8(6), e4373.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4736076/
Risk of second brain tumor after conservative surgery and radiotherapy for pituitary
adenoma: update after an additional 10 years. Minniti G, Traish D, Ashley S, Gonsalves
A, Brada M. J Clin Endocrinol Metab. 2005 Feb; 90(2):800-4.
http://press.endocrine.org/doi/10.1210/jc.2004-1152?url_ver=Z39.88-2003&rfr_id=ori
%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed&
Roach, M., Nam, J., Gagliardi, G., Naqa, I. E., Deasy, J. O., & Marks, L. B. (2010). Radiation Dose–Volume Effects and the Penile Bulb. International Journal of Radiation Oncology, Biology, Physics, 76(3 Suppl), S130–S134. http://doi.org/10.1016/j.ijrobp.2009.04.094. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4786051/
Ron E, Modan B, Boice JD Jr, Alfandary E, Stovall M, Chetrit A, Katz L Tumors of the
brain and nervous system after radiotherapy in childhood. N Engl J Med. 1988 Oct 20;
319(16):1033-9. Abstract only.
http://www.nejm.org/doi/full/10.1056/NEJM198810203191601
Ronckers CM, Sigurdson AJ, Stovall M, Smith SA, Mertens AC, Liu Y, Hammond S,
Land CE, Neglia JP, Donaldson SS, Meadows AT, Sklar CA, Robison LL, Inskip PD.
Thyroid cancer in childhood cancer survivors: a detailed evaluation of radiation dose
Page 38 of 40

response and its modifiers. Radiat Res. 2006;166:618–628.
http://www.bioone.org/doi/10.1667/RR3605.1?url_ver=Z39.88-2003&rfr_id=ori%3Arid
%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed&
Rutqvist L, Rose C, Cavallin-Sta˚hl E. A systematic overview of radiation therapy effects
in breast cancer. Acta Oncol 2003;42(5/6):532/45.
http://www.ncbi.nlm.nih.gov/pubmed/14596511
Schippers JM, Lomax AJ. Emerging technologies in proton therapy. Acta Oncol. . 2011;
50(6):838–850. http://www.tandfonline.com/doi/full/10.3109/0284186X.2011.582513
Sethi, R. V., Shih, H. A., Yeap, B. Y., Mouw, K. W., Petersen, R., Kim, D. Y., …
MacDonald, S. M. (2014). SECOND NON-OCULAR TUMORS AMONG SURVIVORS
OF RETINOBLASTOMA TREATED WITH CONTEMPORARY PHOTON AND
PROTON RADIOTHERAPY. Cancer, 120(1), 126–133.
http://doi.org/10.1002/cncr.28387 http://www.ncbi.nlm.nih.gov/pmc/articles/
PMC3959122/
Sikuade MJ, e., 2010. Outcomes of treatment with stereotactic radiosurgery or proton
beam therapy for choroidal melanoma. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov.
Available at: <http://www.ncbi.nlm.nih.gov/pubmed/26160531> [Accessed 6 Jul. 2016].
Slater JD, Yonemoto LT, Rossi CJ, Jr, Reyes-Molyneux NJ, Bush DA, Antoine JE, et al.
Conformal proton therapy for prostate carcinoma. Int J Radiat Oncol Biol Phys 1998;
42(2):299/304.
Soldatos T, e., 2013. Imaging differentiation of pathologic fractures caused by primary
and secondary bone tumors. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/?term=soft-tissue+and+bone+cancer+pbt>
[Accessed 14 Aug. 2016].
Sugerman, D. and Livingston, E., 2014. Proton Beam Therapy for Prostate Cancer. JAMA, 311(14), p.1462.Suneja G, e., 2013. Acute toxicity of proton beam radiation for pediatric central nervous
system malignancies. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/23610011> [Accessed 6 Jul. 2016].
Takayama K, e., 2016. Treatment results of alternating chemoradiotherapy followed by
proton beam therapy boost combined with intra-arterial infusion chemotherapy for sta... -
Page 39 of 40

PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/26521257> [Accessed 6 Jul. 2016].
Tepper JE. Protons and parachutes. J Clin Oncol. 2008;26(15):2436-2437.
http://jco.ascopubs.org/content/26/15/2436.long
The effectiveness and safety of proton beam radiation therapy in children with malignant
central nervous system (CNS) tumours: protocol for a systematic review
Trofimov, A., Nguyen, P. L., Coen, J. J., Doppke, K. P., Schneider, R. J., Adams, J. A.,
… Shipley, W. U. (2007). Radiotherapy treatment of early stage prostate cancer with
IMRT and protons: a treatment planning comparison. International Journal of Radiation
Oncology, Biology, Physics, 69(2), 444–453.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2695934/
Vamsidhar Velcheti, O., 2008. Pathogenesis of Prostate Cancer: Lessons from Basic
Research. The Ochsner Journal, 8(4), p.213. [Accessed 8 Aug. 2016].
Verma V, e., 2016. A systematic review of the cost and cost-effectiveness studies of
proton radiotherapy. - PubMed - NCBI. [online] Ncbi.nlm.nih.gov. Available at:
<http://www.ncbi.nlm.nih.gov/pubmed/26828647> [Accessed 14 Aug. 2016].
Wai, E. (2015). SP-0356: IMRT: should IMRT be the standard of care for adjuvant breast RT?.
Radiotherapy and Oncology, 115, p.S173.
Wisenbaugh, E. S., Andrews, P. E., Ferrigni, R. G., Schild, S. E., Keole, S. R., Wong, W.
W., & Vora, S. A. (2014). Proton Beam Therapy for Localized Prostate Cancer 101:
Basics, Controversies, and Facts. Reviews in Urology, 16(2), 67–75.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4080851/
Zelefsky MJ, Fuks Z, Hunt M, Yamada Y, Marion C, Ling CC, et al. High-dose intensity
modulated radiation therapy for prostate cancer: early toxicity and biochemical outcome
in 772 patients. Int J Radiat Oncol Biol Phys 2002;53:1111–6.
http://cel.webofknowledge.com/InboundService.do?
product=CEL&SID=T1iB98xOdnvgrf3igVp&UT=WOS
%3A000177217800003&SrcApp=Highwire&action=retrieve&Init=Yes&SrcAuth=High
wire&Func=Frame&customersID=Highwire&IsProductCode=Yes&mode=FullRecord
Page 40 of 40