Segurança nas Vibrações sobre o Corpo Humano Vibração transmitida à mão.
PROGRAMA DE PÓS-GRADUAÇÃO STRICTO SENSU
DOUTORADO EM CIÊNCIAS DA REABILITAÇÃO
LAÍS CAMPOS DE OLIVEIRA
EFEITOS DA VIBRAÇÃO DE CORPO INTEIRO E DO
MÉTODO PILATES NAS MEDIDAS DA DENSIDADE
MINERAL ÓSSEA E DE FORÇA MUSCULAR EM
MULHERES NA PÓS-MENOPAUSA
Londrina
2017
LAÍS CAMPOS DE OLIVEIRA
EFEITOS DA VIBRAÇÃO DE CORPO INTEIRO E DO
MÉTODO PILATES NAS MEDIDAS DA DENSIDADE
MINERAL ÓSSEA E DE FORÇA MUSCULAR EM
MULHERES NA PÓS-MENOPAUSA
Tese apresentada ao Programa de Pós-Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina [UEL] e Universidade Norte do Paraná [UNOPAR]), como requisito parcial para a obtenção do título de Doutora em Ciência da Reabilitação. Orientadora: Profª. Drª. Deise Aparecida de Almeida Pires Oliveira.
Londrina
2017
AUTORIZO A REPRODUÇÃO TOTAL OU PARCIAL DESTE TRABALHO, POR QUALQUER MEIO CONVENCIONAL OU ELETRÔNICO, PARA FINS DE ESTUDO E PESQUISA, DESDE QUE CITADA A FONTE.
Dados Internacionais de catalogação na publicação (CIP) Universidade Pitágoras Unopar
Biblioteca CCBS/CCECA PIZA
Setor de Tratamento da Informação
Oliveira, Laís Campos de
O48e Efeitos da vibração de corpo inteiro e do método pilates nas
medidas da densidade mineral óssea e de força muscular em
mulheres na pós-menopausa. / Laís Campos de Oliveira.
Londrina: [s.n], 2017.
219f.
Tese (Doutorado em Ciências da Reabilitação).
Universidade Pitágoras Unopar.
Orientadora: Profa. Dra. Deise Aparecida de Almeida Pires
Oliveira.
1- Densidade óssea - Tese - UNOPAR 2- Exercício 3-
Pós-menopausa 4- Vibração de Corpo Inteiro 5- Osteoporose
6- Qualidade de vida I- Oliveira, Deise Aparecida de Almeida
Pires; orient. II- Universidade Pitágoras Unopar.
CDD 616.7
LAÍS CAMPOS DE OLIVEIRA
EFEITOS DA VIBRAÇÃO DE CORPO INTEIRO E DO MÉTODO PILATES NAS MEDIDAS DA DENSIDADE MINERAL ÓSSEA E DE FORÇA MUSCULAR EM
MULHERES NA PÓS-MENOPAUSA
Tese apresentada à UNOPAR, no Doutorado em Ciências da Reabilitação, área de
concentração em Ciências da Saúde, como requisito parcial para a obtenção do título
de Doutora conferida pela Banca Examinadora formada pelos professores:
______________________________________________ Profª. Drª. Deise Aparecida de Almeida Pires Oliveira
(Orientadora) Universidade Norte do Paraná
______________________________________________ Prof. Dr. Rodrigo Antonio Carvalho Andraus
Universidade Norte do Paraná
______________________________________________ Prof. Dr. Rodrigo Franco de Oliveira
Universidade Norte do Paraná
______________________________________________ Profª. Drª. Marta Helena de Souza De Conti
Universidade do Sagrado Coração
______________________________________________ Profa. Dra. Fernanda Cristiane de Melo
Universidade Estadual de Londrina
______________________________________________ Prof. Dr. Rubens Alexandre da Silva Junior
Coordenador do Curso
Londrina, 04 de agosto de 2017.

Dedico este trabalho aos profissionais da área da saúde que buscam melhorar a funcionalidade e a qualidade de vida
de mulheres na pós-menopausa.
AGRADECIMENTOS
Agradeço a Deus, autor de minha história, meu protetor e guia providenciador;
Ao meu marido, Raphael Gonçalves de Oliveira, meu amor e melhor amigo, por
toda contribuição durante essa tese;
A todos meus familiares pelas orações;
As voluntárias que se envolveram fielmente com a pesquisa;
Aos profissionais (Paula Roldão, Géssika Castilho, Jadson Márcio; Jorge Junior,
Fabiano Cardoso e funcionários da Ultramed) que realizaram todas as avaliações;
Aos professores da banca examinadora, Fernanda Cristiane de Melo, Marta
Helena de Souza De Conti, Rodrigo Franco de Oliveira, Rubens Alexandre da Silva
Junior e Rodrigo Antonio Carvalho Andraus pelo tempo despendido à leitura e toda
contribuição para o desenvolvimento dessa tese.
A professora Deise Aparecida de Almeida Pires Oliveira, minha amiga e dedicada
orientadora dos meus passos acadêmicos a qual se envolveu integralmente com
a elaboração dessa tese, não limitando esforços para me auxiliar em todos os
momentos do processo de doutorado.

“Descobrir consiste em olhar para o que
todo mundo está vendo e pensar uma
coisa diferente”.
(Roger Von Oech)
OLIVEIRA, Laís Campos de. Efeitos da vibração de corpo inteiro e do método Pilates nas medidas da densidade mineral óssea e de força muscular em mulheres na pós-menopausa. 2017. 219 páginas. Tese de doutorado (Programa de Pós-Graduação em Ciências da Reabilitação - Programa Associado entre UEL e UNOPAR) – Universidade Norte do Paraná, Londrina, 2017.
RESUMO
Introdução: Mulheres no período da pós-menopausa sofrem principalmente com o
declínio dos níveis de estrogênio, o que leva a uma redução da densidade mineral
óssea (DMO). Esse período culmina com a intensificação do processo de
envelhecimento, e com isso, diversas modificações ocorrem, principalmente no
sistema musculoesquelético e influenciam na diminuição de força muscular (FM),
podendo comprometer a qualidade de vida. Dentre as possibilidades de tratamentos
que buscam aumentar DMO e FM, e que não apresentam efeitos colaterais, estão
principalmente a prática regular e sistemática de exercício físico. No entanto,
principalmente em se tratando do metabolismo ósseo, ainda não está claro qual a
modalidade de exercício é mais eficaz nessa população. Objetivo: Verificar os efeitos
da vibração de corpo inteiro (VCI) e do método Pilates (MP) sobre a DMO e FM em
mulheres no período da pós-menopausa. Como objetivo específico, observar os
efeitos das técnicas sobre a qualidade de vida desta população. Métodos: Para o
estudo de revisão sistemática e meta-análise (artigo 1), ensaios clínicos randomizados
(ECRs) foram considerados elegíveis, com seguimento ≥ 6 meses, que verificaram os
efeitos da VCI sobre a DMO de mulheres pós-menopáusicas. Os cálculos da meta-
análise foram realizados por meio da diferença da média ponderada entre os grupos
VCI e controle, ou VCI e treinamento combinado, por meio da variação absoluta entre
pré e pós-intervenção para área da densidade mineral óssea (aDMO) ou densidade
mineral óssea volumétrica trabecular (vDMOt). Para os ECRs (artigos 2 e 3), foram
identificadas inicialmente 620 voluntárias, e após a aplicação dos critérios de
inclusão/exclusão, permaneceram 51 mulheres na pós-menopausa sendo alocadas
aleatoriamente em três grupos: VCI (n = 17), Pilates (n = 17) e controle (n = 17). Para
o artigo 2, os desfechos foram a área da DMO (coluna lombar, colo do fêmur, quadril
total, trocânter, intertrocanter e ward’s área) avaliadas pelo Dual-energy X-ray
Absorptiometry (DXA) no baseline e follow-up. Para o artigo 3, os desfechos foram o
pico de torque isocinético dos extensores e flexores do joelho, à 60º/s e 180º/s, além
da qualidade de vida mensurada pelo questionário SF-36. As intervenções (artigos 2
e 3) foram realizadas três vezes por semana, durante seis meses, o tempo de
intervenção dos grupos VCI e Pilates, foram de cinco minutos, e de 60 minutos
respectivamente. A análise foi feita por intenção de tratar com análises de covariância
ajustadas para os desfechos do baseline. Resultados: No estudo de revisão
sistemática e meta-análise (artigo 1), quinze ECRs foram incluídos na análise
estatística. Não foram observadas diferenças na análise primária. VCI possibilitou
melhora da aDMO em relação ao grupo controle, após exclusão de estudos de baixa
qualidade metodológica (coluna lombar), excluindo os estudos que combinaram VCI
com medicação ou treinamento combinado (coluna lombar), uso de baixa freqüência
e alta magnitude (coluna lombar e trocânter), alta frequência e baixa magnitude
(coluna lombar), alta dose cumulativa e baixa magnitude (coluna lombar), baixa dose
cumulativa e alta magnitude (coluna lombar e trocânter), joelho semi-fletido (coluna
lombar, colo do fêmur e trocânter) e tipo de vibração lado-alternado (coluna lombar e
trocânter). Para os ECRs (artigos 2 e 3), após seis meses de intervenção, 96,1% das
participantes completaram o follow-up. No artigo 2, as análises mostraram diferenças
médias estatisticamente significativas entre os grupos a favor das intervenções: VCI
vs. controle para DMO da coluna lombar (0,014 g/cm2 [IC 95%, 0,006, 0,022] p =
0,018, d = 1,21) e trocânter (0,018 g/cm2 [IC 95%, 0,006, 0,030] p = 0,012, d = 1,03);
e Pilates vs. controle para DMO da coluna lombar (0,016 g/cm2 [IC 95%, 0,007, 0,025]
p = 0,008, d = 1,15) e trocânter (0,020 g/cm2 [IC 95%, 0,010, 0,031] p = 0,005, d =
1,28). No artigo 3, as análises demonstraram que Pilates foi superior à VCI para força
muscular dos flexores do joelho à 60º/s (5,30 N.m [IC 95%, 0,26, 10,34] p = 0,009, d
= 0,70). Nas comparações com o grupo controle, Pilates foi superior (p < 0.05) em
todas as variáveis de força muscular (extensores do joelho à 60º/s, 7,75 N.m [IC 95%
1,11, 14,39] p = 0,015, d = 0,78; flexores do joelho à 60º/s, 5,35 N.m [IC 95% 1,05,
9,65] p = 0,024, d = 0,83; extensores do joelho à 180º/s, 4,67 N.m [IC 95% 0,85, 8,49]
p = 0,028, d = 0,82; flexores do joeho à 180º/s, 4,13 N.m [IC 95% 1,27, 6,99] p = 0,013,
d = 0,96) e em quatro domínios do SF-36. Conclusões: Os dados da meta-análise
(artigo 1) demonstraram que apesar da VCI apresentar potencial para atuar como um
coadjuvante na prevenção ou tratamento da osteoporose, especialmente para DMO
da coluna lombar, a intervenção ideal ainda não está clara. As análises de subgrupos
ajudaram a demonstrar os vários fatores que podem influenciar nos efeitos da VCI
sobre a DMO, contribuindo para a prática clínica e a definição de protocolos para
futuras intervenções. No artigo 2 foi demonstrado que VCI e Pilates tiveram efeitos
semelhantes sobre a DMO em mulheres na pós-menopausa e foram superiores a
nenhuma forma de intervenção para as regiões da coluna lombar e trocânter, mas não
para outras medidas da DMO. Contudo, o artigo 3 demonstrou que Pilates foi superior
a VCI para aumento da força muscular isocinética dos flexores do joelho, sem
diferença entre as técnicas para os extensores do joelho ou domínios da qualidade de
vida. Ainda, apenas Pilates foi superior a nenhuma intervenção para todas as variáveis
de força muscular e em quatro domínios da qualidade de vida (artigo 3).
Palavras-chave: Densidade óssea; Exercício; Pós-menopausa; Vibração de Corpo
Inteiro; Osteoporose; Força Muscular; Qualidade de Vida; Envelhecimento.
OLIVEIRA, Laís Campos de. Effects of whole body vibration and the Pilates method on bone mineral density and muscle strength measurements in postmenopausal women. 2017. 219 pages. PhD thesis (Programa de Pós-Graduação em Ciências da Reabilitação - Programa Associado entre UEL e UNOPAR) – Universidade Norte do Paraná, Londrina, 2017.
ABSTRACT
Background: Postmenopausal women mainly suffer from declining levels of estrogen,
which leads to a reduction in bone mineral density (BMD). This period culminates with
the intensification of the aging process, and with this, several modifications occur,
mainly in the musculoskeletal system and influence in the decrease of muscle strength
(MS), which may compromise the quality of life. Among the possibilities of treatments
that seek to increase BMD and MS, and that do not present side effects, are mainly
the regular and systematic practice of physical exercise. However, especially in the
case of bone metabolism, it is still not clear which exercise modality is most effective
in this population. Objective: To verify the effects of whole body vibration (WBV) and
the Pilates method (MP) on BMD and MS in postmenopausal women. As a specific
objective, observe the effects of the techniques on the quality of life of this population.
Methods: For the systematic review and meta-analysis study (Article 1), randomized
controlled trials (RCTs) were considered eligible, with a follow-up of ≥ 6 months, which
verified the effects of WBV on BMD in postmenopausal women. The meta-analysis
calculations were performed through the weighted mean difference between the WBV
and control groups, or WBV and combined training, through the absolute variation
between pre and post-intervention in the areal bone mineral density (aBMD) or
trabecular volumetric bone mineral density (vBMDt). For the RCTs (articles 2 and 3),
620 volunteers were initially identified, and after inclusion/exclusion criteria, 51
postmenopausal women remained randomly assigned to three groups: WBV (n = 17),
Pilates (n = 17) and control (n = 17). For article 2, the outcomes were the aBMD (lumbar
spine, femoral neck, total hip, trochanter, intertrocanter and ward's area) assessed by
Dual-energy X-ray Absorptiometry (DXA) at baseline and follow-up. For article 3, the
outcomes were the peak isokinetic torque of the knee extensors and flexors, at 60º/s
and 180º/s, in addition to the quality of life measured by the SF-36 questionnaire. The
interventions (articles 2 and 3) were performed three times a week for six months, the
intervention time of the WBV and Pilates groups were five minutes, and 60 minutes
respectively. The analysis was done by intention to treat with covariance analyzes
adjusted for baseline outcomes. Results: In the systematic review and meta-analysis
study (article 1), Fifteen RCTs were included in the meta-analysis. No differences were
observed in the primary analysis. WBV was found to improve aBMD compared with
the control group, after exclusion of studies with low quality methodological (lumbar
spine), when excluding the studies which combined WBV with medication or combined
training (lumbar spine), with the use of low frequency and high magnitude (lumbar
spine and trochanter), high frequency and low magnitude (lumbar spine), high
cumulative dose and low magnitude (lumbar spine), low cumulative dose and high
magnitude (lumbar spine and trochanter), with semi-flexed knee (lumbar spine, femoral
neck, and trochanter), and side-alternating type of vibration (lumbar spine and
trochanter). In article 2, the analyzes showed statistically significant mean differences
between the groups in favor of the interventions: WBV vs. Control for lumbar spine
aBMD (0.014 g/cm2 [95% CI, 0.006, 0.022] p = 0.018, d = 1.21) and trochanter (0.018
g/cm2 [95% CI, 0.006, 0.030] p = 0.012, d = 1.03); and Pilates vs. Control for lumbar
spine aBMD (0.016 g/cm2 [95% CI, 0.007, 0.025] p = 0.008, d = 1.15) and trochanter
(0.020 g/cm2 [95% CI, 0.010, 0.031] p = 0.005, d = 1.28). In the article 3, the analyzes
showed that Pilates was superior to the WBV for knee flexors muscle strength at 60º/s
(5.30 N.m [95% CI, 0.26, 10.34] p = 0.009, d = 0, 70). In the comparisons with the
control group, Pilates was superior (p < 0.05) in all muscle strength variables (knee
extensors at 60º/s, 7.75 N.m [95% CI, 1.11, 14.39] p = 0.015, d = 0.78; knee flexors at
60º/s, 5,35 N.m [95% CI, 1.05, 9.65] p = 0.024, d = 0.83; knee extensors at 180º/s,
4,67 N.m [95% CI, 0.85, 8.49] p = 0.028, d = 0.82; knee flexors at 180º/s, 4.13 N.m
[95% CI, 1.27, 6.99] p = 0.013, d = 0.96) and in four SF-36 domains. Conclusions:
Data from the meta-analysis (article 1) have shown that although the WBV has
potential to act as a coadjuvant in the prevention or treatment of osteoporosis,
especially for lumbar spine BMD, the optimal intervention is still unclear. Subgroup
analyzes have helped to demonstrate the various factors that may influence the effects
of WBV on BMD, contributing to clinical practice and protocol definition for future
interventions. In article 2 it was demonstrated that WBV and Pilates had similar effects
on BMD in postmenopausal women and were superior to no form of intervention for
the lumbar spine and trochanter regions but not for other measures of BMD. However,
article 3 demonstrated that Pilates was superior to WBV for increased isokinetic muscle
strength of the knee flexors, with no difference between techniques for knee extensors

or quality of life domains. Still, only Pilates was superior to no intervention for all muscle
strength variables and in four domains of quality of life (article 3).
Keywords: Bone density; Exercise; Postmenopause; Whole Body Vibration;
Osteoporosis; Muscle strength; Quality of life; Aging.
SUMÁRIO
1 INTRODUÇÃO ....................................................................................................... 15
2 OBJETIVO ............................................................................................................. 17
2.1 OBJETIVO GERAL ................................................................................................... 17
2.2 OBJETIVOS ESPECÍFICOS ........................................................................................ 17
3 HIPÓTESES ........................................................................................................... 18
4 FUNDAMENTAÇÃO TEÓRICA ............................................................................. 19
4.1 PERÍODO PÓS-MENOPAUSA .................................................................................... 19
4.2 DENSIDADE MINERAL ÓSSEA .................................................................................. 21
4.2.1 Métodos de avaliação para densidade mineral óssea ...................................... 23
4.2.2 Osteoporose ..................................................................................................... 26
4.3 FORÇA MUSCULAR ................................................................................................. 29
4.4 QUALIDADE DE VIDA ............................................................................................... 31
4.5 VIBRAÇÃO DE CORPO INTEIRO ................................................................................ 33
4.5.1 Aspectos neurofisiológicos da VCI.................................................................... 37
4.5.2 Indicações e contra-indicações da VCI..............................................................38
4.6 MÉTODO PILATES .................................................................................................. 38
4.6.1 Indicações e contra-indicações do MP..............................................................42
5 REFERÊNCIAS ...................................................................................................... 43
6 PRODUÇÕES CIENTÍFICAS ................................................................................. 64
6.1 ARTIGO 1: REVISÃO SISTEMÁTICA E META-ANÁLISE .................................................. 64
6.2 ARTIGO 2: ESTUDO ORIGINAL .................................................................................132
6.3 ARTIGO 3: ESTUDO ORIGINAL .................................................................................166
7 CONCLUSÃO GERAL .........................................................................................210

8 ANEXOS ..............................................................................................................211
Anexo A – Parecer do Comitê de Ética em Pesquisa .............................................211
Anexo B – Protocolo de Registro no Clinical Trials .................................................214
15
1 INTRODUÇÃO
Mulheres no período da pós-menopausa sofrem com alterações hormonais
tendo em vista o rápido declínio dos níveis de estrogênio, o que desencadeia uma
série de fatores negativos para saúde1-4. Este período em que ocorre a cessação do
ciclo ovulatório está relacionado ao processo de envelhecimento5-8. Ambos fatores
associados aceleram principalmente a redução da densidade mineral óssea (DMO), e
a perda de força muscular (FM), comprometendo a qualidade de vida desta
população9,10.
Dentre as possibilidades de tratamentos que objetivam o aumento da DMO e
FM estão principalmente a prática regular e sistemática de exercício físico11,12 e o uso
de medicamentos13,14. Todavia, o tratamento medicamentoso envolve principalmente
a Terapia de Reposição Hormonal (TRH), que apesar de contribuir de maneira
importante com a reversão dos diferentes fatores que impactam negativamente sobre
a saúde de mulheres na pós menopausa14-18, alguns profissionais optam por não
realizá-la, uma vez que existem evidências para o aumento do risco de doenças
cardíacas, acidente vascular cerebral e câncer de mama, principalmente quando
utilizada por mais de três anos consecutivos e quando existe a pré-disposição a estas
doenças19-22.
Desta forma, o exercício físico destaca-se na literatura por ser um tratamento
conservador, capaz de auxiliar no metabolismo ósseo23-26e no aumento da força
muscular sem causar efeitos colaterais27-29, atuando também como medida preventiva
tendo em vista esse sério problema de saúde pública6,10,23. No entanto, em se tratando
do metabolismo ósseo, ainda não está claro a modalidade de exercício mais eficaz
em mulheres no período pós-menopausa30. Uma forma de terapia investigada
16
recentemente é a vibração de corpo inteiro (VCI), que se caracteriza pelo
posicionamento do indivíduo sobre uma plataforma vibratória capaz de transmitir
aceleração mecânica vertical para o sistema musculoesquelético31-33. Contudo, até o
momento permanecem incertos os melhores parâmetros para potencializar o aumento
da DMO, como intensidade (frequência e magnitude), tipo de vibração (síncrona ou
lado-alternado), tempo de exposição e posicionamento corporal sobre a placa
vibratória34-60. Também tem sido sugerido que a VCI possibilita o aumento da FM em
mulheres na pós-menopausa61-63.
Outras formas de intervenção têm sido recomendadas, principalmente por meio
de exercícios de resistência muscular, que podem contribuir com a melhora da DMO
e da FM em mulheres no período da pós-menopausa23-25. Uma opção de exercício
físico que oferece resistência muscular e vem ganhando popularidade é o Método
Pilates (MP)64-66. Porém, são poucos os estudos que investigaram os efeitos desta
técnica sobre a DMO67, no entanto, estudos demonstraram a potencial contribuição
desse método sobre as variáveis força muscular68-70, e o reflexo positivo na qualidade
de vida dessa população71-73.
Este estudo justifica-se devido a pouca literatura e evidência quanto aos
benefícios da VCI e de modalidades emergentes de exercício físico, como o MP, sobre
a DMO em mulheres pós-menopáusicas. Além disso, são poucas as informações
sobre a influência da VCI na FM de mulheres na pós-menopausa.
Assim, as seguintes questões nortearam a tese: a) quais parâmetros utilizados
na VCI são capazes de potencializar aumento da DMO em mulheres na pós-
menopausa?; b) VCI e MP alteram a DMO de mulheres na pós-menopausa?; c) as
duas modalidades de intervenção contribuem para aumento da força muscular e
qualidade de vida em mulheres pós-menopáusicas?
17
2 OBJETIVO
2.1 OBJETIVO GERAL
Verificar os efeitos da VCI e do MP sobre a densidade mineral óssea, força
muscular e qualidade de vida em mulheres no período da pós-menopausa.
2.2 OBJETIVOS ESPECÍFICOS
Os objetivos específicos da presente tese de doutorado estiveram atrelados as
produções científicas em forma de artigo como segue:
• Analisar os ensaios clínicos que verificaram os efeitos da VCI sobre a DMO em
mulheres pós-menopáusicas, em comparação com nenhuma intervenção ou
intervenção mínima e outras formas de exercício (Artigo 1: Effects of whole
body vibration on bone mineral density in postmenopausal women: a systematic
review and meta-analysis);
• Verificar os efeitos da VCI e do MP sobre a DMO em mulheres na pós-
menopausa (Artigo 2: Effects of whole body vibration and the Pilates method
on bone mineral density in postmenopausal women: a randomized and
controlled clinical trial);
• Observar os efeitos da VCI e do MP sobre o pico de torque isocinético dos
extensores e flexores do joelho (objetivo primário) e qualidade de vida (objetivo
secundário) em mulheres na pós-menopausa. (Pilates vs. vibração de corpo
inteiro na força muscular e qualidade de vida em mulheres na pós-menopausa:
um ensaio clínico randomizado e controlado);
18
3 HIPÓTESES
As hipóteses sobre os artigos foram:
• Artigo 2: Partimos do pressuposto que os parâmetros escolhidos para a VCI e
o protocolo de intervenção selecionado para a prática do MP serão capazes de
proporcionar aumento da DMO nesta população.
• Artigo 3: Partimos da hipótese de que as intervenções possibilitarão efeitos
positivos sobre o pico de torque isocinético dos extensores e flexores do joelho
e qualidade de vida quando comprados a nenhuma intervenção, contudo, uma
vez que Pilates trabalha com resistência muscular progressiva, acreditamos
que será superior a VCI sobre os parâmetros investigados.
19
4 FUNDAMENTAÇÃO TEÓRICA
4.1 PERÍODO PÓS-MENOPAUSA
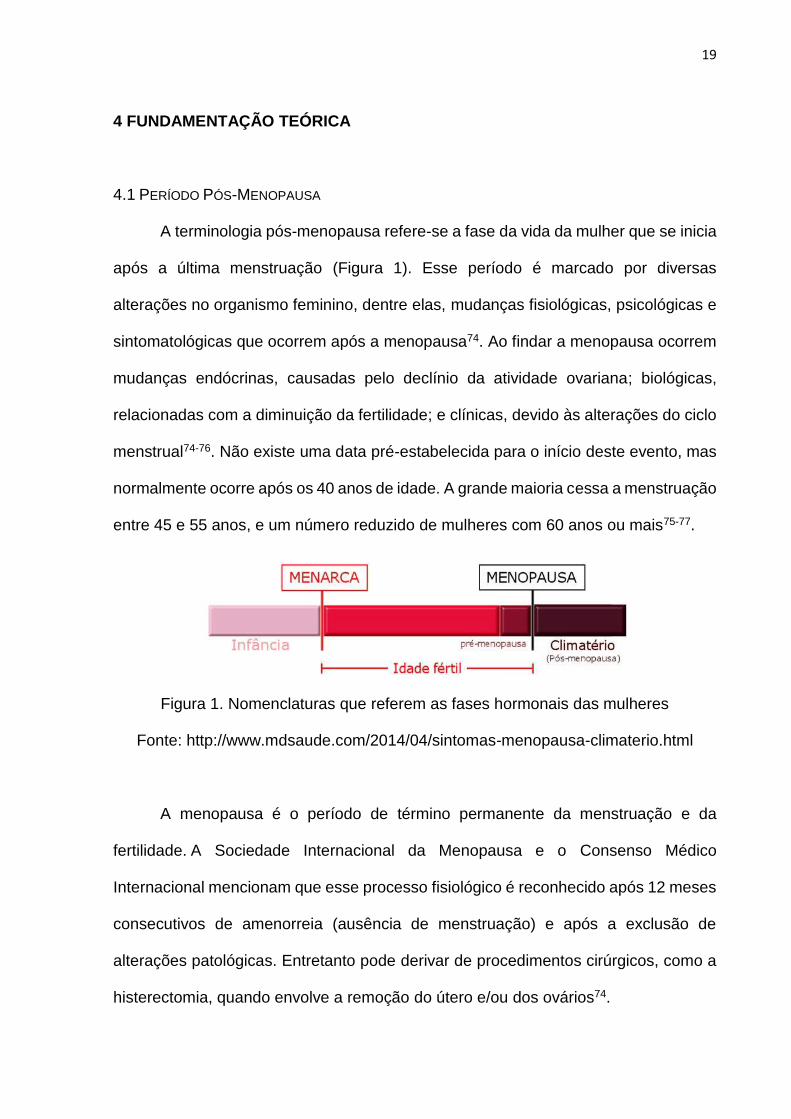
A terminologia pós-menopausa refere-se a fase da vida da mulher que se inicia
após a última menstruação (Figura 1). Esse período é marcado por diversas
alterações no organismo feminino, dentre elas, mudanças fisiológicas, psicológicas e
sintomatológicas que ocorrem após a menopausa74. Ao findar a menopausa ocorrem
mudanças endócrinas, causadas pelo declínio da atividade ovariana; biológicas,
relacionadas com a diminuição da fertilidade; e clínicas, devido às alterações do ciclo
menstrual74-76. Não existe uma data pré-estabelecida para o início deste evento, mas
normalmente ocorre após os 40 anos de idade. A grande maioria cessa a menstruação
entre 45 e 55 anos, e um número reduzido de mulheres com 60 anos ou mais75-77.
Figura 1. Nomenclaturas que referem as fases hormonais das mulheres
Fonte: http://www.mdsaude.com/2014/04/sintomas-menopausa-climaterio.html
A menopausa é o período de término permanente da menstruação e da
fertilidade. A Sociedade Internacional da Menopausa e o Consenso Médico
Internacional mencionam que esse processo fisiológico é reconhecido após 12 meses
consecutivos de amenorreia (ausência de menstruação) e após a exclusão de
alterações patológicas. Entretanto pode derivar de procedimentos cirúrgicos, como a
histerectomia, quando envolve a remoção do útero e/ou dos ovários74.
20
Uma das funções dos ovários é a produção de hormônios sexuais femininos,
sendo os principais denominados estrogênio e progesterona78,79. No período de
interrupção menstrual, os ovários diminuem a produção de estrogênio, hormônio
responsável pelo controle do ciclo menstrual e desenvolvimento das características
sexuais secundárias femininas, que possui forte influência durante toda a
adolescência e fase adulta da mulher. Os receptores de estrogênios localizados no
sistema nervoso central e nos tecidos ósseos, realizam a síntese de proteínas, e entre
outras funções realizam a preservação do cálcio nos ossos80.
Quando finda a mestruação, os ovários também diminuem a produção de
progesterona, hormônio que atua nas diversas fases do ciclo menstrual e ao longo da
fase reprodutiva, sendo responsável pela preparação da membrana mucosa do útero
para receber o óvulo possivelmente fecundado80. A falta e/ou diminuição desses
hormônios (estrogênio e progesterona) provoca o aparecimento de diversos sintomas
da menopausa81.
Dentre os diversos sintomas relatados, os principais são ondas de calor,
distúrbios do sono, alterações do humor, depressão, redução da libido e secura
vaginal81,82. A fase da pós-menopausa culmina com a intensificação do processo de
envelhecimento, e com isso ocorrem diversas modificações fisiológias, principalmente
no sistema musculoesquelético5,7,8, levando principalmente à diminuição da DMO,
força muscular e equilíbrio postural83,84, aumentando o risco de quedas e
potencializando as chances de ocorrer uma fratura, contribuindo para a dimininuição
da funcionalidade25,29.
21
4.2 DENSIDADE MINERAL ÓSSEA
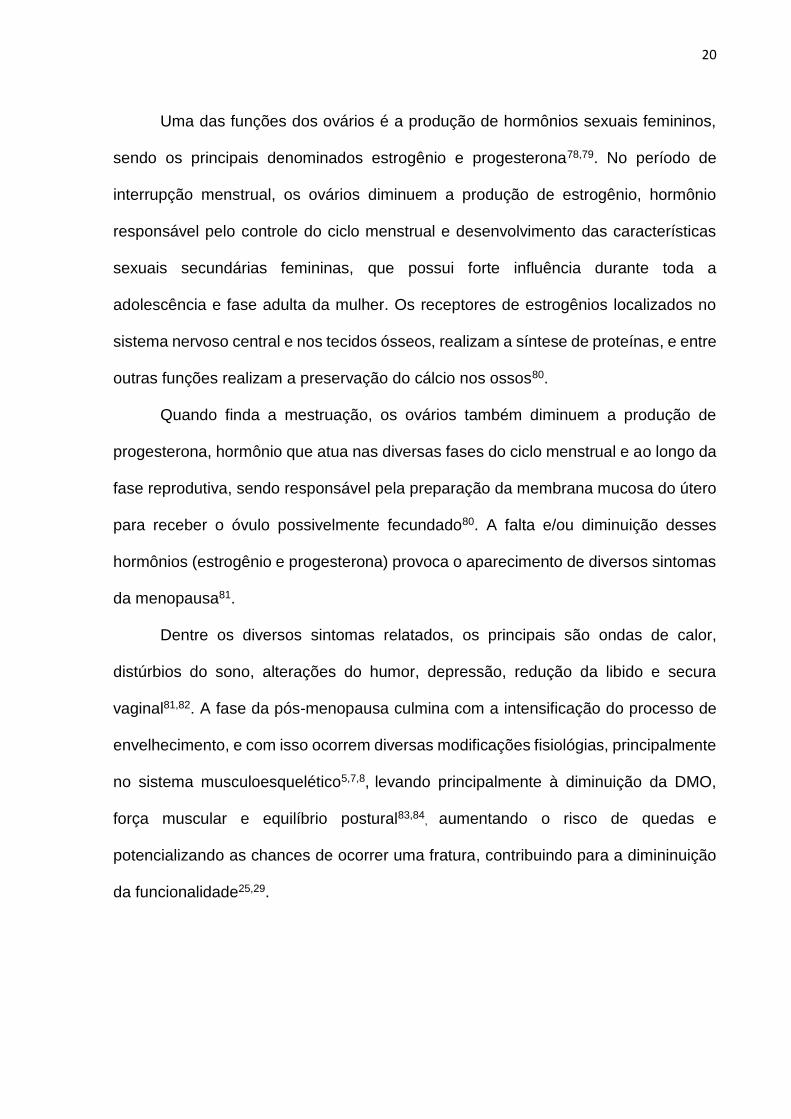
A Densidade Mineral Óssea (DMO) é o resultado do processo dinâmico de
formação de tecido ósseo que está em constante renovação80. Essa renovação óssea
ocorre por meio do trabalho equilibrado entre as células que realizam a decomposição
da matriz, reabsorvendo as células ósseas consideradas “gastas e velhas”,
denominadas de osteoclastos, e as células responsáveis pela
reconstrução/remodelamento e fortalecimento dessa matriz, a qual recebe o nome de
osteoblastos85-87 (figura 2), entretanto existem fatores que podem interferir neste
equilíbrio e comprometer a matriz óssea88. A matriz é o conjunto das células (fibras
colágenas) e de minerais (cálcio e fósforo) que formam o conteúdo mineral ósseo e
por meio da análise deste conteúdo, em um determinado volume de osso, é possível
mensurar a DMO89,90.
Figura 2. Turnover osseo
Fonte: http://www.moreirajr.com.br/revistas.asp?fase=r003&id_materia=4262
Acumular DMO durante a infância e adolescência é fundamental para a saúde
óssea na idade adulta. O pico de DMO de uma pessoa é preditor de incidências de
22
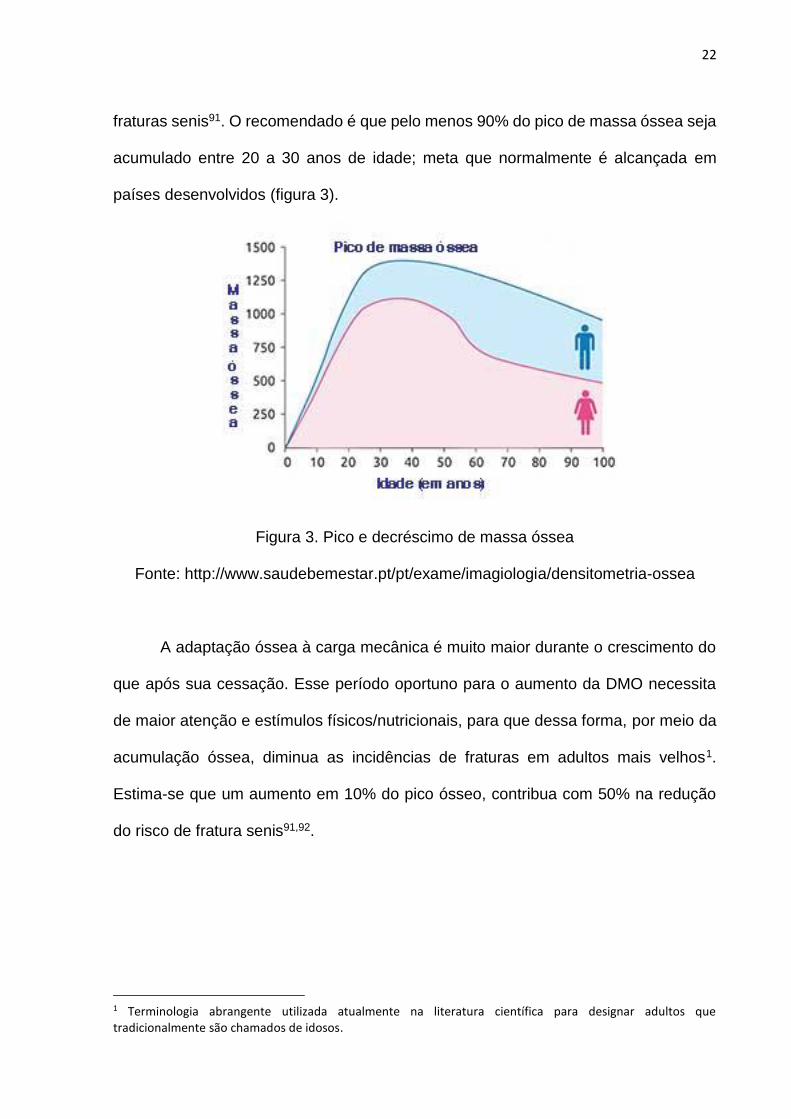
fraturas senis91. O recomendado é que pelo menos 90% do pico de massa óssea seja
acumulado entre 20 a 30 anos de idade; meta que normalmente é alcançada em
países desenvolvidos (figura 3).
Figura 3. Pico e decréscimo de massa óssea
Fonte: http://www.saudebemestar.pt/pt/exame/imagiologia/densitometria-ossea
A adaptação óssea à carga mecânica é muito maior durante o crescimento do
que após sua cessação. Esse período oportuno para o aumento da DMO necessita
de maior atenção e estímulos físicos/nutricionais, para que dessa forma, por meio da
acumulação óssea, diminua as incidências de fraturas em adultos mais velhos1.
Estima-se que um aumento em 10% do pico ósseo, contribua com 50% na redução
do risco de fratura senis91,92.
1 Terminologia abrangente utilizada atualmente na literatura científica para designar adultos que tradicionalmente são chamados de idosos.
23
4.2.1 Métodos de avaliação para densidade mineral óssea
Para avaliar a DMO existem alguns métodos padrões, como por exemplo, a
Ultrassonografia Quantitativa (QUS - Quantitative Ultrasound), que é indicada para
mensuração da predição do risco de fratura, além do diagnóstico e monitoramento da
osteoporose. De acordo com a Sociedade Internacional de Densitometria Clínica
(ISCD - International Society for Clinical Densitometry), o único sitio ósseo validado
para o uso clínico de QUS visando a avaliação da osteoporose é o calcâneo. Essa
técnica utiliza feixes de ultrassom para o estudo da massa óssea, que avalia a
velocidade, a atenuação e a reflexão do ultrassom na matriz. Os pontos fortes do uso
da QUS são relacionados a isenção de radiação ionizante, a portatibilidade e
economia para realizar a avaliação90,93.
Outra opção de análise refere-se à Tomografia Computadorizada Quantitativa
Periférica (pQCT - Peripheral Quantitative Computed Tomography) de alta resolução.
A pQCT é uma técnica de imagem que usa processamento computadorizado da
atenuação de raios-X, medidas em Unidades Hounsfield (HU - Hounsfield Unit) para
a aquisição de imagens seccionais. Esse método permite a diferenciação entre os
ossos cortical e trabecular, sendo capaz de mensurar a densidade mineral óssea
volumétrica, a geometria do osso, entre outras medidas90,94.
Todavia, o método mais utilizado para avaliação da DMO é por intermédio da
Absorciometria por Dupla Emissão de Raios X (DXA - Dual-energy X-ray
Absorptiometry). Esta técnica utiliza dois fótons possibilitando a avaliação da área da
DMO nas regiões que tipicamente apresentam maior perda óssea. As regiões que
normalmente são avaliadas referem-se a coluna lombar, colo do fêmur, quadril total,
trocânter, intertrocanter e ward’s área (pequena área localizada próxima ao colo
femoral, com predomínio de osso trabecular, apresentando menor densidade mineral
24
óssea dentre as áreas analisadas nessa região), todavia, as duas regiões utilizadas
para diagnóstico de osteopenia e osteoporose referem-se a coluna lombar e colo do
fêmur. O DXA é considerado padrão-ouro para diagnóstico, monitoramento e
investigação clínica da massa óssea em função da sua sensibilidade, precisão e
segurança. A avaliação é rápida e indolor, produzindo uma baixa exposição à
radiação, até dez vezes menor que a exposição gerada por uma radiografia normal
de tórax90,95,96.
As avaliações para verificar a DMO são fundamentais para tomadas de decisão
clínica visando a prevenção, manutenção e acompanhamento do trabalho equilibrado
das células ósseas90. Entretanto, existem fatores que podem interferir neste equilíbrio,
e quando isto ocorre a matriz óssea fica comprometida, os ossos ficam mais porosos,
o que pode levar ao diagnóstico de osteopenia. Esta classificação é o primeiro estágio
do déficit na massa óssea, no entanto se a perda de DMO permanece, poderá levar a
um comprometimento maior, até o quadro de osteoporose, doença que afeta
frequentemente mulheres na pós-menopausa97,98.
Em relação as propriedades psicométricas desses instrumentos de avaliação,
no estudo de Iida et al (2010)99 foi investigado a validade da medição do QUS por
meio dos valores do DXA (considerado como padrão ouro), utilizando valores da DMO
da coluna lombar, colo femoral e do fêmur. Os resultados mostraram que a validade
da medição do QUS foi relativamente alta (r ≈ 0.2-0.4) entre mulheres de meia idade
e mais velhas, apresentando correlações significativamente positivas entre coluna
lombar, colo femoral e femur e os índices bilaterais de rigidez calcaneal (r ≈ 0,3-0,4).
No estudo de Behrens (2016)100 foi avaliado um novo dispositivo de QUS
(Bindex® quantitative ultrasound) quanto a sua confiabilidade intra e entre sessões,
por meio dos valores do DXA. Os resultados mostraram alta confiabilidade intra (ICC
25
= 0,977, CV = 1,5%) e entre sessões (ICC = 0,978, CV = 1,4%) para DMO. As maiores
correlações positivas foram encontradas para a espessura cortical do QUS e para
DMO do rádio e da tibia distal (r ⩾ 0,71, p <0,001). Indicando que os dados desse
QUS são repetitivos dentro e entre as sessões de medição, refletindo as medidas de
DMO em regiões ósseas específicas.
Em relação ao equipamento pQCT, Lee et al. (2014)101 analisaram a validade
e a confiabilidade deste, como ferramenta de triagem para osteoporose, por meio dos
valores do DXA. Os resultados mostraram que em termos de validade, a atenuação
óssea na região de coluna lombar, colo femoral e trocânter, por meio da pQCT
apresentou correlações significativas (coeficientes de correlação, 0,399 – 0,613) com
a DMO para todas as regiões do DXA. O mesmo ocorreu para tíbia distal e o talus
respectivamente (coeficientes de correlação, 0,493 – 0,581; 0,396 - 0,579).
Em termos de confiabilidade, todas as medições (coluna lombar, cabeça
femoral, trocânter, fêmur distal, tibia proximal, tíbia distal e talus), exceto colo femoral,
apresentaram boa a excelente confiabilidade inter-observador (coeficientes de
correlação intraclasse, 0,691 – 0,941). Mostrando que a pQCT é uma ferramenta de
rastreio útil para a osteoporose, refletindo adequadamente os valores da DMO pelo
DXA101.
Um estudo realizado por Zack (2002)102 analisou a confiabilidade do
equipamento DXA, os resultados mostraram que os coeficientes de correlação
variaram de 0,993 a 0,996 (p < 0,01). Os coeficientes de variação foram de 0,73%
para corpo total, 0,92% para coluna lombar, 0,69% para fêmur total proximal e 1,09%
para antebraço total; ressaltando que o uso do DXA é confiável para medidas de
DMO102.
26
4.2.2 Osteoporose
A osteoporose é uma doença esquelética sistêmica caracterizada por
diminuição da massa óssea e deteriorização microarquitetural do tecido ósseo, com
consequente aumento da fragilidade óssea e susceptibilidade à fratura, considerada
um sério problema de saúde pública90,98,103. Tendo em vista o aumento da expectativa
de vida populacional, cresce concomitantemente o número de pessoas
diagnosticadas com osteoporose104,105.
Estimativas mostram que a quantidade de fraturas decorrente da osteoporose,
na população brasileira, chegará a 140 mil por ano em 2020. No Brasil estima-se que
33% das mulheres na pós-menopausa tenham osteoporose na coluna lombar e colo
do fêmur, de acordo com os critérios propostos pela Organização Mundial da Saúde
(OMS)105,106.
A osteoporose afeta países desenvolvidos e também em desenvolvimento, à
medida que suas populações começam a envelhecer. Estudo realizado por Wade et
al.107 verificou que 49 milhões de indivíduos dos países: Estados Unidos, Canadá,
Japão, Austrália, Reino Unido, França, Alemanha, Itália e Espanha, com 50 anos ou
mais, apresentam diagnóstico de osteoporose nas regiões de quadril ou coluna
vertebral. A prevalência de osteoporose em mulheres nos Estados Unidos é de 16%,
Canadá 18%, Japão 38%, Austrália 22%, Reino Unido 27%, França 32%, Alemanha
33%, Itália 30%, e Espanha 30%.
Em relação ao Brasil, a prevalência não difere de outros países, mas há um
conhecimento limitado sobre a epidemiologia e prevalência dessa doença. Em um
estudo realizado por Baccaro et al.108 a prevalência relatada de osteoporose em
mulheres brasileiras variou de 15% a 33% dependendo da região geográfica. Em 2013
27
um estudo com mulheres brasileiras de 50 anos ou mais, residentes na cidade de
Campinas, observou prevalência de osteoporose de 21,3%109.
No estudo realizado por Pinheiro et al.110 sobre a prevalência de fraturas por
osteoporose em mulheres acima de 40 anos, não houve diferença estatisticamente
significativa nas cinco regiões do Brasil. A prevalência de fraturas variou de 12,2 a
16,2%, sendo no Norte 12,2%, Nordeste 15,3%, Centro-Oeste 10,5%, Sudeste 16,2%
e Sul 13,8%. A prevalência dessa população com osteoporose é de 15,1%.
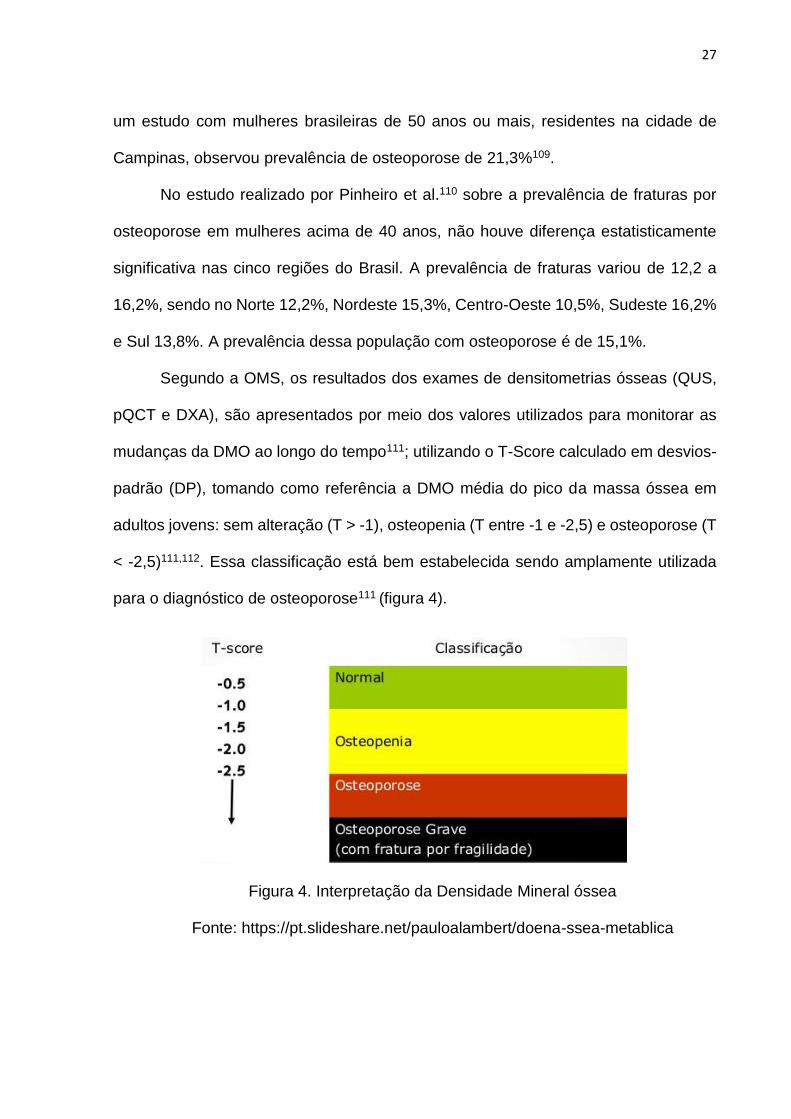
Segundo a OMS, os resultados dos exames de densitometrias ósseas (QUS,
pQCT e DXA), são apresentados por meio dos valores utilizados para monitorar as
mudanças da DMO ao longo do tempo111; utilizando o T-Score calculado em desvios-
padrão (DP), tomando como referência a DMO média do pico da massa óssea em
adultos jovens: sem alteração (T > -1), osteopenia (T entre -1 e -2,5) e osteoporose (T
< -2,5)111,112. Essa classificação está bem estabelecida sendo amplamente utilizada
para o diagnóstico de osteoporose111 (figura 4).
Figura 4. Interpretação da Densidade Mineral óssea
Fonte: https://pt.slideshare.net/pauloalambert/doena-ssea-metablica
28
As mulheres estão mais suscetíveis à osteoporose do que homens, pois além
de apresentarem perda óssea importante durante a pós-menopausa devido a
diminuição na produção de estrogênio, ainda possuem fisiologicamente menor DMO,
por normalmente apresentarem óssos mais tênues113; Além disso, possuem maior
expectativa de vida quando comparadas aos homens, o que as deixam em maior risco
104. Outros fatores que aumentam as chances de osteoporose são a baixa estatura,
etnia branca ou asiática e hereditariedade114. A menarca tardia e a menopausa
precoce, também aumentam as chances de osteoporose, pois nesse caso o
organismo fica exposto por menor tempo aos estrógenos115.
Parker et al.115 identificaram em um estudo de coorte prospectivo, que a idade
da menarca ocorrendo com 11 anos ou menos está associada a uma menor incidência
de osteoporose, enquanto um menor número de anos menstruais é associado a um
risco aumentado de osteoporose. Assim, um tempo menor que 25 anos de
menstruação foi associado a um aumento da incidência de osteoporose em 80% em
comparação com um tempo de menstruação de 35 anos ou mais.
Existem dois tipos de osteoporose: a primária, que se relaciona à perda óssea
que ocorre devido ao processo fisiológico de envelhecimento, sendo a mais
pesquisada em mulheres na pós-menopausa; e a secundária, que resulta de alguns
distúrbios clínicos, medicamentos e/ou hábitos que diminuem a DMO, por exemplo,
diabetes, osteogênese imperfeita, hipertireoidismo, doença renal, síndrome de
Cushing, síndromes de má absorção, anorexia nervosa, medicamentos como
anticonvulsivantes para epilepsia, corticosteróides para artrite reumatóide, asma e
agentes imunossupressores, ou ainda, fatores relacionados ao estilo de vida, como
tabagismo, alcoolismo e sedentarismo116.
29
Um importante fator que deve ser considerado nos quadros de osteoporose
refere-se à associação existente com a redução da massa muscular e o
comprometimento do desempenho muscular (sarcopenia). Durante a última década,
óssos e músculos foram cada vez mais reconhecidos como tecidos que se interagem,
não só por causa de suas superfícies adjacentes como também dos efeitos mecânicos
da carga muscular sobre a função óssea117. Associação entre osteoporose e
sarcopenia geram consequentes alterações nas capacidades físicas, como perda de
força muscular, podendo impactar de maneira significativa na qualidade de vida118.
4.3 FORÇA MUSCULAR
A força muscular é a capacidade física definida como a máxima tensão que
pode ser gerada por um músculo esquelético específico ou por um grupo muscular,
para realizar um determinado movimento corporal11. Uma vez que na musculatura
esquelética existem receptores de estrogênio, quando as taxas desse hormônio caem
devido a menopausa, ocorre um prejuízo ao tônus muscular, que diminui a contração
e a força, com consequente aumento da fadiga1.
Ainda, a força muscular diminui na pós-menopausa devido à sarcopenia,
acarretando déficits na execução de movimentos7,24,26. Sarcopenia é a redução da
massa muscular e o comprometimento do desempenho muscular, que oc
orrem devido ao envelhecimento. A prevalência de sarcopenia pode atingir até
40% da população pós-menopáusica7.
Segundo Sjöblom et al.7 existem alguns estágios que classificam esse processo
em pré-sarcopenia, quando ocorre baixa massa muscular sem qualquer diminuição
na força muscular ou no desempenho físico. Sarcopenia, quando existe uma
diminuição da massa muscular acompanhada por uma diminuição da força muscular
30
ou no desempenho; e sarcopenia grave, quando os três componentes são
prejudicados. Segundo esses autores, a sarcopenia também pode ser categorizada
de acordo com o início, sendo primária, quando é relacionada à idade sem qualquer
outra causa secundária evidente, ou secundária quando for consequência de co-
morbidades.
Estudo de revisão sistemática e meta-análise demonstrou que a redução da
força muscular em adultos mais velhos, avaliada por intermédio do teste de preensão
manual ou pela força dos extensores do joelho, está significativamente associada à
60% maior chance de declínio funcional. Foi demonstrado ainda que menor força
muscular é o fator de risco mais importante do declínio funcional nessa população do
que a perda de massa muscular119. A redução da força muscular frequentemente é
associada ao processo de envelhecimento, sendo responsável pela diminuição da
funcionalidade em mulheres na pós-menopausa7,8. Outro estudo de revisão
sistemática115 demonstrou que a força muscular é reduzida de duas a cinco vezes
mais rápido que a massa muscular. Ao sumarizar resultados de estudos longitudinais
foi demonstrado que aos 75 anos de idade, a força muscular é reduzida a uma taxa
de 3,0 a 4,0% ao ano em homens e de 2,5 a 3,0% ao ano em mulheres, sendo esta
variável mais preponderante para o risco de incapacidade e morte do que a perda de
massa muscular. Além disso, a força dos membros inferiores diminui mais
rapidamente que a dos membros superiores, assim a redução da força de extensão
do joelho está associada à um risco aumentado de invalidez e morte120.
A diminuição da força muscular pode comprometer a qualidade de vida de
mulheres na pós-menopausa, aumentando a dependência, limitando a funcionalidade
para a realização das atividades diárias, diminuindo as oportunidades de auto-
realização e a expectativa de vida121.
31
4.4 QUALIDADE DE VIDA
Qualidade de vida (QV) envolve fatores subjetivos e complexos relacionados
ao bem-estar físico, mental e social, que costumam ser mensurados através de
questionários capazes de estimar estas variáveis. A Organização Mundial da Saúde
elaborou o questionário WHOQOL para verificar o nível da QV dos diferentes grupos
sociais, de diferentes países e culturas. No Brasil, o questionário possui duas versões
validadas para o português, o composto por 100 questões, e o composto por 26
questões, onde as perguntas são separadas em seis domínios: físico, psicológico,
nível de independência, relações sociais, meio ambiente e aspectos religiosos122.
Existem questionários específicos que avaliam o nível da QV de mulheres no
período da pós-menopausa, por exemplo, o Questionário de Qualidade de Vida da
Menopausa (MENQOL) é validado para a avaliação dos sintomas da menopausa,
relacionando com a QV dessa população; O Greene Climacteric Scale é um
questionário auto-relatado que observa 21 sintomas físicos e psicológicos associados
à transição da menopausa e o impacto na QV; O Utian Quality of Life Scale (UQOL)
avalia como as mulheres percebem sua vida em cada dimensão, independentemente
das queixas somáticas ou psicológicas; O MENCAV é um questionário válido e
confiável que inclui 37 itens e cinco dimensões para avaliar a QV de mulheres na
menopausa122.
A Escala de Avaliação da Menopausa (MRS) avalia QV e os sintomas do
climatério através de 11 questões distribuídas em 3 subescalas: sintomas somato-
vegetativos (falta de ar, suores, calores; mal-estar do coração, problemas de sono;
problemas musculares e nas articulações), psicológicos (estado de animo depressivo,
irritabilidade, ansiedade, esgotamento físico e mental) e urogenitais (problemas
sexuais, problemas de bexiga e ressecamento vaginal). A Escala de Cervantes
32
apresenta 31 itens que avaliam a QV relacionada à saúde da mulher durante o
climatério, através dos domínios, psíquico, relacionamento do casal, sintomas
vasomotores, ou envelhecimento122.
O questionário SF-36 (Medical Outcomes Study 36 - Item Short - Form Health
Survey) é um instrumento genérico que avalia QV, sendo de fácil administração e
compreensão, composto por 36 itens que analisam domínios da capacidade funcional,
aspectos físicos, dor, estado geral da saúde, vitalidade, aspectos sociais, aspectos
emocionais e saúde mental122. Estudo de revisão sistemática122 sobre os diversos
questionários que mensuram a QV em mulheres na menopausa, mostrou que o SF-
36 e MENQOL são os instrumentos mais utilizados para analisar essa população.
O termo QV no Brasil de acordo com Dantas, Sawada e Malerbo123 é
relativamente recente e apesar de haver inúmeras definições, não existe uma que seja
amplamente aceita. No geral trata-se das condições básicas e suplementares para
que o ser humano possa viver bem e sua consequente análise. O número de
pesquisas nessa temática cresce a cada ano e mesmo sendo uma terminologia
abrangente, a maior parte dos estudos verificam a QV na população de adultos que
sofrem com algum tipo de patologia, observando o quanto os déficits orgânicos podem
comprometer esta123.
No geral, para se obter uma boa QV são necessários hábitos alimentares
saudáveis, manutenção de relacionamentos sociais saudáveis, reserva de tempo
destinado ao lazer, acesso a higiene, monitoração da saúde através de consultas e
exames, opção religiosa/espiritual, acesso aos meios de reabilitação e aos recursos
que possibilitem maior independência, obtenção de moradia digna e realização de
exercícios físicos de forma regular e sistematizada121-124.
33
Segundo um estudo de revisão sobre os benefícios dos exercícios físicos em
mulheres na pós-menopausa, realizado por Guevara et al.124, foi verificado que em se
tratando de QV, esse é um período da vida em que mudanças naturais ocorrem e com
isso consequentes prejuízos associados ao declínio na função física, resultam em
uma menor QV. Essa redução é revertida através da manutenção ou início de
exercícios que possam melhorar a força muscular e a densidade óssea, importantes
para preservação da função física e da independência funcional, contribuindo com a
melhora da QV e consequentemente com o aumento da expectativa de vida dessa
população124.
4.5 VIBRAÇÃO DE CORPO INTEIRO
A VCI é uma modalidade que passou a ser investigada apenas
recentemente31,125-128. Refere-se a uma opção de terapia que transmite vibrações
mecânicas emitidas através do corpo humano em pé, sobre uma plataforma oscilatória
sinusoidal (sinusoidal-shaped oscillations) para o sistema osteomuscular31-33. A
intensidade das vibrações é aumentada ou diminuída dependendo de diferentes
parâmetros129,130.
Os principais parâmetros são: frequência, expressa em hertz (Hz); amplitude
ou deslocamento pico a pico, expressos em milímetros (mm); magnitude da
aceleração devido à gravidade, expressa em gramas (g) ou metros por segundo ao
quadrado (m/s2); posicionamento do corpo sobre a placa vibratória; e pelo período de
tempo que o corpo recebe a vibração (minutos por sessão, frequência semanal e
meses de intervenção)31,33. O período de tempo que a pessoa recebe as vibrações,
pode ser selecionado através do cálculo da dose cumulativa de VCI, ao longo de todo
34
período de uma intervenção, multiplicando o tempo de exposição, pela frequência
semanal e pelo número de semanas129.
Segundo Rauch131, a frequência refere-se ao número de repetições dos ciclos
oscilatórios por segundo, que tipicamente varia de 15 a 60 Hz; a amplitude
corresponde à diferença entre o ponto estacionário e o maior valor atingido pela placa
oscilante, enquanto o deslocamento pico-a-pico, corresponde a todo movimento
oscilatório, do menor ao maior valor, normalmente variando de 1 a 15 mm; a
magnitude é representada pela aceleração da vibração, sendo que a aceleração é
dependente da frequência e do deslocamento pico-a-pico. A aceleração pode ser
avaliada por meio de um acelerômetro, podendo chegar até 15 g (aceleração
gravitacional, 1 g = 9,8 m/s²), ou estimada por meio da fórmula: m/s2 = 2.π2.f2.m, onde
f é a frequência em Hz e m é o deslocamento pico-a-pico expresso em metros31. A
magnitude é considerada alta, quando ≥ 1g31,32 e a frequência é considerada alta,
quando > 20 Hz45,55.
Em estudo prévio de revisão sistemática e meta-análise de ensaios clínicos
randomizados38, foi possível observar que as áreas da coluna lombar e trocânter
podem ser as mais responsivas para o aumento da DMO em mulheres na pós-
menopausa submetidas à VCI. Porém, resultados significativos somente foram
observados em análises de subgrupo, quando utilizados parâmetros potencialmente
mais adequados para VCI, como vibração de lado alternado, semi-flexão do joelho,
baixa frequência e alta magnitude. Análises de subgrupos que avaliaram estes
parâmetros demonstraram efeitos sobre a área da DMO na coluna lombar entre 0,010
g/cm2 e 0,016 g/cm2, enquanto para o trocânter a variação foi de 0,019 g/cm2 à 0,020
g/cm2.
35
Estudos de Iwamoto et al.53 e de Gusi, Raimundo e Leal52 que utilizaram baixa
frequência, alta magnitude, joelho semi-fletido e vibração do tipo lado-alternado,
encontraram melhora significativa para área da DMO nas regiões da coluna lombar e
colo do fêmur respectivamente. No entanto, seguindo estes mesmos parâmetros,
Liphardt et al.42 ao avaliarem as regiões da coluna lombar e colo do fêmur, e Beck e
Norling58 antebraço proximal, não encontraram melhora significativa da DMO. Como
a VCI possibilita diferentes parâmetros, a maior controvérsia refere-se a quais deles
seriam capazes de possibilitar maior osteogênese.
No que diz respeito ao posicionamento corporal, estudos que utilizaram joelhos
estendidos durante a VCI em sua maioria não encontraram melhoras significativas
para DMO de qualquer região corporal43,48,55, a exceção ao estudo de Lai et al.45 que
observaram efeitos significativos para DMO da coluna lombar. Por outro lado, os
estudos que utilizam joelhos semi-fletidos durante a VCI encontraram melhoras
significativas para DMO da região coluna lombar47,52,53, colo femoral52 e trocanter52.
Em relação aos tipos de vibração, existem dois principais mecanismos: as que
vibram em direção predominantemente vertical, de maneira síncrona em toda sua
base, denominadas plataformas de vibração síncrona (synchronous vibration) e as
que vibram através de um eixo antero-posterior, fazendo com que os lados direito e
esquerdo alternem horizontalmente (enquanto o pé direito se move para cima o pé
esquerdo se move para baixo, e vice-versa), denominadas plataformas de vibração
de lado alternado (side-alternating vibration)31,32.
Os vários estudos que testaram a vibração síncrona não encontraram qualquer
resultado significativo para diferentes regiões da DMO, independentemente de
frequência e magnitude43,47,55,57. Além disso, Von Stengel et al.50 ao compararem dois
tipos de vibração (síncrona e lado-alternado) verificaram que apenas o grupo de
36
mulheres na pós-menopausa submetido a vibração de lado-alternado melhorou
significativamente a DMO da coluna lombar quando comparadas com o grupo
controle.
Estudos vêm demonstrando que o treino de VCI pode ser capaz de aumentar
a atividade anabólica do tecido ósseo, assim como o tecido e a área óssea, por meio
de intervenções com duração de seis meses ou mais45-47,49-54 apesar de controvérsias
41-43,48,55-58,130. Períodos menores que seis meses, parecem não causar efeitos
significativamente positivos sobre a DMO132.
Em se tratando dos efeitos da VCI sobre a força muscular, um estudo de meta-
análise realizado por Lau et al.130 demonstrou que VCI comparada a nenhuma
intervenção melhora significativamente vários aspectos da força muscular dos
membros inferiores de adultos mais velhos. A VCI promoveu um aumento significativo
sobre a força muscular dinâmica dos extensores do joelho, força em extensão
isométrica do joelho e medidas funcionais da força muscular, como altura do salto e
desempenho no teste de sentar e levantar.
No estudo de revisão realizado por Montoro et al.133 foi demonstrado que a VCI
é um método de treinamento seguro, adequado e eficaz para aumento de força
muscular na população de adultos mais velhos do sexo feminino. Uma vantagem
refere-se ao fato da VCI poder ser realizada em casa, e servir como uma intervenção
alternativa nessa população, que normalmente não é atraída pelo exercício de
resistência tradicional ou não pode fazê-lo por causa de alguma condição médica que
limite a sua prática.
37
4.5.1 Aspectos neurofisiológicos da VCI
Segundo estudo de revisão realizado por Alguacil et al.127, a vibração mecânica
emitida pela plataforma oscilatória sinusoidal é transmitida ao longo do corpo, ativando
uma série de receptores sensoriais e musculares cutâneos, principalmente os fusos
musculares (capazes de detectar o comprimento muscular) e órgãos neurotendinosos
de Golgi (monitoram a tensão muscular), desencadeando o reflexo de vibração tônico,
responsável pela contração e relaxamento dos músculos.
Os fusos musculares apresentam papel importante nas sinapses, sendo
compostos de 3 a 12 fibras musculares finas intrafusais circundadas por uma bainha
de tecido conjuntivo, com 3 a 10 mm de comprimento. Os fusos captam informações
sensoriais e transmitem por meio de axônios do tipo 1a, os quais penetram na raiz
dorsal da medula espinhal, formando sinapses excitatórias com os interneurônios e
com os neurônios motores alfa do corno ventral da medula, gerando as contrações
musculares127,128.
O órgão tendinoso de Golgi, localizado nas inserções das fibras musculares
com os tendões, são inervados por fibras nervosas sensoriais Ib. Durante o
alongamento muscular o órgão tendinoso de Golgi é estendido e sua fibra aferente é
ativada, provocando sinal local excitatório que, por sua vez, através dos neurônios
inibitórios, relaxam o músculo, por perceber a tensão muscular e fornecendo dessa
forma, um mecanismo de realimentação negativa que impede uma excessiva tensão
muscular, podendo acarretar lesão127,128.
O uso da VCI duplica os efeitos fisiológicos (aumentando a sincronização das
unidades motoras, melhorando a coordenação entre os músculos sinergistas e
aumentando a inibição dos antagonistas) em um período curto de treinamento, sem
exigir muito esforço por parte do praticante. O alongamento repetitivo dos músculos,
38
tendões e ligamentos que ocorrem por meio do movimento vibratório, ativa o reflexo
de estiramento e aumenta o reflexo das contrações de 30 a 60 vezes por segundo, de
modo que os músculos se contraem continuamente; otimizando a coordenação de
unidades motoras e diminundo a chance de lesões musculares127.
4.5.2 Indicações e contra-indicações da VCI
O uso da VCI é indicado para melhora da flexibilidade e fortalecimento
muscular, equilíbrio postural, aumento da densidade mineral óssea, ativação da
circulação sanguínea e relaxamento muscular. Sendo contra-indicado em casos de
gravidez, alterações vasculares ou cardiovasculares graves, arritmia; utilização de
marca-passo; disfunção na retina, feridas recentes resultantes de uma operação ou
de intervenção cirúrgica, prótese nos membros inferiores ou implantes na coluna
vertebral, hérnias na coluna, discopatia, espondilólise, presença de parafusos ou
placas no corpo, tumores, quadro de epilepsia ou convulsões, labirintite ou
vertigens128.
4.6 MÉTODO PILATES
Uma opção de exercício físico que recentemente vem ganhando cada vez mais
adeptos é o método Pilates (MP)134-136. Esta técnica foi desenvolvida no início do
século XX por Joseph Hubertus Pilates com o objetivo de fortalecimento e
alongamento de todos os músculos do corpo, realizados em aparelhos específicos ou
no solo. O método envolve contrações concêntricas, excêntricas e isométricas de
todos os principais segmentos corporais, com grande enfoque na musculatura
relacionada à estabilização lombo-pélvica136-138.
39
Os exercícios selecionados para um determinado protocolo de intervenção
levam em consideração os objetivos de cada praticante. Durante a execução dos
exercícios, os praticantes buscam respeitar os princípios do método (Centro, Controle,
Concentração, Fluidez, Precisão e Respiração), que são previamente ensinados e
orientados quanto a importância139.
Wells, Kolt e Bialocerkowski140, em sua revisão sistemática sobre essa
temática, explicam que o centro diz respeito a contração dos músculos estabilizadores
da coluna (durante todos os exercícios), conhecidos no método como power house,
localizado entre o assoalho pélvico e a caixa torácica. O controle diz respeito a forma
de execução dos exercícios, que devem ser realizados através de uma boa postura e
do controle das fases concêntricas, excêntricas e isométricas, em velocidade
moderada durante a execução. A concentração, refere-se à atenção cognitiva
necessária para a execução correta dos exercícios. O princípio da fluidez, diz respeito
a transição suave dos movimentos dentro da seqüência dos exercícios, sem trancos
ou solavancos. A precisão menciona que os exercícios devem ser realizados sem
compensações corporais. Enquanto o princípio da respiração refere-se à coordenação
das fases de inspiração e de expiração profunda, que ocorrem durante o exercício.
O MP pode ser praticado em solo ou em equipamentos, neste último caso, a
sobrecarga ocorre principalmente por meio do uso de molas, que são responsáveis
por oferecer uma resistência que se altera proporcionalmente a sua extensibilidade133.
Para o aumento da sobrecarga o posicionamento das molas é alterado nos
equipamentos ou a mesma pode ser trocada por outra de maior resistência. Por outro
lado, nos exercícios de solo a modificação da sobrecarga ocorre por adaptações no
próprio movimento (realizando o exercício com grau de dificuldade maior), o que não
40
permite que a sobrecarga seja alterada de maneira sensível, como ocorre nos
equipamentos29,139.
Em relação aos potenciais efeitos osteogênicos proporcionados por este tipo
de exercício, um estudo de meta-análise26 que agrupou diferentes formas de
intervenção utilizando exercícios resistidos de maior sobrecarga e menor repetição,
encontrou aumento significativo para a área da DMO da coluna lombar (0,86%) e colo
do fêmur (1,03%), mas não para outras regiões corporais (quadril total, trocânter e
ward’s área) em mulheres na pós-menopausa. Quando agrupados estudos que
fizeram uso de exercícios resistidos utilizando uma menor sobrecarga e um maior
número de repetições nenhum resultado significativo foi observado. Apesar de
nenhum estudo dessa meta-análise ter utilizado Pilates, os exercícios resistidos que
foram citados, utilizando uma maior sobrecarga e um menor número de repetições,
assemelham-se com o modo de intervenção que comumente é realizado no MP.
Exercícios do MP tem se mostrado efetivo para atenuar os declínios
característicos do processo de envelhecimento, porém, até o momento, apenas um
ensaio clínico randomizado investigou os efeitos da técnica sobre a DMO de mulheres
na pós-menopausa. Angin, Erden e Can67 demonstraram que seis meses de Pilates
realizados três vezes por semana possibilitou aumento significativo na DMO da coluna
lombar, com grande efeito osteogênico (0,063 g/cm2), enquanto outras regiões
corporais não foram investigadas. Possivelmente o considerável efeito encontrado
pelos autores ao compararem MP com o grupo que não realizou nenhuma
intervenção, pode justificar-se pelo fato de terem incluído apenas participantes com
osteoporose. Estudos mostraram que ossos menos densos podem ter uma resposta
maior a intervenções para aumento da DMO55,141,142.
41
Outros estudos envolvendo o MP em adultos mais velhos do sexo feminino,
não avaliaram a DMO, mas observam alterações relacionadas a força muscular,
equilíbrio postural e qualidade de vida29,64,66,72,73. Em um estudo realizado por Oliveira,
Oliveira e Pires-Oliveira29 com esta população, 32 voluntárias foram randomizadas em
dois grupos de exercícios, que ocorreram duas vezes na semana por 12 semanas. O
grupo que realizou o MP apresentou melhora significativa no pico de torque isocinético
dos extensores e flexores do joelho, equilíbrio postural estático e dinâmico, além da
qualidade de vida, ao serem comparadas com o grupo que realizou exercícios de
alongamento.
Irez et al.66 realizaram um estudo com 60 voluntárias de 65 anos ou mais, que
foram separadas em dois grupos (MP e controle). Os exercícios de Pilates ocorreram
durante 12 semanas, três vezes por semana. A força muscular, equilíbrio dinâmico, e
flexibilidade foram avaliadas antes e após o programa. Para todas essas variáveis
houve melhoras significativas a favor do MP.
De acordo com estudo de revisão sistemática e meta-análise realizado por
Bullo et al.143, o MP apresentou efeitos significativos e com grande tamanho de efeito
sobre a força muscular, e qualidade de vida de adultos mais velhos, podendo ser
considerado desta forma uma modalidade de exercício físico capaz de contribuir com
a melhora destas variáveis para essa população. Observa-se que apesar dos estudos
mostrarem potencial contribuição do MP sobre as variáveis força muscular e qualidade
de vida em mulheres na pós-menopausa ou adultos mais velhos, os efeitos da técnica
sobre a DMO desta população ainda foram pouco explorados.
42
4.6.1 Indicações e contra-indicações do MP
O MP é indicado para indivíduos com diferentes condições físicas, pois os
exercícios são selecionados de acordo com as necessidades de cada praticante,
podendo ser realizadas diversas adaptações144. O Pilates é indicado para
condicionamento físico ou reabilitação, não apresentando limitação de idade145. Os
praticantes devem buscar seguir os princípios básicos para a correta realização da
técnica e obtenção dos benefícios. Muitas pessoas buscam o método para melhora
da densidade mineral óssea, força muscular e flexibilidade muscular, equilíbrio
postural, coordenação motora, consciência corporal, postura, qualidade de vida,
qualidade do sono e diminuição das dores por diversas causas144-146.
Os exercícios apresentam poucas contra-indicações, não sendo recomendado em
casos de lesões agudas, gestação de risco, indivíduos hipertensos sem controle
medicamentoso, estado febril e doenças cardiovasculares sem liberação médica146.
43
5 REFERÊNCIAS
1. Tiidus PM. Estrogen and Menopause: Muscle Damage, Repair and Function in
Females. Sex Hormones, Exercise and Women. 2017:71-85. doi: 10.1007/978-3-319-
44558-8_5.
2. Gordon JL, Eisenlohr-Moul TA, Rubinow DR, Schrubbe L, Girdler SS. Naturally
occurring changes in estradiol concentrations in the menopause transition predict
morning cortisol and negative mood in perimenopausal depression. Clin Psychol Sci.
2016,4(5):919-935. doi: 10.1177/2167702616647924.
3. Norman RL. Reproductive Changes in the Female Lifespan. The Active Female.
2014:25-31. doi: 10.1007/978-1-4614-8884-2_2.
4. Hale GE, Robertson DM, Burger HG. The perimenopausal woman: endocrinology
and management. J Steroid Biochem Mol Biol. 2014,142:121-131. doi:
10.1016/j.jsbmb.2013.08.015.
5. Levine ME, Lu AT, Chen BH, Hernandez DG, Singleton AB, Ferrucci L, et al.
Menopause accelerates biological aging. Proc Natl Acad Sci. 2016,113(33):9327-
9332. doi: 10.1073/pnas.1604558113.
6. Ikegami S, Uchiyama S, Nakamura Y, Mukaiyama K, Hirabayashi H, Kamimura M,
Kato H. Factors that characterize bone health with aging in healthy postmenopausal
women. J Bone Miner Metab. 2015,33(4):440-447. doi: 10.1007/s00774-014-0608-4.
7. Sjöblom S, Suuronen J, Rikkonen T, Honkanen R, Kröger H, Sirola J. Relationship
between postmenopausal osteoporosis and the components of clinical sarcopenia.
Maturitas. 2013,75(2):175-180. doi: 10.1016/j.maturitas.2013.03.016.
8. Tarantino U, Baldi J, Celi M, Rao C, Liuni FM, Iundusi R, et al. Osteoporosis and
sarcopenia: the connections. Aging Clin Exp Res. 2013,25(1):93-95. doi:
10.1007/s40520-013-0097-7.
44
9. Palacios S, Neyro JL, Fernandez de Cabo S, Chaves J, Rejas J. Impact of
osteoporosis and bone fracture on health-related quality of life in postmenopausal
women. Climacteric. 2014,17(1):60-70. doi: 10.3109/13697137.2013.808182.
10. Guillemin F, Martinez L, Calvert M, Cooper C, Ganiats T, Gitlin M, Tosteson A.
Fear of falling, fracture history, and comorbidities are associated with health-related
quality of life among European and US women with osteoporosis in a large
international study. Osteoporos Int. 2013,24(12):3001-3010. doi: 10.1007/s00198-013-
2408-4.
11. Liberman K, Forti LN, Beyer I, Bautmans I. The effects of exercise on muscle
strength, body composition, physical functioning and the inflammatory profile of older
adults: a systematic review. Curr Opin Clin Nutr Metab Care. 2017,20(1):30-53. doi:
10.1097/MCO.0000000000000335.
12. Bolam KA, Van Uffelen JG, Taaffe DR. The effect of physical exercise on bone
density in middle-aged and older men: a systematic review. Osteoporos Int.
2013,24(11):2749-2762. doi: 10.1007/s00198-013-2346-1.
13. Eriksen EF, Díez-Pérez A, Boonen S. Update on long-term treatment with
bisphosphonates for postmenopausal osteoporosis: a systematic review. Bone.
2014,58:126-135. doi: 10.1016/j.bone.2013.09.023.
14. Gambacciani M, Levancini M. Hormone replacement therapy and the prevention
of postmenopausal osteoporosis. Prz Menopauzalny. 2014,13(4):213-220. doi:
10.5114/pm.2014.44996.
15. De Villiers TJ, Pines A, Panay N, Gambacciani M, Archer DF, Baber RJ, Davis SR,
Gompel AA, Henderson VW, Langer R, Lobo RA, Plu-Bureau G, Sturdee DW. Updated
2013 International Menopause Society recommendations on menopausal hormone
45
therapy and preventive strategies for midlife health. Climacteric. 2013,16(3):316-337.
doi: 10.3109/13697137.2013.795683.
16. Panay N, Hamoda H, Arya R, Savvas M. The 2013 British menopause society &
women’s health concern recommendations on hormone replacement therapy.
Menopause Int. 2013,19(2):59-68. doi: 10.1177/1754045313489645.
17. Hiligsmann M, Evers SM, Sedrine WB, Kanis JA, Ramaekers B, Reginster JY,
Silverman S, Wyers CE, Boonen A. A systematic review of cost-effectiveness analyses
of drugs for postmenopausal osteoporosis. Pharmacoeconomics. 2015,33(3):205-224.
doi: 10.1007/s40273-014-0231-1.
18. Yamamoto M, Sugimoto T. Effects of growth hormone replacement therapy on
bone metabolism. Clinical Calcium. 2014,24(6):903-909. doi: CliCa1406903909.
19. Marjoribanks J, Farquhar C, Roberts H, Lethaby A, Lee J. Long‐term hormone
therapy for perimenopausal and postmenopausal women. Cochrane Database Syst
Rev. 2017. doi: 10.1002/14651858.CD004143.
20. Rahim F. Commentary on a Cochrane Review of Hormone Therapy for Preventing
Cardiovascular Disease in Postmenopausal Women. Nurs Womens Health.
2017,21(1):9-11. doi: 10.1016/j.nwh.2016.12.003.
21. Sood R, Faubion SS, Kuhle CL, Thielen JM, Shuster LT. Prescribing menopausal
hormone therapy: an evidence-based approach. Int J Womens Health. 2014,6:47-57.
doi: 10.2147/IJWH.S38342.
22. Canonico M, Carcaillon L, Plu-Bureau G, Oger E, Singh-Manoux A, Tubert-Bitter,
Elbaz A, Scarabin PY. Postmenopausal Hormone Therapy and Risk of Stroke. Stroke.
2016,47(7):1734-1741. doi: 10.1161/STROKEAHA.116.013052.
23. Karinkanta S. Exercise: a comprehensive tool for ageing women to take care of
their health. Menopause. 2017,24(1):7-8. doi: 10.1097/GME.0000000000000799.
46
24. Kemmler W, Kohl M, Von Stengel S. Long-term effects of exercise in
postmenopausal women: 16-year results of the Erlangen Fitness and Osteoporosis
Prevention Study (EFOPS). Menopause. 2017,24(1):45-51. doi:
10.1097/GME.0000000000000720.
25. Giangregorio L, El-Kotob R. Exercise, muscle, and the applied load-bone strength
balance. Osteoporos Int. 2017:1-13. doi: 10.1007/s00198-016-3780-7.
26. Howe TE, Shea B, Dawson LJ, Downie F, Murray A, Ross C, et al. Exercise for
preventing and treating osteoporosis in postmenopausal women. Cochrane Database
Syst Rev. 2011,7:1-160. doi: 10.1002/14651858.CD000333.pub2.
27. Otero M, Esain I, González-Suarez ÁM, Gil SM. The effectiveness of a basic
exercise intervention to improve strength and balance in women with osteoporosis.
Clin Interv Aging. 2017,14(12):505-513. doi: 10.2147/CIA.S127233.
28. El Mohsen AMA, El Ghaffar HEFA, Nassif NS, Elhafez GM. The weight-bearing
exercise for better balance program improves strength and balance in osteopenia: a
randomized controlled trial. J Phys Ther Sci. 2016,28(9):2576-2580. doi:
10.1589/jpts.28.2576.
29. Oliveira LC, Oliveira RG, Pires-Oliveira DAA. Effects of Pilates on muscle strength,
postural balance and quality of life of older adults: a randomized, controlled, clinical
trial. J Phys Ther Sci. 2015,27(3):871-876. doi: 10.1589/jpts.27.871.
30. Moreira LDF, Oliveira MLD, Lirani-Galvão AP, Marin-Mio RV, Santos RND,
Lazaretti-Castro M. Physical exercise and osteoporosis: effects of different types of
exercises on bone and physical function of postmenopausal women. Arq Bras
Endocrinol Metabol. 2014,58(5):514-522. doi: 10.1590/0004-2730000003374.
31. Rauch F, Sievanen H, Boonen S, Cardinale M, Degens H, Felsenberg D, Roth J,
Schoenau E, Verschueren S, Rittweger J. Reporting whole-body vibration intervention
47
studies: recommendations of the International Society of Musculoskeletal and
Neuronal Interactions. J Musculoskelet Neuronal Interact. 2010,10:193-198.
32. Christiansen BA, Silva MJ. The effect of varying magnitudes of whole-body
vibration on several skeletal sites in mice. Ann Biomed Eng. 2006,34:1149-1156. doi:
10.1007/s10439-006-9133-5.
33. Wysocki A, Butler M, Shamliyan T, Kane RL. Whole-body vibration therapy for
osteoporosis: state of the science. Ann Intern Med. 2011,155:680-686. doi:
10.7326/0003-4819-155-10-201111150-00006.
34. Kiel DP, Hannan MT, Barton BA, Bouxsein ML, Sisson E, Lang T, et al. Low-
magnitude mechanical stimulation to improve bone density in persons of advanced
age: a randomized, placebo-controlled trial. J Bone Miner Res. 2015,30:1319-1328.
doi: 10.1002/jbmr.2448.
35. Ma C, Liu A, Sun M, Zhu H, Wu H. Effect of whole-body vibration on reduction of
bone loss and fall prevention in postmenopausal women: a meta-analysis and
systematic review. J Orthop Surg Res. 2016,11(1):24. doi: 10.1186/s13018-016-0357-
2.
36. Fratini A, Bonci T, Bull AM. Whole Body Vibration Treatments in Postmenopausal
Women Can Improve Bone Mineral Density: Results of a Stimulus Focussed Meta-
Analysis. PloS one. 2016,11(12):e0166774. doi: 10.1371/journal.pone.0166774.
37. Xu J, Lombardi G, Jiao W, Banfi G. Effects of exercise on bone status in female
subjects, from young girls to postmenopausal women: an overview of systematic
reviews and meta-analyses. Sports Med. 2016,46(8):1165-1182. doi: 10.1007/s40279
016-0494-0.
48
38. Oliveira LC, Oliveira RG, Pires-Oliveira DAA. Effects of whole body vibration on
bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporos Int. 2016,27(10):2913-2933. doi: 10.1007/s00198-016-3618-3.
39. Dionello CF, Sá-Caputo D, Pereira HVFS, Sousa-Gonçalves CR, Maiworm AI,
Morel DS. et al. Effects of whole body vibration exercises on bone mineral density of
women with postmenopausal osteoporosis without medications: novel findings and
literature review. J Musculoskelet Neuronal Interact. 2016,16(3):193.
40. Luo X, Zhang J, Zhang C, He C, Wang P. The effect of whole-body vibration
therapy on bone metabolism, motor function, and anthropometric parameters in
women with postmenopausal osteoporosis. Disability and Rehabilitation. 2016,1-9.
doi: 10.1080/09638288.2016.1226417.
41. Santin-Medeiros F, Santos-Lozano A, Rey-López JP, Garatachea N. Effects of
eight months of whole body vibration training on hip bone mass in older women. Nutr
Hosp. 2015,31:1654-1659. doi: 10.3305/nh.2015.31.4.8441.
42. Liphardt AM, Schipilow J, Hanley DA, Boyd SK. Bone quality in osteopenic
postmenopausal women is not improved after 12 months of whole-body vibration
training. Osteoporos Int. 2015,26:911-920. doi: 10.1007/s00198-014-2995-8.
43. Leung KS, Li CY, Tse YK, Choy TK, Leung PC, Hung VWY, Chan SY, Leung AH,
Cheung WH. Effects of 18-month low-magnitude high-frequency vibration on fall rate
and fracture risks in 710 community elderly - a cluster - randomized controlled trial.
Osteoporos Int. 2014,25:1785-1795. doi: 10.1007/s00198-014-2693-6.
44. Zaki ME. Effects of whole body vibration and resistance training on bone mineral
density and anthropometry in obese postmenopausal women. J Osteoporos.
2014,702589. doi: 10.1155/2014/702589.
49
45. Lai CL, Tseng SY, Chen CN, Liao WC, Wang CH, Lee MC, Hsu PS. Effect of 6
months of whole body vibration on lumbar spine bone density in postmenopausal
women: a randomized controlled trial. Clin Interv Aging. 2013,8:1603-1609. doi:
10.2147/CIA.S53591.
46. Stolzenberg N, Belavý DL, Beller G, Armbrecht G, Semler J, Felsenberg D. Bone
strength and density via pQCT in postmenopausal osteopenic women after 9 months
resistive exercise with whole body vibration or proprioceptive exercise. J
Musculoskelet Neuronal Interact. 2013,13:66-76.
47. Karakiriou SK, Douda HT, Smilios IG, Volaklis KA, Tokmakidis SP. Effects of
vibration and exercise training on bonemineral density and muscle strength in post-
menopausal women. Eur J Sport Sci. 2012,12:81-88. doi:
10.1080/17461391.2010.536581.
48. Slatkovska L, Alibhai SMH, Beyene J, Hu H, Demaras A, Cheung AM. Effect of
12months of whole-body vibration therapy on bone density and structure in
postmenopausal women. A randomized trial. Ann Intern Med. 2011,155:668-679. doi:
10.7326/0003-4819-155-10-201111150-00005.
49. Verschueren SMP, Bogaerts A, Delecluse C, Claessens AL, Haentjens P,
Vanderschueren D, et al. The effects of whole-body vibration training and vitamin D
supplementation on muscle strength, muscle mass, and bone density in
institutionalized elderly women: a 6-month randomized, controlled trial. J Bone Miner
Res. 2011,26:42-49. doi: 10.1002/jbmr.181.
50. Von Stengel S, Kemmler W, Bebenek M, Engelke K, Kalender WA. Effects of
whole-body vibration training on different devices on bone mineral density. Med Sci
Sports Exerc. 2011,43:1071-1079. doi: 10.1249/MSS.0b013e318202f3d3.
50
51. Von Stengel S, Kemmler W, Engelke K, Kalender WA. Effects of whole body
vibration on bone mineral density and falls: results of the randomized controlled ELVIS
study with postmenopausal women. Osteoporos Int. 2011,22:317-325. doi:
10.1007/s00198-010-1215-4.
52. Gusi N, Raimundo A, Leal A. Low-frequency vibratory exercise reduces the risk of
bone fracture more than walking: a randomized controlled trial. BMC Musculoskelet
Disord. 2006,7:92. doi: 10.1186/1471-2474-7-92.
53. Iwamoto J, Takeda T, Sato Y, Uzawa M. Effect of whole body vibration exercise
on lumbar bone mineral density, bone turnover, and chronic back pain in post-
menopausal osteoporotic women treated with alendronate. Aging Clin Exp Res.
2005,17:157-163. doi: 10.1007/BF03324589.
54. Verschueren SMP, Roelants M, Delecluse C, Swinnen S, Vanderschueren D,
Boonen S. Effect of 6-month whole body vibration training on hip density, muscle
strength, and postural control in postmenopausal women: a randomized controlled pilot
study. J Bone Miner Res. 2004,19:352-359. doi: 10.1359/JBMR.0301245.
55. Rubin C, Recker R, Cullen D, Ryaby J, McCabe J, McLeod K. Prevention of
postmenopausal bone loss by a low-magnitude, high-frequency mechanical stimuli: a
clinical trial assessing compliance, efficacy, and safety. J Bone Miner Res.
2004,19:343-351. doi: 10.1359/JBMR.0301251.
56. Russo CR, Lauretani F, Bandinelli S, Bartali B, Cavazzini C, Guralnik JM, Ferrucci
L. High-frequency vibration training increases muscle power in postmenopausal
women. Arch Phys Med Rehabil. 2003,84:1854-1857. doi: 10.1016/S0003-
9993(03)00357-5.
57. Slatkovska L, Beyene J, Alibhai SMH, Wong Q, Sohail QZ, Cheung AM. Effect of
whole-body vibration on calcaneal quantitative ultrasound measurements in
51
postmenopausal women: a randomized controlled trial. Calcif Tissue Int. 2014,95:547-
556. doi: 10.1007/s00223-014-9920-1.
58. Beck BR, Norling TL. The effect of eight months of twice weekly low or higher
intensity whole body vibration on risk factors for postmenopausal hip fracture. Am J
Phys Med Rehabil. 2010,89:997-1009. doi: 10.1097/PHM.0b013e3181f71063.
59. Bemben DA, Palmer IJ, Bemben MG, Knehans AW. Effects of combined whole-
body vibration and resistance training on muscular strength and bone metabolism in
postmenopausal women. Bone. 2010,47:650-656. doi: 10.1016/j.bone.2010.06.019.
60. Lam FM, Lau RW, Chung RC, Pang MY. The effect of whole body vibration on
balance, mobility and falls in older adults: a systematic review and meta-
analysis. Maturitas. 2012,72(3):206-213. doi: 10.1016/j.maturitas.2012.04.009.
61. Dutra MC, Oliveira ML, Marin RV, Kleine HC, Silva OL, Lazaretti-Castro M. Whole-
body vibration improves neuromuscular parameters and functional capacity in
osteopenic postmenopausal women. Menopause. 2016,23(8):870-875. doi:
10.1097/GME.0000000000000644.
62. Luo X, Zhang J, Zhang C, He C, Wang P. The effect of whole-body vibration
therapy on bone metabolism, motor function, and anthropometric parameters in
women with postmenopausal osteoporosis. Disabil Rehabil. 2016.10:1-9. doi:
10.1080/09638288.2016.1226417.
63. Marin-Cascales E, Alcaraz PE, Rubio-Arias JA. Effects of 24 weeks of Whole Body
Vibration vs. Multi-component training on Muscle Strength and Body Composition in
Postmenopausal Women: a randomized controlled trial. Rejuvenation Res. 2016. doi:
10.1089/rej.2016.1877.
52
64. Cancela JM, Oliveira IM, Rodríguez-Fuentes G. Effects of Pilates method in
physical fitness on older adults. A systematic review. Eur Rev Aging Phys Act.
2014,11(2):81-94. doi: 10.1007/s11556-014-0143-2.
65. Oliveira LC, Oliveira RG, Pires-Oliveira DAA. Effects of Pilates on muscle strength,
postural balance and quality of life of older adults: a randomized, controlled, clinical
trial. J Phys Ther Sci. 2015,27(3):871-876. doi: 10.1589/jpts.27.871.
66. Irez GB, Ozdemir RA, Evin R, Irez SG, Korkusuz F. Integrating Pilates exercise
into an exercise program for 65+ year-old women to reduce falls. J Sports Sci Med.
2011,10(1):105-111.
67. Angın E, Erden Z, Can F. The effects of clinical pilates exercises on bone mineral
density, physical performance and quality of life of women with postmenopausal
osteoporosis. J Back Musculoskelet Rehabil. 2015,28(4): 849-858. doi: 10.3233/BMR-
150604.
68. Fourie M, Gildenhuys GM, Shaw I, Shaw BS, Toriola AL, Goon DT. Effects of a
mat Pilates programme on muscular strength and endurance in elderly women:
exercise physiology. African J Phys Heal Educ Rec Dance. 2012,18(2):299-307.
69. Vieira ND, Testa DRPC, Fátima ST, Catai AM, Melo RC. The effects of 12 weeks
Pilates-inspired exercise training on functional performance in older women: A
randomized clinical trial. J Bodyw Mov Ther. 2016. doi: 10.1016/j.jbmt.2016.06.010.
70. Kao YH, Liou TH, Huang YC, Tsai YW, Wang KM. Effects of a 12-week Pilates
course on lower limb muscle strength and trunk flexibility in women living in the
community. Health Care Women Int. 2015;36(3):303-319. doi:
10.1080/07399332.2014.900062.
71. Cruz-Ferreira A, Fernandes J, Gomes D, Bernardo LM, Kirkcaldy BD, Barbosa TM,
Silva A. Effects of Pilates-based exercise on life satisfaction, physical self-concept and
53
health status in adult women. Women Health. 2011,51(3):240-255. doi:
10.1080/03630242.2011.563417.
72. Küçükçakır N, Altan L, Korkmaz N. Effects of Pilates exercises on pain, functional
status and quality of life in women with postmenopausal osteoporosis. J Bodyw Mov
Ther. 2013,17(2):204-211. doi: 10.1016/j.jbmt.2012.07.003.
73. Rodríguez-Fuentes G, Oliveira IM, Ogando-Berea H, Otero-Gargamala MD. An
observational study on the effects of Pilates on quality of life in women during
menopause. Eur J Int Med. 2014,6(6):631-636. doi: 10.1016/j.eujim.2014.08.003.
74. Blumel JE, Lavín P, Vallejo MS, Sarrá S. Menopause or climacteric, just a semantic
discussion or has it clinical implications? Climacteric. 2014,17(3):235-241. doi:
10.3109/13697137.2013.838948.
75. Muka T, Oliver-Williams C, Kunutsor S, Laven JS, Fauser BC, Chowdhury R, et al.
Association of age at onset of menopause and time since onset of menopause with
cardiovascular outcomes, intermediate vascular traits, and all-cause mortality: a
systematic review and meta-analysis. Jama Cardiol. 2016,1(7):767-776. doi:
10.1001/jamacardio.2016.2415.
76. Schoenaker DA, Jackson CA, Rowlands JV, Mishra GD. Socioeconomic position,
lifestyle factors and age at natural menopause: a systematic review and meta-analyses
of studies across six continents. Int J Epidemiol. 2014,43(5):1542-1562. doi:
10.1093/ije/dyu094.
77. Gold EB, Crawford SL, Avis NE, Crandall CJ, Matthews KA, Waetjen LE, Lee JS,
Thurston R, Vuga M, Harlow SD. Factors related to age at natural menopause:
longitudinal analyses from SWAN. Am J Epidemiol. 2013,kws421. doi:
10.1093/aje/kws421.
54
78. Wira CR, Rodriguez-Garcia M, Patel MV. The role of sex hormones in immune
protection of the female reproductive tract. Nat Rev Immunol. 2015,15(4):217-230. doi:
10.1038/nri3819.
79. Puts DA, Bailey DH, Cárdenas RA, Burriss RP, Welling LL, Wheatley JR, Dawood
K. Women's attractiveness changes with estradiol and progesterone across the
ovulatory cycle. Horm Behav. 2013,63(1):13-19. doi: 10.1016/j.yhbeh.2012.11.007.
80.Stachenfeld NS. Hormonal changes during menopause and the impact on fluid
regulation. Reprod Sci. 2014,21(5):555-561. doi: 10.1177/1933719113518992.
81. Al-Safi ZA, Santoro N. Menopausal hormone therapy and menopausal symptoms.
Fertil Steril. 2014,101(4):905-915. doi: 10.1016/j.fertnstert.2014.02.032.
82. Stuenkel CA, Davis SR, Gompel A, Lumsden MA, Murad MH, Pinkerton JV, Santen
RJ. Treatment of symptoms of the menopause: an endocrine society clinical practice
guideline. J Clin Endocrinol Metab. 2015,100(11):3975-4011. doi: 10.1210/jc.2015-
2236.
83. Kochi MN, Marques NR, Costa GDC, Reis JG, Paula FJA, Ferreira CHJ, Abreu,
DCC. Impact of First 10 Years of Post Menopause on Muscle Function, Muscle Mass
and Bone Mineral Density in Adult Women. J Osteoporos Phys Act. 2015,3(3):1-5. doi:
10.4172/2329-9509.1000151.
84. Dasgupta D, Ray S. Is menopausal status related to women’s attitudes toward
menopause and aging? Women Health. 2016,3:1-18. doi:
10.1080/03630242.2016.1160965.
85. Ikeda K, Takeshita S. Factors and mechanisms involved in the coupling from bone
resorption to formation: how osteoclasts talk to osteoblasts. J Bone Metab.
2014,21(3):163-167. doi: 10.11005/jbm.2014.21.3.163.
55
86. Chen X, Wang Z, Duan N, Zhu G, Schwarz EM, Xie C. Osteoblast-Osteoclast
interactions. Con Tis Res. 2017.
87. Nabavi N, Khandani A, Camirand A, Harrison RE. Effects of microgravity on
osteoclast bone resorption and osteoblast cytoskeletal organization and adhesion.
Bone. 2011,49(5):965-974. doi: 10.1016/j.bone.2011.07.036.
88. Razi H, Birkhold AI, Weinkamer R, Duda GN, Willie BM, Checa S. Aging leads to
a dysregulation in mechanically driven bone formation and resorption. J Bone Miner
Res. 2015,30(10):1864-1873. doi: 10.1002/jbmr.2528.
89. Bakker CM, Tseng WJ, Li Y, Zhao H, Liu XS. Clinical Evaluation of Bone Strength
and Fracture Risk. Curr Osteoporos Rep. 2017,15(1):32-42. doi: 10.1007/s11914-017-
0346-3.
90. Sheu A, Diamond T. Diagnostic tests: Bone mineral density: testing for
osteoporosis. Aust Prescr. 2016,39(2):35-39. doi: 10.18773/austprescr.2016.020.
91. Lappe JM, Watson P, Gilsanz V, Hangartner T, Kalkwarf HJ, Oberfield S, Zemel
B. The longitudinal effects of physical activity and dietary calcium on bone mass
accrual across stages of pubertal development. J Bone Miner Res. 2015,30(1):156-
164. doi: 10.1002 / jbmr.2319.
92. Bielemann RM, Martinez-Mesa J, Gigante DP. Physical activity during life course
and bone mass: a systematic review of methods and findings from cohort studies with
young adults. BMC Musculoskelet Disord. 2013,14(1):77. doi: 10.1186/1471-2474-14-
77.
93. Xu Y, Xu Y, Ding Z, Chen Y, Su B, Ma Z, Sun YN. Correlation between ultrasonic
power spectrum and bone density on the heel. Ultrasonics. 2017,73:77-81. doi:
10.1016/j.ultras.2016.08.023.
56
94. Alvarenga JC, Fuller H, Pasoto SG, Pereira RMR. Age-related reference curves of
volumetric bone density, structure, and biomechanical parameters adjusted for weight
and height in a population of healthy women: an HR-pQCT study. Osteoporos Int.
2016,1-12. doi: 10.1007/s00198-016-3876-0.
95. Uddin MF, Islam SMM, Khan MN, Khatun R, Biman TA, Ahasan MM, Akter S,
Monika AN. Bone Mineral Densitometry (BMD) Precision and Scattered Radiation
Level of Dual Energy X-ray Absorptiometry (DXA) Installed in Mymensingh Nuclear
Medicine Unit, Bangladesh. Univer J Med Sci. 2016,4(2):65-68. doi:
10.13189/ujmsj.2016.040202.
96. Lewiecki EM, Binkley N, Morgan SL, Shuhart CR, Camargos BM, Carey JJ, Gordon
CM, Jankowski LG, Lee JK, Leslie WD. Best practices for dual-energy X-ray
absorptiometry measurement and reporting: International Society for Clinical
Densitometry Guidance. J Clin Densitom. 2016,19(2):127-140. doi:
10.1016/j.jocd.2016.03.003.
97. Patil R, Uusi-Rasi K, Pasanen M, Kannus P, Karinkanta S, Sievänen H. Sarcopenia
and osteopenia among 70–80-year-old home-dwelling Finnish women: prevalence and
association with functional performance. Osteoporos Int. 2013,24(3):787-796. doi:
10.1007/s00198-012-2046-2.
98. Greene LW. Ethics in Osteoporosis and Osteopenia: The bare bones of a surrogate
marker. Ethic Biol Eng Med Int J. 2014,5(4):353-364.
99. Iida T, Chikamura C, Aoi S, Ikeda H, Matsuda Y, Oguri Y, Ono Y, Katada K, Ishizaki
F. A study on the validity of quantitative ultrasonic measurement used the bone mineral
density values on dual-energy X-ray absorptiometry in young and in middle-aged or
older women. Radiol Phys Technol. 2010,3(2):113-119. doi: 10.1007/s12194-010-
0086-x.
57
100. Behrens M, Felser S, Mau-Moeller A, Weippert M, Pollex J, Skripitz R, Herlyn PK,
Fischer DC, Bruhn S, Schober HC, Zschorlich V, Mittlmeier T. The Bindex(®)
ultrasound device: reliability of cortical bone thickness measures and their relationship
to regional bone mineral density. Physiol Meas. 2016,37(9):1528-1540. doi:
10.1088/0967-3334/37/9/1528.
101. Lee SY, Kwon SS, Kim HS, Yoo JH, Kim J, Kim JY, Min BC, Moon SJ, Sung KH.
Reliability and validity of lower extremity computed tomography as a screening tool for
osteoporosis. Osteoporos Int. 2015,26(4):1387-94. doi: 10.1007/s00198-014-3013-x.
102. ZACK MK. Reliability and Validity of body composition and bone mineral density
measurements by DXA. Thesis submitted to the Graduate Faculty of Virginia
Polytechnic Institute and State University in partial fulfillment of the requirements for
the degree of Master of Science in Human Nutrition, Foods, and Exercise. 2002.
Blacksburg, Virginia.
103. Cosman F, De Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, Lindsay
R. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int.
2014,25(10):2359-2381. doi: 10.1007/s00198-014-2794-2.
104. Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures.
Lancet. 2002,359(9319):1761-1767. doi: 10.1016/S0140-6736(02)08657-9.
105. Siqueira FV, Facchini LA, Hallal PC. The burden of fractures in Brazil: a
population-based study. Bone. 2005,37(2):261-266. doi: 10.1016/j.bone.2005.04.002.
106. Costa ALD, Silva MACN, Brito LMO, Nascimento ACB, Barbosa MDCL, Batista
JE, et al. Osteoporose na atenção primária: uma oportunidade para abordar os fatores
de risco. Rev Bras Reumatol. 2016,56(2):111-116. doi: 10.1016/j.rbr.2015.03.004.
58
107. Wade SW, Strader C, Fitzpatrick LA, Anthony MS, O’Malley CD. Estimating
prevalence of osteoporosis: examples from industrialized countries. Arch Osteoporos.
2014,9(1):182. doi: 10.1007/s11657-014-0182-3.
108. Baccaro LF, Conde DM, Costa-Paiva L, Pinto-Neto AM. The epidemiology and
management of postmenopausal osteoporosis: a viewpoint from Brazil. Clin Interv
Aging. 2015,10:583-591. doi: 10.2147/CIA.S54614.
109. Baccaro LF, de Souza Santos Machado V, Costa-Paiva L, Sousa MH, Osis MJ,
Pinto-Neto AM. Factors associated with osteoporosis in Brazilian women: a population-
based household survey. Arch Osteoporos. 2013, 8:138. doi: 10.1007/s11657-013-
0138-z. Epub 2013 Apr 11.
110. Pinheiro MM, Ciconelli RM, Jacques NO, Genaro PS, Martini LA, Ferraz MB. O
impacto da osteoporose no Brasil: dados regionais das fraturas em homens e
mulheres adultos – The Brazilian Osteoporosis Study (BRAZOS). Rev Bras Reumatol.
2010,50(2):113-120.
111. Siris ES, Adler R, Bilezikian J, Bolognese M, Dawson-Hughes B, Favus MJ, et al.
The clinical diagnosis of osteoporosis: a position statement from the National Bone
Health Alliance Working Group. Osteoporos Int. 2014,25(5):1439-1443. doi:
10.1007/s00198-014-2655-z.
112. Alarkawi D, Bliuc D, Nguyen TV, Eisman JA, Center JR. Contribution of Lumbar
Spine BMD to Fracture Risk in Individuals With T‐Score Discordance. J Bone Miner
Res. 2016,31(2):274-280. doi: 10.1002/jbmr.2611.
113. Seeman E. Pathogenesis of bone fragility in women and men. Lancet. 2002,
359(9320):1841-1850. doi: 10.1016/S0140-6736(02)08706-8.
59
114. Melton LJ, Chrischilles EA, Cooper C, Lane AW, Riggs BL. How many women
have osteoporosis? J Bone Miner Res. 2005,20(5):886-892. doi:
10.1359/jbmr.2005.20.5.886.
115. Parker SE, Troisi R, Wise LA, Palmer JR, Titus-Ernstoff L, Strohsnitter WC, Hatch
EE. Menarche, menopause, years of menstruation, and the incidence of osteoporosis:
the influence of prenatal exposure to diethylstilbestrol. J Clin Endocrinol Metab. 2013,
99(2):594-601. doi: 10.1210/jc.2013-2954.
116. Lorentzon M, Cummings SR. Osteoporosis: the evolution of a diagnosis. J Intern
Med. 2015,277(6):650-661. doi: 10.1111/joim.12369.
117. Reginster JY, Beaudart C, Buckinx F, Bruyère O. Osteoporosis and sarcopenia:
two diseases or one? Curr Opin Clin Nutr Metab Care. 2016,19(1):31-36. doi:
10.1097/MCO.0000000000000230.
118. Kull M, Kallikorm R, Lember M. Impact of a new sarco-osteopenia definition on
health-related quality of life in a population-based cohort in Northern Europe. J Clin
Densitom. 2012,15(1):32-38. doi: 10.1016/j.jocd.2011.08.007.
119. Schaap LA, Koster A, Visser M. Adiposity, muscle mass, and muscle strength in
relation to functional decline in older persons. Epidemiol Rev. 2013,35(1):51-65. doi:
10.1093/epirev/mxs006.
120. Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M. Sarcopenia,
dynapenia, and the impact of advancing age on human skeletal muscle size and
strength; a quantitative review. Front Physiol. 2012,11(3):260. doi:
10.3389/fphys.2012.00260.
121. Caputo EL, Costa MZ. Influence of physical activity on quality of life in
postmenopausal women with osteoporosis. Rev Bras Reumatol. 2014,54(6):467-473.
doi: 10.1016/j.rbr.2014.02.008.
60
122. Jenabi E, Shobeiri F, Hazavehei SM, Roshanaei G. Assessment of Questionnaire
Measuring Quality of Life in Menopausal Women: A Systematic Review. Oman Med J.
2015,30(3):151-156. doi: 10.5001/omj.2015.34.
123. Dantas RAS, Sawada NO, Malerbo MB. Pesquisas sobre qualidade de vida:
revisão da produção científica das universidades públicas do Estado de São Paulo.
Rev Latino-Am Enfermagem. 2003, 11(4):532-538.
124. Mendoza N, De Teresa C, Cano A, Godoy D, Hita-Contreras F, Lapotka M,
Llaneza P, Manonelles P, Martínez-Amat A, Ocón O, Rodríguez-Alcalá L, Vélez M,
Sánchez-Borrego R. Benefits of physical exercise in postmenopausal women.
Maturitas. 2016,93:83-88. doi: 10.1016/j.maturitas.2016.04.017.
125. Liphardt AM, Schipilow J, Hanley DA, Boyd SK. Bone quality in osteopenic
postmenopausal women is not improved after 12 months of whole-body vibration
training. Osteoporos Int. 2015,26:911-920. doi: 10.1007/s00198-014-2995-8.
126. Beck BR, Norling TL. The effect of eight months of twiceweekly low or higher
intensity whole body vibration on risk factors for postmenopausal hip fracture. Am J
Phys Med Rehabil. 2010,89:997-1009. doi: 10.1097/PHM.0b013e3181f71063.
127. Alguacil IM, Conches MG, Fraile AM, Morales M. Plataformas vibratorias: bases
neurofisiológicas, efectos fisiológicos y aplicaciones terapêuticas. Arch Med Deporte.
2009,26:119-129.
128. Amaral PC, Pécora WC. Plataforma vibratória: Introdução ao treinamento
vibratório. 2012,1ª Ed. 97p. São Paulo. Editora Paulo Costa Amaral. São Paulo. ISBN:
9788591315901.
129. Slatkovska L, Alibhai SMH, Beyene J, Cheung AM. Effect of whole-body vibration
on BMD: a systematic review and meta-analysis. Osteoporos Int. 2010,21:1969-1980.
doi: 10.1007/s00198-010-1228-z.
61
130. Lau RWK, Liao LR, Yu F, Teo T, Chung RCK, Pang MYC. The effects of whole
body vibration Therapy on bone mineral density and leg muscle strength in older
adults: A systematic review and meta-analysis. Clin Rehabil. 2011,25:975:988. doi:
10.1177/0269215511405078.
131. Rauch F. Vibration Therapy. Dev Med Child Neurol. 2009,51:166-168. doi:
10.1111/j.1469-8749.2009.03418.x.
132. Gómez-Cabello A, González-Agüero A, Morales S, Ara I, Casajús JA, Vicente-
Rodríguez G. Effects of a short-term whole body vibration intervention on bone mass
and structure in elderly people. J Sci Med Sport. 2014,17(2):160-164. doi:
10.1016/j.jsams.2013.04.020.
133. Montoro MVP, Montilla JAP, Aguilera EL, Checa MA. El entrenamiento vibratorio
como intervención en la sarcopenia: repercusiones en el sistema neuromuscular de
los adultos mayores. Nutr Hosp. 2015,32(n04):1454-1461. doi:
10.3305/nh.2015.32.4.9505.
134. Granacher U, Gollhofer A, Hortobágyi T, Kressig RW, Muehlbauer T. The
importance of trunk muscle strength for balance, functional performance, and fall
prevention in seniors: a systematic review. Sports Med. 2013,43:627-41. doi:
10.1007/s40279-013-0041-1.
135. Ferrreira CB, Aidar FJ, Novaes GDS, Vianna JM, Carneiro AL, Menezes LDS. O
método Pilates sobre a resistência muscular localizada em mulheres adultas. Motri.
2007,3(4):76-81.
136. Marés G, Oliveira KBD, Piazza MC, Preis C, Bertassoni Neto L. A importância da
estabilização central no método Pilates: uma revisão sistemática. Fisioter Mov. 2012,
25(2):445-51. doi: 10.1590/S0103-51502012000200022.
62
137. Parikh CM, Arora M. Role of Pilates in rehabilitation: A literature review. Inter J
Ther Rehabil Res. 2016,5(4):77-83. doi: 10.5455/ijtrr.000000148.
138. Phrompaet S, Paungmali A, Pirunsan U, Sitilertpisan P. Effects of pilates training
on lumbo-pelvic stability and flexibility. Asian J Sports Med. 2011,2(1):16-22.
139. Oliveira LC, Pires-Oliveira DAA, Abucarub AC, Oliveira LS, Oliveira RG. Pilates
increases isokinetic muscular strength of the elbow flexor and extensor muscles of
older women: A randomized controlled clinical trial. J Bodyw Mov Ther. 2017,21(1):2-
10. doi: 10.1016/j.jbmt.2016.03.002.
140. Wells C, Kolt GS, Bialocerkowski A. Defining Pilates exercise: a systematic
review. Complement Ther Med. 2012,20(4):253-262. doi: 10.1016/j.ctim.2012.02.005.
141. Flieger J, Karachalios T, Khaldi L, Raptou P, Lyritis G. Mechanical stimulation in
the form of vibration prevents postmenopausal bone loss in ovariectomized rats. Calcif
Tissue Int. 1998,63:510-514. doi: 10.1007/s002239900566.
142. Judex S, Donahue LR, Rubin C. Genetic predisposition to low bone mass is
paralleled by an enhanced sensitivity to signals anabolic to the skeleton. FASEB J.
2002,16:1280-1282. doi: 10.1096/fj.01-0913fje.
143. Bullo V, Bergamin M, Gobbo S, Sieverdes JC, Zaccaria M, Neunhaeuserer D,
Ermolao A. The effects of Pilates exercise training on physical fitness and wellbeing in
the elderly: A systematic review for future exercise prescription. Prev Med. 2015,75:1-
11. doi: 10.1016/j.ypmed.2015.03.002.
144. Silva ACLG, Mannrich G. Pilates na reabilitação: uma revisão sistemática.
Fisioter Mov. 2009, 22(3):449-455.
145. Mętel S, Milert A, Szczygieł E. Pilates Based Exercise in Muscle Disbalances
Prevention and Treatment of Sports Injuries. In Persp Topics Sports Med Sports Injury.
InTech. 2012,1:381-402.
63
146. Geweniger V, Bohlander A. Pilates - A Teachers` Manual: Exercises with Mats
and Equipment for Prevention and Rehabilitation. 2014, 1ª Ed. 309p. Berlin. Springer.
Berlin. ISBN: 9783642381140.
64
6 PRODUÇÕES CIENTÍFICAS
6.1. ARTIGO 1: REVISÃO SISTEMÁTICA E META-ANÁLISE
Artigo publicado no periódico Osteoporosis International (ISSN: 0937-941X), v.27,
n.10, p. 2913-2933, 2016. doi: 10.1007/s00198-016-3618-3.
Fator de Impacto JCR de 2016: 3,591
Effects of whole body vibration on bone mineral density in postmenopausal
women: a systematic review and meta-analysis
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de
Almeida Pires-Oliveira
LC Oliveira1,2; RG Oliveira1,2; DAA Pires-Oliveira1
1. Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brasil
2. Universidade Estadual do Norte do Paraná (UENP), Jacarezinho, PR, Brasil
Corresponding author: Laís Campos de Oliveira
Centro de Ciências da Saúde, Universidade Estadual do Norte do Paraná (UENP)
Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR,
Brasil
e-mail: [email protected]
55+(43) 9613-7944.
65
Abstract
Summary This systematic review and meta-analysis of randomized controlled trials
(RCTs) identified significant effects of whole body vibration (WBV) on bone mineral
density (BMD) of the lumbar spine (in the sensitivity analysis and seven subgroup
analyses) femoral neck (in one subgroup analysis) and trochanter (four subgroup
analyses) in postmenopausal women, but not other measurements of BMD.
Purpose Interventions using WBV training have been conducted in postmenopausal
women, aimed at increasing BMD, however, the results are contradictory. Our
objective is to conduct a systematic review and meta-analysis of RCTs examining WBV
effect on BMD.
Methods RCTs were considered eligible, with follow-up ≥6 months, which verified the
effects of WBV on the BMD of postmenopausal women. The calculations of the meta-
analysis were performed through the weighted mean difference between the WBV and
control groups, or the WBV and combined training, through the absolute change
between pre- and post-intervention in the areal bone mineral density (aBMD) or
trabecular volumetric bone mineral density (vBMDt).
Results Fifteen RCTs were included in the meta-analysis. No differences were
observed in the primary analysis. WBV was found to improve aBMD compared with
the control group, after exclusion of studies with low quality methodological (lumbar
spine), when excluding the studies which combined WBV with medication or combined
training (lumbar spine), with the use of low frequency and high magnitude (lumbar
spine and trochanter), high frequency and low magnitude (lumbar spine), high
cumulative dose and low magnitude (lumbar spine), low cumulative dose and high
magnitude (lumbar spine and trochanter), with semi-flexed knee (lumbar spine, femoral
66
neck and trochanter) and side-alternating type of vibration (lumbar spine and
trochanter).
Conclusions Despite WBV presenting potential to act as a coadjuvant in the prevention
or treatment of osteoporosis, especially for aBMD of the lumbar spine, the ideal
intervention is not yet clear. Our subgroup analyses helped to demonstrate the various
factors which appear to influence the effects of WBV on BMD, contributing to clinical
practice and the definition of protocols for future interventions.
Keywords: Bone Density; Postmenopause; Whole-body vibration; Exercise; Meta-
analysis.
67
Introduction
Clinical trials using whole body vibration (WBV) training have been frequently
published. Among the various investigated conditions are studies that aim to evaluate
the effects of WBV on bone mineral density (BMD) levels. In particular, great interest
is focused on populations which are more susceptible to significant losses in bone
mineral content, including women in the postmenopausal period [1-20].
This period begins after the final menstrual period (menopause), i.e., the period
after the cessation of menstrual cycles. Postmenopause leads to hormonal alterations,
such as decreased levels of estrogen, contributing to a number of negative health
factors. A reduction in BMD is one of the consequences of this period, thereby
increasing the risk of fractures and their complications [21]. One alternative is drug
treatment; however, the side effects of this approach limit its wider use [22]. Another
alternative is the practice of physical exercise, such as resistance or combined training,
which are most effective at increasing femoral neck and spine BMD, respectively.
However, fractures and falls were identified as adverse events in some studies [23].
As WBV is considered a relatively safe modality, several studies [1-20] have sought to
verify the influence of this form of training, to prevent or mitigate the effects BMD loss
in postmenopausal women.
In animal models, it has been observed that a WBV intervention, with low
magnitude and high frequency, can improve BMD [24-26]. However, clinical trials in
humans present conflicting results. One hypothesis for these contradictions in the
studies is the use of different vibration parameters (frequency, amplitude and
acceleration), which can vary widely [7, 11, 14, 15]. Other relevant factors are: the
position of the volunteer on the platform; the use or not of exercise during the WBV;
68
the use or not of footwear; exposure time to WBV during a session (minutes); the
weekly frequency; the intervention period (months); and the model of platform used
(providing synchronous oscillation or side alternating oscillation) [27-29].
To elucidate on the possible alterations in BMD in postmenopausal women
submitted to WBV, some systematic reviews and meta-analysis have been performed.
The study of Slatkovska et al. [30] in 2010, found that WBV had significant effects on
BMD of the hip, but not the lumbar spine. Lau et al. [31], also in a systematic review
with metaanalysis published in 2011, did not observe any effect of WBV on BMD in
older women (over 50 years), either for the hip or lumbar spine.
In view of the contradictory results reported in the literature; and the emergence
of new studies in recent years, the aim of this systematic review and meta-analysis
was to analyse clinical trials that verified the effects of WBV on BMD in
postmenopausal women, compared with no intervention or minimal intervention and
other forms of exercise.
Methods
The present study is characterized as a systematic review and meta-analysis [32, 33].
To perform this study, the recommendations of the PRISMA protocol were followed
[34]. The inclusion criteria were randomized controlled trials (RCTs), which
investigated the effects of WBV on BMD in postmenopausal women (there were no
restrictions on ethnicity or level of physical activity); studies with an intervention period
of six months or more, since this is the minimum period used to verify positive effects
on BMD; studies where WBV training took place using a sinusoidal vibration platform
(since these studies offered the frequency, in addition to the magnitude and/or
amplitude).
69
The exclusion criteria were: study designs that were not RCTs; studies with
duplicate information to another RCT, or which presented preliminary data from a
subsequently published study; did not use WBV training on sinusoidal vibration
platforms (e.g., localized electrical stimulation or mechanical vibration); WBV training
not linked to the observation of BMD; women who were not presented as being in the
postmenopausal period; women who were diagnosed with a pathological framework
or secondary causes of osteoporosis; studies in which the volunteers were not
standing on the oscillation platform (i.e., sitting or lying position); WBV studies
conducted with male volunteers or animals; studies in which volunteers who used
medication to improve BMD were not equally divided between vibration and control
groups; WBV studies associated with another form of exercise which did not include a
comparison group that used the same form of exercise.
Databases and Search strategies
The search was conducted in the following databases: PubMed, Web of Science,
LILACS, The Cochrane Library and PEDro, without the use of a filter to limit the date
of publication or language. A search in a database to register clinical trials
(clinicaltrials.gov) was performed in order to find unpublished studies. The final search
took place on January 8, 2016.
In the search strategy, the following keywords were selected: (whole body
vibration OR WBV OR vibration OR vibration therapy OR vibration training OR
oscillating platforms) AND (bone mineral density OR bone density OR bone OR bones
OR bone mass OR bone mineral content OR BMC OR BMD OR bone strength OR
osteoporosis OR osteopenia) AND (postmenopausal OR menopause OR
70
perimenopause OR climacteric OR older adults OR aged OR elderly). The search
strategies were adapted for each database when necessary.
Study selection
One reviewer (LCO) conducted the initial search strategy in the databases, extracting
the titles and abstracts. Subsequently, the study selection, evaluation and data
extraction were conducted independently by two authors (LCO and RGO), based on
reading the titles and abstracts. Potentially eligible articles were read in full. A manual
search in the reference lists of all eligible articles was conducted in an attempt to find
new references. Any unresolved disagreements between the two researchers, were
passed on to a third researcher (DAAPO) to decide on the issue. The same data
extraction form was used by all the authors.
The PICO method [35] was used to structure the literature search and data
extraction: P (population) = postmenopausal women; I (intervention) = WBV training
using sinusoidal vibration platforms; C (comparison) = no intervention, or other
activities intended, or not, to improve BMD; O (outcome) = BMD.
Data extraction
The following information was extracted from each study: a) name of the first author
and year of publication; b) number of volunteers allocated to each group; c) mean and
standard deviation for each age group; d) time exposed to vibration (months, weekly
frequency, daily minutes of vibration); e) frequency of vibration, displacement peak to
peak and/or magnitude, and type of vibration (synchronous oscillation or side
alternating); f) body position or activity performed on the vibration platform; g) activities
71
carried out by other exercise groups; h) activities of the control group; i) BMD
evaluation tool and evaluated region; j) condition of the volunteers regarding alterations
in BMD (no alterations, osteopenic or osteoporotic); k) use of calcium, vitamin D or
medications; l) results reported for BMD; m) percentage of volunteers who completed
the WBV program; n) adverse events due to the WBV.
Evaluation of the methodological quality of the studies
Methodological quality was evaluated by two independent reviewers using the PEDro
scale (Physiotherapy Evidence Database) [36-38]. This scale takes into account the
internal validity and sufficiency of statistical information of the studies, and contains 11
questions with three items from the Jadad scale [39] and nine items from the Delphi
list [40]. The first question is not scored (related to external validity) and the other ten
questions are scored. Each item that meets the required criteria receives a point,
making it possible to classify the quality of each study as: excellent (9-10), good (6-8),
fair (4-5) or poor (<4). Studies with a score ≥ 6 are considered high quality. Maher et
al. [37] demonstrated good reliability between evaluators, with an intraclass correlation
coefficient of 0.68 when using consensus classifications generated by two or three
independent evaluators on the PEDro scale.
Definition of WBV
The mechanical vibrations which are carried out with a human body standing on an
oscillating sinusoidal platform are defined as WBV (sinusoidal-shaped oscillations).
The intensity of the vibrations is increased or decreased depending on various
parameters, chief among which are: frequency expressed in hertz (Hz); amplitude or
72
displacement peak to peak expressed in millimeters (mm); magnitude of the
acceleration due to gravity expressed in grams (g) or meters per second (m/s); and the
period of time that the body receives the vibration (minutes per session, weekly
frequency and months of intervention) [27, 41]. The period of time may be used to
calculate the cumulative dose of WBV throughout the intervention period by multiplying
the exposure time by the weekly frequency and number of weeks, corresponding to a
previously used strategy [30].
According to Rauch [28], the frequency refers to the number of repetitions of
oscillatory cycles per second, which typically ranges from 15 to 60 Hz; the amplitude
corresponds to the difference between the stationary point and the highest value
reached by the oscillating plate, while the peak-to-peak displacement corresponds to
the entire oscillating movement, from the smallest to largest value, typically ranging
from 1 to 15 mm; the magnitude is represented by the vibration acceleration, being that
the acceleration is dependent upon the frequency and peak-to-peak displacement. The
acceleration can be evaluated using an accelerometer and can reach up to 15g
(gravitational acceleration, 1 g = 9.8 m/s), or estimated using the formula: m/s2 = 2.π
2.f2.m, where f is the frequency in Hz and m is the peak-to-peak displacement
expressed in meters [27]. The magnitude is considered high ≥ 1g [27, 29] and the
frequency > 20 Hz [4, 14].
There are two main types of vibration platforms: those that vibrate in a
predominantly vertical direction, synchronously across their base, denominated
synchronous vibration platforms (synchronous vibration) and those that vibrate through
an anteroposterior axis, so that the right and left sides alternate horizontally,
denominated side alternating vibration platforms (side-alternating vibration) [27-29].
73
Synthesis of the results
The descriptive results are presented in a table. For the meta-analysis, the
measurement of effect was the weighted mean difference between the WBV groups
vs. control, or WBV vs. combined training, in absolute alteration of the bone mineral
density area (aBMD) between pre and post intervention, for each segment (lumbar
spine, total hip, femoral neck, trochanter and ward's area) evaluated using DXA (dual-
energy x-ray absorptiometry) expressed in g/cm2, or trabecular volumetric bone
mineral density (vBMDt) measured by pQCT (peripheral quantitative computed
tomography) for the tibia and radius, expressed in mg/cm3.
The Cochran Q test for heterogeneity was performed and considered
statistically significant if p ≤ 0.10. Heterogeneity was also quantified with statistical I2,
whereby 0-40% may not be important, 30-60% may represent moderate heterogeneity,
50-90% may represent high heterogeneity and 75-100% is defined as considerable
heterogeneity [42]. Fixed effects models were used when there was no statistically
significant heterogeneity, otherwise random effect models were used. A meta-analysis
on the primary data was only performed if two or more studies evaluated the same
outcome of interest. However, for sensitivity and subgroup analyses, there could only
be one study evaluating the same outcome of interest. The values for the effect of
treatment were considered statistically significant when p <0.05. To evaluate the risk
of publication bias, a funnel plot was used when there were ≥10 trials in a meta-
analysis. All analyses were performed using the program Review Manager (RevMan)
[Computer program], version 5.3, Copenhagen: The Nordic Cochrane Centre, The
Cochrane Collaboration.
74
Extraction of quantitative data and primary analysis
When extracting the BMD results in each study, preference was given to the data with
the intent to treat analysis (ITT), unless this was not reported. BMD results from studies
with intervention groups or similar control groups (e.g., two intervention groups with
vibrations occurring at different intensities) were combined into one group where
appropriate. For the primary analysis, groups that enabled verification of the effects of
WBV on no form of intervention or minimal intervention (light exercise and relaxation
[9] walking [11], or false vibration [14]) were always compared. Studies that associated
WBV with another form of exercise were included only when there was a comparison
group, which used the same form of exercise [5, 10]. One study [12] which used
medication (Alendronate) was included as the medication was administered equally
between the WBV and control. One study [11] used walking as an activity for the control
group and described this activity as walking outdoors, without any control of the
intensity of the effort; this activity was thus classified as a minimal intervention.
Analysis of sensitivity and subgroups
For the sensitivity analysis, studies with low methodological quality (score <6),
according to the PEDro scale, were excluded [37]. Considering that the effects of WBV
on BMD may be influenced by many factors, several subgroup analyses were
performed: a) exclusion of studies using vibration training associated with other forms
of exercise, or which used medication; b) comparison between WBV and combined
training (resistance training associated with cardiovascular training); c) low frequency
(≤ 20 Hz) and high magnitude (≥ 1g); d) high frequency (> 20 Hz) and low magnitude
(<1g); e) high frequency (> 20 Hz) and high magnitude (≥ 1g); f) cumulative dose of
75
WBV greater than the median and high magnitude (≥ 1g); g) cumulative dose of WBV
greater than the median and low magnitude (<1g); h) cumulative dose of WBV less
than or equal to the median and high magnitude (≥ 1g); i) conducting exercises during
vibration; j) keeping the knees extended during vibration; k) keeping the knees semi-
flexed during vibration; l) type of vibration with side alternating oscillation; m) type of
vibration with synchronous oscillation; n) use of supplements or medication aimed at
equating the intervention and control groups; o) no use of supplements or medication.
Statistical manipulation of BMD data
All data handling and result combination procedures followed the recommendations
described in the Cochrane Handbook for Systematic Reviews of Interventions [42].
The original authors of each study with missing data (mean and standard deviation of
the absolute difference between the pre- and post-intervention) were contacted [1-3,
5-8, 11-15] by two reviewers (LCO and RGO). There was a 58.3% response rate [1-3,
6, 7, 11, 14]. Santin-Medeiros et al. [1] and Karakiriou et al. [6] sent all the study data,
so that we could perform the calculation. Slatkovska et al. [7] sent in the mean and
standard deviation of the difference between the pre and post-intervention. Iwamoto et
al. [12] and Verschueren et al. [13] made the data available for a previously performed
meta-analysis [30], from which we extracted the values. When the data were not
available [2, 3, 5, 8, 11, 14, 15], estimates and/or statistical inferences were used to
obtain the BMD results, in the form of mean and standard deviation of the difference
between the pre- and post-intervention, using the raw data provided in the original
publication.
76
For the studies [3, 8] which provided the pre- and post-intervention alterations
in percentage format, the values were converted to absolute. Where confidence
intervals [3, 11] or standard error [8, 15] were reported, statistical calculations were
used to convert these values into standard deviations (SD). When the absolute values
of mean and standard deviation for the pre and post intervention [2, 5, 15] were
available, the mean absolute difference was calculated by subtracting the mean of the
post-intervention from the mean pre-intervention. In this case, the SD corresponding
to the absolute change in BMD was estimated using the Follmann’s method [42]. The
correlation coefficient value (r) of 0.95 was used in all the Follmann's calculations, as
described and explained in a previous meta-analysis [30]. This correlation coefficient
(r = 0.95) was proven to be conservative in simulations performed with data from the
studies in this review, whose authors reported the absolute values (mean and SD) of
the difference between the pre and post intervention in the original publication [4, 9,
10].
One study [14] did not provide enough information to calculate the standard
deviation, requiring input from data presented in another study [11], with similar
characteristics. This technique follows the recommendations of the Cochrane
Handbook for Systematic Reviews of Interventions [42] and has been used in the same
way in a previous meta-analysis, which examined the effects of WBV in
postmenopausal women [30]. When the BMD data for more than one group were
brought together in a single group [7-9], calculations for the absolute changes in the
mean and standard deviation between the groups were obtained using the “weighted
mean” or “pooled or weighted standard deviation" formula, respectively. In the study of
Slatkovska et al. [7], two vibration groups (frequency of 90 Hz and 30 Hz) were brought
together in a single group. In the study of Verschueren et al. [8], the two vibration
77
groups (normal supplementation and additional supplementation) were also brought
together in one group, as were the two control groups (normal supplementation and
additional supplementation). Finally, in the study of Von Stengel et al. [9], the two
vibration groups (synchronous and side alternating side), were brought together in one
group for the majority of the analyses, except for comparisons of subgroups related to
different types of frequency and different types of vibration.
Results
Qualitative synthesis of the studies
Initially, 1.618 titles and potentially relevant abstracts were identified. After removal of
the duplicates, the titles and abstracts of 1.577 studies were read. In this step, the
majority of the studies excluded (1.545) were due to their not being treated as RCTs,
or the intervention not occurring through WBV. The 32 remaining studies were read in
their entirety; of which 15 did not meet the eligibility criteria (a complete list of studies
excluded at this stage is available in Supplementary Table 1). The main reasons for
exclusion were due to the studies not evaluating BMD (3 studies), or the fact that men
and women formed part of the voluntary sample in the same group (4 studies). Two
studies presented interventions of less than six months.
Two other studies with the potential for inclusion were not treated as RCTs,
since the groups were divided for convenience [18, 19]. A third study [20] with the
potential for inclusion, which compared the effects of WBV with resistance training in
obese women, did not describe the parameters of amplitude or magnitude of vibration
and placement of volunteers on the platform, leaving doubts as to whether they
remained standing during the vibration. One study was excluded for not having used
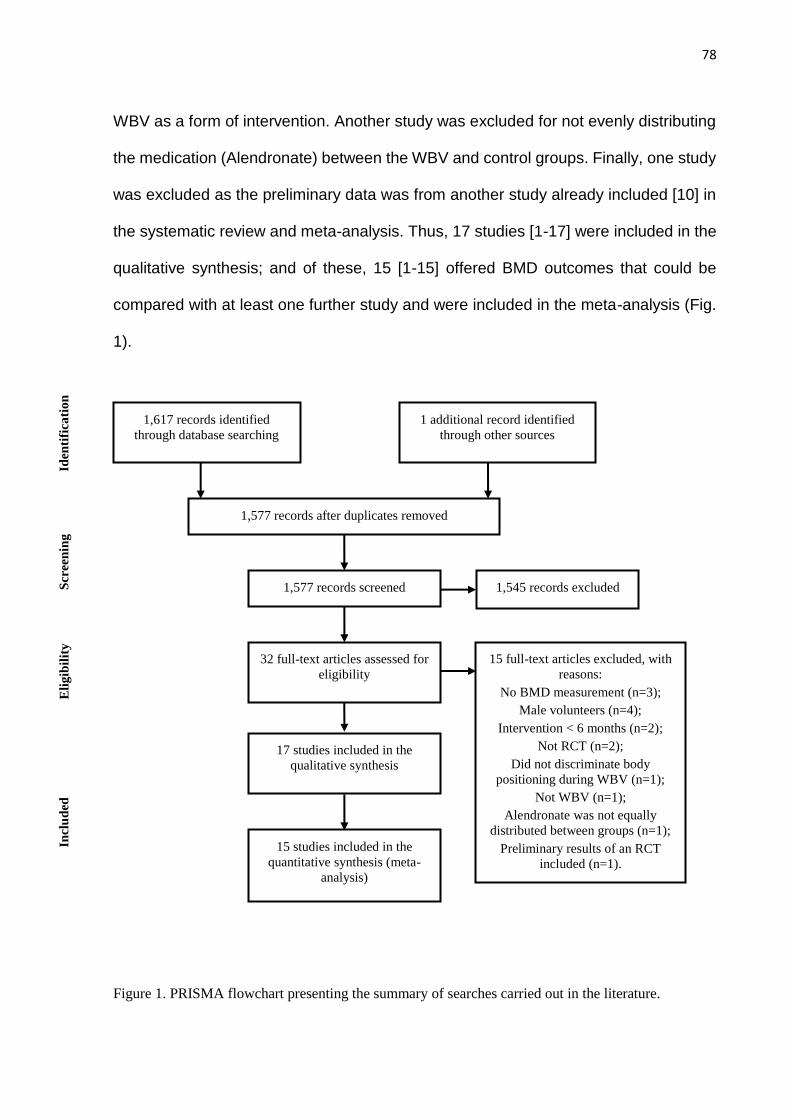
78
WBV as a form of intervention. Another study was excluded for not evenly distributing
the medication (Alendronate) between the WBV and control groups. Finally, one study
was excluded as the preliminary data was from another study already included [10] in
the systematic review and meta-analysis. Thus, 17 studies [1-17] were included in the
qualitative synthesis; and of these, 15 [1-15] offered BMD outcomes that could be
compared with at least one further study and were included in the meta-analysis (Fig.
1).
Figure 1. PRISMA flowchart presenting the summary of searches carried out in the literature.
1,617 records identified
through database searching
1 additional record identified
through other sources
1,577 records after duplicates removed
1,577 records screened 1,545 records excluded
32 full-text articles assessed for
eligibility
17 studies included in the
qualitative synthesis
15 full-text articles excluded, with
reasons:
No BMD measurement (n=3);
Male volunteers (n=4);
Intervention < 6 months (n=2);
Not RCT (n=2);
Did not discriminate body
positioning during WBV (n=1);
Not WBV (n=1);
Alendronate was not equally
distributed between groups (n=1);
Preliminary results of an RCT
included (n=1).
15 studies included in the
quantitative synthesis (meta-
analysis)
Iden
tifi
cati
on
S
creen
ing
Eli
gib
ilit
y
Incl
ud
ed
79
The RCTs included in this systematic review (Table 1 [1-17]) were published
between the years 2003 to 2015, and the total number of participants was 1.833
(ranging from 28 [4, 11] to 596 women [3]). The number of groups in each study ranged
from two [1-5, 11, 12, 14, 15] to four [8], the mean age of the volunteers from 53 [6] to
82.3 [1] years and the interventions from six [4, 6, 8, 13, 15] to eighteen months [3, 10].
The weekly frequency of WBV varied from one [12] to seven times [7, 14, 16] and the
exposure time between one minute (at a given periodization moment) [8] to 30 minutes
[13]. The mean cumulative dose ranged from 208 minutes WBV [12] to 7.800 minutes
[3] (median 864 minutes [11]). Regarding the WBV parameters, the frequency varied
from 12 [15] to 90 Hz [7, 16]; the peak to peak displacement (presented by nine studies)
varied from 0.7 mm [12] to 12 mm [9]; the magnitude (presented by 10 studies) varied
from 0.1g [15] to 10.9g [5]. The vibration type was synchronous [1, 3, 6, 7, 9, 10, 14,
16] or side alternating [2, 4, 5, 9, 11, 12, 15, 17]; two studies did not report this
information [8, 13].
In four trials WBV training was performed barefoot or wearing socks [4, 7, 11,
16], while in three studies [5, 9, 13], the volunteers made use of shoes. Other studies
did not report this condition. No study described was used any type of card or object
on the vibrating platform, which could dampen the intensity of the vibration. The
activities of the groups which performed WBV were: strengthening exercises for the
lower limbs during vibration [1, 5, 8-10, 13]; keeping the knees extended [3, 4, 7, 14,
16, 17]; or with semi-flexion of the knees [2, 6, 11, 12, 15, 17]. In two studies, the
vibration training was associated with combined training [5, 10]. In four studies there
was a specific combined training group [5, 6, 10, 13]; and only one study [5] lacked a
control group (no intervention or minimal intervention).
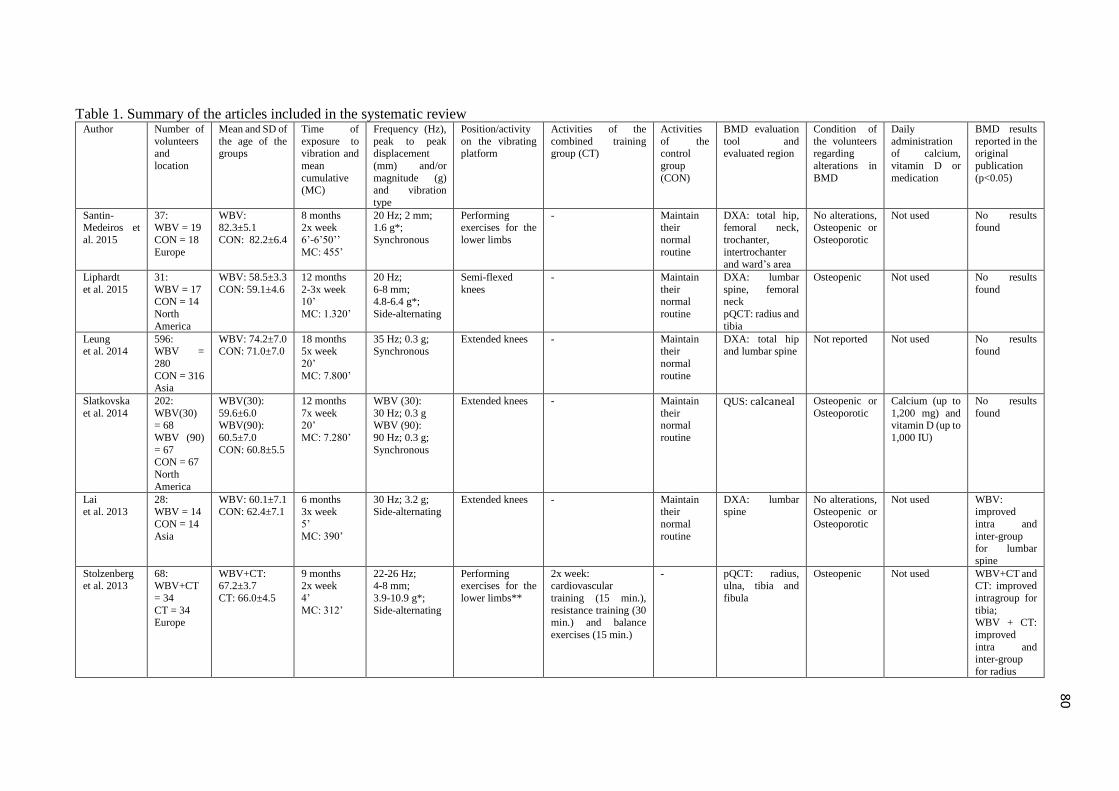
80
Table 1. Summary of the articles included in the systematic review Author Number of
volunteers and
location
Mean and SD of
the age of the groups
Time of
exposure to vibration and
mean
cumulative (MC)
Frequency (Hz),
peak to peak displacement
(mm) and/or
magnitude (g) and vibration
type
Position/activity
on the vibrating platform
Activities of the
combined training group (CT)
Activities
of the control
group
(CON)
BMD evaluation
tool and evaluated region
Condition of
the volunteers regarding
alterations in
BMD
Daily
administration of calcium,
vitamin D or
medication
BMD results
reported in the original
publication
(p<0.05)
Santin-Medeiros et
al. 2015
37: WBV = 19
CON = 18
Europe
WBV: 82.3±5.1
CON: 82.2±6.4
8 months 2x week
6’-6’50’’
MC: 455’
20 Hz; 2 mm; 1.6 g*;
Synchronous
Performing exercises for the
lower limbs
- Maintain their
normal
routine
DXA: total hip, femoral neck,
trochanter,
intertrochanter and ward’s area
No alterations, Osteopenic or
Osteoporotic
Not used No results found
Liphardt
et al. 2015
31:
WBV = 17 CON = 14
North
America
WBV: 58.5±3.3
CON: 59.1±4.6
12 months
2-3x week 10’
MC: 1.320’
20 Hz;
6-8 mm; 4.8-6.4 g*;
Side-alternating
Semi-flexed
knees
- Maintain
their normal
routine
DXA: lumbar
spine, femoral neck
pQCT: radius and
tibia
Osteopenic Not used No results
found
Leung et al. 2014
596: WBV =
280
CON = 316 Asia
WBV: 74.2±7.0 CON: 71.0±7.0
18 months 5x week
20’
MC: 7.800’
35 Hz; 0.3 g; Synchronous
Extended knees - Maintain their
normal
routine
DXA: total hip and lumbar spine
Not reported Not used No results found
Slatkovska
et al. 2014
202:
WBV(30) = 68
WBV (90)
= 67 CON = 67
North
America
WBV(30):
59.6±6.0 WBV(90):
60.5±7.0
CON: 60.8±5.5
12 months
7x week 20’
MC: 7.280’
WBV (30):
30 Hz; 0.3 g WBV (90):
90 Hz; 0.3 g;
Synchronous
Extended knees - Maintain
their normal
routine
QUS: calcaneal Osteopenic or
Osteoporotic
Calcium (up to
1,200 mg) and vitamin D (up to
1,000 IU)
No results
found
Lai
et al. 2013
28:
WBV = 14
CON = 14
Asia
WBV: 60.1±7.1
CON: 62.4±7.1
6 months
3x week
5’
MC: 390’
30 Hz; 3.2 g;
Side-alternating
Extended knees - Maintain
their
normal
routine
DXA: lumbar
spine
No alterations,
Osteopenic or
Osteoporotic
Not used WBV:
improved
intra and
inter-group for lumbar
spine
Stolzenberg et al. 2013
68: WBV+CT
= 34
CT = 34 Europe
WBV+CT: 67.2±3.7
CT: 66.0±4.5
9 months 2x week
4’
MC: 312’
22-26 Hz; 4-8 mm;
3.9-10.9 g*;
Side-alternating
Performing exercises for the
lower limbs**
2x week: cardiovascular
training (15 min.),
resistance training (30 min.) and balance
exercises (15 min.)
- pQCT: radius, ulna, tibia and
fibula
Osteopenic Not used WBV+CT and CT: improved
intragroup for
tibia; WBV + CT:
improved
intra and
inter-group
for radius
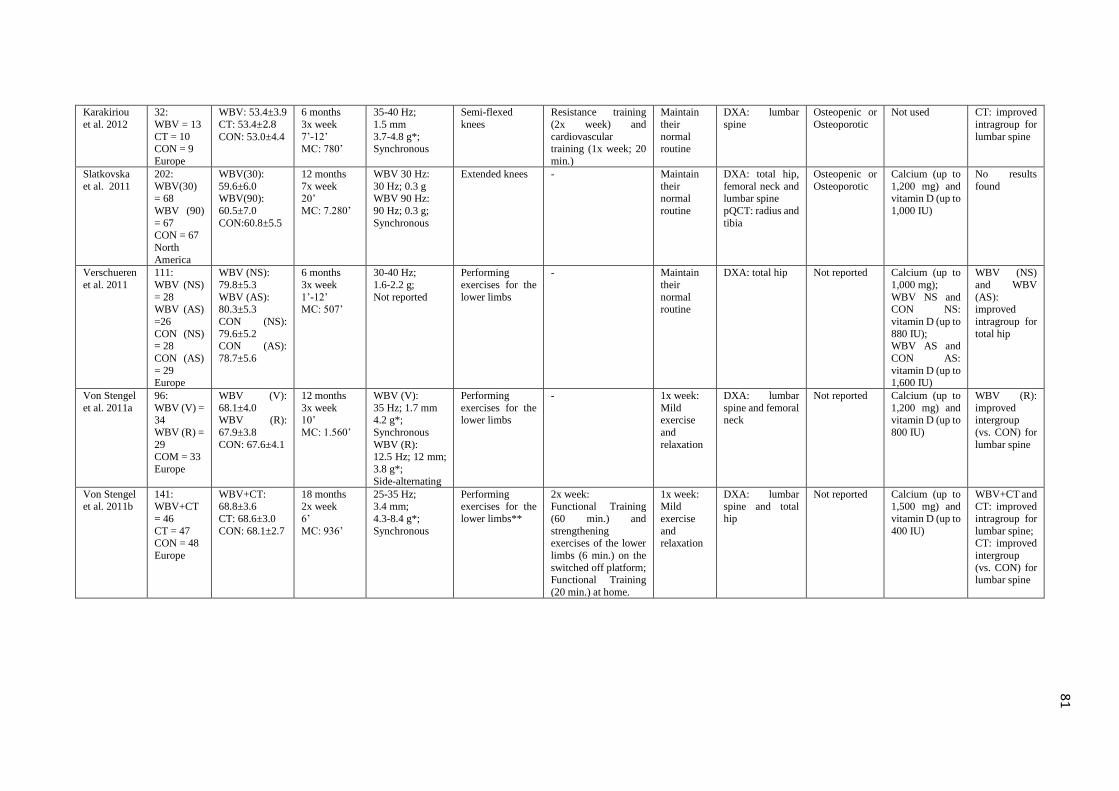
81
Karakiriou
et al. 2012
32:
WBV = 13
CT = 10 CON = 9
Europe
WBV: 53.4±3.9
CT: 53.4±2.8 CON: 53.0±4.4
6 months
3x week
7’-12’ MC: 780’
35-40 Hz;
1.5 mm
3.7-4.8 g*; Synchronous
Semi-flexed
knees
Resistance training
(2x week) and
cardiovascular training (1x week; 20
min.)
Maintain
their
normal routine
DXA: lumbar
spine
Osteopenic or
Osteoporotic
Not used CT: improved
intragroup for
lumbar spine
Slatkovska
et al. 2011
202:
WBV(30) = 68
WBV (90)
= 67 CON = 67
North
America
WBV(30):
59.6±6.0 WBV(90):
60.5±7.0
CON:60.8±5.5
12 months
7x week 20’
MC: 7.280’
WBV 30 Hz:
30 Hz; 0.3 g WBV 90 Hz:
90 Hz; 0.3 g;
Synchronous
Extended knees - Maintain
their normal
routine
DXA: total hip,
femoral neck and lumbar spine
pQCT: radius and
tibia
Osteopenic or
Osteoporotic
Calcium (up to
1,200 mg) and vitamin D (up to
1,000 IU)
No results
found
Verschueren
et al. 2011
111:
WBV (NS)
= 28 WBV (AS)
=26
CON (NS) = 28
CON (AS)
= 29 Europe
WBV (NS):
79.8±5.3
WBV (AS): 80.3±5.3
CON (NS):
79.6±5.2 CON (AS):
78.7±5.6
6 months
3x week
1’-12’ MC: 507’
30-40 Hz;
1.6-2.2 g;
Not reported
Performing
exercises for the
lower limbs
- Maintain
their
normal routine
DXA: total hip Not reported Calcium (up to
1,000 mg);
WBV NS and CON NS:
vitamin D (up to
880 IU); WBV AS and
CON AS:
vitamin D (up to 1,600 IU)
WBV (NS)
and WBV
(AS): improved
intragroup for
total hip
Von Stengel
et al. 2011a
96:
WBV (V) = 34
WBV (R) =
29 COM = 33
Europe
WBV (V):
68.1±4.0 WBV (R):
67.9±3.8
CON: 67.6±4.1
12 months
3x week 10’
MC: 1.560’
WBV (V):
35 Hz; 1.7 mm 4.2 g*;
Synchronous
WBV (R): 12.5 Hz; 12 mm;
3.8 g*;
Side-alternating
Performing
exercises for the lower limbs
- 1x week:
Mild exercise
and
relaxation
DXA: lumbar
spine and femoral neck
Not reported Calcium (up to
1,200 mg) and vitamin D (up to
800 IU)
WBV (R):
improved intergroup
(vs. CON) for
lumbar spine
Von Stengel
et al. 2011b
141:
WBV+CT
= 46
CT = 47 CON = 48
Europe
WBV+CT:
68.8±3.6
CT: 68.6±3.0
CON: 68.1±2.7
18 months
2x week
6’
MC: 936’
25-35 Hz;
3.4 mm;
4.3-8.4 g*;
Synchronous
Performing
exercises for the
lower limbs**
2x week:
Functional Training
(60 min.) and
strengthening exercises of the lower
limbs (6 min.) on the
switched off platform; Functional Training
(20 min.) at home.
1x week:
Mild
exercise
and relaxation
DXA: lumbar
spine and total
hip
Not reported Calcium (up to
1,500 mg) and
vitamin D (up to
400 IU)
WBV+CT and
CT: improved
intragroup for
lumbar spine; CT: improved
intergroup
(vs. CON) for lumbar spine
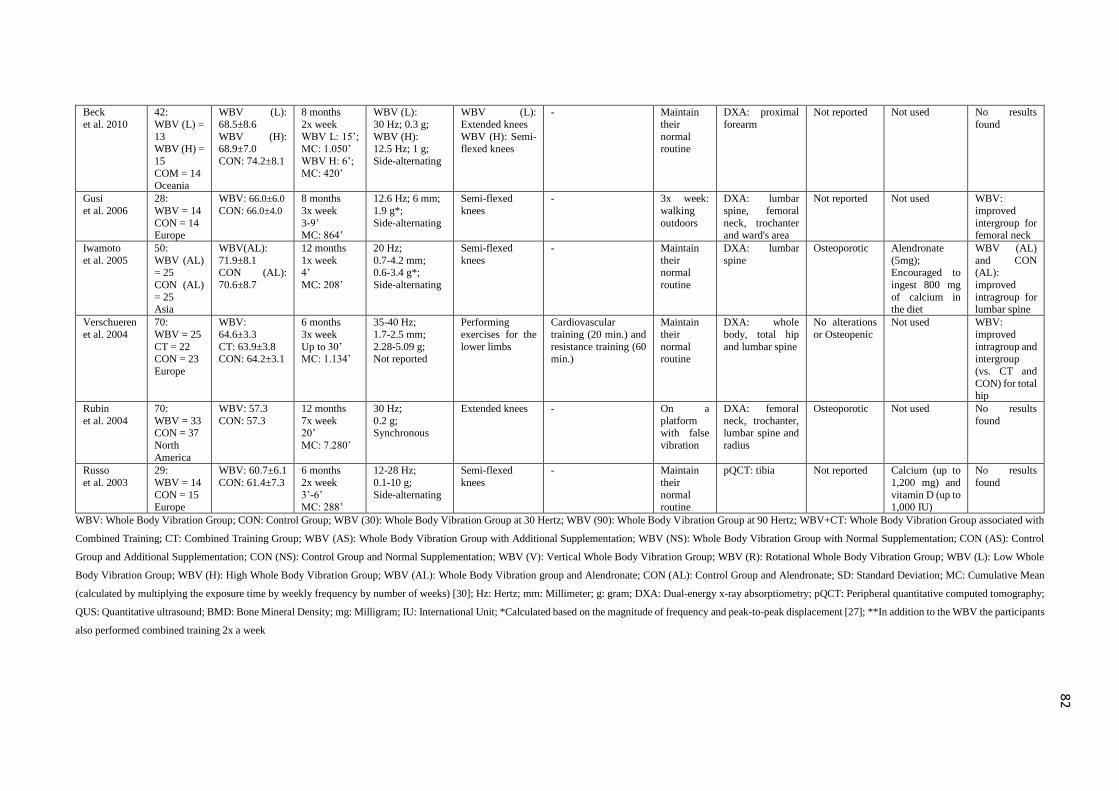
82
Beck
et al. 2010
42:
WBV (L) =
13 WBV (H) =
15
COM = 14 Oceania
WBV (L):
68.5±8.6
WBV (H): 68.9±7.0
CON: 74.2±8.1
8 months
2x week
WBV L: 15’; MC: 1.050’
WBV H: 6’;
MC: 420’
WBV (L):
30 Hz; 0.3 g;
WBV (H): 12.5 Hz; 1 g;
Side-alternating
WBV (L):
Extended knees
WBV (H): Semi-flexed knees
- Maintain
their
normal routine
DXA: proximal
forearm
Not reported Not used No results
found
Gusi
et al. 2006
28:
WBV = 14
CON = 14 Europe
WBV: 66.0±6.0
CON: 66.0±4.0
8 months
3x week
3-9’ MC: 864’
12.6 Hz; 6 mm;
1.9 g*;
Side-alternating
Semi-flexed
knees
- 3x week:
walking
outdoors
DXA: lumbar
spine, femoral
neck, trochanter and ward's area
Not reported Not used WBV:
improved
intergroup for femoral neck
Iwamoto
et al. 2005
50:
WBV (AL) = 25
CON (AL)
= 25 Asia
WBV(AL):
71.9±8.1 CON (AL):
70.6±8.7
12 months
1x week 4’
MC: 208’
20 Hz;
0.7-4.2 mm; 0.6-3.4 g*;
Side-alternating
Semi-flexed
knees
- Maintain
their normal
routine
DXA: lumbar
spine
Osteoporotic Alendronate
(5mg); Encouraged to
ingest 800 mg
of calcium in the diet
WBV (AL)
and CON (AL):
improved
intragroup for lumbar spine
Verschueren
et al. 2004
70:
WBV = 25
CT = 22
CON = 23
Europe
WBV:
64.6±3.3
CT: 63.9±3.8
CON: 64.2±3.1
6 months
3x week
Up to 30’
MC: 1.134’
35-40 Hz;
1.7-2.5 mm;
2.28-5.09 g;
Not reported
Performing
exercises for the
lower limbs
Cardiovascular
training (20 min.) and
resistance training (60
min.)
Maintain
their
normal
routine
DXA: whole
body, total hip
and lumbar spine
No alterations
or Osteopenic
Not used WBV:
improved
intragroup and
intergroup
(vs. CT and
CON) for total hip
Rubin
et al. 2004
70:
WBV = 33 CON = 37
North
America
WBV: 57.3
CON: 57.3
12 months
7x week 20’
MC: 7.280’
30 Hz;
0.2 g; Synchronous
Extended knees - On a
platform with false
vibration
DXA: femoral
neck, trochanter, lumbar spine and
radius
Osteoporotic Not used No results
found
Russo
et al. 2003
29:
WBV = 14
CON = 15
Europe
WBV: 60.7±6.1
CON: 61.4±7.3
6 months
2x week
3’-6’
MC: 288’
12-28 Hz;
0.1-10 g;
Side-alternating
Semi-flexed
knees
- Maintain
their
normal
routine
pQCT: tibia Not reported Calcium (up to
1,200 mg) and
vitamin D (up to
1,000 IU)
No results
found
WBV: Whole Body Vibration Group; CON: Control Group; WBV (30): Whole Body Vibration Group at 30 Hertz; WBV (90): Whole Body Vibration Group at 90 Hertz; WBV+CT: Whole Body Vibration Group associated with
Combined Training; CT: Combined Training Group; WBV (AS): Whole Body Vibration Group with Additional Supplementation; WBV (NS): Whole Body Vibration Group with Normal Supplementation; CON (AS): Control
Group and Additional Supplementation; CON (NS): Control Group and Normal Supplementation; WBV (V): Vertical Whole Body Vibration Group; WBV (R): Rotational Whole Body Vibration Group; WBV (L): Low Whole
Body Vibration Group; WBV (H): High Whole Body Vibration Group; WBV (AL): Whole Body Vibration group and Alendronate; CON (AL): Control Group and Alendronate; SD: Standard Deviation; MC: Cumulative Mean
(calculated by multiplying the exposure time by weekly frequency by number of weeks) [30]; Hz: Hertz; mm: Millimeter; g: gram; DXA: Dual-energy x-ray absorptiometry; pQCT: Peripheral quantitative computed tomography;
QUS: Quantitative ultrasound; BMD: Bone Mineral Density; mg: Milligram; IU: International Unit; *Calculated based on the magnitude of frequency and peak-to-peak displacement [27]; **In addition to the WBV the participants
also performed combined training 2x a week
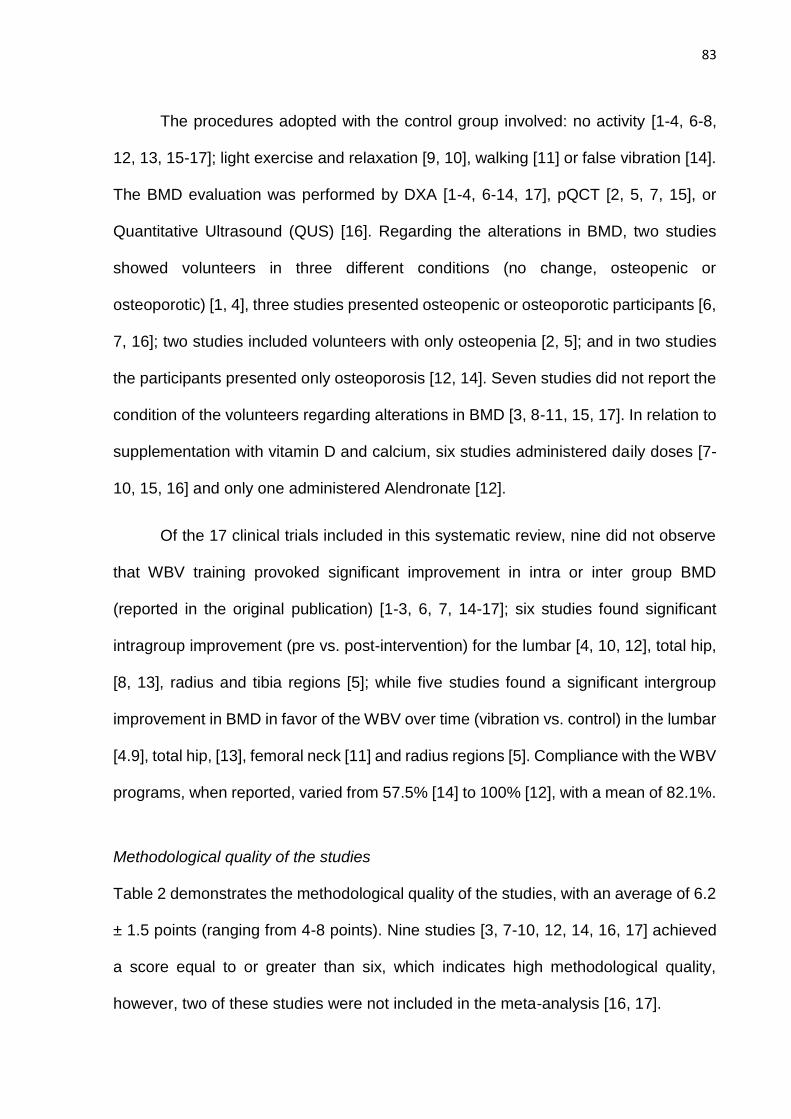
83
The procedures adopted with the control group involved: no activity [1-4, 6-8,
12, 13, 15-17]; light exercise and relaxation [9, 10], walking [11] or false vibration [14].
The BMD evaluation was performed by DXA [1-4, 6-14, 17], pQCT [2, 5, 7, 15], or
Quantitative Ultrasound (QUS) [16]. Regarding the alterations in BMD, two studies
showed volunteers in three different conditions (no change, osteopenic or
osteoporotic) [1, 4], three studies presented osteopenic or osteoporotic participants [6,
7, 16]; two studies included volunteers with only osteopenia [2, 5]; and in two studies
the participants presented only osteoporosis [12, 14]. Seven studies did not report the
condition of the volunteers regarding alterations in BMD [3, 8-11, 15, 17]. In relation to
supplementation with vitamin D and calcium, six studies administered daily doses [7-
10, 15, 16] and only one administered Alendronate [12].
Of the 17 clinical trials included in this systematic review, nine did not observe
that WBV training provoked significant improvement in intra or inter group BMD
(reported in the original publication) [1-3, 6, 7, 14-17]; six studies found significant
intragroup improvement (pre vs. post-intervention) for the lumbar [4, 10, 12], total hip,
[8, 13], radius and tibia regions [5]; while five studies found a significant intergroup
improvement in BMD in favor of the WBV over time (vibration vs. control) in the lumbar
[4.9], total hip, [13], femoral neck [11] and radius regions [5]. Compliance with the WBV
programs, when reported, varied from 57.5% [14] to 100% [12], with a mean of 82.1%.
Methodological quality of the studies
Table 2 demonstrates the methodological quality of the studies, with an average of 6.2
± 1.5 points (ranging from 4-8 points). Nine studies [3, 7-10, 12, 14, 16, 17] achieved
a score equal to or greater than six, which indicates high methodological quality,
however, two of these studies were not included in the meta-analysis [16, 17].
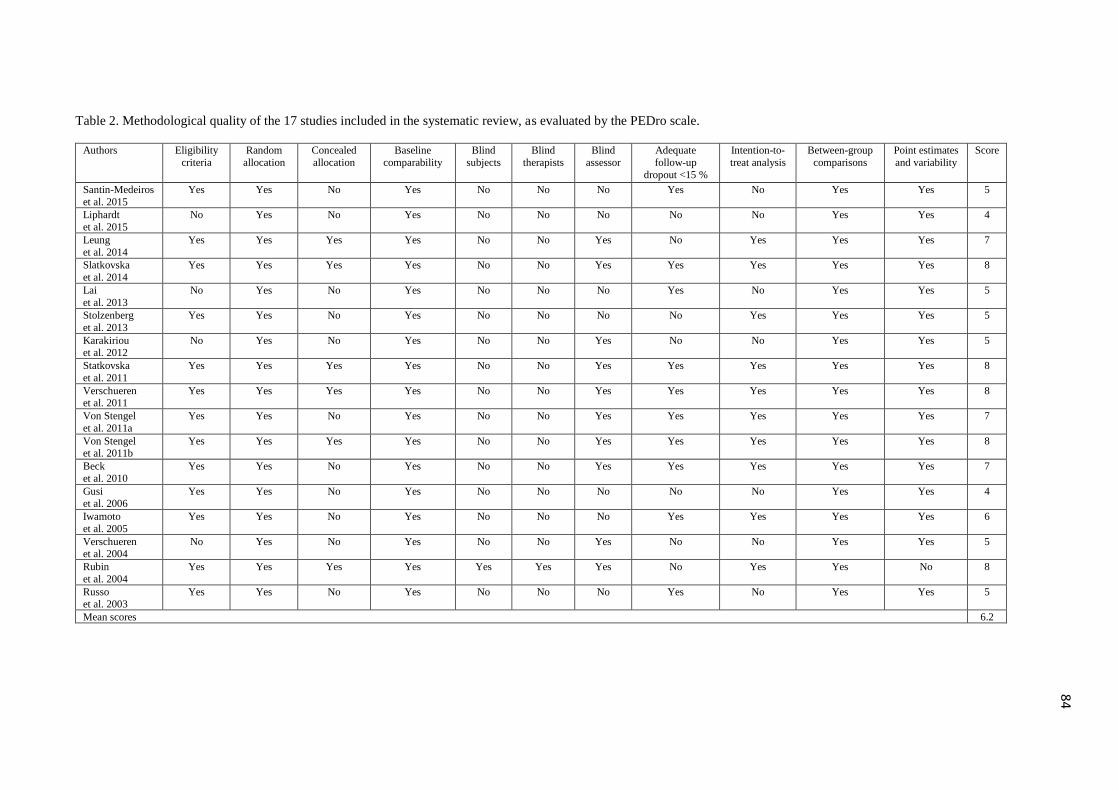
84
Table 2. Methodological quality of the 17 studies included in the systematic review, as evaluated by the PEDro scale.
Authors Eligibility
criteria
Random
allocation
Concealed
allocation
Baseline
comparability
Blind
subjects
Blind
therapists
Blind
assessor
Adequate
follow-up
dropout <15 %
Intention-to-
treat analysis
Between-group
comparisons
Point estimates
and variability
Score
Santin-Medeiros
et al. 2015
Yes Yes No Yes No No No Yes No Yes Yes 5
Liphardt
et al. 2015
No Yes No Yes No No No No No Yes Yes 4
Leung
et al. 2014
Yes Yes Yes Yes No No Yes No Yes Yes Yes 7
Slatkovska
et al. 2014
Yes Yes Yes Yes No No Yes Yes Yes Yes Yes 8
Lai
et al. 2013
No Yes No Yes No No No Yes No Yes Yes 5
Stolzenberg
et al. 2013
Yes Yes No Yes No No No No Yes Yes Yes 5
Karakiriou et al. 2012
No Yes No Yes No No Yes No No Yes Yes 5
Statkovska
et al. 2011
Yes Yes Yes Yes No No Yes Yes Yes Yes Yes 8
Verschueren et al. 2011
Yes Yes Yes Yes No No Yes Yes Yes Yes Yes 8
Von Stengel
et al. 2011a
Yes Yes No Yes No No Yes Yes Yes Yes Yes 7
Von Stengel et al. 2011b
Yes Yes Yes Yes No No Yes Yes Yes Yes Yes 8
Beck
et al. 2010
Yes Yes No Yes No No Yes Yes Yes Yes Yes 7
Gusi et al. 2006
Yes Yes No Yes No No No No No Yes Yes 4
Iwamoto
et al. 2005
Yes Yes No Yes No No No Yes Yes Yes Yes 6
Verschueren et al. 2004
No Yes No Yes No No Yes No No Yes Yes 5
Rubin
et al. 2004
Yes Yes Yes Yes Yes Yes Yes No Yes Yes No 8
Russo et al. 2003
Yes Yes No Yes No No No Yes No Yes Yes 5
Mean scores 6.2

85
Quantitative synthesis of the studies (meta-analysis)
Primary analysis
In the primary analysis, which included all studies, there was no significant effect for
any skeletal sites when comparing the WBV and control groups, for the aBMD of the;
lumbar spine (0.005 g/cm2 [95% confidence interval (CI), -0.000 to 0.010] p = 0.07, n
= 1,233, studies = 10; Fig. 2.a), total hip (0.002 g/cm2 [95% confidence interval (CI), -
0.002 to 0.007] p = 0.31, n = 1,087, studies = 6; Fig. 2.b), femoral neck (-0.001 g/cm2
[95% confidence interval (CI), -0.006 to 0.003] p = 0.55, n = 433, studies = 5; Fig. 2.c),
trochanter (0.009 g/cm2 [95% confidence interval (CI), -0.007 to 0.027] p = 0.26, n =
135, studies = 3; Fig. 2.d), ward’s area (0.004 g/cm2 [95% confidence interval (CI), -
0.036 to 0.044] p = 0.84, n = 65, studies = 2; Fig. 2.e); radius vBMDt (-0.71 mg/cm3
[95% confidence interval (CI), -2.25 to 0.83] p = 0.37, n = 301, studies = 3; Fig. 3.a) or
tibia vBMDt (0.27 mg/cm3 [95% confidence interval (CI), -0.65 to 1.18] p = 0.57, n =
330, studies = 4; Fig. 3.b).
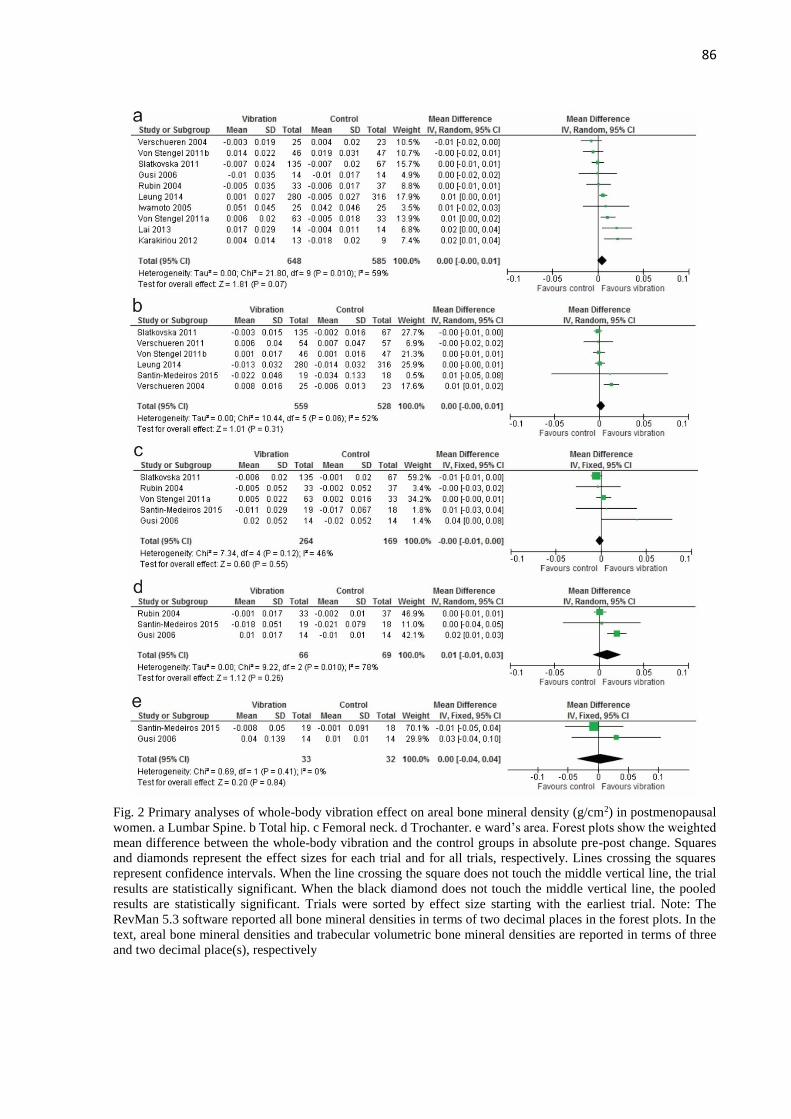
86
Fig. 2 Primary analyses of whole-body vibration effect on areal bone mineral density (g/cm2) in postmenopausal
women. a Lumbar Spine. b Total hip. c Femoral neck. d Trochanter. e ward’s area. Forest plots show the weighted
mean difference between the whole-body vibration and the control groups in absolute pre-post change. Squares
and diamonds represent the effect sizes for each trial and for all trials, respectively. Lines crossing the squares
represent confidence intervals. When the line crossing the square does not touch the middle vertical line, the trial
results are statistically significant. When the black diamond does not touch the middle vertical line, the pooled
results are statistically significant. Trials were sorted by effect size starting with the earliest trial. Note: The
RevMan 5.3 software reported all bone mineral densities in terms of two decimal places in the forest plots. In the
text, areal bone mineral densities and trabecular volumetric bone mineral densities are reported in terms of three
and two decimal place(s), respectively
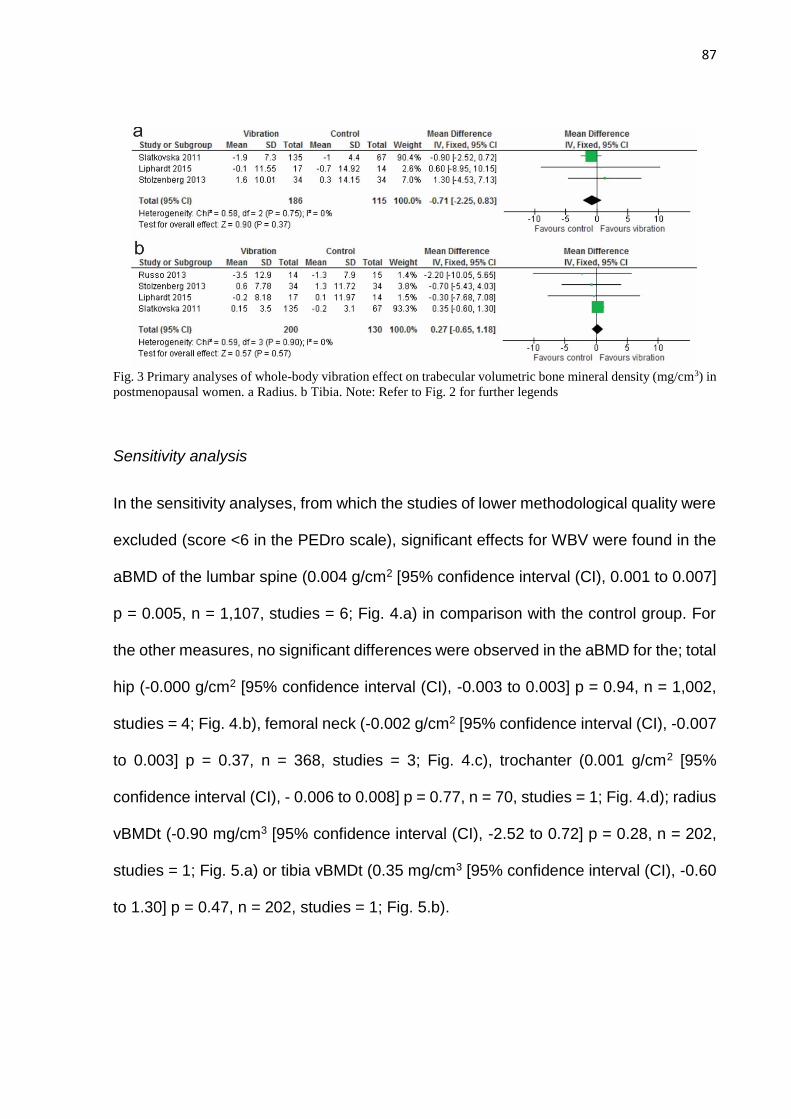
87
Fig. 3 Primary analyses of whole-body vibration effect on trabecular volumetric bone mineral density (mg/cm3) in
postmenopausal women. a Radius. b Tibia. Note: Refer to Fig. 2 for further legends
Sensitivity analysis
In the sensitivity analyses, from which the studies of lower methodological quality were
excluded (score <6 in the PEDro scale), significant effects for WBV were found in the
aBMD of the lumbar spine (0.004 g/cm2 [95% confidence interval (CI), 0.001 to 0.007]
p = 0.005, n = 1,107, studies = 6; Fig. 4.a) in comparison with the control group. For
the other measures, no significant differences were observed in the aBMD for the; total
hip (-0.000 g/cm2 [95% confidence interval (CI), -0.003 to 0.003] p = 0.94, n = 1,002,
studies = 4; Fig. 4.b), femoral neck (-0.002 g/cm2 [95% confidence interval (CI), -0.007
to 0.003] p = 0.37, n = 368, studies = 3; Fig. 4.c), trochanter (0.001 g/cm2 [95%
confidence interval (CI), - 0.006 to 0.008] p = 0.77, n = 70, studies = 1; Fig. 4.d); radius
vBMDt (-0.90 mg/cm3 [95% confidence interval (CI), -2.52 to 0.72] p = 0.28, n = 202,
studies = 1; Fig. 5.a) or tibia vBMDt (0.35 mg/cm3 [95% confidence interval (CI), -0.60
to 1.30] p = 0.47, n = 202, studies = 1; Fig. 5.b).
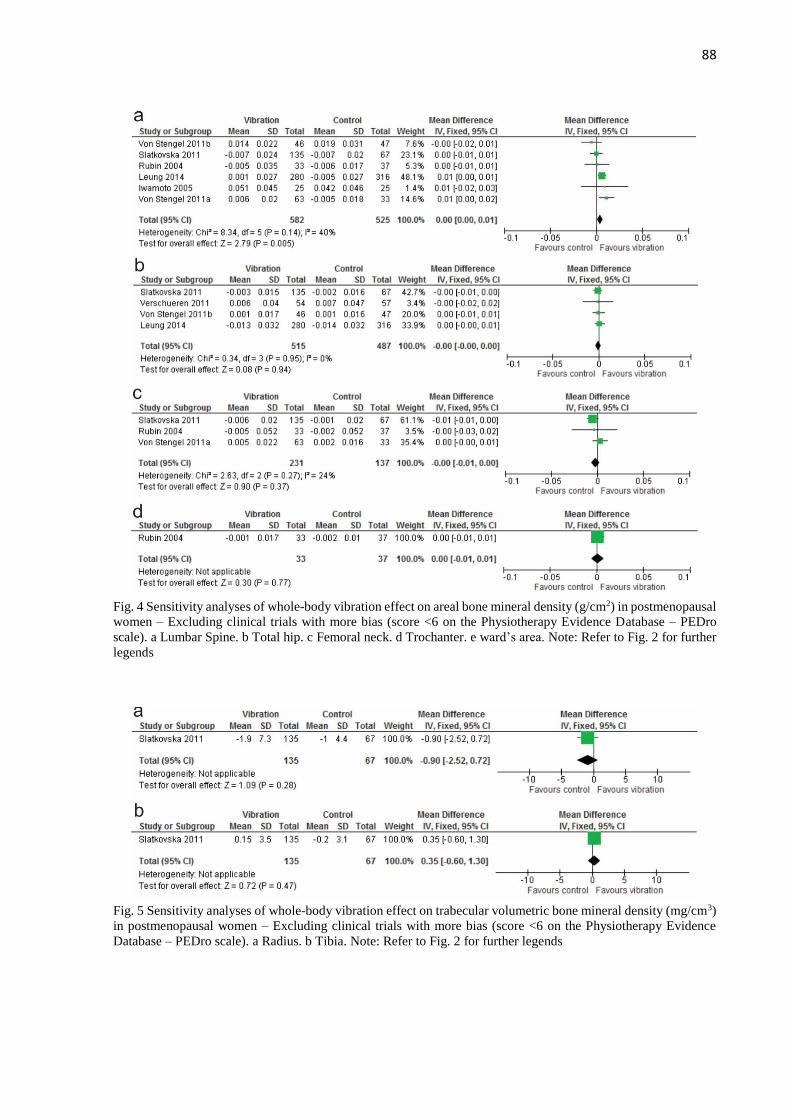
88
Fig. 4 Sensitivity analyses of whole-body vibration effect on areal bone mineral density (g/cm2) in postmenopausal
women – Excluding clinical trials with more bias (score <6 on the Physiotherapy Evidence Database – PEDro
scale). a Lumbar Spine. b Total hip. c Femoral neck. d Trochanter. e ward’s area. Note: Refer to Fig. 2 for further
legends
Fig. 5 Sensitivity analyses of whole-body vibration effect on trabecular volumetric bone mineral density (mg/cm3)
in postmenopausal women – Excluding clinical trials with more bias (score <6 on the Physiotherapy Evidence
Database – PEDro scale). a Radius. b Tibia. Note: Refer to Fig. 2 for further legends
89
Exclusion of RCTs in which the WBV was associated with combined training or
medication; and comparison between WBV and combined training
After withdrawal of one study that associated WBV with combined training [10] and
another study that associated medication with WBV (Alendronate) [12], significant
effects were found for the aBMD of the lumbar spine (0.006 g/cm2 [95% confidence
interval (CI), 0.000 to 0.011] p = 0.04, n = 1,090, studies = 8), but not for total hip (0.003
g/cm2 [95% confidence interval (CI), -0.003 to 0.009] p = 0.30, n = 994, studies = 5), in
the comparison between the WBV and control groups. After excluding one study [5]
which performed WBV associated with combined training, for the radius vBMDt (-0.86
mg/cm3 [95% confidence interval (CI), -2.46 to 0.74] p = 0.29, n = 233, studies = 2)
and tibia vBMDt (0.30 mg/cm3 [95% confidence interval (CI), -0.63 to 1.24] p = 0.52, n
= 262, studies = 3), no effect was observed in the comparison between the WBV and
control groups. In the only possible comparison between WBV and combined training,
there was no significant difference in lumbar spine aBMD (-0.006 g/cm2 [95%
confidence interval (CI), -0.015 to 0.003] p = 0.17, n = 70, studies = 2) (Supplementary
Fig. 1).
Low frequency and high magnitude
In the subgroup analysis, in which only studies that used low frequency (≤ 20 Hz) and
high magnitude (≥ 1g) were included, significant effects were observed when
comparing WBV with the control groups for the aBMD of the lumbar spine (0.010 g/cm2
[95% confidence interval (CI), 0.001 to 0.018] p = 0.03, n = 140, studies = 3) and
trochanter (0.019 g/cm2 [95% confidence interval (CI), 0.009 to 0.029] p = 0.0002, n =
65, studies = 2), but not for total hip (0.012 g/cm2 [95% confidence interval (CI), -0.053
90
to 0.077] p = 0.72, n = 37, studies = 1), femoral neck (0.003 g/cm2 [95% confidence
interval (CI), -0.005 to 0.011] p = 0.46, n = 127, studies = 3), ward’s area (0.004 g/cm2
[95% confidence interval (CI), - 0.036 to 0.044] p = 0.84, n = 65, studies = 2); radius
vBMDt (0.60 mg/cm3 [95% confidence interval (CI), -8.95 to 10.15] p = 0.90, n = 31,
studies = 1) or tibia vBMDt (-0.30 mg/cm3 [95% confidence interval (CI), -7.68 to 7.08]
p = 0.94, n = 31, studies = 1) (Supplementary Fig. 2).
High frequency and low magnitude
When the studies using high-frequency (> 20 Hz) and low magnitude (<1g) were
grouped together, only the lumbar spine aBMD (0.004 g/cm2 [95% confidence interval
(CI), 0.000 to 0.007] p = 0.03, n = 868, studies = 3) presented a significant difference
between the WBV and control groups. No significant effect was found for total hip (-
0.000 g/cm2 [95% confidence interval (CI), -0.004 to 0.003] p = 0.95, n = 798, studies
= 2), femoral neck (-0.005 g/cm2 [95% confidence interval (CI), -0.011 to 0.001] p =
0.09, n = 272, studies = 2), trochanter (0.001 g/cm2 [95% confidence interval (CI), -
0.016 to 0.008] p = 0.77, n = 70, studies = 1); radius vBMDt (-0.90 mg/cm3 [95%
confidence interval (CI), -2.52 to 0.72] p = 0.28, n = 202, studies = 1) or tibia vBMDt
(0.35 mg/cm3 [95% confidence interval (CI), -0.60 to 1.30] p = 0.47, n = 202, studies =
1) (Supplementary Fig. 3).
High frequency and high magnitude
In the analyses grouping the studies that used high-frequency and high magnitude, no
significant effect was found in the comparison between the WBV and control groups;
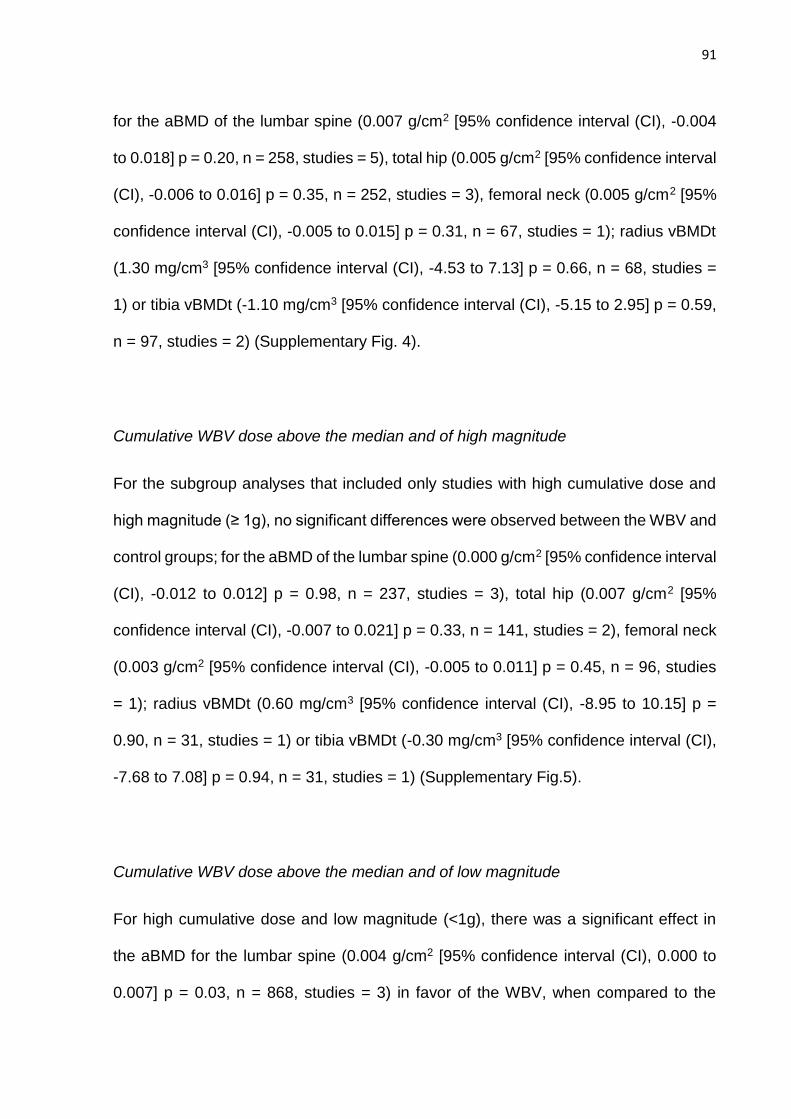
91
for the aBMD of the lumbar spine (0.007 g/cm2 [95% confidence interval (CI), -0.004
to 0.018] p = 0.20, n = 258, studies = 5), total hip (0.005 g/cm2 [95% confidence interval
(CI), -0.006 to 0.016] p = 0.35, n = 252, studies = 3), femoral neck (0.005 g/cm2 [95%
confidence interval (CI), -0.005 to 0.015] p = 0.31, n = 67, studies = 1); radius vBMDt
(1.30 mg/cm3 [95% confidence interval (CI), -4.53 to 7.13] p = 0.66, n = 68, studies =
1) or tibia vBMDt (-1.10 mg/cm3 [95% confidence interval (CI), -5.15 to 2.95] p = 0.59,
n = 97, studies = 2) (Supplementary Fig. 4).
Cumulative WBV dose above the median and of high magnitude
For the subgroup analyses that included only studies with high cumulative dose and
high magnitude (≥ 1g), no significant differences were observed between the WBV and
control groups; for the aBMD of the lumbar spine (0.000 g/cm2 [95% confidence interval
(CI), -0.012 to 0.012] p = 0.98, n = 237, studies = 3), total hip (0.007 g/cm2 [95%
confidence interval (CI), -0.007 to 0.021] p = 0.33, n = 141, studies = 2), femoral neck
(0.003 g/cm2 [95% confidence interval (CI), -0.005 to 0.011] p = 0.45, n = 96, studies
= 1); radius vBMDt (0.60 mg/cm3 [95% confidence interval (CI), -8.95 to 10.15] p =
0.90, n = 31, studies = 1) or tibia vBMDt (-0.30 mg/cm3 [95% confidence interval (CI),
-7.68 to 7.08] p = 0.94, n = 31, studies = 1) (Supplementary Fig.5).
Cumulative WBV dose above the median and of low magnitude
For high cumulative dose and low magnitude (<1g), there was a significant effect in
the aBMD for the lumbar spine (0.004 g/cm2 [95% confidence interval (CI), 0.000 to
0.007] p = 0.03, n = 868, studies = 3) in favor of the WBV, when compared to the
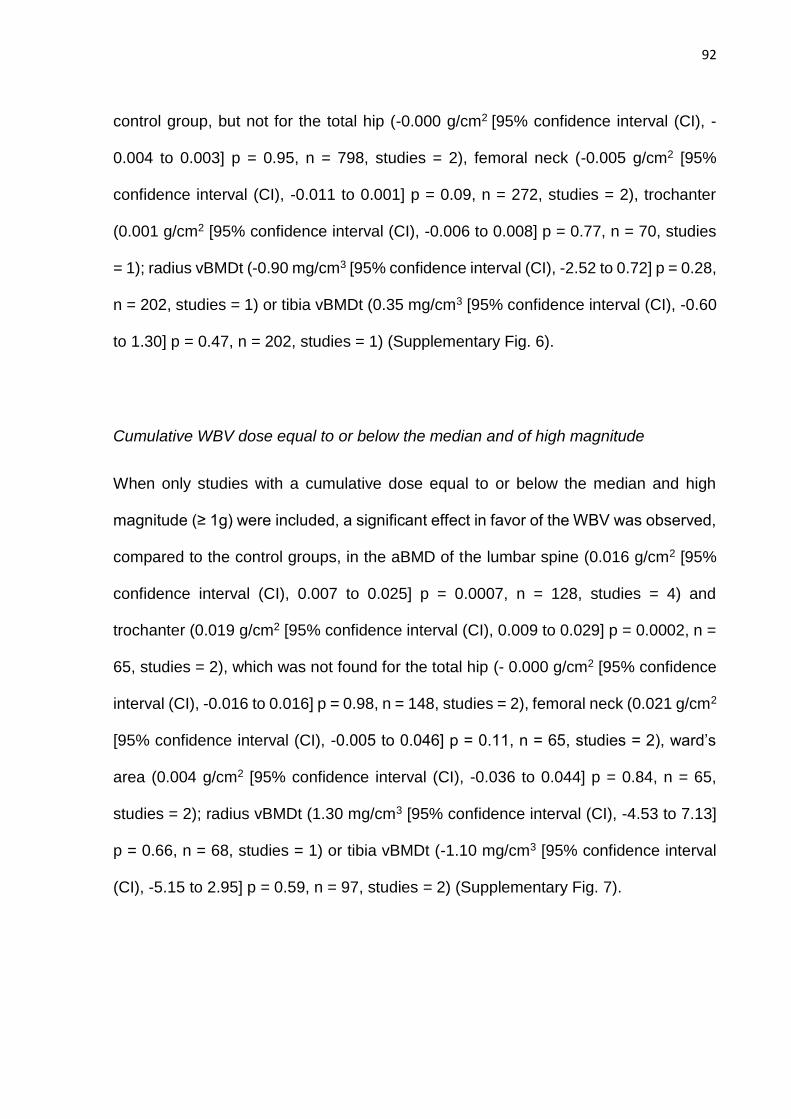
92
control group, but not for the total hip (-0.000 g/cm2 [95% confidence interval (CI), -
0.004 to 0.003] p = 0.95, n = 798, studies = 2), femoral neck (-0.005 g/cm2 [95%
confidence interval (CI), -0.011 to 0.001] p = 0.09, n = 272, studies = 2), trochanter
(0.001 g/cm2 [95% confidence interval (CI), -0.006 to 0.008] p = 0.77, n = 70, studies
= 1); radius vBMDt (-0.90 mg/cm3 [95% confidence interval (CI), -2.52 to 0.72] p = 0.28,
n = 202, studies = 1) or tibia vBMDt (0.35 mg/cm3 [95% confidence interval (CI), -0.60
to 1.30] p = 0.47, n = 202, studies = 1) (Supplementary Fig. 6).
Cumulative WBV dose equal to or below the median and of high magnitude
When only studies with a cumulative dose equal to or below the median and high
magnitude (≥ 1g) were included, a significant effect in favor of the WBV was observed,
compared to the control groups, in the aBMD of the lumbar spine (0.016 g/cm2 [95%
confidence interval (CI), 0.007 to 0.025] p = 0.0007, n = 128, studies = 4) and
trochanter (0.019 g/cm2 [95% confidence interval (CI), 0.009 to 0.029] p = 0.0002, n =
65, studies = 2), which was not found for the total hip (- 0.000 g/cm2 [95% confidence
interval (CI), -0.016 to 0.016] p = 0.98, n = 148, studies = 2), femoral neck (0.021 g/cm2
[95% confidence interval (CI), -0.005 to 0.046] p = 0.11, n = 65, studies = 2), ward’s
area (0.004 g/cm2 [95% confidence interval (CI), -0.036 to 0.044] p = 0.84, n = 65,
studies = 2); radius vBMDt (1.30 mg/cm3 [95% confidence interval (CI), -4.53 to 7.13]
p = 0.66, n = 68, studies = 1) or tibia vBMDt (-1.10 mg/cm3 [95% confidence interval
(CI), -5.15 to 2.95] p = 0.59, n = 97, studies = 2) (Supplementary Fig. 7).
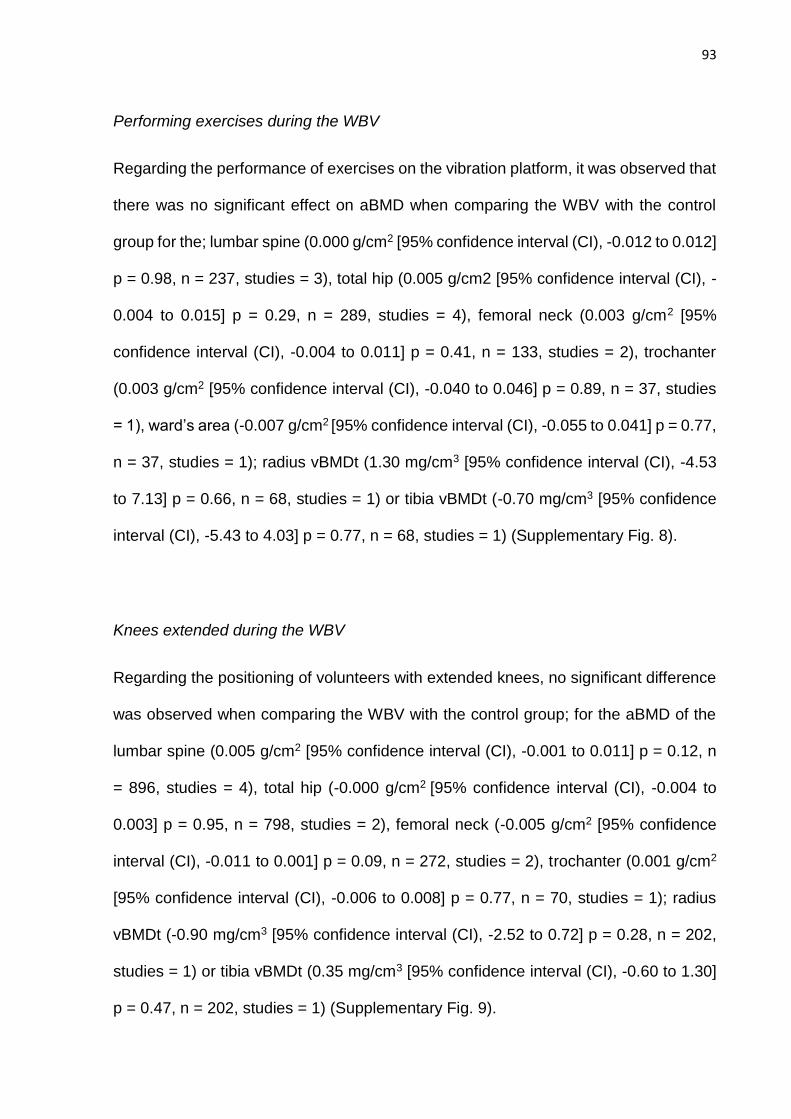
93
Performing exercises during the WBV
Regarding the performance of exercises on the vibration platform, it was observed that
there was no significant effect on aBMD when comparing the WBV with the control
group for the; lumbar spine (0.000 g/cm2 [95% confidence interval (CI), -0.012 to 0.012]
p = 0.98, n = 237, studies = 3), total hip (0.005 g/cm2 [95% confidence interval (CI), -
0.004 to 0.015] p = 0.29, n = 289, studies = 4), femoral neck (0.003 g/cm2 [95%
confidence interval (CI), -0.004 to 0.011] p = 0.41, n = 133, studies = 2), trochanter
(0.003 g/cm2 [95% confidence interval (CI), -0.040 to 0.046] p = 0.89, n = 37, studies
= 1), ward’s area (-0.007 g/cm2 [95% confidence interval (CI), -0.055 to 0.041] p = 0.77,
n = 37, studies = 1); radius vBMDt (1.30 mg/cm3 [95% confidence interval (CI), -4.53
to 7.13] p = 0.66, n = 68, studies = 1) or tibia vBMDt (-0.70 mg/cm3 [95% confidence
interval (CI), -5.43 to 4.03] p = 0.77, n = 68, studies = 1) (Supplementary Fig. 8).
Knees extended during the WBV
Regarding the positioning of volunteers with extended knees, no significant difference
was observed when comparing the WBV with the control group; for the aBMD of the
lumbar spine (0.005 g/cm2 [95% confidence interval (CI), -0.001 to 0.011] p = 0.12, n
= 896, studies = 4), total hip (-0.000 g/cm2 [95% confidence interval (CI), -0.004 to
0.003] p = 0.95, n = 798, studies = 2), femoral neck (-0.005 g/cm2 [95% confidence
interval (CI), -0.011 to 0.001] p = 0.09, n = 272, studies = 2), trochanter (0.001 g/cm2
[95% confidence interval (CI), -0.006 to 0.008] p = 0.77, n = 70, studies = 1); radius
vBMDt (-0.90 mg/cm3 [95% confidence interval (CI), -2.52 to 0.72] p = 0.28, n = 202,
studies = 1) or tibia vBMDt (0.35 mg/cm3 [95% confidence interval (CI), -0.60 to 1.30]
p = 0.47, n = 202, studies = 1) (Supplementary Fig. 9).
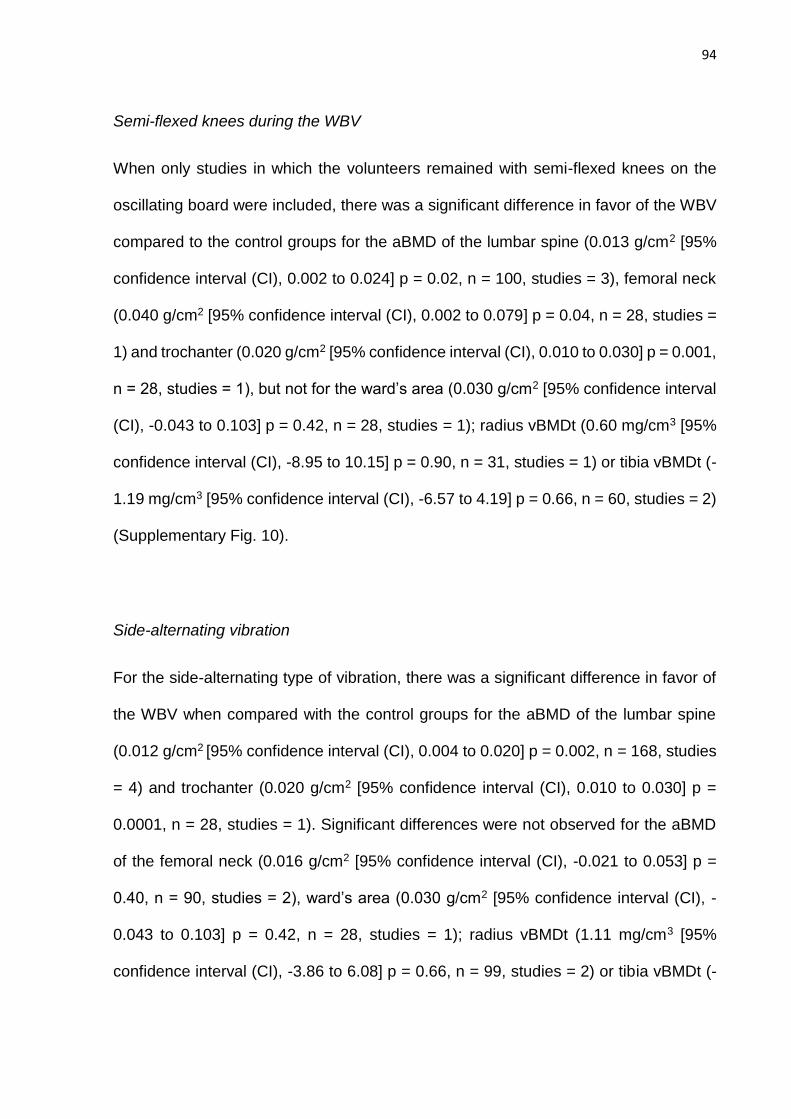
94
Semi-flexed knees during the WBV
When only studies in which the volunteers remained with semi-flexed knees on the
oscillating board were included, there was a significant difference in favor of the WBV
compared to the control groups for the aBMD of the lumbar spine (0.013 g/cm2 [95%
confidence interval (CI), 0.002 to 0.024] p = 0.02, n = 100, studies = 3), femoral neck
(0.040 g/cm2 [95% confidence interval (CI), 0.002 to 0.079] p = 0.04, n = 28, studies =
1) and trochanter (0.020 g/cm2 [95% confidence interval (CI), 0.010 to 0.030] p = 0.001,
n = 28, studies = 1), but not for the ward’s area (0.030 g/cm2 [95% confidence interval
(CI), -0.043 to 0.103] p = 0.42, n = 28, studies = 1); radius vBMDt (0.60 mg/cm3 [95%
confidence interval (CI), -8.95 to 10.15] p = 0.90, n = 31, studies = 1) or tibia vBMDt (-
1.19 mg/cm3 [95% confidence interval (CI), -6.57 to 4.19] p = 0.66, n = 60, studies = 2)
(Supplementary Fig. 10).
Side-alternating vibration
For the side-alternating type of vibration, there was a significant difference in favor of
the WBV when compared with the control groups for the aBMD of the lumbar spine
(0.012 g/cm2 [95% confidence interval (CI), 0.004 to 0.020] p = 0.002, n = 168, studies
= 4) and trochanter (0.020 g/cm2 [95% confidence interval (CI), 0.010 to 0.030] p =
0.0001, n = 28, studies = 1). Significant differences were not observed for the aBMD
of the femoral neck (0.016 g/cm2 [95% confidence interval (CI), -0.021 to 0.053] p =
0.40, n = 90, studies = 2), ward’s area (0.030 g/cm2 [95% confidence interval (CI), -
0.043 to 0.103] p = 0.42, n = 28, studies = 1); radius vBMDt (1.11 mg/cm3 [95%
confidence interval (CI), -3.86 to 6.08] p = 0.66, n = 99, studies = 2) or tibia vBMDt (-
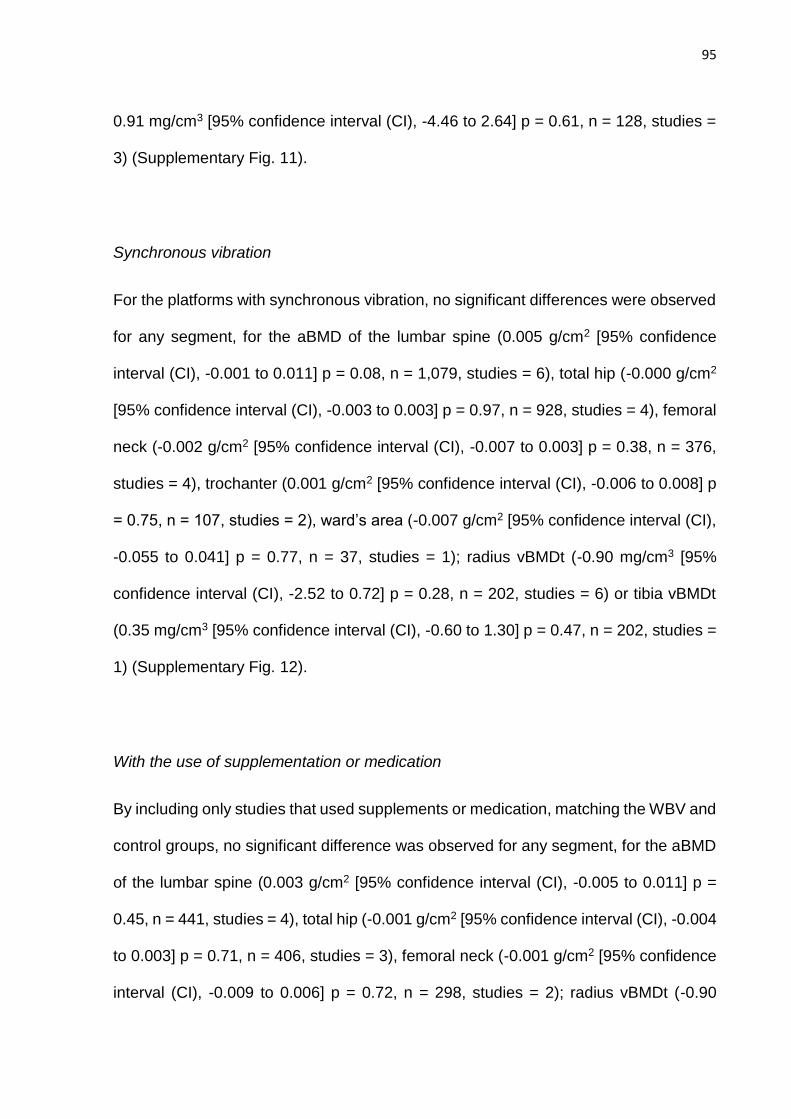
95
0.91 mg/cm3 [95% confidence interval (CI), -4.46 to 2.64] p = 0.61, n = 128, studies =
3) (Supplementary Fig. 11).
Synchronous vibration
For the platforms with synchronous vibration, no significant differences were observed
for any segment, for the aBMD of the lumbar spine (0.005 g/cm2 [95% confidence
interval (CI), -0.001 to 0.011] p = 0.08, n = 1,079, studies = 6), total hip (-0.000 g/cm2
[95% confidence interval (CI), -0.003 to 0.003] p = 0.97, n = 928, studies = 4), femoral
neck (-0.002 g/cm2 [95% confidence interval (CI), -0.007 to 0.003] p = 0.38, n = 376,
studies = 4), trochanter (0.001 g/cm2 [95% confidence interval (CI), -0.006 to 0.008] p
= 0.75, n = 107, studies = 2), ward’s area (-0.007 g/cm2 [95% confidence interval (CI),
-0.055 to 0.041] p = 0.77, n = 37, studies = 1); radius vBMDt (-0.90 mg/cm3 [95%
confidence interval (CI), -2.52 to 0.72] p = 0.28, n = 202, studies = 6) or tibia vBMDt
(0.35 mg/cm3 [95% confidence interval (CI), -0.60 to 1.30] p = 0.47, n = 202, studies =
1) (Supplementary Fig. 12).
With the use of supplementation or medication
By including only studies that used supplements or medication, matching the WBV and
control groups, no significant difference was observed for any segment, for the aBMD
of the lumbar spine (0.003 g/cm2 [95% confidence interval (CI), -0.005 to 0.011] p =
0.45, n = 441, studies = 4), total hip (-0.001 g/cm2 [95% confidence interval (CI), -0.004
to 0.003] p = 0.71, n = 406, studies = 3), femoral neck (-0.001 g/cm2 [95% confidence
interval (CI), -0.009 to 0.006] p = 0.72, n = 298, studies = 2); radius vBMDt (-0.90
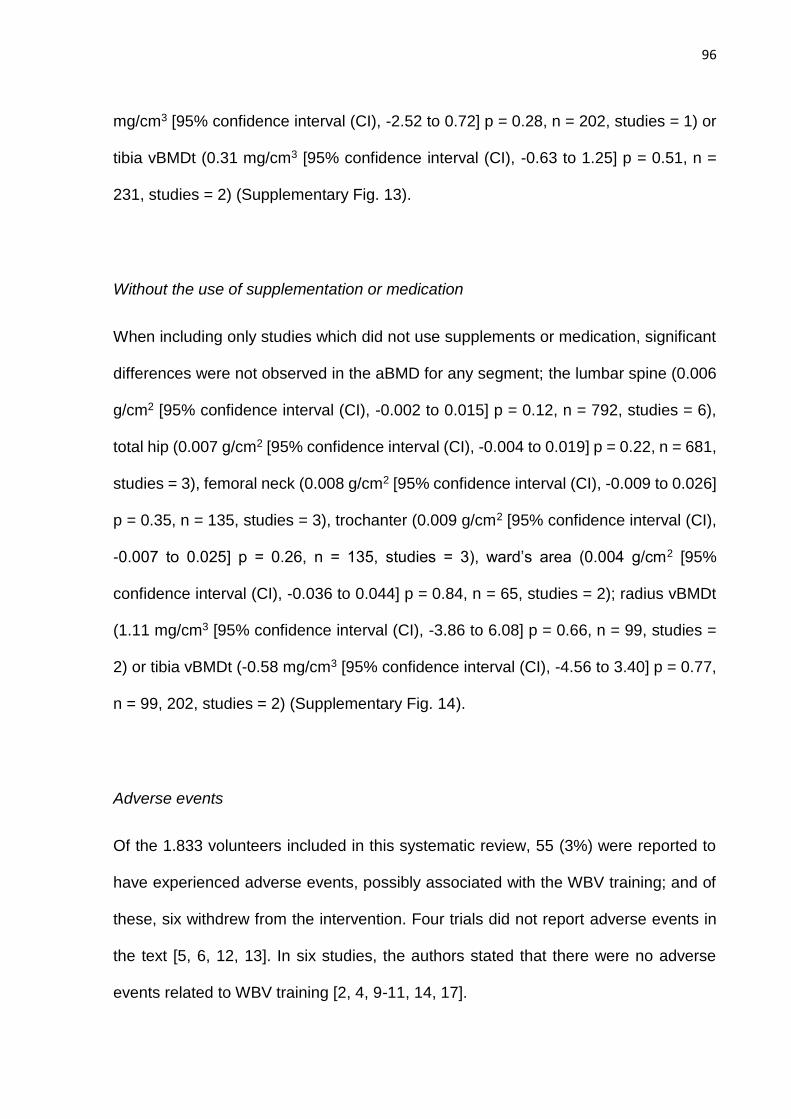
96
mg/cm3 [95% confidence interval (CI), -2.52 to 0.72] p = 0.28, n = 202, studies = 1) or
tibia vBMDt (0.31 mg/cm3 [95% confidence interval (CI), -0.63 to 1.25] p = 0.51, n =
231, studies = 2) (Supplementary Fig. 13).
Without the use of supplementation or medication
When including only studies which did not use supplements or medication, significant
differences were not observed in the aBMD for any segment; the lumbar spine (0.006
g/cm2 [95% confidence interval (CI), -0.002 to 0.015] p = 0.12, n = 792, studies = 6),
total hip (0.007 g/cm2 [95% confidence interval (CI), -0.004 to 0.019] p = 0.22, n = 681,
studies = 3), femoral neck (0.008 g/cm2 [95% confidence interval (CI), -0.009 to 0.026]
p = 0.35, n = 135, studies = 3), trochanter (0.009 g/cm2 [95% confidence interval (CI),
-0.007 to 0.025] p = 0.26, n = 135, studies = 3), ward’s area (0.004 g/cm2 [95%
confidence interval (CI), -0.036 to 0.044] p = 0.84, n = 65, studies = 2); radius vBMDt
(1.11 mg/cm3 [95% confidence interval (CI), -3.86 to 6.08] p = 0.66, n = 99, studies =
2) or tibia vBMDt (-0.58 mg/cm3 [95% confidence interval (CI), -4.56 to 3.40] p = 0.77,
n = 99, 202, studies = 2) (Supplementary Fig. 14).
Adverse events
Of the 1.833 volunteers included in this systematic review, 55 (3%) were reported to
have experienced adverse events, possibly associated with the WBV training; and of
these, six withdrew from the intervention. Four trials did not report adverse events in
the text [5, 6, 12, 13]. In six studies, the authors stated that there were no adverse
events related to WBV training [2, 4, 9-11, 14, 17].
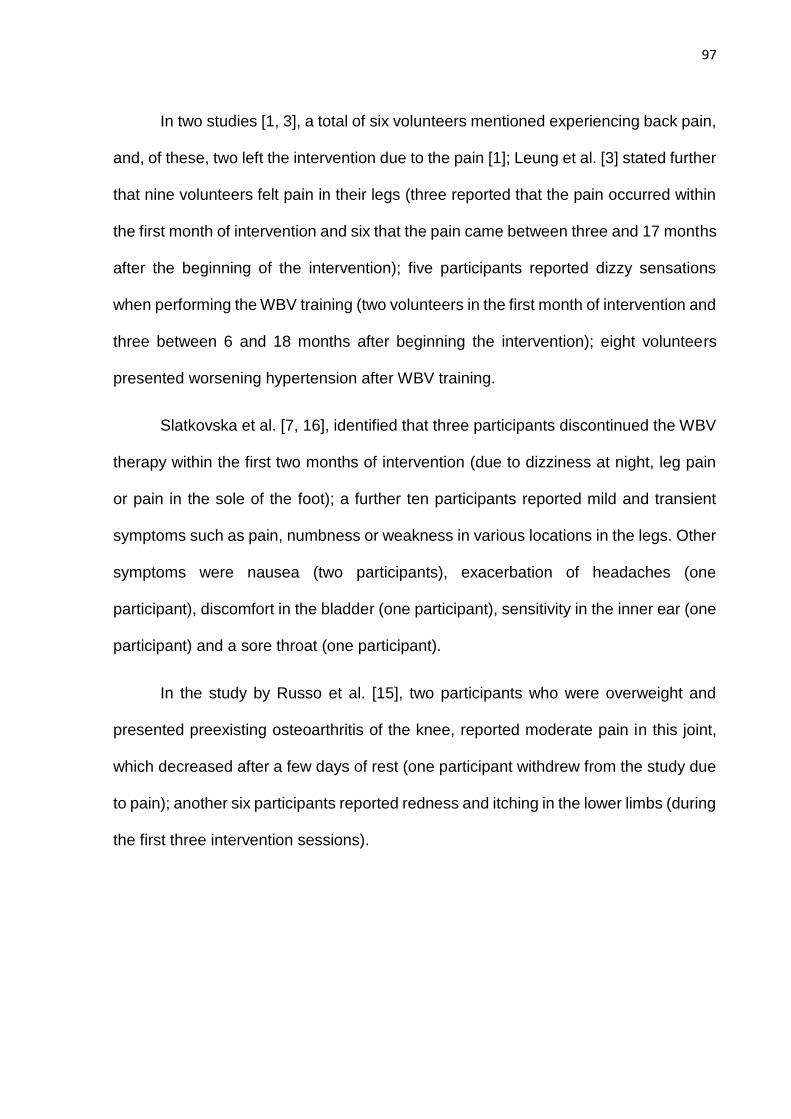
97
In two studies [1, 3], a total of six volunteers mentioned experiencing back pain,
and, of these, two left the intervention due to the pain [1]; Leung et al. [3] stated further
that nine volunteers felt pain in their legs (three reported that the pain occurred within
the first month of intervention and six that the pain came between three and 17 months
after the beginning of the intervention); five participants reported dizzy sensations
when performing the WBV training (two volunteers in the first month of intervention and
three between 6 and 18 months after beginning the intervention); eight volunteers
presented worsening hypertension after WBV training.
Slatkovska et al. [7, 16], identified that three participants discontinued the WBV
therapy within the first two months of intervention (due to dizziness at night, leg pain
or pain in the sole of the foot); a further ten participants reported mild and transient
symptoms such as pain, numbness or weakness in various locations in the legs. Other
symptoms were nausea (two participants), exacerbation of headaches (one
participant), discomfort in the bladder (one participant), sensitivity in the inner ear (one
participant) and a sore throat (one participant).
In the study by Russo et al. [15], two participants who were overweight and
presented preexisting osteoarthritis of the knee, reported moderate pain in this joint,
which decreased after a few days of rest (one participant withdrew from the study due
to pain); another six participants reported redness and itching in the lower limbs (during
the first three intervention sessions).
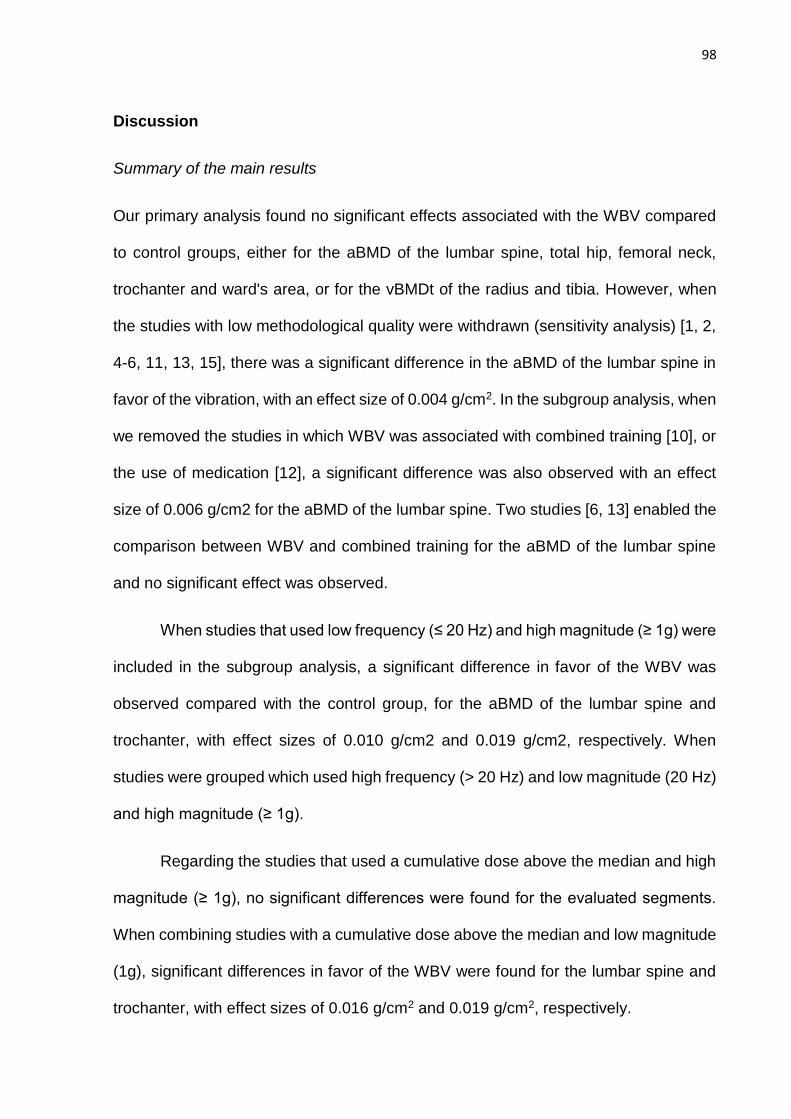
98
Discussion
Summary of the main results
Our primary analysis found no significant effects associated with the WBV compared
to control groups, either for the aBMD of the lumbar spine, total hip, femoral neck,
trochanter and ward's area, or for the vBMDt of the radius and tibia. However, when
the studies with low methodological quality were withdrawn (sensitivity analysis) [1, 2,
4-6, 11, 13, 15], there was a significant difference in the aBMD of the lumbar spine in
favor of the vibration, with an effect size of 0.004 g/cm2. In the subgroup analysis, when
we removed the studies in which WBV was associated with combined training [10], or
the use of medication [12], a significant difference was also observed with an effect
size of 0.006 g/cm2 for the aBMD of the lumbar spine. Two studies [6, 13] enabled the
comparison between WBV and combined training for the aBMD of the lumbar spine
and no significant effect was observed.
When studies that used low frequency (≤ 20 Hz) and high magnitude (≥ 1g) were
included in the subgroup analysis, a significant difference in favor of the WBV was
observed compared with the control group, for the aBMD of the lumbar spine and
trochanter, with effect sizes of 0.010 g/cm2 and 0.019 g/cm2, respectively. When
studies were grouped which used high frequency (> 20 Hz) and low magnitude (20 Hz)
and high magnitude (≥ 1g).
Regarding the studies that used a cumulative dose above the median and high
magnitude (≥ 1g), no significant differences were found for the evaluated segments.
When combining studies with a cumulative dose above the median and low magnitude
(1g), significant differences in favor of the WBV were found for the lumbar spine and
trochanter, with effect sizes of 0.016 g/cm2 and 0.019 g/cm2, respectively.
99
When interventions were grouped which used performance of strengthening
exercises for the lower limbs during the WBV; or standing with the knees extended
during the WBV, no significant effects were observed. However, for positioning with
semi-flexed knees during the WBV, a significant difference was observed in favor of
vibration for the aBMD of the lumbar spine, femoral neck and trochanter, with effect
sizes of 0.013 g/cm2, 0.040 g/cm2 and 0.020 g/cm2, respectively.
Regarding the type of vibration, a significant difference was observed when the
platforms were side alternating for the aBMD of the lumbar spine and trochanter, with
effect sizes of 0.012 g/cm2 and 0.020 g/cm2, respectively. No difference was observed
when studies with synchronous vibration platforms were grouped. When including
studies that used supplementation of calcium, vitamin D or medication, in order to
equate the WBV and control groups, no significant effect was observed, or when only
studies that did not use these substances were included.
It is possible to observe that, in general, the significant results for the aBMD
were not accompanied by large effect sizes; ranging from 0.004 g/cm2 to 0.016 g/cm2
for the lumbar spine (in the sensitivity analysis in seven subgroup analyses), 0.019
g/cm2 to 0.020 g/cm2 for the trochanter (four subgroup analyses) and 0.040 g/cm2 for
the femoral neck (in one subgroup analysis). However, these effect sizes are
comparable with other forms of intervention, pharmacological or otherwise, such as
appropriate supplementation of calcium and vitamin D [22, 43], the use of alendronate
or hormone replacement therapy [22] and interventions with different forms of physical
exercise [23].
Our meta-analysis found that, independent of factors that may influence the
intensity of the vibration (e.g., frequency, magnitude, cumulative dose and position of
100
the volunteer), the lumbar spine presented a significant improvement when the low
methodological quality studies were removed (sensitivity analysis) and when the
studies that combined WBV with combined training or medication were removed. The
lumbar spine presented a significant difference for aBMD in six other subgroup
analyses (low frequency and high magnitude; high-frequency and low magnitude;
cumulative dose above the median and low magnitude; cumulative dose equal to or
below the median and high magnitude; side alternating vibration, and positioned with
semi-flexed knees). In addition, for all analyses for the aBMD of the lumbar spine,
where significant results were reported, there was homogeneity between the studies,
with the exception of one subgroup analysis (which excluded studies that combined
WBV and combined training, or WBV and medication). However, the low number of
RCTs included in the analysis (between three and eight), limit extrapolation of these
findings which should be analyzed with caution, added to the fact that studies were
included in the subgroup analyses regardless of their methodological quality.
The inferences regarding the significant effect found for the aBMD of the femoral
neck (semi-flexed knee during WBV) and trochanter (low frequency and high
magnitude; cumulative dose equal to or below the median and high magnitude, side
alternating side vibration, and positioned with semi-flexed knees) are weakened
primarily by the number of studies included in the analysis (between one and two
RCTs), which had, for the most part, only one RCT, and by the methodological quality
of the studies being low. For the other segments included in the meta-analysis (total
hip, ward's area, radius and tibia) no significant differences were observed. The low
number of studies including such segments may have been a limiting factor, especially
in relation to the aBMD of the ward's area and the vBMDt of the radius and tibia.
101
Agreements and disagreements with other studies
In a previously performed meta-analysis [31], which aimed to identify the effects of
WBV on BMD of the hip and lumbar spine in older women (50 years or more), the
authors found no significant differences in the comparisons of WBV, between the
control group and exercise groups. At that time, only a few studies were available to
the authors for the metaanalysis, which was carried out with comparisons involving
only two studies for the hip and three studies for the lumbar spine.
Another meta-analysis [30], conducted with postmenopausal women, found a
significant difference in favor of WBV for the aBMD of the total hip (0.014 g/cm2), but
there was only one RCT included in the analysis. In the present study, six RCTs were
included that evaluated the aBMD of the total hip and no significant results were found.
Other data that differ are those related to the significant effects we found for the aBMD
of the lumbar spine (in the sensitivity analysis and seven subgroup analyses). The
authors [30], on that occasion, had only four RCTs that evaluated the aBMD of the
lumbar spine and found no significant differences for this segment in any comparison
(primary, sensitivity or subgroup).
Another difference was found when excluding the studies that combined the use
of medication with WBV or combined training with WBV, wherein a significant
difference in favor of vibration was observed for the aBMD of the lumbar spine. The
authors [30] had only one study that combined medication with WBV; and found
significant results only for aBMD of the hip when excluding this study from the analysis.
As in the present study, no difference was observed in the comparison between WBV
and other forms of physical exercise [30]. Finally, in our analysis, we found significant
102
results regarding the inclusion of studies with a cumulative dose above the median and
low magnitude (for aBMD of the lumbar spine); and cumulative dose equal to or below
the median and high magnitude (with an even greater effect size for the lumbar spine
and a significant effect for the trochanter), whereas at that time, due to the lower
number of RCTs, the authors [30] found no differences for these same subgroup
analyses.
Unlike the two previous reviews [30, 31], the larger number of RCTs included in
our meta-analysis allowed us to explore different subgroup analyses. We observed
that a high frequency associated with low magnitude contributed to the increase in the
aBMD of the lumbar spine (0.004 g/cm2). This premise (low magnitude and high
frequency) has been shown to be effective for improving BMD in animal models [24-
26], however, in our meta-analysis involving postmenopausal women, only three
studies [3, 7, 14] tested this hypothesis. As previously mentioned in another study [30],
the use of low magnitude can also contribute to increased BMD, disproving Wolff's law
of bone remodeling [44], in which there is a need for high impact activities (high
magnitude) to enable an osteogenic effect.
However, we found that a low frequency, associated with high magnitude, also
enabled significant effects on the aBMD of the lumbar spine, with a greater effect size
(0.010 g/cm2), as well as the aBMD of the trochanter (0.019 g/cm2). Despite enabling
a greater effect on BMD, the safety of the participants, when exposed to high
magnitudes (≥ 1g) during WBV, has been discussed, especially as people undergoing
treatment or prevention of osteoporosis are mainly older adults who are more prone to
adverse events [41], which should be considered in interventions involving high
magnitudes. Interestingly, despite the higher number of studies [4-6, 8-10, 13, 15] that
investigated the association between highfrequency and high magnitude, no significant
103
difference was observed in this subgroup analysis. The lack of effects observed in this
case may be related to the placement of the volunteers during the WBV, which
diverged in the studies between maintaining the knees straight [4], semi-flexed knees
[6, 15] and performing exercises during vibration [5, 8, 9, 10, 13]. The previous
analyses demonstrated a higher standardization in positioning, wherein all volunteers
had their knees extended (in the subgroups analysis of high frequency and low
magnitude) [3, 7, 14] or the majority of the studies opted to maintain the semi-flexed
knee position (in the subgroups analysis of low frequency and high magnitude) [2, 11,
12].
In fact, the position of the body on the oscillating plate of the platform during the
WBV appears to influence the transmissibility of the vibration to the skeleton [45, 46].
Our subgroup analyses demonstrated that maintaining the knees semi-flexed
contributed to a significant improvement in the aBMD of the lumbar spine, femoral neck
and trochanter, while no effect was observed in the subgroup analyses with the knees
straight, or when performing strengthening exercises during the WBV. Hypothetically,
a static posture with knees straight would be capable of higher transmissibility
throughout the skeleton. However, it was demonstrated that the dampening as a
function of the position with semi-flexed knees is insignificant for the femur and lumbar
spine at frequencies up to 30 Hz [46], which may explain the significant effects that
were found, since most studies [2, 11, 12], in which the static posture was with the
knees semi-flexed, used low frequency and high magnitude.
Our subgroup analysis also demonstrated that the performance of strengthening
exercises for the lower limbs (principally squats) during the WBV had no significant
effect. It is possible this can be explained by the alternating body position during the
oscillations which hampers the transmission of vibrations through the skeleton.
104
Moreover, it has been discussed that the vibration itself, independent of muscle
activity, would be capable of inducing bone remodeling, as in the position with the
knees extended [46]. On the other hand, in our subgroup analysis, we observed no
significant effect on BMD when the volunteers maintained this position. This result
might be explained by the type of vibration, as the majority of studies (in which the
position of the volunteers was with knees extended), used synchronous vibration
platforms [3, 7, 14].
When the studies that used this type of platform (synchronous vibration) were
grouped, no significant effect was observed, however, for the platforms with side
alternating oscillation, significant effects were observed for the aBMD of the lumbar
spine and trochanter. Unlike the synchronous platforms, in which both legs move up
and down at the same time, in the side alternating platforms, the oscillations take place
around a pivot at the center of the platform, which exposes the user to alternate
vibrations between the sides, that is, while the right foot moves up, the left foot moves
down, and vice versa [28]. The only study in the present review which compared the
effects of side alternating and synchronous oscillation, found no differences between
the intervention groups, although only the side alternating vibration was statistically
different from the control group in the post-intervention [9].
Finally, the use or not of medicaments or supplements, identically distributed
between the experimental and control groups, did not indicate any significant effect on
the subgroup analyses. This occurred because the randomization process, if
performed properly, distributed the differences equally between the volunteers in the
groups. Thus, the use of such substances, aiming to match experimental and control
groups, does not appear to be crucial in RCTs, which have as their objective to verify
the effects of WBV on BMD in postmenopausal women.
105
Quality of evidence
The 15 studies included in our meta-analysis were from North America [2, 7, 14],
Europe [1, 5, 6, 8-11, 13, 15] and Asia [3, 4, 12], which limits generalizations about the
applicability of the evidence in other locations. The quality of the studies was variable
and this should be taken into account when interpreting the results of this review (with
the exception of the sensitivity analysis, which only included RCTs with high
methodological quality). The majority of studies presented a high risk of bias. Only
seven studies were considered high quality [3, 7-10, 12, 14]. Only one study blinded
patients and therapists [14], while the majority blinded evaluators [3, 6-10, 13, 14]. In
therapies where the stimuli are perceived, it is very difficult, if not impossible, to blind
patients or therapists [36], as is the case of interventions involving WBV. However, it
is unlikely that this bias influenced the BMD measures.
The majority of RCTs [1, 4, 7-10, 12, 15] included follow-up of at least 85% of
the participants. However, most studies used small samples. Another limitation relates
to the intervention time, which was close to six months in the majority of studies (the
minimum time used to find differences in BMD). Six studies did not report the condition
of the volunteers regarding the BMD classification (unchanged, osteopenic or
osteoporotic), a fact that does not allow a subgroup analysis of this variable. Another
factor, refers to the great heterogeneity among the studies regarding the parameters
used in WBV (frequency, magnitude, cumulative dose, positioning on the oscillation
board and type of vibration), making it difficult to compare studies. Moreover, most of
the studies did not report whether the subjects were using shoe or were barefoot during
vibration; and no study has described the use of mats (e.g., EVA) on the oscillation
plate of the vibrating platform. These details are important, since they can interfere
with the intensity of the WBV [27].
106
Finally, we did not perform a subgroup analysis taking into account different age
groups, since the RCTs, generally included women from the beginning of
postmenopause to a more advanced age. It has been suggested in the literature [47]
that the skeleton of younger women may respond differently to mechanical vibration
stimuli compared with that of older individuals.
Potential biases in the review process
The present review included only RCTs, which reduces the risk of bias. However, the
majority of studies did not hide the distribution of volunteers into each group. Most of
the studies adequately dealt with the incomplete follow-up data, performing ITT
analysis [3, 5, 7-10, 12, 14]. In this respect, the results by protocol (only participants
who completed the intervention), were used in our analysis only when ITT was not
available. For the majority of the studies [1, 4, 6, 7, 9, 10, 12, 13], the mean and
standard deviation of the absolute difference in BMD between pre- and post-
intervention was available. However, for some studies [2, 3, 5, 8, 11, 14, 15], statistical
manipulation was necessary, which reduces the accuracy of the data entered in the
meta-analysis. Finally, the search did not extend to all existing databases.
Nonetheless, we performed searches in three primary databases (PubMed, Web of
Science and LILACS), two secondary databases (The Cochrane Library, and PEDro)
and a base of registered clinical trials (clinicaltrials.gov), aiming to find unpublished
studies. In addition, we conducted a thorough search of all the references of the studies
included in the review in an attempt to find other RCTs. Regarding the use of the funnel
plot, it is not recommended to distinguish possible risk of bias in analysis with less than
10 studies [42]. Thus, it was possible to perform the test only in the primary analysis,
107
which verified the effects of WBV on aBMD of the lumbar spine, in which no asymmetry
was observed (Supplementary Fig. 15).
Conclusions
Implications for practice
Our results in the sensitivity analysis suggest that WBV training has the potential to
contribute to increasing BMD in postmenopausal women, particularly when the
objective is related to the area of the lumbar spine, which was shown to be the most
responsive osteogenesis area. Other skeletal sites appear to be more dependent on
different factors that can influence the intensity of the vibration, such as the trochanter,
where alterations in BMD were dependent on lowfrequency, low cumulative dose, high
magnitude, semi-flexed knees and side alternating vibration type; while the femoral
neck region demonstrated some potential benefits regarding increased BMD only in
the semi-flexed knee position.
As WBV training is considered relatively safe, does not depend on great
motivation for its practice and has few adverse events, its use can be considered as
an adjunctive treatment to combat the loss of BMD, especially in patients who present
limitations to the practice of high impact physical exercise. However, despite our study
having contributed to preliminary discussions, all the factors that represent an ideal
intervention are still not clear; and the low methodological quality of the studies
included in our subgroup analyses should be taken into account. In addition, our
primary analyses found no evidence of a beneficial effect of WBV on BMD.
108
Implications for research
Our different subgroup analyses have helped in the understanding of how different
factors (frequency, magnitude, cumulative dose, body positioning and vibration type)
influence the effects of WBV on the BMD of postmenopausal women, subjected to
WBV training, and could contribute to the definition of future research protocols.
However, the small number of RCTs and low methodological quality of the majority of
studies limited extrapolations of our findings. For future studies, we suggest greater
methodological care, especially with regard to allocation concealment and blinding of
evaluators. Larger samples and longer follow-up times are also necessary, which could
help clarify the long-term effects of WBV on the BMD of postmenopausal women.
Conflicts of interest Oliveira, Laís Campos de; Oliveira, Raphael Gonçalves de; and
Pires-Oliveira, Deise Aparecida de Almeida, declare that they have no conflict of
interest
References
1. Santin-Medeiros F, Santos-Lozano A, Rey-López JP, Garatachea N (2015) Effects
of eight months of whole body vibration training on hip bone mass in older women.
Nutr Hosp 31: 1654-1659. doi: 10.3305/nh.2015.31.4.8441
2. Liphardt AM, Schipilow J, Hanley DA, Boyd SK (2015) Bone quality in osteopenic
postmenopausal women is not improved after 12 months of whole-body vibration
training. Osteoporos Int. 26: 911-920. doi: 10.1007/s00198-014-2995- 8
109
3. Leung KS, Li CY, Tse YK, Choy TK, Leung PC, Hung VWY, Chan SY, Leung AHC,
Cheung WH (2014) Effects of 18-month low-magnitude high-frequency vibration on fall
rate and fracture risks in 710 community elderly - a cluster - randomized controlled
trial. Osteoporos Int 25: 1785-1795. doi: 10.1007/s00198-014-2693-6
4. Lai CL, Tseng SY, Chen CN, Liao WC, Wang CH, Lee MC, Hsu PS (2013) Effect of
6 months of whole body vibration on lumbar spine bone density in postmenopausal
women: a randomized controlled trial. Clin Interv Aging 8: 1603-1609. doi:
10.2147/CIA.S53591
5. Stolzenberg N, Belavý DL, Beller G, Armbrecht G, Semler J, Felsenberg D (2013)
Bone strength and density via pQCT in post-menopausal osteopenic women after 9
months resistive exercise with whole body vibration or proprioceptive exercise. J
Musculoskelet Neuronal Interact 13: 66-76
6. Karakiriou SK, Douda HT, Smilios IG, Volaklis KA, Tokmakidis SP (2012) Effects of
vibration and exercise training on bone mineral density and muscle strength in post-
menopausal women. Eur J Sport Sci 12: 81-88. doi: 10.1080/17461391.2010.536581
7. Slatkovska L, Alibhai SMH, Beyene J, Hu H, Demaras A, Cheung AM (2011) Effect
of 12 Months of Whole-Body Vibration Therapy on Bone Density and Structure in
Postmenopausal Women. A Randomized Trial. Annals Intern Med 155: 668-679. doi:
10.7326/0003-4819-155-10-201111150-00005
8. Verschueren SMP, Bogaerts A, Delecluse C, Claessens AL, Haentjens P,
Vanderschueren D, Boonen S (2011) The Effects of Whole-Body Vibration Training
and Vitamin D Supplementation on Muscle Strength, Muscle Mass, and Bone Density
in Institutionalized Elderly Women: A 6-Month Randomized, Controlled Trial. J Bone
Miner Res 26: 42-49. doi: 10.1002/jbmr.181
110
9. Von Stengel S, Kemmler W, Bebenek M, Engelke K, Kalender WA (2011a) Effects
of Whole-Body Vibration Training on Different Devices on Bone Mineral Density.
ACSM 43: 1071-1079. doi: 10.1249/MSS.0b013e318202f3d3
10. Von Stengel S, Kemmler W, Engelke K, Kalender WA (2011b) Effects of whole
body vibration on bone mineral density and falls: results of the randomized controlled
ELVIS study with postmenopausal women. Osteoporos Int 22: 317-325. doi:
10.1007/s00198-010-1215-4
11. Gusi N, Raimundo A, Leal A (2006) Low-frequency vibratory exercise reduces the
risk of bone fracture more than walking: a randomized controlled trial. BMC
Musculoskelet Disord 7: 92. doi: 10.1186/1471-2474-7-92
12. Iwamoto J, Takeda T, Sato Y, Uzawa M (2005) Effect of whole-body vibration
exercise on lumbar bone mineral density, bone turnover, and chronic back pain in post-
menopausal osteoporotic women treated with alendronate. Aging Clin Exp Res 17:
157-163
13. Verschueren SMP, Roelants M, Delecluse C, Swinnen S, Vanderschueren D,
Boonen S (2004) Effect of 6-Month Whole Body Vibration Training on Hip Density,
Muscle Strength, and Postural Control in Postmenopausal Women: A Randomized
Controlled Pilot Study. J Bone Miner Res 19: 352-359 doi: 10.1359/JBMR.0301245
14. Rubin C, Recker R, Cullen D, Ryaby J, McCabe J, McLeod K (2004) Prevention of
Postmenopausal Bone Loss by a Low-Magnitude, High-Frequency Mechanical Stimuli:
A Clinical Trial Assessing Compliance, Efficacy, and Safety. J Bone Miner Res 19:
343-351. doi: 10.1359/JBMR.0301251
15. Russo CR, Lauretani F, Bandinelli S, Bartali B, Cavazzini C, Guralnik JM, Ferrucci
L (2003) High-Frequency Vibration Training Increases Muscle Power in
111
Postmenopausal Women. Arch Phys Med Rehabil 84: 1854-1857. doi:
10.1016/S0003-9993(03)00357-5
16. Slatkovska L, Beyene J, Alibhai, SMH, Wong Q, Sohail QZ, Cheung AM (2014)
Effect of Whole-Body Vibration on Calcaneal Quantitative Ultrasound Measurements
in Postmenopausal Women: A Randomized Controlled Trial. Calcif Tissue Int 95: 547-
556. doi: 10.1007/s00223-014-9920-1
17. Beck BR, Norling TL (2010) The Effect of Eight Months of Twice-Weekly Low or
Higher Intensity Whole Body Vibration on Risk Factors for Postmenopausal Hip
Fracture. Am J Phys Med Rehabil 89: 997-1009. doi:
10.1097/PHM.0b013e3181f71063
18. Bemben DA, Palmer IJ, Bemben MG, Knehans AW (2010) Effects of combined
whole-body vibration and resistance training on muscular strength and bone
metabolism in postmenopausal women. Bone 47: 650-656. doi:
10.1016/j.bone.2010.06.019
19. Ruan X, Jin F, Liu Y, Peng Z, Sun Y (2008) Effects of vibration therapy on bone
mineral density in postmenopausal women with osteoporosis. Chin Med J 121: 1155-
1158
20. Zaki ME (2014) Effects of whole body vibration and resistance training on bone
mineral density and anthropometry in obese postmenopausal women. J Osteoporos
2014: 702589. doi: 10.1155/2014/702589
21. Christenson ES, Jiang X, Kagan R, Schnatz PF (2012) Osteoporosis management
in post-menopausal women. Min Ginecol 64: 181-194
22. Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P, Rosen C, Osteoporosis
Methodology Group and The Osteoporosis Research Advisory Group (2002) Meta-
112
analyses of therapies for postmenopausal osteoporosis. IX: Summary of meta-
analyses of therapies for postmenopausal osteoporosis. Endocr Rev
23: 570-578. doi: 10.1210/er.2001- 9002 23. Howe TE, Shea B, Dawson LJ, Downie
F, Murray A, Ross C, Harbour RT, Caldwell LM, Creed G (2011) Exercise for
preventing and treating osteoporosis in postmenopausal women. Cochrane Database
Syst Rev 6: CD000333. doi: 10.1002/14651858.CD000333.pub2
24. Liang Y-Q, Qi M-C, Xu J, Xu J, Liu H-W, Dong W, Li JY, Hu M (2014) Low-
magnitude high-frequency loading, by whole-body vibration, accelerates early implant
osseointegration in ovariectomized rats. Mol Med Rep 10: 2835-2842. doi:
10.3892/mmr.2014.2597
25. Vanleene M, Shefelbine SJ (2013) Therapeutic impact of low amplitude high
frequency whole body vibrations on the osteogenesis imperfecta mouse bone. Bone
53: 507-514. doi: 10.1016/j.bone.2013.01.023
26. Shi H-F, Cheung W-H, Qin L, Leung AH-C, Leung KS (2010) Low-magnitude high-
frequency vibration treatment augments fracture healing in ovariectomy-induced
osteoporotic bone. Bone 46: 1299-1305. doi: 10.1016/j.bone.2009.11.028
27. Rauch F, Sievanen H, Boonen S, Cardinale M, Degens H, Felsenberg D, Roth J,
Schoenau E, Verschueren S, Rittweger J (2010) Reporting whole-body vibration
intervention studies: Recommendations of the International Society of Musculoskeletal
and Neuronal Interactions. J Musculoskelet Neuronal Interact 10: 193-198
28. Rauch F (2009) Vibration Therapy. Dev Med Child Neurol 51: 166-168. doi:
10.1111/j.1469-8749.2009.03418.x
29. Christiansen BA, Silva MJ (2006) The Effect of Varying Magnitudes of Whole-Body
Vibration on Several Skeletal Sites in Mice. Ann Biomed Engin 34: 1149-1156. doi:
10.1007/s10439-006-9133-5
113
30. Slatkovska L, Alibhai SMH, Beyene J, Cheung AM (2010) Effect of whole-body
vibration on BMD: a systematic review and meta-analysis. Osteoporos Int 21: 1969-
1980. doi: 10.1007/s00198-010-1228-z
31. Lau RWK, Liao LR, Yu F, Teo T, Chung RCK, Pang MYC (2011) The effects of
whole body vibration therapy on bone mineral density and leg muscle strength in older
adults: A systematic review and meta-analysis. Clin Rehabil 25: 975-988. doi:
10.1177/0269215511426644
32. Uman LS (2011) Systematic Reviews and Meta-Analyses. J Can Acad Child
Adolesc Psychiatry 20: 57-59
33. Mancini MC, Cardoso JR, Sampaio RF, Costa LCM, Cabral CMN, Costa LOP
(2014) Tutorial for writing systematic reviews for the Brazilian Journal of Physical
Therapy (BJPT). Braz J Phys Ther 18: 471-480. doi: 10.1590/bjptrbf.2014.0077
34. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA, et al
(2009) The PRISMA statement for reporting systematic reviews and meta-analyses of
studies that evaluate health care interventions: explanation and elaboration. PLoS Med
6: e1000100. doi: 10.1371/journal.pmed.1000100
35. Centre for Evidence-Based Medicine. Oxford (2012) Available from:
http://www.cebm.net
36. Maher CG, Moseley AM, Sherrington C, Elkins MR, Herbert RD (2008) A
description of the trials, reviews and practice guidelines indexed in the PEDro
database. Phys Ther 88: 1068-1077. doi: 10.2522/ptj.20080002
37. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M (2003) Reliability of
the PEDro scale for rating quality of randomized controlled trials. Phys Ther 83: 713-
721
114
38. The Centre of Evidence-Based Physiotherapy. Sydney (2012) Available from:
http://www.pedro.org.au
39. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ,
McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is
blinding necessary? Control Clin Trials 17: 1-12. doi: 10.1016/0197- 2456(95)00134-4
40. Verhagen AP, de Vet HC, de Bie RA, Kessels AG, Boers M, Bouter LM, Knipschild
PG (1998) The Delphi list: a criteria list for quality assessment of randomized clinical
trials for conducting systematic reviews developed by Delphi consensus. J Clin
Epidemiol 51: 1235-1241. doi: 10.1016/S0895-4356(98)00131-0
41. Wysocki A, Butler M, Shamliyan T, Kane RL (2011) Whole-Body Vibration Therapy
for Osteoporosis: State of the Science. Annals Intern Med 155: 680-686. doi:
10.7326/0003-4819-155-10-201111150-00006
42. Higgins JPT, Green S (2011) Cochrane's handbook for systematic reviews of
interventions version 5.1.0 [updated March 2011]. In: The Cochrane Collaboration.
Available via http:// http://handbook.cochrane.org/Accessed 18 November 2015
43. Tang BM, Eslick GD, Nowson C, Smith C, Bensoussan A (2007) Use of calcium or
calcium in combination with vitamin D supplementation to prevent fractures and bone
loss in people aged 50 years and older: a meta-analysis. Lancet 370: 657-666. doi:
10.1016/S0140-6736(07)61342-7
44. Wolff J (1986) The Law Of Bone Remodeling. Berlin: Springer. doi: 10.1007/978-
3-642-71031-5
45. Rubin C, Pope M, Fritton JC, Magnusson M, Hansson T, McLeod K (2003)
Transmissibility of 15-hertz to 35-hertz vibrations to the human hip and lumbar spine:
determining the physiologic feasibility of delivering low-level anabolic mechanical
115
stimuli to skeletal regions at greatest risk of fracture because of osteoporosis. Spine
(Phila Pa 1976) 28: 2621- 2627
46. Judex S, Rubin CT (2010) Is bone formation induced by high-frequency mechanical
signals modulated by muscle activity? J Musculoskelet Neuronal Interact 10: 3-11
47. Kiel DP, Hannan MT, Barton BA, Bouxsein ML, Sisson E, Lang T, Allaire B,
Dewkett D, Carroll D, Magaziner J, Shane E, Leary ET, Zimmerman S, Rubin CT
(2015) Low-magnitude mechanical stimulation to improve bone density in persons of
advanced age: a randomized, placebo-controlled trial. J Bone Miner Res 30: 1319-
1328. doi: 10.1002/jbmr.2448
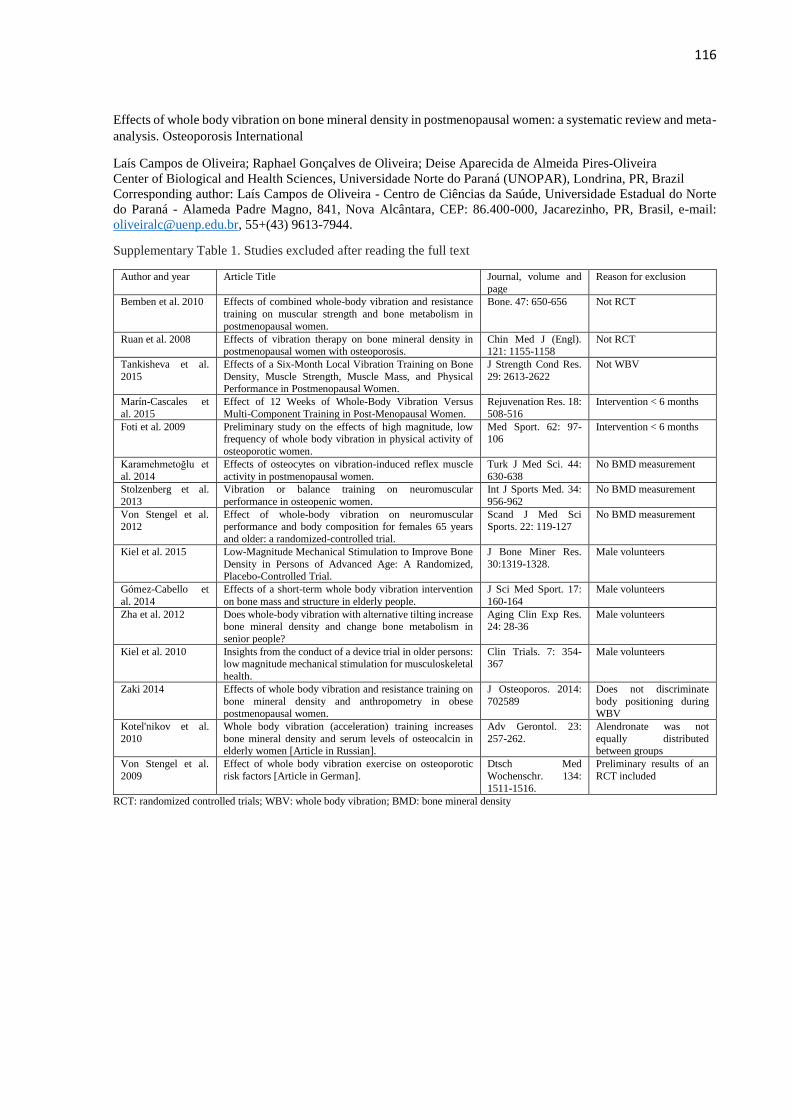
116
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Table 1. Studies excluded after reading the full text
Author and year Article Title Journal, volume and
page
Reason for exclusion
Bemben et al. 2010 Effects of combined whole-body vibration and resistance
training on muscular strength and bone metabolism in
postmenopausal women.
Bone. 47: 650-656 Not RCT
Ruan et al. 2008 Effects of vibration therapy on bone mineral density in postmenopausal women with osteoporosis.
Chin Med J (Engl). 121: 1155-1158
Not RCT
Tankisheva et al.
2015
Effects of a Six-Month Local Vibration Training on Bone
Density, Muscle Strength, Muscle Mass, and Physical Performance in Postmenopausal Women.
J Strength Cond Res.
29: 2613-2622
Not WBV
Marín-Cascales et
al. 2015
Effect of 12 Weeks of Whole-Body Vibration Versus
Multi-Component Training in Post-Menopausal Women.
Rejuvenation Res. 18:
508-516
Intervention < 6 months
Foti et al. 2009 Preliminary study on the effects of high magnitude, low frequency of whole body vibration in physical activity of
osteoporotic women.
Med Sport. 62: 97-106
Intervention < 6 months
Karamehmetoğlu et
al. 2014
Effects of osteocytes on vibration-induced reflex muscle
activity in postmenopausal women.
Turk J Med Sci. 44:
630-638
No BMD measurement
Stolzenberg et al.
2013
Vibration or balance training on neuromuscular
performance in osteopenic women.
Int J Sports Med. 34:
956-962
No BMD measurement
Von Stengel et al. 2012
Effect of whole-body vibration on neuromuscular performance and body composition for females 65 years
and older: a randomized-controlled trial.
Scand J Med Sci Sports. 22: 119-127
No BMD measurement
Kiel et al. 2015 Low-Magnitude Mechanical Stimulation to Improve Bone
Density in Persons of Advanced Age: A Randomized,
Placebo-Controlled Trial.
J Bone Miner Res.
30:1319-1328.
Male volunteers
Gómez-Cabello et
al. 2014
Effects of a short-term whole body vibration intervention
on bone mass and structure in elderly people.
J Sci Med Sport. 17:
160-164
Male volunteers
Zha et al. 2012 Does whole-body vibration with alternative tilting increase bone mineral density and change bone metabolism in
senior people?
Aging Clin Exp Res. 24: 28-36
Male volunteers
Kiel et al. 2010 Insights from the conduct of a device trial in older persons: low magnitude mechanical stimulation for musculoskeletal
health.
Clin Trials. 7: 354-367
Male volunteers
Zaki 2014 Effects of whole body vibration and resistance training on
bone mineral density and anthropometry in obese postmenopausal women.
J Osteoporos. 2014:
702589
Does not discriminate
body positioning during WBV
Kotel'nikov et al.
2010
Whole body vibration (acceleration) training increases
bone mineral density and serum levels of osteocalcin in elderly women [Article in Russian].
Adv Gerontol. 23:
257-262.
Alendronate was not
equally distributed between groups
Von Stengel et al.
2009
Effect of whole body vibration exercise on osteoporotic
risk factors [Article in German].
Dtsch Med
Wochenschr. 134:
1511-1516.
Preliminary results of an
RCT included
RCT: randomized controlled trials; WBV: whole body vibration; BMD: bone mineral density
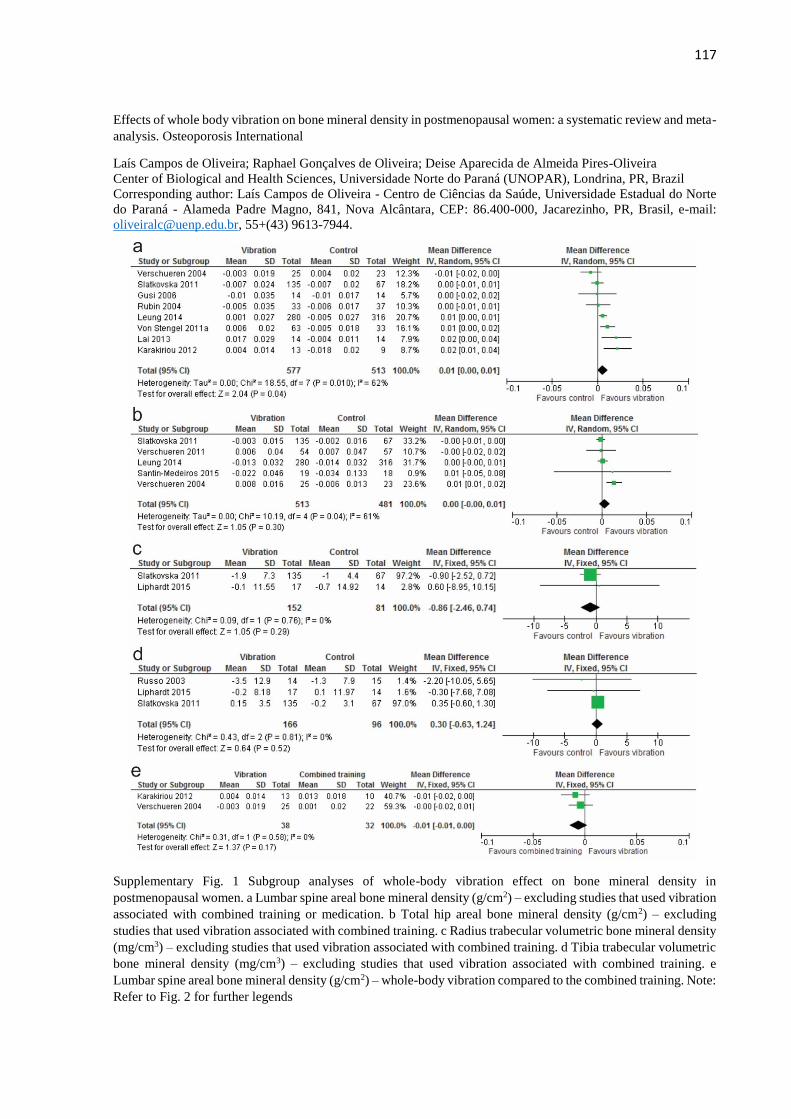
117
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 1 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women. a Lumbar spine areal bone mineral density (g/cm2) – excluding studies that used vibration
associated with combined training or medication. b Total hip areal bone mineral density (g/cm2) – excluding
studies that used vibration associated with combined training. c Radius trabecular volumetric bone mineral density
(mg/cm3) – excluding studies that used vibration associated with combined training. d Tibia trabecular volumetric
bone mineral density (mg/cm3) – excluding studies that used vibration associated with combined training. e
Lumbar spine areal bone mineral density (g/cm2) – whole-body vibration compared to the combined training. Note:
Refer to Fig. 2 for further legends
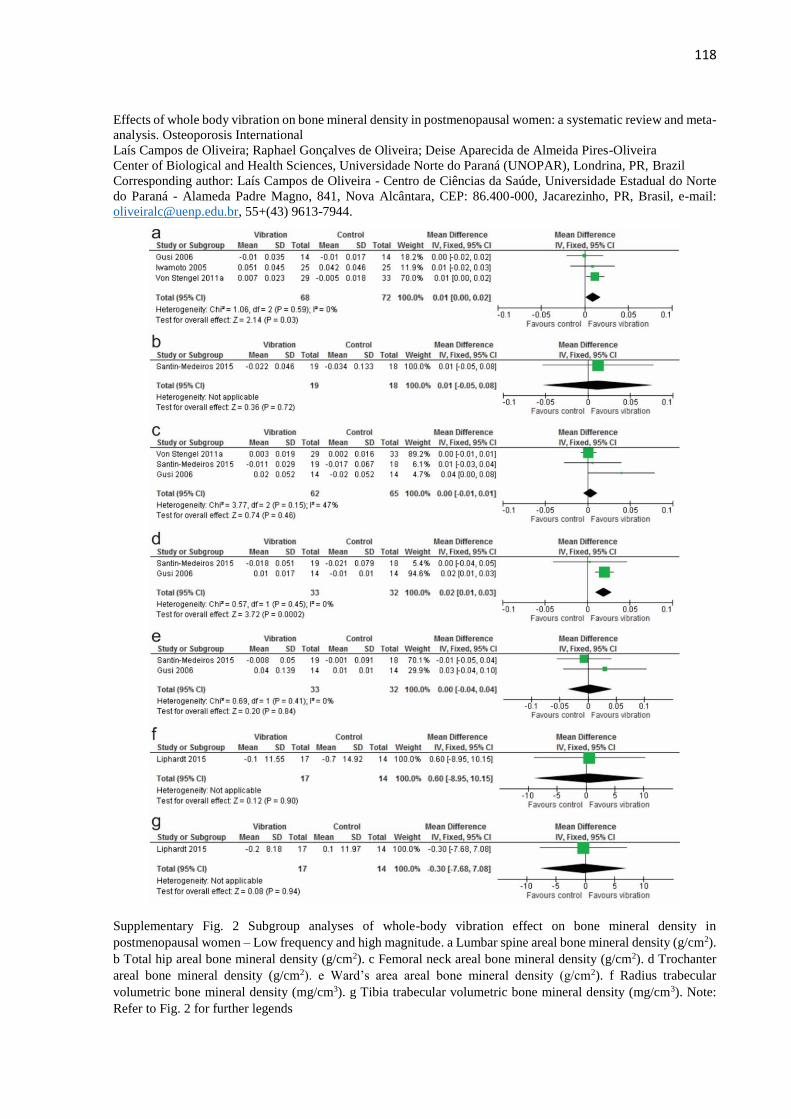
118
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 2 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Low frequency and high magnitude. a Lumbar spine areal bone mineral density (g/cm2).
b Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2). d Trochanter
areal bone mineral density (g/cm2). e Ward’s area areal bone mineral density (g/cm2). f Radius trabecular
volumetric bone mineral density (mg/cm3). g Tibia trabecular volumetric bone mineral density (mg/cm3). Note:
Refer to Fig. 2 for further legends
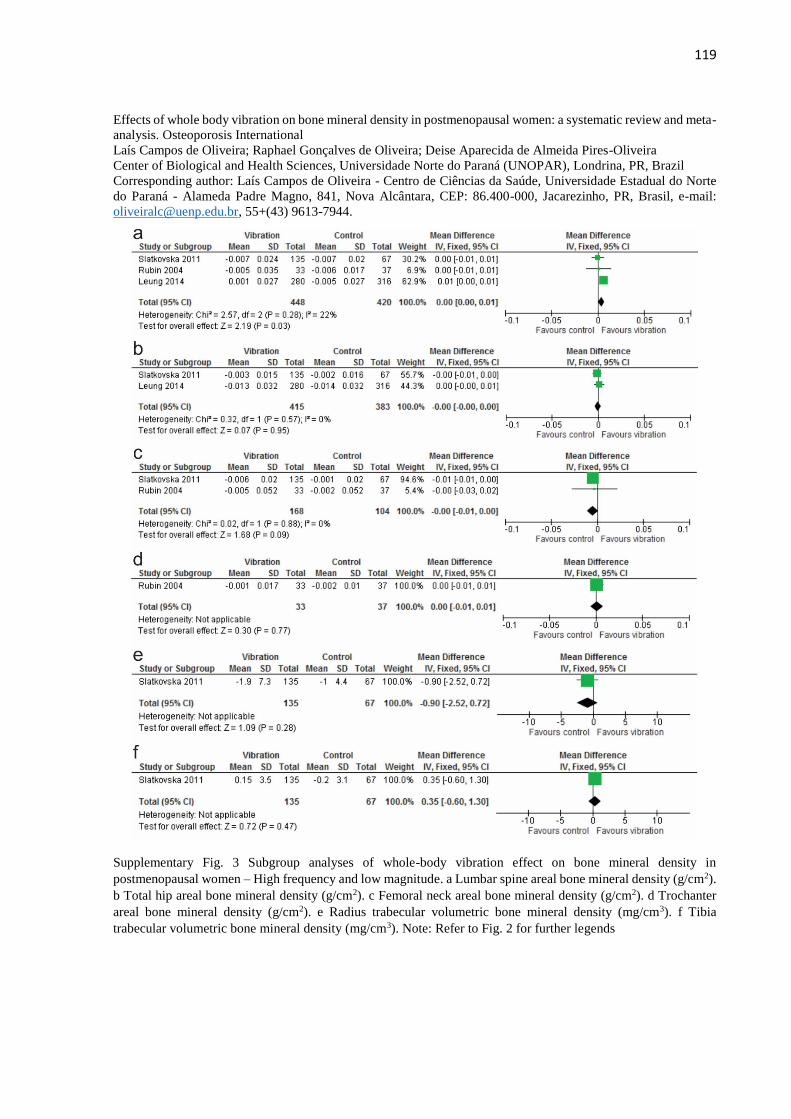
119
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 3 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – High frequency and low magnitude. a Lumbar spine areal bone mineral density (g/cm2).
b Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2). d Trochanter
areal bone mineral density (g/cm2). e Radius trabecular volumetric bone mineral density (mg/cm3). f Tibia
trabecular volumetric bone mineral density (mg/cm3). Note: Refer to Fig. 2 for further legends
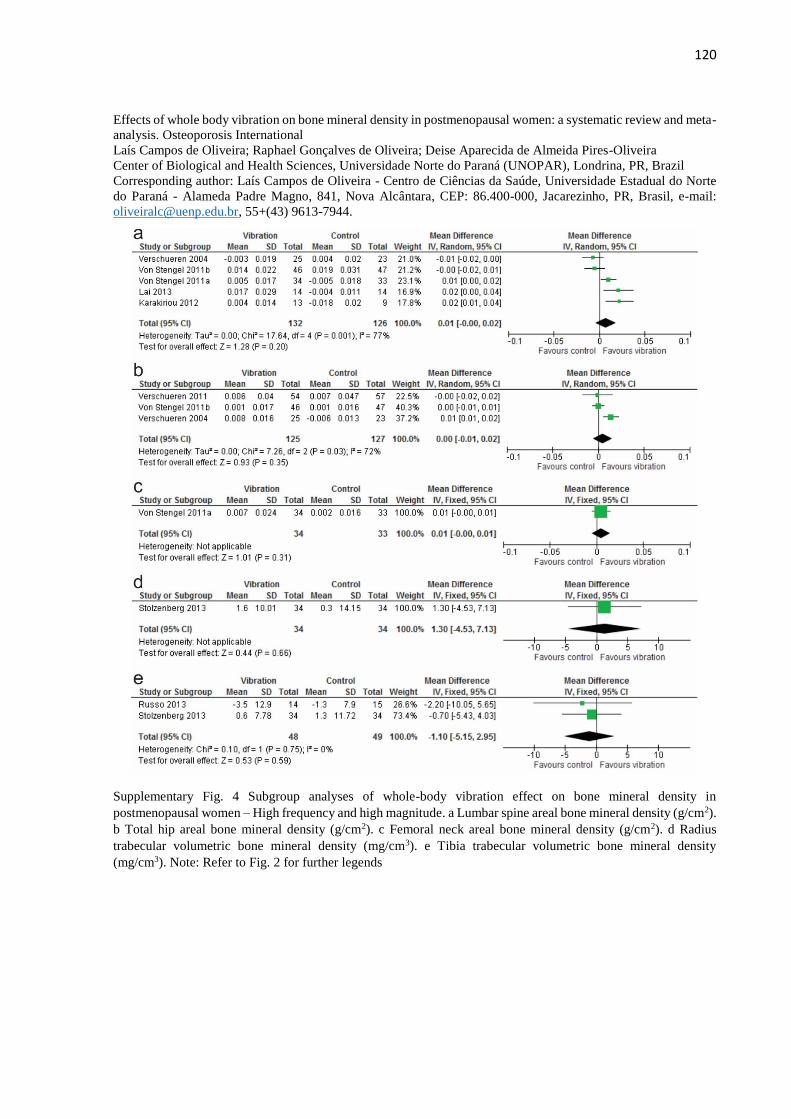
120
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 4 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – High frequency and high magnitude. a Lumbar spine areal bone mineral density (g/cm2).
b Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2). d Radius
trabecular volumetric bone mineral density (mg/cm3). e Tibia trabecular volumetric bone mineral density
(mg/cm3). Note: Refer to Fig. 2 for further legends
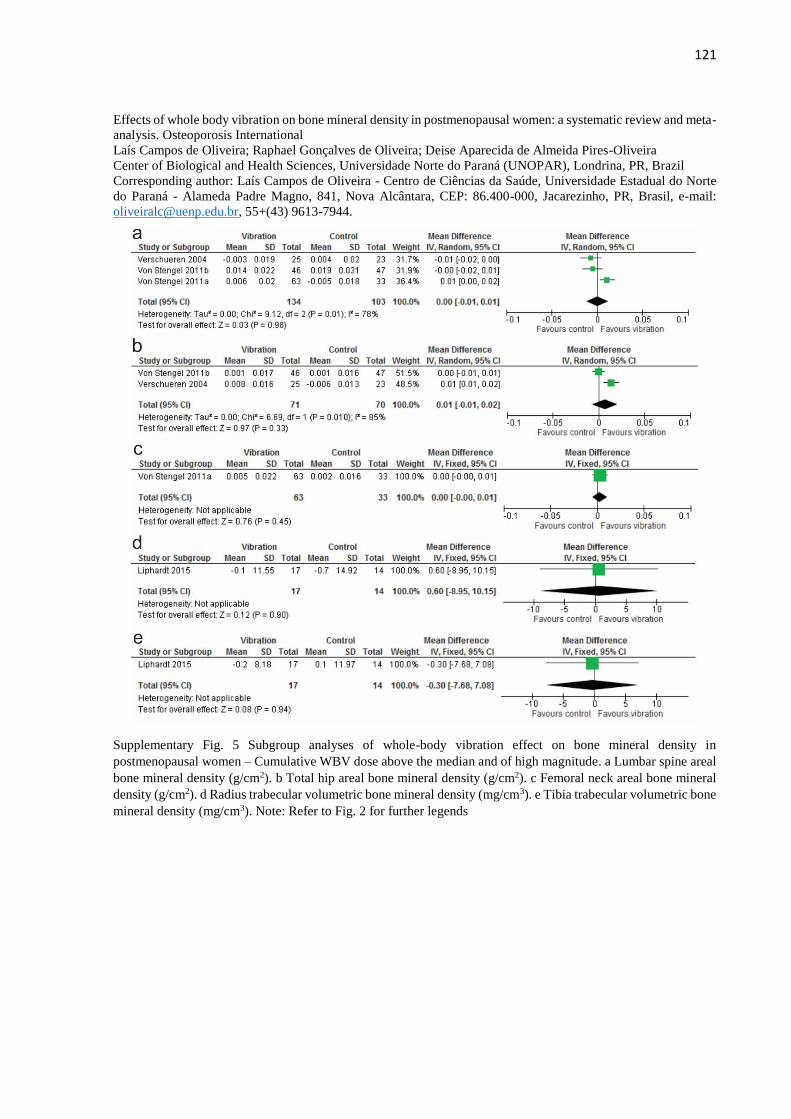
121
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 5 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Cumulative WBV dose above the median and of high magnitude. a Lumbar spine areal
bone mineral density (g/cm2). b Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral
density (g/cm2). d Radius trabecular volumetric bone mineral density (mg/cm3). e Tibia trabecular volumetric bone
mineral density (mg/cm3). Note: Refer to Fig. 2 for further legends
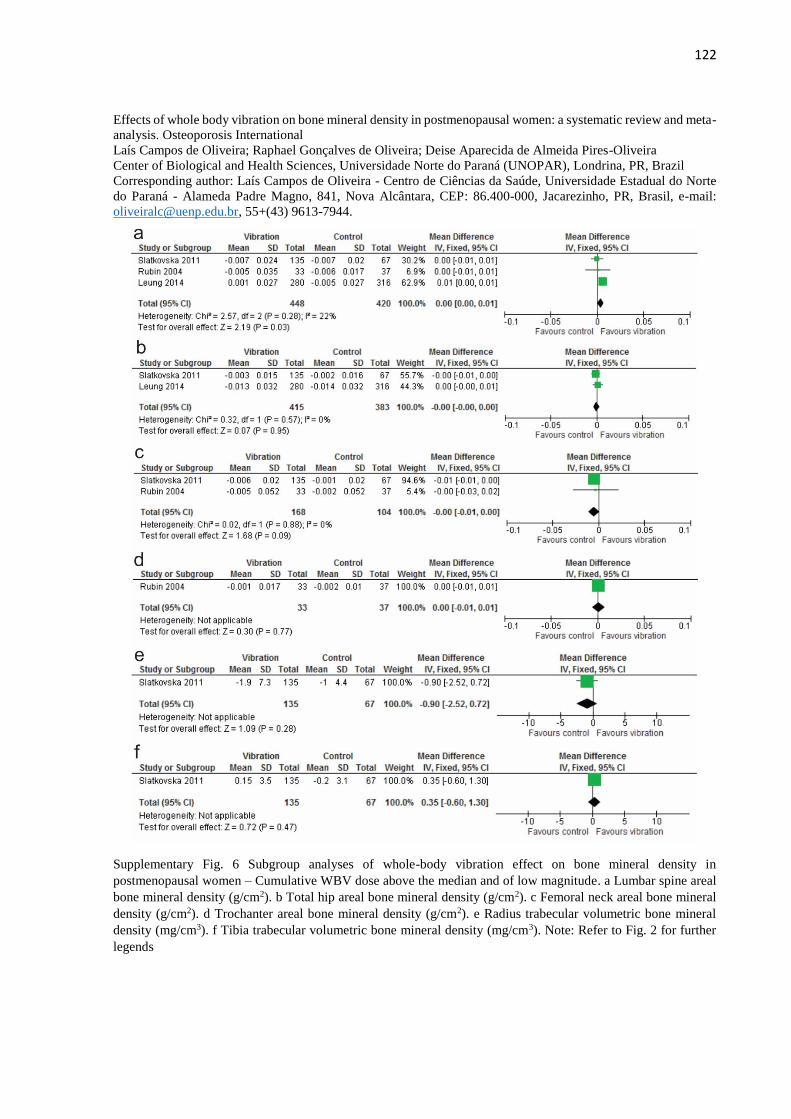
122
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 6 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Cumulative WBV dose above the median and of low magnitude. a Lumbar spine areal
bone mineral density (g/cm2). b Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral
density (g/cm2). d Trochanter areal bone mineral density (g/cm2). e Radius trabecular volumetric bone mineral
density (mg/cm3). f Tibia trabecular volumetric bone mineral density (mg/cm3). Note: Refer to Fig. 2 for further
legends
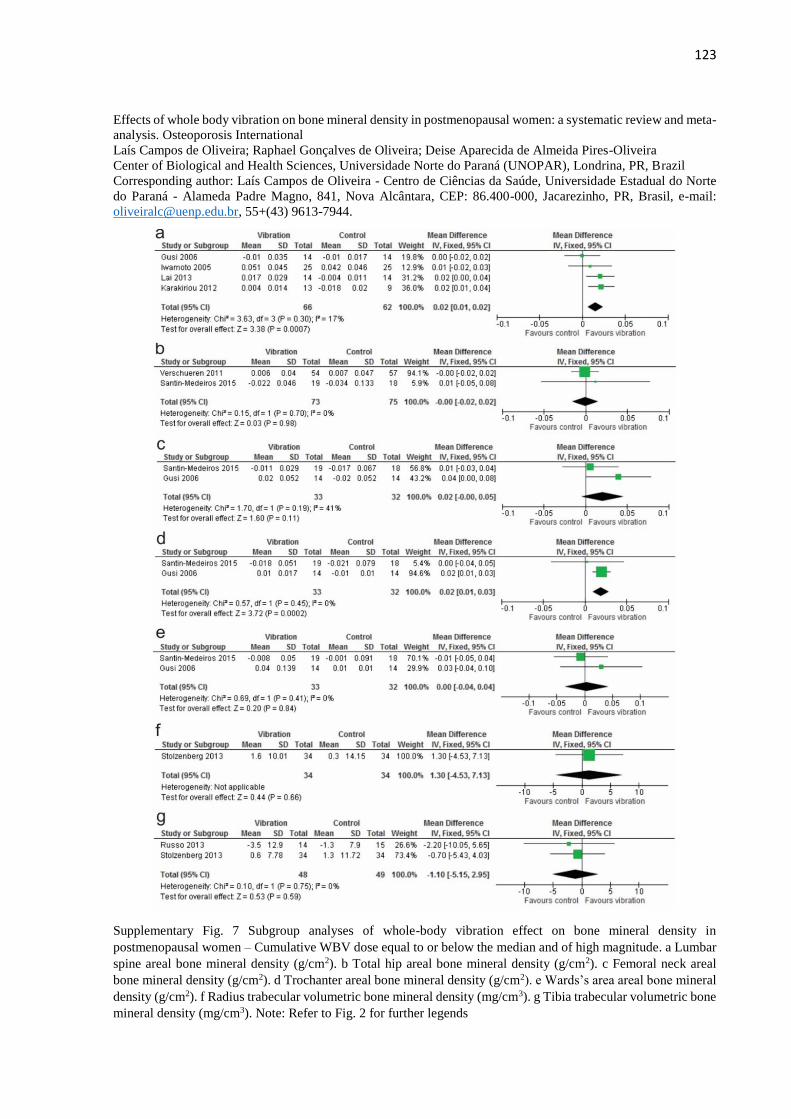
123
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 7 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Cumulative WBV dose equal to or below the median and of high magnitude. a Lumbar
spine areal bone mineral density (g/cm2). b Total hip areal bone mineral density (g/cm2). c Femoral neck areal
bone mineral density (g/cm2). d Trochanter areal bone mineral density (g/cm2). e Wards’s area areal bone mineral
density (g/cm2). f Radius trabecular volumetric bone mineral density (mg/cm3). g Tibia trabecular volumetric bone
mineral density (mg/cm3). Note: Refer to Fig. 2 for further legends
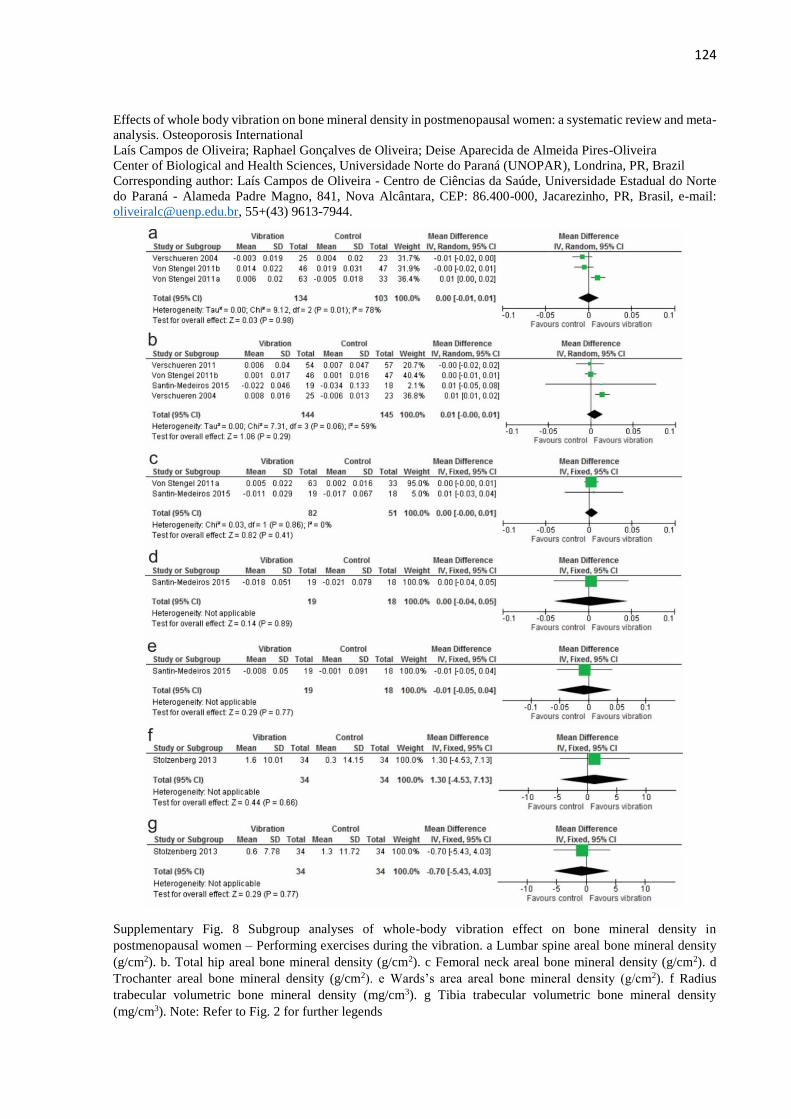
124
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 8 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Performing exercises during the vibration. a Lumbar spine areal bone mineral density
(g/cm2). b. Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2). d
Trochanter areal bone mineral density (g/cm2). e Wards’s area areal bone mineral density (g/cm2). f Radius
trabecular volumetric bone mineral density (mg/cm3). g Tibia trabecular volumetric bone mineral density
(mg/cm3). Note: Refer to Fig. 2 for further legends
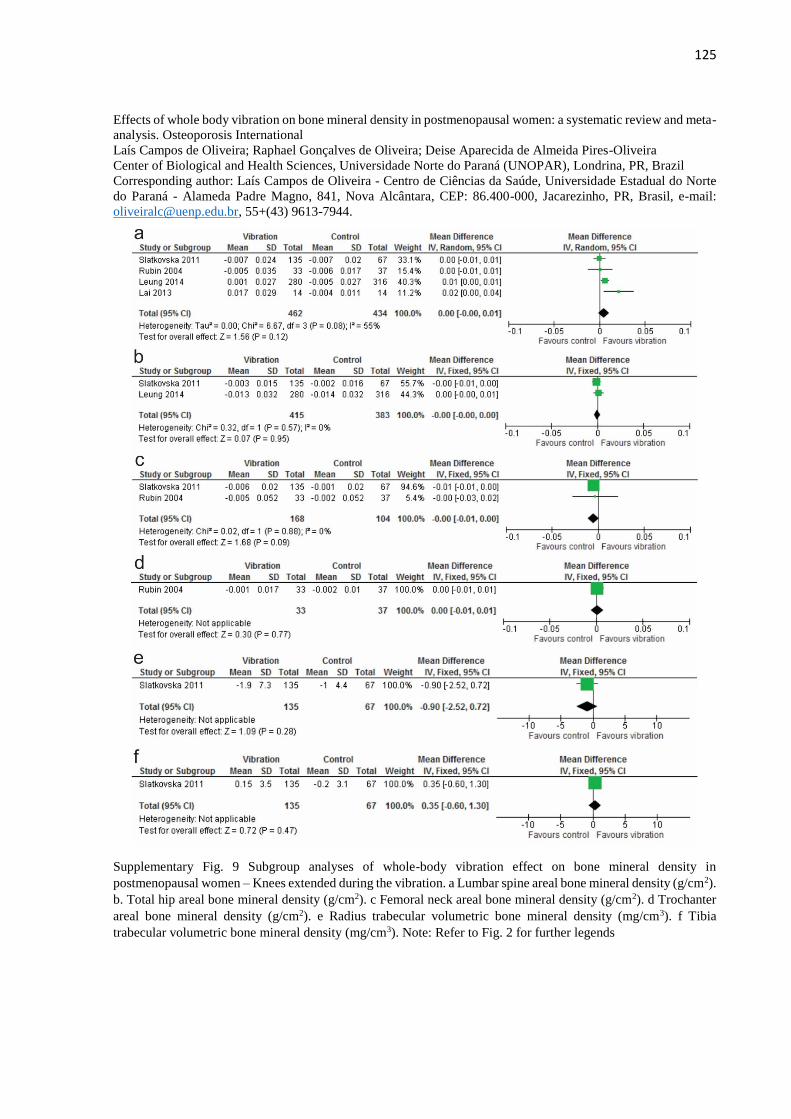
125
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 9 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Knees extended during the vibration. a Lumbar spine areal bone mineral density (g/cm2).
b. Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2). d Trochanter
areal bone mineral density (g/cm2). e Radius trabecular volumetric bone mineral density (mg/cm3). f Tibia
trabecular volumetric bone mineral density (mg/cm3). Note: Refer to Fig. 2 for further legends
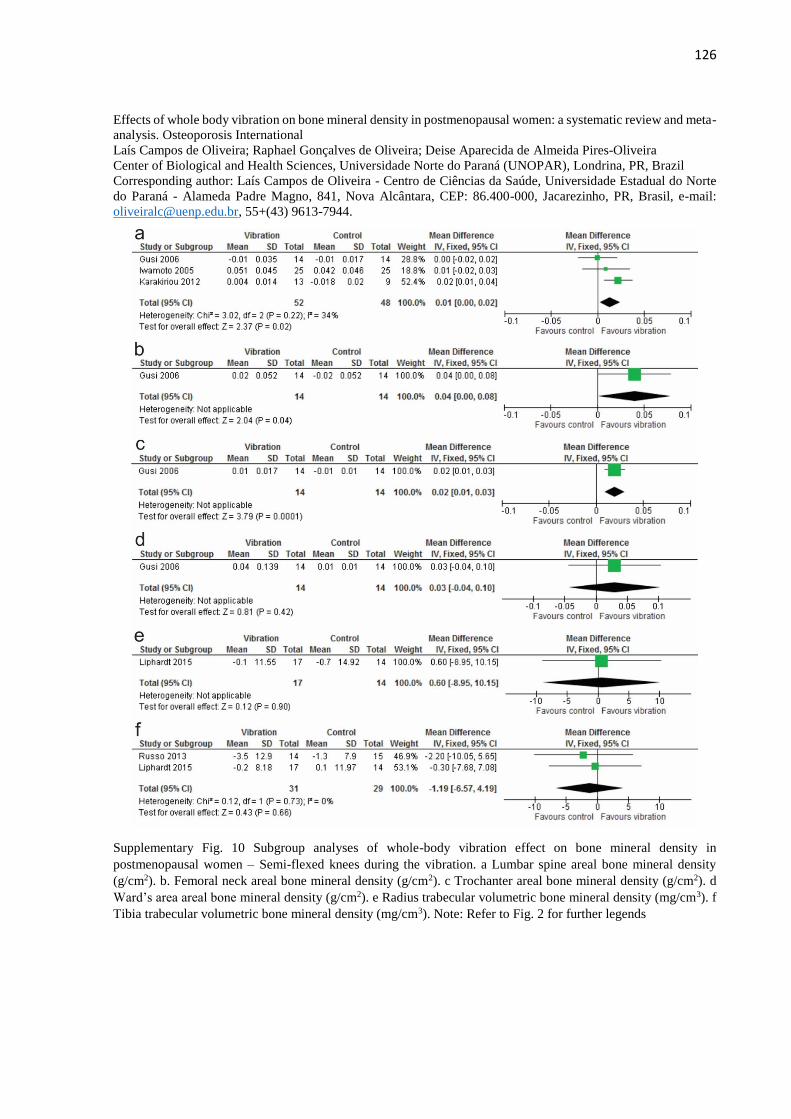
126
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 10 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Semi-flexed knees during the vibration. a Lumbar spine areal bone mineral density
(g/cm2). b. Femoral neck areal bone mineral density (g/cm2). c Trochanter areal bone mineral density (g/cm2). d
Ward’s area areal bone mineral density (g/cm2). e Radius trabecular volumetric bone mineral density (mg/cm3). f
Tibia trabecular volumetric bone mineral density (mg/cm3). Note: Refer to Fig. 2 for further legends
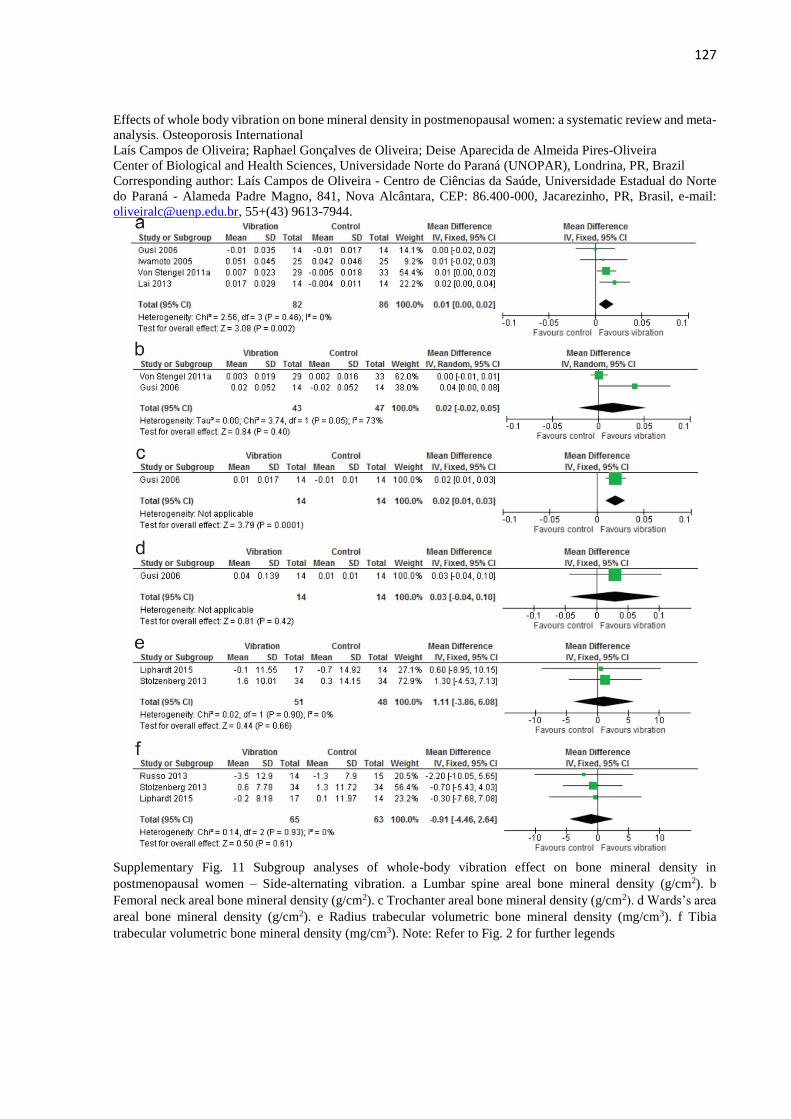
127
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 11 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Side-alternating vibration. a Lumbar spine areal bone mineral density (g/cm2). b
Femoral neck areal bone mineral density (g/cm2). c Trochanter areal bone mineral density (g/cm2). d Wards’s area
areal bone mineral density (g/cm2). e Radius trabecular volumetric bone mineral density (mg/cm3). f Tibia
trabecular volumetric bone mineral density (mg/cm3). Note: Refer to Fig. 2 for further legends
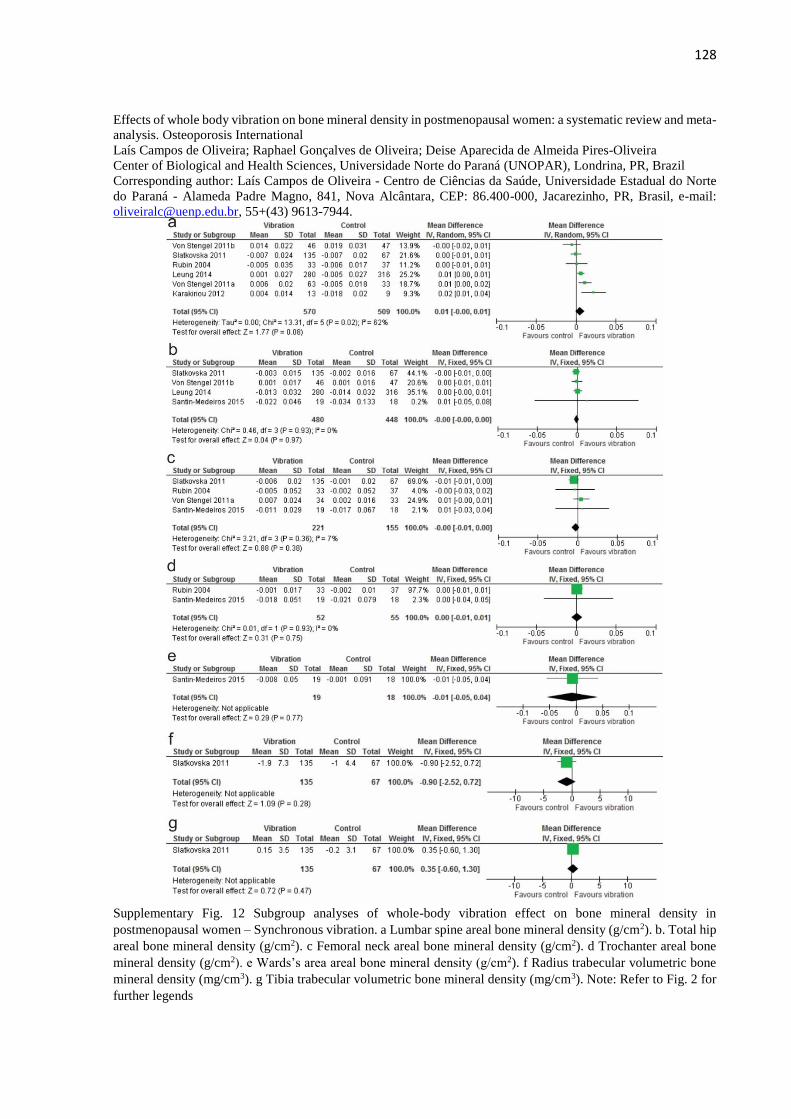
128
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 12 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Synchronous vibration. a Lumbar spine areal bone mineral density (g/cm2). b. Total hip
areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2). d Trochanter areal bone
mineral density (g/cm2). e Wards’s area areal bone mineral density (g/cm2). f Radius trabecular volumetric bone
mineral density (mg/cm3). g Tibia trabecular volumetric bone mineral density (mg/cm3). Note: Refer to Fig. 2 for
further legends
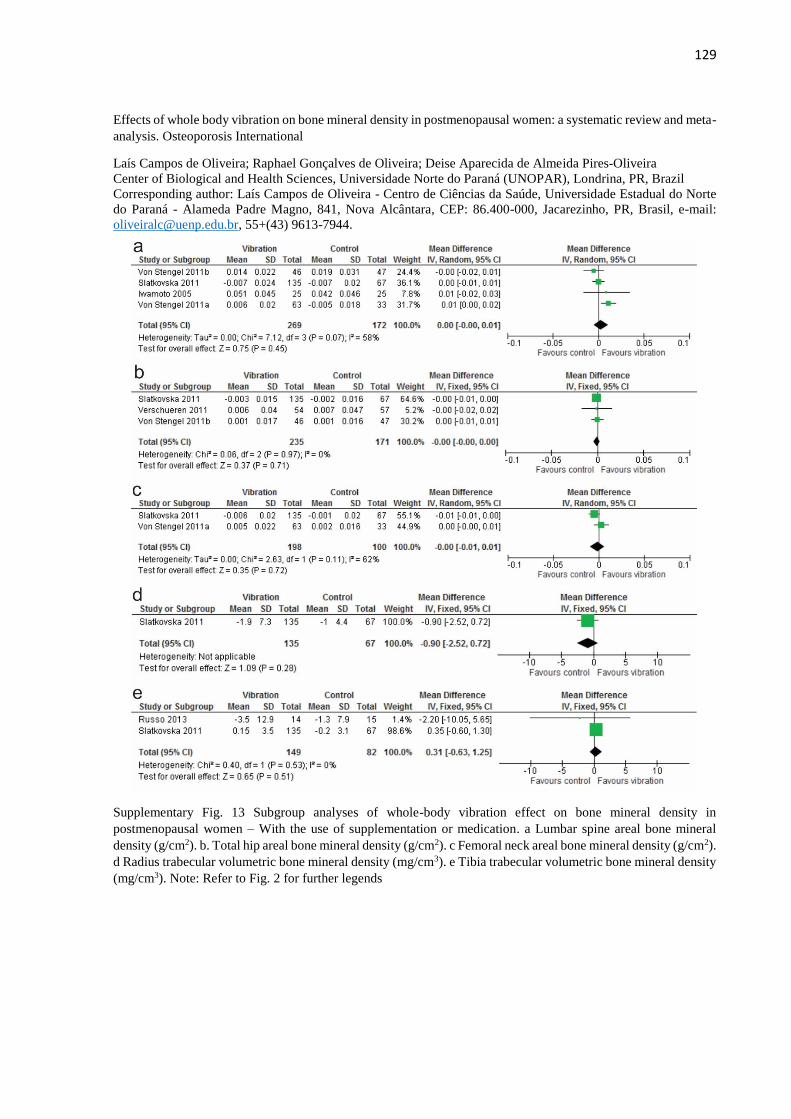
129
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 13 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – With the use of supplementation or medication. a Lumbar spine areal bone mineral
density (g/cm2). b. Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2).
d Radius trabecular volumetric bone mineral density (mg/cm3). e Tibia trabecular volumetric bone mineral density
(mg/cm3). Note: Refer to Fig. 2 for further legends
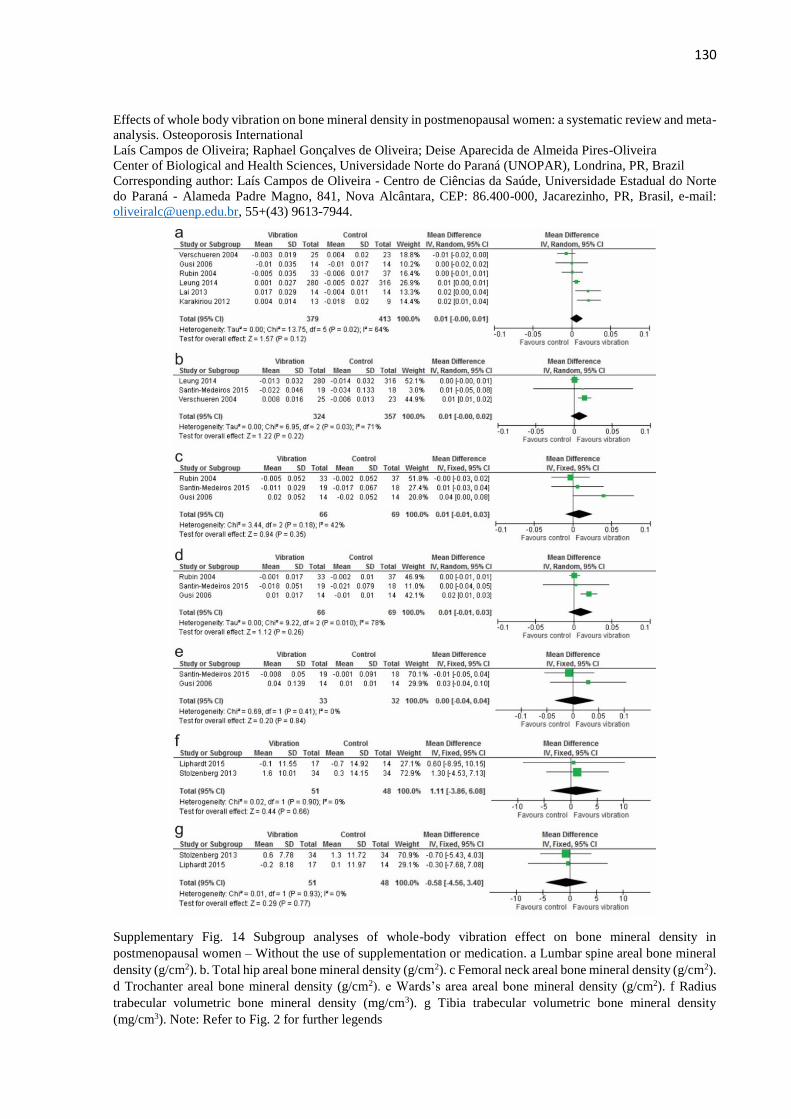
130
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 14 Subgroup analyses of whole-body vibration effect on bone mineral density in
postmenopausal women – Without the use of supplementation or medication. a Lumbar spine areal bone mineral
density (g/cm2). b. Total hip areal bone mineral density (g/cm2). c Femoral neck areal bone mineral density (g/cm2).
d Trochanter areal bone mineral density (g/cm2). e Wards’s area areal bone mineral density (g/cm2). f Radius
trabecular volumetric bone mineral density (mg/cm3). g Tibia trabecular volumetric bone mineral density
(mg/cm3). Note: Refer to Fig. 2 for further legends
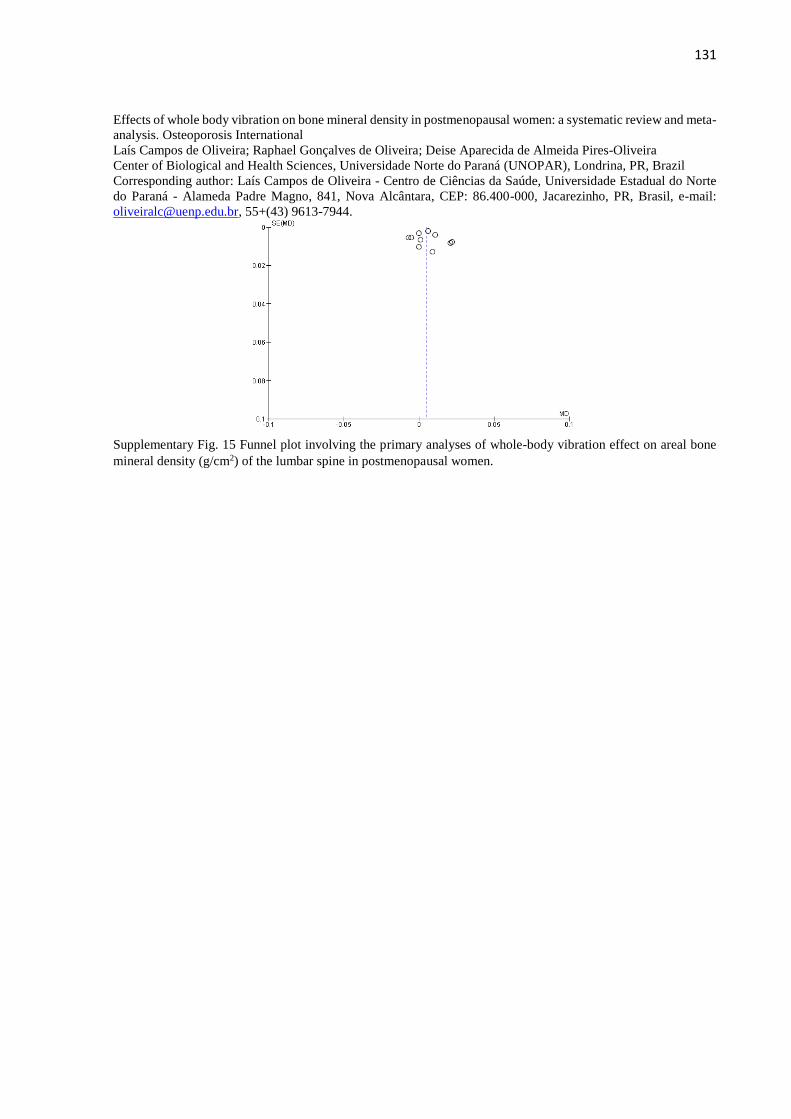
131
Effects of whole body vibration on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Center of Biological and Health Sciences, Universidade Norte do Paraná (UNOPAR), Londrina, PR, Brazil
Corresponding author: Laís Campos de Oliveira - Centro de Ciências da Saúde, Universidade Estadual do Norte
do Paraná - Alameda Padre Magno, 841, Nova Alcântara, CEP: 86.400-000, Jacarezinho, PR, Brasil, e-mail:
[email protected], 55+(43) 9613-7944.
Supplementary Fig. 15 Funnel plot involving the primary analyses of whole-body vibration effect on areal bone
mineral density (g/cm2) of the lumbar spine in postmenopausal women.
132
6.2 ARTIGO 2: ESTUDO ORIGINAL
Artigo submetido ao periódico Osteoporosis International (ISSN: 0937-941X).
Fator de Impacto JCR de 2016: 3,591.
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in
Postmenopausal Women: A Randomized and Controlled Clinical Trial
Laís Campos de Oliveira, PhD1,2 • Raphael Gonçalves de Oliveira, PhD2 • Deise Aparecida de
Almeida Pires-Oliveira, PhD1
1Centro de Pesquisa em Ciências da Saúde, Universidade Norte do Paraná (UNOPAR),
Londrina, PR, Brazil. 2Centro de Ciências da Saúde, Universidade Estadual do Norte do Paraná
(UENP), Jacarezinho, PR, Brazil.
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira, Centro de Pesquisa em
Ciências da Saúde, Universidade Norte do Paraná (UNOPAR), Rua Marselha, 591, Jardim Piza,
CEP: 86.041-140, Londrina, PR, Brazil. Email address: [email protected];
Telephone/Fax: +55 43 3371-7990.
ORCID: 0000-0002-9853-7337 (Laís Campos de Oliveira); 0000-0003-0904-9305 (Raphael
Gonçalves de Oliveira); 0000-0002-5765-1897 (Deise Aparecida de Almeida Pires-Oliveira)
The authors further declare that there are no conflicts of interest and no funding was received.
The authors certify that they have no affiliations with or financial involvement in any
organization or entity with a direct financial interest in the subject matter or materials discussed
in the article.
133
Abstract
Introduction: Decreased bone mineral density (BMD) is a common condition in
postmenopausal women that can be managed with impact activities such as whole body
vibration (WBV) therapy or exercise. Our objective is to compare the effects of WBV and the
Pilates method on BMD in postmenopausal women.
Methods: In this study, 51 postmenopausal women were randomized into three groups:
vibration (n = 17), Pilates (n = 17) and control (n = 17). Outcomes were the area of BMD
(lumbar spine, femoral neck, total hip, trochanter, intertrochanter, and ward's area) assessed by
DXA at baseline and follow-up. The interventions were performed three times a week for six
months, totaling 78 sessions. The analysis was performed with intention to treat and covariance
analyses adjusted for baseline outcomes.
Results: After six months, 96.1% of the participants completed the follow-up. The analyses
demonstrated significant mean difference between-group in favor of the interventions: vibration
vs. control, for the BMD of the lumbar spine (0.014 g/cm2 [95 % CI, 0.006 to 0.022] p=0.018,
d=1.21) and trochanter (0.018 g/cm2 [95 % CI, 0.006 to 0.030] p=0.012, d=1.03); and Pilates
vs. control, for the BMD of the lumbar spine (0.016 g/cm2 [95 % CI, 0.007 to 0.025] p=0.008,
d=1.15) and trochanter (0.020 g/cm2 [95 % CI, 0.010 to 0.031] p=0.005, d=1.28).
Conclusion: In postmenopausal women, three weekly sessions of WBV or Pilates administered
for six months provided an equal effect on BMD.
Keywords: osteoporosis, osteopenia, rehabilitation, exercise therapy, aging
Mini Abstract
Whole body vibration and Pilates had similar effects on bone mineral density in
postmenopausal women and were superior to no form of intervention for the lumbar spine and
trochanter regions but not for other bone mineral density measures.
134
INTRODUCTION
The term postmenopausal refers to the stage of a woman's life that begins after the
cessation of menstrual cycles [1]. This stage is marked by alterations in the body that occur
principally due to hormonal changes such as a reduction in estrogen levels, causing several
factors that are detrimental to health [2]. One of these factors relates to decreased bone mineral
density (BMD), which can lead to osteoporosis and substantially increase the risk of fracture
[3]. Osteoporosis is more common than diabetes, heart attack, and stroke in older women [4].
Approximately one-third of postmenopausal women present osteoporosis and of these, at least
40% will suffer one or more fractures in their remaining lifetime, which can lead to morbidity
and mortality [5].
In order to mitigate these factors, different forms of treatment aimed at increasing BMD
have been investigated in postmenopausal women [6-8]. The use of drugs is highlighted as a
possible treatment method, however the side effects limit their use in the long-term or when the
individual has a pre-disposition for certain types of diseases [9]. Thus, the use of alternative
means to increase bone metabolism has been investigated [10, 7, 8].
One of the forms of intervention that has demonstrated few adverse events and is
considered relatively safe is therapy involving whole body vibration (WBV) [11]. This
technique uses an sinusoidal-shaped oscillations platform that offers mechanical stimulation to
the human skeleton according to pre-established parameters [12, 13]. Different intensities
(frequency and magnitude), types of vibration, and body positioning during WBV have been
used without consensus regarding the best parameters to increase BMD [14]. A recent
systematic review and meta-analysis involving randomized controlled trials (RCTs) showed
that low frequency, high magnitude, side-alternating vibration and body positioning with semi-
flexed knees may be the best parameters for increasing BMD in postmenopausal women,
principally in the lumbar spine and trochanter regions. However, the low number of RCTs
135
involved in the meta-analysis and the poor methodological quality of some studies limit
extrapolations, demonstrating the need for further studies [8].
In addition to WBV, another alternative to using medication is the practice of exercises
involving muscular strengthening. A systematic review and meta-analysis of RCTs
demonstrated that progressive resistance exercises with a low number of repetitions and greater
overload were efficient for increasing lumbar spine and femoral neck BMD in postmenopausal
women, while no significant results were observed for resistance training involving low
overload and a high number of repetitions. However, at the time the meta-analysis was
performed, no study had investigated the effects of the Pilates method on the BMD of
postmenopausal women [7]. Pilates makes use of progressive resistance exercises with few
repetitions and higher overload [15] and has become increasingly popular [16]. To date, only
one RCT has verified the effects of Pilates on the BMD of postmenopausal women, identifying
significant improvements for the lumbar spine, however other bone regions were not
investigated [17].
With this problem in mind the objective of the present study was to verify the effects of
WBV and the Pilates method on the BMD of postmenopausal women. As a hypothesis, we
assumed that the parameters chosen for WBV and the intervention protocol selected for Pilates
practice would be able to provide an increase in BMD in this population.
METHODS
This is a randomized controlled trial (registered at www.clinicaltrials.gov on May 7,
2016: NCT02769143), which followed the CONSORT recommendations (Supplementary
Table 1), and had a duration of six months, involving 51 women within the postmenopausal
period (having experienced menopause for at least one year), subdivided into three groups of
equal size. All participants were apparently healthy, aged between 40 and 70 years, living in
136
the city of Jacarezinho, Paraná state, Brazil. The present study followed the ethical norms
established in the Declaration of Helsinki (1975, revised in 1983) and was approved by the
Human Research Ethics Committee of the Northern University of Paraná, Brazil (opinion
1,032,182). Informed consent was obtained from all individual participants included in the
study.
Recruitment and Participants
Participants were randomly recruited in May 2016, through posters in public places,
advertisements in printed newspapers, radios, internet news sites, and newsletters intended for
medical clinics and health facilities, all with local coverage, until the target sample size was
reached (51 participants). The sample calculation was performed in the statistical program
Bioestat 5.3 (Instituto Mamiraua, Amazonas, Brazil), taking into account the values for the
lumbar spine BMD area measured by Dual-energy X-ray Absorptiometry (DXA) in a previous
study [18]. In this case, the weighted mean difference and its respective standard deviation,
between the vibration group (0.017 ± 0.029) and the control group (-0.004 ± 0.011) was used,
in absolute alteration (g/cm2) between pre- and post-intervention, with a test power of 80% and
alpha value of 0.05, which generated the need for 17 participants in each group.
The inclusion criteria were: a) post-menopausal, clinically confirmed, for at least 12
months; b) not practicing physical exercise for at least six months; c) agreement not to practice
another type of exercise during the research; d) ability to perform activities of daily living
without assistance [19, 20]; e) presentation of a medical certificate indicating fitness for
exercise; f) body mass index (BMI) below 30.0 Kg/m2; and g) score ≥ 19 in the Mini-Mental
State Examination [21].
The exclusion criteria were: a) musculoskeletal dysfunctions in the spine or lower limbs
in the previous six months; b) fracture in the vertebral column or in the lower limbs after 40
137
years of age; c) prosthesis in the lower limbs or implants in the vertebral column; d) secondary
causes of loss of bone mass; e) other metabolic bone diseases or diseases that affect bone
metabolism; f) a history of cancer in the previous five years; g) vascular alterations, epilepsy,
or seizures; h) arrhythmia; i) the use of a pacemaker; j) eye disease affecting the retina; k)
cardiorespiratory diseases; l) diseases of the neuromuscular system; m) labyrinthitis or vertigo;
n) hospitalization in the previous six months for surgical reasons; o) thyroid alteration; p)
smoking; q) frequent use of alcoholic beverages; r) use of supplements based on calcium or
vitamin D, isoflavone, medication to increase bone mineral density or to increase muscle mass
in the previous 12 months.
All participants included in the present study were instructed to maintain their usual
routines, as well as their daily physical activities (e.g., sweeping the house or washing dishes)
and nutritional habits. They were also instructed not to use any medication or supplement that
could influence muscle mass or BMD (including soy and its derivatives).
Evaluation of Bone Mineral Density
Soon after the end of the recruitment period the participants were submitted to bone
mass evaluation through DXA equipment (HologicQDR 1000 Plus, Waltham, MA., USA).
BMD was expressed in absolute values (grams of bone mineral content per square centimeter
[g/cm2]). For the initial classification of participants the criteria of the World Health
Organization were used [22], in T-score values (difference in the standard deviation of the bone
mass with reference to the average of young adults): no alteration (T > -1), osteopenia (T
between -1 and -2.5), and osteoporosis (T < -2.5). Six different bone regions were considered:
lumbar spine (L1-L4), femoral neck, total hip, trochanter, intertrochanter and ward's area. The
procedure was performed by an independent evaluator, not directly involved in the research
project, with experience in DXA assessment of BMD and blinded to the allocation of
138
participants in each group. Calibration of the device was performed daily prior to the start of
the assessments to ensure the same BMD measurement conditions for all participants. Variation
coefficients for this device were 1.3% for the lumbar spine, 1.4% for the femoral neck, and
1.2% for the total hip in precision studies [23]. The same equipment, evaluator, and procedures
used at baseline were repeated at follow-up (after six months).
Randomization
After the BMD assessment, the participants were submitted to the randomization
process (random allocation of participants into one of the three groups), performed by a blind
researcher who was not part of the study team. The random numbers were generated by specific
software (randomization.com), which distributed the participants into three groups: Vibration
Group (VG); Pilates Group (PG), and Control Group (CG), with 17 participants in each. The
same researcher who carried out the randomization process sealed the dark envelopes
containing the group of each participant in and delivered them to the principal investigator who
remained blind regarding the allocation of the participants in each group. The blinded
participants then individually received the envelope containing their name and the name of their
group.
Intervention
Interventions occurred three times a week on non-consecutive days for six months
beginning in June 2016. The experimental groups (VG and PG) were supervised by two
physiotherapists with professional experience in WBV therapy and Pilates. As the intervention
was with exercise, it was not possible to blind the participants and the physiotherapists
responsible for the interventions in relation to the therapy.
139
Vibration Group
The VG was exposed to WBV for five minutes on a sinusoidal-shaped oscillations
platform, side-alternating vibration (Supplementary Fig. 1) (Arktus, Cascavel, PR, Brazil),
which oscillates through an anteroposterior axis, causing the right and left sides to alternate
horizontally. A frequency of 20 Hz (1 Hz = 1 oscillation/second) was used and a peak-to-peak
displacement of 4 mm (with reference to the second toe), resulting in a magnitude of 31.5 m/s2
or 3.2 g (gravity: 1 g = 9.8 m/s2). Participants were instructed to stand on the platform oscillation
plate with the knees semi-flexed at 30 degrees, and bare feet spaced at a distance of 50 cm,
keeping the torso upright and holding the platform support with both hands. No accessories
(such as an EthyleneVinyl Acetate [EVA] plate) were placed on the platform's oscillating plate
to cushion the impacts. All the parameters used in the equipment and the positioning of the
participants were maintained throughout the six months of intervention. A slippage test ensured
that the feet of the participants always remained in contact with the oscillating plate during
WBV [13].
The intensity of WBV is mainly defined by the frequency and magnitude parameters,
which are considered low when ≤ 20 Hz and < 1 g respectively. In this study, low frequency
and high magnitude were used. These parameters, type of vibration, time of exposure, and body
positioning of the participants were chosen based on a recent systematic review and meta-
analysis that demonstrated that they are potentially the most effective for increasing BMD in
postmenopausal women [8].
Pilates Group
The first session of the PG was used to familiarize participants with Pilates, providing
an explanation of the correct execution of each movement and a better understanding of the
principles of the method. The following equipment was used to perform the exercises: Cadillac,
140
Reformer, Ladder Barrel, Wall Unit, Chair, Spine Corrector and Small Barrel (Supplementary
Fig. 2) (ISP, Cascavel, PR, Brazil). Twenty-one strengthening and stretching exercises were
selected for the main body segments: a) lower limbs b) flexors, extensors, and lateral flexors of
the trunk; and c) upper limbs. Two exercise protocols were applied during the six months of
intervention, each performed for three months (Supplementary Table 2). The duration of each
session was 60 minutes. The intervention protocols were developed specifically for this study,
aiming to improve the BMD of the evaluated regions.
All exercises were performed in a series of ten repetitions, with a one-minute rest
interval between exercises. The intensity of the work overload in Pilates is principally
determined by the spring, which was modified according to the evolution of the force of the
participants (changing the positioning of the springs in the equipment, or changing the spring
to another one of greater resistance) [24], always maintaining the number of repetitions and
series. To determine the level of effort of the participants and consequent evolution of the
overload, a verbal description according to the Borg CR10 scale was used [25]: light load (Borg
≤ 2), moderate load (Borg > 2 and < 5), heavy load ≥ 5 and < 7), and close to maximum load
(Borg ≥ 7). The level of perception of effort maintained during the sessions was heavy (Borg
between 5 and 6). Whenever the intensity of the exercise was changed, the new load used was
immediately annotated in an individual file, used for recording.
Control Group
The CG did not carry out any type of intervention. The physiotherapist responsible for
the study contacted the CG participants every month during the six months of intervention to
emphasize the importance of not exercising, not using alcohol or smoking, not consuming
calcium, vitamin D, foods that contain isoflavones, supplements, or medications that could
141
influence BMD or muscle mass. At this time the participants were also questioned about
possible adverse events.
Adverse events
A standardized form was used to record occurrences of adverse events in all three
groups. The participants were questioned every month about any complication, such as muscle
spasms or pains, joint pain, dizziness, falls, cramps, and changes in blood pressure.
Statistical Analysis
The normality of the data was verified by the Shapiro-Wilk test. Descriptive data are
expressed as mean and standard deviation (SD). The Student t test for independent samples was
used to compare the number of participants' absences during the interventions (VG vs. PG).
The homogeneity of the variances was determined by the Levene’s test. To verify if the three
groups presented differences at baseline, one-way analysis of variance (ANOVA) was used for
data with normal distribution (age, weight, height, BMI and DXA areal BMD measurement).
Otherwise a Kruskal–Wallis test was calculated (time since menopause). Pearson's Chi-squared
test was used for comparison between different conditions of BMD (no alterations, osteopenic,
and osteoporotic). Intra-group changes between baseline and follow-up were analyzed via the
Student t test for dependent samples. To verify the between-group differences for the bone
parameters, covariance analysis (ANCOVA) was applied, with the follow-up data used as the
dependent variable and baseline data as covariate. The Bonferroni Post Hoc was used for
multiple comparisons between pairs (PG vs.VG; VG vs. CG; and PG vs. CG). Intra-group and
between-group effect sizes were calculated using Cohen's d, which was considered small (0.20),
medium (0.50), or large (0.80) [26]. Initially the data were analyzed using intention-to-treat
analysis (ITT), including all randomized subjects (missing data for the follow-up of two CG
142
participants were imputed by the group mean). Subsequently, per protocol analysis was
performed, excluding the two participants from the CG who abandoned the study. As the results
were similar, only the ITT analysis is presented in this report. For all tests, the level of
significance adopted was 95% (p < 0.05). The analyses were processed in SPSS 20.0 program
(Chicago, IL, USA), except for effect size calculations (Cohen's d), which were processed in
GPower 3.1 (Franz Faul, Universita¨t Kiel, Germany).
RESULTS
Adherence
After the six months of intervention, 96.1% of participants completed the study. Two
CG participants dropped out of the study (one started supplementation with calcium and the
other started exercise) (Fig. 1). The six months of intervention allowed for 78 sessions. The
number of participant absences did not differ significantly between the experimental groups (p
= 0.558), the variation was from 0 to 17 (6.76 ± 5.65) for the VG and 0 to 14 (5.76 ± 4.07) for
the PG. Thus, the mean frequency in the two groups was 91.3% and 92.6% respectively
(Supplementary Table 3).
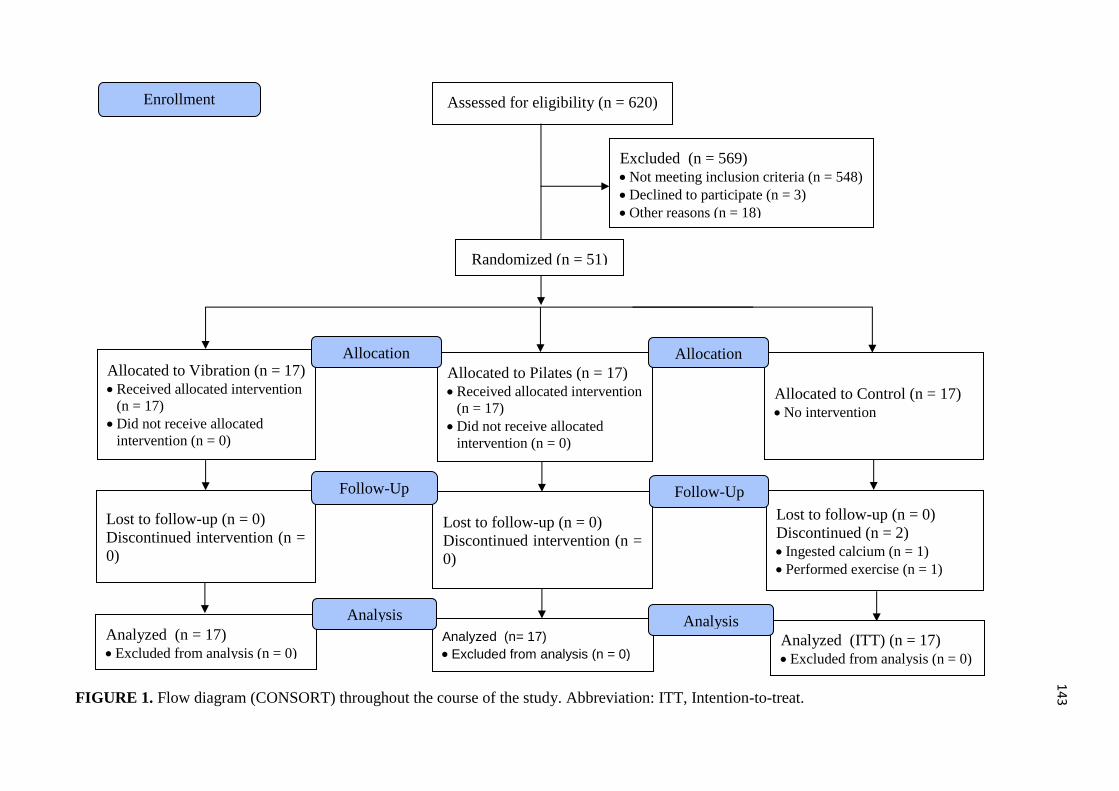
143
FIGURE 1. Flow diagram (CONSORT) throughout the course of the study. Abbreviation: ITT, Intention-to-treat.
Analyzed (n= 17)
• Excluded from analysis (n = 0)
Lost to follow-up (n = 0)
Discontinued (n = 2)
• Ingested calcium (n = 1)
• Performed exercise (n = 1)
Assessed for eligibility (n = 620)
Excluded (n = 569)
• Not meeting inclusion criteria (n = 548)
• Declined to participate (n = 3)
• Other reasons (n = 18)
Analyzed (n = 17)
• Excluded from analysis (n = 0)
Lost to follow-up (n = 0)
Discontinued intervention (n =
0)
Allocated to Vibration (n = 17)
• Received allocated intervention
(n = 17)
• Did not receive allocated
intervention (n = 0)
Allocated to Pilates (n = 17)
• Received allocated intervention
(n = 17)
• Did not receive allocated
intervention (n = 0)
Allocation
Analysis
Randomized (n = 51)
Enrollment
Allocated to Control (n = 17)
• No intervention
Allocation
Lost to follow-up (n = 0)
Discontinued intervention (n =
0)
Follow-Up Follow-Up
Analyzed (ITT) (n = 17)
• Excluded from analysis (n = 0)
Analysis
144
Baseline and Bone Outcomes
Table 1 lists the age, anthropometric parameters, menopausal time, condition related to
BMD, and DXA areal BMD measurement of the three groups at baseline. There were no
significant differences between the groups for any baseline parameter. Table 2 lists the DXA
values of the lumbar spine, femoral neck, total hip, trochanter, intertrochanter, and ward’s area
at baseline and follow-up, for intra-group changes and between-group interaction. The
experimental groups (VG and PG) significantly (p ≤ 0.001) improved DXA values intra-group
of the lumbar spine and trochanter, but no other measurements of BMD. For the lumbar spine
and trochanter, a significant (p ≤ 0.004) difference was observed between-group at follow-up.
In this case, the multiple comparisons in pairs presented in Table 3 show that the VG and PG
obtained a significant (p ≤ 0.018) improvement in DXA values of the lumbar spine and
trochanter when compared with the CG. In all cases where there was significant improvement
in DXA values there was a large effect size (Cohen’s d > 0.80).
Adverse Events
Serious adverse events were reported in all three groups: two falls in the VG; two in the
PG; and a fall in the CG that led to a fractured wrist. Reports of pain occurred mainly in the VG
and PG. The principal complaint of the participants was delayed muscle soreness, provided by
the WBV (58.8%) and Pilates (100%), principally in the first weeks of intervention. Other less
serious adverse events, such as pain in specific body regions, muscle spasms, and cramps
occurred less frequently (Supplementary Table 4).
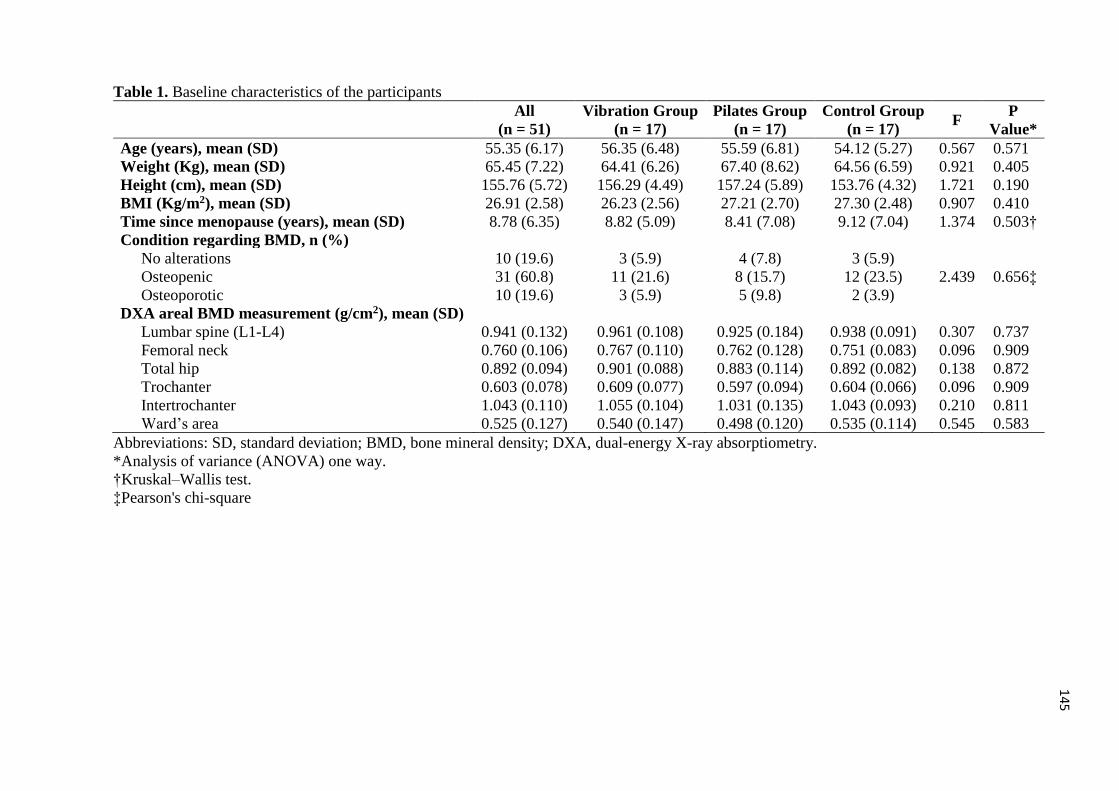
145
Table 1. Baseline characteristics of the participants
All
(n = 51)
Vibration Group
(n = 17)
Pilates Group
(n = 17)
Control Group
(n = 17) F
P
Value*
Age (years), mean (SD) 55.35 (6.17) 56.35 (6.48) 55.59 (6.81) 54.12 (5.27) 0.567 0.571
Weight (Kg), mean (SD) 65.45 (7.22) 64.41 (6.26) 67.40 (8.62) 64.56 (6.59) 0.921 0.405
Height (cm), mean (SD) 155.76 (5.72) 156.29 (4.49) 157.24 (5.89) 153.76 (4.32) 1.721 0.190
BMI (Kg/m2), mean (SD) 26.91 (2.58) 26.23 (2.56) 27.21 (2.70) 27.30 (2.48) 0.907 0.410
Time since menopause (years), mean (SD) 8.78 (6.35) 8.82 (5.09) 8.41 (7.08) 9.12 (7.04) 1.374 0.503†
Condition regarding BMD, n (%)
No alterations 10 (19.6) 3 (5.9) 4 (7.8) 3 (5.9)
2.439 0.656‡ Osteopenic 31 (60.8) 11 (21.6) 8 (15.7) 12 (23.5)
Osteoporotic 10 (19.6) 3 (5.9) 5 (9.8) 2 (3.9)
DXA areal BMD measurement (g/cm2), mean (SD)
Lumbar spine (L1-L4) 0.941 (0.132) 0.961 (0.108) 0.925 (0.184) 0.938 (0.091) 0.307 0.737
Femoral neck 0.760 (0.106) 0.767 (0.110) 0.762 (0.128) 0.751 (0.083) 0.096 0.909
Total hip 0.892 (0.094) 0.901 (0.088) 0.883 (0.114) 0.892 (0.082) 0.138 0.872
Trochanter 0.603 (0.078) 0.609 (0.077) 0.597 (0.094) 0.604 (0.066) 0.096 0.909
Intertrochanter 1.043 (0.110) 1.055 (0.104) 1.031 (0.135) 1.043 (0.093) 0.210 0.811
Ward’s area 0.525 (0.127) 0.540 (0.147) 0.498 (0.120) 0.535 (0.114) 0.545 0.583
Abbreviations: SD, standard deviation; BMD, bone mineral density; DXA, dual-energy X-ray absorptiometry.
*Analysis of variance (ANOVA) one way.
†Kruskal–Wallis test.
‡Pearson's chi-square
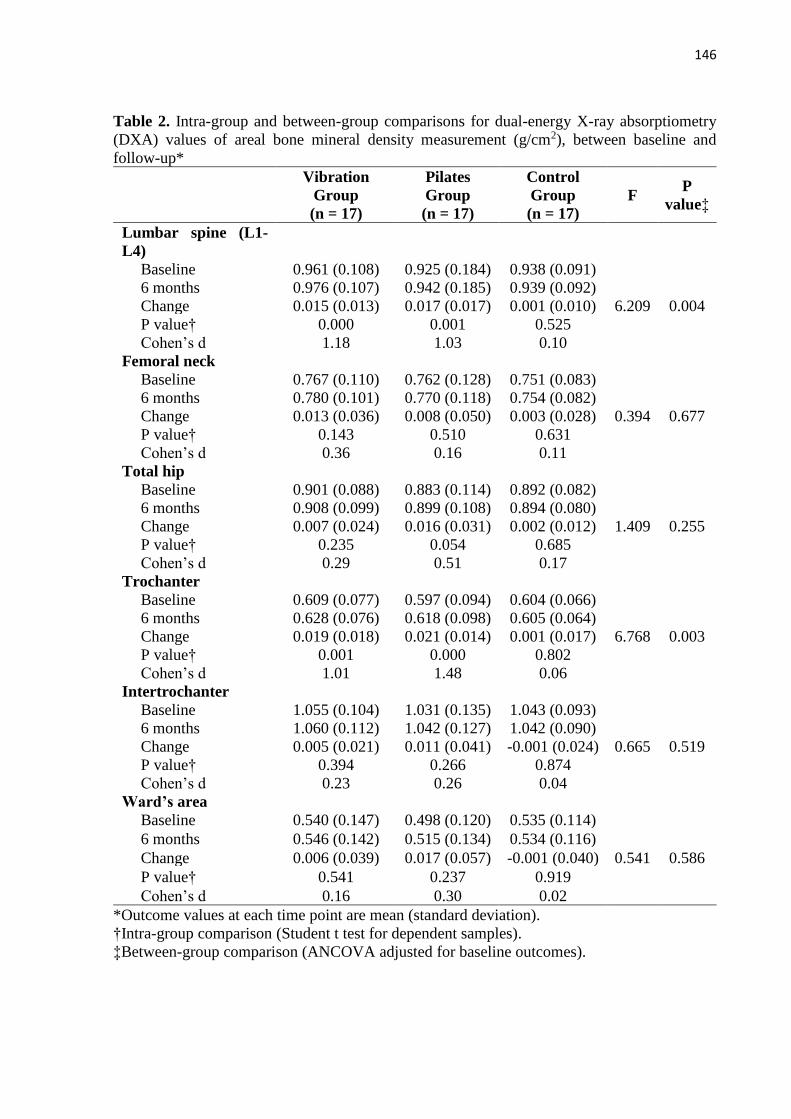
146
Table 2. Intra-group and between-group comparisons for dual-energy X-ray absorptiometry
(DXA) values of areal bone mineral density measurement (g/cm2), between baseline and
follow-up*
Vibration
Group
(n = 17)
Pilates
Group
(n = 17)
Control
Group
(n = 17)
F P
value‡
Lumbar spine (L1-
L4)
Baseline 0.961 (0.108) 0.925 (0.184) 0.938 (0.091)
6.209 0.004
6 months 0.976 (0.107) 0.942 (0.185) 0.939 (0.092)
Change 0.015 (0.013) 0.017 (0.017) 0.001 (0.010)
P value† 0.000 0.001 0.525
Cohen’s d 1.18 1.03 0.10
Femoral neck
Baseline 0.767 (0.110) 0.762 (0.128) 0.751 (0.083)
0.394 0.677
6 months 0.780 (0.101) 0.770 (0.118) 0.754 (0.082)
Change 0.013 (0.036) 0.008 (0.050) 0.003 (0.028)
P value† 0.143 0.510 0.631
Cohen’s d 0.36 0.16 0.11
Total hip
Baseline 0.901 (0.088) 0.883 (0.114) 0.892 (0.082)
1.409 0.255
6 months 0.908 (0.099) 0.899 (0.108) 0.894 (0.080)
Change 0.007 (0.024) 0.016 (0.031) 0.002 (0.012)
P value† 0.235 0.054 0.685
Cohen’s d 0.29 0.51 0.17
Trochanter
Baseline 0.609 (0.077) 0.597 (0.094) 0.604 (0.066)
6.768 0.003
6 months 0.628 (0.076) 0.618 (0.098) 0.605 (0.064)
Change 0.019 (0.018) 0.021 (0.014) 0.001 (0.017)
P value† 0.001 0.000 0.802
Cohen’s d 1.01 1.48 0.06
Intertrochanter
Baseline 1.055 (0.104) 1.031 (0.135) 1.043 (0.093)
0.665 0.519
6 months 1.060 (0.112) 1.042 (0.127) 1.042 (0.090)
Change 0.005 (0.021) 0.011 (0.041) -0.001 (0.024)
P value† 0.394 0.266 0.874
Cohen’s d 0.23 0.26 0.04
Ward’s area
Baseline 0.540 (0.147) 0.498 (0.120) 0.535 (0.114)
0.541 0.586
6 months 0.546 (0.142) 0.515 (0.134) 0.534 (0.116)
Change 0.006 (0.039) 0.017 (0.057) -0.001 (0.040)
P value† 0.541 0.237 0.919
Cohen’s d 0.16 0.30 0.02
*Outcome values at each time point are mean (standard deviation).
†Intra-group comparison (Student t test for dependent samples).
‡Between-group comparison (ANCOVA adjusted for baseline outcomes).
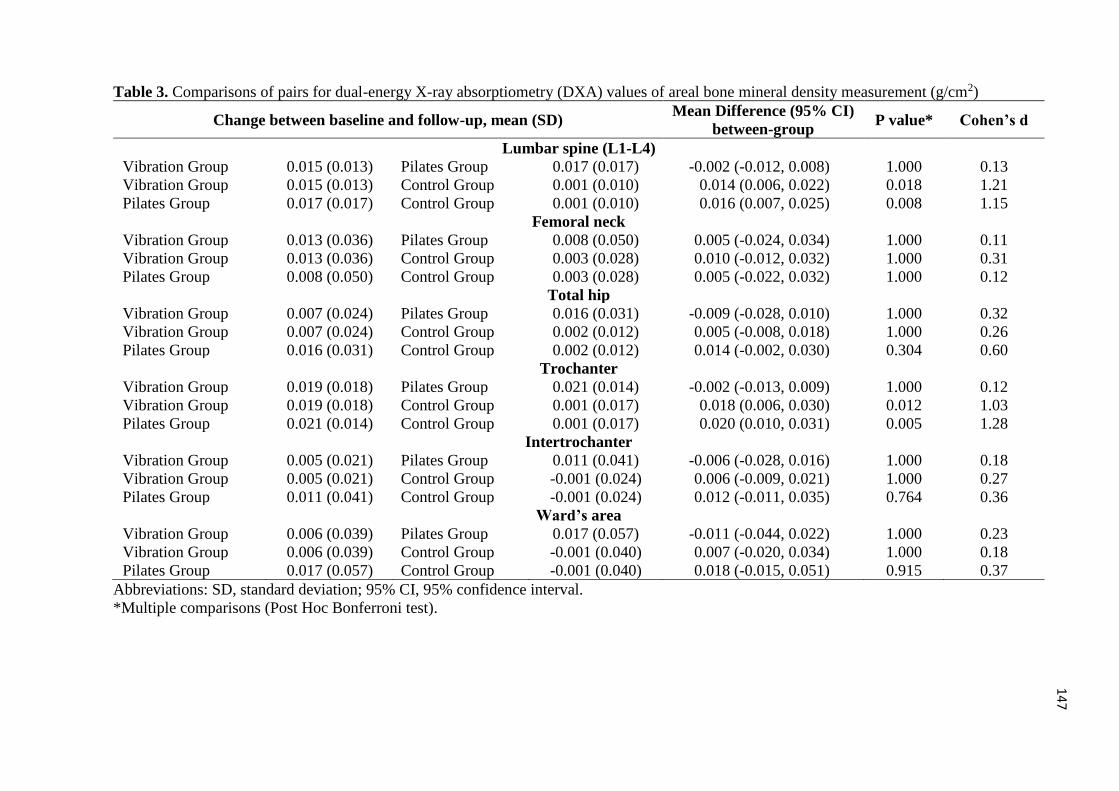
147
Table 3. Comparisons of pairs for dual-energy X-ray absorptiometry (DXA) values of areal bone mineral density measurement (g/cm2)
Change between baseline and follow-up, mean (SD) Mean Difference (95% CI)
between-group P value* Cohen’s d
Lumbar spine (L1-L4)
Vibration Group 0.015 (0.013) Pilates Group 0.017 (0.017) -0.002 (-0.012, 0.008) 1.000 0.13
Vibration Group 0.015 (0.013) Control Group 0.001 (0.010) 0.014 (0.006, 0.022) 0.018 1.21
Pilates Group 0.017 (0.017) Control Group 0.001 (0.010) 0.016 (0.007, 0.025) 0.008 1.15
Femoral neck
Vibration Group 0.013 (0.036) Pilates Group 0.008 (0.050) 0.005 (-0.024, 0.034) 1.000 0.11
Vibration Group 0.013 (0.036) Control Group 0.003 (0.028) 0.010 (-0.012, 0.032) 1.000 0.31
Pilates Group 0.008 (0.050) Control Group 0.003 (0.028) 0.005 (-0.022, 0.032) 1.000 0.12
Total hip
Vibration Group 0.007 (0.024) Pilates Group 0.016 (0.031) -0.009 (-0.028, 0.010) 1.000 0.32
Vibration Group 0.007 (0.024) Control Group 0.002 (0.012) 0.005 (-0.008, 0.018) 1.000 0.26
Pilates Group 0.016 (0.031) Control Group 0.002 (0.012) 0.014 (-0.002, 0.030) 0.304 0.60
Trochanter
Vibration Group 0.019 (0.018) Pilates Group 0.021 (0.014) -0.002 (-0.013, 0.009) 1.000 0.12
Vibration Group 0.019 (0.018) Control Group 0.001 (0.017) 0.018 (0.006, 0.030) 0.012 1.03
Pilates Group 0.021 (0.014) Control Group 0.001 (0.017) 0.020 (0.010, 0.031) 0.005 1.28
Intertrochanter
Vibration Group 0.005 (0.021) Pilates Group 0.011 (0.041) -0.006 (-0.028, 0.016) 1.000 0.18
Vibration Group 0.005 (0.021) Control Group -0.001 (0.024) 0.006 (-0.009, 0.021) 1.000 0.27
Pilates Group 0.011 (0.041) Control Group -0.001 (0.024) 0.012 (-0.011, 0.035) 0.764 0.36
Ward’s area
Vibration Group 0.006 (0.039) Pilates Group 0.017 (0.057) -0.011 (-0.044, 0.022) 1.000 0.23
Vibration Group 0.006 (0.039) Control Group -0.001 (0.040) 0.007 (-0.020, 0.034) 1.000 0.18
Pilates Group 0.017 (0.057) Control Group -0.001 (0.040) 0.018 (-0.015, 0.051) 0.915 0.37
Abbreviations: SD, standard deviation; 95% CI, 95% confidence interval.
*Multiple comparisons (Post Hoc Bonferroni test).
148
DISCUSSION
Summary of the main results
The results demonstrated that WBV or Pilates administered for six months, three times
a week, were equally effective for significant improvement of BMD in the lumbar spine and
trochanter in postmenopausal women but not for other bone regions. The techniques did not
differ between them, however were superior to no therapy. It is noteworthy that only two CG
participants abandoned the study, resulting in a follow-up of 96.1% of the participants initially
randomized. In addition, other relevant information is that the average frequency of the
participants submitted to the interventions (VG and PG) was higher than 90%. Serious adverse
events (mainly falls) occurred in 9.8% of all participants and affected all three groups.
Effects of Whole Body Vibration on Bone Mineral Density
With regard to WBV our research group had already discovered in a previous systematic
review and meta-analysis of RCTs that the lumbar spine and trochanter areas may be the most
responsive to increases in BMD in postmenopausal women [8]. However, significant results
were only observed in subgroup analyses, when parameters potentially more suitable for WBV
were used, such as side-alternating vibration, knee semi-flexion, low frequency and high
magnitude. Subgroup analyses that evaluated these parameters demonstrated effects on the
lumbar spine BMD area between 0.010 g/cm2 and 0.016 g/cm2, while for the trochanter the
variation was 0.019 g/cm2 to 0.020 g/cm2 [8], close to the values found in the present study.
Compared to the CG, participants in the VG demonstrated an increase in the BMD area of 0.014
g/cm2 and 0.018 g/cm2 for the lumbar spine and trochanter respectively. In addition, for the two
variables, a large effect size (Cohen's d > 0.80) was observed.
Iwamoto et al [27] and Gusi et al [28] also using low frequency, high magnitude, semi-
flexed knee and side-alternating type vibration found significant improvement in BMD area in
149
the lumbar spine and femoral neck regions respectively. However, following these same
parameters Liphardt et al [29] evaluating the regions of the lumbar spine and femoral neck and
Beck et al [30] evaluating the proximal forearm did not find significant improvements in BMD.
As WBV allows different parameters, the greatest controversy concerns which parameters
enable greater osteogenesis. For example, the fact that all studies with postmenopausal women
performed so far using high frequency and low magnitude have not found significant results for
BMD in any of the bone regions draws attention [30-34]. This premise refutes Wolff's bone
remodeling law in which there is a need for high impact (great magnitude) to enable greater
osteogenic effect [35]. The use of these parameters (high frequency and low magnitude) is
typically justified in the different studies because they have been successfully tested in animal
models [36-38], however, they do not appear to enable the same effects in humans.
Another important fact is that all the studies that tested synchronous vibration also did
not find any significant results for different BMD regions, regardless of frequency and
magnitude [39, 31, 32, 33, 34, 40, 41]. In addition, Von Stengel et al [41] compared two types
of vibration (synchronous and side-alternating) and verified that only the group of
postmenopausal women submitted to side-alternating vibration significantly improved lumbar
spine BMD when compared to the control group. The basic difference between vibration types
is that the synchronous platforms cause the right and left feet to move up and down at the same
time, while on the side-alternating platforms oscillations occur around a pivot in the center of
the platform, exposing the user to alternating vibrations between the sides (while the right foot
moves up the left foot moves down, and vice versa) [42], which supposedly alters the osteogenic
effect during WBV.
Regarding body positioning, studies that used knees extended during WBV generally
did not find significant improvements in BMD of any bone region [30-34], with the exception
of the study of Lai et al [18] who observed significant effects for lumbar spine BMD. This can
150
be justified by the type of vibration; while this study [18] used side-alternating vibration, the
others predominantly used synchronous vibration [31-34]. Supposedly, positioning with the
knees extended allows greater dissipation of the vibration by the skeleton, however, it has been
demonstrated that at frequencies of up to 30 Hz the damping of the vibrations in the position of
semi-flexed knees is insignificant for the regions of the lumbar spine and femur [43]. Thus,
although there is a need for further research, the parameters chosen for WBV training in the
present study seem to contribute more effectively to the increase of BMD in postmenopausal
women than other parameters tested to date.
Effects of Pilates on Bone Mineral Density
To date, only one RCT has investigated the effects of the Pilates method on BMD in
postmenopausal women. Angin et al [17] demonstrated that six months of Pilates performed
three times a week provided a significant increase in lumbar spine BMD, with great osteogenic
effect (0.063 g/cm2), while other body regions were not investigated. Perhaps the large effect
found by the authors when comparing Pilates to no intervention can be justified by the fact that
they included only participants with osteoporosis. Studies have shown that less dense bones
may demonstrate a greater response to interventions to increase BMD [32, 44, 45]. In the present
study in which participants were included regardless of bone condition (no alterations,
osteopenic, and osteoporotic), the osteogenic effect on the lumbar spine BMD area was 0.016
g/cm2 in favor of the PG compared to the CG (Cohen's d > 0.80 ).
A meta-analysis study [7] that grouped different forms of intervention using resistance
exercises of greater overload and less repetition found a significant increase for the DMO area
of the lumbar spine (0.86%) and femoral neck (1.03%), but not for other body regions (total
hip, trochanter, and ward's area) in postmenopausal women. When grouping studies that made
use of resistance exercises with lower overload and a greater number of repetitions no
151
significant results were observed. Although no meta-analysis study has used Pilates, this form
of intervention with resistance exercises uses higher overload and fewer repetitions. Coinciding
with the findings of Howe et al [7], in the present study a significant osteogenic effect was
found for lumbar spine BMD area, however the authors found improvement in the femoral
neck, while the present study observed improvement for the trochanter.
The elaboration of the Pilates exercise protocol for the present study was conducted in
a way that stimulated the increase in BMD, adequately controlling the intensity of therapy with
a heavy exercise level (Borg CR10: between 5 and 6) maintained during the muscle
strengthening exercises, resulting in increased overload and fewer repetitions. Nevertheless, we
attempted to maintain a traditional sequence of the method, which is typically adopted in
clinical practice, with stretching at the beginning and end of the sessions. In addition, all muscle
strengthening exercises were performed on equipment, which mostly enabled the use of springs,
facilitating the increase of the overload. Melo et al [24] demonstrated that the resistance torque
provided by the springs during Pilates movements can vary depending on two factors (their
positioning on the equipment or the level of resistance offered by the springs). The resistance
torque also changes during the execution of the movement as the spring lengthens, offering
different stresses during the same movement; factors that were considered in the prescription
and evolution of the Pilates intervention protocol in the present study, allowing adequate
overload. These parameters are important for outcomes such as BMD, which requires greater
overload and fewer repetitions [7].
Strengths and limitations
This is the first RCT to compare the effects of WBV vs. Pilates on the area of BMD in
postmenopausal women. Since the parameters chosen for WBV vary widely in different studies,
in the present research we explored those that until now have been identified as enabling greater
152
osteogenic effects [8]. On the other hand, in relation to Pilates, there has only been one RCT
performed with postmenopausal women to verify the effects on BMD, but without exploring
different bone regions [17]. In the present study we explored six different bone regions, which
made it possible to identify the areas most responsive to osteogenesis. As a limitation, since the
intervention involved WBV and Pilates it was not possible to blind the randomized participants
in the three groups and the physiotherapists who administered the therapies. However, it is
unlikely that this limitation influenced the bone outcomes investigated.
CONCLUSION
The WBV and Pilates techniques administered three times a week over six months
provided the same effect on the BMD area in postmenopausal women. Both were superior to
no intervention on the bone regions of the lumbar spine and trochanter. Since the techniques
are relatively safe and offer the same osteogenic effect, the choice of which to use can take into
account the existing resources or patient's preferences. In addition, as there is no conclusive
evidence on the best parameters of WBV or Pilates, based on multiple RCTs of good size,
concordant and/or robust meta-analysis of RCTs, the parameters presented in the present study
can be used provisionally as a reference in future interventions.
All procedures performed in studies involving human participants were in accordance with the
ethical standards of the institutional and/or national research committee and with the 1964
Helsinki declaration and its later amendments or comparable ethical standards.
Conflicts of interest Oliveira, Laís Campos de; Oliveira, Raphael Gonçalves de; and Pires-
Oliveira, Deise Aparecida de Almeida, declare that they have no conflict of interest.
153
REFERENCES
1. Blumel JE, Lavín P, Vallejo MS, Sarrá S (2014) Menopause or climacteric, just a semantic
discussion or has it clinical implications? Climacteric 17:235-241. doi:
10.3109/13697137.2013.838948
2. Gordon JL, Eisenlohr-Moul TA, Rubinow DR, Schrubbe L, Girdler SS (2016) Naturally
occurring changes in estradiol concentrations in the menopause transition predict morning
cortisol and negative mood in perimenopausal depression. Clin Psychol Sci 4:919-935. doi:
10.1177/2167702616647924
3. Christenson ES, Jiang X, Kagan R, Schnatz PF (2012) Osteoporosis management in post-
menopausal women. Min Ginecol 64:181-194
4. Holick MF (2017) Skeletal fragility, a common menopausal burden: risk assessment,
diagnosis, and management. In: Pal L. Sayegh RA, eds. Essentials of menopause management:
a case-based approach. Springer International Publishing 145-164. doi: 10.1007/978-3-319-
42451-4_8
5. International Osteoporosis Foundation (2017) What is Osteoporosis? Epidemiology.
Available from: http://www.iofbonehealth.org. Accessed 14 mar 2017
6. Hiligsmann M, Evers SM, Ben Sedrine W, Kanis JA, Ramaekers B, Reginster J, Silverman
S et al (2015) A systematic review of cost-effectiveness analyses of drugs for postmenopausal
osteoporosis. Pharmacoeconomics 33:205-224. doi: 10.1007/s40273-014-0231-1
7. Howe TE, Shea B, Dawson LJ, Downie F, Murray A, Ross C, Harbour RT et al (2011)
Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane
Database Syst Rev 6(7):CD000333. doi: 10.1002/14651858.CD000333.pub2
8. Oliveira LC, Oliveira RG, Pires-Oliveira DAA (2016) Effects of whole body vibration on
bone mineral density in postmenopausal women: a systematic review and meta-analysis.
Osteoporos Int 27:2913-2933. doi: 10.1007/s00198-016-3618-3
154
9. Marjoribanks J, Farquhar C, Roberts H, Lethaby A, Lee J, Lee J (2017) Long‐term hormone
therapy for perimenopausal and postmenopausal women. Cochrane Database Syst Rev
1:CD004143. doi: 10.1002/14651858.CD004143.pub5
10. Cosman F, De Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, Lindsay R (2015)
Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 26:2045-2047.
doi: 10.1007/s00198-015-3037-x
11. Ma C, Liu A, Sun M, Zhu H, Wu H (2016) Effect of whole-body vibration on reduction of
bone loss and fall prevention in postmenopausal women: a meta-analysis and systematic
review. J Orthop Surg Res 11:24. doi: 10.1186/s13018-016-0357-2
12. Christiansen BA, Silva MJ (2006) The effect of varying magnitudes of whole-body
vibration on several skeletal sites in mice. Ann Biomed Eng 34:1149-1156. doi:
10.1007/s10439-006-9133-5
13. Rauch F, Sievanen H, Boonen S et al (2010) Reporting whole-body vibration intervention
studies: recommendations of the International Society of Musculoskeletal and Neuronal
Interactions. J Musculoskelet Neuronal Interact 10:193-198
14. Wysocki A, Butler M, Shamliyan T, Kane RL (2011) Whole-body vibration therapy for
osteoporosis: state of the science. Ann Intern Med 155:680-686. doi: 10.7326/0003-4819-155-
10-201111150-00006
15. Kloubec J (2011) Pilates: how does it work and who needs it? Muscles Ligaments Tendons
J 1:61-66
16. Di Lorenzo CE (2011) Pilates: what is it? Should it be used in rehabilitation? Sports Health
3(4):352-361. doi: 10.1177/1941738111410285
17. Angın E, Erden Z, Can F (2015) The effects of clinical pilates exercises on bone mineral
density, physical performance and quality of life of women with postmenopausal osteoporosis.
J Back Musculoskelet Rehabil 28:849-858. doi: 10.3233/BMR-150604
155
18. Lai CL, Tseng SL, Chen CN, Liao WC, Wang CH, Lee MC, Hsu PS (2013) Effect of 6
months of whole body vibration on lumbar spine bone density in postmenopausal women: a
randomized controlled trial. Clin Interv Aging 8:1603-1609. doi: 10.2147/CIA.S53591
19. Katz S, Ford A, Moskowitz RW, Jackson BA, Jaffe MW (1963) Studies of illness in the
aged. The index of ADL: a standardized measure of biological and psychosocial function.
JAMA 21:914-919
20. Lawton MP, Brody EM (1969) Assessment of older people: self-maintaining and
instrumental activities of daily living. Gerontologist 9:179-186
21. Folstein MF, Folstein SE, McHugh PR (1975) "Mini-mental state". A practical method for
grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189-198
22. World Health Organization (1994) Assessment of fracture risk and its application to
screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health
Organ Tech Rep Ser 843:1-129
23. Tothill P, Hannan WJ (2007) Precision and accuracy of measuring changes in bone mineral
density by dual-energy X-ray absorptiometry. Osteoporos Int 18:1515-1523. doi:
10.1007/s00198-007-0382-4
24. Melo MO, Gomes LE, Silva YO, Bonezi A, Loss JF (2011) Assessment of resistance torque
and resultant muscular force during Pilates hip extension exercise and its implications to
prescription and progression. Rev Bras Fisioter 15:23-30
25. Borg GAV (1982) Psychophysical bases of perceived exertion. Med Sci Sport Exerc
14:377-381
26. Cohen J (1988) Statistical power analysis for the behavioral sciences. 2rd ed. Hillsdale, NJ:
Lawrence Erlbaum Associates
27. Iwamoto J, Takeda T, Sato Y, Uzawa M (2005) Effect of whole body vibration exercise on
lumbar bone mineral density, bone turnover, and chronic back pain in post-menopausal
156
osteoporotic women treated with alendronate. Aging Clin Exp Res 17:157-163. doi:
10.1007/BF03324589
28. Gusi N, Raimundo A, Leal A (2006) Low-frequency vibratory exercise reduces the risk of
bone fracture more than walking: a randomized controlled trial. BMC Musculoskelet Disord
7:92. doi: 10.1186/1471-2474-7-92
29. Liphardt AM, Schipilow J, Hanley DA, Boyd SK (2015) Bone quality in osteopenic
postmenopausal women is not improved after 12 months of whole-body vibration training.
Osteoporos Int 26:911-920. doi: 10.1007/s00198-014-2995-8
30. Beck BR, Norling TL (2010) The effect of eight months of twiceweekly low or higher
intensity whole body vibration on risk factors for postmenopausal hip fracture. Am J Phys Med
Rehabil 89:997-1009. doi: 10.1097/PHM.0b013e3181f71063
31. Leung KS, Li CY, Tse YK, Choy TK, Leung PC, Hung VWY, Chan SY et al (2014) Effects
of 18-month low-magnitude high-frequency vibration on fall rate and fracture risks in 710
community elderly - a cluster - randomized controlled trial. Osteoporos Int 25:1785-1795. doi:
10.1007/s00198-014-2693-6
32. Rubin C, Recker R, Cullen D, Ryaby J, McCabe J, McLeod K (2004) Prevention of
postmenopausal bone loss by a low-magnitude, high-frequency mechanical stimuli: a clinical
trial assessing compliance, efficacy, and safety. J Bone Miner Res 19:343-351. doi:
10.1359/JBMR.0301251
33. Slatkovska L, Beyene J, Alibhai SMH, Wong Q, Sohail QZ, Cheung AM (2014) Effect of
whole-body vibration on calcaneal quantitative ultrasound measurements in postmenopausal
women: a randomized controlled trial. Calcif Tissue Int 95:547-556. doi:10.1007/s00223-014-
9920-1
34. Slatkovska L, Alibhai SMH, Beyene J, Hu H, Demaras A, Cheung AM (2011) Effect of
12months of whole-body vibration therapy on bone density and structure in postmenopausal
157
women. A randomized trial. Ann Intern Med 155:668-679. doi: 10.7326/0003-4819-155-10-
201111150-00005
35. Wolff J (1986) The law of bone remodeling. Springer doi: 10.1007/978-3-642-71031-5
36. Liang Y-Q, Qi M-C, Xu J, Xu J, Liu HW, Dong W, Li J et al (2014) Low-magnitude high-
frequency loading, by whole-body vibration, accelerates early implant osseointegration in
ovariectomized rats. Mol Med Rep 10:2835-2842. doi: 10.3892/mmr.2014. 2597
37. Shi HF, Cheung WH, Qin L, Leung AHC, Leung KS (2010) Low-magnitude high-
frequency vibration treatment augments fracture healing in ovariectomy-induced osteoporotic
bone. Bone 46:1299-1305. doi: 10.1016/j.bone.2009.11.028
38. Vanleene M, Shefelbine SJ (2013) Therapeutic impact of low amplitude high frequency
whole body vibrations on the osteogenesis imperfecta mouse bone. Bone 53:507-514. doi:
10.1016/j.bone. 2013.01.023
39. Karakiriou SK, Douda HT, Smilios IG, Volaklis KA, Tokmakidis SP (2012) Effects of
vibration and exercise training on bonemineral density and muscle strength in post-menopausal
women. Eur J Sport Sci 12:81-88. doi: 10.1080/17461391.2010.536581
40. Santin-Medeiros F, Santos-Lozano A, Rey-López JP, Garatachea N (2015) Effects of eight
months of whole body vibration training on hip bone mass in older women. Nutr Hosp 31:1654-
1659. doi: 10.3305/nh.2015.31.4.8441
41. Von Stengel S, Kemmler W, Bebenek M, Engelke K, Kalender WA (2011) Effects of
whole-body vibration training on different devices on bone mineral density. Med Sci Sports
Exerc 43:1071-1079. doi: 10.1249/MSS.0b013e318202f3d3
42. Rauch F (2009) Vibration Therapy. Dev Med Child Neurol 51:166-168. doi:
10.1111/j.1469-8749.2009.03418.x
43. Judex S, Rubin CT (2010) Is bone formation induced by highfrequency mechanical signals
modulated by muscle activity? J Musculoskelet Neuronal Interact 10:3-11
158
44. Flieger J, Karachalios T, Khaldi L, Raptou P, Lyritis G (1998) Mechanical stimulation in
the form of vibration prevents postmenopausal bone loss in ovariectomized rats. Calcif Tissue
Int 63:510-514. doi: 10.1007/s002239900566
45. Judex S, Donahue LR, Rubin C (2002) Genetic predisposition to low bone mass is paralleled
by an enhanced sensitivity to signals anabolic to the skeleton. FASEB J 16:1280-1282. doi:
10.1096/fj.01-0913fje
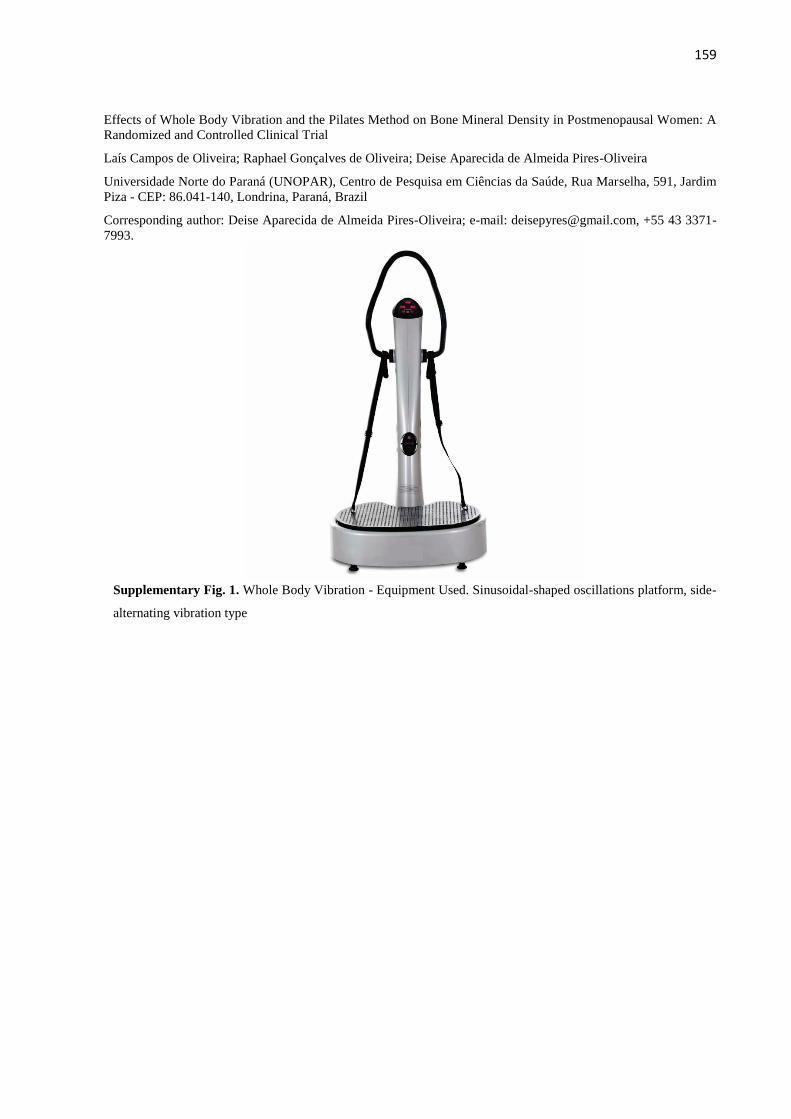
159
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in Postmenopausal Women: A
Randomized and Controlled Clinical Trial
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Universidade Norte do Paraná (UNOPAR), Centro de Pesquisa em Ciências da Saúde, Rua Marselha, 591, Jardim
Piza - CEP: 86.041-140, Londrina, Paraná, Brazil
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira; e-mail: [email protected], +55 43 3371-
7993.
Supplementary Fig. 1. Whole Body Vibration - Equipment Used. Sinusoidal-shaped oscillations platform, side-
alternating vibration type
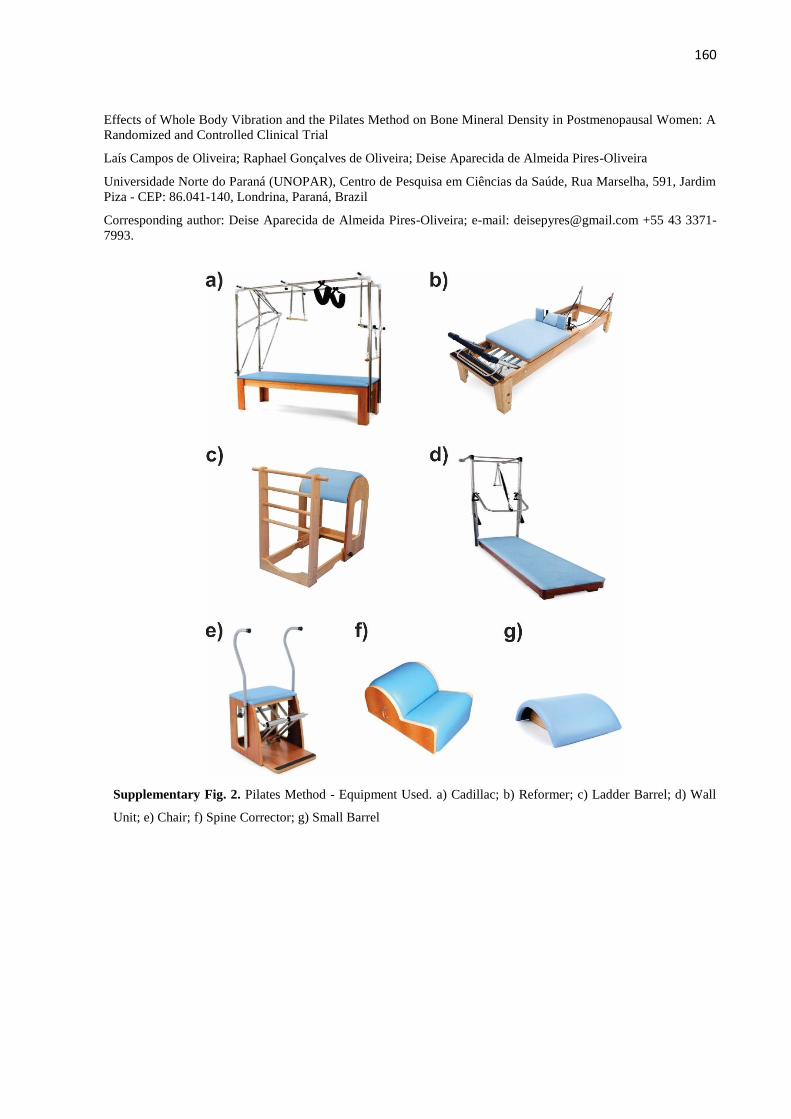
160
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in Postmenopausal Women: A
Randomized and Controlled Clinical Trial
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Universidade Norte do Paraná (UNOPAR), Centro de Pesquisa em Ciências da Saúde, Rua Marselha, 591, Jardim
Piza - CEP: 86.041-140, Londrina, Paraná, Brazil
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira; e-mail: [email protected] +55 43 3371-
7993.
Supplementary Fig. 2. Pilates Method - Equipment Used. a) Cadillac; b) Reformer; c) Ladder Barrel; d) Wall
Unit; e) Chair; f) Spine Corrector; g) Small Barrel
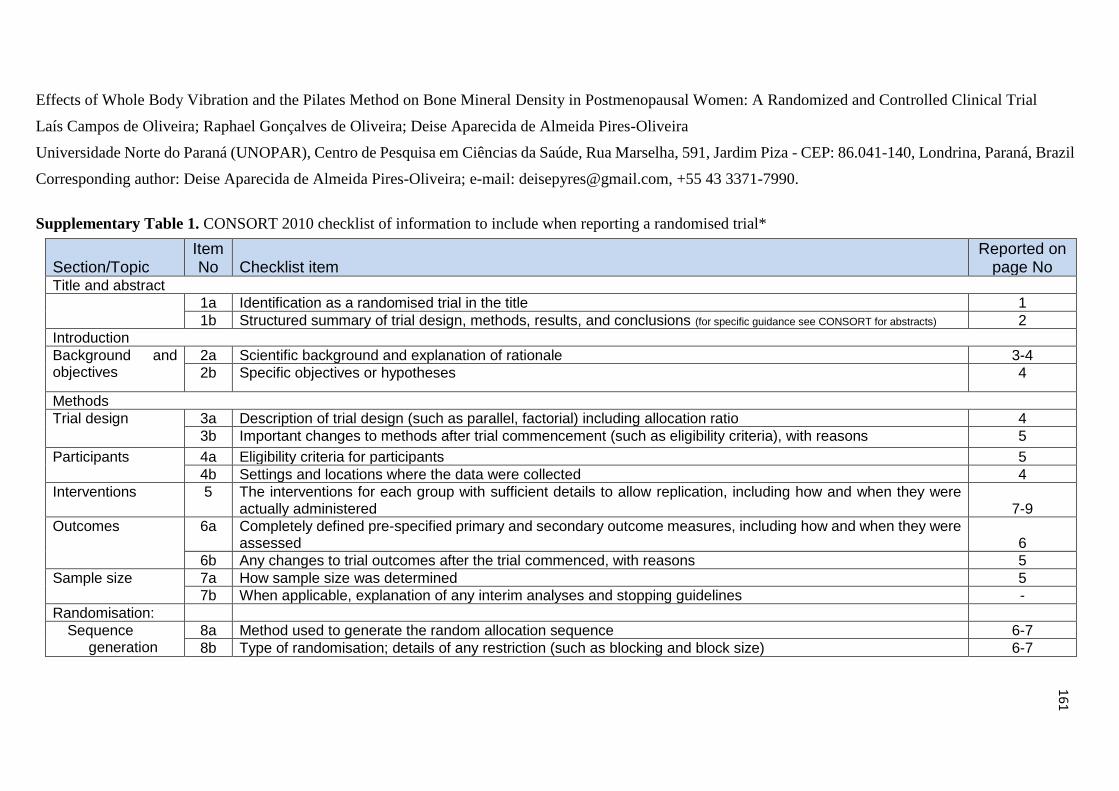
161
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in Postmenopausal Women: A Randomized and Controlled Clinical Trial
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Universidade Norte do Paraná (UNOPAR), Centro de Pesquisa em Ciências da Saúde, Rua Marselha, 591, Jardim Piza - CEP: 86.041-140, Londrina, Paraná, Brazil
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira; e-mail: [email protected], +55 43 3371-7990.
Supplementary Table 1. CONSORT 2010 checklist of information to include when reporting a randomised trial*
Section/Topic Item No Checklist item
Reported on page No
Title and abstract
1a Identification as a randomised trial in the title 1
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) 2
Introduction
Background and objectives
2a Scientific background and explanation of rationale 3-4
2b Specific objectives or hypotheses 4
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio 4
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons 5
Participants 4a Eligibility criteria for participants 5
4b Settings and locations where the data were collected 4
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were actually administered
7-9
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed
6
6b Any changes to trial outcomes after the trial commenced, with reasons 5
Sample size 7a How sample size was determined 5
7b When applicable, explanation of any interim analyses and stopping guidelines -
Randomisation:
Sequence generation
8a Method used to generate the random allocation sequence 6-7
8b Type of randomisation; details of any restriction (such as blocking and block size) 6-7
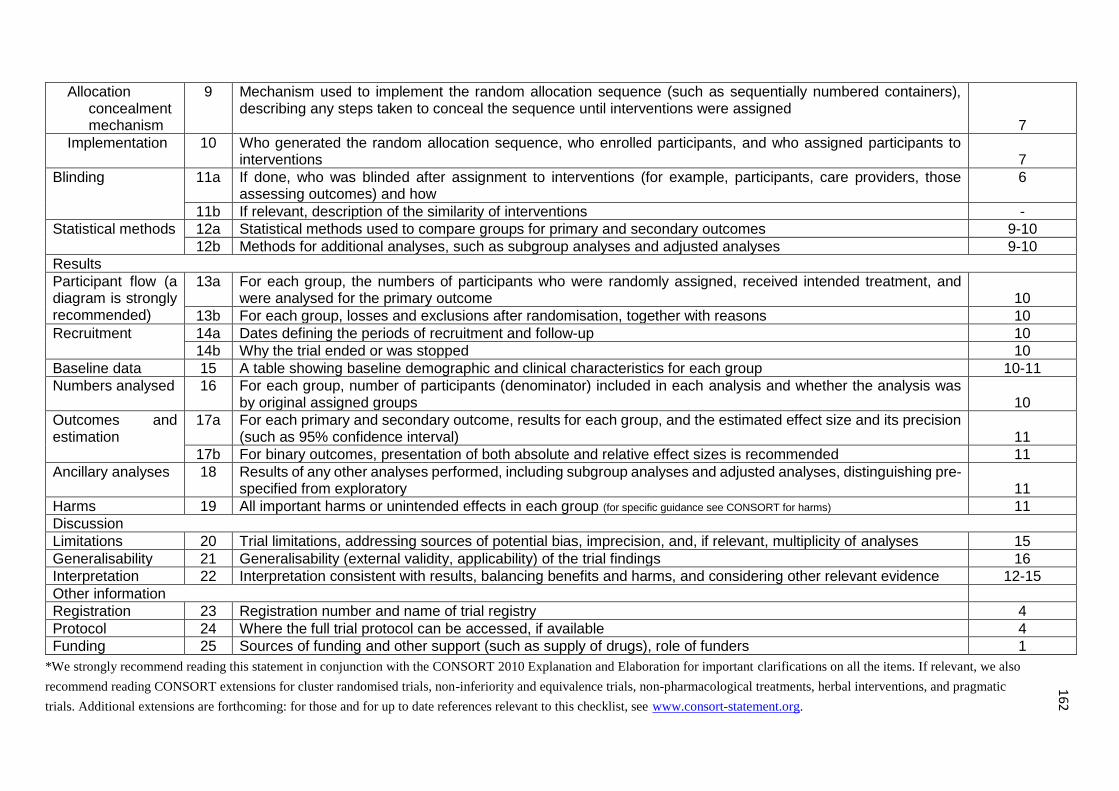
162
Allocation
concealment mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned
7
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions
7
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how
6
11b If relevant, description of the similarity of interventions -
Statistical methods 12a Statistical methods used to compare groups for primary and secondary outcomes 9-10
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses 9-10
Results
Participant flow (a diagram is strongly recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analysed for the primary outcome
10
13b For each group, losses and exclusions after randomisation, together with reasons 10
Recruitment 14a Dates defining the periods of recruitment and follow-up 10
14b Why the trial ended or was stopped 10
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group 10-11
Numbers analysed 16 For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups
10
Outcomes and estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval)
11
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended 11
Ancillary analyses 18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory
11
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) 11
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses 15
Generalisability 21 Generalisability (external validity, applicability) of the trial findings 16
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence 12-15
Other information
Registration 23 Registration number and name of trial registry 4
Protocol 24 Where the full trial protocol can be accessed, if available 4
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders 1
*We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also
recommend reading CONSORT extensions for cluster randomised trials, non-inferiority and equivalence trials, non-pharmacological treatments, herbal interventions, and pragmatic
trials. Additional extensions are forthcoming: for those and for up to date references relevant to this checklist, see www.consort-statement.org.
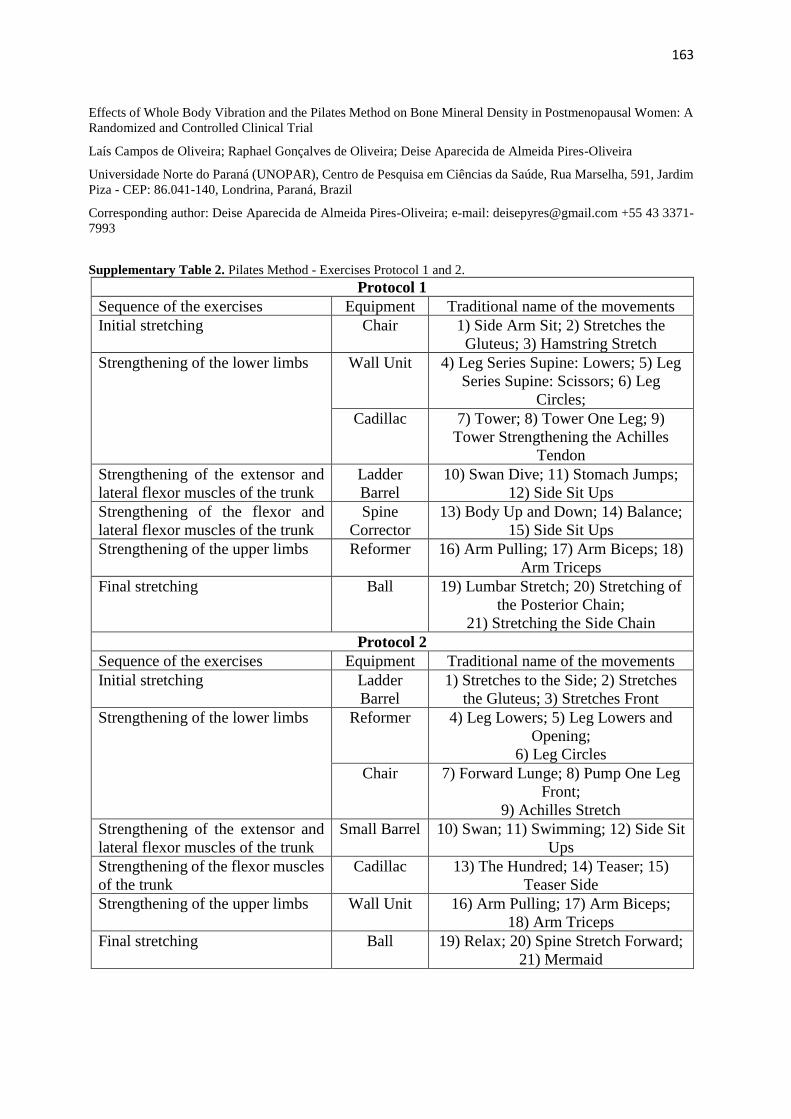
163
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in Postmenopausal Women: A
Randomized and Controlled Clinical Trial
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Universidade Norte do Paraná (UNOPAR), Centro de Pesquisa em Ciências da Saúde, Rua Marselha, 591, Jardim
Piza - CEP: 86.041-140, Londrina, Paraná, Brazil
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira; e-mail: [email protected] +55 43 3371-
7993
Supplementary Table 2. Pilates Method - Exercises Protocol 1 and 2.
Protocol 1
Sequence of the exercises Equipment Traditional name of the movements
Initial stretching Chair 1) Side Arm Sit; 2) Stretches the
Gluteus; 3) Hamstring Stretch
Strengthening of the lower limbs Wall Unit 4) Leg Series Supine: Lowers; 5) Leg
Series Supine: Scissors; 6) Leg
Circles;
Cadillac 7) Tower; 8) Tower One Leg; 9)
Tower Strengthening the Achilles
Tendon
Strengthening of the extensor and
lateral flexor muscles of the trunk
Ladder
Barrel
10) Swan Dive; 11) Stomach Jumps;
12) Side Sit Ups
Strengthening of the flexor and
lateral flexor muscles of the trunk
Spine
Corrector
13) Body Up and Down; 14) Balance;
15) Side Sit Ups
Strengthening of the upper limbs Reformer 16) Arm Pulling; 17) Arm Biceps; 18)
Arm Triceps
Final stretching Ball 19) Lumbar Stretch; 20) Stretching of
the Posterior Chain;
21) Stretching the Side Chain
Protocol 2
Sequence of the exercises Equipment Traditional name of the movements
Initial stretching Ladder
Barrel
1) Stretches to the Side; 2) Stretches
the Gluteus; 3) Stretches Front
Strengthening of the lower limbs Reformer 4) Leg Lowers; 5) Leg Lowers and
Opening;
6) Leg Circles
Chair 7) Forward Lunge; 8) Pump One Leg
Front;
9) Achilles Stretch
Strengthening of the extensor and
lateral flexor muscles of the trunk
Small Barrel 10) Swan; 11) Swimming; 12) Side Sit
Ups
Strengthening of the flexor muscles
of the trunk
Cadillac 13) The Hundred; 14) Teaser; 15)
Teaser Side
Strengthening of the upper limbs Wall Unit 16) Arm Pulling; 17) Arm Biceps;
18) Arm Triceps
Final stretching Ball 19) Relax; 20) Spine Stretch Forward;
21) Mermaid
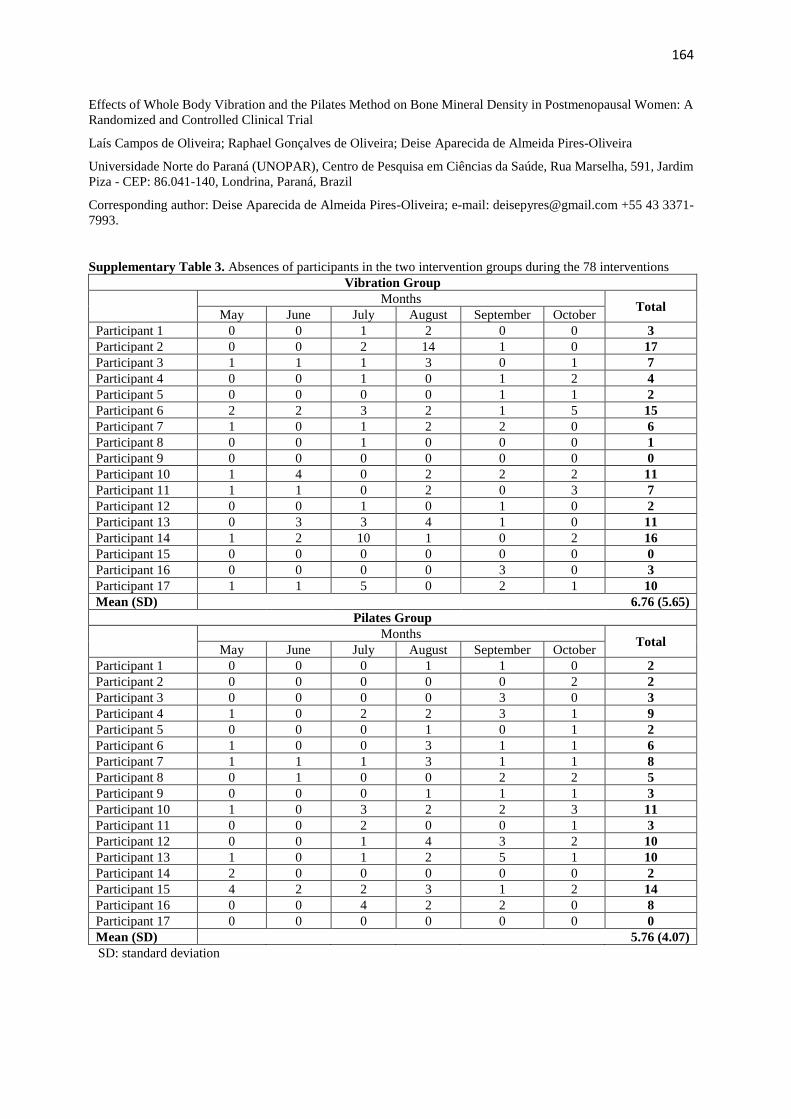
164
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in Postmenopausal Women: A
Randomized and Controlled Clinical Trial
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Universidade Norte do Paraná (UNOPAR), Centro de Pesquisa em Ciências da Saúde, Rua Marselha, 591, Jardim
Piza - CEP: 86.041-140, Londrina, Paraná, Brazil
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira; e-mail: [email protected] +55 43 3371-
7993.
Supplementary Table 3. Absences of participants in the two intervention groups during the 78 interventions
Vibration Group
Months Total
May June July August September October
Participant 1 0 0 1 2 0 0 3
Participant 2 0 0 2 14 1 0 17
Participant 3 1 1 1 3 0 1 7
Participant 4 0 0 1 0 1 2 4
Participant 5 0 0 0 0 1 1 2
Participant 6 2 2 3 2 1 5 15
Participant 7 1 0 1 2 2 0 6
Participant 8 0 0 1 0 0 0 1
Participant 9 0 0 0 0 0 0 0
Participant 10 1 4 0 2 2 2 11
Participant 11 1 1 0 2 0 3 7
Participant 12 0 0 1 0 1 0 2
Participant 13 0 3 3 4 1 0 11
Participant 14 1 2 10 1 0 2 16
Participant 15 0 0 0 0 0 0 0
Participant 16 0 0 0 0 3 0 3
Participant 17 1 1 5 0 2 1 10
Mean (SD) 6.76 (5.65)
Pilates Group
Months Total
May June July August September October
Participant 1 0 0 0 1 1 0 2
Participant 2 0 0 0 0 0 2 2
Participant 3 0 0 0 0 3 0 3
Participant 4 1 0 2 2 3 1 9
Participant 5 0 0 0 1 0 1 2
Participant 6 1 0 0 3 1 1 6
Participant 7 1 1 1 3 1 1 8
Participant 8 0 1 0 0 2 2 5
Participant 9 0 0 0 1 1 1 3
Participant 10 1 0 3 2 2 3 11
Participant 11 0 0 2 0 0 1 3
Participant 12 0 0 1 4 3 2 10
Participant 13 1 0 1 2 5 1 10
Participant 14 2 0 0 0 0 0 2
Participant 15 4 2 2 3 1 2 14
Participant 16 0 0 4 2 2 0 8
Participant 17 0 0 0 0 0 0 0
Mean (SD) 5.76 (4.07)
SD: standard deviation
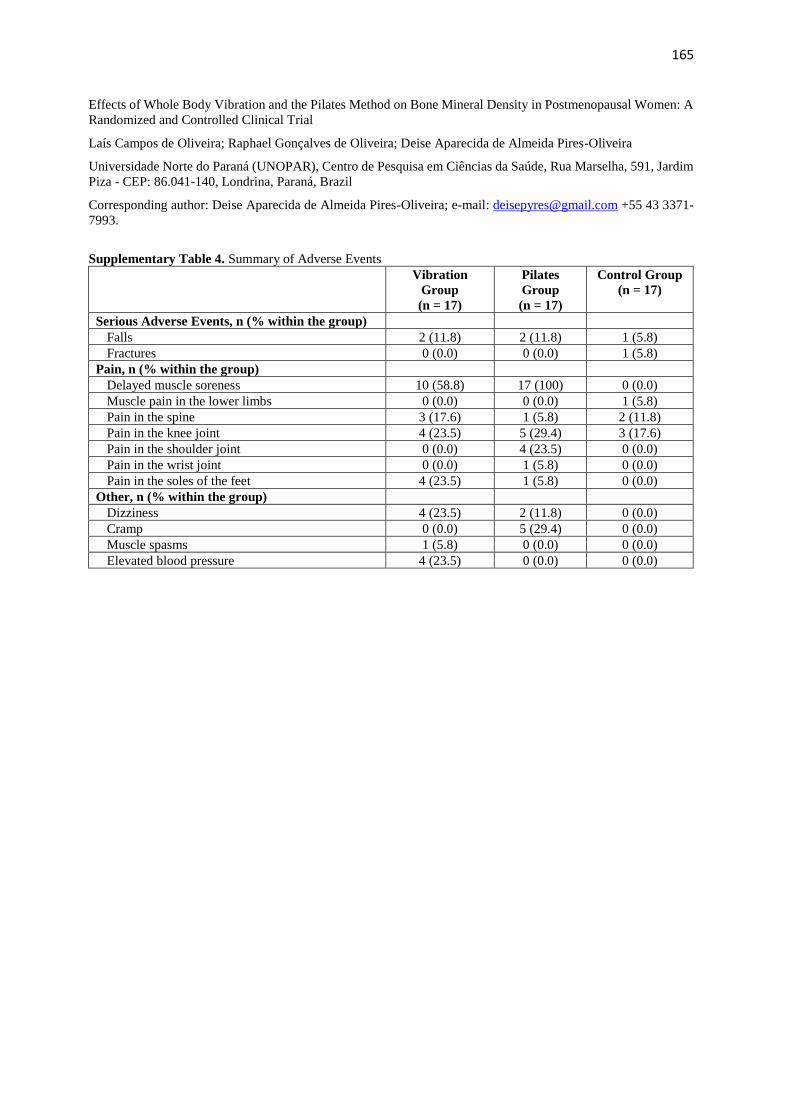
165
Effects of Whole Body Vibration and the Pilates Method on Bone Mineral Density in Postmenopausal Women: A
Randomized and Controlled Clinical Trial
Laís Campos de Oliveira; Raphael Gonçalves de Oliveira; Deise Aparecida de Almeida Pires-Oliveira
Universidade Norte do Paraná (UNOPAR), Centro de Pesquisa em Ciências da Saúde, Rua Marselha, 591, Jardim
Piza - CEP: 86.041-140, Londrina, Paraná, Brazil
Corresponding author: Deise Aparecida de Almeida Pires-Oliveira; e-mail: [email protected] +55 43 3371-
7993.
Supplementary Table 4. Summary of Adverse Events
Vibration
Group
(n = 17)
Pilates
Group
(n = 17)
Control Group
(n = 17)
Serious Adverse Events, n (% within the group)
Falls 2 (11.8) 2 (11.8) 1 (5.8)
Fractures 0 (0.0) 0 (0.0) 1 (5.8)
Pain, n (% within the group)
Delayed muscle soreness 10 (58.8) 17 (100) 0 (0.0)
Muscle pain in the lower limbs 0 (0.0) 0 (0.0) 1 (5.8)
Pain in the spine 3 (17.6) 1 (5.8) 2 (11.8)
Pain in the knee joint 4 (23.5) 5 (29.4) 3 (17.6)
Pain in the shoulder joint 0 (0.0) 4 (23.5) 0 (0.0)
Pain in the wrist joint 0 (0.0) 1 (5.8) 0 (0.0)
Pain in the soles of the feet 4 (23.5) 1 (5.8) 0 (0.0)
Other, n (% within the group)
Dizziness 4 (23.5) 2 (11.8) 0 (0.0)
Cramp 0 (0.0) 5 (29.4) 0 (0.0)
Muscle spasms 1 (5.8) 0 (0.0) 0 (0.0)
Elevated blood pressure 4 (23.5) 0 (0.0) 0 (0.0)
166
6.3 ARTIGO 3: ESTUDO ORIGINAL
Artigo a ser submetido para o Journal of Aging and Physical Activity (ISSN: 1543-
267X).
Fator de Impacto JCR de 2016: 1,837.
Efeitos do método Pilates vs. vibração de corpo inteiro nas medidas de força muscular e
qualidade de vida em mulheres na pós-menopausa: um ensaio clínico randomizado e
controlado
Pilates vs. VCI na força muscular
Resumo
Introdução: Mulheres na pós-menopausa apresentam diminuição da força muscular e da
qualidade de vida. Pilates e vibração de corpo inteiro (VCI) podem melhorar estas variáveis.
Objetivo: Verificar os efeitos do Pilates vs. VCI na força muscular e qualidade de vida em
mulheres na pós-menopausa.
Métodos: 51 mulheres foram aleatoriamente designadas para esses grupos, Pilates (n = 17),
vibração (n = 17) ou controle sem intervenção (n = 17). Avaliações foram realizadas para força
muscular isocinética (N.m) dos extensores e flexores do joelho (60º/s e 180º/s) e qualidade de
vida pelo SF-36.
Resultados: Pilates foi superior (p < 0.05) à VCI apenas para força muscular dos flexores do
joelho à 60º/s. Nas comparações com o grupo controle, Pilates foi superior (p < 0.05) em todas
as variáveis de força muscular e em quatro domínios do SF-36.
Conclusão: Pilates é uma alternativa de intervenção superior a VCI quando o objetivo estiver
atrelado a força da musculatura flexora do joelho.
Palavras-chave: exercício; força muscular isocinética; menopausa; saúde da mulher.
167
INTRODUÇÃO
Mulheres no período da pós-menopausa sofrem com alterações hormonais em
decorrência do rápido declínio dos níveis de estrogênio (Gordon et al., 2016; Hale, Robertson,
& Burger, 2014). Neste período ocorre a cessação do ciclo ovulatório, que coincide com
alterações fisiológicas importantes, típicas do processo de envelhecimento (Levine et al.,
2016), que potencializa o aparecimento de efeitos negativos para saúde, como a diminuição
da força muscular (Lee, & Lee, 2013) e o comprometimento da qualidade de vida (Mirhaghjou
et al., 2016).
Dentre as formas para atenuar ou reverter estes fatores, destaca-se a prática regular e
sistemática de exercícios físicos (Mendoza et al., 2016). Uma opção emergente de exercício
que tem sido investigado, em relação aos seus benefícios para mulheres na pós-menopausa é
o método Pilates (Lee et al., 2016; Hita-Contreras, Martínez-Amat, Cruz-Díaz, & Pérez-
López, 2016; Angın, Erden, & Can, 2015). Esta técnica atua por meio de exercícios de
resistência muscular progressiva e tem se mostrado efetiva para o aumento da força muscular
(Oliveira, Oliveira, & Pires-Oliveira, 2017; Vieira et al., 2017; Oliveira et al., 2017; Bergamin
et al., 2015; Bird, & Fell, 2014; Plachy, Kovách, & Bognár, 2012; Irez et al., 2011) e a melhora
da qualidade de vida em mulheres mais velhas (Angın, Erden, & Can, 2015; Campos de
Oliveira, Gonçalves de Oliveira, & Pires-Oliveira, 2015; Küçükçakır, Altan, & Korkmaz,
2013; Siqueira Rodrigues et al., 2010). Um estudo de meta-análise que teve como objetivo
mensurar os efeitos do Pilates sobre diferentes desfechos de saúde em adultos mais velhos,
identificou que o método possibilita significativa melhora da força muscular e qualidade de
vida (Bullo et al., 2015). No entanto, outros estudos demonstraram que Pilates pode não
aumentar a força muscular (Bird, Hill, & Fell, 2012) ou contribuir com a melhora de diferentes
domínios da qualidade de vida em adultos mais velhos (Kovách et al., 2013).
168
Outra técnica que tem demonstrado diferentes beneficios para desfechos de saúde em
mulheres no período da pós-menopausa é a vibração de corpo inteiro (VCI) (Oliveira, Oliveira,
& Pires-Oliveira, 2016; Lau et al., 2011). Estudos tem demonstrado que VCI pode possibilitar
aumento da força muscular (Wei, Pang, Ng, & Ng, 2016; Von Stengel et al., 2011;
Verschueren et al., 2004) e melhora da qualidade de vida em adultos mais velhos (Furness, &
Maschette, 2009; Bruyere et al., 2005), contudo, alguns estudos não observaram os beneficios
desta técnica sobre a força muscular (Liphardt, Schipilow, Hanley, & Boyd, 2015; Raimundo,
Gusi, & Tomas-Carus, 2009) ou qualidade de vida (Santin-Medeiros, Santos-Lozano, Cristi-
Montero, & Garatachea Vallejo, 2017).
Diferente das modalidades convencionais de exercício físico, na VCI a pessoa
permanece em pé sobre uma placa oscilatória, que transmite vibrações mecânicas por todo
corpo (Rauch et al., 2010). Vários estudos já compararam a VCI com diferentes formas de
intervenção por meio de exercícios físicos sobre variáveis relacionadas à força muscular
(Marín-Cascales, Alcaraz, & Rubio-Arias, 2017; Tapp, & Signorile, 2014; Rees, Murphy, &
Watsford, 2008; Verschueren et al., 2004; Roelants, Delecluse, & Verschueren, 2004).
Na maior parte destes estudos, VCI não se mostrou significativamente diferente de
exercícios convencionais que oferecem fortalecimento muscular, quando levado em
consideração o pico de torque isocinético dos extensores do joelho (Marín-Cascales, Alcaraz,
& Rubio-Arias, 2017; Verschueren et al., 2004; Roelants, Delecluse, & Verschueren, 2004),
podendo ser mais efetiva para aumento da força dos flexores do tornozelo (Rees, Murphy, &
Watsford, 2008), ou menos efetiva quando levado em consideração a força dos membros
superiores (Tapp, & Signorile, 2014). Uma revisão sistemática e meta-análise demonstrou que
VCI possibilita efeitos significativos sobre a força muscular de membros inferiores em adultos
mais velhos, quando comparada a nenhuma intervenção, mas sem diferenças para outras
modalidades de exercícios físicos (Lau et al., 2011).
169
A maior controvérsia nas intervenções envolvendo VCI, refere-se aos diferentes
parâmetros que podem ser utilizados para modificar a intensidade das vibrações, como
frequência, magnitude e tempo de exposição (Rauch et al., 2010). Ainda, a maior parte dos
estudos realizados até o momento, prescreveram exercícios de fortalecimento para os
membros inferiores durante a VCI (Tapp, & Signorile, 2014; Von Stengel et al., 2011; Klarner
et al., 2011, Machado, García-López, González-Gallego, & Garatachea, 2010; Rees, Murphy,
& Watsford, 2008; Verschueren et al., 2004; Roelants, Delecluse, & Verschueren, 2004), o
que suscita dúvidas se os eventuais efeitos sobre a força muscular decorreram das vibrações
mecânicas ou da realização de exercícios de fortalecimento muscular.
Tendo em vista que até o momento, não foram encontrados estudos que tiveram por
objetivo identificar os diferentes efeitos entre Pilates e VCI, sobre a força muscular e qualidade
de vida em mulheres na pós-menopausa, o objetivo deste estudo foi verificar os efeitos de seis
meses de intervenção de Pilates vs. VCI sobre o pico de torque isocinético dos músculos
extensores e flexores do joelho em mulheres na pós-menopausa. Como objetivo secundário
buscamos identificar os efeitos das técnicas sobre a qualidade de vida desta população.
MÉTODOS
Este estudo foi um ensaio clínico randomizado e controlado (registrado em
www.clinicaltrials.gov em 7 de maio de 2016: NCT02769143), que seguiu as recomendações
do CONSORT (Tabela Suplementar 1). O tempo de intervenção teve duração de seis meses e
envolveu 51 mulheres na pós-menopausa (que haviam experimentado a menopausa há no
mínimo um ano), subdivididas em três grupos de igual tamanho. Todas as participantes
estavam aptas para praticarem exercício físico, apresentando idades entre 40 e 70 anos,
residentes na cidade de Jacarezinho, estado do Paraná, Brasil. O presente estudo seguiu as
normas éticas estabelecidas pela Declaração de Helsinki (1975, revisada em 1983) e foi
170
aprovado pelo Comitê de Ética em Seres Humanos da Universidade Norte do Paraná, Brasil
(parecer 1.032.182). Todas as participantes assinaram um Termo de Consentimento Livre e
Esclarecido.
Recrutamento e Participantes
As participantes foram aleatoriamente recrutadas em Maio de 2016, por meio de
cartazes disponibilizados em locais públicos, anúncios em jornais, rádios, sites de notícias da
internet e panfletos deixados em clínicas médicas e unidades de saúde, todos de abrangência
local. O cálculo amostral foi realizado no programa Bioestat 5.3 (Instituto Mamirauá,
Amazonas, Brasil), levando em consideração os valores da força muscular isocinética (N.m)
dos extensores do joelho, na velocidade angular de 60º/s, disponibilizado em estudo anterior
(Oliveira, Oliveira, & Pires-Oliveira, 2017). Neste caso, a média e desvio padrão pós-
intervenção entre o grupo Pilates (101,1 ± 14,1) e grupo controle (81,9 ± 19,6) foi utilizada,
com o poder do teste em 80% e valor alfa em 0,05, que gerou a necessidade de no mínimo 13
participantes em cada grupo. A amostra final foi composta por 17 participantes em cada grupo,
inicialmente, 620 mulheres foram entrevistadas, porem devido os critérios de exclusão, apenas
51 voluntarias foram elegíveis para o estudo.
Os critérios de inclusão foram: a) pós-menopausa há pelo menos 12 meses
clinicamente confirmada; b) não praticar exercício físico a pelo menos seis meses; c) não
iniciar a prática de exercício físico durante o estudo; d) habilidade para realizar atividades da
vida diária sem auxílio (Katz, et al., 1963; Lawton, & Brody, 1969); e) apresentação de
liberação médica indicando aptidão para a prática de exercícios físicos; f) índice de massa
corporal < 30,0 Kg/m2; e g) escore ≥ 19 no Mini Exame do Estado Mental (Folstein, Folstein,
& McHugh, 1975).
171
Os critérios de exclusão foram: a) disfunções musculoesqueléticas na coluna vertebral
ou nos membros inferiores nos últimos seis meses; b) fratura na coluna vertebral ou nos
membros inferiores após os 40 anos de idade; c) próteses nos membros inferiores ou implantes
na coluna vertebral; d) causas secundárias de perda óssea; e) doenças que afetam o
metabolismo ósseo; f) histórico de câncer nos últimos cinco anos; g) alterações vasculares,
epilepsia ou convulsões; h) arritmia; i) uso de marca-passo; j) doenças que afetem a retina; k)
doenças cardiorrespiratórias; l) doenças no sistema neuromuscular; m) labirintite ou vertigens;
n) hospitalização nos últimos seis meses por motivos cirúrgicos; o) alteração da tireóide; p)
fumante; q) uso frequente de bebidas alcoólicas; r) uso de suplementos a base de cálcio,
vitamina D, isoflavona, medicações para aumento da densidade mineral óssea ou massa
muscular nos últimos 12 meses.
Todas as participantes incluídas no presente estudo foram orientadas a manter sua
rotina habitual, suas atividades de vida diária (ex., limpar a casa ou lavar a louça) e hábitos
nutricionais. Também foram instruídas a não usar medicações ou suplementos que pudessem
influenciar na massa óssea ou muscular durante o período do estudo.
Avaliação da força muscular
Para avaliar a força muscular dos extensores e flexores do joelho foi utilizado um
dinamômetro isocinético (Biodex System 4.0, Biodex Medical Systems, Shirley, NY, USA).
Todos os procedimentos foram realizados por um avaliador independente, não envolvido
diretamente com o projeto de pesquisa, experiente em avaliação isocinética e cego em relação
a alocação das voluntárias em cada grupo. O equipamento foi previamente calibrado
antecedendo o teste conforme as normas do fabricante. Precedendo ao teste, as participantes
realizaram um aquecimento durante cinco minutos em bicicleta ergométrica vertical,
utilizando carga leve (25 watts) e velocidade confortável (50 rotações por minuto). Na
172
sequência, o avaliador posicionou a participante no equipamento, com a articulação do quadril
perfazendo um ângulo de 120º de flexão.
O eixo de rotação do braço do dinamômetro foi alinhado com o epicôndilo lateral do
fêmur do membro inferior dominante. O local da aplicação da força foi posicionado
aproximadamente a dois centímetros do maléolo medial. Cintos foram afixados ao tronco,
pelve e coxa para evitar movimentos compensatórios (Stumbo et al., 2001). Após uma breve
familiarização com o equipamento e amplitude de movimento, as participantes realizaram os
movimentos de extensão e flexão do joelho (concêntrico/concêntrico) na velocidade angular
de 60 graus por segundo (60º/s), iniciando com a posição do joelho em 90 graus de flexão.
Foram realizadas três séries de cinco repetições, com 30 segundos de intervalo entre as séries
(Bottaro, Russo, & de Oliveira, 2005). Em seguida, o mesmo protocolo foi utilizado para
velocidade angular de 180 graus por segundo (180°/s). As participantes foram instruídas a
realizarem a máxima força de contração voluntária dos músculos extensores do joelho, seguida
imediatamente pela máxima contração dos músculos flexores do joelho, continuamente.
Durante a execução do teste a palavra de encorajamento “mais força” foi utilizada de forma
padronizada. A variável considerada para fins de análise foi o pico de torque isocinético,
expresso em newtons por metro (N.m).
Avaliação da qualidade de vida
Para avaliação da qualidade de vida foi utilizada a versão brasileira do questionário
SF-36 (Ciconelli, et al., 1999). Este questionário possui 11 questões e 36 itens, subdivididos
em oito componentes (domínios), representados por capacidade funcional (10 itens), aspectos
físicos (quatro itens), dor (dois itens), estado geral de saúde (cinco itens), vitalidade (quatro
itens), aspectos sociais (dois itens), aspectos emocionais (três itens) e saúde mental (cinco
itens). Os primeiros quatro domínios avaliam a saúde física, enquanto os quatro últimos
173
avaliam a saúde mental. As participantes recebem um escore para cada domínio, que varia de
0 até 100, sendo 0 o pior escore e 100 o melhor (Ware, & Gandek, 1998). O questionário foi
aplicado por um avaliador não diretamente envolvido com o estudo e cego em relação a
alocação das participantes em cada grupo.
Randomização
Após a avaliação da força muscular e qualidade de vida, as participantes foram
submetidas ao processo de randomização (alocação aleatória das participantes em cada um
dos três grupos), realizada por um pesquisador que não fazia parte da equipe deste estudo. Os
números aleatórios foram gerados por um software específico (randomization.com), que
distribuiu as participantes em um dos três grupos: Grupo Pilates (GP), Grupo Vibração (GP);
e Grupo Controle (GC), com 17 participantes em cada. O mesmo pesquisador que realizou o
processo de randomização selou os envelopes escuros contendo o grupo que cada participante
estaria alocada e entregou ao pesquisador principal que esteve sempre cego em relação a
alocação das participantes em cada grupo. As participantes de forma cega receberam
individualmente os envelopes contendo o seu nome. Após romper o lacre do envelope, a
participante verificou junto com o pesquisador principal em qual grupo estaria alocada.
Intervenção
As intervenções ocorreram três vezes por semana em dias não consecutivos por seis
meses (78 sessões), a partir de junho de 2016, em uma clínica particular localizada na cidade
de Jacarezinho, Paraná, Brasil. Os grupos experimentais (GP e GV) foram supervisionados
por duas fisioterapeutas com experiência profissional em Pilates e VCI. Como a intervenção
foi com o exercício físico, não foi possível cegar as participantes e as fisioterapeutas
responsáveis pelas intervenções.
174
Grupo Pilates
A primeira sessão do GP foi utilizada para familiarizar as participantes com a técnica,
fornecendo uma explicação sobre a execução correta de cada movimento e uma melhor
compreensão dos princípios do método. Os seguintes equipamentos foram utilizados para
realizar os exercícios: Cadillac, Reformer, Ladder Barrel, Wall Unit, Cadeira, Step Barrel e
Meia Lua (Figura Suplementar 1) (ISP, Cascavel, PR, Brasil). Vinte e um exercícios de
fortalecimento e alongamento foram selecionados para os principais segmentos corporais: a)
membros inferiores b) flexores, extensores e flexores laterais do tronco; e c) membros
superiores. Dois protocolos de exercício foram aplicados durante os seis meses de intervenção,
cada um realizado por três meses (Tabela Suplementar 2), mantendo a mesma sequencia de
fortalecimento e alongamento, assim como, os mesmos segmentos corporais citados acima;
mas alterando a ordem dos equipamentos. Cada sessão teve duração de 60 minutos.
Todos os exercícios foram realizados em uma série de dez repetições, com um intervalo
de descanso de um minuto entre os exercícios. A intensidade da sobrecarga no Pilates é
determinada principalmente pelo uso de molas, que foi modificada de acordo com a evolução
da força de cada participante (alterando o posicionamento das molas no equipamento ou
trocando a mola para outra de maior resistência) (Melo et al., 2011), mantendo sempre o
número de repetições e série. Para determinar o nível de esforço das participantes e a
consequente evolução da sobrecarga, utilizou-se uma descrição verbal de acordo com a escala
Borg CR10 (Borg, 1982): carga leve (Borg ≤ 2), carga moderada (Borg > 2 e < 5), carga pesada
≥ 5 e < 7), e carga próxima à máxima (Borg ≥ 7). O nível de percepção do esforço mantido
durante as sessões foi pesado (Borg entre 5 e 6). Sempre que a intensidade do exercício foi
alterada, a nova carga utilizada anotada imediatamente em uma ficha individual, utilizada para
registro do treinamento.
175
Grupo vibração
O GV foi exposto a VCI durante cinco minutos em uma plataforma vibratória do tipo
lado alternado (Figura Suplementar 2) (Arktus, Cascavel, PR, Brasil), que oscila por meio de
um eixo ântero-posterior, fazendo com que os lados direito e esquerdo se alternem
horizontalmente. Foi utilizada uma frequência de 20 Hz (1 Hz = 1 oscilação/segundo) e um
deslocamento de pico a pico de 4 mm (com referência ao segundo dedo do pé), resultando em
uma magnitude de 31,5 m/s2 ou 3,2 g (gravidade: 1 g = 9,8 m/s2). As participantes foram
instruídas a ficarem em pé sobre a placa de oscilação da plataforma, com os joelhos semi-
flexionados a 30 graus e os pés descalços espaçados a uma distância de 50 cm, mantendo o
tronco ereto e segurando o suporte da plataforma com as duas mãos. Não foram colocados
acessórios (como um tapete de EtilenoVinil Acetato [EVA]) sobre a placa oscilante da
plataforma para amortecer os impactos. Todos os parâmetros utilizados no equipamento e o
posicionamento das participantes foram mantidos ao longo dos seis meses de intervenção. Um
teste de derrapagem assegurou que os pés das participantes permaneciam sempre em contato
com a placa oscilante durante a VCI (Rauch, et al., 2010).
Grupo controle
O GC não realizou nenhum tipo de intervenção. A fisioterapeuta responsável pelo
estudo contactou as participantes do GC todos os meses durante a intervenção, para enfatizar
a importância de manter a rotina usual relacionada à atividade física, aos hábitos alimentares,
em relação a importância da não utilização de suplementos ou medicamentos que pudessem
afetar a massa óssea ou muscular e não iniciar nenhum tipo de exercício físico, conforme
procedimento também adotado com o GP e GV. Neste momento, as participantes também
foram questionadas sobre possíveis eventos adversos.
176
Eventos adversos
Um formulário padronizado foi utilizado para registrar ocorrências de eventos adversos
nos três grupos. As participantes foram questionadas todos os meses sobre qualquer
complicação, como espasmos ou dores musculares, dores nas articulações, tonturas, quedas,
cãimbras e mudanças na pressão arterial.
Análise estatística
Os dados paramétricos são apresentados como média e o respectivo desvio padrão
(DP), enquanto os não paramétricos como mediana e o respectivo intervalo interquartil
(percentis 25 e 75). A normalidade dos dados foi verificada pelo teste de Shapiro-Wilk. O teste
t de Student para amostras independentes foi utilizado para comparar o número de ausências
das participantes durante as intervenções (GP vs. GV). A homogeneidade das variâncias foi
determinada pelo teste de Levene. Para verificar se os três grupos apresentavam diferenças na
pré-intervenção, análise de variância unidirecional (ANOVA one-way) foi utilizada para
dados com distribuição normal (idade, peso, altura, IMC e força muscular isocinética). Caso
contrário, foi utilizado o teste de Kruskal-Wallis (tempo de menopausa e qualidade de vida).
Para verificar as diferenças intragrupo entre a pré e a pós-intervenção foi utilizado o teste t de
Student para amostras dependentes (força muscular isocinética) ou teste de Wilcoxon
(qualidade de vida). Para verificar as diferenças entre os grupos para a força muscular
isocinética, foi aplicada a análise de covariância (ANCOVA), com os dados da pós-
intervenção utilizados como variáveis dependentes e os dados da pré-intervenção como
covariáveis de ajustamento. Como post hoc foi utilizado teste de Bonferroni visando verificar
as comparações múltiplas entre os pares (GP vs. GV, GP vs. GC e GV vs. GC). Para as
variáveis de força muscular isocinética, os tamanhos de efeito das intervenções intragrupo e
inter-grupos foram calculados usando Cohen's d, que foi considerado pequeno (0,20), médio
177
(0,50) ou grande (0,80) (Cohen, 1988). Para verificar as diferenças inter-grupos para a
qualidade de vida após as intervenções, foi utilizado teste de Kruskal-Wallis. Inicialmente,
utilizou-se análise por intenção de tratar (ITT), incluindo todas as participantes randomizadas
(os dados faltantes para a pós-intervenção de duas participantes do GC foram imputados pela
média do grupo). Posteriormente, uma análise por protocolo foi realizada, excluindo as duas
participantes do GC que abandonaram o estudo. Como os resultados foram semelhantes,
apenas análise de ITT é apresentada nos resultados deste estudo. Para todos os testes, o nível
de significância adotado foi de 95% (p < 0,05). As análises foram processadas no programa
SPSS 20.0 (Chicago, IL, EUA), exceto para os cálculos de tamanho de efeito (Cohen's d), que
foram processados no programa GPower 3.1 (Franz Faul, Universita Ä Kiel, Alemanha).
RESULTADOS
Aderência
Das 51 participantes inicialmente randomizadas, 49 (96,1%) completaram o
seguimento. Duas participantes do GC abandonaram o estudo (uma começou a praticar
exercício físico e a outra fez uso de suplemento a base de cálcio) (Figura 1). O número de
ausências das participantes não diferiu significativamente entre os grupos experimentais (p =
0,558), a variação foi de 0 a 14 (5,76 ± 4,07) para o GP e 0 a 17 (6,76 ± 5,65) para o GV.
Assim, a frequência média nos dois grupos foi de 92,6% e 91,3%, respectivamente (Tabela
Suplementar 3).
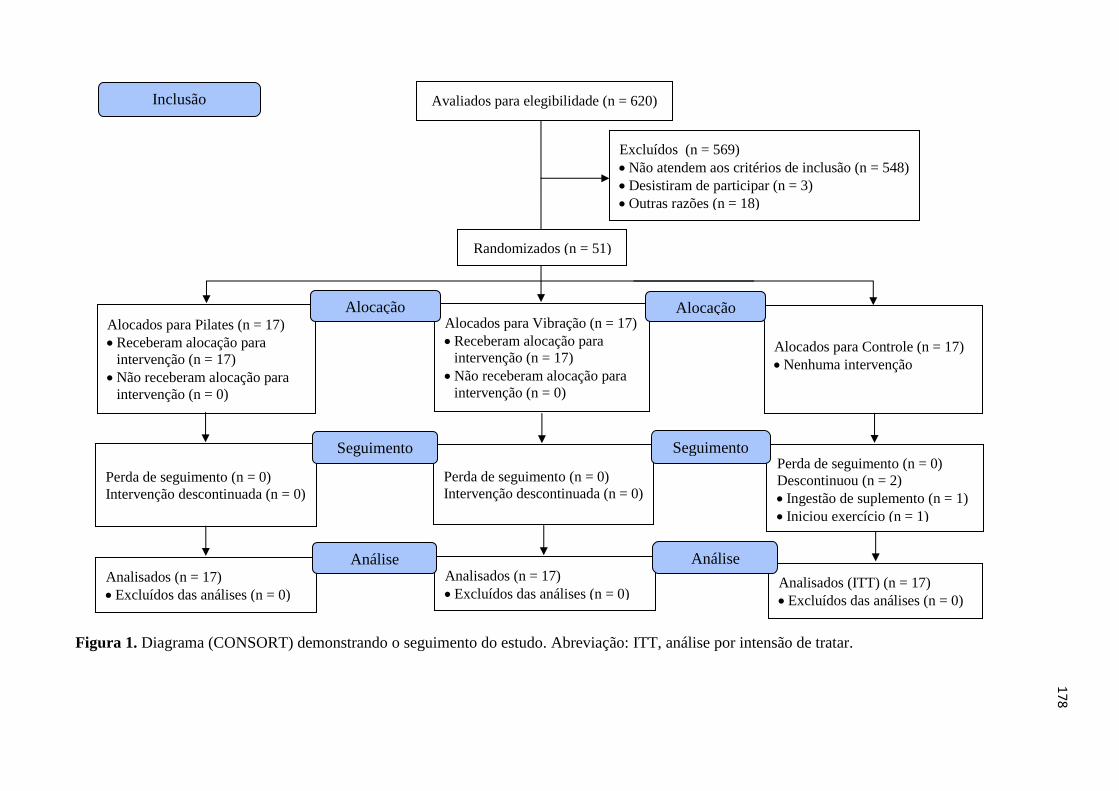
178
Figura 1. Diagrama (CONSORT) demonstrando o seguimento do estudo. Abreviação: ITT, análise por intensão de tratar.
Analisados (n = 17)
• Excluídos das análises (n = 0)
Perda de seguimento (n = 0)
Descontinuou (n = 2)
• Ingestão de suplemento (n = 1)
• Iniciou exercício (n = 1)
Avaliados para elegibilidade (n = 620)
Excluídos (n = 569)
• Não atendem aos critérios de inclusão (n = 548)
• Desistiram de participar (n = 3)
• Outras razões (n = 18)
Analisados (n = 17)
• Excluídos das análises (n = 0)
Perda de seguimento (n = 0)
Intervenção descontinuada (n = 0)
Alocados para Pilates (n = 17)
• Receberam alocação para
intervenção (n = 17)
• Não receberam alocação para
intervenção (n = 0)
Alocados para Vibração (n = 17)
• Receberam alocação para
intervenção (n = 17)
• Não receberam alocação para
intervenção (n = 0)
Alocação
Análise
Randomizados (n = 51)
Inclusão
Alocados para Controle (n = 17)
• Nenhuma intervenção
Alocação
Perda de seguimento (n = 0)
Intervenção descontinuada (n = 0)
Seguimento Seguimento
Analisados (ITT) (n = 17)
• Excluídos das análises (n = 0)
Análise
179
Características iniciais
A Tabela 1 mostra as características iniciais das participantes. A idade, variáveis
antropométricas, tempo da menopausa e os domínios do questionário SF-36 foram
semelhantes nos três grupos (p > 0,05). Entre as variáveis da força muscular isocinética, o pico
de torque a 180º/s, dos músculos extensores do joelho foi significativamente diferente entre
os grupos (p = 0,037), no qual análise post hoc de Bonferroni demonstrou que o GP foi superior
ao GV (p = 0,032). Para as demais variáveis de força muscular isocinética, os grupos foram
semelhantes no início do estudo (p > 0,05).
Força Muscular
A Tabela 2 apresenta os resultados da força muscular isocinética dos extensores e
flexores do joelho a 60º/s e 180º/s, intragrupo e inter-grupos. Na comparação intragrupo, o GP
apresentou uma melhora significativa (p < 0,05) para todas as variáveis analisadas, com
tamanho de efeito moderado (Cohen's d entre 0,50 e 0,80) para os músculos extensores do
joelho e grande tamanho de efeito (Cohen's d > 0,80) para os músculos flexores do joelho. Na
comparação inter-grupos, o GP foi significativamente (p < 0,05) superior ao GC para todas as
variáveis analisadas, com grande tamanho de efeito (Cohen's d > 0,80), exceto o pico de torque
isocinético dos extensores do joelho a 60º/s, que apresentou tamanho de efeito moderado
(Cohen's d = 0,78). Ainda, o GP foi significativamente (p < 0,05) superior ao GV para o pico
de torque isocinético dos flexores do joelho a 60º/s, com tamanho de efeito moderado (Cohen's
d = 0,70). Apesar de não significativo (p > 0,05), o GP apresentou grande tamanho de efeito
(Cohen's d = 1,00) comparado ao GV, para o pico de torque isocinético dos flexores do joelho
a 180º/s. A Tabela Suplementar 4 apresenta detalhes da análise post hoc para força muscular
isocinética.
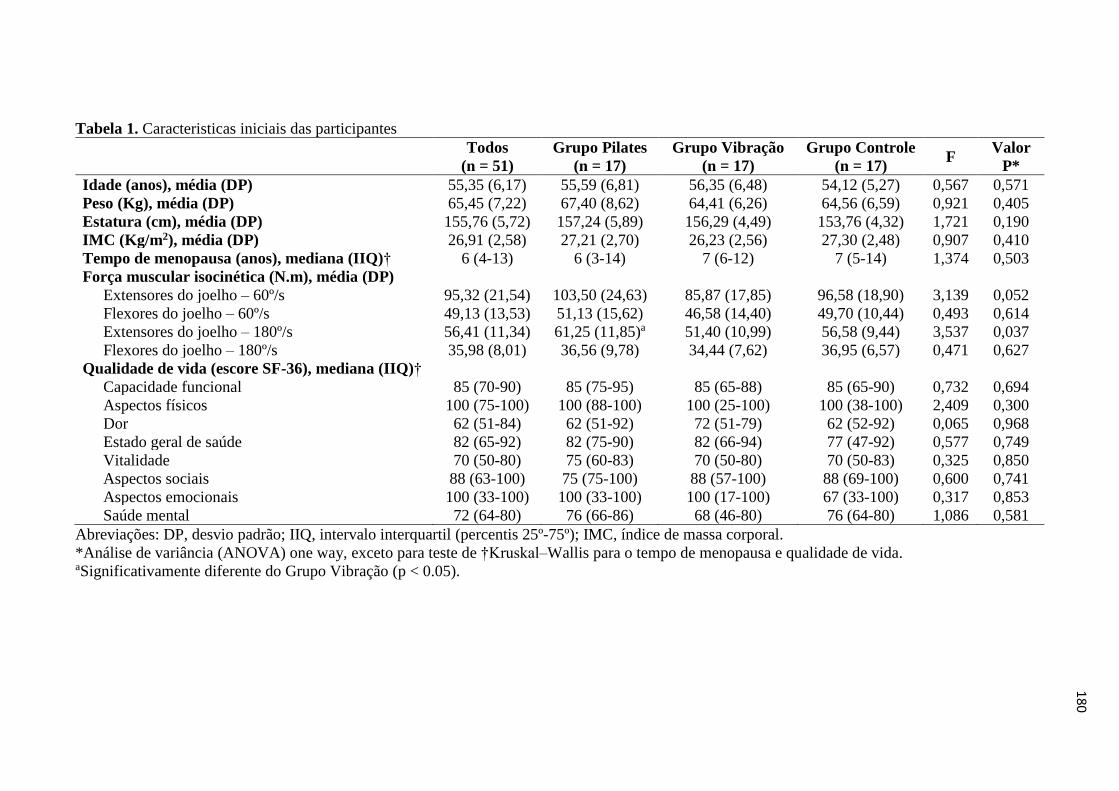
180
Tabela 1. Caracteristicas iniciais das participantes
Todos
(n = 51)
Grupo Pilates
(n = 17)
Grupo Vibração
(n = 17)
Grupo Controle
(n = 17) F
Valor
P*
Idade (anos), média (DP) 55,35 (6,17) 55,59 (6,81) 56,35 (6,48) 54,12 (5,27) 0,567 0,571
Peso (Kg), média (DP) 65,45 (7,22) 67,40 (8,62) 64,41 (6,26) 64,56 (6,59) 0,921 0,405
Estatura (cm), média (DP) 155,76 (5,72) 157,24 (5,89) 156,29 (4,49) 153,76 (4,32) 1,721 0,190
IMC (Kg/m2), média (DP) 26,91 (2,58) 27,21 (2,70) 26,23 (2,56) 27,30 (2,48) 0,907 0,410
Tempo de menopausa (anos), mediana (IIQ)† 6 (4-13) 6 (3-14) 7 (6-12) 7 (5-14) 1,374 0,503
Força muscular isocinética (N.m), média (DP)
Extensores do joelho – 60º/s 95,32 (21,54) 103,50 (24,63) 85,87 (17,85) 96,58 (18,90) 3,139 0,052
Flexores do joelho – 60º/s 49,13 (13,53) 51,13 (15,62) 46,58 (14,40) 49,70 (10,44) 0,493 0,614
Extensores do joelho – 180º/s 56,41 (11,34) 61,25 (11,85)a 51,40 (10,99) 56,58 (9,44) 3,537 0,037
Flexores do joelho – 180º/s 35,98 (8,01) 36,56 (9,78) 34,44 (7,62) 36,95 (6,57) 0,471 0,627
Qualidade de vida (escore SF-36), mediana (IIQ)†
Capacidade funcional 85 (70-90) 85 (75-95) 85 (65-88) 85 (65-90) 0,732 0,694
Aspectos físicos 100 (75-100) 100 (88-100) 100 (25-100) 100 (38-100) 2,409 0,300
Dor 62 (51-84) 62 (51-92) 72 (51-79) 62 (52-92) 0,065 0,968
Estado geral de saúde 82 (65-92) 82 (75-90) 82 (66-94) 77 (47-92) 0,577 0,749
Vitalidade 70 (50-80) 75 (60-83) 70 (50-80) 70 (50-83) 0,325 0,850
Aspectos sociais 88 (63-100) 75 (75-100) 88 (57-100) 88 (69-100) 0,600 0,741
Aspectos emocionais 100 (33-100) 100 (33-100) 100 (17-100) 67 (33-100) 0,317 0,853
Saúde mental 72 (64-80) 76 (66-86) 68 (46-80) 76 (64-80) 1,086 0,581
Abreviações: DP, desvio padrão; IIQ, intervalo interquartil (percentis 25º-75º); IMC, índice de massa corporal.
*Análise de variância (ANOVA) one way, exceto para teste de †Kruskal–Wallis para o tempo de menopausa e qualidade de vida. aSignificativamente diferente do Grupo Vibração (p < 0.05).
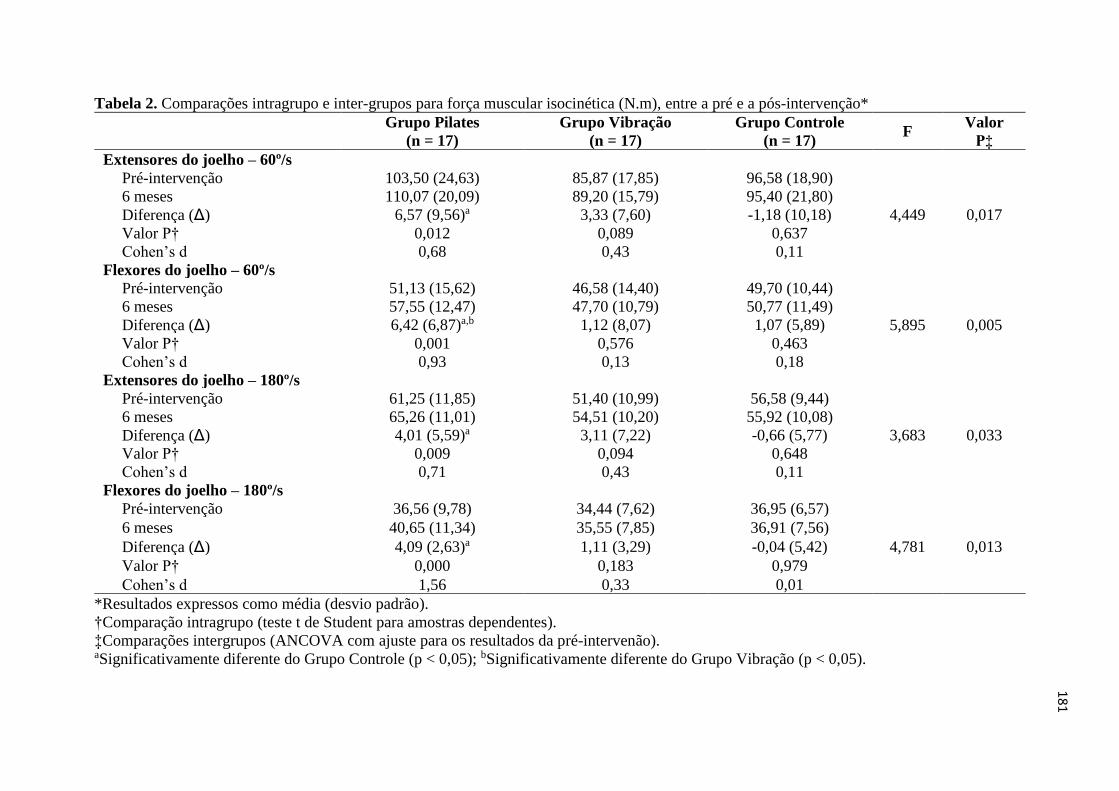
181
Tabela 2. Comparações intragrupo e inter-grupos para força muscular isocinética (N.m), entre a pré e a pós-intervenção*
Grupo Pilates
(n = 17)
Grupo Vibração
(n = 17)
Grupo Controle
(n = 17) F
Valor
P‡
Extensores do joelho – 60º/s
Pré-intervenção 103,50 (24,63) 85,87 (17,85) 96,58 (18,90)
4,449 0,017
6 meses 110,07 (20,09) 89,20 (15,79) 95,40 (21,80)
Diferença (Δ) 6,57 (9,56)a 3,33 (7,60) -1,18 (10,18)
Valor P† 0,012 0,089 0,637
Cohen’s d 0,68 0,43 0,11
Flexores do joelho – 60º/s
Pré-intervenção 51,13 (15,62) 46,58 (14,40) 49,70 (10,44)
5,895 0,005
6 meses 57,55 (12,47) 47,70 (10,79) 50,77 (11,49)
Diferença (Δ) 6,42 (6,87)a,b 1,12 (8,07) 1,07 (5,89)
Valor P† 0,001 0,576 0,463
Cohen’s d 0,93 0,13 0,18
Extensores do joelho – 180º/s
Pré-intervenção 61,25 (11,85) 51,40 (10,99) 56,58 (9,44)
3,683 0,033
6 meses 65,26 (11,01) 54,51 (10,20) 55,92 (10,08)
Diferença (Δ) 4,01 (5,59)a 3,11 (7,22) -0,66 (5,77)
Valor P† 0,009 0,094 0,648
Cohen’s d 0,71 0,43 0,11
Flexores do joelho – 180º/s
Pré-intervenção 36,56 (9,78) 34,44 (7,62) 36,95 (6,57)
4,781 0,013
6 meses 40,65 (11,34) 35,55 (7,85) 36,91 (7,56)
Diferença (Δ) 4,09 (2,63)a 1,11 (3,29) -0,04 (5,42)
Valor P† 0,000 0,183 0,979
Cohen’s d 1,56 0,33 0,01
*Resultados expressos como média (desvio padrão).
†Comparação intragrupo (teste t de Student para amostras dependentes).
‡Comparações intergrupos (ANCOVA com ajuste para os resultados da pré-intervenão). aSignificativamente diferente do Grupo Controle (p < 0,05); bSignificativamente diferente do Grupo Vibração (p < 0,05).
182
Qualidade de vida
A Figura 2 e a Tabela Suplementar 5 apresentam os resultados da qualidade de vida,
medida pelo questionário SF-36, intragrupo e inter-grupos. Na comparação intragrupo, o GP
apresentou melhora significativa (p < 0,05) para os domínios: capacidade funcional, dor,
vitalidade, aspectos sociais e saúde mental; enquanto o GV apresentou melhora significativa
(p < 0,05) para os domínios: estado geral de saúde, vitalidade e saúde mental. Por outro lado,
o GC mostrou uma diminuição significativa (p < 0,05) para dois domínios: dor e aspectos
sociais. Na comparação inter-grupos, o GP foi significativamente (p < 0,05) superior ao GC
para os domínios: aspectos físicos, dor, aspectos sociais e aspectos emocionais. A Tabela
Suplementar 6 apresenta detalhes da análise post hoc para a qualidade de vida.
Eventos adversos
Eventos adversos graves foram relatados nos três grupos: duas quedas no GP e outras
duas no GV; e uma queda no GC que levou a fratura do punho. Os relatos de dor ocorreram
principalmente no GP e GV. A principal queixa das participantes foi dor muscular tardia,
relatada pelo GP (100%) e GV (58,8%), principalmente nas primeiras semanas de intervenção.
Outros eventos adversos menos graves, como dor em regiões específicas do corpo, espasmos
musculares e cãimbras ocorreram com menos freqüência (Tabela Suplementar 7).
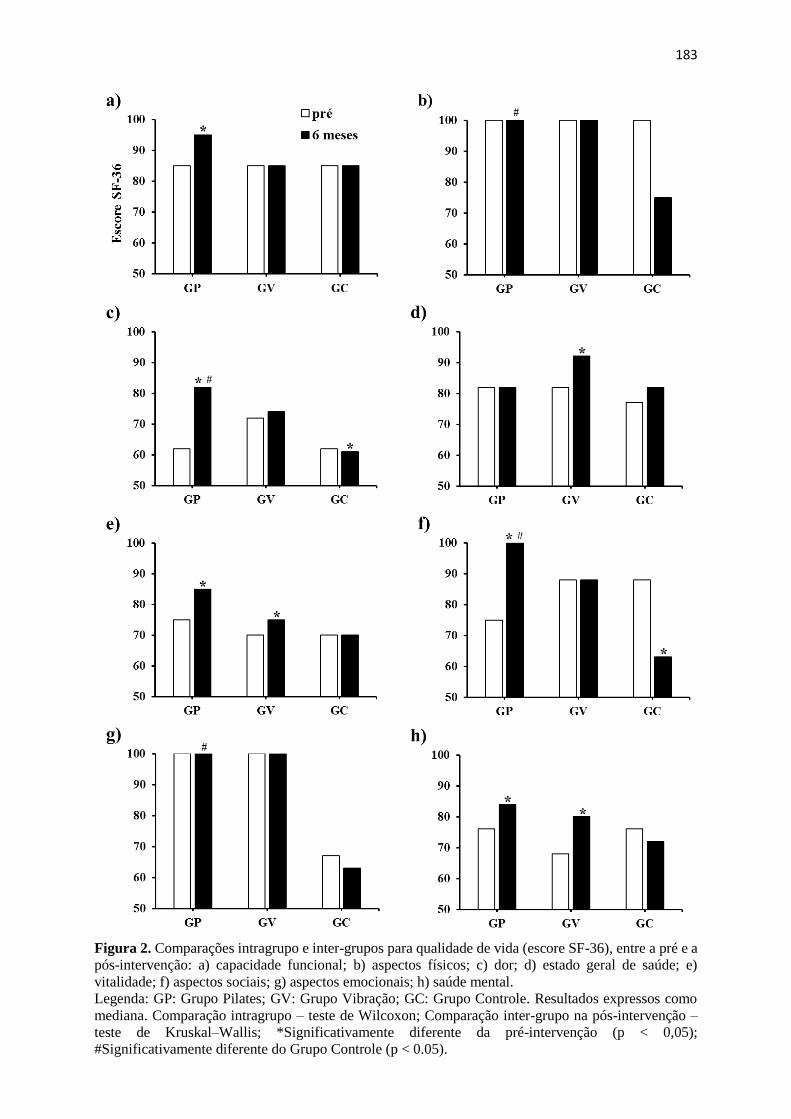
183
Figura 2. Comparações intragrupo e inter-grupos para qualidade de vida (escore SF-36), entre a pré e a
pós-intervenção: a) capacidade funcional; b) aspectos físicos; c) dor; d) estado geral de saúde; e)
vitalidade; f) aspectos sociais; g) aspectos emocionais; h) saúde mental.
Legenda: GP: Grupo Pilates; GV: Grupo Vibração; GC: Grupo Controle. Resultados expressos como
mediana. Comparação intragrupo – teste de Wilcoxon; Comparação inter-grupo na pós-intervenção –
teste de Kruskal–Wallis; *Significativamente diferente da pré-intervenção (p < 0,05);
#Significativamente diferente do Grupo Controle (p < 0.05).
184
DISCUSSÃO
Resumo dos principais resultados
Este estudo teve por objetivo verificar os efeitos do método Pilates e VCI, sobre a força
muscular isocinética dos extensores e flexores do joelho e qualidade de vida em mulheres na
pós-menopausa. Após seis meses de intervenção, Pilates foi superior (p < 0.05) à VCI apenas
para força muscular dos flexores do joelho à 60º/s. Nas comparações com o grupo controle,
Pilates foi superior (p < 0.05) em todas as variáveis de força muscular e em quatro domínios
do SF-36. Comparações intragrupo demonstram que Pilates possibilitou aumento para todas
as variáveis de força muscular e cinco domínios da qualidade de vida, enquanto VCI
possibilitou aumento para três domínios da qualidade de vida.
Força muscular
Coincidindo com os achados do presente estudo, outras pesquisas identificaram
melhora significativa da força muscular de membros inferiores após intervenção com o
método Pilates em mulheres mais velhas, nas comparações intragrupo ou com grupos controle.
Oliveira, Oliveira, & Pires-Oliveira (2017) avaliaram o pico de torque isocinético dos
extensores e flexores do joelho a 60º/s, enquanto Campos de Oliveira, Gonçalves de Oliveira,
& Pires-Oliveira (2015) testaram a velocidade de 300º/s. Após 12 semanas de Pilates, ambos
os estudos identificaram melhora significativa para as variáveis analisadas. Com o mesmo
tempo de intervenção, Vieira et al. (2017) e Bergamin et al. (2015) observaram melhora
significativa da força muscular de membros inferiores por intermédio do teste de sentar e
levantar da cadeira, enquanto Plachy, Kovách, & Bognár (2012) identificaram melhora
significativa para este mesmo teste, após seis meses de intervenção com Pilates. Irez et al.
(2011) verificaram melhora significativa da força muscular dos flexores, adutores e abdutores
do quadril após 12 semanas de Pilates.
185
Além disso, meta-análise que agrupou os diferentes estudos que aplicaram o método
Pilates como forma de intervenção, identificou que a técnica possibilita um grande tamanho
de efeito (d = 1.23) sobre a força muscular de adultos mais velhos. Isoladamente, Bird, Hill,
& Fell (2012) não identificaram melhora significativa da força muscular dos extensores do
joelho e dorsiflexores do tornozelo em adultos mais velhos, para o teste de uma repetição
máxima, após seis semanas de Pilates. Possivelmente a falta de resultados significativos possa
ser explicada pelo tempo de intervenção (seis semanas). Todos os demais estudos que
identificaram resultados significativos para força muscular de adultos mais velhos, realizaram
no mínimo 12 semanas de intervenção.
Em relação a VCI, nossos resultados demonstraram que a técnica não foi efetiva para
aumento do pico de torque isocinético dos extensores e flexores do joelho, tanto intra-grupo,
como comparada ao grupo controle, corroborando com alguns achados da literatura, que
investigaram os efeitos desta técnica em mulheres na pós-menopausa. Liphardt, Schipilow,
Hanley, & Boyd (2015) utilizaram VCI em plataforma de lado alternado à 20 Hz, amplitude
de pico a pico de 3 a 4 mm, com as participantes em posição de semi-flexão do joelho à 30º,
por 10 minutos. Após 12 meses de intervenção, os autores não identificaram melhora
significativa para força muscular isocinética dos extensores do joelho. Raimundo, Gusi, &
Tomas-Carus (2009) utilizaram VCI em plataforma lado-alternado à 12,6 Hz, amplitude pico
a pico de 3 mm, em posição de flexão do joelho à 120º, por 3 minutos. Após oito meses de
intervenção, nenhum resultado significativo foi observado para força muscular isocinética dos
extensores do joelho à 60º/s e 300º/s. Exceção foi o estudo de Wei, Pang, Ng, & Ng (2016)
que realizou a vibração síncrona em três diferentes frequências, 20, 40 e 60 Hz, com tempo de
exposição respectivamente de 12, 6 e 4 minutos, amplitude pico a pico de 4 mm, com semi-
flexão do joelho à 60º. Após 12 semanas de intervenção, foi observada melhora significativa
186
para força muscular isocinética dos extensores do joelho à 60º/s e 180º/s, mas apenas para o
grupo que realizou VCI à 40 Hz.
Contudo, os estudos que associaram exercícios de fortalecimento muscular para os
membros inferiores durante a VCI, observaram que a técnica pode ser efetiva para aumento
da força muscular em mulheres na pós-menopausa. Von Stengel et al. (2011) ao utilizarem
vibração síncrona (35 Hz, amplitude pico a pico de 1,7 mm) e vibração lado alternado (12,5
Hz, amplitude pico a pico de 12 mm), com tempo de exposição de 15 minutos, verificaram
após 12 semanas de intervenção que os dois tipos de vibração possibilitaram melhora
significativa da força muscular isométrica dos extensores do joelho à 100º/s. Verschueren et
al. (2004) ao utilizarem vibração síncrona entre 35 a 40 Hz, amplitude de pico a pico de 1,7 a
2,5 mm, por 30 minutos, identificaram após seis meses de intervenção, melhora significativa
para força muscular isométrica e isotônica dos extensores do joelho.
Uma meta-análise demonstrou que VCI comparada a nenhuma intervenção, possibilita
efeitos significativos sobre a força muscular de membros inferiores em adultos mais velhos
(Lau et al., 2011). No entanto, os autores não realizaram análises de subgrupo considerando
isoladamente estudos que realizaram exercícios de fortalecimento muscular durante a VCI,
assim como para as diferentes frequências, magnitudes, tipos de vibração ou tempo de
exposição.
A realização de exercícios dinâmicos durante a VCI, pode configurar-se como uma
importante variável moderadora para ganho de força muscular. Outro estudo de meta-análise
envolvendo diferentes populações, demonstrou que nas intervenções com VCI para as quais
os participantes associam contrações musculares dinâmicas e isométricas, o ganho de força
muscular é quase o dobro ao ser comparado com as intervenções que utilizam à contração
isométrica isoladamente (como permanecer com o joelho semi-fletido). Foi demonstrado
ainda, que as plataformas síncronas foram mais efetivas para ganho de força muscular, quando
187
comparadas com as plataformas do tipo lado alternado (Marín, & Rhea, 2010), o que pode
justificar a não obtenção de resultados significativos para esta variável, no grupo de
participantes do presente estudo que realizou VCI.
Na pesquisa atual, quando comparados VCI e Pilates, uma diferença significativa (p <
0,05) foi observada apenas para o pico de torque isocinético dos flexores do joelho a 60º/s, em
que Pilates foi superior, com moderado tamanho de efeito (d = 0,70). Para os flexores do joelho
à 180º/s, apesar de não ter havido diferença significativa (p > 0,05), Pilates apresentou grande
tamanho de efeito (d = 1,00) quando comparado à VCI, o que demonstra representatividade
clínica do tratamento. Para o nosso conhecimento, nenhum estudo até o momento, comparou
os efeitos da VCI com qualquer outra forma de exercício físico, sobre o pico de torque
isocinético dos flexores do joelho, o que necessita ser melhor investigado.
O presente estudo não encontrou diferenças significativas entre VCI e Pilates para o
pico de torque isocinético dos extensores do joelho à 60º/s e 180º/s. Outros ensaios clínicos
randomizados que compararam VCI com diferentes formas de exercício físico, também não
identificaram diferenças significativas para a força muscular isocinética dos extensores do
joelho, em mulheres na pós-menopausa (Marín-Cascales, Alcaraz, & Rubio-Arias, 2017;
Verschueren et al., 2004; Roelants, Delecluse, & Verschueren, 2004). Além disso, meta-
análise que comparou os efeitos da VCI com diferentes formas de exercício físico, não
encontrou diferenças significativas entre as técnicas, para força dinâmica de extensão do
joelho, força de extensão isométrica da perna, salto vertical, ou sentar e levantar da cadeira
(Lau et al., 2011).
Qualidade de vida
Em relação a qualidade de vida, no presente estudo, melhoras significativas intragrupo
foram observadas para cinco domínios (capacidade funcional, dor, vitalidade, aspectos sociais
188
e saúde mental) no GP. Nas comparações intergrupos, o GP foi superior ao GC em quatro
domínios (aspectos físicos, dor, aspectos sociais e aspectos emocionais) do questionário SF-
36. Observa-se que o método Pilates foi eficiente para melhora da qualidade de vida em
componentes relacionados a saúde física e saúde mental. Apenas o domínio estado geral de
saúde não apresentou qualquer diferença no GP (levando em consideração as análises
intragrupo ou intergrupos).
Outros estudos que utilizaram este mesmo questionário em mulheres na pós-
menopausa, verificaram após 12 semanas de Pilates, melhora significativa intragrupo para
todos os domínios da qualidade de vida (Campos de Oliveira, Gonçalves de Oliveira, & Pires-
Oliveira, 2015; Rodríguez-Fuentes, Oliveira, & Otero-Gargamala, 2014; Küçükçakır, Altan,
& Korkmaz, 2013). Ainda, nas comparações com grupos controle, Campos de Oliveira,
Gonçalves de Oliveira, & Pires-Oliveira (2015) observaram melhorara em seis domínios do
questionário, enquanto Küçükçakır, Altan, & Korkmaz (2013) verificaram melhora em todos
os oito domínios.
Estudos que utilizaram outros modelos de questionário para qualidade de vida,
identificaram melhora significativa após a prática de Pilates, intragrupo e comparado ao grupo
controle. Angın, Erden, & Can (2015) constataram melhora em todos os domínios do
questionário QUALEFFO-41, em mulheres na pós-menopausa após seis meses de Pilates.
Siqueira Rodrigues et al. (2010) verificaram após oito semanas de intervenção com o método,
melhora para o índice geral de qualidade de vida, mensurada pelo questionário WHOQOL-
OLD, em mulheres mais velhas. Por outro lado, o estudo de Kovách et al. (2013) ao utilizar
este mesmo questionário, identificou melhora intragrupo em apenas um domínio (percepção)
e piora em outro (autonomia), após seis meses de Pilates em adultos mais velhos.
Possivelmente este último, foi um resultado isolado, tendo em vista que uma meta-análise, ao
sumarizar os resultados de diferentes estudos, que tiveram por objetivo observar os efeitos do
189
Pilates sobre a qualidade de vida em adultos mais velhos, verificou que a técnica possibilita
um grande tamanho de efeito (d = 0.94) para esta variável (Bullo et al., 2015).
Em relação a VCI, no estudo atual, uma melhora significativa foi observada para três
domínios do questionário SF-36 na comparação intragrupo, sendo um componente
relacionado à saúde física (estado geral de saúde) e dois relacionados a saúde mental
(vitalidade e saúde mental). Quando comparado ao GC, nenhuma diferença significativa foi
observada a favor do GV. Poucos estudos até o momento observaram os efeitos da VCI sobre
a qualidade de vida em adultos mais velhos. Os estudos de Furness, & Maschette (2009) e
Bruyere et al. (2005) identificaram que seis semanas de VCI, foram suficientes para promover
melhora significativa para todos os domínios do SF-36, intragrupo e comparada ao grupo
controle, respectivamente. Contudo, Santin-Medeiros, Santos-Lozano, Cristi-Montero, &
Garatachea Vallejo (2017) após oito meses de VCI, não observaram diferenças para qualquer
domínio do SF-36, intragrupo e comparada ao controle.
Destaca-se que no presente estudo, não houve diferenças significativas nas
comparações entre VCI e Pilates, para os domínios da qualidade de vida mensurados pelo SF-
36. Tendo em vista que poucos estudos até o momento observaram os efeitos da VCI sobre a
qualidade de vida de mulheres na pós-menopausa, e que nenhum estudo comparou a técnica
com outra forma de exercício físico, mais estudos devem ser realizados, para que
extrapolações seguras dos resultados aqui demonstrados possam ser realizadas.
Pontos fortes e limitações
Este foi o primeiro estudo que buscou identificar os efeitos do Pilates, comparado a
VCI, sobre a força muscular e qualidade de vida em mulheres na pós-menopausa. Ainda, para
o nosso conhecimento, este foi o primeiro estudo que investigou os efeitos da VCI sobre o
pico de torque isocinético dos flexores do joelho em mulheres na pós-menopausa. Outro ponto
190
forte que merece destaque, refere-se a aderência das participantes a intervenção, com
abandono de apenas duas voluntárias do grupo controle, assim como, a taxa de frequência que
foi superior a 90% nos dois grupos de intervenção. Como limitação, por se tratar de
intervenção envolvendo exercício físico, não foi possível mascarar as participantes e as
profissionais que ministraram as intervenções.
CONCLUSÃO
Pilates foi superior a VCI sobre o pico de torque isocinético dos flexores do joelho em
mulheres na pós-menopausa, enquanto nenhuma diferença entre as técnicas foi observada para
o pico de torque isocinético dos extensores do joelho e qualidade de vida. Apenas Pilates foi
superior a nenhuma intervenção, sobre as variáveis do pico de torque isocinético dos
extensores e flexores do joelho, e para quatro dos oito domínios do questionário SF-36.
REFERÊNCIAS
Angın, E., Erden, Z., & Can, F. (2015). The effects of clinical pilates exercises on bone mineral
density, physical performance and quality of life of women with postmenopausal
osteoporosis. Journal of Back and Musculoskeletal Rehabilitation, 28(4), 849-858. doi:
10.3233/BMR-150604.
Bergamin, M., Gobbo, S., Bullo, V., Zanotto, T., Vendramin, B., Duregon, F., Cugusi, L.,
Camozzi, V., Zaccaria, M., Neunhaeuserer, D., & Ermolao, A. (2015). Effects of a
Pilates exercise program on muscle strength, postural control and body composition:
results from a pilot study in a group of post-menopausal women. Age, 37(6), 118. doi:
10.1007/s11357-015-9852-3.
191
Bird, M. L., & Fell, J. (2014). Positive long-term effects of Pilates exercise on the aged-related
decline in balance and strength in older, community-dwelling men and women. Journal
of Aging and Physical Activity, 22(3), 342-347. doi: 10.1123/japa.2013-0006.
Bird., M. L., Hill., K. D., & Fell., J. W. (2012). A randomized controlled study investigating
static and dynamic balance in older adults after training with Pilates. Archives of
Physical Medicine and Rehabilitation, 93(1), 43-49. doi: 10.1016/j.apmr.2011.08.005.
Borg, G. A. V. (1982). Psychophysical bases of perceived exertion. Medicine and Science in
Sports and Exercise, 14(5), 377-381.
Bottaro M, Russo AF, & de Oliveira RJ. (2005). The effects of rest interval on quadriceps
torque during an isokinetic testing protocol in elderly. Journal of Sports Science &
Medicine, 4(3), 285-290.
Bruyere, O., Wuidart, M. A., Di Palma, E., Gourlay, M., Ethgen, O., Richy, F., & Reginster,
J. Y. (2005). Controlled whole body vibration to decrease fall risk and improve health-
related quality of life of nursing home residents. Archives of Physical Medicine and
Rehabilitation, 86(2), 303-307. doi: 10.1016/j.apmr.2004.05.019.
Bullo, V., Bergamin, M., Gobbo, S., Sieverdes, J. C., Zaccaria, M., Neunhaeuserer, D., &
Ermolao, A. (2015). The effects of Pilates exercise training on physical fitness and
wellbeing in the elderly: A systematic review for future exercise prescription. Preventive
Medicine, 75, 1-11. doi: 10.1016/j.ypmed.2015.03.002.
Campos de Oliveira, L., Gonçalves de Oliveira, R., & Pires-Oliveira, D.A.A. (2015). Effects
of Pilates on muscle strength, postural balance and quality of life of older adults: a
randomized, controlled, clinical trial. Journal of Physical Therapy Science, 27(3), 871-
876. doi: 10.1589/jpts.27.871.
192
Ciconelli, R. M., Ferraz, M. B., Santos, W., Meinão, I., & Quaresma, M. R. (1999). Brazilian-
Portuguese version of the SF-36. A reliable and valid quality of life outcome measure.
Revista Brasileira de Reumatologia, 39(3), 143-50.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale:
Lawrence Erlbaum Associates.
Dutra, M. C., de Oliveira, M. L., Marin, R. V., Kleine, H. C., Silva, O. L., & Lazaretti-Castro,
M. (2016). Whole-body vibration improves neuromuscular parameters and functional
capacity in osteopenic postmenopausal women. Menopause, 23(8), 870-875. doi:
10.1097/GME.0000000000000644.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state". A practical
method for grading the cognitive state of patients for the clinician. Journal of Psychiatric
Research, 12, 189-198. doi: 10.1016/0022-3956(75)90026-6.
Furness, T. P., & Maschette, W. E. (2009). Influence of whole body vibration platform
frequency on neuromuscular performance of community-dwelling older adults. Journal
of Strength and Conditioning Research, 23(5), 1508-1513. doi:
10.1519/JSC.0b013e3181a4e8f9.
Gordon, J. L., Eisenlohr-Moul, T. A., Rubinow, D. R., Schrubbe, L., & Girdler, S. S. (2016).
Naturally Occurring Changes in Estradiol Concentrations in the Menopause Transition
Predict Morning Cortisol and Negative Mood in Perimenopausal Depression. Clinical
Psychological Science, 4(5), 919-935. doi: 10.1177/2167702616647924.
Hale, G. E., Robertson, D. M., & Burger, H. G. (2014). The perimenopausal woman:
endocrinology and management. The Journal of Steroid Biochemistry and Molecular
Biology, 142, 121-131. doi: 10.1016/j.jsbmb.2013.08.015.
193
Hita-Contreras, F., Martínez-Amat, A., Cruz-Díaz, D., & Pérez-López, F. R. (2016). Fall
prevention in postmenopausal women: the role of Pilates exercise training. Climacteric,
19(3), 229-233. doi: 10.3109/13697137.2016.1139564.
Irez, G. B., Ozdemir, R. A., Evin, R., Irez, S. G., & Korkusuz, F. (2011). Integrating pilates
exercise into an exercise program for 65+ year-old women to reduce falls. Journal of
Sports Science & Medicine. 10(1), 105-111.
Katz, S., Ford, A., Moskowitz, R. W., Jackson, B. A., & Jaffe, M. W. (1963). Studies of illness
in the aged. The index of ADL: a standardized measure of biological and psychosocial
function. JAMA, 21, 914-919. doi: 10.1001/jama.1963.03060120024016.
Klarner, A., Von Stengel, S., Kemmler, W., Kladny, B., & Kalender, W. (2011). Effects of
two different types of whole body vibration on neuromuscular performance and body
composition in postmenopausal women. Deutsche Medizinische Wochenschrift,
136(42), 2133-2139. doi: 10.1055/s-0031-1292023.
Kovách, M. V., Plachy, J. K., Bognár, J., Balogh, Z. O., & Barthalos, I. (2013). Effects of
Pilates and aqua fitness training on older adults’ physical functioning and quality of life.
Biomedical Human Kinetics, 5(1), 22-27. doi: 10.2478/bhk-2013-0005.
Küçükçakır, N., Altan, L., & Korkmaz, N. (2013). Effects of Pilates exercises on pain,
functional status and quality of life in women with postmenopausal osteoporosis.
Journal of Bodywork and Movement Therapies, 17(2), 204-211. doi:
10.1016/j.jbmt.2012.07.003.
Lau, R. W., Liao, L. R., Yu, F., Teo, T., Chung, R. C., & Pang, M. Y. (2011). The effects of
whole body vibration therapy on bone mineral density and leg muscle strength in older
adults: a systematic review and meta-analysis. Clinical Rehabilitation, 25(11), 975-988.
doi: 10.1177/0269215511405078.
194
Lawton, M. P., & Brody, E. M. (1969). Assessment of older people: self-maintaining and
instrumental activities of daily living. The Gerontologist, 9, 179-186.
Lee, H., Caguicla, J. M., Park, S., Kwak, D. J., Won, D. Y., Park, Y., … & Kim, M. (2016).
Effects of 8-week Pilates exercise program on menopausal symptoms and lumbar
strength and flexibility in postmenopausal women. Journal of Exercise Rehabilitation,
12(3), 247-251. doi: 10.12965/jer.1632630.315.
Lee, J. Y., & Lee, D. C. (2013). Muscle strength and quality are associated with severity of
menopausal symptoms in peri- and post-menopausal women. Maturitas, 76(1), 88-94.
doi: 10.1016/j.maturitas.2013.06.007.
Levine, M. E., Lu, A. T., Chen, B. H., Hernandez, D. G., Singleton, A. B., Ferrucci, L., … &
Horvath, S. (2016). Menopause accelerates biological aging. Proceedings of the
National Academy of Sciences of the United States of America, 113(33), 9327-9332. doi:
10.1073/pnas.1604558113.
Liphardt, A. M., Schipilow, J., Hanley, D. A., & Boyd, S. K. (2015). Bone quality in
osteopenic postmenopausal women is not improved after 12 months of whole-body
vibration training. Osteoporosis International, 26(3), 911-920. doi: 10.1007/s00198-
014-2995-8.
Machado, A., García-López, D., González-Gallego, J., & Garatachea, N. (2010). Whole-body
vibration training increases muscle strength and mass in older women: a randomized-
controlled trial. Scandinavian Journal of Medicine & Science in Sports, 20(2), 200-207.
doi: 10.1111/j.1600-0838.2009.00919.x.
Marín-Cascales, E., Alcaraz, P. E., & Rubio-Arias, J. A. (2017). Effects of 24 Weeks of Whole
Body Vibration Versus Multicomponent Training on Muscle Strength and Body
Composition in Postmenopausal Women: A Randomized Controlled Trial. Rejuvenation
Research, In Press. doi: 10.1089/rej.2016.1877.
195
Marín, P. J., & Rhea, M. R. (2010). Effects of vibration training on muscle strength: a meta-
analysis. Journal of Strength and Conditioning Research, 24(2), 548-556. doi:
10.1519/JSC.0b013e3181c09d22.
Melo, M. O., Gomes, L. E., Silva, Y. O., Bonezi, A., & Loss, J. F. (2011). Assessment of
resistance torque and resultant muscular force during Pilates hip extension exercise and
its implications to prescription and progression. Revista Brasileira de Fisioterapia,
15(1), 23-30.
Mendoza, N., De Teresa, C., Cano, A., Godoy, D., Hita-Contreras, F., Lapotka, M., … &
Sánchez-Borrego, R. (2016). Benefits of physical exercise in postmenopausal women.
Maturitas, 93, 83-88. doi: 10.1016/j.maturitas.2016.04.017.
Mirhaghjou, S. N., Niknami, M., Moridi, M., Pakseresht, S., & Kazemnejad, E. (2016).
Quality of life and its determinants in postmenopausal women: a population-based
study. Applied Nursing Research, 30, 252-256. doi: 10.1016/j.apnr.2015.10.004.
Oliveira, L. C., Oliveira, R. G., & Pires-Oliveira, D. A. (2016). Effects of whole body vibration
on bone mineral density in postmenopausal women: a systematic review and meta-
analysis. Osteoporosis International, 27(10), 2913-2933. doi: 10.1007/s00198-016-
3618-3.
Oliveira, L. C., Oliveira, R. G., & Pires-Oliveira, D. A. (2017). Pilates increases the isokinetic
muscular strength of the knee extensors and flexors in elderly women. Journal of
Bodywork and Movement Therapies, In Press. doi: 10.1016/j.jbmt.2017.01.006.
Oliveira, L. C., Pires-Oliveira, D. A., Abucarub, A. C., Oliveira, L. S., & Oliveira, R. G.
(2017). Pilates increases isokinetic muscular strength of the elbow flexor and extensor
muscles of older women: A randomized controlled clinical trial. Journal of Bodywork
and Movement Therapies, 21(1), 2-10. doi: 10.1016/j.jbmt.2016.03.002.
196
Plachy, J., Kovách, M., & Bognár, J. (2012). Improving flexibility and endurance of elderly
women through a six-month training programme. Human Movement, 13(1), 22-27. doi:
10.2478/v10038-011-0050-6.
Raimundo, A. M., Gusi, N., & Tomas-Carus, P. (2009). Fitness efficacy of vibratory exercise
compared to walking in postmenopausal women. European Journal of Applied
Physiology, 106(5), 741-748. doi: 10.1007/s00421-009-1067-9.
Rauch, F., Sievanen, H., Boonen, S., Cardinale, M., Degens, H., Felsenberg, D., … &
International Society of Musculoskeletal and Neuronal Interactions. (2010). Reporting
whole-body vibration intervention studies: recommendations of the International
Society of Musculoskeletal and Neuronal Interactions. Journal of Musculoskeletal &
Neuronal Interactions, 10(3), 193-198.
Rees, S. S., Murphy, A. J., & Watsford, M. L. (2008). Effects of whole-body vibration exercise
on lower-extremity muscle strength and power in an older population: a randomized
clinical trial. Physical Therapy, 88(4), 462-470. doi: 10.2522/ptj.20070027.
Rodríguez-Fuentes, G., Oliveira, I. M., Ogando-Berea, H., & Otero-Gargamala, M. D. (2014).
An observational study on the effects of Pilates on quality of life in women during
menopause. European Journal of Integrative Medicine, 6(6), 631-636. doi:
10.1016/j.eujim.2014.08.003.
Roelants, M., Delecluse, C., & Verschueren, S. M. (2004). Whole-body-vibration training
increases knee-extension strength and speed of movement in older women. Journal of
the American Geriatrics Society, 52(6), 901-908. doi: 10.1111/j.1532-
5415.2004.52256.x.
Santin-Medeiros, F., Santos-Lozano, A., Cristi-Montero, C., & Garatachea Vallejo, N. (2017).
Effect of 8 months of whole-body vibration training on quality of life in elderly women.
Research in Sports Medicine, 25(1), 101-107. doi: 10.1080/15438627.2016.1258638.
197
Siqueira Rodrigues, B. G., Ali Cader, S., Bento Torres, N. V., Oliveira, E. M., & Martin
Dantas, E. H. (2010). Pilates method in personal autonomy, static balance and quality of
life of elderly females. Journal of Bodywork and Movement Therapies, 14(2), 195-202.
doi: 10.1016/j.jbmt.2009.
Stumbo, T. A., Merriam, S., Nies, K., Smith, A., Spurgeon, D., & Weir, J. P. (2001). The
effect of hand-grip stabilization on isokinetic torque at the knee. Journal of Strength and
Conditioning Research, 15(3), 372-377.
Tapp, L. R., & Signorile, J. F. (2014). Efficacy of WBV as a modality for inducing changes
in body composition, aerobic fitness, and muscular strength: a pilot study. Clinical
Interventions in Aging, 9, 63-72. doi: 10.2147/CIA.S30048.
Verschueren, S. M., Bogaerts, A., Delecluse, C., Claessens, A. L., Haentjens, P.,
Vanderschueren, D., & Boonen, S. (2011). The effects of whole-body vibration training
and vitamin D supplementation on muscle strength, muscle mass, and bone density in
institutionalized elderly women: a 6-month randomized, controlled trial. Journal of
Bone and Mineral Research, 26(1), 42-49. doi: 10.1002/jbmr.181.
Verschueren, S. M., Roelants, M., Delecluse, C., Swinnen, S., Vanderschueren, D., & Boonen,
S. (2004). Effect of 6-month whole body vibration training on hip density, muscle
strength, and postural control in postmenopausal women: a randomized controlled pilot
study. Journal of Bone and Mineral Research, 19(3), 352-359. doi:
10.1359/JBMR.0301245.
Vieira, N. D., Testa, D., Ruas, P. C., Salvini, T. F., Catai, A. M., & Melo, R. C. (2017). The
effects of 12 weeks Pilates-inspired exercise training on functional performance in older
women: A randomized clinical trial. Journal of Bodywork and Movement Therapies,
21(2), 251-258. doi: 10.1016/j.jbmt.2016.06.010.
198
Von Stengel, S., Kemmler, W., Bebenek, M., Engelke, K., & Kalender, W. A. (2011). Effects
of whole-body vibration training on different devices on bone mineral density. Medicine
and Science in Sports and Exercise, 43(6), 1071-1079. doi:
10.1249/MSS.0b013e318202f3d3.
Ware, J. E., Jr., & Gandek, B. (1998). Overview of the SF-36 Health Survey and the
International Quality of Life Assessment (IQOLA) Project. Journal of Clinical
Epidemiology, 51(11), 903-912.
Wei, N., Pang, M. Y., Ng, S. S., & Ng, G. Y. (2016). Optimal frequency/time combination of
whole-body vibration training for improving muscle size and strength of people with
age-related muscle loss (sarcopenia): A randomized controlled trial. Geriatrics &
Gerontology International, In Press. doi: 10.1111/ggi.12878.
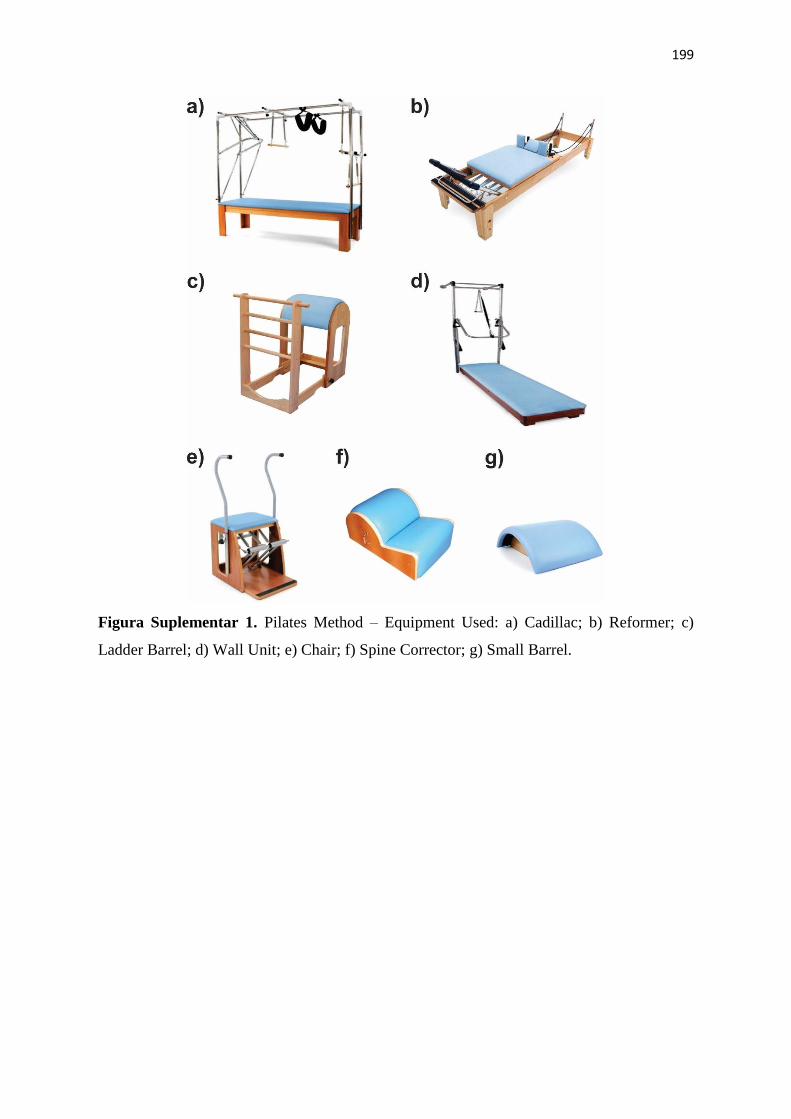
199
Figura Suplementar 1. Pilates Method – Equipment Used: a) Cadillac; b) Reformer; c)
Ladder Barrel; d) Wall Unit; e) Chair; f) Spine Corrector; g) Small Barrel.
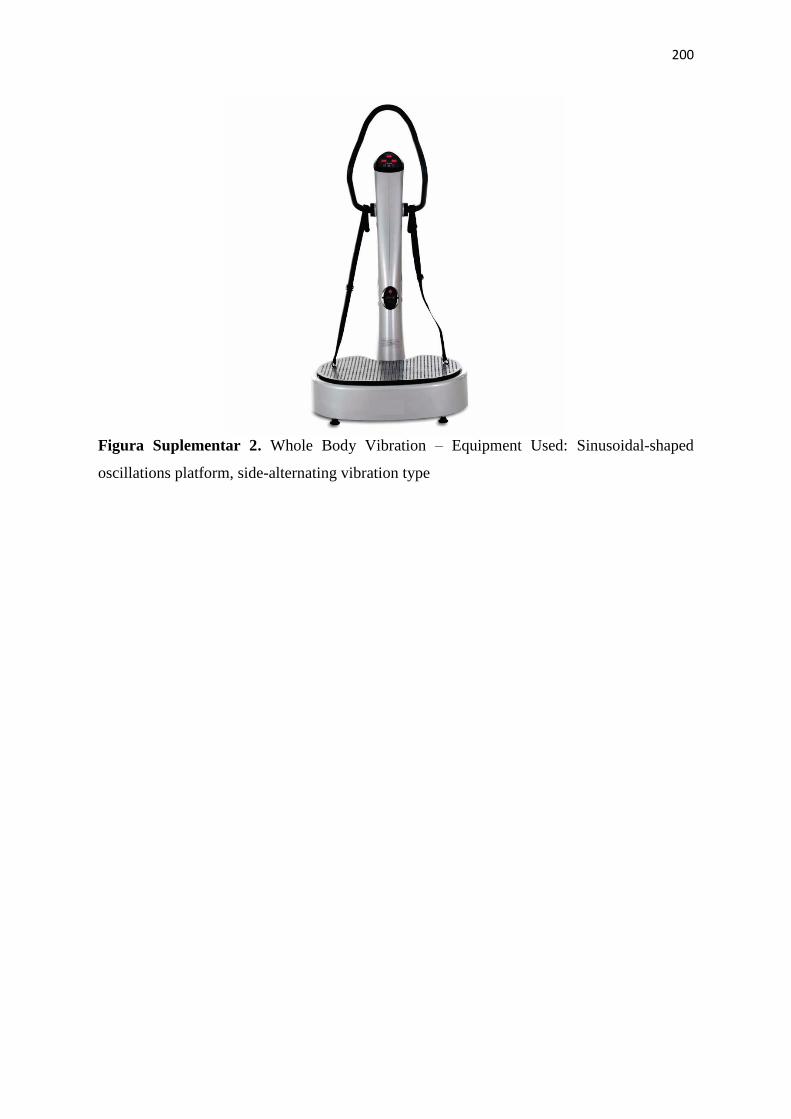
200
Figura Suplementar 2. Whole Body Vibration – Equipment Used: Sinusoidal-shaped
oscillations platform, side-alternating vibration type
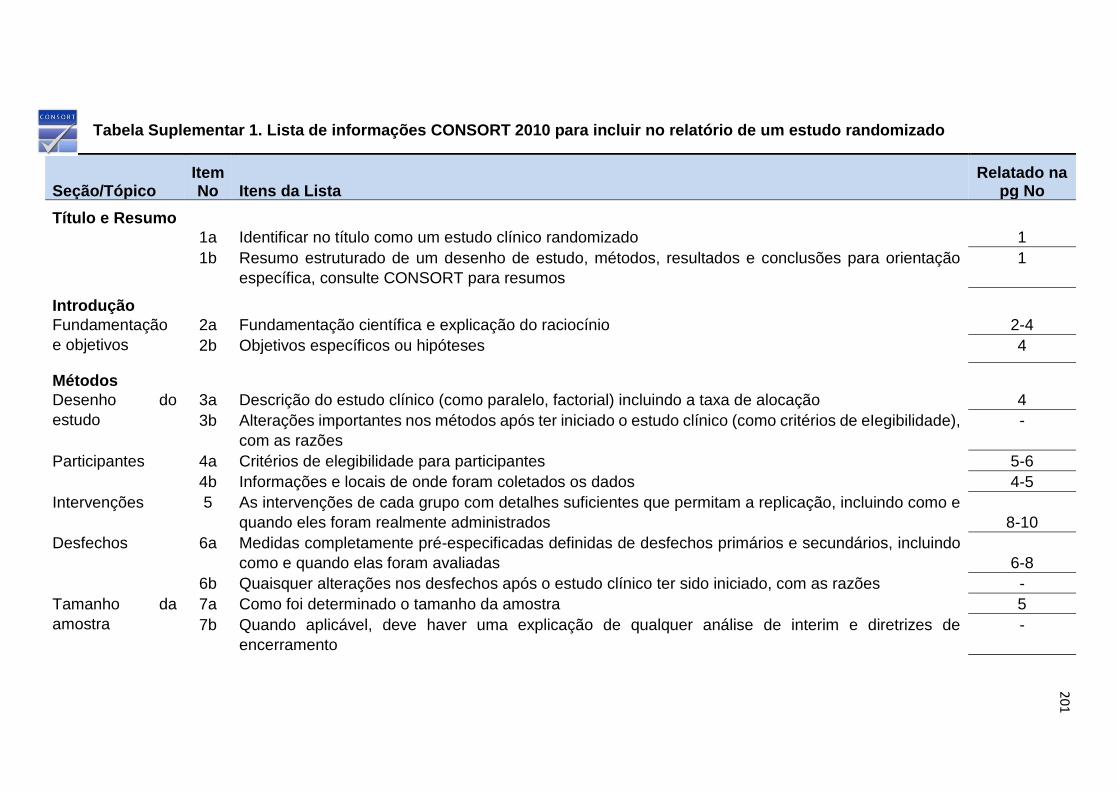
201
Tabela Suplementar 1. Lista de informações CONSORT 2010 para incluir no relatório de um estudo randomizado
Seção/Tópico Item No Itens da Lista
Relatado na pg No
Título e Resumo
1a Identificar no título como um estudo clínico randomizado 1
1b Resumo estruturado de um desenho de estudo, métodos, resultados e conclusões para orientação
específica, consulte CONSORT para resumos
1
Introdução
Fundamentação
e objetivos
2a Fundamentação científica e explicação do raciocínio 2-4
2b Objetivos específicos ou hipóteses 4
Métodos
Desenho do
estudo
3a Descrição do estudo clínico (como paralelo, factorial) incluindo a taxa de alocação 4
3b Alterações importantes nos métodos após ter iniciado o estudo clínico (como critérios de eIegibilidade),
com as razões
-
Participantes 4a Critérios de elegibilidade para participantes 5-6
4b Informações e locais de onde foram coletados os dados 4-5
Intervenções 5 As intervenções de cada grupo com detalhes suficientes que permitam a replicação, incluindo como e
quando eles foram realmente administrados
8-10
Desfechos 6a Medidas completamente pré-especificadas definidas de desfechos primários e secundários, incluindo
como e quando elas foram avaliadas
6-8
6b Quaisquer alterações nos desfechos após o estudo clínico ter sido iniciado, com as razões -
Tamanho da
amostra
7a Como foi determinado o tamanho da amostra 5
7b Quando aplicável, deve haver uma explicação de qualquer análise de interim e diretrizes de
encerramento
-
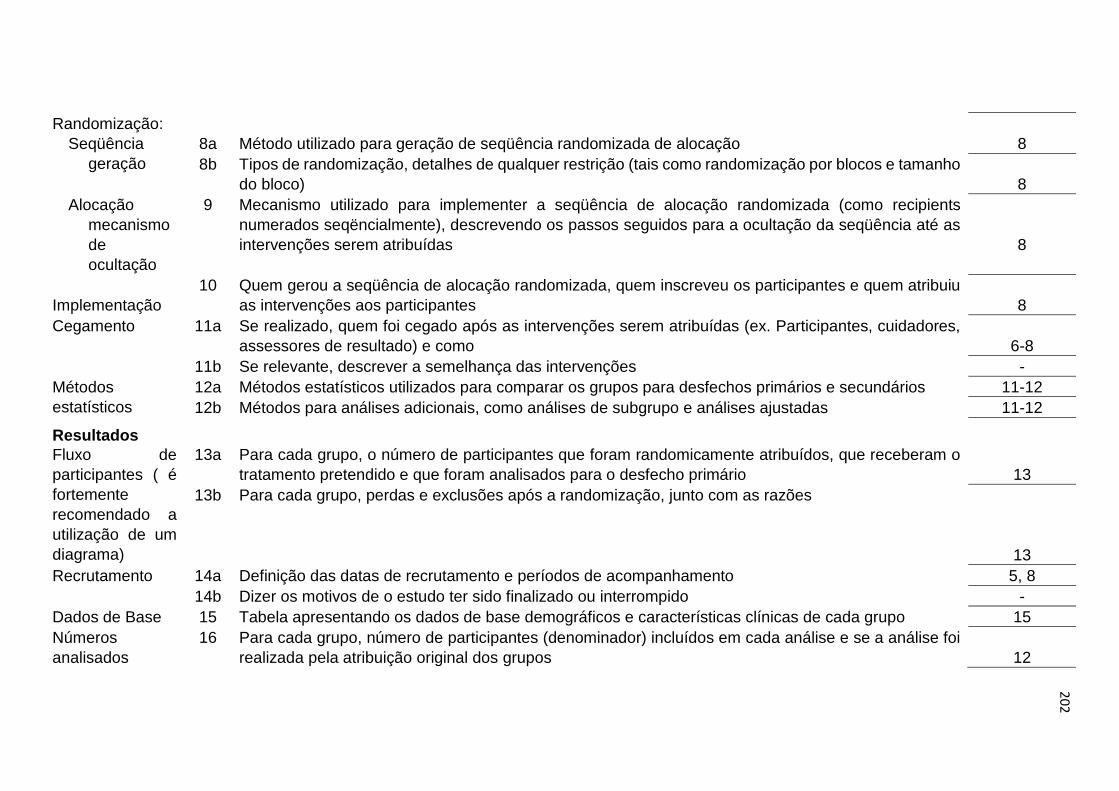
202
Randomização:
Seqüência
geração
8a Método utilizado para geração de seqüência randomizada de alocação 8
8b Tipos de randomização, detalhes de qualquer restrição (tais como randomização por blocos e tamanho
do bloco)
8
Alocação
mecanismo
de
ocultação
9 Mecanismo utilizado para implementer a seqüência de alocação randomizada (como recipients
numerados seqëncialmente), descrevendo os passos seguidos para a ocultação da seqüência até as
intervenções serem atribuídas
8
Implementação
10 Quem gerou a seqüência de alocação randomizada, quem inscreveu os participantes e quem atribuiu
as intervenções aos participantes
8
Cegamento 11a Se realizado, quem foi cegado após as intervenções serem atribuídas (ex. Participantes, cuidadores,
assessores de resultado) e como
6-8
11b Se relevante, descrever a semelhança das intervenções -
Métodos
estatísticos
12a Métodos estatísticos utilizados para comparar os grupos para desfechos primários e secundários 11-12
12b Métodos para análises adicionais, como análises de subgrupo e análises ajustadas 11-12
Resultados
Fluxo de
participantes ( é
fortemente
recomendado a
utilização de um
diagrama)
13a Para cada grupo, o número de participantes que foram randomicamente atribuídos, que receberam o
tratamento pretendido e que foram analisados para o desfecho primário
13
13b Para cada grupo, perdas e exclusões após a randomização, junto com as razões
13
Recrutamento 14a Definição das datas de recrutamento e períodos de acompanhamento 5, 8
14b Dizer os motivos de o estudo ter sido finalizado ou interrompido -
Dados de Base 15 Tabela apresentando os dados de base demográficos e características clínicas de cada grupo 15
Números
analisados
16 Para cada grupo, número de participantes (denominador) incluídos em cada análise e se a análise foi
realizada pela atribuição original dos grupos
12
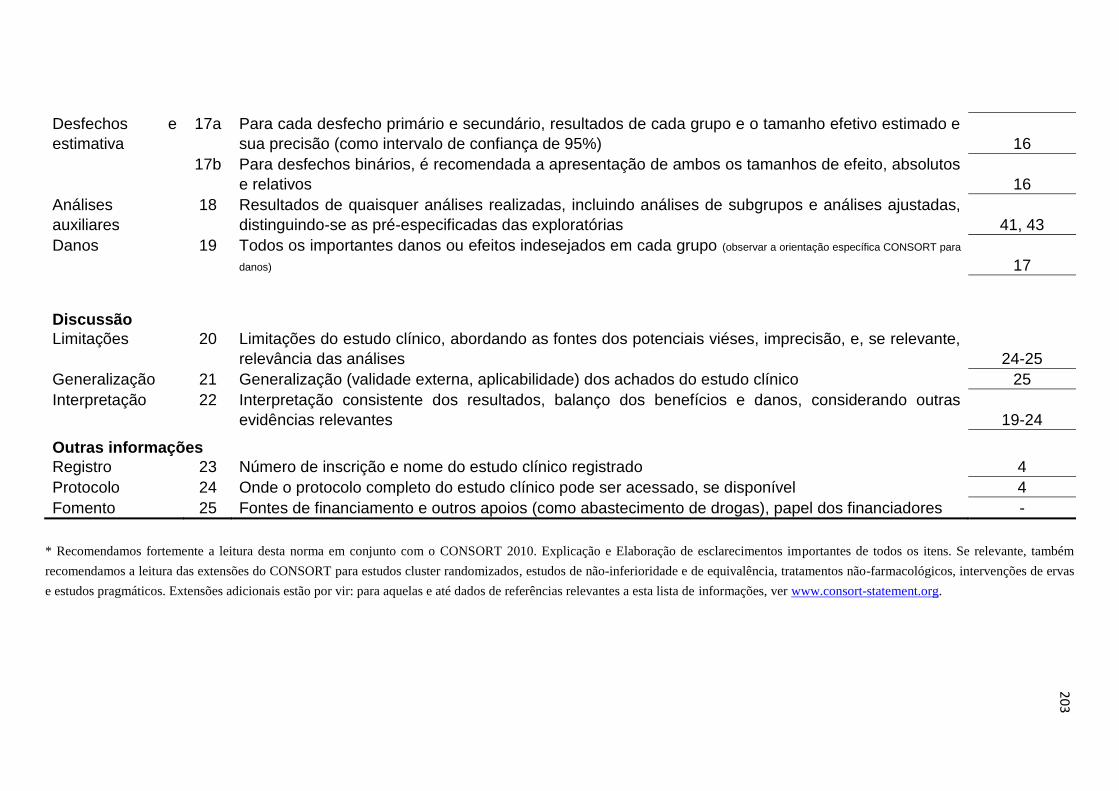
203
Desfechos e
estimativa
17a Para cada desfecho primário e secundário, resultados de cada grupo e o tamanho efetivo estimado e
sua precisão (como intervalo de confiança de 95%)
16
17b Para desfechos binários, é recomendada a apresentação de ambos os tamanhos de efeito, absolutos
e relativos
16
Análises
auxiliares
18 Resultados de quaisquer análises realizadas, incluindo análises de subgrupos e análises ajustadas,
distinguindo-se as pré-especificadas das exploratórias
41, 43
Danos 19 Todos os importantes danos ou efeitos indesejados em cada grupo (observar a orientação específica CONSORT para
danos)
17
Discussão
Limitações 20 Limitações do estudo clínico, abordando as fontes dos potenciais viéses, imprecisão, e, se relevante,
relevância das análises
24-25
Generalização 21 Generalização (validade externa, aplicabilidade) dos achados do estudo clínico 25
Interpretação 22 Interpretação consistente dos resultados, balanço dos benefícios e danos, considerando outras
evidências relevantes
19-24
Outras informações
Registro 23 Número de inscrição e nome do estudo clínico registrado 4
Protocolo 24 Onde o protocolo completo do estudo clínico pode ser acessado, se disponível 4
Fomento 25 Fontes de financiamento e outros apoios (como abastecimento de drogas), papel dos financiadores -
* Recomendamos fortemente a leitura desta norma em conjunto com o CONSORT 2010. Explicação e Elaboração de esclarecimentos importantes de todos os itens. Se relevante, também
recomendamos a leitura das extensões do CONSORT para estudos cluster randomizados, estudos de não-inferioridade e de equivalência, tratamentos não-farmacológicos, intervenções de ervas
e estudos pragmáticos. Extensões adicionais estão por vir: para aquelas e até dados de referências relevantes a esta lista de informações, ver www.consort-statement.org.
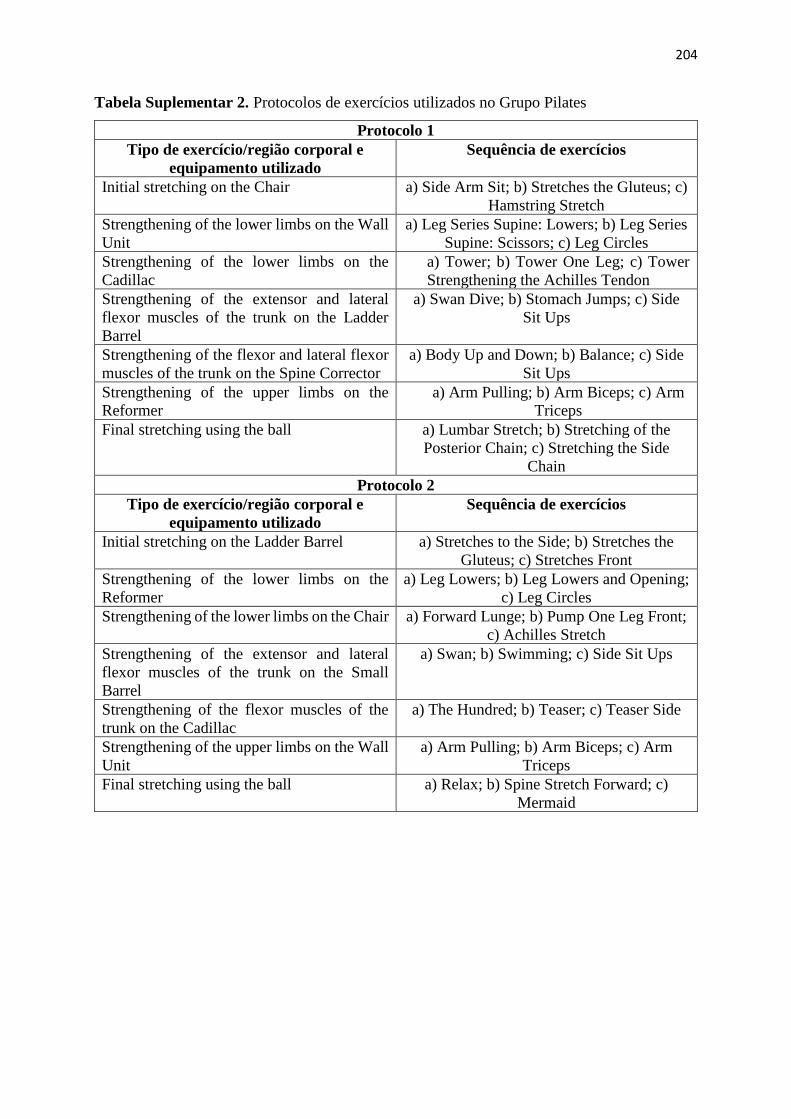
204
Tabela Suplementar 2. Protocolos de exercícios utilizados no Grupo Pilates
Protocolo 1
Tipo de exercício/região corporal e
equipamento utilizado
Sequência de exercícios
Initial stretching on the Chair a) Side Arm Sit; b) Stretches the Gluteus; c)
Hamstring Stretch
Strengthening of the lower limbs on the Wall
Unit
a) Leg Series Supine: Lowers; b) Leg Series
Supine: Scissors; c) Leg Circles
Strengthening of the lower limbs on the
Cadillac
a) Tower; b) Tower One Leg; c) Tower
Strengthening the Achilles Tendon
Strengthening of the extensor and lateral
flexor muscles of the trunk on the Ladder
Barrel
a) Swan Dive; b) Stomach Jumps; c) Side
Sit Ups
Strengthening of the flexor and lateral flexor
muscles of the trunk on the Spine Corrector
a) Body Up and Down; b) Balance; c) Side
Sit Ups
Strengthening of the upper limbs on the
Reformer
a) Arm Pulling; b) Arm Biceps; c) Arm
Triceps
Final stretching using the ball a) Lumbar Stretch; b) Stretching of the
Posterior Chain; c) Stretching the Side
Chain
Protocolo 2
Tipo de exercício/região corporal e
equipamento utilizado
Sequência de exercícios
Initial stretching on the Ladder Barrel a) Stretches to the Side; b) Stretches the
Gluteus; c) Stretches Front
Strengthening of the lower limbs on the
Reformer
a) Leg Lowers; b) Leg Lowers and Opening;
c) Leg Circles
Strengthening of the lower limbs on the Chair a) Forward Lunge; b) Pump One Leg Front;
c) Achilles Stretch
Strengthening of the extensor and lateral
flexor muscles of the trunk on the Small
Barrel
a) Swan; b) Swimming; c) Side Sit Ups
Strengthening of the flexor muscles of the
trunk on the Cadillac
a) The Hundred; b) Teaser; c) Teaser Side
Strengthening of the upper limbs on the Wall
Unit
a) Arm Pulling; b) Arm Biceps; c) Arm
Triceps
Final stretching using the ball a) Relax; b) Spine Stretch Forward; c)
Mermaid
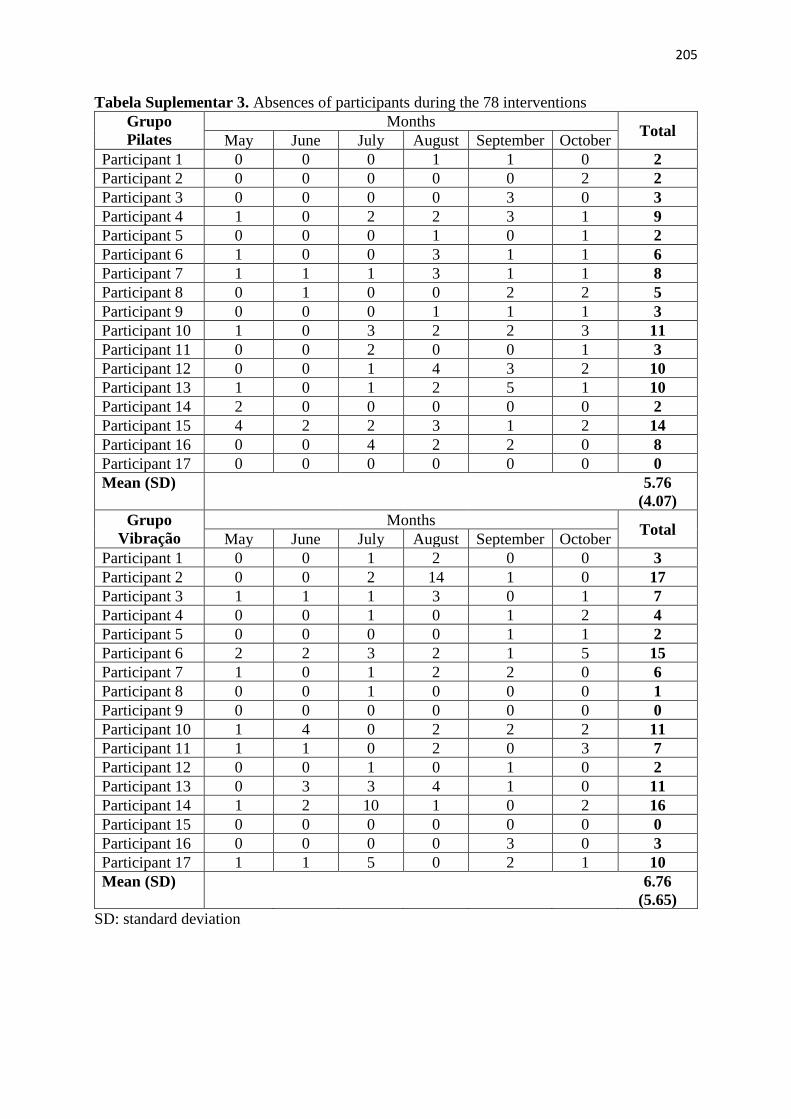
205
Tabela Suplementar 3. Absences of participants during the 78 interventions
Grupo
Pilates
Months Total
May June July August September October
Participant 1 0 0 0 1 1 0 2
Participant 2 0 0 0 0 0 2 2
Participant 3 0 0 0 0 3 0 3
Participant 4 1 0 2 2 3 1 9
Participant 5 0 0 0 1 0 1 2
Participant 6 1 0 0 3 1 1 6
Participant 7 1 1 1 3 1 1 8
Participant 8 0 1 0 0 2 2 5
Participant 9 0 0 0 1 1 1 3
Participant 10 1 0 3 2 2 3 11
Participant 11 0 0 2 0 0 1 3
Participant 12 0 0 1 4 3 2 10
Participant 13 1 0 1 2 5 1 10
Participant 14 2 0 0 0 0 0 2
Participant 15 4 2 2 3 1 2 14
Participant 16 0 0 4 2 2 0 8
Participant 17 0 0 0 0 0 0 0
Mean (SD) 5.76
(4.07)
Grupo
Vibração
Months Total
May June July August September October
Participant 1 0 0 1 2 0 0 3
Participant 2 0 0 2 14 1 0 17
Participant 3 1 1 1 3 0 1 7
Participant 4 0 0 1 0 1 2 4
Participant 5 0 0 0 0 1 1 2
Participant 6 2 2 3 2 1 5 15
Participant 7 1 0 1 2 2 0 6
Participant 8 0 0 1 0 0 0 1
Participant 9 0 0 0 0 0 0 0
Participant 10 1 4 0 2 2 2 11
Participant 11 1 1 0 2 0 3 7
Participant 12 0 0 1 0 1 0 2
Participant 13 0 3 3 4 1 0 11
Participant 14 1 2 10 1 0 2 16
Participant 15 0 0 0 0 0 0 0
Participant 16 0 0 0 0 3 0 3
Participant 17 1 1 5 0 2 1 10
Mean (SD) 6.76
(5.65)
SD: standard deviation
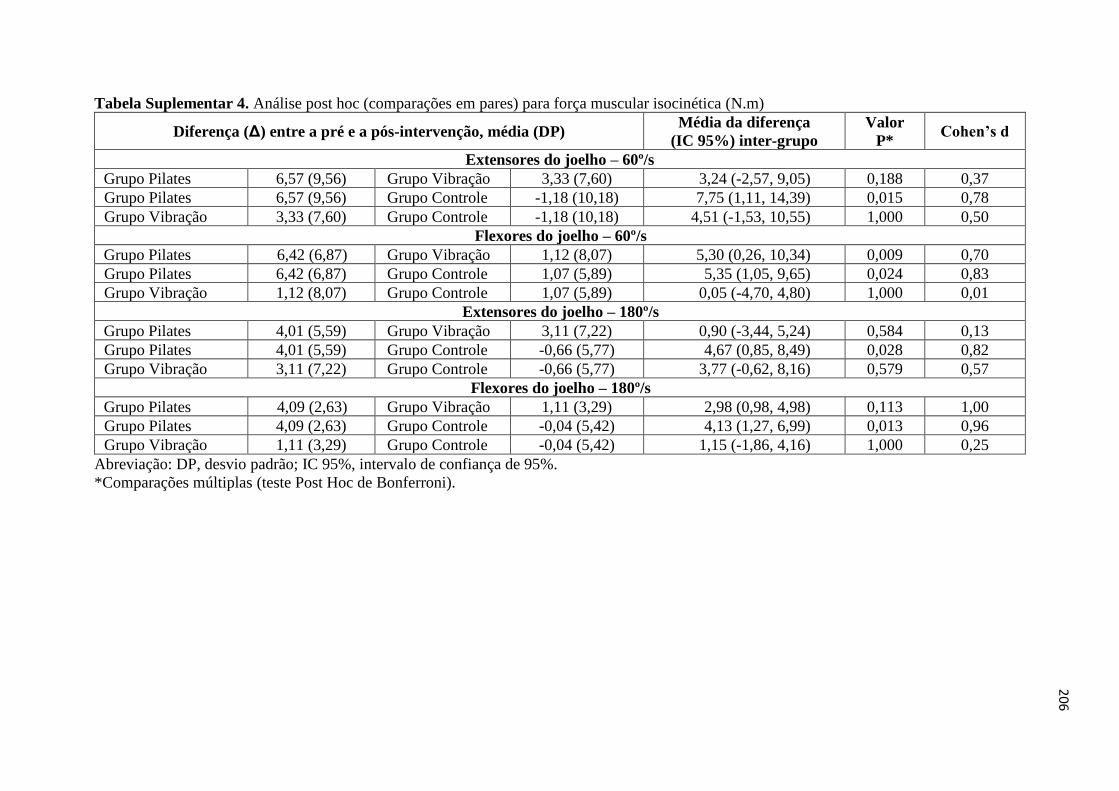
206
Tabela Suplementar 4. Análise post hoc (comparações em pares) para força muscular isocinética (N.m)
Diferença (Δ) entre a pré e a pós-intervenção, média (DP) Média da diferença
(IC 95%) inter-grupo
Valor
P* Cohen’s d
Extensores do joelho – 60º/s
Grupo Pilates 6,57 (9,56) Grupo Vibração 3,33 (7,60) 3,24 (-2,57, 9,05) 0,188 0,37
Grupo Pilates 6,57 (9,56) Grupo Controle -1,18 (10,18) 7,75 (1,11, 14,39) 0,015 0,78
Grupo Vibração 3,33 (7,60) Grupo Controle -1,18 (10,18) 4,51 (-1,53, 10,55) 1,000 0,50
Flexores do joelho – 60º/s
Grupo Pilates 6,42 (6,87) Grupo Vibração 1,12 (8,07) 5,30 (0,26, 10,34) 0,009 0,70
Grupo Pilates 6,42 (6,87) Grupo Controle 1,07 (5,89) 5,35 (1,05, 9,65) 0,024 0,83
Grupo Vibração 1,12 (8,07) Grupo Controle 1,07 (5,89) 0,05 (-4,70, 4,80) 1,000 0,01
Extensores do joelho – 180º/s
Grupo Pilates 4,01 (5,59) Grupo Vibração 3,11 (7,22) 0,90 (-3,44, 5,24) 0,584 0,13
Grupo Pilates 4,01 (5,59) Grupo Controle -0,66 (5,77) 4,67 (0,85, 8,49) 0,028 0,82
Grupo Vibração 3,11 (7,22) Grupo Controle -0,66 (5,77) 3,77 (-0,62, 8,16) 0,579 0,57
Flexores do joelho – 180º/s
Grupo Pilates 4,09 (2,63) Grupo Vibração 1,11 (3,29) 2,98 (0,98, 4,98) 0,113 1,00
Grupo Pilates 4,09 (2,63) Grupo Controle -0,04 (5,42) 4,13 (1,27, 6,99) 0,013 0,96
Grupo Vibração 1,11 (3,29) Grupo Controle -0,04 (5,42) 1,15 (-1,86, 4,16) 1,000 0,25
Abreviação: DP, desvio padrão; IC 95%, intervalo de confiança de 95%.
*Comparações múltiplas (teste Post Hoc de Bonferroni).
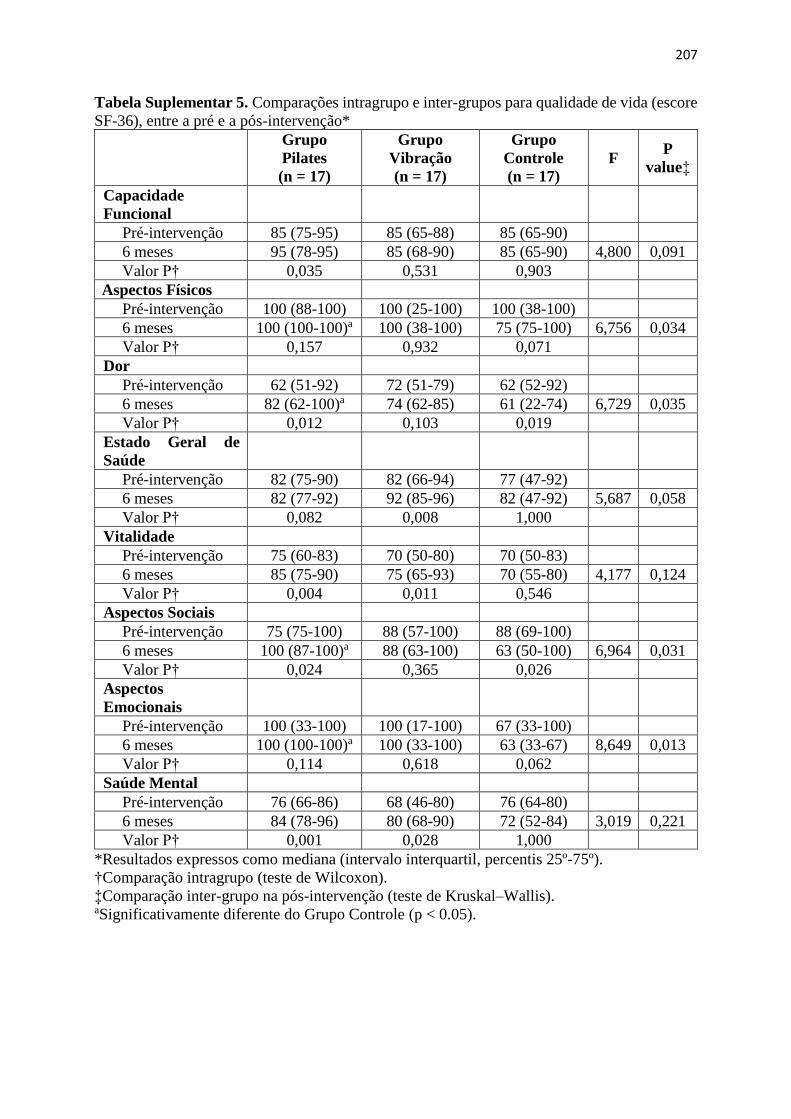
207
Tabela Suplementar 5. Comparações intragrupo e inter-grupos para qualidade de vida (escore
SF-36), entre a pré e a pós-intervenção*
Grupo
Pilates
(n = 17)
Grupo
Vibração
(n = 17)
Grupo
Controle
(n = 17)
F P
value‡
Capacidade
Funcional
Pré-intervenção 85 (75-95) 85 (65-88) 85 (65-90)
6 meses 95 (78-95) 85 (68-90) 85 (65-90) 4,800 0,091
Valor P† 0,035 0,531 0,903
Aspectos Físicos
Pré-intervenção 100 (88-100) 100 (25-100) 100 (38-100)
6 meses 100 (100-100)a 100 (38-100) 75 (75-100) 6,756 0,034
Valor P† 0,157 0,932 0,071
Dor
Pré-intervenção 62 (51-92) 72 (51-79) 62 (52-92)
6 meses 82 (62-100)a 74 (62-85) 61 (22-74) 6,729 0,035
Valor P† 0,012 0,103 0,019
Estado Geral de
Saúde
Pré-intervenção 82 (75-90) 82 (66-94) 77 (47-92)
6 meses 82 (77-92) 92 (85-96) 82 (47-92) 5,687 0,058
Valor P† 0,082 0,008 1,000
Vitalidade
Pré-intervenção 75 (60-83) 70 (50-80) 70 (50-83)
6 meses 85 (75-90) 75 (65-93) 70 (55-80) 4,177 0,124
Valor P† 0,004 0,011 0,546
Aspectos Sociais
Pré-intervenção 75 (75-100) 88 (57-100) 88 (69-100)
6 meses 100 (87-100)a 88 (63-100) 63 (50-100) 6,964 0,031
Valor P† 0,024 0,365 0,026
Aspectos
Emocionais
Pré-intervenção 100 (33-100) 100 (17-100) 67 (33-100)
6 meses 100 (100-100)a 100 (33-100) 63 (33-67) 8,649 0,013
Valor P† 0,114 0,618 0,062
Saúde Mental
Pré-intervenção 76 (66-86) 68 (46-80) 76 (64-80)
6 meses 84 (78-96) 80 (68-90) 72 (52-84) 3,019 0,221
Valor P† 0,001 0,028 1,000
*Resultados expressos como mediana (intervalo interquartil, percentis 25º-75º).
†Comparação intragrupo (teste de Wilcoxon).
‡Comparação inter-grupo na pós-intervenção (teste de Kruskal–Wallis). aSignificativamente diferente do Grupo Controle (p < 0.05).
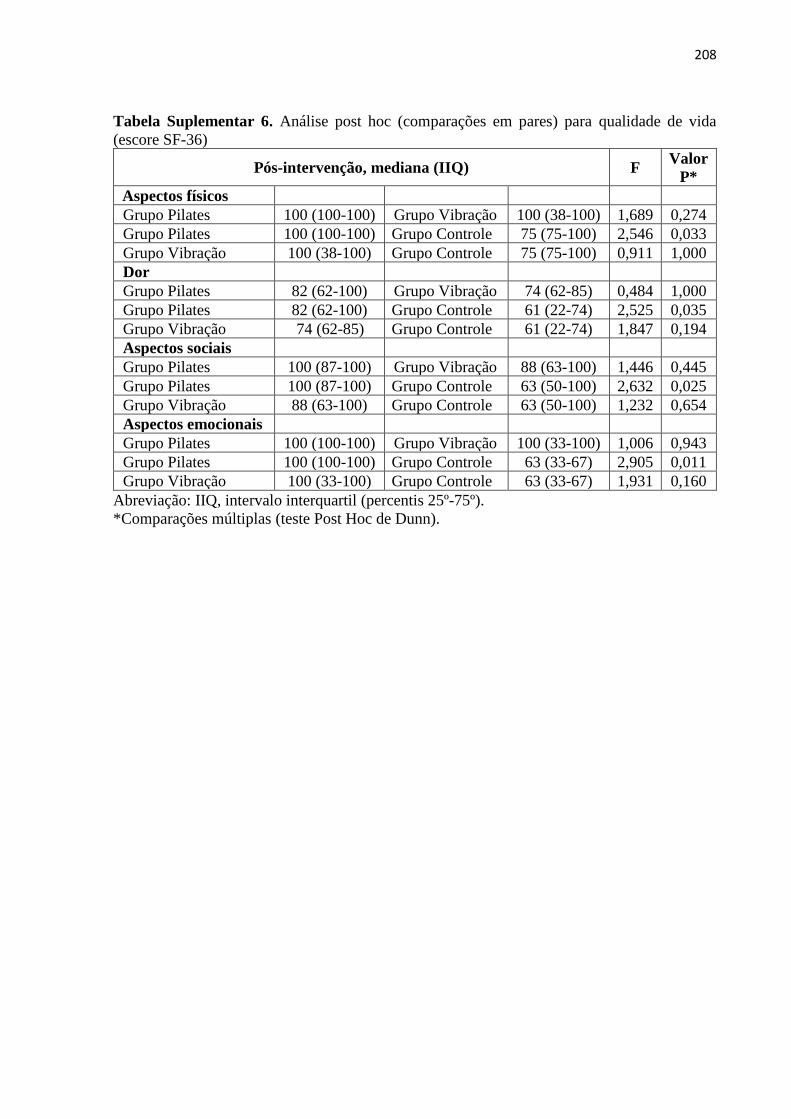
208
Tabela Suplementar 6. Análise post hoc (comparações em pares) para qualidade de vida
(escore SF-36)
Pós-intervenção, mediana (IIQ) F Valor
P*
Aspectos físicos
Grupo Pilates 100 (100-100) Grupo Vibração 100 (38-100) 1,689 0,274
Grupo Pilates 100 (100-100) Grupo Controle 75 (75-100) 2,546 0,033
Grupo Vibração 100 (38-100) Grupo Controle 75 (75-100) 0,911 1,000
Dor
Grupo Pilates 82 (62-100) Grupo Vibração 74 (62-85) 0,484 1,000
Grupo Pilates 82 (62-100) Grupo Controle 61 (22-74) 2,525 0,035
Grupo Vibração 74 (62-85) Grupo Controle 61 (22-74) 1,847 0,194
Aspectos sociais
Grupo Pilates 100 (87-100) Grupo Vibração 88 (63-100) 1,446 0,445
Grupo Pilates 100 (87-100) Grupo Controle 63 (50-100) 2,632 0,025
Grupo Vibração 88 (63-100) Grupo Controle 63 (50-100) 1,232 0,654
Aspectos emocionais
Grupo Pilates 100 (100-100) Grupo Vibração 100 (33-100) 1,006 0,943
Grupo Pilates 100 (100-100) Grupo Controle 63 (33-67) 2,905 0,011
Grupo Vibração 100 (33-100) Grupo Controle 63 (33-67) 1,931 0,160
Abreviação: IIQ, intervalo interquartil (percentis 25º-75º).
*Comparações múltiplas (teste Post Hoc de Dunn).
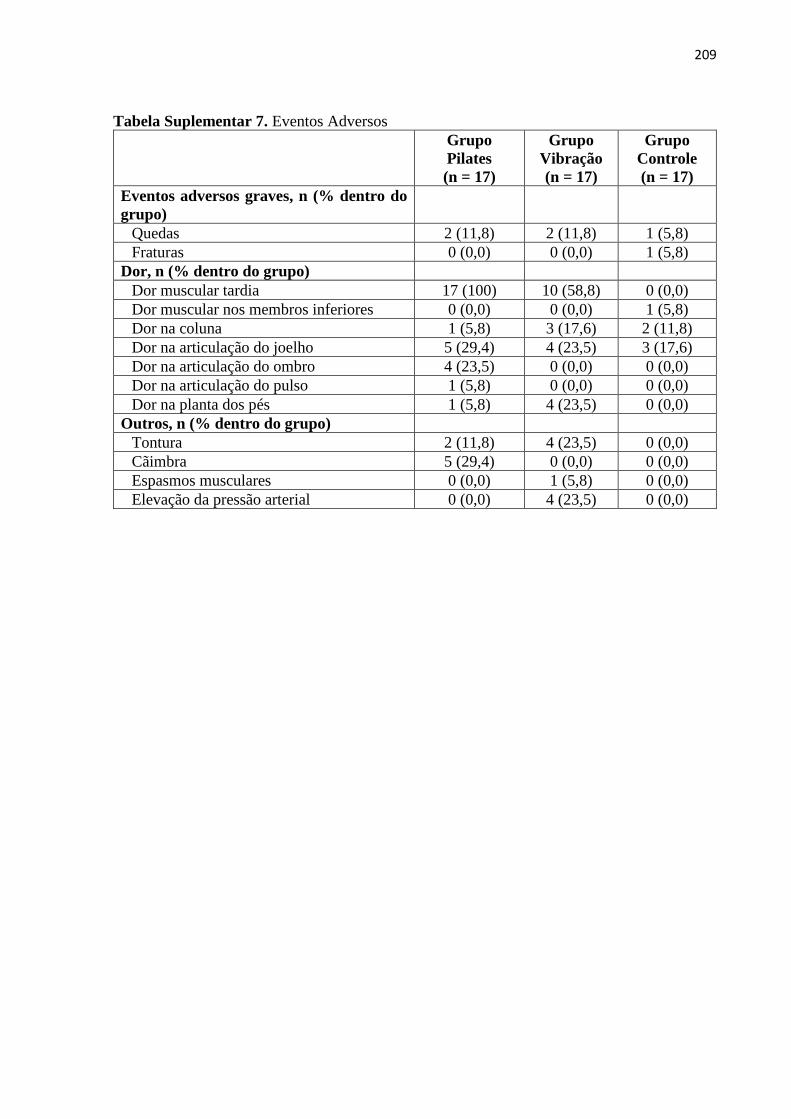
209
Tabela Suplementar 7. Eventos Adversos
Grupo
Pilates
(n = 17)
Grupo
Vibração
(n = 17)
Grupo
Controle
(n = 17)
Eventos adversos graves, n (% dentro do
grupo)
Quedas 2 (11,8) 2 (11,8) 1 (5,8)
Fraturas 0 (0,0) 0 (0,0) 1 (5,8)
Dor, n (% dentro do grupo)
Dor muscular tardia 17 (100) 10 (58,8) 0 (0,0)
Dor muscular nos membros inferiores 0 (0,0) 0 (0,0) 1 (5,8)
Dor na coluna 1 (5,8) 3 (17,6) 2 (11,8)
Dor na articulação do joelho 5 (29,4) 4 (23,5) 3 (17,6)
Dor na articulação do ombro 4 (23,5) 0 (0,0) 0 (0,0)
Dor na articulação do pulso 1 (5,8) 0 (0,0) 0 (0,0)
Dor na planta dos pés 1 (5,8) 4 (23,5) 0 (0,0)
Outros, n (% dentro do grupo)
Tontura 2 (11,8) 4 (23,5) 0 (0,0)
Cãimbra 5 (29,4) 0 (0,0) 0 (0,0)
Espasmos musculares 0 (0,0) 1 (5,8) 0 (0,0)
Elevação da pressão arterial 0 (0,0) 4 (23,5) 0 (0,0)
210
7 CONCLUSÃO GERAL
A presente tese acrescenta as seguintes evidências: a) coluna lombar e
trocânter são as regiões ósseas que apresentaram maior osteogênese em mulheres
na pós-menopausa submetidas à VCI, sendo que os parâmetros mais favoráveis para
influenciar aumento da DMO referem-se a baixa frequência, alta magnitude, vibração
do tipo lado-alternado, posicionamento com semi-flexão dos joelhos e baixo tempo de
exposição (artigo 1); b) VCI e MP são intervenções capazes de possibilitar melhora
significativa da DMO da coluna lombar e trocânter em mulheres na pós-menopausa,
sem diferenças entre as técnicas, mas superiores ao grupo controle que não realizou
nenhuma intervenção (artigo 2); c) MP foi superior a VCI sobre o pico de torque
isocinético dos flexores do joelho, porém, as técnicas foram semelhantes para o pico
de torque dos extensores do joelho e qualidade de vida em mulheres na pós-
menopausa. Quando comparadas as técnicas com nenhuma intervenção, apenas MP
foi superior, para todas as variáveis de força muscular isocinética, além de quatro
domínios da qualidade de vida (artigo 3).
Uma vez que VCI e o MP se mostraram relativamente seguros e ofereceram
efeitos osteogênicos similares, a escolha em relação a qual técnica utilizar para esta
finalidade, poderá levar em consideração os recursos existentes ou preferências do
paciente. Por outro lado, quando o objetivo estiver atrelado ao ganho de força
muscular, o MP deve ser priorizado em relação a VCI. Ainda, como não existem
evidências conclusivas sobre os melhores parâmetros de VCI ou MP, pautadas por
multiplos ECRs de bom porte, concordantes e/ou meta-analise robusta de ECRs, os
parâmetros apresentados na presente tese podem contribuir com a escolha
profissional sobre qual técnica utilizar.

211
8 ANEXOS
ANEXO A – Parecer do Comitê de Ética em Pesquisa
212

213
214
ANEXO B – Protocolo de Registro no Clinical Trials
215
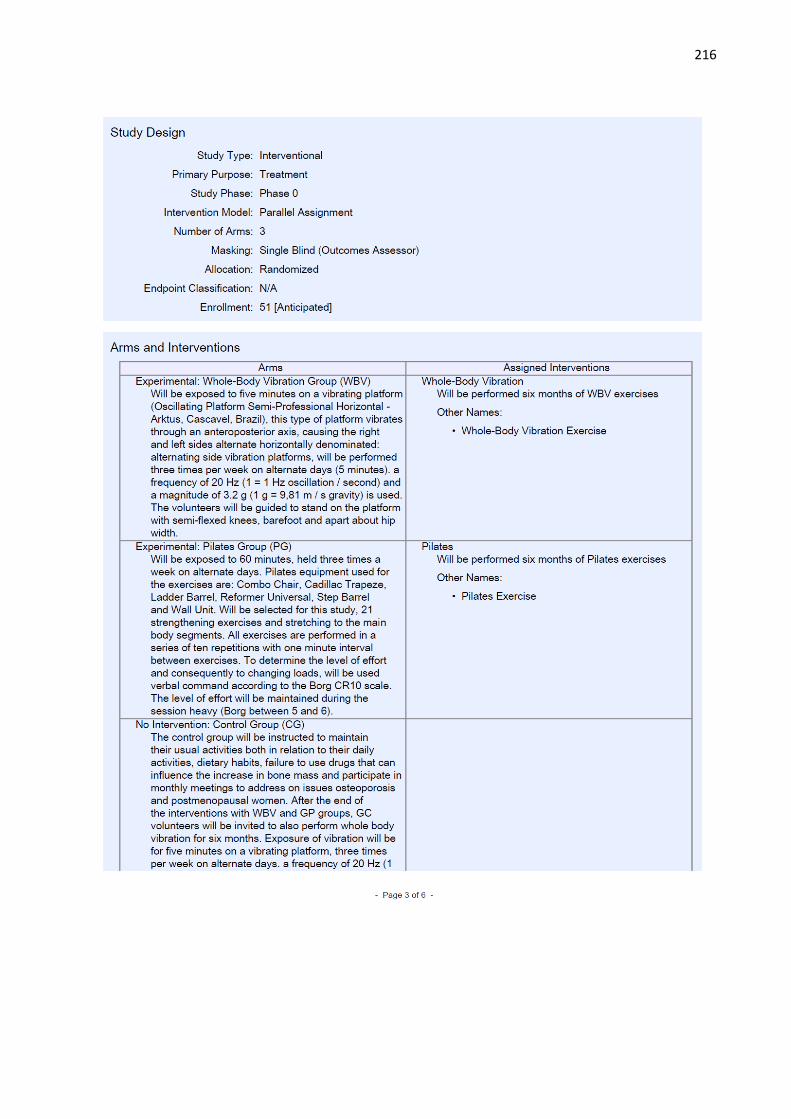
216
217
218
219