Limited Intimal Aorta Tearshave intramural hematomas, yet at surgery or au-topsy, only 5% have no...
4
EDITORIAL COMMENT Limited Intimal Aorta Tears Royalty Torn Asunder, and a Nation Was Created* Lars G. Svensson, MD, PHD I n 1760, King George II of Great Britain died from a ruptured aortic dissection, as revealed at autopsy (1). He was succeeded by his unstable grandson, King George III, who imposed various stamp and other taxes on the American colonies as part of a NAFTA- like deal. British tea shipping agents, cut out of the deal, instigated the Boston Tea Party, unleashing the New England militia and leading to the American War of Independence. Perhaps this is a stretch of the historical narrative, but aortic dissection ultimately led to the creation of the United States! Despite our increased knowledge and under- standing of the treatment of aortic dissection, its etiology, pathophysiology and classification, and detection remain a conundrum. For example, there are 3 classifications of aortic dissection extents (2,3). The original Stanford classification, although it is often misrepresented as not including “non-A–non-B,” is the most widely used (Figure 1) (2). Type A involves the ascending aorta, whereas Type B does not, and hence includes the aortic arch (the so-called non-A and non-B). The DeBakey classification, however, divides dissection extent into type I, involving the ascending aorta and arch and beyond (2), type II, involving the ascending aorta only, and type III, involving the descending aorta. Type IIIa involves only the descending aorta, whereas type IIIb also includes dissections extending below the diaphragm. Furthermore, DeBakey told me that he included “non-A–non-B” under type I. The third classification is proximal or distal dissection to the subclavian artery (2,3). The broad consensus is that type A, DeBakey type I and II, and proximal dissection should be treated by immediate surgical repair tempered by comorbidity risks, such as delay for catheterization for coronary artery reoperation and decision about likely survival related to, for example, gut gangrene (1). Generally, “stroke” is not an exclusion, because most comatose patients have “watershed” areas of inade- quate flow related to greater vessel-associated dissec- tion that frequently recovers with reperfusion. Many aortic surgeons use proximal or distal to the left subclavian artery extent of dissection to decide on surgery (3). Proximal dissections are immediately operated on, whereas distal ones are dependent on complications. There is, however, controversy about immediate surgery for extents involving the arch and beyond, but more often than not, the ascending aorta is involved at the time of surgery (2). Of note, apart from the issue of extent of dissection and treatment, there remains the problem of identifying tear types. Before the advent of high-resolution 3-dimensional (3D) and axis-of-flow computed tomography (CT) imaging of the aorta, it was difficult to detect subtle forms of aortic dissection, particularly localized tears. Even multiplanar angiography often missed localized tears (4). For example, 15% of patients are said to have intramural hematomas, yet at surgery or au- topsy, only 5% have no defined intimal tear. We previously categorized tear types (Figure 2) into 5 classes (4): 1) classic, with 2 lumens and blood flow in both; 2) intramural hematoma with clot in the aortic wall; 3) intimal tears without dissection propagation, often with rolled intimal edges (Figure 3); 4) penetrating ulcers associated with atherosclerosis or infection; and 5) traumatic or post- catheterization or intervention tears, typically of the root. In this issue of the Journal, the Stanford group (5) examined all of their aortic dissection patients for SEE PAGE 2773 ISSN 0735-1097/$36.00 https://doi.org/10.1016/j.jacc.2018.03.530 *Editorials published in the Journal of the American College of Cardiology reflect the views of the authors and do not necessarily represent the views of JACC or the American College of Cardiology. From the Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio. Dr. Svensson has reported that he has no relationships relevant to the contents of this paper to disclose. JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 71, NO. 24, 2018 ª 2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER
Transcript of Limited Intimal Aorta Tearshave intramural hematomas, yet at surgery or au-topsy, only 5% have no...

J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 1 , N O . 2 4 , 2 0 1 8
ª 2 0 1 8 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
EDITORIAL COMMENT
Limited Intimal Aorta TearsRoyalty Torn Asunder, and a Nation Was Created*
Lars G. Svensson, MD, PHD
SEE PAGE 2773
I n 1760, King George II of Great Britain died from aruptured aortic dissection, as revealed at autopsy(1). He was succeeded by his unstable grandson,
King George III, who imposed various stamp and othertaxes on the American colonies as part of a NAFTA-like deal. British tea shipping agents, cut out of thedeal, instigated the Boston Tea Party, unleashing theNew England militia and leading to the AmericanWar of Independence. Perhaps this is a stretch of thehistorical narrative, but aortic dissection ultimatelyled to the creation of the United States!
Despite our increased knowledge and under-standing of the treatment of aortic dissection, itsetiology, pathophysiology and classification, anddetection remain a conundrum. For example, thereare 3 classifications of aortic dissection extents (2,3).
The original Stanford classification, although it isoftenmisrepresented as not including “non-A–non-B,”is the most widely used (Figure 1) (2). Type A involvesthe ascending aorta, whereas Type B does not, andhence includes the aortic arch (the so-called non-Aand non-B). The DeBakey classification, however,divides dissection extent into type I, involving theascending aorta and arch and beyond (2), type II,involving the ascending aorta only, and type III,involving the descending aorta. Type IIIa involvesonly the descending aorta, whereas type IIIb alsoincludes dissections extending below the diaphragm.Furthermore, DeBakey told me that he included“non-A–non-B” under type I. The third classificationis proximal or distal dissection to the subclavianartery (2,3). The broad consensus is that type A,
ISSN 0735-1097/$36.00
*Editorials published in the Journal of the American College of Cardiology
reflect the views of the authors and do not necessarily represent the
views of JACC or the American College of Cardiology.
From the Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio.
Dr. Svensson has reported that he has no relationships relevant to the
contents of this paper to disclose.
DeBakey type I and II, and proximal dissection shouldbe treated by immediate surgical repair tempered bycomorbidity risks, such as delay for catheterization forcoronary artery reoperation and decision about likelysurvival related to, for example, gut gangrene (1).Generally, “stroke” is not an exclusion, because mostcomatose patients have “watershed” areas of inade-quate flow related to greater vessel-associated dissec-tion that frequently recovers with reperfusion. Manyaortic surgeons use proximal or distal to the leftsubclavian artery extent of dissection to decide onsurgery (3). Proximal dissections are immediatelyoperated on, whereas distal ones are dependent oncomplications. There is, however, controversy aboutimmediate surgery for extents involving the arch andbeyond, butmore often than not, the ascending aorta isinvolved at the time of surgery (2). Of note, apart fromthe issue of extent of dissection and treatment, thereremains the problem of identifying tear types.
Before the advent of high-resolution 3-dimensional(3D) and axis-of-flow computed tomography (CT)imaging of the aorta, it was difficult to detect subtleforms of aortic dissection, particularly localized tears.Even multiplanar angiography often missed localizedtears (4). For example, 15% of patients are said tohave intramural hematomas, yet at surgery or au-topsy, only 5% have no defined intimal tear.
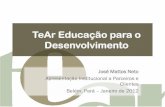
We previously categorized tear types (Figure 2)into 5 classes (4): 1) classic, with 2 lumens and bloodflow in both; 2) intramural hematoma with clot inthe aortic wall; 3) intimal tears without dissectionpropagation, often with rolled intimal edges(Figure 3); 4) penetrating ulcers associated withatherosclerosis or infection; and 5) traumatic or post-catheterization or intervention tears, typically of theroot. In this issue of the Journal, the Stanford group(5) examined all of their aortic dissection patients for
https://doi.org/10.1016/j.jacc.2018.03.530

FIGURE 1 Classifications of Extent of Tears for Classic Aortic Dissection Tears
(A) Proximal, DeBakey I and II, Stanford A. (B) Proximal, Stanford B. (C) Distal, DeBakey IIIa and IIIb, Stanford B.
J A C C V O L . 7 1 , N O . 2 4 , 2 0 1 8 SvenssonJ U N E 1 9 , 2 0 1 8 : 2 7 8 6 – 9 Aortic Dissection Tear Types and Missed Subtle Classes
2787
the tear classes and found that 4.8% had Class 3intimal tears (limited intimal tears). They also founda high prevalence of missed diagnoses. As they pointout, an advance since our report was published isthat modern CT studies should now be able to pickup these more subtle tears. Nonetheless, we recentlyoperated on an airline pilot with aortic dissection–type chest pain who twice presented at an emer-gency department with pain and was sent home. Hesent his CT scans to us for review, and we immedi-ately asked him to come in for surgery, which heunderwent successfully.
Although such events are not common, physiciansshould be aware of these less common entities andlook carefully for localized tears on the CT scans ofpatients with classic pain symptoms. Indeed, in arecent study of Medicare claim patients, 4.5% ofaortic dissections were missed in the emergencydepartment (6). Unfortunately, these localized tearsare frequently not picked up on echocardiography.Even more concerning, particularly when the resultsof surgery have considerably improved (7), are thosecases of classic aortic dissection that are missedbecause of lack of awareness in emergency de-partments. Nonetheless, prophylactic surgery, like
aortic root implantation for enlarged aortic roots toprevent aortic dissection, has considerably improvedfor the prevention of aortic dissection (8).
The key to more accurately diagnosing aorticdissection, particularly localized tears, is to ask one-self if despite preliminary tests, and if a patient hastypical symptoms, “Is this is a limited type ofdissection?” The symptoms can be classic chest pain,a fact, unfortunately, not available in this excellentstudy from Stanford (5). However, a number of find-ings may also be suggestive. These include a systolicregurgitation murmur from a disrupted commissure,a rub or muffled heart sounds from a pericardialeffusion, including from localized tears, or signs of anunexplained pleural effusion. At this time, we do nothave reliable blood markers, particularly for localizedtears, because there is little or no intra-aortic clotformation. The best evidence is an electrocardiogram-gated 3D CT scan that eliminates motion artifact fromaortic pulsation and permits 3D reconstruction of theintimal surface of the aorta. Although highly selec-tive, multiplanar angiography may identify bulging ofthe aorta, this takes time, extra dye load, and expe-rience, and hence our best current option is gated 3DCT. With the increasing accuracy of CT for diagnosis

FIGURE 3 Intraoperative Photograph of a Localized Tear
This tear is adjacent to the left main coronary atrium in a patient
undergoing root reimplantation. The original presenting pain
was classic for aortic dissection.
FIGURE 2 Classes of Aortic Dissection Tear Types
(Class 1) Classic tear. (Class 2) Intramural hematoma. (Class 3) Localized tear without tear extension. (Class 4) Penetrating ulcer. (Class 5)
Post-traumatic or intervention tear.
Svensson J A C C V O L . 7 1 , N O . 2 4 , 2 0 1 8
Aortic Dissection Tear Types and Missed Subtle Classes J U N E 1 9 , 2 0 1 8 : 2 7 8 6 – 9
2788
of various causes of chest pain, such as coronary ar-tery disease (including assessing ischemia using CTfractional flow reserve) and pulmonary embolism,perhaps the time will come when a rapid CT in com-bination with a high-sensitivity troponin T test will beconsidered standard of care for managing chest painwithout electrocardiogram changes.
Although King George II’s death may have changedthe course of history, it is unfortunate that today,despite all our modern technical advances, some pa-tients still die from missed aortic dissection. Withimproved awareness of subtle subclasses of aorticdissection, we anticipate that this will become a lesscommon event.
ADDRESS FOR CORRESPONDENCE: Dr. Lars G.Svensson, Heart and Vascular Institute, ClevelandClinic, 9500 Euclid Avenue, Desk J1-127, Cleveland,Ohio 44195. E-mail: [email protected]. Twitter:@LarsSvenssonMD, @ClevelandClinic.

J A C C V O L . 7 1 , N O . 2 4 , 2 0 1 8 SvenssonJ U N E 1 9 , 2 0 1 8 : 2 7 8 6 – 9 Aortic Dissection Tear Types and Missed Subtle Classes
2789
RE F E RENCE S
1. Svensson LG, Crawford ES. Historical aspects ofcardiovascular and vascular disease. In:Svensson LG, Crawford ES, editors. Cardiovascularand Vascular Disease of the Aorta. Philadelphia,PA: W.B. Saunders Company, 1997:1–5.
2. Hiratzka LF, Bakris GL, Beckman JA, et al.2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and man-agement of patients with thoracic aortic dis-ease. A report of the American College ofCardiology Foundation/American Heart Associa-tion Task Force on Practice Guidelines, Amer-ican Association for Thoracic Surgery,American College of Radiology, AmericanStroke Association, Society of CardiovascularAnesthesiologists, Society for CardiovascularAngiography and Interventions, Society of
Interventional Radiology, Society of ThoracicSurgeons, and Society for Vascular Medicine.J Am Coll Cardiol 2010;55:e27–129.
3. Svensson LG, Crawford ES, Hess KR,Coselli JS, Safi HJ. Dissection of the aorta anddissecting aortic aneurysms. Improving early andlong-term surgical results. Circulation 1990;82:IV24–38.
4. Svensson LG, Labib SB, Eisenhauer AC,Butterly JR. Intimal tear without hematoma: animportant variant of aortic dissection that canelude current imaging techniques. Circulation1999;99:1331–6.
5. Chin AS, Willemink MJ, Kino A, et al. Acutelimited intimal tears of the thoracic aorta. J AmColl Cardiol 2018;71:2773–85.
6. Waxman DA, Kanzaria HK, Schriger DL. Unrec-ognized cardiovascular emergencies amongMedicare patients. JAMA Intern Med 2018;178:477–84.
7. Roselli EE, Idrees JJ, Bakaeen FG, et al. Evolu-tion of simplified frozen elephant trunk repair foracute DeBakey Type I dissection: midterm out-comes. Ann Thorac Surg 2018;105:749–55.
8. Svensson LG, Pillai ST, Rajeswaran J, et al.Long-term survival, valve durability, and reoper-ation for 4 aortic root procedures combined withascending aorta replacement. J Thorac CardiovascSurg 2016;151:764–71.e4.
KEY WORDS aorta, dissection, dissectionclasses and types


















