LUCAS MACIEL RABELLO - Cloud Object Storage · Obrigado por estarem comigo a milhares de Km, seja...
98
Londrina 2013 CENTRO DE PESQUISA EM CIÊNCIAS DA SAÚDE MESTRADO EM CIÊNCIAS DA REABILITAÇÃO LUCAS MACIEL RABELLO COMPARAÇÃO DA ELETROMIOGRAFIA DE SUPERFÍCIE E ULTRASSONOGRAFIA DE IMAGEM NA ANÁLISE DO COMPORTAMENTO DO MÚSCULO OBLÍQUO EXTERNO EM DIFERENTES TAREFAS LUCAS MACIEL RABELLO
Transcript of LUCAS MACIEL RABELLO - Cloud Object Storage · Obrigado por estarem comigo a milhares de Km, seja...
Londrina 2013
CENTRO DE PESQUISA EM CIÊNCIAS DA SAÚDE MESTRADO EM CIÊNCIAS DA REABILITAÇÃO
LUCAS MACIEL RABELLO
COMPARAÇÃO DA ELETROMIOGRAFIA DE SUPERFÍCIE E
ULTRASSONOGRAFIA DE IMAGEM NA ANÁLISE DO
COMPORTAMENTO DO MÚSCULO OBLÍQUO EXTERNO EM
DIFERENTES TAREFAS
LUCAS MACIEL RABELLO

Londrina 2013
COMPARAÇÃO DA ELETROMIOGRAFIA DE SUPERFÍCIE E
ULTRASSONOGRAFIA DE IMAGEM NA ANÁLISE DO
COMPORTAMENTO DO MÚSCULO OBLÍQUO EXTERNO EM
DIFERENTES TAREFAS
Dissertação apresentada ao Programa de Pós-Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina - UEL e Universidade Norte do Paraná - UNOPAR), como requisito parcial à obtenção do título de Mestre em Ciências da Reabilitação.
Orientador: Prof. Dr. Rubens Alexandre da Silva Junior.

LUCAS MACIEL RABELLO
COMPARAÇÃO DA ELETROMIOGRAFIA DE SUPERFÍCIE E
ULTRASSONOGRAFIA DE IMAGEM NA ANÁLISE DO
COMPORTAMENTO DO MÚSCULO OBLÍQUO EXTERNO EM
DIFERENTES TAREFAS
Dissertação apresentada ao Programa de Pós-Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina [UEL] e Universidade Norte do Paraná [UNOPAR]), como requisito parcial à obtenção do título de Mestre em Ciências da Reabilitação.
BANCA EXAMINADORA
___________________________________
Prof. Dr. Rubens Alexandre da Silva Jr. (Orientador)
Universidade Norte do Paraná
____________________________________ Prof. Dr.Rodrigo Franco de Oliveira
(Membro interno) Universidade Norte do Paraná
____________________________________ Prof. Dr. Leandro Ricardo Altimari
(Membro externo) Universidade Estadual de Londrina
Londrina, _____de ___________de _____.

DEDICATÓRIA
Dedido este trabalho à minha família e todos
aqueles que me incentivaram e me apoioaram
até a concretização deste sonho.

AGRADECIMENTOS
Primeiramente, agradeço a Deus. Agradeço a Ele por estar presente durante
toda a minha vida, nos momentos alegres e tristes, nos momentos em que decisões
importantes deveriam ser tomadas e Ele me mostrou o caminho a seguir. Foi Ele
quem ouviu minhas perguntas e me deu todas as respostas (no tempo certo). Meu
Deus, obrigado por abençoar meus passos e de todos que estiveram nesta jornada
comigo. “Não esqueço o que fez por mim./ Entregando sua vida em meu lugar. /
Nunca ninguém, Senhor, me amou de modo assim. / Eu descobri, ao Seu lado é
meu lugar.” – Rosa de Saron)
Aos meus pais, Beth e Heleno, obrigado por me apoiarem durante esses dois
anos de Mestrado (e durante os 26 anos da minha vida) e por estarem ao meu lado
quando aceitei o convite de estudar no Canadá. Tenho certeza que não teria
suportado toda a distância e não teria encarado todos os desafios se vocês não
estivessem tão presentes durante TODOS os dias!
Obrigado a minha Vó Elza e meu Tio Osvaldo por sempre me fazerem sentir
muito especial e fazendo a distância entre a gente tornar-se mínima! Muito Obrigado
por esse amor! E como minha vó disse: “Nunca estivemos tão próximos.”
Agradeço ao meu irmão Mateus e minha cunhada Silvia por também dividirem
esse momento comigo e por me suportarem! E aproveitando, agradeço a Fer. Minha
amiga, minha irmã... tudo!
A minha Família Maciel, tias, tios, primas e primo, muito obrigado! Sei que não
podemos estar juntos sempre, mas nem por isso deixamos de estar próximos!
Agradeço aos meus Avós que guiam meus passos ao lado de Deus e que
tenho certeza que estão vibrando com essa conquista. Obrigado!
Aos meus amigos e amigas de longa data e aos amigos que fiz durante os
dois anos de mestrado, muito obrigado! Sei que muitas vezes tive que abrir mão de
sair com vocês devido aos compromissos (principalmente nas últimas semanas).
Obrigado por estarem comigo a milhares de Km, seja por mensagens ou por Skype!
Vocês sempre me disseram: “Calma, vai dar tudo certo!”. E vocês estavam certos!
Aos meus amigos de Banda (Dirty Harrys). Juliano, Marcos, Zé e meu irmão! E
obrigado aos meus colegas Canadenses!! Em especial a Audrey, Annie Phan,
Annie-Claude, Hugo, Nabil e Alex! Obrigado ao Phillipe Paquette, que foi
fundamental para a realização deste Projeto.
Obrigado aos meus companheiros de Mestrado! Aprendemos juntos,
compartilhamos conhecimentos, alegrias e também momentos difíceis... foram horas
de conversas, de estudos durante dias e noites. Mas também tínhamos nossos
momentos de tranqüilidade nos churrascos e nas “reuniões” na Casa da Cachaça!
Em especial, agradeço o “Grupo”, vocês são pra sempre!
Aos Professores do Mestrado, muito obrigado! Obrigado por ensinarem
“conteúdos”, mas também muito obrigado por ensinarem “valores”. Obrigado a
Coordenação (Prof Fábio e Prof Vanessa).
Aos funcionários do Mestrado, em especial o secretário Gleydson. Sempre
disponível para ajudar. Além de secretário, tornou-se um grande amigo! Obrigado!
Agradeço os Engenheiros e colaboradores que estiveram comigo em
Montreal. Aos engenheiros Phillipe, Youseff (e Seléna), Michel e Daniel. Aos
professores do Instituto, aos alunos de Doutorado e Mestrado e todos os
funcionários. Em especial, obrigado ao engenheiro Hakim por desenvolver o
software para minhas análises e por estar sempre disponível!
Meus amigos de Laboratório. André, Rogério, Ana, Stheace, Camila, Patrícia
e todos os outros que estiveram com a gente durante esses 2 anos. A união de um
grupo nos leva a sonhos muito maiores! As publicações em Revista são
conseqüências de um trabalho bem feito. E obrigado aos professores que nos
orientam!
Agora, um “obrigado” mais do que especial. Professor Rubens, obrigado por
confiar em mim desde o começo. Foi você que confiou em mim e me deu a
oportunidade de realizar sonhos. Muito obrigado por ser mais do que um orientador,
obrigado por ser um Amigo! Compartilhamos nossas alegrias e nossas dificuldades.
E você me proporcionou a oportunidade de viver algo “mágico”! Obrigado por ser tão
diferente dos “outros” e por acreditar em valores a cima do que estamos
acostumados. Obrigado pela oportunidade de experimentar o que você viveu
durante anos em Montreal. A minha responsabilidade era muito grande (visto que
até hoje eles possuem um Banner fixo a parede de um dos seus trabalhos), tentei
não decepcionar! E tenho certeza que esta parceria só esta começando. Estamos
juntos para o que der e vier!
Ao meu orientador em Montreal, Dany Gagnon. Obrigado por me aceitar e
obrigado por aceitar esse desafio. Não foi fácil fazer um projeto em 6 meses, mas
conseguimos (obrigado por acreditar e confiar desde o começo!)! Obrigado por todos
os ensinamentos e por compartilhar todo conhecimento. Aprendi muitas coisas
novas e tive a oportunidade de realizar um trabalho maravilhoso. E que esta parceria
ainda possa ir além!
E ao Professor Christian Larivière que participou do nosso Projeto e orientou
o trabalho, compartilhando seu conhecimento. Obrigado pelos seus ensinamentos e
obrigado por me mostrar visões diferentes de um mesmo conteúdo.
ENFIM, OBRIGADO A TODOS VOCÊS!
“Quem acredita sempre alcança.”

“Todas as vitórias ocultam uma abdicação.”
(Simone de Beauvoir)
RABELLO, Lucas Maciel. Comparação da eletromiografia de superfície e ultrassonografia de imagem na análise do comportamento do músculo oblíquo externo em diferentes tarefas. 2013. 89 folhas. Trabalho de Conclusão de Curso
do Programa de Pós Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina [UEL] e Universidade Norte do Paraná [UNOPAR]) – Universidade Norte do Paraná, Londrina, 2012.
RESUMO
A parede abdominal é composta de múltiplos músculos com arquitetura diferente e com o papel de controlar os movimentos do tronco nos três planos e promover a estabilidade da coluna lombar. Todavia, estes músculos estão envolvidos nas patologias comuns da coluna vertebral, como a dor lombar crônica. No processo de reabilitação é essencial avaliar especificamente a função dos músculos abdominais utilizando os sistemas de análise de alta tecnologia como o ultrassom de imagem (USI) e a eletromiografia (EMG) de superficie. A relação entre a atividade elétrica do músculo medida, por meio da EMG, e a espessura muscular, proveniente da medida do USI, permanecer ainda incerta, especialmente para os músculos abdominais superficiais tais como o oblíquo externo.O objetivo do presente estudo foi determinar a associação entre a espessura muscular e a atividade eletromiográfica do músculo oblíquo externo (OE). Dezoito sujeitos foram recrutados para realizar uma contração isométrica em rampa, de intensidade entre 5 à 50% de uma contração voluntária máxima, em três diferentes direções do movimento: flexião, flexão lateral e rotação do tronco. Os sujeitos foram posicionados em posição sentada no dinamômetro e dois eletrodos de EMG foram posicionados superficialmente sobre o músculo OE direito em dois ângulos diferentes (18º e 27º). O transdutor do ultrassom foi posicionado cinco mm abaixo dos eletrodos e as imagens foram registradas simultaneamente com a atividade elétrica do músculo. De acordo com a análise de variância, o músculo oblíquo externo foi mais ativo durante a flexão anterior e a rotação do tronco em comparação a flexão lateral (P < 0,05). Também, o comportamento da EMG entre os níveis de força (5-50%) não foi comparado com as alterações da espessura muscular. Somente para as medidas de EMG, os níveis de força durante a contração em rampa foram significamente diferentes (P < 0,05) entre eles (do menor para o maior). A relação entre a EMG e o USI foi determinada para cada sujeito individualmente devido a alta variabilidade entre os mesmos. A correlação entre as duas medidas variou de fraca a forte para as tarefas avaliadas. O presente estudo conclui que a ultrassonografia de imagem pode ser utilizada para avaliar a atividade do músculo oblíquo externo durante atividades de baixa intensidade (até 30% da CVM). Este resultado implica no uso do ultrassom de imagem no processo de avaliação e intervenção da função dos músculos do tronco em programas de reabilitação. Palavras chave: eletromiografia, ultrassom de imagem, músculos abdominais.

RABELLO, Lucas Maciel. Comparison of surface electromyography and ultrasound imaging in the analysis of the behavior of the external oblique muscle in different tasks. 2013. 89 pages. Trabalho de Conclusão de Curso do
Programa de Pós Graduação em Ciências da Reabilitação (Programa Associado entre Universidade Estadual de Londrina [UEL] e Universidade Norte do Paraná [UNOPAR]) – Universidade Norte do Paraná, Londrina, 2012.
ABSTRACT
The abdominal wall is composed of multiples muscles with different architecture and potential roles in controlling the movements of the trunk in three planes and promote stability of the lumbar spine. Though, those muscles are involved in common pathologies of the spine, as chronic low back pain. During the rehabilitation process, it is essential to assess specifically the function of the abdominal muscles using high-tech analysis system such as ultrasound imaging (USI) and superficial electromyography (EMG). The relationship between electrical muscle activity (measured with EMG) and the muscle thickness (measured with USI) remains still unclear, specially to the superficial abdominal muscle, such as the external oblique. The purpose of the present study was to determine the association between the relative muscular thickness change and the EMG muscular utilization ratio of the external oblique (EO) muscle. Eighteen subjects were recruited to perform ramp isometric, of intensity between 5 to 50% of the maximum voluntary contraction, in three different movement directions: flexion, lateral bending and rotation of the trunk. Subjects were positioned sitting on the dynamometer and two EMG electrodes were placed superficially over the right EO muscle, with different angles (18º and 27º). The US probe was placed five mm above the electrodes and the US images were registred simultaneously with the electrical muscle activity (EMG). According to analysis of variance, the external oblique muscle was more active during the anterior flexion and rotation effort, compared to the lateral bending (P<0,05). Also, the behavior of the EMG between the force levels (5 to 50%) was not compered to the muscle thickness changes (USI). Only for the meaures of the EMG, force levels during the ramp contraction were significant different (P < 0,05) between them (from lowest to highest). The relationship between the EMG and the USI was determined for each subject due the great variance between them. The correlation between the two measures ranged from poor to strong for tasks assessed. The present study concluded that ultrasound imaging can be used to evaluate the activity of the external oblique muscle during low intensity activities (up to 30% of MVC). These results implicate in the use of the ultrasound imaging in the evaluation and intervation process in the function of trubk muscles, specifically the external oblique muscle, in a rehabilitation program. Key words: electromyography, ultrasound imaging, abdominal muscles.

LISTA DE ILUSTRAÇÕES
Figura 1 – Músculos que compõe a parede abdominal .......................................... 23
Figura 2 – Posição do sujeito e do avaliador durante o teste .................................. 50
Figura 3 – Gabarito desenhado pelos autores para padronização da posição
dos eletrodos da EMG e do transdutor do USI ......................................................... 51
Figura 4 – Imagem do US descrevendo os locais utilizados para mensuração
da espessura do músculo oblíquo externo .............................................................. 52

LISTA DE TABELAS
Tabela 1 – Valores de %EMG e %Thickness em 5-50% da contração em
rampa para a direção em flexão ............................................................................... 53
Tabela 2 – Valores de %EMG e %Thickness em 5-50% da contração em
rampa para a direção em rotação ........................................................................... 54
Tabela 3 – Coeficiente de correlação de Pearson entre as médias dos valores
de %EMG e %Thickness em 5-50% da contração em rampa durante a flexão ....... 55
Tabela 4 – Coeficiente de correlação de Pearson entre as médias dos valores
de %EMG e %Thickness em 5-50% da contração em rampa durante rotação ........ 56

LISTA DE ABREVIATURAS E SIGLAS
RA Reto Abdominal / Rectus Abdominis
OE Oblíquo Externo
OI Oblíquo Interno
TrA Transverso do Abdome / Transversus Abdominis
EMG Eletromiografia / Electromyography
USI Ultrassom de Imagem / Ultrasound Imaging
FTL Fáscia Tóraco-lombar
RM Ressonância Magnética
LBP Low Back Pain
MRI Magnetic Resonance Imaging
SEMG Superficial Electromyography
EO External Oblique
IO Internal Oblique
BMI Body Mass Index
CRIR Center of Interdisciplinary Research in Rehabilitation of the Greater
Montreal
mm Milímetros / Millimeters
s Segundos / Second
MVC Maximum Voluntary Contraction
MVIC Maximum Voluntary Isometric Contraction
RMS Root Mean Square
TLF Thoracolumbar Fascia
DLC Dor Lombar Crônica
SUMÁRIO
1 INTRODUÇÃO ....................................................................................................... 12
2 OBJETIVOS.........................................................................................................15
2.1 OBJETIVO GERAL.................................................................................................15
2.2OBJETIVO ESPECÍFICO...........................................................................................15
3 REVISÃO DE LITERATURA - CONTEXTUALIZAÇÃO ........................................ 16
3.1 MÚSCULOS ABDOMINAIS ......................................................................................... 16
3.1.1 Orientação Dos Fascículos Musculares Do Abdome ....................................... 16
3.2 FUNÇÃO DOS MÚSCULOS ABDOMINAIS .................................................................... 17
3.3 PRINCIPAIS PATOLOGIAS DO TRONCO ASSOCIADAS AOS MÚSCULOS ABDOMINAIS ...... 18
3.4 MÉTODOS DE AVALIAÇÃO DA FUNÇÃO DO TRONCO .................................................... 19
3.4.1 Emetromiografia (EMG) .................................................................................... 19
3.4.2 Ultrassom de Imagem (USI) ............................................................................. 20
3.4.2.1 “Thickness” muscular .................................................................................... 21
3.5 Evidências Científicas Entre As Medidas De EMG e USI Na Avaliação Dos
Músculos Abominais.................................................................................................. 22
4 ARTIGO: ......... ....................................................................................................... 26
CONCLUSÃO GERAL .............................................................................................. 57
REFERÊNCIAS ........................................................................................................ 58
ANEXOS ................................................................................................................... 64
ANEXO A – Normas de formatação do periódico Journal of Electromyography
and Kinesiology ......................................................................................................... 65
ANEXO B – Carta de aceite do Comitê de Ética Local e Protocolo .......................... 77
ANEXO C – Termo de Conscentimento Livre e Esclarecido ..................................... 87

12
1 INTRODUÇÃO
Os principais problemas associados à disfunção da coluna vertebral,
como a lombalgia crônica de origem não específica, têm relação com os músculos
do tronco, por exemplo, os músculos abdominais. Os quatro músculos que compõe a
parede abdominal, reto abdominal (RA), oblíquo externo (OE), oblíquo interno (OI) e
o transverso do abdome (TrA), são responsáveis por uma variedade de funções
essenciais nas atividades do corpo humano. Estes músculos produzem torque
necessário para realizar os movimentos de flexão, rotação e inclinação lateral da
coluna vertebral1,2, sustentam a cavidade abdominal, preservam a estabilidade da
coluna lombar durante tarefas simples como levantar-se, sentar-se e locomover-se3,4
assim como tarefas mais complexas durante os movimentos dinâmicos e com
sobrecargas5,6 e por fim, auxiliam também na respiração7. Sendo assim, esses
músculos apresentam um papel extremamente importante na prevenção e no
tratamento de doenças e disfunções da coluna vertebral8.
Bergmark (1989)9 propôs uma definição para tais músculos do
tronco quanto a sua funcionalidade. Segundo o autor, estes músculos responsáveis
pelo controle funcional do tronco podem ser classificados em dois grupos: 1) o
primeiro grupo, composto pelos músculos que se inserem diretamente na vértebra
lombar (multífidos, TrA e OI), os quais promovem a estabilidade segmentar da
coluna; e 2) o segundo grupo que consiste de grandes músculos geradores de
torque articular, mas sem inserções diretas na coluna lombar. Estes músculos
controlam os movimentos mais amplos do tronco (em grandes amplitudes de
movimento) e promovem também a estabilidade da coluna vertebral. Os músculos
que compõe este segundo grupo são: RA, OE e eretor da coluna torácica. Para o
interesse do presente trabalho e devido à utilização da eletromiografia de superfície,
somente uma investigação aprofundada do músculo obliquo externo (OE) será
realizada.
Apesar do número crescente de estudos desenvolvidos para avaliar
a funcionalidade do tronco com ênfase na prevenção e intervenção das disfunções
da coluna vertebral, pouco se sabe sobre os mecanismos específicos dos músculos
abdominais quando agindo de forma individual e/ou em conjunto com outras
estruturas passivas e ativas do tronco10. Estudos prévios avaliaram o papel dos
músculos abdominais com uso da eletromiografia (EMG) de superfície durante a
13
execução de diferentes tarefas para melhor entendimento do papel desses
músculos11. Sabe-se que o músculo OE está envolvido na orientação da coluna
vertebral12. Seroussi & Poupe (1987)13 observaram que o músculo OE, por exemplo,
se torna ativo durante o movimento sustentado de inclinação lateral do tronco em
indivíduos saudáveis. McGill (1991)14 observou também com uso da EMG que este
músculo, assim como o OI, participa dos movimentos de rotação do tronco durante
uma tarefa resistida. Outras evidências apontam que os músculos abdominais são
ativos simultaneamente para múltiplas funções do tronco15,16.
Por outro lado, a atividade dos músculos abdominais pode ser
influenciada pela postura adotada pelo indivíduo e, conseqüentemente, pela
estabilidade articular12,17,18. Em um estudo de Snijders et al (1995)19, observou-se
uma maior ativação dos músculos abdominais na posição sentada quando
comparada a posição supina. Porém, os mesmo autores, comparando a posição
sentada versus ortostática, encontraram uma menor ativação dos músculos
abdominais na posição sentada, devido o aumento na estabilidade da articulação
sacroilíaca20. A avaliação dos músculos abdominais na posição sentada é de
fundamental importância visto que o sedentarismo da vida moderna faz com que os
indivíduos permaneçam nesta posição por mais tempo21, levando ao
descondicionamento dos músculos do tronco, à sobrecarga lombar e ocasionando
assim, uma maior incidência de patologias da coluna vertebral22. Portanto, a
necessidade de se avaliar e compreender a função destes músculos para tomadas
de decisões clínicas na reabilitação é de suma importância.
A cada dia novos métodos e protocolos envolvendo a alta tecnologia
surgem para avaliar o papel dos músculos do tronco. Nos últimos anos, métodos de
avaliação desta musculatura, como a ultrassonografia de imagem (USI), tornaram-se
mais difundidos. Este sistema permite avaliar isoladamente o papel de alguns
músculos da parede abdominal, como por exemplo, as ações de um dos principais
músculos, o OE, durante diferentes tarefas motoras específicas23. A confiabilidade e
a validade do uso deste novo método para medidas da geometria muscular, quando
comparada a outras técnicas (ex: EMG, ressonância magnética), têm sido
confirmada na literatura24-27. Entretanto, ainda são necessários mais estudos para
avaliar a utilização da ultrassonografia de imagem para avaliar os músculos
abdominais. As mudanças nas medidas da espessura (thickness) dos músculos da
parede abdominal têm sido correlacionadas com o aumento dos valores (RMS)

14
obtidos com a EMG durante uma contração isométrica submáxima na posição
sentada reclinada28. Todavia, um recente estudo (2007)23 comparando a ativação do
músculo OE na posição supina por meio da EMG e USI, concluiu que as mudanças
na espessura muscular utilizadas como medida de atividade muscular deveriam ser
vistas com precaução na avaliação da funcionalidade do tronco devido a falta de
consistência entre as medidas. Sendo assim, mais estudos são ainda necessários
para melhor compreender o comportamento destes músculos em diferentes
posições, direções do movimento e sob a ação de diferentes intensidades de
contração muscular.

15
2 OBJETIVOS
2.1. Geral
Quantificar a espessura (thickness) muscular com o ultrassom de
imagem e a porcentagem da ativação muscular com a eletromiografia do oblíquo
externo direito durante as contrações unidirecionais em rampa na posição sentada
em indivíduos saudáveis.
2.2. Específicos
Determinar em qual(ais) direção(ões) do movimento o músculo
oblíquo externo apresenta maior ativação. E então para esta(s) direção(ões)
somente:
a) comparar os níveis de contração muscular submáxima para as
principais variáveis (atividade elétrica e thcinkness muscular) com a finalidade de
determinar se as intensidades de contração muscular distinguem tanto nas
mudanças da espessura quanto na ativadade elétrica; e
b) determinar a associação entre as medidas de espessura muscular
e atividade eletromiográfica do músculo oblíquo externo.
.
16
3 REVISÃO DE LITERATURA – CONTEXTUALIZAÇÃO
3.1 MÚSCULOS ABDOMINAIS
A musculatura abdominal pode ser dividida em parede abdominal
lateral, composta pelo oblíquo externo (OE), oblíquo interno (OI), e o transverso do
abdômen (TrA); e parede anterior, composta pelo reto abdominal (RA) e a fáscia
abdominal anterior27.
Em geral, estes músculos são importantes para funcionalidade do
tronco para os diferentes movimentos corporais. Também, eles preservam e auxiliam
na estabilidade da região lombar quanto aos stress e as sobrecargas nas estruturas
passivas da coluna vertebral29. É importante ressaltar que a disfunção desses
músculos pode promover a instabilidade da coluna vertebral, aumentar as
sobrecargas e consequentemente os riscos de lesões nas estruturas ligamentares e
articulares da região lombar. Alguns autores apontam que a instabilidade da coluna
vertebral leva a dor lombar crônica e as incapacidades funcionais em adultos30,31.
3.1.1 Orientação dos Fascículos Musculares do Abdome
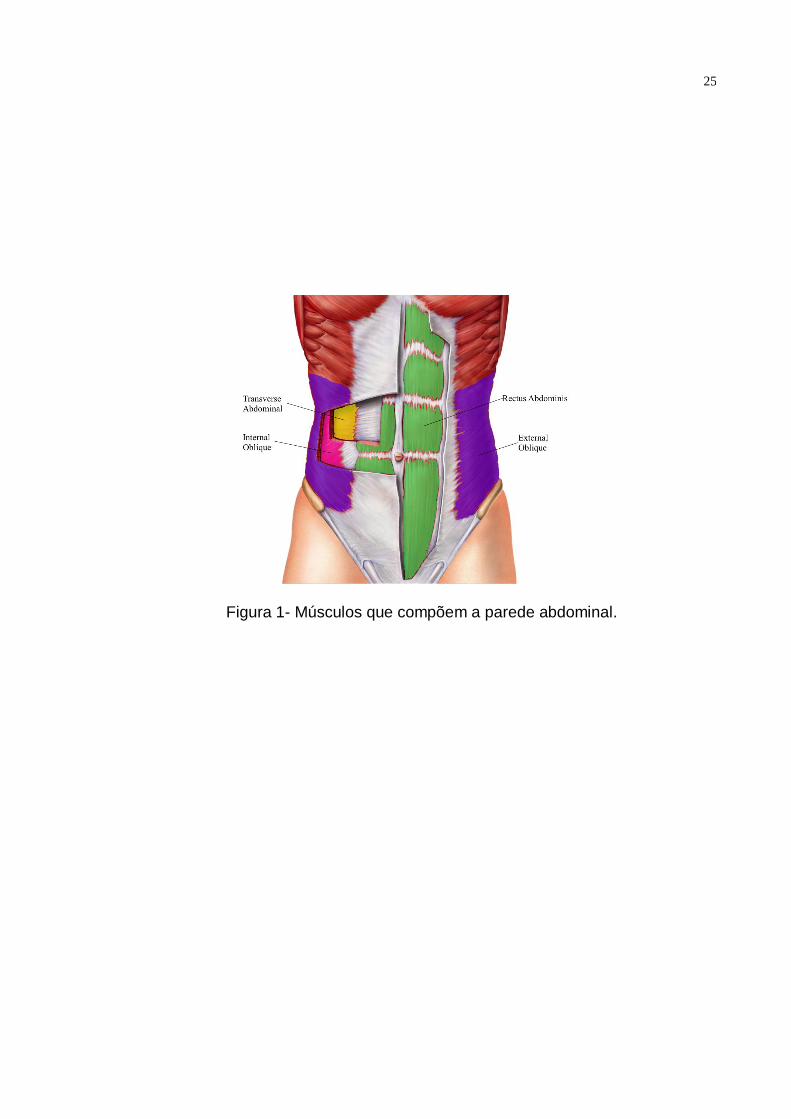
A parede abdominal (Figura 1) pode ser dividida em: parede abdominal
lateral e parede abdominal anterior.
Os músculos da parede abdominal lateral podem ser divididos em três
regiões: superior (acima da décima primeira cartilagem costal), medial (entre a
décima primeira cartilagem e a crista ilíaca) e inferior (abaixo da crista ilíaca)35. Os
músculos que compõe a parede abdominal lateral são: OE, OI e TrA.
Em relação a parede abdominal anterior, esta é composta pelo
músculo reto abdominal e pela fáscia abdominal anterior. A linha alba divide a
parede abdominal anterior em direita e esquerda27.
As fibras musculares do OE se originam na borda externa das oito
costelas inferiores e se inserem na linha alba e na metade ou no terço anterior da
crista ilíaca33,34. Alguns autores descrevem a inserção do OE na fáscia toracolombar
(FTL) nos níveis lombares superiores35, enquanto outros autores descrevem a
localização na margem posterior livre34. Biomecanicamente, o músculo OE
17
apresenta três direções de fibras (ventral, lateral e dorsal), sendo cada uma dessas
responsáveis por produzir diferentes forças direcionais. A contração unilateral deste
músculo resulta na rotação do tronco para o lado oposto e quando contraído
bilateralmente, realiza a flexão anterior do tronco e aumenta a pressão
intrabdominal36.
O músculo OI se origina nos dois terços anteriores da crista ilíaca e a
na metade ou no terço lateral do ligamento inguinal, e se insere nas cartilagens
costais inferiores, na linha alba e na sínfise púbica33,34.
Já o músculo TrA se origina na superfície interna da cartilagem das
seis costelas inferiores, da FTL, nos dois terços anteriores da crista ilíaca e no terço
lateral do ligamento inguinal e se insere anteriormente na linha alba e na pelve33,34.
O RA tem a maior espessura de todos os músculos abdominais. Este
músculo se origina no processo xifóide e nas cartilagens costais (da quinta a sétima
costelas) e se insere na sínfise púbica, crista púbica e tubérculo púbico37.
A fáscia abdominal lateral para o músculo RA é um arranjo complexo
de conexões aponeuróticas de cada músculo que compõe a parede abdominal
lateral e o “RA sheath” (compartimento aponeurórico onde o reto abdominal esta
contido)33,34,38. As fibras de cada músculo da parede lateral cruzam a linha média e
se unem às fibras dos músculos que compõe a parede abdominal lateral
contralateral para formar a linha Alba. Esta linha auxilia na distribuição de cargas
entre os lados para parede abdominal27.
3.2 FUNÇÃO DOS MÚSCULOS ABDOMINAIS
Sabe-se que o papel principal dos músculos abdominais é de gerar
força para produzir movimento do tronco e estabilização da coluna vertebral, em
especial da região lombar. Porém, ainda não está bem elucidado os mecanismos de
ação conjunta e individual de cada músculo para cada tipo de movimento do
tronco39. Diversos autores têm estudado a função dos músculos da parede
abdominal anterolateral nos últimos anos. Três modelos predominam para a função
desses músculos em associação com os músculos paraespinhais: 1) a cocontração
entre os músculos flexores e extensores do tronco40,41; 2) a integração de todos os
músculos durante uma tarefa específica42,43, e 3) a função muscular local versus
global9,44,45.
18
Os resultados do trabalho de Gardner-Morse et al (1998)40, mostraram
que os músculos agonistas e antagonistas coativados aumentam a estabilidade da
coluna lombar. Esses achados suportam a hipótese de que os músculos funcionam
não somente como promotores de torque articular durante o movimento do tronco,
mas também como molas estabilizadoras na contenção de sobrecargas articulares
da coluna vertebral41.
Para Bergmark (1989)9, os músculos transverso do abdomem e oblíquo
interno são parte de um grupo muscular capaz de promover a estabilidade
segmentar da coluna. Enquanto que, os músculos reto abdominal e oblíquo externo
são parte de um segundo grupo responsável pelo controle dos movimentos amplos
do tronco além de promoverem a estabilidade da coluna vertebral. Outra teoria,
conforme Richardson et al (1999)44, salienta que os músculos abdominais laterais
são teoricamente responsáveis pelo controle do movimento e por promover a
estabilidade do tronco para atividades funcionais, enquanto que o músculo
transverso do abdome é responsável pelo suporte e proteção da coluna46.
Já a teoria de Panjabi (1992)29,30 sugere que o sistema de estabilidade
da coluna é composto por três subsistemas: 1) Subsistema passivo (vértebras,
facetas articulares, discos intervertebrais, ligamentos espinhais e capsulas
articulares) que promove a estabilidade intrínsica da coluna; 2) Subsistema ativo
(músculos e tendões ao redor da coluna) responsável pela estabilidade dinâmica e
os movimentos da coluna vertebral; e 3) Subsistema neural (central e periférico, tais
como os receptores sensitivos localizados nos ligamentos, tendões e músculos)
associado ao controle motor. Este último subsistema é responsável por avaliar e
determinar os requisitos de estabilidade e coordenação das respostas musculares
do tronco. Para Panjabi, a instabilidade toda da coluna vertebral é presente quando
um ou mais destes subsistemas não funcionam adequadamente ou são
deteriorados.
3.3 PRINCIPAIS PATOLOGIAS DO TRONCO ASSOCIADAS AOS MÚSCULOS ABDOMINAIS
As disfunções lombo-pélvicas, como espondilólise, espondilolistese,
dor pélvica posterior associada à gravidez e dor lombar crônica são associadas com
a disfunção dos músculos do tronco, incluindo os músculos abdominais27.

19
A dor lombar tem sido uma das patologias do tronco de maior estudo e
pesquisa nos últimos anos. Em adultos jovens, o descondicionamento muscular e a
má coordenação motora dos músculos do tronco estão associados à dor lombar
crônica47. A dor lombar crônica é uma patologia comum, com incidência superior a
80%48, e uma prevalência em crescimento contínuo mundialmente49.
Os músculos abdominais têm um importante papel na prevenção e no
processo de intervenção das disfunções da coluna vertebral. Programas de
treinamento de estabilização da coluna lombar, o qual requer a participação
constante desta importante musculatura, têm demonstrado resultados positivos
quanto aos sintomas clínicos (redução da dor, incapacidades e recorrência das
dores) de pacientes com dor lombar crônica50-52. Assim, a utilização de novos
métodos de avaliação desta musculatura, que sejam válidos e fidedignos, é de suma
importância para o diagnóstico e as tomadas de decisões clínicas quanto às
diferentes intervenções propostas para conter a disfunção desta musculatura.
3.4 MÉTODOS DE AVALIAÇÃO DA FUNÇÃO DO TRONCO
Uma das técnicas mais utilizadas para avaliação da ativação muscular
é a eletromiografia (EMG) de superfície. A EMG é definida como o registro da
atividade elétrica muscular. O registro do sinal eletromiografico pelo equipamento é
a soma do potencial de ação de diferentes unidades motoras ativas durante a
contração muscular53. Recentemente outros métodos têm sido empregados na
prática clínica e para pesquisas científicas para avaliação da atividade muscular. Um
desses métodos é a Ultrasonografia de imagem (USI).
Esses dois métodos de avaliação serão abordados nas próximas sessões
deste trabalho.
3.4.1 Eletromiografia (EMG)
A eletromiografia é amplamente utilizada por possibilitar a observação
do comportamento muscular durante atividades funcionais específicas, além de
possibilitar a quantificação da atividade muscular elétrica para descrição e
comparação entre diferentes músculos e indivíduos54,55. Além disso, a EMG pode ser
relacionada com a quantidade de força desenvolvida por um músculo56.

20
Para avaliação dos músculos abdominais alguns autores utilizam a
EMG intramuscular50,57, porém, devido ao alto custo, desconforto do paciente e a
dificuldade de aplicação desta técnica na prática clínica58, a EMG de superfície vem
sendo empregada por diversos autores23,59,60.
A avaliação por meio da eletromiografia de superfície tornou-se um
método popular de investigação da função muscular. Em diversos estudos clínicos, a
EMG é utilizada para analisar a função dos músculos do membro superior, inferior e
tronco61, as disordens do movimento62 e alteraçoes posturais relacionadas as cargas
de trabalho dentro da ergonomia63.
Uma forma de interpretar os sinais provenientes da EMG, é quantificar
os dados brutos em raiz quadrada da média da amplitude do sinal, chamada de:
RMS – Root Mean Square. Esta forma de análise contempla as alterações
fisiológicas do sinal eletromiográfico, e reflete o número de unidades motoras ativas,
além da frequência de disparo dessas mesmas unidades motoras e a forma do
potencial de ação64. Outras formas de se interpretar os sinais da EMG são
destacadas na literatura, principalmente no domínio da frequência65. Todavia,
somente a forma RMS será aplicada no presente estudo.
3.4.2 Ultrassom de Imagem (USI)
O Ultra-ssom de imagem (USI) é utilizado na área médica desde os
anos 50. O principal uso do USI continua sendo na radiologia tradicional, a qual
considera as características morfológicas e a integridade estrutural de vários órgãos
e tecidos. Entretanto, como esta tecnologia foi comprovada como uma forma segura,
portátil, objetiva e relativamente barata para a realização de exames, a diversidade
de aplicações estendeu além da prática médica66.
Em 1968, Ikai e Fukunaga (1968)67 fizeram o primeiro relato de uma
imagem muscular relacionada a reabilitação. Neste estudo, os autores relacionaram
o comprimento e espessura do membro superior (ex: braço) com a força muscular.
Porém, foi o trabalho do Dr Archie Young et al na Universidade de Oxford em 1980
que deu início ao uso do USI pelos fisioterapeutas. A descoberta do seu trabalho foi
como a atrofia dos membros inferiores era substimado com uma fita métrica68.
Desde então, o USI vem sendo usado para a reabilitação musculoesquelética.
21
Em maio de 2006, um simpósio organizado pela US Army-Baylor
University Doctoral Program em San Diego-Tx foi proposto um consenso o qual
declara: “Ultra-som de imagem para reabilitação é um procedimento usado pelo
fisioterapeuta para avaliar a morfologia e função dos músculos e tecidos moles
adjacentes durante os exercícios físicos e tarefas funcionais”69.
O USI pode avaliar a espessura muscular e a área de secção-
transversa. Este método pode determinar a atrofia muscular70,71 e os déficits da
ativação26,28,72. Além disso, a espessura muscular obtida pelo ultrassom pode ser
interpretada com um indicador de geração de força muscular73. Em estudos
anteriores, autores observaram uma relação positiva entre a espessura dos
músculos da mastigação e a magnitude da força da mordida74,75.
Em uma comparação feita entre a ressonância magnética e o USI,
Hides et al (2006)24 observaram que as medidas da espessura muscular do
transverso abdominal e do oblóquo interno, assim como também o deslocamento da
fáscia, eram correlacionados com as medidas obtidas por meio da ressonância
magnética. Em uma revisão sistemática, Hebert et al (2009)76 concluiram que apesar
do USI apresentar uma confiabilidade e precisão adequada para a quantificação da
espessura e da área-transversa dos músculos abdominais e lombares, ainda são
necessários novas pesquisas para aumentar o entendimento da área.
3.4.2.1 Espessura muscular
Considerando-se a espessura relativa dos músculos abdominais, o
músculo RA é o de maior espessura enquanto o músculo TrA é o de menor. Em
indivíduos sem história de dor lombo-pélvica, os músculos RA, OI, OE, e TrA
representam 35%, 28% , 22%, e 13% de toda espessura somada do músculo
abdominal (±2,4% para ±4,8%), respectivamente37. Este padrão é independente do
gênero, local avaliado (esquerda e/ou direita), e região abdominal27.
O exame de Ressonância Magnética (RM) é considerado o padrão-
ouro para avaliar a morfologia muscular. Recentemente, a RM começou a ser
utilizada para avaliar a mudança do “thickness” dos músculos da parede abdominal
lateral durante o respouso24. Porém esta técnica apresenta alto custo e restrições de
uso em determinados pacientes (ex. Pacientes com implantes metálicos) devido ao
campo magnético gerado. Sendo assim, o ultrassom de imagem torna-se uma boa

22
opção para avaliar a morfologia muscular e comportamento de alguns músculos
durante o movimento humano.
3.5 EVIDÊNCIAS CIENTÍFICAS ENTRE AS MEDIDAS DE EMG E USI NA AVALIAÇÃO DOS
MÚSCULOS ABDOMINAIS
A relação entre a medida do thickness muscular com uso do ultrassom
e da ativação muscular pela eletromiografia ainda necessita de novos estudos,
porém, alguns autores apresentam resultados interessantes para diferentes tipos de
contração dos músculos abdominais. Os achados são claramente inconclusivos até
o momento, com uma correlação estatística entre os dois métodos que varia de fraca
a forte (0.14 a 0.93).
Em um estudo realizado por McMeeken et al (2004)26, oberservou-se
uma boa correlação entre o USI e a EMG para o músculo transverso do abdome (R²
= 0.87). Sendo assim, os autores concluíram que a mudança do thickness do
músculo TrA pode ser utilizada para indicar mudanças na atividade elétrica deste
músculo.
Para Hodges et al (2003)28, as medidas da arquitetura muscular por
meio do USI promovem medidas da atividade para menores níveis de contração
muscular (< que 20 ou 30% de uma contração voluntária máxima). Todavia, este
método não pode ser utilizado para diferenciar as atividades musculares em níveis
de força de moderado a alto, em razão que os músculos abdominais apresentam
pequenas mudanças em suas estruturas morfológicas para essas intensidades. Por
fim, estes autores observaram um comportamento diferente do músculo OE quando
comparado ao OI e o TrA durante a contração isométrica da parede abdominal. Os
autores concluíram que, par ao músculo OE, não há uma relação consistente entre a
atividade elétrica muscular (EMG) e a espessura muscular (USI) durante a
flexão/extensão e contração isométrica do tronco.
Em um estudo mais recente realizado por Brown e McGill (2010)73,
concluiu-se que existe uma relação complexa entre a ativação muscular e a
mudança do thickness muscular. Estes autores não encontraram nenhuma relação
entre a USI e a EMG para os músculos OE (r = 0.22) e OI (r = 0.14) durante a
contração isométrica em rampa.

23
Já o estudo de John & Beithe (2007)23 concluiu que a mudança na
espessura do músculo OE caracterizada por medida de atividade muscular deve ser
usada com cautela quando este músculo atua na rotação do tronco como agonista
principal do movimento durante a contração isométrica.
Por fim, ainda é necessário mais estudos na área para melhor entender
a relação entre as duas medidas, principalmente utilizando novos protocolos de
avaliação. O presente trabalho pretende avaliar somente um músculo abdominal, o
OE. Outro aspecto importante é avaliar os dois métodos (USI e EMG) usando um
tipo de contração muscular que promova diferentes intensidades de força (5 a 50%
da contração voluntária máxima), em uma contração do tipo rampa, na qual é
definida como a produção de uma única força progressiva de contração linear de
baixa a alta intensidade (0 a 100%) durante poucos segundos (ex: 5 a 10 s)75. Para
conhecimento autoral, poucos estudos utilizaram este procedimento e compararam
as medidas em diferentes níveis de contração muscular e direções do movimento
como flexão, inclinação lateral e rotação do tronco em um mesmo estudo. Por fim a
postura do individuo durante a avaliação é de suma importância. No presente estudo
foi escolhida a posição sentada com apoio pois esta pode representar mais as
atividades diárias e também por esta se relacionar com a dor lombar crônica70.

24
Ilustrações
25
Figura 1- Músculos que compõem a parede abdominal.

26
ARTIGO
(Artigo completosubmetido no periódico Jounal of Electromyography and Kinesiology no mês de Abril
de 2013)

27
<Title>
External Abdominal Oblique Muscle Thickness Changes Measured Using Ultrasound
Imaging is Not an Appropriate Surrogate Measure of Electromyographic Activity During
Isometric Trunk Contractions
<Authors>
Lucas M. Rabelloa,b,c
; Dany Gagnonc,d
; Christian Larivièrec,e
; Philippe Paquettec,d
; Rubens A.
da Silvaa,b,c*
Affiliation
a. Centre for Health Science Research, Laboratory of functional evaluation and human
motor performance, Universidade Norte do Paraná (UNOPAR), Londrina-PR, Brazil.
b. Master’s Program in Rehabilitation Sciences UEL/UNOPAR, Londrina-PR, Brazil.
c. Pathokinesiology Laboratory, Centre for Interdisciplinary Research in
Rehabilitation of Greater Montreal, Institut de réadaptation Gingras-Lindsay-de-
Montréal, Montreal, Quebec, Canada.
d.School of Rehabilitation, Faculty of Medicine, Université de Montréal, Montreal,
Quebec, Canada.
e. Occupational Health and Safety Research Institute Robert-Sauvé (IRSST) Montreal,
Quebec, Canada.
*Corresponding Author
Rubens A. da Silva, Ph.D.
Centre for Health Science Research, Laboratory of functional evaluation and human motor
performance (LAFUP).
Universidade Norte do Paraná (UNOPAR).
Av. Paris, 675 - Jd. Piza CEP 86041-140 - Cx. P. 401
Londrina-PR, Brazil.
Telephone: 011 55 (43) 3371-7700 #7990
Fax: 011 55 (43) 3371-7721
Email: [email protected]

28
Abstract
This study was conducted to assess the validity of ultrasound imaging (USI) thickness
measures of right external oblique (EO) muscle activity. Eighteen subjects were instructed to
sit on a dynamometer and execute ramp isometric efforts progressing from 0 to 50% of the
maximal voluntary contraction (MVC) in three trunk directions: (1) forward flexion; (2) right
lateral flexion; and (3) left axial rotation. USI and surface electromyography (EMG) of the
EO muscle were measured concomitantly. EMG and USI thickness changes were both
normalized against rest and maximal EMG respectively. Based on the EMG results, the EO
muscle was significantly more activated (p 0.001) during forward flexion (42% on average)
and axial rotation (35%) than during lateral flexion (24%). Non-significant (r = 0.01; P =
0.979) to highly significant (r = 0.98; P < 0.0001) negative and positive Pearson correlations
were observed between EMG and USI for both flexion and rotation directions across
individuals. The USI validity was better related to rotation direction efforts. These results
support the idea that quantitative musculoskeletal ultrasound imaging and EMG of the EO
muscle provides different but complementary information when investigating muscular
recruitment during isometric trunk contractions.
Keywords: Electromyography, ultrasonography, trunk muscle, biomechanics, rehabilitation

29
1. Introduction
Abdominal wall muscle function is often an area of interest within rehabilitation
programs related to lumbar spine stabilization in patients with low back pain (LBP). In
keeping with the mechanical stability of the spine hypothesis (Panjabi, 1992a, Panjabi,
2006b), some evidence suggests that LBP patients can present spinal dysfunctions related to
the trunk neuromuscular system (Dankaerts et al., 2006), potentially leading to unstable spinal
segments and back pain. The abdominal muscles play a crucial role in adequate
neuromuscular control of the lumbar spine because they are involved during various efforts
generated in forward flexion, lateral bending and axial rotation (Marras et al., 1990; McGill,
1991; Thelen et al., 1994).
The function of specific abdominal muscles can be assessed using a variety of
techniques such as intramuscular fine-wire electromyography (EMG) or functional magnetic
resonance imaging (D´hooge B et al., 2013). However, these two techniques are both costly
and uncomfortable and therefore impractical for clinical use. More practical methods such as
surface EMG (De Luca et al., 2012) and more recently, ultrasound imaging (USI) (Whittaker
et al., 2007; Teyhen, 2006a), have been used for assessing the abdominal muscles during
various tasks.
USI has grown in popularity in research and clinical settings as a reliable, non-
invasive technique for assessing abdominal muscle function (McMeeken et al., 2004; Teyhen
et al., 2007b; Costa et al., 2009). This technique has been used to estimate the activity of
transversus abdominis (Hodges et al., 2003; McMeeken et al., 2004) and external and internal
oblique muscles (Hodges et al., 2003) by measuring changes in muscle thickness. However,
the relationship between EMG activity and muscle thickness changes remains unclear in
terms of the abdominal wall muscles (Brown and McGill, 2010), which calls into question the
validity of USI-based thickness measures of muscle activity.

30
As recently discussed by Brown and McGill (2010), “the mechanical interaction
between the abdominal muscle layers makes for complex deformation patterns that differ
dependent upon the relative action of each muscle.” Consequently, the validity of USI
measures as an estimate of muscle activity may depend on the complexity of the tasks as well
as the muscle being investigated. There are some obvious advantages of studying the three
abdominal layers (external and internal obliques and transversus abdominis) at the same time
using USI to understand the relative contribution of each muscle (Rankin et al., 2006).
However, the relationship between external oblique (EO) USI thickness and EMG activity has
seldom been studied (Brown and McGill, 2010; John & Beith, 2007; Hodges et al., 2003),
despite playing a primary role in axial trunk rotation and participating in some movements of
trunk flexion and lateral bending (Peach et al., 1998). As a result, further research is certainly
required.
To date, two studies (Brown and McGill, 2010; Hodges et al., 2003) found no
significant relationship (r correlation of -0.22 and 0.23, respectively) between the two
measures (EMG and USI) during trunk flexion contraction (in both studies) and brace, hollow
and extension trunk efforts (in Brow and McGill only). However, these studies used a small
sample of subjects (5 and 3, respectively), which likely did not accurately represent inter-
individual variations. Neither of these two studies investigated a task involving the primary
role of this muscle (axial rotation), which clearly appears to make a difference according to
the results previously reported by John & Beith (2007). John & Beith (2007) substantiated the
EO USI and EMG relationship in 24 subjects during axial rotation effort and found a
significant linear relationship in 21 of the 24 subject but the strength of this relationship was
undoubtedly different across subjects. However, the axial rotation effort was controlled using
the EO EMG as biofeedback, which is not an ideal method for standardizing the EO
biomechanical demand. The main purpose of this study was therefore to assess the

31
relationship between USI thickness and EMG (concurrent validity) with respect to right EO
muscle activation using a dynamometer to produce isometric efforts in three trunk directions
(forward flexion, right lateral flexion and left axial rotation) with real-time contraction
direction- and velocity-specific visual feedback controlling isometric contraction efforts from
one plane (e.g., axial rotation in the transverse plane) while minimizing efforts in the other
planes (e.g., frontal and sagittal planes) (Larivière et al., (2009). Finally, since the EO muscle
is comprised of many fascicules having different directions and functions (Mirka et al., 1997),
we tested whether previously observed inter-individual variations could be partly explained
by the tested EO fascicule.
2. Methods
2.1. Subjects
Twenty-three men were recruited from the local community using a convenient and
voluntary sampling method. The inclusion criteria for the study were as follows: participants
must be healthy and must not be involved in regular physical activity programs. Subjects were
excluded if they had suffered back pain in the previous year or back pain lasting longer than
one week in previous years; had a history of self-reported injuries, illnesses, musculoskeletal
disorders, systemic–neurological or degenerative disorders or cardiovascular or respiratory
disease. Five of the 23 subjects were excluded at the laboratory due to excessive fat in the
abdominal region and reduced space between the last rib and the iliac crest, making USI much
too difficult. This resulted in a total sample of 18 subjects. The mean characteristics of these
18 subjects were: 25 years of age [Standard Deviation (SD) = 8], height of 1.78 m (SD = 1),
mass of 73 kg (SD = 5), and a body mass index of 23 kg/m2 (SD = 2).

32
The research was conducted at the Institut de réadaptation Gingras-Lindsay-de-
Montréal, a research site of the Centre for Interdisciplinary Research in Rehabilitation of
Greater Montreal (CRIR). The subjects signed the consent form after receiving verbal and
written information about the study. The protocol and consent form were approved by the
local ethics committee (CRIR 716-0312).
2.2. Experimental procedures
All subjects were invited to one evaluation session only. They first underwent a
structured interview conducted by a physiotherapist to collect basic information including
demographics and anthropometric measures, followed by a physical examination.
Subjects were then placed in a sitting position, with their trunk straight, on a
dynamometer. EMG electrodes were attached to the skin while seated on the dynamometer.
The pelvis, legs and thorax segments were stabilized to better isolate the EO biomechanical
demand (Figure 1). Subjects were asked to keep their arms crossed during all tests. Next, they
were instructed to remain at rest while a baseline USI image (EO thickness measures at rest)
was recorded.
To familiarize the subjects with the protocol and visual feedback, three submaximal
contractions were performed in each of the following three directions: (1) forward flexion, (2)
right lateral flexion and (3) left axial rotation of the trunk. Five minutes after the
familiarization period, three isometric maximal voluntary contractions (MVC) were
performed in each direction to record maximal EMG activation for normalization purposes.
Each MVC lasted 8 seconds (s), with 2 minutes (m) of rest between trials. Visual feedback
and verbal encouragement were given to obtain maximal effort.
Ten minutes after the MVCs, the subjects performed three ramp contractions ranging
from 0 to 55% of the MVC in each direction (forward flexion, lateral flexion and axial

33
rotation). The directions were randomly presented. Each submaximal ramp contraction lasted
6 seconds (s), with 1 minute of rest between each trial. In order to obtain stable EMG and USI
measurements, the subjects were required to hold their breath (after an inhalation) during all
the contractions.
2.3. Measurement techniques
Dynamometric, EMG and ultrasound data was synchronized by triggering the data
collection of all instruments with the ultrasound pedal, which was pressed by the ultrasound
operator.
Dynamometry
A 3D isometric dynamometer was used to measure and control the L5/S1 moments
during the tasks (Larivière et al., 2009). This dynamometer is comprised of a tri-axial force
platform (Advanced Mechanical Technology Incorporated, model MC6-6-1000) that records
the force produced on the three axes at a sampling rate of 100 Hz. This equipment allows for
the stabilization of the feet, knees, pelvis and trunk. As explained elsewhere (Larivière et al.,
2009), this dynamometer is combined with visual feedback (3D – feedback), which allows the
subjects to produce the main effort in one direction (e.g., flexion, rotation or lateral bending)
while minimizing the production of force moments in the other directions.
Ultrasound imaging
To assess muscular thickness, a Phillips HD11 1.0.6 ultrasound machine and a 5–12
MHz 50-mm linear array transducer (model L12-5; Philips Medical Systems, Bothell, WA)
were used. The position of the USI transducer was standardized (see Electromyography
section below), a distance which prevented the electrodes from coming into contact with the
34
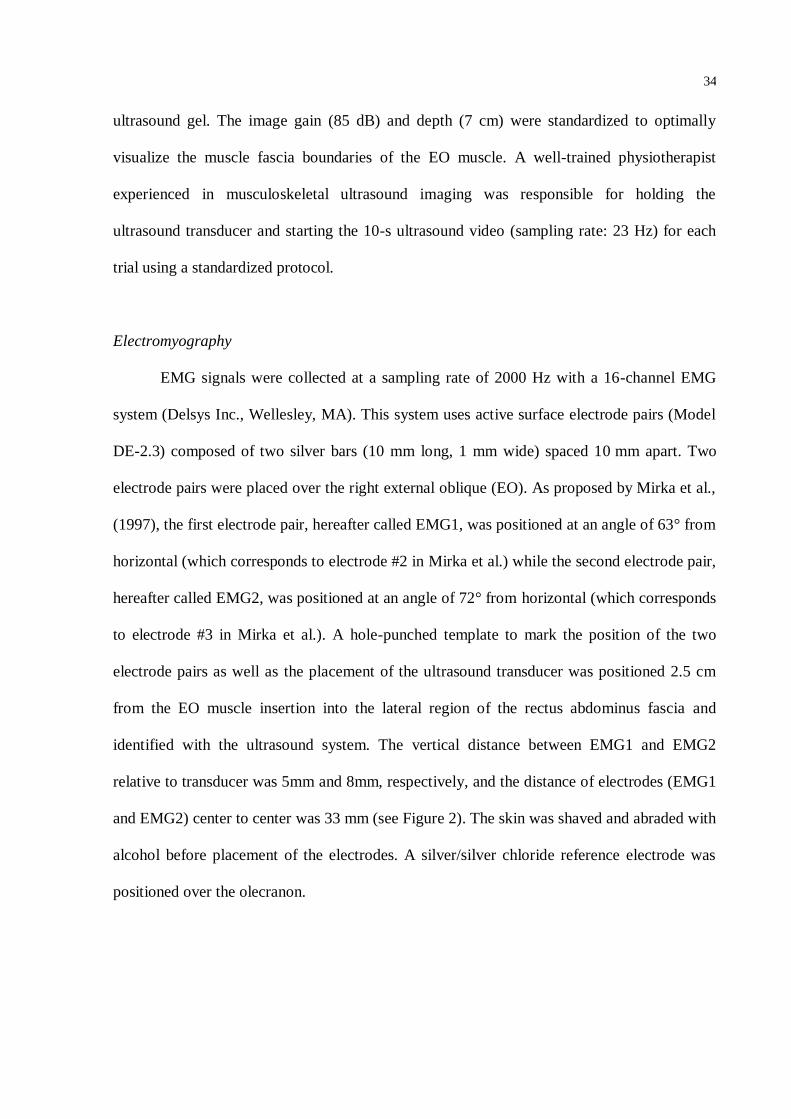
ultrasound gel. The image gain (85 dB) and depth (7 cm) were standardized to optimally
visualize the muscle fascia boundaries of the EO muscle. A well-trained physiotherapist
experienced in musculoskeletal ultrasound imaging was responsible for holding the
ultrasound transducer and starting the 10-s ultrasound video (sampling rate: 23 Hz) for each
trial using a standardized protocol.
Electromyography
EMG signals were collected at a sampling rate of 2000 Hz with a 16-channel EMG
system (Delsys Inc., Wellesley, MA). This system uses active surface electrode pairs (Model
DE-2.3) composed of two silver bars (10 mm long, 1 mm wide) spaced 10 mm apart. Two
electrode pairs were placed over the right external oblique (EO). As proposed by Mirka et al.,
(1997), the first electrode pair, hereafter called EMG1, was positioned at an angle of 63° from
horizontal (which corresponds to electrode #2 in Mirka et al.) while the second electrode pair,
hereafter called EMG2, was positioned at an angle of 72° from horizontal (which corresponds
to electrode #3 in Mirka et al.). A hole-punched template to mark the position of the two
electrode pairs as well as the placement of the ultrasound transducer was positioned 2.5 cm
from the EO muscle insertion into the lateral region of the rectus abdominus fascia and
identified with the ultrasound system. The vertical distance between EMG1 and EMG2
relative to transducer was 5mm and 8mm, respectively, and the distance of electrodes (EMG1
and EMG2) center to center was 33 mm (see Figure 2). The skin was shaved and abraded with
alcohol before placement of the electrodes. A silver/silver chloride reference electrode was
positioned over the olecranon.
35
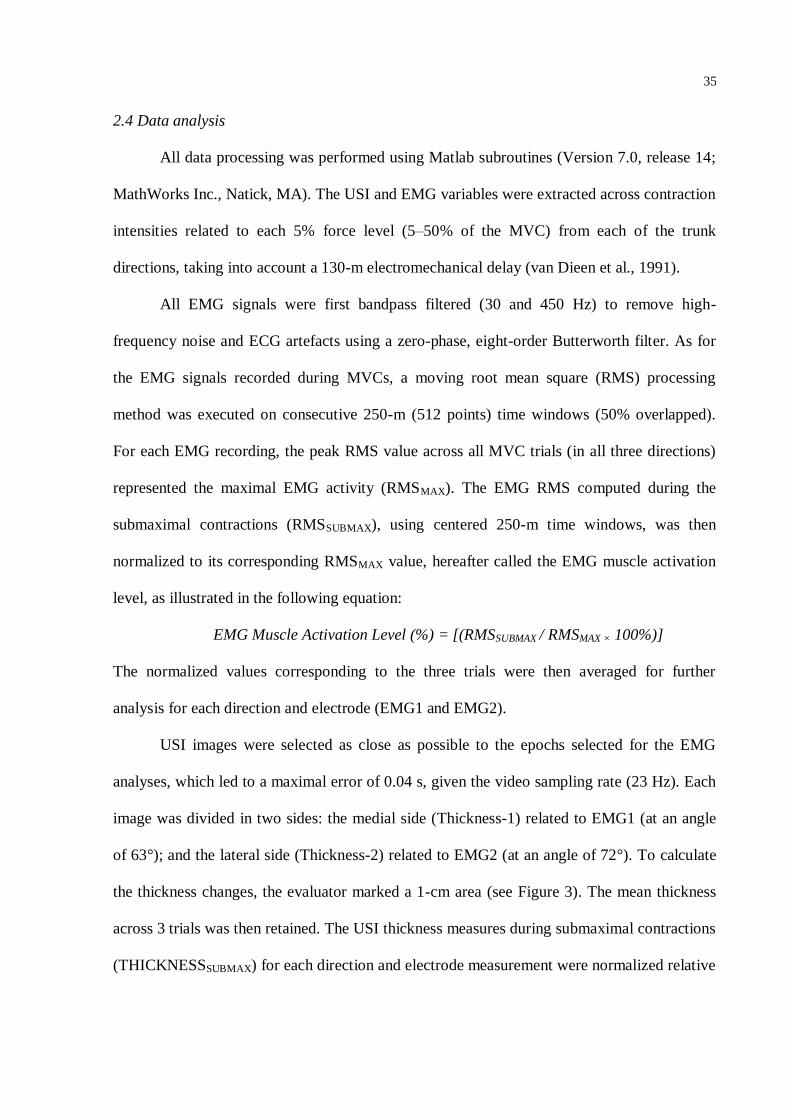
2.4 Data analysis
All data processing was performed using Matlab subroutines (Version 7.0, release 14;
MathWorks Inc., Natick, MA). The USI and EMG variables were extracted across contraction
intensities related to each 5% force level (5–50% of the MVC) from each of the trunk
directions, taking into account a 130-m electromechanical delay (van Dieen et al., 1991).
All EMG signals were first bandpass filtered (30 and 450 Hz) to remove high-
frequency noise and ECG artefacts using a zero-phase, eight-order Butterworth filter. As for
the EMG signals recorded during MVCs, a moving root mean square (RMS) processing
method was executed on consecutive 250-m (512 points) time windows (50% overlapped).
For each EMG recording, the peak RMS value across all MVC trials (in all three directions)
represented the maximal EMG activity (RMSMAX). The EMG RMS computed during the
submaximal contractions (RMSSUBMAX), using centered 250-m time windows, was then
normalized to its corresponding RMSMAX value, hereafter called the EMG muscle activation
level, as illustrated in the following equation:
EMG Muscle Activation Level (%) = [(RMSSUBMAX / RMSMAX × 100%)]
The normalized values corresponding to the three trials were then averaged for further
analysis for each direction and electrode (EMG1 and EMG2).
USI images were selected as close as possible to the epochs selected for the EMG
analyses, which led to a maximal error of 0.04 s, given the video sampling rate (23 Hz). Each
image was divided in two sides: the medial side (Thickness-1) related to EMG1 (at an angle
of 63°); and the lateral side (Thickness-2) related to EMG2 (at an angle of 72°). To calculate
the thickness changes, the evaluator marked a 1-cm area (see Figure 3). The mean thickness
across 3 trials was then retained. The USI thickness measures during submaximal contractions
(THICKNESSSUBMAX) for each direction and electrode measurement were normalized relative

36
to the thickness recorded when the subject was asked to relax at the beginning of the protocol
(THICKNESSREST), using the following equation:
USI-based thickness (%) = [(THICKNESSSUBMAX / THICKNESSREST× 100%)]
Based on this equation, 110% means that the muscle thickness was 10% greater than at rest.
2.4.1 Statistical analysis
All statistical analyses were done with SPSS software (version 15.0 for Windows)
with an alpha level of 0.05 indicating statistical significance. The normality of the data was
verified with the Wilk–Shapiro test. Since the data from both measures (USI and EMG)
followed a normal distribution, the analyses were subsequently performed using parametric
statistical tests and the results were presented using mean and Standard Deviation (SD)
values.
To determine which trunk direction activated the EO muscle the most, as assessed
only with EMG1 and EMG2 electrodes, a one-way ANOVA with repeated measures was
carried out to compare EMG muscle activation level values at 50% of the MVC of the ramp
contraction among the three isometric direction efforts.
Considering that USI thickness measures are burdensome, we elected to reject the
lateral bending task based on these EMG results. Subsequently, a one-way ANOVA with
repeated measures was performed to compare EMG muscle activation and USI-based
thickness level values across the 10 intensities (ranging from 5 to 50% of the MVC) for the
isometric forward flexion and left axial rotation contraction directions. A one-way ANOVA
was independently run for each variable (EMG1, EMG2, Thickness-1, Thickness-2). Post-hoc
Tukey tests were applied as required to further identify differences between the intensities for
each direction.
37
To look at inter-individual variability in the EMG/USI relationship in each isometric
flexion and rotation effort direction, Pearson correlation coefficients (r) were calculated
between muscular thickness and EMG variables across the intensities for each participant
individually in order to determine the validity of the USI-based thickness measures of EO
muscle activation.
3. Results
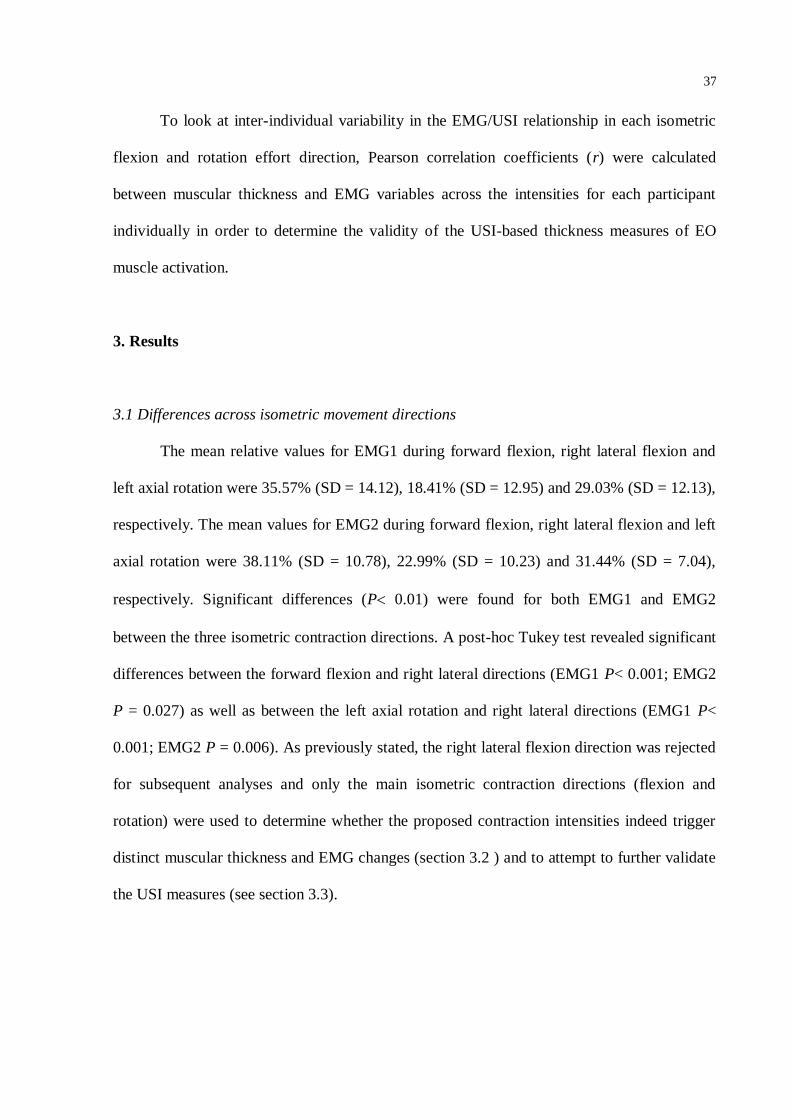
3.1 Differences across isometric movement directions
The mean relative values for EMG1 during forward flexion, right lateral flexion and
left axial rotation were 35.57% (SD = 14.12), 18.41% (SD = 12.95) and 29.03% (SD = 12.13),
respectively. The mean values for EMG2 during forward flexion, right lateral flexion and left
axial rotation were 38.11% (SD = 10.78), 22.99% (SD = 10.23) and 31.44% (SD = 7.04),
respectively. Significant differences (P 0.01) were found for both EMG1 and EMG2
between the three isometric contraction directions. A post-hoc Tukey test revealed significant
differences between the forward flexion and right lateral directions (EMG1 P< 0.001; EMG2
P = 0.027) as well as between the left axial rotation and right lateral directions (EMG1 P<
0.001; EMG2 P = 0.006). As previously stated, the right lateral flexion direction was rejected
for subsequent analyses and only the main isometric contraction directions (flexion and
rotation) were used to determine whether the proposed contraction intensities indeed trigger
distinct muscular thickness and EMG changes (section 3.2 ) and to attempt to further validate
the USI measures (see section 3.3).
38
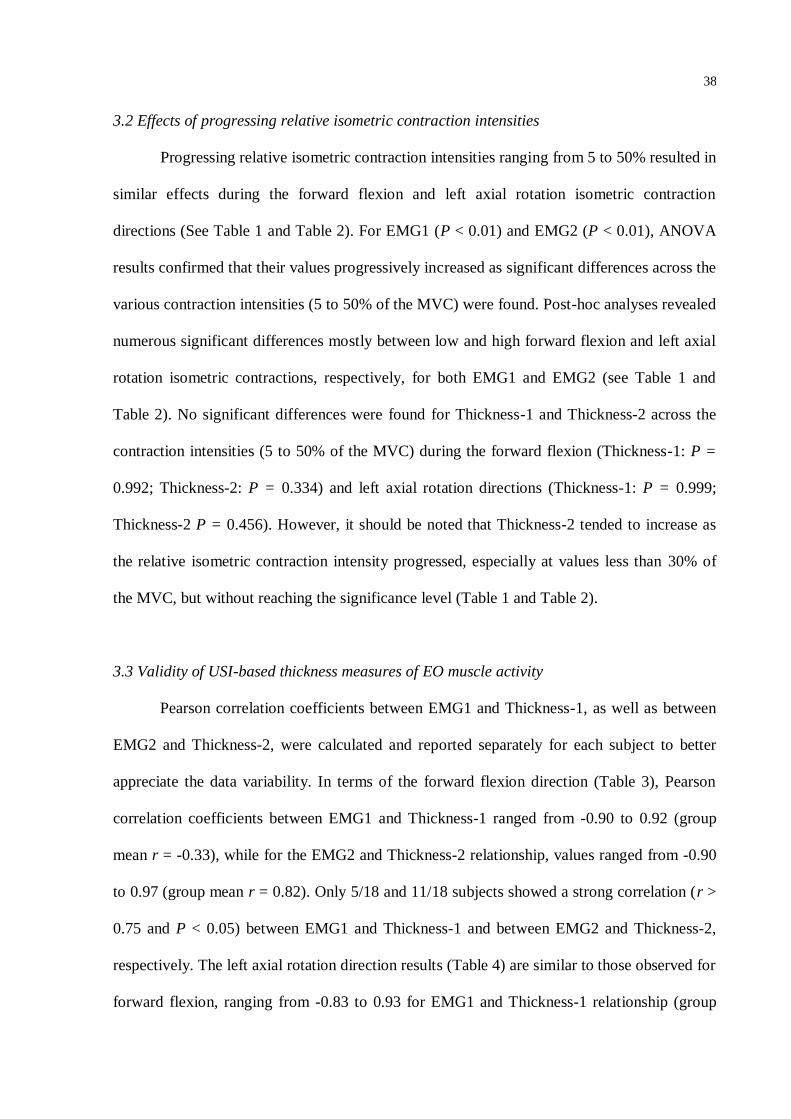
3.2 Effects of progressing relative isometric contraction intensities
Progressing relative isometric contraction intensities ranging from 5 to 50% resulted in
similar effects during the forward flexion and left axial rotation isometric contraction
directions (See Table 1 and Table 2). For EMG1 (P < 0.01) and EMG2 (P < 0.01), ANOVA
results confirmed that their values progressively increased as significant differences across the
various contraction intensities (5 to 50% of the MVC) were found. Post-hoc analyses revealed
numerous significant differences mostly between low and high forward flexion and left axial
rotation isometric contractions, respectively, for both EMG1 and EMG2 (see Table 1 and
Table 2). No significant differences were found for Thickness-1 and Thickness-2 across the
contraction intensities (5 to 50% of the MVC) during the forward flexion (Thickness-1: P =
0.992; Thickness-2: P = 0.334) and left axial rotation directions (Thickness-1: P = 0.999;
Thickness-2 P = 0.456). However, it should be noted that Thickness-2 tended to increase as
the relative isometric contraction intensity progressed, especially at values less than 30% of
the MVC, but without reaching the significance level (Table 1 and Table 2).
3.3 Validity of USI-based thickness measures of EO muscle activity
Pearson correlation coefficients between EMG1 and Thickness-1, as well as between
EMG2 and Thickness-2, were calculated and reported separately for each subject to better
appreciate the data variability. In terms of the forward flexion direction (Table 3), Pearson
correlation coefficients between EMG1 and Thickness-1 ranged from -0.90 to 0.92 (group
mean r = -0.33), while for the EMG2 and Thickness-2 relationship, values ranged from -0.90
to 0.97 (group mean r = 0.82). Only 5/18 and 11/18 subjects showed a strong correlation (r >
0.75 and P < 0.05) between EMG1 and Thickness-1 and between EMG2 and Thickness-2,
respectively. The left axial rotation direction results (Table 4) are similar to those observed for
forward flexion, ranging from -0.83 to 0.93 for EMG1 and Thickness-1 relationship (group

39
mean r = 0.37) and from -0.59 to 0.98 for EMG2/Thickness-2 relationship (group mean r =
0.97). Only 4/18 and 9/18 participants showed a strong correlation (r > 0.75 and P < 0.05)
between EMG1 and Thickness-1 and between EMG2 and Thickness-2, respectively. Hence,
the validity of USI-based thickness measures of EO muscle activity was better related to the
EMG2 and Thicknness-2 variables in both directions, despite the large variability observed
across subjects.
4. Discussion
The present study assessed muscular activity changes of the right external oblique
(EO) muscle using electromyography and ultrasound image-based thickness measures during
three isometric contraction directions: (1) forward trunk flexion; (2) right lateral flexion; and
(3) left axial rotation. All isometric effort directions were performed in a stabilized sitting
position on a dynamometer to better isolate the EO biomechanical demand relative to planes
of movement. Interestingly, in this standardized and well-controlled protocol, the EO muscle
was more activated only in forward flexion (45% on average) and left axial rotation (35% on
average ) effort directions as compared to the right lateral flexion direction (24% on average).
These two main effort directions (flexion and rotation) were thus retained for subsequent
analyses, which showed that the EO EMG values increases somewhat proportionally with
increases in relative contraction intensities, whereas no clear pattern was established with
regard to EO thickness during the same period. The validity of USI-based thickness measures
of EO muscle activity during low intensity contractions (<50% of the MVC) was accepted
only for the EMG2 and Thicknness-2 relationship for both of these directions, despite
substantial variability across subjects.
The external oblique muscle is involved in different activities of the trunk, such as
flexion (Sheeran et al., 2012), lateral bending (Huang et al., 2001) and axial rotation (Kumar

40
et al., 2001). Some authors (Ng et al., 2002) have demonstrated, however, that the external
oblique can be more activated during lateral bending, which is contrary to the present results.
It is known that abdominal muscle activity can change across different postures (Anderson et
al., 2002), and this could partly explain the differences between our results and those reported
by Ng et al., (2002). Furthermore, Ng et al., (2002) gathered their results during a maximal
effort instead of various submaximal contraction intensities as performed in the present study.
Our subjects were evaluated in a sitting position with the pelvis and lower limbs stabilized,
which might better isolate the biomechanical action of this muscle on each plane of
movement and consequently generate more activity during each specific direction such as in
forward flexion and left axial rotation (Brown and McGill, 2009a).
To determine whether the proposed contractions intensities trigger distinct muscular
thickness and EMG changes, we compared EMG and USI variables across various intensities
(ranging from 5 to 50% of the MVC) for isometric flexion and rotation directions. Previous
studies (Brown and McGill, 2010; John & Beith, 2007; Hodges, 2003), evaluating one or two
directions only, observed a small change in muscular thickness with an increase in the
contraction intensity level, which coincides with the results of the present study. Our results
conclude that only EMG variables presented a somewhat linear increase with a force increase
during forward flexion and axial rotation isometric contractions. The relationship between
EMG and an increase of force is well known in the literature (De Luca, 1997, Lawrence and
De Luca, 1983), even though it changes the pattern depending on the nature of the task (static
or dynamic). As observed in Table 1 and 2, the percentage of EO EMG relative to maximal
increases in contraction intensity (5 to 50% of the MVC), which is indicative of motor unit
recruitment with an increased mechanical load on this muscle. However, this pattern is not
similar to EO thickness during the same period. The explanation for these USI measure results
remains unclear in the literature. A plausible hypothesis could be associated with a

41
mechanical link between the abdominal muscular layers as described by Brown and McGill
(2010), where the shortening and thickening of EO muscle are compromised when the other
abdominal layers are contracted simultaneously. This could directly affect USI changes with
the increase in contraction intensities. In other words, depending on the force generated by the
muscle with the increase in intensity, the stretching force becomes the dominate force
(compared to the deformation force) and the muscle may show a tendency to stretch out and
thus attenuate the USI/force relationship. This may partly explain the results found in the
literature (Ferreira et al., 2004; John & Beith, 2007; Hodges et al., 2003) and those in the
present study, where the EO muscle showed very little increased thickness with high EMG
activity during increases in contraction intensities.
We must remember that USI-based thickness measures are influenced by inter-subject
variability. Our results showed that some subjects presented a positive relationship of
thickness and electrical muscle activity with an increase in contraction intensity, while other
subjects had a negative direction, or even, null correlation. When specifically comparing the
correlation between EMG2 and Thickness-2 measures, we observed 13 and 15 positive
correlations for the forward flexion and left axial rotation directions, respectively. The mean
EMG/USI relationship was r = 0.97 (Table 4), based on the results for the left axial rotation,
which thus supports the validity of EO muscle activity USI-based thickness measures. These
results are consistent with those reported by John & Beith (2007) for this isometric
contraction direction. These authors also demonstrated a significant relationship between an
increase in EO thickness and an increase in EMG activity within the muscle during the left
axial rotation direction for the majority of subjects. Although, the correlations between the
two measures ranged from weak to strong depending on the subjects, we observed that 11
subjects (61% of our sample) presented a significant relationship between EMG2 and
Thickness-2 measures for the left axial rotation effort direction (Table 4), while John & Beith

42
reported that 87% of their sample had a positive correlation between both measures. However,
compared to the study by John & Beith, the advantage of the present study was the use of a
robust experimental protocol to better control the EO biomechanical demand during each
isometric contraction direction in order to minimize EO fascicle compensations in one plane
of movement compared to another. John & Beith only used EO EMG biofeedback to control
the axial rotation effort during all testing, which could limit their validity of measurement.
Ultrasound imaging can provide a visual representation of muscle function as
previously supported (Teyhen et al., 2007). One aspect of muscle function that has been
studied in recent years is muscular electrical activity, and the relationship between changes in
muscular thickness and EMG activity. However, the present study, as well as others before it,
does not clearly support the use of USI measures for quantifying muscular activity of the
trunk muscles, dependent from effort direction and isometric contraction intensity. The
findings are still inconclusive concerning the relationship between these two measures in
terms of the lateral abdominal wall. However, the validity between these two measures can be
accepted in some cases depending on subject variability. Furthermore, some authors suggest
that USI can be used with different applications for research and more specifically for clinical
practice to 1) provide the physical therapist and patient with feedback and 2) to assist physical
therapists in their decision-making process related to exercise prescription and progression
(Teyhen et al., 2007).
Finally, the results of the present study should be interpreted with caution. Only
surface EMG signals were recorded, which is different from some previous studies (Hodges et
al., 2003; McMeeken et al., 2004) that have used intramuscular recordings to capture
electrical muscle activity simultaneously with the measures of USI to assess the muscular
activation of the abdominal muscles. The surface EMG does not make it possible for the
evaluator to place the USI transducer in the same location where the electrical muscle activity

43
was recorded. To minimize these effects, the present study used a device to standardize the
position between the US transducer and the EMG electrodes, as stated previously under
Methods (section 2.2.1). In addition, the results of the present study can neither be generalized
to individuals with impairments or disability (e.g., individuals with low back pain), nor to
women. Finally, in terms of statistical power, the possibility of Type I errors (false findings)
and Type II errors (missed findings) appears unlikely in the present study, except for USI
measures of Thickness-2 with increases in intensity (P = 0.334 for flexion direction and P =
0.456 for rotation direction), which could have reached statistical significance (Type II errors)
with a larger sample of subjects.
5. Conclusion
The results of present study support the idea that quantitative musculoskeletal
ultrasound imaging and EMG of the EO muscle provides different but complementary
information when investigating muscular recruitment during isometric trunk contractions.
Relative EMG activity of the EO muscles, especially of the lateral compartment, is more
responsive to progressive increased isometric trunk contraction intensity than EO muscular
thickness. The association documented only for a small proportion of subjects between the
EMG intensity and muscular thickness of the EO muscle during isometric trunk contractions
remains to be strengthened. In the present study, the validity between two measures was better
accepted for the relationship between EMG2 and thickness-2 during the left axial rotation
direction. Hence, quantitative ultrasound imaging of the abdominal muscles should be used
with caution in clinical practice and in rehabilitation research protocols.
44
Conflict of interest statement
None declared.
Acknowledgement
This study was funded in part by the Fonds de la recherche du Québec-Santé (FRQS). The
equipment and material required for this research project was financed in part by the
Occupational Health and Safety Research Institute Robert-Sauvé (IRSST) and the Canada
Foundation for Innovation (CFI). Dany Gagnon holds a Junior 1 Research Career Award from
the FRQS. Rubens A. da Silva, was funded by from the National Foundation for the
Development of Private Higher Education (FUNADESP, Brazil). The authors thank the
assistance of Hakim Mecheri for help with data processing and analysis. We thank Prof.
Rodrigo Franco (UNOPAR University, Brazil) for his contribution to and comments on the
Master’s degree thesis by Lucas Rabello, upon which this research study is based. We thank
Université de Montréal and UNOPAR for the official collaboration in the international
student exchange program.

45
References
1. Andersson EA, Grundström H, Thorstensson A. Diverging Intramuscular Activity
Patterns in Back and Abdominal Muscles During Trunk Rotation. Spine.
2002;27(6):E152-E160.
2. Brown SHM, McGill SM. Transmission of muscularly generated force and stiffness
between layers of the rat abdominal wall. Spine. 2009a;34:E70–E75.
3. Brown SHM, McGill SM. A comparison of ultrasound and electromyography
measures of force and activation to examine the mechanics of abdominal wall
contraction. Clinical Biomechanics. 2010b;25: 115-123.
4. Costa LOP, Maher CG, Latimer J, Smeets RJ. Systematic Review for the
Measurement of Abdominal Muscle Activity: A Reproducibility of Rehabilitative
Ultrasound Imaging. Phys Ther. 2009;89:756-769.
5. Dankaerts W O’Sullivan P, Burnett A, Straker L. Altered Patterns of Superficial Trunk
Muscle Activation During Sitting in Nonspecific Chronic Low Back Pain Patients.
SPINE. 2006;319(17):2017–2023
6. De Luca CJ. The use of surface electromyography in biomechanics. Journal of
Applied Biomechanics. 1997;13:135-163.
7. D'hooge R, Cagnie B, Crombez G, Vanderstraeten G, et al. Lumbar muscle
dysfunction during remission of unilateral recurrent nonspecific low-back pain:
evaluation with muscle functional MRI.Clin J Pain 29 (3):187-194, 2013.
8. DeLuca CJ, Kuznetsov M, Gilmore LD, Roy SH. Inter-electrode spacing of surface
EMG sensors - Reduction of crosstalk contamination during voluntary contractions.
Journal of Biomechanics. 2012;45:555–561.
9. Hodges PW. Ultrasound Imaging in Rehabilitation: Just a Fad?. J Orthop Sports Phys
Ther. 2005;35(6):333-337.
46
10. Hodges PW, Pengel LH, Herbert RD, Gandevia SC. Measurement of muscle
contraction with ultrasound imaging. Muscle and Nerve. 2003;27:682-692.
11. Huang QM, Andersson E, Thorstensson A. Intramuscular Myoelectric Activity and
Selective Coactivation of Trunk Muscles During Lateral Flexion With and Without
Load. Spine. 2001;26(13):1465–1472.
12. John EK, Beith ID. Can activity within the external abdominal oblique be measured
using real-time ultrasound imaging?. Clinical Biomechanics. 2007;22:972-979.
13. Kumar S, Narayan Y, Garand D. Isometric axial rotation of the trunk in the neutral
posture. Eur J Appl Physiol. 2001;86:53-61.
14. Larivière C, Gagnon D, Genest K. Offering proper feedback to control for out-of-
plane lumbar moments influences the activity of trunk muscles during unidirectional
isometric trunk exertions. Journal of Biomechanics. 2009;42:1498-1505.
15. Lawrence JH; De Luca CJ. Myoelectric signal versus force relationship in different
human muscles. Journal of Applied Physiology. 1983; 54:1653-1659.
16. Marras WS, Mirka GA. Muscle activities during asymmetric trunk angular
accelerations. J. Orthopaed. Res. 1990;8:824–832.
17. McGill SM. Kinetic potential of the lumbar trunk musculature about 3 orthogonal
orthopedic axes in extreme postures. Spine. 1991;16:809–815.
18. McMeeken JM, Beith ID, Newham DJ, Milligan P, Critchley DJ. The relationship
between EMG and changes in thickness of transverses abdominis. Clin Biomech
2004;19(4):337e42.
19. Mirka G, Kelaher D, Baker A , Harrison A, Davis J. Selective activation of the
external oblique musculature during axial torque production. Clinical Biomechanics.
1997;12:172-180.

47
20. Ng JK, Kippers V, Parnianpour M, Richardson CA. EMG activity normalization for
trunk muscles in subjects with and without low back pain. Med Sci Sports Exerc.
2002;34(7):1082-6.
21. Panjabi M.M. The stabilizing system of the spine. Part I. Function, dysfunction,
adaptation, and enhancement. Journal of Spinal Disorders. 1992a;5(4):383-389.
22. Panjabi M.M. A hypothesis of chronic back pain: ligament subfailure injuries lead to
muscle control dysfunction. Eur.Spine J. 2006b;15(5):668-676.
23. Peach JP, Sutarno CG, McGill SM. Three-dimensional kinematics and trunk muscle
myoelectric activity in the young lumbar spine: a database. Arch. Phys. Med. Rehabil.
1998;79:663–669.
24. Rankin G, Stokes M and Newham DJ. Abdominal muscle size and symmetry in
normal subjects. Muscle Nerve. 2006;34, 320-326.
25. Sheeran L, Sparkes V, Caterson B, Busse-Morris M, van Deursen R. Spinal Position
Sense and Trunk Muscle Activity During Sitting and Standing in Nonspecific Chronic
Low Back Pain.Spine. 2012;37(8):E486–E495.
26. Stetts DM, Freund JE, Allison SC, Carpenter G. A Rehabilitative Ultrasound Imaging
Investigation of Lateral Abdominal Muscle Thickness in Healthy Aging Adults.
Journal of Geriatric Physical Therapy. 2009;32(2):16-22.
27. Thelen DG, Schultz AB, Ashton-Miller JA. Quantitative interpretation of lumbar
muscle myoelectric signals during rapid cyclic attempted trunk flexions and
extensions. J. Biomech. 1994;27:157–167.
28. Teyhen DS. Rehabilitative Ultrasound Imaging Symposium San Antonio, TX, May 8–
10, 2006. J Orthop Sports Phys Ther.2006a;36:A1–3.

48
29. Teyhen DS, Gill NW, Whittaker JL, Henry SM, Hides JA, Hodges P. Rehabilitative
ultrasound imaging of the abdominal muscles. J Orthop Sports Phys Ther
2007b;37(8):450e66.
30. Teyhen DS, Childs JD, Flynm TW. Rehabilitative Ultrasound Imaging: When Is a
Picture Necessary?. J Orthop Sports Phys Ther. 2007c;37(10):579-580
31. van Dieen JH, Thissen CEAM, van de Ven AJGM, Toussaint HM. The electro-
mechanical delay of the erector spinae muscle: influence of rate of force development,
fatigue and electrode location.European Journal of Applied Physiology 63:216-222,
1991.
32. Whittaker JL,Teyhen DS,Elliott JM,et al. Rehabilitative ultra sound imaging:
understanding the technology and its applications. J Orthop Sports Phys
Ther.2007;37:434–449.

49
Figure legends:
Figure 1. Represents the position of the evaluator and the subjects during the test.
Figure 2. Sheet designed by the authors to standardize EMG and USI electrode placement.
EMG1 and EMG2 electrodes were placed at an angle of 63° and 72°, respectively, relative to
horizontal line. Vertical distance between EMG1 and transducer was of 5mm, while for the
EMG2 in relation to transducer was of 8mm. The distance of electrodes (EMG1 and EMG2)
center to center was of 33 mm.
Figure 3. Ultrasound image corresponding to the lateral abdominal wall during the analysis
process using a custom-made Matlab program. USI image was selected as close as possible to
the epochs selected for the EMG analyses. Each image was divided in two sides (white
circles): the right side (Thickness-1) related to EMG1 (at an angle of 63°) and the left side
(Thickness-2) related to EMG2 (at an angle of 72°). The yellow lines (superior and inferior
EO fascias) represent 1-cm area to calculate the Thickness values.

50
Figure 1. Represents the position of the evaluator and the subjects during the test.

51
Figure 2. Sheet designed by the authors to standardize EMG and USI electrode placement.
EMG1 and EMG2 electrodes were placed at an angle of 63° and 72°, respectively, relative to
horizontal line. Vertical distance between EMG1 and transducer was of 5mm, while for the
EMG2 in relation to transducer was of 8mm. The distance of electrodes (EMG1 and EMG2)
center to center was of 33 mm.

52
Figure 3. Ultrasound image corresponding to the lateral abdominal wall during the analysis
process using a custom-made Matlab program. USI image was selected as close as possible to
the epochs selected for the EMG analyses. Each image was divided in two sides (white
circles): the right side (Thickness-1) related to EMG1 (at an angle of 63°) and the left side
(Thickness-2) related to EMG2 (at an angle of 72°). The yellow lines (superior and inferior
EO fascias) represent 1-cm area to calculate the Thickness values.
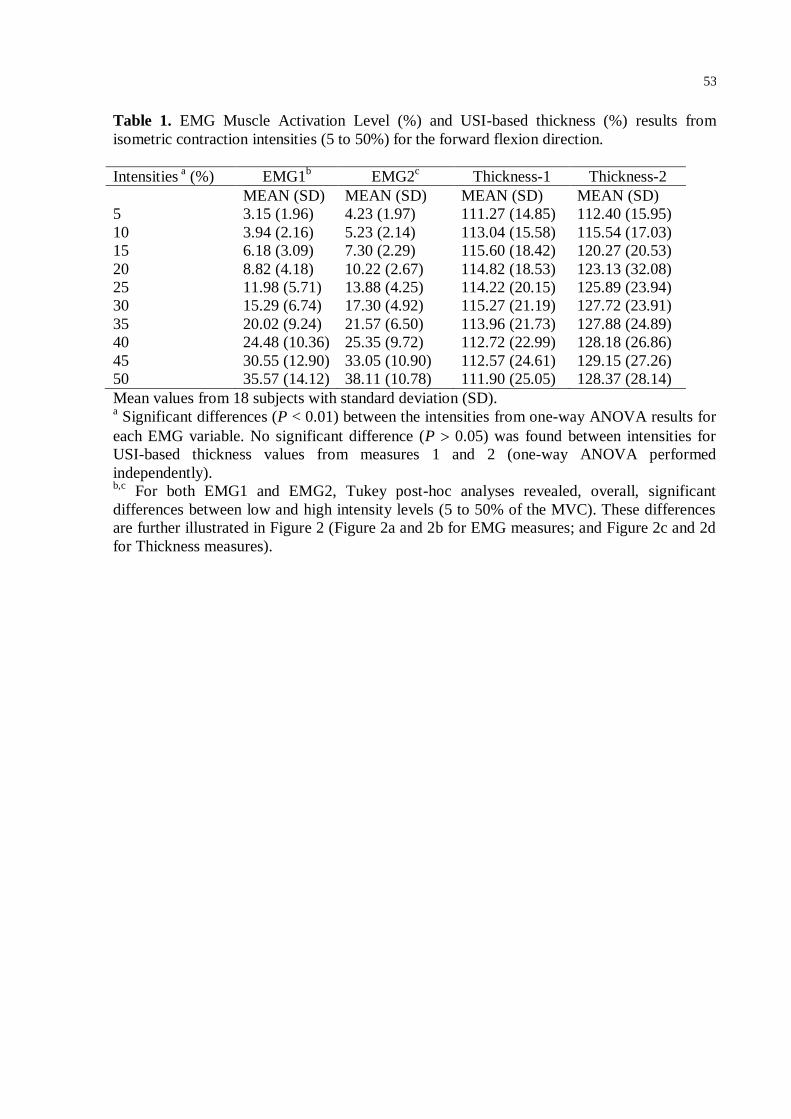
53
Table 1. EMG Muscle Activation Level (%) and USI-based thickness (%) results from
isometric contraction intensities (5 to 50%) for the forward flexion direction.
Intensities a (%) EMG1
b EMG2
c Thickness-1 Thickness-2
MEAN (SD) MEAN (SD) MEAN (SD) MEAN (SD)
5 3.15 (1.96) 4.23 (1.97) 111.27 (14.85) 112.40 (15.95)
10 3.94 (2.16) 5.23 (2.14) 113.04 (15.58) 115.54 (17.03)
15 6.18 (3.09) 7.30 (2.29) 115.60 (18.42) 120.27 (20.53)
20 8.82 (4.18) 10.22 (2.67) 114.82 (18.53) 123.13 (32.08)
25 11.98 (5.71) 13.88 (4.25) 114.22 (20.15) 125.89 (23.94)
30 15.29 (6.74) 17.30 (4.92) 115.27 (21.19) 127.72 (23.91)
35 20.02 (9.24) 21.57 (6.50) 113.96 (21.73) 127.88 (24.89)
40 24.48 (10.36) 25.35 (9.72) 112.72 (22.99) 128.18 (26.86)
45 30.55 (12.90) 33.05 (10.90) 112.57 (24.61) 129.15 (27.26)
50 35.57 (14.12) 38.11 (10.78) 111.90 (25.05) 128.37 (28.14)
Mean values from 18 subjects with standard deviation (SD). a Significant differences (P < 0.01) between the intensities from one-way ANOVA results for
each EMG variable. No significant difference (P 0.05) was found between intensities for
USI-based thickness values from measures 1 and 2 (one-way ANOVA performed
independently). b,c
For both EMG1 and EMG2, Tukey post-hoc analyses revealed, overall, significant
differences between low and high intensity levels (5 to 50% of the MVC). These differences
are further illustrated in Figure 2 (Figure 2a and 2b for EMG measures; and Figure 2c and 2d
for Thickness measures).
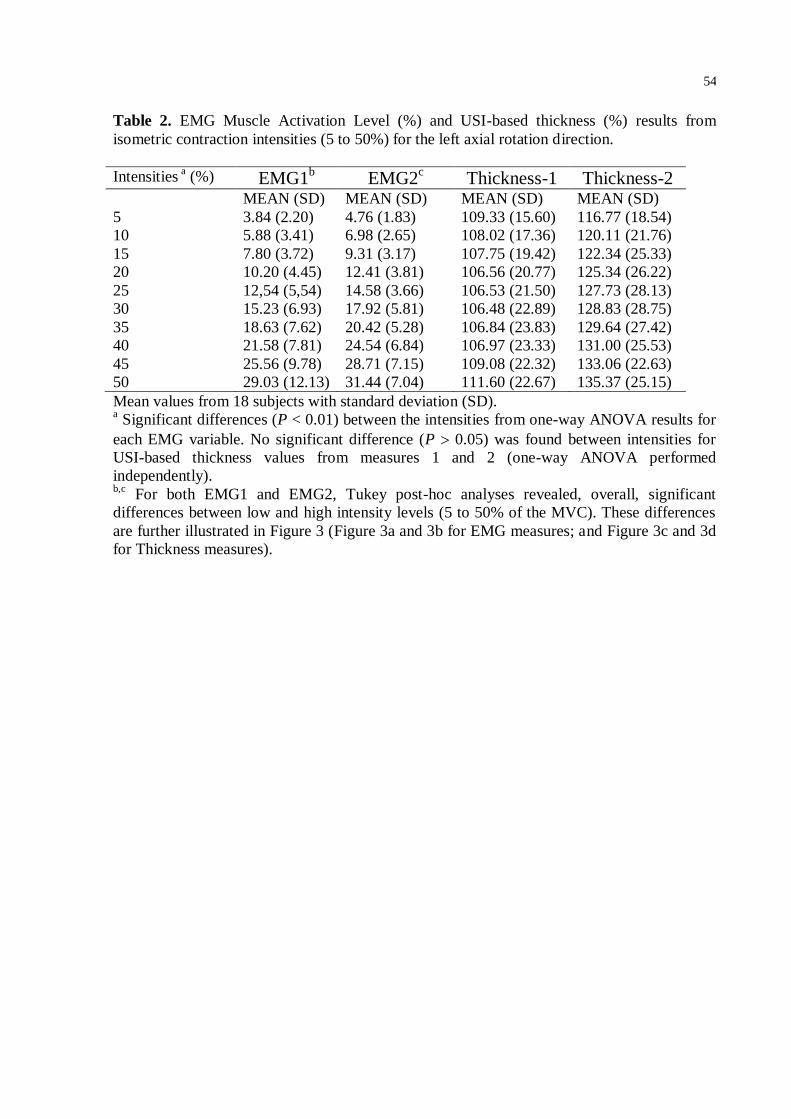
54
Table 2. EMG Muscle Activation Level (%) and USI-based thickness (%) results from
isometric contraction intensities (5 to 50%) for the left axial rotation direction.
Intensities a (%) EMG1
b EMG2
c Thickness-1 Thickness-2
MEAN (SD) MEAN (SD) MEAN (SD) MEAN (SD)
5 3.84 (2.20) 4.76 (1.83) 109.33 (15.60) 116.77 (18.54)
10 5.88 (3.41) 6.98 (2.65) 108.02 (17.36) 120.11 (21.76)
15 7.80 (3.72) 9.31 (3.17) 107.75 (19.42) 122.34 (25.33)
20 10.20 (4.45) 12.41 (3.81) 106.56 (20.77) 125.34 (26.22)
25 12,54 (5,54) 14.58 (3.66) 106.53 (21.50) 127.73 (28.13)
30 15.23 (6.93) 17.92 (5.81) 106.48 (22.89) 128.83 (28.75)
35 18.63 (7.62) 20.42 (5.28) 106.84 (23.83) 129.64 (27.42)
40 21.58 (7.81) 24.54 (6.84) 106.97 (23.33) 131.00 (25.53)
45 25.56 (9.78) 28.71 (7.15) 109.08 (22.32) 133.06 (22.63)
50 29.03 (12.13) 31.44 (7.04) 111.60 (22.67) 135.37 (25.15)
Mean values from 18 subjects with standard deviation (SD). a Significant differences (P < 0.01) between the intensities from one-way ANOVA results for
each EMG variable. No significant difference (P 0.05) was found between intensities for
USI-based thickness values from measures 1 and 2 (one-way ANOVA performed
independently). b,c
For both EMG1 and EMG2, Tukey post-hoc analyses revealed, overall, significant
differences between low and high intensity levels (5 to 50% of the MVC). These differences
are further illustrated in Figure 3 (Figure 3a and 3b for EMG measures; and Figure 3c and 3d
for Thickness measures).

55
Table 3. EMG Muscle Activation Level (%) and USI-based thickness (%) correlation results
from the mean (5 to 50%) value of isometric contraction during the forward flexion direction.
Subject EMG1 vs. Thickness-1 EMG2 vs. Thickness-2
r (P value) r (P value)
1 0.92 (0.001)* 0.67 (0.033)*
2 -0.73 (0.017)* -0.90 (0.000)*
3 0.92 (0.000)* 0.97 (0.000)*
4 -0.92 (0.000)* 0.41 (0.236)
5 0.59 (0.074) 0.82 (0.003)*
6 -0.35 (0.326) -0.30 (0.395)
7 0.38 (0.276) 0.93 (0.000)*
8 -0.25 (0.478) 0.95 (0.000)*
9 -0.74 (0.013)* 0.82 (0.004)*
10 0.92 (0.000)* 0.97 (0.000)*
11 0.26 (0.472) 0.87 (0.001)*
12 0.15 (0.671) 0.95 (0.000)*
13 -0.90 (0.000)* -0.01 (0.979)
14 -0.35 (0.328) -0.88 (0.001)*
15 0.88 (0.001)* -0.18 (0.615)
16 -0.66 (0.038)* 0.88 (0.001)*
17 0.82 (0.003)* 0.19 (0.600)
18 0.28 (0.426) 0.40 (0.258)
Mean -0.33 (0.348) 0.82 (0.004)*
*Significant Pearson correlation coefficient (r) between EMG Muscle Activation Level (%)
and USI-based thickness (%) measures by individual.

56
Table 4. EMG Muscle Activation Level (%) and USI-based thickness (%) correlation results
from the mean (5 to 50%) value of isometric contraction during the left axial rotation
direction.
Subject EMG1 vs. Thickness-1 EMG2 vs. Thickness-2
r (P value) r (P value)
1 -0.27 (0.437) 0.27 (0.433)
2 -0.74 (0.014)* 0.91 (0.000)*
3 0.83 (0.002)* 0.52 (0.120)
4 0.01 (0.970) 0.73 (0.014)*
5 0.43 (0.211) 0.84 (0.002)*
6 -0.005 (0.987) 0.89 (0.000)*
7 0.93 (0.000)* 0.98 (0.000)*
8 -0.55 (0.093) 0.51 (0.131)
9 -0.66 (0.034)* -0.59 (0,070)
10 -0.02 (0.093) 0.85 (0.000)*
11 0.86 (0.001)* 0.81 (0.004)*
12 0.79 (0.005)* 0.95 (0.000)*
13 -0.81 (0.004)* -0.15 (0.660)
14 -0.53 (0.109) 0.67 (0.031)*
15 0.15 (0.673) -0.56 (0.086)
16 0.33 (0.340) 0.84 (0.002)*
17 -0.40 (0.239) 0.11 (0.753)
18 0.47 (0.170) 0.94 (0.001)*
Mean 0.37 (0.285) 0.97 (0.001)*
*Significant Pearson correlation coefficient (r) between EMG Muscle Activation Level (%)
and USI-based thickness (%) measures by individual.

57
CONCLUSÃO GERAL
Esta pesquisa avaliou a utilização de uma nova ferramenta, o
ultrassom de imagem (USI), para avaliação o músculo externo oblíquo (OE). Esta
ferramenta pode ser utilizada por fisioterapeutas para avaliação e reabilitação dos
músculos abdominais em pacientes com diversas patologias, como a lombalgia.
Para estes profissionais utilizarem novas tecnologias, estas devem ser comparadas
ao padrão-ouro de medida da atividade muscular, no caso, a eletromiografia (EMG).
Devido aos poucos estudos e a grande diferença metodológica, a relação entre o
USI e a EMG ainda não esta clara na literatura. A diferença do nosso estudo em
relação aos anteriores foi o protocolo utilizando, no qual os sujeitos foram
posicionados sentados com apoio e foi realizada a contração em rampa (5 a 50% da
contração voluntária máxima [CVM]). Além disso, dois eletrodos foram posicionados
sobre o músculo EO e a medida da espessura muscular foi realizada em regiões
correspondentes a estes eletrodos.
Os resultados do presente estudo suportam a ideia de que o USI
não fornece, necessariamente, a mesma informação em relação a atividade elétrica
muscular captada pela EMG.
Desta forma, sugere-se que as medidas USI sejam utilizadas com
precaução, especialmente no que diz respeito a realização de pesquisas científicas
e na realização de avaliações clínicas para pacientes com alguma patologia.
Principalmente devido a alta variabilidade dos resultados encontrado entre os
sujeitos.
Novas pesquisas são necessárias utilizando um protocolo similar de
avaliação, porém com maior número de participantes. Sendo assim, a correlação
entre a EMG e o USI permanece inconclusiva.

58
REFERÊNCIAS
1. McGill SM. Kinetic potential of the lumbar trunk musculature about 3 orthogonal
orthopedic axes in extreme postures. Spine. 1991;(16):809–816.
2. Arjmand N, Shirazi-Adl A, Parnianpour M. Trunk biomechanics during maximum
isometric axial torque exertions in upright standing. Clinical
Biomechanics.2008;23:969–978.
3. Callaghan JP, Patla AE, McGill SM. Low back three-dimensional joint forces,
kinematics, and kinetics during walking. Clinical Biomechanics. 1999;14:203–216.
4. Masani K, Sin VW, Vette AH, Thrasher TA, Kawashima N, Morris A, Preuss R,
Popovic MR. Postural reactions of the trunk muscles to multi-directional
perturbations in sitting. Clinical Biomechanics. 2009;24:176–182.
5. Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine:
Implications for injury and chronic low back pain. Clinical Biomechanics. 1996;
11:1–15.
6. El Ouaaid Z, Arjmand N, Shirazi-Adl A, Parnianpur M. A novel approach to
evaluate abdominal coactivities for optimal spinal stability and compression force
in lifting. Computer Methods in Biomechanics and Biomedical Engineering.2009;
12(6):735-45
7. Campbell EJM, Green JH. The variations in intra-abdominal pressure and the
activity of the abdominal muscles during breathing: a study in man. Journal of
Physiology. 1953;122:282–290.
8. Monfort-Pañego M, Vera-García FJ, Sánchez-Zuriaga D, Sarti-Martínez MA.
Electromyographic studies in abdominal exercises: A literature synthesis. Journal
of Manipulative and Physiological Therapeutics. Volume 32, Number 3. 232-2444,
2009
9. Bergmark A. Stability of the lumbar spine: A study in mechanical engineering. Acta
Orthop Scand. 1989;230:20–4.
10.Brown SHM, Banuelos K, Ward SR, Lieber RL. Architectural and morphological
assessment of rat abdominal wall muscles: comparison for use as a human model.
J Anat. 2010; 217(3): 196–202.
11.Hu H, Meijer OG, Hodges PW, Bruijn SM, Strijers RL, et al. Control of the lateral
abdominal muscles during walking. Human Movement Science. 2011; 25: [Epub
ahead of print]

59
12.Hodges PW, Richardson CA. Relationship between limb movement speed and
associated contraction of the trunk muscles. Ergonomics. 1997;40(11):1220–30.
13.Seroussi RE, Pope MH. The relationship between trunk muscle electromyography
and lifting moments in the sagittal and frontal planes. Journal of Biomechanics.
1987; 20:135–146.
14.McGill SM. Electromyographic activity of the abdominal and low back musculature
during the generation of isometric and dynamic axial trunk torque: Implications for
lumbar mechanics. Journal of Orthopaedic Research.1991; 9:91–103.
15.Benninghoff A, Goerttler K. Lehrbuch der Anatomie des Menschen, Erster Band
[Textbook of human anatomy, Volume One]. München: Urban &
Schwarzenberg;1994.
16.Hodges P. Transversus abdominis: A different view of the elephant. British
Journal of Sports Medicine.2008; 42: 941–944.
17.Cordo PJ, Nashner LM. Properties of postural adjustments associated with rapid
arm movements. J Neurophysiol.1982;47(2):287–302.
18.Friedli WG, Cohen L, Hallet M, Stanhope S, Simon SR. Postural adjustments
associated with rapid voluntary arm movements II. Biomechanical analysis. J
Neurol Neurosurg Psychiatry. 1988;51(2): 232–43.
19.Snijders CJ, Bakkerl MP, Weeming A, Stoeckaw R, Stam HJ. Oblique abdominal
muscle activity in standing and in sitting on hard and soft seats. Clinical
Biomechanics.1995; 10(2):73-78.
20.Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation
between the tranvsersus abdominis muscles, sacroiliac joint mechanics, and low
back pain. Spine. 2002; 27(4):399–405.
21.Callaghan JP, McGill SM. Low back joint loading and kinematics during standing
and unsupported sitting. Ergonomics. 2001;44:280–94.
22.O’Sullivan PB, Dankaerts W, Burnett AF, Farrell GT, et al. Effect of Different
Upright Sitting Postures on Spinal- Pelvic Curvature and Trunk Muscle Activation
in a Pain-Free Population. Spine.2006; 31(19):707-712.
23.John EK, Beith ID. Can activity within the external abdominal oblique be
measured using real-time ultrasound imaging?. Clinical Biomechanics.2007;
22:972–979
24.Hides J, Wilson S, Stanton W, et al. An MRI investigation into the function of the
transversus abdominis muscle during “drawing- in” of the abdominal wall. Spine.

60
2006;31(6):175-178.
25.Juul-Kristensen B, Bojsen-Moller F, Holst E, et al. Comparison of muscle sizes
and moment arms of two rotator cuff muscles measured by ultrasonography and
magnetic resonance imaging. Eur J Ultrasound.2000; 11:161-73.
26.McMeeken JM, Beith ID, Newham DJ, et al. The relationship between EMG and
change in thickness of transverses abdominis. Clin Biomech.2004; 19:337-42.
27.Teyhen DS, Gill NW, Whittaker JL, Henry SM, Hides JA, Hodges P. Rehabilitative
ultrasound imaging of the abdominal muscles. J Orthop Sports Phys Ther.
2007;37 (8): 450-466.
28.Hodges PW, Pengel LH, Herbert RD, Gandevia SC. Measurement of muscle
contraction with ultrasound imaging. Muscle Nerve.2003; 27: 682-692.
29.Panjabi M.M. The stabilizing system of the spine. Part I. Function, dysfunction,
adaptation, and enhancement. Journal of Spinal Disorders.1992; 5(4):383-389.
30.Panjabi M.M. Clinical spinal instability and low back pain. Journal of
Electromyogr.Kinesiol.2003; 13(4): 371-379.
31.Panjabi M.M. A hypothesis of chronic back pain: ligament subfailure injuries lead
to muscle control dysfunction. Eur.Spine J.2006; 15(5): 668-676.
32.Urquhart DM, Barker PJ, Hodges PW, Story IH, Briggs CA. Regional morphology
of the transversus abdominis and obliquus internus and externus abdominis
muscles. Clin Biomech .2005; 20: 233-241.
33.Moore, K., Dalley, A. Clinically Oriented Anatomy, 4th edition, Baltimore:
Lippincott Williams & Wilkins; 1999.
34.Williams PL, Bannister LH, Berry MM. Gray’s Anatomy. The Anatomical Basis of
Medicine and Surgery. London, UK: Churchill Livingstone; 1999.
35.Barker PJ. Applied Anatomy and Biomechanics of the Lumbar Fascia:
Implications for Segmental Control [dissertation]. Melbourne, Australia: University
of Melbourne; 2005.
36.G. Mirka, D. Kelaher, A. Baker, A. Harrison, J. Davis. Selective activation of the
external oblique musculature during axial torque production. Clinical
Biomechanics.1997; 12: 172-180.
37.Rankin G, Stokes M, Newham DJ. Abdominal muscle size and symmetry in
normal subjects. Muscle Nerve.2006; 34: 320-326.
38.Rizk NN. A new description of the anterior abdominal wall in man and mammals. J
Anat.1980; 131: 373-385.
61
39.Stephen H. M. Brown, Samuel R. Ward, Mark S. Cook, Richard L. Lieber.
Architectural Analysis of Human Abdominal Wall Muscles: Implications for
Mechanical Function. Spine (Phila Pa 1976). 2011; 36(5): 355–362.
40.Gardner-Morse, M., Stokes, I. The effects of abdominal muscle coactivation on
lumbar spine stability. Spine.1998; 23: 86–91.
41.Granata, K.P., Marras, W.S. Cost–benefit of muscle cocontraction in protecting
against spinal instability. Spine.2000; 25: 1398–1404.
42.McGill, S.M. Low back stability: from formal description to issues for performance
and rehabilitation. Exerc. Sport. Sci. Rev.2001; 29: 26–31.
43.Cholewicki, J., VanVliet, J.J. Relative contribution of trunk muscles to the stability
of the lumbar spine during isometric exertions. Clin. Biomech.2002; 17: 99–105.
44.Richardson, C., Jull, G., Hodges, P., Hides, J. Therapeutic Exercise for Spinal
Segmental Stabilization in Low Back Pain. Churchill Livingstone. 1999.
45.Richardson, C., Hodges, P.W., Hides, J. Therapeutic Exercise for Lumbopelvic
Stabilization: A Motor Control Approach for the Treatment and Prevention of Low
Back Pain. Churchill Livingstone. 2004.
46.Hodges PW; Richardson CA. Inefficient muscular stabilization of the lumbar spine
associated with low back pain. A motor control evaluation of transverses
abdominis. Spine.1996; 21: 2640-2650.
47.Stetts DM, Freund JE, Allison SC, Carpenter G. A Rehabilitative Ultrasound
Imaging Investigation of Lateral Abdominal Muscle Thickness in Healthy Aging
Adults. Journal of Geriatric Physical Therapy.2009; 32(2): 60-6.
48.Rubin DI. Epidemiology and risk factors for spine pain. Neurol Clin. 2007; 25(2):
353–371.
49.Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of chronic low
back pain. Arch Intern Med. 2009; 169(3): 251–258.
50.Ferreira PH, Ferreira ML,Hodges PW. Changes in Recruitment of the Abdominal
Muscles in People With Low Back Pain - Ultrasound Measurement of Muscle
Activity. Spine.2004; 29(22): 2560–2566.
51.Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing
exercises for first-episode low back pain. Spine.2001; 26: 243-248.
52.Stuge B, Veierod MB, Laerum E, Vollestad N. The efficacy of a treatment program
focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a
two-year follow-up of a randomized clinical trial. Spine.2004; 29: 197-203.

62
53.Bouisset S, Maton B. Muscles, posture et mouvement. Bases et applications de la
méthode électromyographique. Paris. 1995.
54.Portney LG, Roy SH. Eletromiografia e testes de velocidade de condução
nervosa. In: O´Sullivan SB, Schmitz TJ. Fisioterapia avaliação e tratamento. 4ª Ed.
São Paulo: Manole; 2004. p. 213-256.
55.De Lucca CJ. The use of surface electromyography in biomechanics. J Appl
Biomech.1997; 13: 135-63.
56.Bigland-Ritchie B, Lippold OCJ. The relations between force, velocity and
integrated electrical activity in human muscles. J Physiol.1984; 123: 214-224.
57.Vasseljen O, Fladmarkb AM, Westad C, Torp HS. Onset in abdominal muscles
recorded simultaneously by ultrasound imaging and intramuscular
electromyography. Journal of Electromyography and Kinesiology.2009; 19: 23-31.
58.Costa LOP, Maher CG, Latimer J, Smeets RJ. Systematic Review for the
Measurement of Abdominal Muscle Activity: A Reproducibility of Rehabilitative
Ultrasound Imaging. Phys Ther. 2009; 89: 756-769.
59.Comfort P Pearson SJ, Mather D. An electromyographical comparison of trunk
muscle activity during isometric trunk and dynamic strengthening exercises.
Journal of Strength and Conditioning Research.2011; 25(1): 149-54.
60.Parnianpour JKF, Kippers V, Richardson CA. Reliability of electromyographic and
torque measures during isometric axial rotation exertions of the trunk. Clinical
Neurophysiology.2003; 114: 2355–2361.
61.Soderberg GL, Knutson LM. A guide for use and interpretation of kinesiologic
electromyographic data. Phys Ther.2000; 80: 485–98.
62.Pullman SL, Goodin DS, Marquinez AI, Tabbal S, Rubin M. Clinical utility of
surface EMG. Report of the Therapeutics and Technology Assessment
Subcommittee of the American Academy of Neurology.2000; 55: 171–7.
63.Kumar S, Mital A. Electromyography in ergonomics. London: Taylor and Francis.
1996.
64.Basmakian JV, Lucca CJ. Muscle alive: their function revealed by
electromyography. 5th ed. Williams & Wilkins; Baltimore, 1985.
65.Sodeberg GL, Knuston LM. A guide for use and interpretation of kinesiologic
electromyographic data. Phys Ther.2000; 80(5): 485-498.
66.Whittaker JL, Teyhen DS, Elliott JM, Langevin KC, Dahl H, Stokes M.
Rehabilitative Ultrasound Imaging: Understanding the Technology and Its

63
Applications. Journal of Orthopaedic & Sports Physical therapy.2007; 37(8): 434-
49.
67.Ikai M, Fukunaga T. Calculation of muscle strength per unit cross-sectional area
of human muscle by means of ultrasonic measurement. Int Z Angew Physiol.1968;
26: 26-32.
68.Young A, Hughes I, Russell P, Parkers MJ, Nichols PJ. Measurement of
quadriceps muscle wasting by ultrasonography. Rheumatol Rehabil.1980; 19: 141-
148.
69.Teyhen D. Rehabilitative Ultrasound Imaging Symposium. Journal of Orthopaedic
& Sports Physical therapy.2006; 36(8): A1-17.
70.Hides JA, Stokes MJ, Saide M, et al. Evidence of lumbar multifidus muscle
wasting ipsilateral to symptoms in patients with acute/subacute low back pain.
Spine.1994; 19: 165–72.
71.Hodges P, Holm AK, Hansson T, et al. Rapid atrophy of the lumbar multifidus
follows experimental disc or nerve root injury. Spine.2006; 3: 2926–33.
72.Kiesel KB, Uhl TL, Underwood FB, et al. Measurement of lumbar multifidus
muscle contraction with rehabilitative ultrasound imaging. Man Ther.2007; 12:
161–6.
73.Brown SHM, McGill SM. A comparison of ultrasound and electromyography
measures of force and activation to examine the mechanics of abdominal wall
contraction. Clinical Biomechanics.2010; 25: 115–123.
74.Castelo PM, Gavião MBD, Pereira LJ, Bonjardim LR. Masticatory muscle
thickness, bite force, and occlusal contacts in young children with unilateral
posterior crossbite. European Journal of Orthodontics.2007; 29: 149–156.
75.Bilodeau M, Arsenault AB, Gravel D, Bourbonnais D. EMG power spectra of
elbow extensors during ramp and step isometric contractions. Eur J Appl
Physiol.1991; 63: 24-28.
76.Hebert JJ, Koppenhaver SL, Parent EC, Fritz JM. A Systematic Review of the
Reliability of Rehabilitative Ultrasound Imaging for the Quantitative Assessment of
the Abdominal and Lumbar Trunk Muscles. Spine.2009; 34(23): 848–856.

64
ANEXOS

65
ANEXO A
Normas de formatação do periódico Journal of Electromyography
and Kinesiology.
http://www.elsevier.com/wps/find/journaldescription.cws_home/3044
2/authorinstructions

66
1. Guide for Authors
The Journal of Electromyography and Kinesiology aims to provide a single,
authoritative forum for the publication of original research and clinical studies on muscle contraction and
human motion through combined or separate mechanical and electrical detection techniques. Some of
the key topics covered include: control of movement; muscle and nerve properties; electrical
stimulation; sports and exercise; rehabilitation; muscle fatigue; joint biomechanics; motion analysis;
measures of human performance; neuromuscular diseases; physiological modelling; posture and
movement. The Journal welcomes the submission of original papers, reviews and letters to the Editors.
The Journal will also publish book reviews and a calendar of forthcoming events. Please note that, at the
discretion of the Editor in Chief, some papers may be accepted for online publication only.
PUBLICATION CONDITION
A manuscript submitted to this journal can only be published if it (or a similar version) has not been
published and will not be simultaneously submitted or published elsewhere. A violation of this condition is
considered as fraud, and will be answered by appropriate sanctions against all authors. Two manuscripts
are considered similar if their subjects concern the same hypothesis, question or goal, addressed with
the same scientific methodology.
REFEREEING
All contributions are read by two or more referees to ensure both accuracy and relevance, and
amendments to the script may thus be required before final acceptance. On acceptance, contributions
are subject to editorial amendment to suit house style.
AUTHORSHIP
All authors should have made substantial contributions to all of the following: (1) the conception and
design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article
or revising it critically for important intellectual content, (3) final approval of the version to be submitted.

67
CHANGES TO AUTHORSHIP
This policy concerns the addition, deletion, or rearrangement of author names in the authorship of
accepted manuscripts:
Before the accepted manuscript is published in an online issue: Requests to add or remove an author, or
to rearrange the author names, must be sent to the Journal Manager from the corresponding author of
the accepted manuscript and must include: (a) the reason the name should be added or removed, or the
author names rearranged and (b) written confirmation (e-mail, fax, letter) from all authors that they
agree with the addition, removal or rearrangement. In the case of addition or removal of authors, this
includes confirmation from the author being added or removed. Requests that are not sent by the
corresponding author will be forwarded by the Journal Manager to the corresponding author, who must
follow the procedure as described above. Note that: (1) Journal Managers will inform the Journal Editors
of any such requests and (2) publication of the accepted manuscript in an online issue is suspended until
authorship has been agreed.
After the accepted manuscript is published in an online issue: Any requests to add, delete, or rearrange
author names in an article published in an online issue will follow the same policies as noted above and
result in a corrigendum.
ACKNOWLEDGEMENT OF OTHER CONTRIBUTORS
All contributors who do not meet the criteria for authorship as defined above should be listed in an
acknowledgements section. Examples of those who might be acknowledged include a person who
provided purely technical help, writing assistance, or a department chair who provided only general
support. Authors should disclose whether they had any writing assistance and identify the entity that
paid for this assistance.
CONFLICT OF INTEREST
"Conflict of interest statement" all authors must disclose any financial and personal relationships with
other people or organisations that could inappropriately influence (bias) their work. Examples of potential
conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert
testimony, patent applications/registrations, and grants or other funding. If there are no conflicts of
interest, the authors should state there are none.

68
ROLE OF THE FUNDING SOURCE
All sources of funding should be declared as an acknowledgement at the end of the text. Authors should
declare the role of study sponsors, if any, in the study design, in the collection, analysis and
interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for
publication. If the study sponsors had no such involvement, the authors should so state.
PREPARATION OF SCRIPTS
All publications will be in English. Authors whose 'first' language is not English should arrange for their
manuscripts to be written in idiomatic English before submission. Please also ensure that your
manuscript has been thoroughly checked for errors prior to submission.
Language Editing: International Science Editing and Asia Science Editing can provide English language
and copyediting services to authors who want to publish in scientific, technical and medical journals and
need assistance before they submit their article or, it is accepted for publication. Authors can contact
these services directly: International Science Editing http://www.internationalscienceediting.com and
Asia Science Editing http://www.asiascienceediting.com or, for more information about language editing
services, please [email protected] who will be happy to deal with any questions.
Please note Elsevier neither endorses nor takes responsibility for any products, goods or services offered
by outside vendors through our services or in any advertising. For more information please refer to our
terms & conditions http://authors.elsevier.com/terms_and_conditions.html.
You should have your contribution typed in double-line spacing, on one side only of A4 paper. Do not
underline anything and leave wide margins. Please also add line numbers to your submitted manuscript
(e.g. 5, 10 , 15 etc.) and number every page.
EMG data should be collected and presented according to the 'Standards for Reporting EMG Data' printed
at the back of each issue of this journal.
All authors should sign a cover note to acknowledge that they have read, and approve of, the content of
the manuscript as submitted.

69
SUBMISSIONS
Authors are requested to submit their original manuscript and figures online
via http://ees.elsevier.com/jek. This is the Elsevier web-based submission and review system. You will
find full instructions located on this site. Please follow these guidelines to prepare and upload your
article. Once the uploading is done, the system automatically creates an electronic pdf proof, which is
then used for reviewing. All correspondence, including notification of the Editor's decision and requests
for revisions, will be managed via this system. Paper copies and email submissions are also currently
accepted. Please submit to:
For the Americas, Europe, Africa and the Middle East:
Professor M. Solomonow, Professor & Director, Bioengineering Division & Musculoskeletal Disorders
Research Laboratory, University of Colorado Health Sciences Center, Mailstop 8343, PO Box 6511,
Aurora, CO., 80045, USA; Tel.: (303) 724-0383, Fax: (303) 724-0394
For the Far East and Australia:
Professor T. Moritani, Laboratory of Applied Physiology, The Graduate School of Environmental Studies,
Kyoto University, Sakyo-ku, Kyoto 606, Japan; Tel: 81 75 753 6888, Fax: 81 75 753 6734
No page charges are made to authors for material published.
Arrangement of papers
JEK now accepts original articles within a word limit of 5,000 words (including title page, abstract, text,
references & figure legends). Reviews and special articles (keynote lectures or a Special issue articles)
are exempted from this limit.
You should arrange your contribution in the following order:
1. Title page including the article title, author(s), affiliation(s), keywords and one author identified for
correspondence

70
2. A 200 word abstract outlining the purpose, scope and conclusions of the paper
3. The text, suitably divided under headings
4. Acknowledgements (if any)
5. References
6. Tables (each on separate sheet)
7. Captions to illustrations (grouped on a separate sheet or sheets)
8. Illustrations, each on a separate sheet containing no text.
All submissions should be accompanied by a declaration signed by each author that the paper has not
been previously published or submitted for consideration elsewhere.
TEXT
Subdivide your paper in the simplest way possible, consistent with clarity using the standard format of
introduction, methods, results and discussion.
TABLES
Number tables consecutively throughout the paper (with Arabic numerals) referring to them in the text
as Table 1, Table 2 etc. with a caption at the top of each table. Avoid the use of vertical rules. Tables
should not duplicate results presented in graphs.
ILLUSTRATIONS
All illustrations should be identified with the author's name and figure number marked in pencil.
Line illustrations

71
Articles may be published more quickly if illustrations are supplied to the required standards, authors
should not be deterred if they are unable to meet these standards as illustrations can be redrawn in-
house. The originals must be supplied on separate sheets, with two photocopies. Illustrations will be
reduced in size photographically, typically to fit one or two columns of the journal and this should be
borne in mind to ensure that lines and lettering remain clear when reduced. If you label the original
illustrations do so in black ink using a suitable stencil. Lower case letters should be used throughout, with
an initial capital letter for the first word only. If suitable stencils are unavailable label a photocopy, not
the original illustrations, and our studio will complete the work to the correct standard. If your
illustrations are computer-generated follow the lettering standards as above and supply the blackest
possible laser printout.
For full instructions on the electronic submission of artwork, please visit: http://ees.elsevier.com/jek.
Graphs
The minimum amount of descriptive text should be used on graphs and drawings (label curves, points,
etc, with single-letter symbols). Descriptive matter should be placed in the figure caption. Scale grids
should not be used in graphs, unless required for actual measurements. Graph axes should be labelled
with variables written out in full, along the length of the axes, with the unit in parentheses (for example,
Time(s)). A table is usually more satisfactory for recording data.
Photographs
Supply glossy, black and white, unmounted prints or 35 mm transparencies, plus two photocopies. A
scale, where appropriate, should be marked on the photographs or included in the caption.
Colour Illustrations
If, together with your accepted article, you submit usable colour figures then Elsevier will ensure, at no
additional charge, that these figures will appear in colour on the web (e.g., ScienceDirect and other sites)
regardless of whether or not these illustrations are reproduced in colour in the printed version. For colour
reproduction in print, you will receive information regarding the costs from Elsevier after receipt of your
accepted article. For further information on the preparation of electronic artwork, please
see http://ees.elsevier.com/jek. Please note: Because of the technical complications which can arise by
72
converting colour figures to 'grey scale' (for the printed version should not opt for colour in print) please
submit in addition usable black and white prints corresponding to all the colour illustrations. Submit
colour illustrations as original photographs high-quality computer prints or transparencies, close to the
size expected in publication, or as 35 mm slides. Polaroid colour prints are not suitable.
REFERENCES
The reference list should be constructed alphabetically. Where more than one reference has the same
first author, use the next named author to construct the list alphabetically. For identical author groups,
list the references by date. References should be cited in the text using the first author name plus the
year of the paper, eg Solomonow et al, 2004, in square brackets. References should be in the following
form:
Journal article
Paivio A, Jansen B, Becker LJ. Comparisons through the mind's eye. Cognition 1975;37(2):635-47
Book
Strunk W, White EB. The elements of style. 3rd ed. New York: Macmillan, 1979
Article or chapter in edited book
Gurman AS, Kniskern DP. Family therapy outcome research: knowns and unknowns. In: Gurman AS,
Kniskern DP, editors. Handbook of family therapy. New York: Brunner/Maazel, 1981:742-75.
Please ensure that references are complete, in that they include where relevant, author's name, article or
book title, volume and issue number, publisher, year and page reference. Journal titles should appear in
full.
UNITS AND ABBREVIATIONS
SI units and their accepted abbreviations should be used.

73
RANDOMISED CONTROLLED TRIALS
All randomised controlled trials submitted for publication in the journal should include a completed
Consolidated Standards of Reporting Trials (CONSORT) flow chart. Please refer to the CONSORT
statement website at http://www.consort-statement.org for more information. The Journal of
Electromyography and Kinesiology has adopted the proposal from the International Committee of Medical
Journal Editors (ICMJE) which require, as a condition of consideration for publication of clinical trials,
registration in a public trials registry. Trials must register at or before the onset of patient enrolment.
The clinical trial registration number should be included at the end of the abstract of the article. For this
purpose, a clinical trial is defined as any research project that prospectively assigns human subjects to
intervention or comparison groups to study the cause-and-effect relationship between a medical
intervention and a health outcome. Studies designed for other purposes, such as to study
pharmacokinetics or major toxicity (e.g. phase I trials) would be exempt. Further information can be
found at www.icmje.org.
ETHICS
Work on human beings that is submitted to the Journal should comply with the principles laid down in
the Declaration of Helsinki; Recommendations guiding physicians in biomedical research involving human
subjects. Adopted by the 18th World Medical Assembly, Helsinki, Finland, June 1964, amended by the
29th World Medical Assembly, Tokyo, Japan, October 1975, the 35th World Medical Assembly, Venice,
Italy, October 1983, and the 41st World Medical Assembly, Hong Kong, September 1989. The manuscript
should contain a statement that the work has been approved by the appropriate ethical committees
related to the institution(s) in which it was performed and that subjects gave informed consent to the
work. Studies involving experiments with animals must state that their care was in accordance with
institution guidelines. Patients' and volunteers' names, initials, and hospital numbers should not be used.
CHECKLIST
Have you told readers, at the outset, what they might gain by reading your paper?
Have you made the aim of your work clear?
Have you explained the significance of your combination?

74
Have you set your work in the appropriate context by giving sufficient background (including a complete
set of relevant references) to your work?
Have you addressed the question of practicality and usefulness?
Have you identified future developments that may result from your work?
Have you structured your paper in a clear and logical fashion?
COPYRIGHT
Upon acceptance of an article, authors will be asked to sign a "Journal Publishing Agreement" (for more
information on this and copyright see http://ees.elsevier.com/jek. Acceptance of the agreement will
ensure the widest possible dissemination of information. An e-mail (or letter) will be sent to the
corresponding author confirming receipt of the manuscript together with a "Journal Publishing
Agreement" form. If excerpts from other copyrighted works are included, the author(s) must obtain
written permission from the copyright owners and credit the source(s) in the article. Elsevier has
preprinted forms for use by authors in these cases : contact Elsevier's Rights Department, Philadelphia,
PA, USA: Tel. (+1) 215 238 7869; Fax (+1) 215 238 2239; e-mail [email protected] .
Requests may also be completed online via the Elsevier homepage
(http://www.elsevier.com/locate/permissions).
AGREEMENTS WITH FUNDING BODIES
Elsevier has established agreements and developed policies to allow authors who publish in this journal
to comply with manuscript archiving requirements of the following funding bodies, as specified as
conditions of researcher grant awards. Please
seewww.elsevier.com/wps/find/authorsview.authors/fundingbodyagreements for full details of the
agreements that are in place for these bodies:
• Arthritis Research Campaign (UK)
• British Heart Foundation (UK)
• Cancer Research (UK)
• Howard Hughes Medical Institute (USA)

75
• Medical Research Council (UK)
• National Institutes of Health (USA)
• Wellcome Trust (UK)
These agreements and policies enable authors to comply with their funding body's archiving policy
without having to violate their publishing agreements with Elsevier. The agreements and policies are
intended to support the needs of Elsevier authors, editors, and society publishing partners, and protect
the quality and integrity of the peer review process. They are examples of Elsevier's ongoing
engagement with scientific and academic communities to explore ways to deliver demonstrable and
sustainable benefits for the research communities we serve.
Authors who report research by funding bodies not listed above, and who are concerned that their author
agreement may be incompatible with archiving requirements specified by a funding body that supports
an author's research are strongly encouraged to contact Elsevier's author support team
([email protected]). Elsevier has a track-record of working on behalf of our authors to ensure
authors can always publish in Elsevier journals and still comply with archiving conditions defined in
research grant awards.
PROOFS
One set of page proofs in PDF format will be sent by e-mail to the corresponding author (if we do not
have an e-mail address then paper proofs will be sent by post). Elsevier now sends PDF proofs which can
be annotated; for this you will need to download Adobe Reader version 7 available free
from http://www.adobe.com/products/acrobat/readstep2.html. Instructions on how to annotate PDF
files will accompany the proofs. The exact system requirements are given at the Adobe site:
http://www.adobe.com/products/acrobat/acrrsystemreqs.html#70win. If you do not wish to use the PDF
annotations function, you may list the corrections (including replies to the Query Form) and return to
Elsevier in an e-mail. Please list your corrections quoting line number. If, for any reason, this is not
possible, then mark the corrections and any other comments (including replies to the Query Form) on a
printout of your proof and return by fax, or scan the pages and e-mail, or by post. Please use this proof
only for checking the typesetting, editing, completeness and correctness of the text, tables and figures.
Significant changes to the article as accepted for publication will only be considered at this stage with
permission from the Editor. We will do everything possible to get your article published quickly and

76
accurately. Therefore, it is important to ensure that all of your corrections are sent back to us in one
communication: please check carefully before replying, as inclusion of any subsequent corrections cannot
be guaranteed. Proofreading is solely your responsibility. Note that Elsevier may proceed with the
publication of your article if no response is received.
OFFPRINTS
The corresponding author, at no cost, will be provided with a PDF file of the article via e-mail or,
alternatively, 25 free paper offprints. The PDF file is a watermarked version of the published article and
includes a cover sheet with the journal cover image and a disclaimer outlining the terms and conditions
of use. Additional paper offprints can be ordered by the authors. An order form with prices will be sent to
the corresponding author.
PREPARATION OF SUPPLEMENTARY DATA
Elsevier now accepts electronic supplementary material to support and enhance your scientific research.
Supplementary files offer the author additional possibilities to publish supporting applications, movies,
animation sequences, high-resolution images, background datasets, sound clips and more.
Supplementary files supplied will be published online alongside the electronic version of your article in
Elsevier web products, including ScienceDirect: http://wwww.sciencedirect.com. In order to ensure that
your submitted material is directly usable, please ensure that data is provided in one of our
recommended file formats. Authors should submit the material in electronic format together with the
article and supply a concise and descriptive caption for each file. For more detailed instructions please
visit: http://ees.elsevier.com/jek.
AUTHOR ENQUIRIES
For enquiries relating to the submission of articles (including electronic submission where available)
please visit: http://ees.elsevier.com/jek.
Contact details for questions arising after acceptance of an article, especially those relating to proofs, are
provided after registration of an article for publication.

77
ANEXO B
Carta de aceite do Comitê de Ética Local e Protocolo.

78

79
80
81

82

83

84

85
86

87
ANEXO C
Termo de Conscentimento Livre e Esclarecido

88
89

90

91

92

93

94

95