Ministério da Saúde Fundação Oswaldo Cruz - Fiocruz Depto. de Imunologia - IOC Lab. de AIDS e...
52
Ministério da Saúde Fundação Oswaldo Cruz - Fiocruz Depto. de Imunologia - IOC Lab. de AIDS e Imunologia Molecular Seminário Brasil França 2006 Diversidade Genética e Genotipagem do HIV-1 aos Anti-Retrovirais José Carlos Couto-Fernandez Fortaleza,CE NOVEMBRO 2006
Transcript of Ministério da Saúde Fundação Oswaldo Cruz - Fiocruz Depto. de Imunologia - IOC Lab. de AIDS e...

Ministério da SaúdeFundação Oswaldo Cruz - FiocruzDepto. de Imunologia - IOCLab. de AIDS e Imunologia Molecular
Seminário Brasil França 2006
Diversidade Genética e Genotipagem do HIV-1 aos Anti-Retrovirais
José Carlos Couto-Fernandez
Fortaleza,CENOVEMBRO 2006

Histórico
1981 - Descrição dos primeiros casos de AIDS (Gottlieb 1981, CDC 1982)
1983 - Isolamento do HIV-1: L. Montagnier, França (Barré-Sinossi 1983)
1986 - Isolamento do HIV-2: Clavel, França
HIV Acentuada variabilidade genômica e fenotípica (Alizon 1984, 1986;
Wain-Hobson 1985; Asjo 1986)
1987 - Primeiro isolamento do HIV-1 no Brasil (Galvão-Castro 1987)
HIV Acentuada variabilidade genômica e fenotípica (Couto-Fernandez
1992, 1994; Potts 1993; WHO 1992,1994)
Estudos sobre diversidade do HIV são de fundamental relevância em relação
ao desenvolvimento de vacinas anti-HIV/AIDS e a susceptibilidade aos ARV.

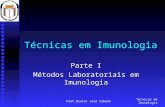
ESTIMATIVA DE ADULTOS/CRIANÇAS ESTIMATIVA DE ADULTOS/CRIANÇAS VIVENDO COM HIV/AIDSVIVENDO COM HIV/AIDS
Oeste Europeu
720 000720 000Norte e Centro-Leste da África
510 000510 000África Sub-
Saariana
25,8 25,8 milhõesmilhões
Leste Europeu e Ásia Central
1,6 milhão1,6 milhão
Sul e Sudeste da Ásia
7,4 milhões7,4 milhõesAustrália e
Nova Zelândia
74 00074 000
América do Norte
1,2 milhão1,2 milhãoCaribe
300 000300 000
América Latina
1,8 1,8 milhãomilhão
Total: 40,3 milhões
Leste Asiático e Pacífico
870 000870 000
Fonte: http://www.unaids.orgDezembro 2005

SUMÁRIO DA EPIDEMIA DE HIV/AIDS NO BRASIL 1980-2005
Número de casos de HIV/aids Total 371.827 Homens 251.979Mulheres 118.520 Crianças < 13 anos 10.404
Categoria de exposição(Adultos)
Sexual 224.463 Sanguínea 60.732
Vertical 10.404
Mortes por aids 1980-2004 Total 172.048
Ignorada 39.894
* Casos notificados até junho/2005
Fonte: Boletim Epidemiológico do Ministério da Saúde/ PN-DST e Aids-MS, 2005.
Prevalência: 0,65%

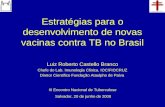
Notificações de Casos de Infecção pelo HIV-1 em Municípios Brasileiros (1980-2001)
1980-86
1987-93
1994-2001
Fonte:PN-DST/AIDS-MS, 2003

ESTRUTURA ESQUEMÁTICA DO HIV-1
Fonte: http://www.vircolab.com
FamíliaFamília
RETROVIRIDAERETROVIRIDAE
Subfamília Subfamília LENTiVIRINAELENTiVIRINAE
Gênero Gênero
LENTIVIRUSLENTIVIRUS

ORGANIZAÇÃO ESQUEMÁTICA DO GENOMA DO HIV-1
Adaptado de: http://www.hivmedicine.com/

• Length: 882.5 feet • Weight: 46,329 tons
• Length: .4 inches• Weight: < 1 ug
Comparison of Genomes: Human and VirusesComparação dos genomas: humano e víral
HIV-1 has to do many things with a limited genetic repertoire. Therefore, it exploits host factors in order to replicate.
O HIV-1 tem muitas coisas para fazer com um repertório genético limitado, por isso ele utiliza fatores do hospedeiro para se replicar.

HIV-1 Life CycleCiclo de Vida do HIV-1
REVERSE TRANSCRIPTION
VIRUS MATURATION
VIRION BINDING /UNCOATING
NUCLEAR ASSOCIATION OF VIRAL cDNA

Protease inhibitors(PI) act to bind directly to the HIV protease and block its activity
Os Inibidores de Protease(IP) agem ligando-se diretamente a protease do HIV bloqueando sua atividade

• Erros de transcrição da transcriptase reversa (TR) viral
• TR não possui atividade de reparo de DNA > Transcrição Reversa = Mutação
• Genoma (RNA) de ~104 nucleotídeos
• Taxa de erro da TR = ~2,7 X 10-4 mut / nt
• Índice de mutação de 1 erro/ 30.000 pb
• Elevada taxa de replicação viral (> Vírus gerados por dia = 1010 a 1011) e de ciclos replicativos (> 300 ciclos/ano)
Substituições de nucleotídeos, deleções e inserções Capacidade de recombinação Pressao das drogas ARV seleciona virus mutantes
ORIGEM DA DIVERSIDADE DO HIV-1

CLASSIFICAÇÃO DO HIV
• HIV-1HIV-1
--Pandemia MundialPandemia Mundial
-3 grupos: -3 grupos:
• HIV-2HIV-2
--OOeste da Áfricada África
-Homologia de 80% com -Homologia de 80% com SIVSIVsooty mangabeysooty mangabey
-Homologia entre 40-60% -Homologia entre 40-60% com HIV-1com HIV-1
- 8 subtipos: A, B e (C, D, E, - 8 subtipos: A, B e (C, D, E, F, G, H)F, G, H)
Grupo MGrupo M9 Subtipos: 9 Subtipos: A-D, F-H, J e KA-D, F-H, J e K
- 32 CRF- 32 CRF - Várias URF- Várias URF
Grupo OGrupo OGuiné Equatorial,Guiné Equatorial,Camarões e GabãoCamarões e Gabão
Grupo NGrupo N Camarões Camarões

Árvore filogenética dos diferentes
grupos e subtipos de HIV-1

DISTRIBUIÇÃO GLOBAL DOS SUBTIPOS DISTRIBUIÇÃO GLOBAL DOS SUBTIPOS GENÉTICOS (GENÉTICOS (envenv) DO HIV-1) DO HIV-1
CC
BB
EEBB
CC
BB
BB
BB AA
BBAA
AADD
OtherOther
BB AA
OtherOther
AA
BB
CC
Others 5%(F, G, H, J, NT)
DD5.3%
CC 47.2%
E E 3.2%
B B 12.3%
AA 27%
Adaptado de: Osmanov S, 2005. WHO-UNAIDS HIV Isolation and Characterization
BB
CC
CC
CC

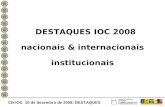
RORAIMARORAIMA
(1)(1)
B,F,B/F
B,F,B/F,C
B,F,B/F
B,F,B/F,C,D,A,CRF02_AG
C,B,B/C,F,B/F,A
DISTRIBUIÇÃO DOS SUBTIPOS DE HIV-1 NO BRASIL

DETECÇÃO E QUANTIFICAÇÃO VIRALDETECÇÃO E QUANTIFICAÇÃO VIRAL
VACINASVACINAS
SOROLOGIASOROLOGIA
RESISTÊNCIA aos ANTI-RETROVIRAISRESISTÊNCIA aos ANTI-RETROVIRAIS
PATOGENICIDADEPATOGENICIDADE
IMPLICAÇÕES DA DIVERSIDADE DO HIV-1IMPLICAÇÕES DA DIVERSIDADE DO HIV-1

• Isolados de HIV-1 grupo O e HIV-2 são naturalmente resistentes aos ITRNN (Descamps, 1997).
• Redução de susceptibilidade in vitro aos ITR (ZDV, 3TC, ddI, NVP) de isolados de HIV-1 subtipo D (Palmer, 1997).
• Redução de susceptibilidade in vitro aos IP de isolados do subtipo G (Descamps, 1998).
• Redução de susceptibilidade in vitro aos ITRNN em isolados do subtipo F (Apetrei, 1998).
• Elevada ocorrência de mutações de resistência em amostras do subtipo C após dose única de nevirapina, em comparação aos subtipos A e D (Eshleman 2005)
• Diferentes estudos tem mostrado a existência de polimorfismos (‘minor mutation” e substituições atípicas) entre amostras não-B em posições associadas a resistência na protease e TR (Vergne 2000; Kantor & Katzenstein 2003).
Subtipos de HIV e Susceptibilidade as Subtipos de HIV e Susceptibilidade as Drogas Anti-retroviraisDrogas Anti-retrovirais

Resposta ARV e Subtipos B/F
0
1
2
3
4
5
6
W=0p<0.16
W=4p<0.12
W=24p<0.13
W=32p<0.06
W=48p<0.02
Vira
l Loa
d (L
OG
)
B
F
JAIDS 24,4:399-4000, 2000


Resistência in vivo ao Nelfinavir
Primeira Falha ao Nelfinavir
D30N L90M
Resgate fácilResgate fácil Resistência cruzadaResistência cruzada
(Não B = 100%)(Não B = 100%)57.1%57.1% 43.9%43.9%

Diversidade Genética do HIV e alteração natural da susceptibilidade a ARVs
Subtipo C e rápida resistência a ITRNN (V106M)
Subtipo F “resistência natural” aos IPs (L89M)
Subtipo C hipersusceptibilidade ao Lopinavir-r
(I93L, CH50 = 0,35)

Programa Brasileiro para Terapia anti-HIV/AIDS Entre os diferentes programas conduzidos pelo Programa Nacional de DST e Aids-MS para pessoas vivendo com HIV/Aids, destaca-se o acesso universal gratuito as diferentes drogas que compoem a terapia anti-retroviral (TARV).
Inicida nos anos 90 através da distribuição do AZT, este programa se consolidou ao longo dos anos.
Em 1996 com a introdução da terapia combinada de alta potência (HAART), a grande maioria de dos indivíduos infectados pelo HIV-1, tem acesso garantido a todas medicações que compoem a TARV.
Estabelecimento das redes de laboratorios para quantificacao de CD4/CD8 e carga viral do HIV-1.
A politica brasileira de acesso universal a terapia anti-HIV tem resultado na queda dos níveis de morbidade e motalidade e uma melhora significativa da qualidade de vida dos indivíduos infectados (Marins e cols., 2003).

O desenvolvimento de resistência às drogas anti-HIV/Aids, além de acarretar a falha em suprimir a replicação viral, pode comprometer o Programa Brasileiro de acesso universal a TARV aos pacientes infectados.
Com isto, o Ministério da Saúde através do Programa Nacional de DST e AIDS estabeleceu em 2002 a Rede Nacional de Genotipagem da Resistência do HIV-1 (RENAGENO).
Objetivo Principal
Instalar uma rede composta de laboratórios e médicos de referência em genotipagem (MRGs), capacitados a realizar a interpretação dos exames de genotipagem para pacientes infectados pelo HIV/Aids através rede pública de saúde,.
RELEVÂNCIA

Composto de 21 laboratórios nas 5 diferentes regiões do Brasil.
Pará (PA): 01
Pernambuco (PE): 01
Bahia (BA): 01
Brasília (DF): 01
Minas Gerais (MG): 01
Rio de Janeiro (RJ): 03
São Paulo (SP): 03
Rio G. do Sul (RS): 01
ES, PR, SC,CE: 01
Rede de Laboratórios da RENAGENO

RENAGENO STRUCTURE
Clinical
Genotyping Reference Doctor-MRG
Laboratory
Analysis Collect samples

METODOLOGIA
ViroSeqTM HIV-1 Genotyping System V 2.0 (ABBOTT)
Extraction / purification of viral RNA
Stage 1,3 mL plasma
Sample Preparation Module
HIV Plasmatic RNA
Quantification agarose gelDNA Mass Ladder*
RT-PCR Module, Prt/5’ RT
cDNA
PCR Module
Amplified HIV-1 DNA
Purificated DNA fragments
* 1.8Kb

METODOLOGIA 2
Sequencing Module
Sequencing
Processing Sequences
Analysis
Sequence Analysis HIV-1 Resistance Report

Fisher’s exact test: *p <0.05.
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
80,0%
M4
1L
E44
D
A62
V
K65
R
D67
N
S68
G
T6
9D
Ins
69
K70
R
L7
4V
V75
I
F7
7L
Y11
5F
F1
16Y
V11
8I
Q15
1M
M1
84
V
L2
10W
T2
15Y
/F
K21
9Q
/E
G33
3E
L1
00I
K10
1E
K10
3N
V10
6M
/A
V10
8I
Y18
1C
/I
Y18
8C
/L
G19
0S
/A
P22
5H
M2
30
L
B
non-B
*
*
*
*
NRTIs NNRTIs
Prevalence of resistance-associated mutations in the reverse transcriptase gene
Couto-Fernandez et al., 2005
*
*
**

0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
80,0%
90,0%
100,0%
L1
0I/V
K2
0M
/R
L2
4I
D3
0N
V3
2I
L3
3F
M3
6I
M4
6I/L
I47
V
G4
8V
I50
V/L
F5
3L
I54
L/V
L6
3P
A7
1V
/T
G7
3S
V7
7I
V8
2A
/F
I84
V
N8
8S
L9
0M
B
non-B
Fisher’s exact test: *p< 0.05
*
Prevalence of resistance-associated mutations in the protease gene
Couto-Fernandez et al., 2005
*
** *

INRT
0
10
20
30
40
50
60
70
80
% d
e M
uta
ções
Mar-02
2003
2004
2005
Prevalência de mutações de resistência aos inibidores nucleosídicos da transcriptase reversa (INTR)
Couto-Fernandez et al., 2006

INNRT
0
5
10
15
20
25
30
35
40
45
% d
e M
uta
ções
Mar-02
2003
2004
2005
Prevalência de mutações de resistência aos inibidores não-nucleosídicos da transcriptase reversa (INTR)
Couto-Fernandez et al., 2006

IP
0
10
20
30
40
50
60
70
80
% d
e M
uta
ções
Mar-02
2003
2004
2005
Prevalência de mutações de resistência aos inibidores da protease (IP)
Couto-Fernandez et al., 2006

Couto-Fernandez et al., 2005
Geographical distribution of the HIV-1 genetic subtypes in Rio de Janeiro State, Brazil.

Geographical distribution of the human immunodeficiency virus type 1 genetic subtypes in the state of Rio de Janeiro, Brazil
Couto-Fernandez et al., 2006

ABSTRACTHIV-1 Subtype D occurs mainly in East and Central African countries, especially Uganda, where the prevalenceof HIV-1 infection is among the highest in the world. We present the phylogenetic analysis of one nonautochthonous and four autochthonous (including a near full-length genome) Brazilian HIV-1 subtype D strains identified in Rio de Janeiro State, where subtypes B, F1, and BF1 recombinants predominate. Phylogenetic inferences using maximum likelihood were applied on a near-full length genome and on concatenated gag, protease, reverse transcriptase, integrase, C2V3/env, gp41, and nef segments. Sequences from an Angolan immigrant showed close genetic similarity with a strain described in Finland, from an HIV patient of African origin, whereas all four autochthonous Brazilian sequences clustered with South African strains, where subtype D occurs only in isolated cases. Our results suggest the successful introduction and circulation in Brazil of closely related HIV-1 subtype D strains, possibly of South African origin.

FIG. 1. Maximum likelihood phylogenetic analysis places the near-full length 96BRRJ100 genome within the subtype D branch. Alignments were prepared with reference group M sequences gathered from the Los Alamos HIV database.
Resultados 1

Resultados 2

Short Communication
Accepted to AIDS Research and Human Retroviruses 2006
Molecular Epidemiology of HIV Type 1 in Inner Rio de Janeiro State, BrazilWalter A. Eyer-Silva, José Carlos Couto-Fernandez and Mariza G. Morgado
ABSTRACTIn the State of Rio de Janeiro, Brazil, HIV-1 diversity surveys have been performed mainly in the capital, and little is known about its
molecular epidemiology in inner cities of the State. We studied a total of 87 polymerase sequences recovered from 2 different cohorts in 30 inner cities throughout the Rio de Janeiro State. Subtypes B (83.9%), F1 (8%), D (2.3%), and unique BF1 recombinants (5.7%) were
demonstrated. The cross-sectional study found evidence that 41.6% of the patients harbored genetically related clusters of strains and probably took part in the same chain of viral spread. These clusters were phylogenetically unrelated to previously reported clusters from a
neighboring city, suggesting that each small city harbors its own set of micro-epidemic lineages.
0.10.10.1
C
A1
G
H
03BRRJ237
Position1.3001.2001.1001.0009008007006005004003002001000
% o
f P
erm
ute
d T
rees
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
BF recombinant
F1
F2DBF recombinant
05BRRJ164
Position1.3001.2001.1001.0009008007006005004003002001000
% o
f P
erm
ute
d T
ree
s
100
90
80
70
60
50
40
30
20
10
0
04BRSAP0104BRSAP0204BRSAP0404BRSAP1804BRSAP2405BRSAP25
Subtype Bcluster
98
Subtype Bcluster05BRSAP2605BRSAP2806BRSAP3106BRSAP33
100
100
Subtype Bcouple05BRSAP2706BRSAP29
B
100
BF recombinants05BRSAP2305BRSAP09
05BRSAP09_PED
Position900850800750700650600550500450400350300250200150100500
% o
f Per
mut
ed T
rees
100
90
80
70
60
50
40
30
20
10
0
99
100
100
100
100100
100
92
Subtype D05BRRJ09504BRSAP19
03BRRJ12405BRRJ263
04BRSAP0704BRSAP1303BRRJ12403BRRJ17804BRRJ14705BRRJ15105BRRJ263
Subtype F1
0.1
M45M48
M54
M63M58
M23M69
M53M28
M4104BRSAP18
04BRSAP0404BRSAP24
05BRSAP2504BRSAP01
04BRSAP02 04BRSAP05
M38M16
M66
M52M64M20
M65M50
M40
05BRSAP26 06BRSAP33
05BRSAP28 06BRSAP31
04BRSAP08 04BRSAP03
05BRSAP10 M44
M42
M78M77
M6705BRSAP27
06BRSAP29 M76
06BRSAP30 M12
M4904BRSAP06
M75M39
CETH2220C92BR025
0.1
M45M48
M54
M63M58
M23M69
M53M28
M4104BRSAP18
04BRSAP0404BRSAP24
05BRSAP2504BRSAP01
04BRSAP02 04BRSAP05
M38M16
M66
M52M64M20
M65M50
M40
05BRSAP26 06BRSAP33
05BRSAP28 06BRSAP31
04BRSAP08 04BRSAP03
05BRSAP10 M44
M42
0.1
M45M48
M54
M63M58
M23M69
M53M28
M4104BRSAP18
04BRSAP0404BRSAP24
05BRSAP2504BRSAP01
04BRSAP02 04BRSAP05
M38M16
M66
M52M64M20
M65M50
M40
05BRSAP26 06BRSAP33
05BRSAP28 06BRSAP31
04BRSAP08 04BRSAP03
05BRSAP10 M44
M42
M78M77
M6705BRSAP27
06BRSAP29 M76
06BRSAP30 M12
M4904BRSAP06
M75M39
CETH2220C92BR025
M56
M03
9999
M06 M46
Cluster M-D
10094
M07
M62
Cluster SAP-A
Cluster M-C100M22
M14M57
82
8390 M51
M34M33
M37
Cluster M-A85
Cluster SAP-B100
M43
100
97
97100 Cluster M-EM05
95
100
M17 M11M61
M21M55M25 M24
M47
M68M70
Cluster M-B
100

Prevalence of mutations known to confer reduced susceptibility to antiretroviral agents among 50 treatment-naïve and 45 antiretroviral-experienced HIV-1-infected patients receiving
care in small cities of inner Rio de Janeiro State, Brazil, 2004-2006.
No. Presence of mutations known to confer reduced susceptibility Total
RT only PR only RT + PR
Treatment-experienced patients (n=45)
Patients on HAART as of sampling 38 8 (21%) 1 (2.6%) 2 (5.2%) 11 (28.9%)
Patients off-treatment as of sampling 7 1 (14%) - - 1 (14%)
Treatment-naïve subjects 50 7 (14%) - - 7 (14%)
Total 95

ABSTRACTThe reconstruction of the epidemic history of several HIV populations, by using methodsthat infer the population history from sampled gene sequence data, has revealed importantsubtype-specific and regional-specific differences in patterns of epidemic growth. Here, weemploy Bayesian coalescent-based methods to compare the population history of the HIV-1subtype B and F1 epidemics in Brazil from non-contemporary env and pol gene sequences.Our results suggest that after the introduction of the subtypes B and F1 into Brazilian population, around mid to late 1960s and late 1970s, respectively; these subtypes experienced an initial period of exponential growth with similar epidemic growth rates (~0.5-0.6 year-1). Later, the spreading rate of both subtypes seems to have slowed-down since mid to late 1980s. This demographic pattern is very similar to that reported for the subtype B epidemics in high income countries where HIV was initially transmitted through homosexual intercourse and injecting drug use, as in Brazil; suggesting that the characteristics of transmission networks may be a key determinant of the HIV epidemic growth pattern. It is important to note that most of the subtype B and F1 sequences used in this study come from the Southeast region that has been the most affected by the AIDS epidemic in Brazil, being responsible for around 63 % of all AIDS cases reported since the early eighties; but may not represent the demographic trend of the HIV-1 epidemic in otherBrazilian regions.
Infection, Genetics and Evolution, in press 2006

RESULTS

Fig 1. Bayesian phylogenetic trees of Brazilian C2-C3 env sequences. (a) Subtype F1sequences. Indexes: Brazilian sequences (.), sequences of African origin (.), and Romanian sequences (.). Subtype F2 reference sequences were used to
root the tree, and the Most Recent Common Ancestor (MRCA) node of the Brazilian subtype F1 cluster is highlighted. (b) Brazilian subtype B sequences. Indexes: Brazilian “GPG” sequences (.),Brazilian “GWG”, “GCG”, “GLG”, “GRG”, and
“GGG” sequences (.), non-Brazilian subtype B sequencesscale is in calendar years.

Fig 2. Bayesian skyline plots representing nonparametric estimates of effective number of infections through time for
HIV-1 subtypes B (a) and F1 (b) epidemics in Brazil,

INRT
0
20
40
60
80
M41
LE44
D
A62V
K65R
D67N
S68G
T69D
Ins
69K70
RL7
4V V75I
F77L
Y115F
F116Y
V118I
Q15
1M
M18
4V
L210
W
T215Y
F
K219Q
E
G33
3E
Per
cen
tual
F (n=55)
B (n=165)
INNRT
0
10
20
30
40
50
A98G
L100
I
K101E
K103N
V106A
MV10
8I
Y181C
I
Y188L
G190A
P225H
M23
0L
P236L
Per
cen
tual
F (n=55)
B (n=165)
Prevalência de mutações de resistência aos inibidores da transcriptase reversa

IP
020
4060
80100
120
D30N
L33I
F
M46
IL
G48
VI5
0VL
V82AF
I84V
L90M
L10I
RV
K20M
RL2
4IV32
I
M36
IL
I47V
AF53
L
I54L
VML6
3P
A71VT
G73
SV77
I
N88DS
Per
cen
tual
F (n=55)
B (n=165)
Prevalência de mutações de resistência aos inibidores da protease

According to our findings, subtype F1 appears to have been introduced into Brazil
between 10 and 15 years later (late 1970s) than the subtype B (mid to late 1960s),
consistent with our previous report (Bello et al, 2006).
This clearly suggests that subtype B HIV-1 epidemics in US, Western Europe, and Brazil
started around the same time, which is fully consistent with the concurrent detection of the
first Aids cases in those regions during early 1980s.
These analyses also suggest that the Br-B variant emerged since the beginning of
subtype B epidemic in Brazil, which explains the high prevalence of this variant in the
country.
The high growth rates described for the Brazilian subtypes B and F1 epidemics in the
present work are consistent with such hypothesis, since in Brazil a significant proportion of
the HIV-1 infections (~60%) can be attributed to homo/bisexuals and injecting drug users
networks, in particular during the first years of the epidemic (1980-1993) (Brazilian Ministry
of Health., December 2005).
No significant correlation was observed in the drug resistance evolution between
subtype B and F strains.
CONCLUSIONS

Submited to AIDS Research and Human Retroviruses 2006
SEARCHING FOR A CRF_B/F IN HIV-1 RECOMBINANT B/F VIRUSES FROM RIO DE JANEIRO, BRAZIL
M Guimarães, Couto-Fernandez JC, Walter Eyer-Silva,C Siva-de-Jesus, S Teixeira, S Chequer-Fernandez, ,M Morgado
Lab. de AIDS & Imunol. Mol., Dep. de Imunologia, IOC; Rio de Janeiro, RJ, 21045-900, Fundação Oswaldo Cruz
Background: Brazil has been referred to be the one of “geographic recombination hotspots”, with a high frequency of mosaic viruses and up to now, at least three CRFs(12,28,29) and several URFs evolving subtypes B and F have been described. The present study is to search for common genetic recombinant profile among BF HIV-1 samples from Rio de Janeiro and compare them with those CRF B/F.
Results: From these 1500 samples already analyzed just 47 could be characterized as BF in the pol gene, most of them presenting different patterns of recombination, but we were also able to identify 4 distinct well defined phylogenetic clusters, composed at least by 3 samples that share the same pattern of recombination.
Conclusions: None of the four distinct B/F recombinant genetic profiles analyzed, gathered with high bootstrap value with CRF12,28 or 29, although some of them present some equal breakpoint.

0.1
100
91
100
BF1 recombinants (this study)Other Brazilian BF1 strainsSubsubtype F1Subtype BCRF_12
83
Subsubtype F1
CRF_12 81
88
100
Subtype B
Position (bp)1.3001.2001.1001.0009008007006005004003002001000
% o
f P
erm
ute
d T
rees
110
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
-10
REN213.03
REN049.04 & REN269.04
REN025.04
Position (bp)1.3001.2001.1001.0009008007006005004003002001000
% o
f P
erm
ute
d T
rees
110
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
-10
REN232.03
REN090.02 & 99UFRJ2BF
Position (bp)1.1001.000900800700600500400300200
% o
f P
erm
ute
d T
rees
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
REN123.02 & REN210.04
Position (bp)1.1001.000900800700600500400300200
% o
f P
erm
ute
d T
ree
s
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5Position (bp)
1.2001.1001.000900800700600500400300200100
% o
f P
erm
ute
d T
rees
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
REN034.02 & BREPM108
Position (bp)1.2001.1001.000900800700600500400300200100
% o
f P
erm
ute
d T
ree
s
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
REN046.02 & REN287.04
Position (bp)1.1001.000900800700600500400300
% o
f P
erm
ute
d T
ree
s
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
Position (bp)1.1001.000900800700600500400300200
% o
f P
erm
ute
d T
rees
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
REN178.04
REN137.04
Position (bp)1.2001.1001.000900800700600500400300200100
% o
f P
erm
ute
d T
rees
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
Position (bp)1.1001.000900800700600500400300200
% o
f P
erm
ute
d T
ree
s
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
REN010.02Position (bp)
1.1001.000900800700600500400300200
% o
f P
erm
ute
d T
ree
s
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
Position (bp)1.1001.000900800700600500400300200
% o
f P
erm
ute
d T
rees
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
-5
59
REN207.03 & REN214.03
F1BRBZ126C92BR025BBZ167
Position (bp)1.1001.000900800700600500400300200100
% o
f P
erm
ute
d T
rees
105
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
REN217.03
77
Phylogenetic analyzes of BF recombinant forms

CRF_12
CRF_28 CRF_29
SUBTYPE B
GROUP 3
GROUP4
GROUP 5
GROUP6
GROUP 7
GROUP1
B F
GROUP 2
Sub-Subtype F1
B F
B F B
F B
B F B
B F
B F
Samples were analyzed using the SplitsTree Decomposition methodology. Subtype B and F as well as CRF 12, 28 and 29 references were used in this evaluation. Bootscanning representation of samples characterized as recombinant in the different regions were represented here. Analysis of pol- PR/RT (1280bp)
Phylogenetic analyzes of BF recombinant forms

CONCLUSÕES FINAIS 1
Uma grande proporção do subtipo B do HIV-1 foi observada em pacientes do Estado Rio de Janeiro, apresentando falha a terapia anti-antiretroviral.
A baixa prevalência do subtipo F neste grupo, quando comparada a estudos prévios baseados no envelope viral, pode ser devido a elevada frequência de vírus recombinantes entre amostras do subtipo F. Observamos a circulação dos subtipos C e D do HIV-1, URFs CF e AF, além da primeira descrição no Brasil da presença das CRF02_AG e CFR01_AE no Estado do Rio de Janeiro.
A distribuição das diferentes mutações de resistência no grupo de estudo mostrou correlação com a TAR utilizada.

A manutenção e implementação dos Programas de Genotipagem da Resistência do HIV-1 no Brasil, são de fundamental importância para a condução e reestruturação da TARV em pacientes apresentando falha virológica.
A análise das sequências genômicas geradas pelo teste de genotipagem, pode servir para estudos de epidemiologia molecular de mapeamento da circulação de subtipos de HIV, bem como, para análises filogenéticas e evolutivas entre as diferentes amostras virais.
CONCLUSÕES 2

COLABORADORESMariangela B. Galvão Simão, Lilian I. Amaral, Orival S. Silveira, Denise FC. Souza e P. Chequer- PN DST&AIDS – Ministério da Saúde (www.aids.gov.br/renageno).
Marcia Rachid - Programa Estadual de DST e AIDS - SESRJ
Programas Municipais de DST e AIDS - SMSRJ
Grupo de Médicos de Referência em Genotipagem (MRGs) do Estado do Rio de Janeiro
Francisco I. Bastos - Centro de Informacao Cientifica – CICT/Fiocruz
Waldilea Veloso - Centro de Pesquisa Clinica Evandro Chagas – IPEC/Fiocruz
Martine Peeters, Eric Delaporte - Lab. Retrovirus – IRD, Montpellier, FR
SUPORTE
PN DST e AIDS-MS