
publicação oficial do conselho brasileiro de oftalmologia ... › Reader › uploads ›...
84
A RQUIVOS B RASILEIROS DE 77 01 PUBLICAÇÃO OFICIAL DO CONSELHO BRASILEIRO DE OFTALMOLOGIA JANEIRO/FEVEREIRO 2014 ISSN 0004-2749 versão impressa Head posture and visual acuity in nystagmus Cataract surgery rates in Argentina Subconjunctival bevacizumab for pterygium UBM in cyclopexy surgery for cyclodialysis Finite element modelling of the cornea INDEXADA NAS BASES DE DADOS MEDLINE | EMBASE | ISI | SciELO
Transcript of publicação oficial do conselho brasileiro de oftalmologia ... › Reader › uploads ›...
A r q u i v o s b r a s i l e i r o s d e
77 01publicação oficial do conselho brasileiro de oftalmologia
Janeiro/feVereiro 2014
issn 0004-2749versão impressa
Head posture and visual acuity in nystagmus
Cataract surgery rates in Argentina
Subconjunctival bevacizumab for pterygium
UbM in cyclopexy surgery for cyclodialysis
Finite element modelling of the cornea
indexada nas bases de dados
medline | embase | isi | scielO
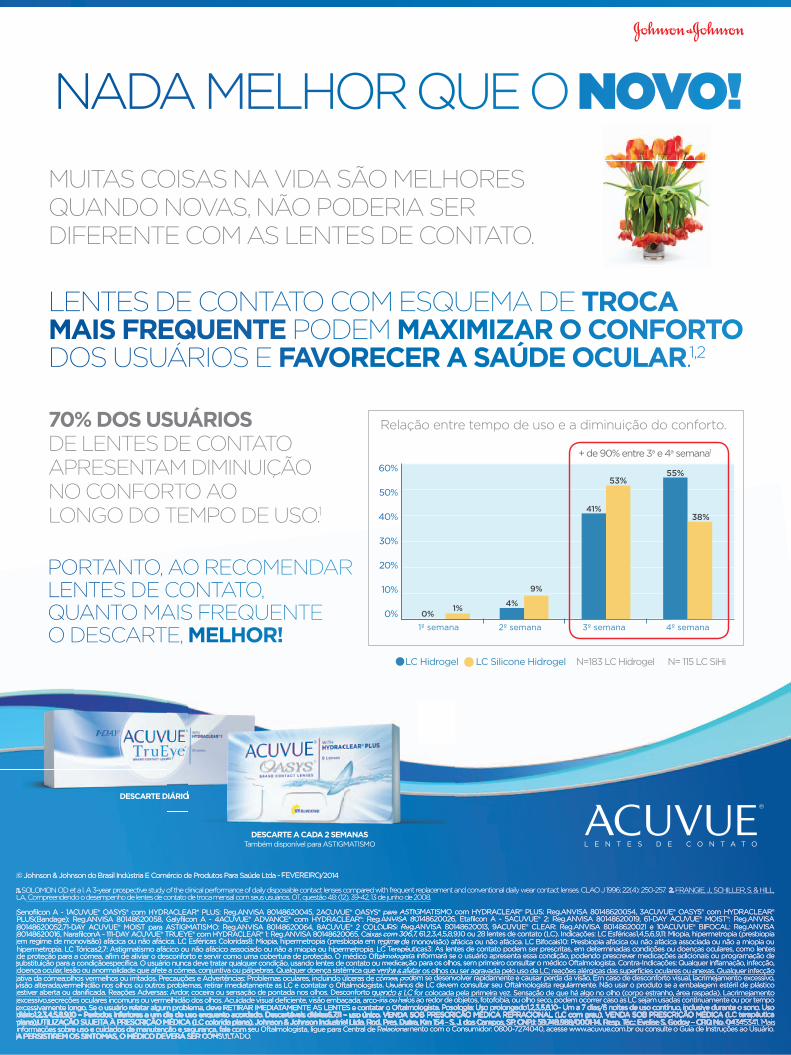
NADA MELHOR QUE O NOVO!
70% DOS USUÁRIOS DE LENTES DE CONTATO APRESENTAM DIMINUIÇÃO NO CONFORTO AO LONGO DO TEMPO DE USO.1
DESCARTE DIÁRIO
DESCARTE A CADA 2 SEMANASTambém disponível para ASTIGMATISMO
DESCARTE DIÁRIO
MUITAS COISAS NA VIDA SÃO MELHORES QUANDO NOVAS, NÃO PODERIA SER DIFERENTE COM AS LENTES DE CONTATO.
PORTANTO, AO RECOMENDAR LENTES DE CONTATO, QUANTO MAIS FREQUENTE O DESCARTE, MELHOR! 1º semana 2º semana 3º semana 4º semana
60%
50%
40%
30%
20%
10%
0% 0%1%
9%
4%
53%
41%
55%
38%
+ de 90% entre 3a e 4a semana1
N=183 LC Hidrogel N= 115 LC SiHiLC Hidrogel LC Silicone Hidrogel
LENTES DE CONTATO COM ESQUEMA DE TROCA MAIS FREQUENTE PODEM MAXIMIZAR O CONFORTO DOS USUÁRIOS E FAVORECER A SAÚDE OCULAR.1,2
© Johnson & Johnson do Brasil Indústria E Comércio de Produtos Para Saúde Ltda - FEVEREIRO/2014FEVEREIRO/2014FEVEREIRO
1.SOLOMON OD et a l. A 3-year prospective study of the clinical performance of daily disposable contact lenses compared with frequent replacement and conventional daily wear contact lenses. CLAO J 1996; 22(4): 250-257. 2. FRANGIE, J., SCHILLER, S. & HILL, LA. Compreendendo o desempenho de lentes de contato de troca mensal com seus usuários. OT, questão 48: (12), 39-42, 13 de junho de 2008. LA. Compreendendo o desempenho de lentes de contato de troca mensal com seus usuários. OT, questão 48: (12), 39-42, 13 de junho de 2008. LA.
Senofilcon A - 1ACUVUE® OASYS® com HYDRACLEAR® PLUS: Reg.ANVISA 80148620045, 2ACUVUE® OASYS® para ASTIGMATISMO com HYDRACLEAR® PLUS: Reg.ANVISA 80148620054, 3ACUVUE® OASYS® com HYDRACLEAR® PLUS(Bandage): Reg.ANVISA 80148620058, Galyfilcon A - 4ACUVUE® ADVANCE® com HYDRACLEAR®: Reg.ANVISA 80148620026, Etafilcon A - 5ACUVUE® 2: Reg.ANVISA 80148620019, 61-DAY ACUVUE® MOIST®: Reg.ANVISA 80148620052,71-DAY ACUVUE® MOIST para ASTIGMATISMO: Reg.ANVISA 80148620064, 8ACUVUE® 2 COLOURS: Reg.ANVISA 80148620013, 9ACUVUE® CLEAR: Reg.ANVISA 80148620021 e 10ACUVUE® BIFOCAL: Reg.ANVISA 80148620016, NarafilconA - 111-DAY ACUVUE® TRUEYE® com HYDRACLEAR® 1: Reg.ANVISA 80148620065. Caixas com 306,7, 61,2,3,4,5,8,9,10 ou 28 lentes de contato (LC). Indicações: LC Esféricas1,4,5,6,9,11: Miopia, hipermetropia (presbiopia em regime de monovisão) afácica ou não afácica. LC Esféricas Coloridas8: Miopia, hipermetropia (presbiopia em regime de monovisão) afácica ou não afácica. LC Bifocais10: Presbiopia afácica ou não afácica associada ou não a miopia ou hipermetropia. LC Tóricas2,7: Astigmatismo afácico ou não afácico associado ou não a miopia ou hipermetropia. LC Terapêuticas3: As lentes de contato podem ser prescritas, em determinadas condições ou doenças oculares, como lentes de proteção para a córnea, afim de aliviar o desconforto e servir como uma cobertura de proteção. O médico Oftalmologista informará se o usuário apresenta essa condição, podendo prescrever medicações adicionais ou programação de substituição para a condiçãoespecífica. O usuário nunca deve tratar qualquer condição, usando lentes de contato ou medicação para os olhos, sem primeiro consultar o médico Oftalmologista. Contra-Indicações: Qualquer inflamação, infecção, doença ocular, lesão ou anormalidade que afete a córnea, conjuntiva ou pálpebras. Qualquer doença sistêmica que venha a afetar os olhos ou ser agravada pelo uso de LC; reações alérgicas das superfícies oculares ou anexas. Qualquer infecção ativa da córnea;olhos vermelhos ou irritados. Precauções e Advertências: Problemas oculares, incluindo úlceras de córnea, podem se desenvolver rapidamente e causar perda da visão. Em caso de desconforto visual, lacrimejamento excessivo, visão alterada,vermelhidão nos olhos ou outros problemas, retirar imediatamente as LC e contatar o Oftalmologista. Usuários de LC devem consultar seu Oftalmologista regularmente. Não usar o produto se a embalagem estéril de plástico estiver aberta ou danificada. Reações Adversas: Ardor, coceira ou sensação de pontada nos olhos. Desconforto quando a LC for colocada pela primeira vez. Sensação de que há algo no olho (corpo estranho, área raspada). Lacrimejamento excessivo,secreções oculares incomuns ou vermelhidão dos olhos. Acuidade visual deficiente, visão embaçada, arco-íris ou halos ao redor de objetos, fotofobia, ou olho seco, podem ocorrer caso as LC sejam usadas continuamente ou por tempo excessivamente longo. Se o usuário relatar algum problema, deve RETIRAR IMEDIATAMENTE AS LENTES e contatar o Oftalmologista. Posologia: Uso prolongado1,2,3,5,8,10– Um a 7 dias/6 noites de uso contínuo, inclusive durante o sono. Uso diário1,2,3,4,5,8,9,10 – Períodos inferiores a um dia de uso enquanto acordado. Descartáveis diárias6,7,11 – uso único. VENDA SOB PRESCRIÇÃO MÉDICA REFRACIONAL (LC com grau), VENDA SOB PRESCRIÇÃO MÉDICA (LC terapêutica excessivamente longo. Se o usuário relatar algum problema, deve RETIRAR IMEDIATAMENTE AS LENTES e contatar o Oftalmologista. Posologia: Uso prolongado1,2,3,5,8,10– Um a 7 dias/6 noites de uso contínuo, inclusive durante o sono. Uso diário1,2,3,4,5,8,9,10 – Períodos inferiores a um dia de uso enquanto acordado. Descartáveis diárias6,7,11 – uso único. VENDA SOB PRESCRIÇÃO MÉDICA REFRACIONAL (LC com grau), VENDA SOB PRESCRIÇÃO MÉDICA (LC terapêutica excessivamente longo. Se o usuário relatar algum problema, deve RETIRAR IMEDIATAMENTE AS LENTES e contatar o Oftalmologista. Posologia: Uso prolongado1,2,3,5,8,10– Um a 7 dias/6 noites de uso contínuo, inclusive durante o sono. Uso
plana),UTILIZAÇÃO SUJEITA À PRESCRIÇÃO MÉDICA (LC colorida plana). Johnson & Johnson Industrial Ltda. Rod. Pres. Dutra, Km 154 - S. J. dos Campos, SP. CNPJ: 59.748.988/0001-14. Resp. Téc.: Evelise S. Godoy – CRQ No. 04345341. Mais diário1,2,3,4,5,8,9,10 – Períodos inferiores a um dia de uso enquanto acordado. Descartáveis diárias6,7,11 – uso único. VENDA SOB PRESCRIÇÃO MÉDICA REFRACIONAL (LC com grau), VENDA SOB PRESCRIÇÃO MÉDICA (LC terapêutica plana),UTILIZAÇÃO SUJEITA À PRESCRIÇÃO MÉDICA (LC colorida plana). Johnson & Johnson Industrial Ltda. Rod. Pres. Dutra, Km 154 - S. J. dos Campos, SP. CNPJ: 59.748.988/0001-14. Resp. Téc.: Evelise S. Godoy – CRQ No. 04345341. Mais diário1,2,3,4,5,8,9,10 – Períodos inferiores a um dia de uso enquanto acordado. Descartáveis diárias6,7,11 – uso único. VENDA SOB PRESCRIÇÃO MÉDICA REFRACIONAL (LC com grau), VENDA SOB PRESCRIÇÃO MÉDICA (LC terapêutica
informações sobre uso e cuidados de manutenção e segurança, fale com seu Oftalmologista, ligue para Central de Relacionamento com o Consumidor: 0800-7274040, acesse www.acuvue.com.br ou consulte o Guia de Instruções ao Usuário. A PERSISTIREM OS SINTOMAS, O MÉDICO DEVERÁ SER CONSULTADO.informações sobre uso e cuidados de manutenção e segurança, fale com seu Oftalmologista, ligue para Central de Relacionamento com o Consumidor: 0800-7274040, acesse www.acuvue.com.br ou consulte o Guia de Instruções ao Usuário. A PERSISTIREM OS SINTOMAS, O MÉDICO DEVERÁ SER CONSULTADO.informações sobre uso e cuidados de manutenção e segurança, fale com seu Oftalmologista, ligue para Central de Relacionamento com o Consumidor: 0800-7274040, acesse www.acuvue.com.br ou consulte o Guia de Instruções ao Usuário.
Relação entre tempo de uso e a diminuição do conforto.

AF_Anuncio_Centurion_21x28_pt.indd 1 3/27/14 10:24 AM
Frequency of publication: Bimonthly Arq Bras Oftalmol. São Paulo, v. 77, issue 1, pages 1-70, Jan./Feb. 2014
Continuous publication since 1938
Publisher: Ipsis Gráfica e Editora S.A. Divulgation: Brazilian Council of OphthalmologyCirculation: 8.600 copies
CODEN - AQBOAP
PUBLICAÇÃO OFICIAL DOCONSELHO BRASILEIRO
DE OFTALMOLOGIA
OffiCiAl PuBliCAtiON Of thE BrAziliAN COuNCil Of OPhthAlmOlOgy (CBO)
Editorial BoardNationalAna Luísa Höfling-Lima (São Paulo-SP)André Augusto Homsi Jorge (Ribeirão Preto-SP)André Messias (Ribeirão Preto-SP)Andrea Zin (Rio de Janeiro-RJ)Antonio Augusto Velasco e Cruz (Ribeirão Preto-SP)Ayrton Roberto B. Ramos (Florianópolis-SC)Cristina Muccioli (São Paulo-SP)Denise de Freitas (São Paulo-SP)Eduardo Cunha de Souza (São Paulo-SP)Eduardo Ferrari Marback (Salvador-BA)Érika Hoyama (Londrina-PR)Fábio Ejzenbaum (São Paulo-SP)Flávio Jaime da Rocha (Uberlândia-MG)João Antonio Prata Jr. (Uberaba-MG)João Borges Fortes Filho (Porto Alegre-RS)João J. Nassaralla Jr. (Goiânia-GO)João Luiz Lobo Ferreira (Florianópolis-SC)José Beniz Neto (Goiânia-GO)José Paulo Cabral Vasconcellos (Campinas-SP)Keila Monteiro de Carvalho (Campinas-SP)Lisandro Sakata (Curitiba-PR)Luiz V. Rizzo (São Paulo-SP)Marcelo Francisco Gaal Vadas (São Paulo-SP)Marcelo Hatanaka (São Paulo-SP)
Marcelo Vieira Netto (São Paulo-SP)Marcony Santhiago (Rio de Janeiro-RJ)Maria Cristina Nishiwaki Dantas (São Paulo-SP)Maria de Lourdes V. Rodrigues (Ribeirão Preto-SP)Martha Maria Motono Chojniak (São Paulo-SP)Maurício Maia (Assis-SP)Mauro Campos (São Paulo-SP)Mauro Goldchmit (São Paulo-SP)Midori Hentona Osaki (São Paulo-SP)Milton Ruiz Alves (São Paulo-SP)Mônica Alves (Campinas-SP)Mônica Fialho Cronemberger (São Paulo-SP)Newton Kara-José Júnior (São Paulo-SP)Norma Helen Medina (São Paulo-SP)Paulo E. Correa Dantas (São Paulo-SP)Procópio Miguel dos Santos (Brasília-RJ)Ramon Ghanem (Joinvile-SC)Remo Susanna Jr. (São Paulo-SP)Roberto L. Marback (Salvador-BA)Roberto Pinto Coelho (Ribeirão Preto-SP)Rosane da Cruz Ferreira (Porto Alegre-RS)Rubens Belfort Jr. (São Paulo-SP)Sebastião Cronemberger (Belo Horizonte-MG)Sérgio Kwitko (Porto Alegre-RS)Sidney Júlio de Faria e Souza (Ribeirão Preto-SP)Silvana Artioli Schellini (Botucatu-SP)
Tiago Prata (São Paulo-SP)Vital Paulino Costa (São Paulo-SP)Walter Yukihiko Takahashi (São Paulo-SP)
InternationalAlan B. Scott (E.U.A.)Andrew Lee (E.U.A.)Baruch D. Kuppermann (E.U.A.)Bradley Straatsma (E.U.A.)Careen Lowder (E.U.A.)Cristian Luco (Chile)Emílio Dodds (Argentina)Fernando M. M. Falcão-Reis (Portugal)Fernando Prieto Díaz (Argentina)James Augsburger (E.U.A.)José Carlos Cunha Vaz (Portugal)José C. Pastor Jimeno (Espanha)Marcelo Teixeira Nicolela (Canadá)Maria Amélia Ferreira (Portugal)Maria Estela Arroyo-Illanes (México)Miguel N. Burnier Jr. (Canadá)Pilar Gomez de Liaño (Espanha)Richard L. Abbott (E.U.A.)Zélia Maria da Silva Corrêa (E.U.A.)
iSSN 0004-2749(Printed version)
iSSN 1678-2925(Electronic version)
SubScriptionS - braSil: CBO Members: Free Distribuiton
Non-members: Annual Subscription: R$ 630.00 Single issue: R$ 95.00
Foreign: Annual Subscription: US$ 200.00 Single issue: US$ 40.00
Chief-editor: Wallace Chamon
Commercial Manager: Mauro Nishi
Executive Secretary: Claudete N. Moral Claudia Moral
Final Review: Paulo Mitsuru Imamura
Technical Editorship: Edna Terezinha Rother Maria Elisa Rangel Braga
Cover: Ipsis
Administrative BoardHarley E. A. Bicas Milton Ruiz Alves Roberto Lorens Marback Rubens Belfort Jr. Wallace Chamon
Chief-EditorWallace Chamon
Former EditorsWaldemar Belfort MattosRubens Belfort MattosRubens Belfort Jr.Harley E. A. Bicas
Associate EditorsAugusto Paranhos Jr. José Álvaro Pereira GomesBruno Machado Fontes Karolinne Maia RochaEduardo Melani Rocha Luiz Alberto S. Melo Jr.Eduardo Sone Soriano Mário Luiz Ribeiro MonteiroGalton Carvalho Vasconcelos Michel Eid FarahHaroldo Vieira de Moraes Jr. Norma AllemannIvan Maynart Tavares Rodrigo Pessoa Cavalcanti LiraJayter Silva de Paula Suzana Matayoshi
Cover: Photograph taken at the slit lamp with gonioscopy lens, showing the anterior chamber angle of a patient with iris melanoma. Photographer: Laércio da Silva Gonçalves (Department of Ophthalmology-UNIFESP).
ABO – ARquivOS BRASilEiROS DE OFTAlMOlOgiA • Bimonthly PuBlication of the Brazilian council of oPhthalmology (cBo)Editorial Office: R. Casa do Ator, 1.117 - 2nd Floor - São Paulo - SP - Brazil - 04546-004
Phone: +55 (11) 3266-4000 - Fax: +55 (11) 3171-0953 - E-mail: [email protected] - www.scielo.br/abo
OffiCiAl PuBliCAtiON Of thE BrAziliAN COuNCil Of OPhthAlmOlOgy (CBO)PUBLICAÇÃO OFICIAL DOCONSELHO BRASILEIRO
DE OFTALMOLOGIAiSSN 0004-2749(Printed version)
iSSN 1678-2925(Electronic version)
Support:
www.freemedicaljournals.com
www.scielo.org
www.periodicos.capes.gov.br
• iSi Web of Knowledge (SM)
CBO Board of Directors - 2013-2015Milton Ruiz Alves (President)
Renato Ambrósio Jr. (Vice-President)
leonardo Mariano Reis (First Secretary)
Keila monteiro de carvalho (General Secretary)
Mauro Nishi (Treasurer)
Societies Affiliated to the Brazilian Council of Ophthalmology and Their Presidents
Centro Brasileiro de Estrabismo Marcelo Francisco Gaal Vadas
Sociedade Brasileira de Administração em Oftalmologia Flávio Rezende Dias
Sociedade Brasileira de Catarata e implantes intra-Oculares Armando Stefano Crema
Sociedade Brasileira de Cirurgia Plástica Ocular Guilherme Herzog
Sociedade Brasileira de Cirurgia Refrativa Renato Ambrósio Júnior
Sociedade Brasileira de Ecografia em Oftalmologia Norma Allemann
Sociedade Brasileira de glaucoma Francisco Eduardo Lopes de Lima
Sociedade Brasileira de laser e Cirurgia em Oftalmologia Caio Vinicius Saito Regatieri
Sociedade Brasileira de lentes de Contato, Córnea e Refratometria Newton Kara José
Sociedade Brasileira de Oftalmologia Pediátrica João Borges Fortes Filho
Sociedade Brasileira de Oncologia em Oftalmologia Virgínia Laura Lucas
Sociedade Brasileira de Retina e vítreo Walter Yukihiko Takahashi
Sociedade Brasileira de Trauma Ocular André Barbosa Castelo Branco
Sociedade Brasileira de uveítes Áisa Haidar Lani
Sociedade Brasileira de visão Subnormal Maria de Fátima Neri Góes
www.scirus.com
• aBo Arquivos Brasileiros de Oftalmologia www.abonet.com.br • copernicus
www.copernicusmarketing.com
• meDline
• lilacS literatura latino-americana
em Ciências da Saúde

Contents
OffiCiAl PuBliCAtiON Of thE BrAziliAN COuNCil Of OPhthAlmOlOgy (CBO) iSSN 0004-2749(Printed version)
iSSN 1678-2925(Electronic version)
Frequency of publication: Bimonthly Arq Bras Oftalmol. São Paulo, v. 77, issue 1, pages 1-70, Jan./Feb. 2014
PUBLICAÇÃO OFICIAL DOCONSELHO BRASILEIRO
DE OFTALMOLOGIA
EditorialV Restoration of accommodation: new perspectives Restauração da acomodação: novas perspectivas Tracy Schroeder Swartz, Karolinne Maia Rocha, Mitch Jackson, David HK Ma, Daniel Goldberg, AnnMarie Hipsley
Original Articles1 Anterior segment optical coherence tomography in acute anterior uveitis Tomografia de coerência óptica do segmento anterior em uveíte anterior aguda Cristiana Agra, Lydianne Agra, Jeanine Dantas, Tiago Eugênio Faria e Arantes, João Lins de Andrade Neto
4 Efficacy and safety of subconjunctival bevacizumab for recurrent pterygium Eficácia e segurança da aplicação subconjuntival de bevacizumabe em pterígio recidivado Larissa Rossana Souza Stival, Anelise Medeiros Lago, Marisa Novaes Falleiro Chaves de Figueiredo, Ricardo Henrique Goulart Bittar, Márcia Leite Machado,
João Jorge Nassaralla Junior
8 influence of head posture on the visual acuity of children with nystagmus Influência da postura da cabeça na acuidade visual de crianças com nistagmo Ana Carla Ramos Vieira da Costa, Márcia Caires Bestilleiro Lopes, Célia Regina Nakanami
12 life quality assessment of patients after phacoemulsification or extracapsular cataract extraction Avaliação da qualidade de vida de pacientes submetidos à facoemulsificação ou extração extracapsular de catarata Paula Teixeira de Mendonça, Leonardo Teixeira de Mendonça, Alexandre Antônio Marques Rosa, Luiz Carlos de Lima Silveira
17 Assessment of anterior and posterior corneal indices using two Scheimpflug analyzers Índices da córnea anterior e posterior com dois analisadores Scheimpflug Daoud Charbel Fahd, Carole George Cherfan, Claudia Raad, Marc Asouad, Shady Tanus Awwad
21 Translation and validation of Convergence insufficiency Symptom Survey (CiSS) to Portuguese - psychometric results Tradução e validação do CISS para a língua portuguesa - resultados psicométricos Catarina Tavares, Amélia Maria Monteiro Fernandes Nunes, António João Santos Nunes, Maria Vaz Pato, Pedro Miguel Lourenço Monteiro
25 Complexities and challenges of surgical data collection from cataract patients: comparison of cataract surgery rates between 2001 and 2008 in all provinces of Argentina
Complexidades e desafios da coleta de dados cirúrgicos de catarata: comparação das taxas de cirurgia de catarata em todas as províncias da Argentina de 2001 em relação a 2008
Van C. Lansingh, Maria E. Nano, Marissa J. Carter, Natalia Zárate, Serge Resnikoff, Kristen A. Eckert
30 Clinical and epidemiological characteristics of patients with uveitis in an emergency eye care center in Brazil Características clínicas e epidemiológicas das uveítes em um serviço de urgência oftalmológica no Brasil Eduardo Nery Rossi Camilo, Guilherme Lucena Moura, Tiago Eugênio Faria e Arantes

34 Comparative study of visual functions in premature pre-school children with and without retinopathy of prematurity Estudo comparativo das funções visuais em pré-escolares nascidos prematuros com e sem retinopatia da prematuridade Lígia Beatriz Bonotto, Ana Tereza Ramos Moreira, Silvia Chuffi, Susana Maria Bittencourt Sckudlarek
40 Treatment of astigmatism during phacoemulsification Tratamento do astigmatismo durante a facoemulsificação Giuliano Oliveira Freitas, Joel Edmur Boteon, Mario José Carvalho, Rogerio Melo Costa Pinto
Case Reports47 Ophthalmic evaluation, treatment, and follow-up of two cases of incontinentia pigmenti Avaliação oftalmológica, tratamento e seguimento de dois casos de incontinentia pigmenti Carlos Augusto Moreira Neto, Ana Tereza Ramos Moreira, Carlos Augusto Moreira Jr.
50 Direct cyclopexy surgery for post-traumatic cyclodialysis with persistent hypotony: ultrasound biomicroscopic evaluation Ciclopexia direta em ciclodiálise pós-traumática com hipotonia ocular persistente - acompanhamento por biomicroscopia ultrassônica (UBM) Fabiola Murta, Somaia Mitne, Norma Allemann, Augusto Paranhos Junior
54 Case report of a metachronous multiple tumor: Mantle cell lymphoma in the orbital region associated with epithelial malignancies at other sites
Tumor múltiplo metacrônico: linfoma do manto na região orbital associado a neoplasias malignas epiteliais em outros sítios - relato de caso Juliana S. F. Medrado, Mirtha Ramírez Dittrich, Jacqueline M. Sousa, Luiz F. Teixeira, Paulo Góis Manso
57 Amelanotic corneally displaced malignant conjunctival melanoma: a case report evaluated with impression cytology Melanoma amelanótico conjuntival maligno deslocado sobre a córnea com citologia de impressão: relato de caso Jeison de Nadai Barros, Márcia Motono, Felipe D’Almeida Costa, Marcelo Carvalho da Cunha, Martha Motono Chojniak
Review Articles60 Finite element modelling of cornea mechanics: a review Modelagem de elementos finitos da mecânica da córnea: uma revisão Talisa Mohammad Nejad, Craig Foster, Dipika Gongal
67 Instructions to Authors

V
Editorial
Restoration of accommodation: new perspectivesRestauração da acomodação: novas perspectivas
Tracy Schroeder SwarTz1, Karolinne Maia rocha2, MiTch JacKSon3, david hK Ma4, daniel GoldberG5, annMarie hipSley6
Presbyopia is the loss of accommodative ability that occurs with age. Current accommodative theory postu-lates that the lens is primarily responsible for the refractive change that allows us to read. Our understanding of this process has grown substantially with the advent of new technologies, including ultrasound biomicroscopy (UBM), endoscopy, optical coherence tomography (OCT), ray-tracing and wavefront analysis. Goldberg’s Postu-late incorporates all elements of the zonular apparatus into the phenomenon of accommodation(1). The ciliary body contracts during accommodation. Biometry has shown that the lens thickness increases and the anterior chamber depth decreases(2). It has also demonstrated the lens capsule steepens, as the posterior-lens surface moves backwards(2).
In addition, there is a decrease in the distance from scleral spur to the ora serrata. UBM identified an attach-ment zone of the posterior zonules adjacent to the ora, and contraction of these zonules is thought to be the etiology of the decrease in distance found with accommodation. This complex action of the zonules is suspec-ted to be reciprocal. As the same time the anterior zonules relax, reducing their tension on the lens such that the lens changes shape anteriorly, the posterior zonules contract, moving the posterior capsule backward. This vitreal-zonular complex stiffens with age, losing its elasticity(1-3). The age-related changes in these structures and their biomechanical interactions with the ciliary-lens complex may contribute to presbyopia(3). It has been newly discovered that there are also changes in extralenticular structures which may have an impact on the loss of accommodation which were previously deemed to be of very little importance, namely the sclera and choroid(2).
All ocular tissues are made of collagen and are impacted like all other connective tissues by age. Ocular rigi-dity has been correlated with age(4) and the sclera undergoes scleral sclerosis as well as metabolic physiological stress. With the loss of elasticity, the more rigid sclera elicits compression and loading stresses upon underlying structures, specifically those related to accommodative function. Increased ocular rigidity affects other tissues as well, including ocular blood flow through the sclera and optic nerve. It has been correlated to the pathogenesis of macular degeneration(5) and other age-related eye diseases(6). Ocular rigidity may not only impact the loss of visual accommodation but also have more extensive clinical significance.
The impact of age on the lenticular-based model of loss of accommodation is well documented. The amount of accommodation lost with age related to extralenticular apparatus (primarily the zonules, choroid, and sclera) was only recently investigated(7). It is also now known that the sclera becomes less deformable during accommodation in the nasal area with age(2). New models suggest up to 2 diopters that might be contributed by ex tralenticular structures(7).
To date, there has been at least up to 1-2 diopters of a loss of accommodation unaccounted for that might be contributed by extralenticular structures(7). The investigation improving ocular resilience for the restoration of accommodation is of clinical importance. The Laser anterior ciliary excision procedure is designed to do so by altering biomechanical scleral properties. This is achieved by creating micropores in a matrix over four oblique quadrants. The VisioLite erbium-YAG laser creates micro-excisions in critical zones of physiologic importance overlying the ciliary-lens complex. The matrix pattern of nine 600 µm laser spots in the sclera of each quadrant aims to increase plasticity in those regions across the anterior globe. The Laser anterior cilary excision primary mechanism of action is to decrease scleral resistive forces in order to restore accommodative ability in the aging eye by increasing resultant ciliary muscle constriction (Figure 1).
Laboratory studies of ocular rigidity demonstrated use of a reference model, and effect of laser anterior ciliary ablation on aging porcine eyes in vitro(8). Investigators concluded that the scleral crosslinking method might be useful for correlation of age-related rigidity, as well as the efficacy of the laser anterior ciliary ablation procedure to decrease ocular rigidity(8).
Submitted for publication: February 12, 2014 Accepted for publication: February 13, 20141 Madison, Alabama, USA.2 Cleveland Clinic Foundation, Cole Eye Institute, Ohio, USA.3 Jackson Eye, Chicago, Illinois, USA.4 Chang Gung Memorial Hospital, Taipei, Taiwan.5 Drexel College of Medicine, Philadelphia, PA.; Atlantic Eye Physicians, Little Silver NJ, USA.6 Ace Vision Group, Newark California, USA.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: T.S. Swartz, None; K.M. Rocha, None; M. Jackson, None; D.H.K. Ma, None; D. Goldberg, None; A. Hipsley, None.
Correspondence address: Karolinne Rocha. Cleveland Clinic Foundation. Cole Eye Institute, Ohio, USA - E-mail: [email protected]; [email protected]
Restoration of accommodation: new perspectives
VI
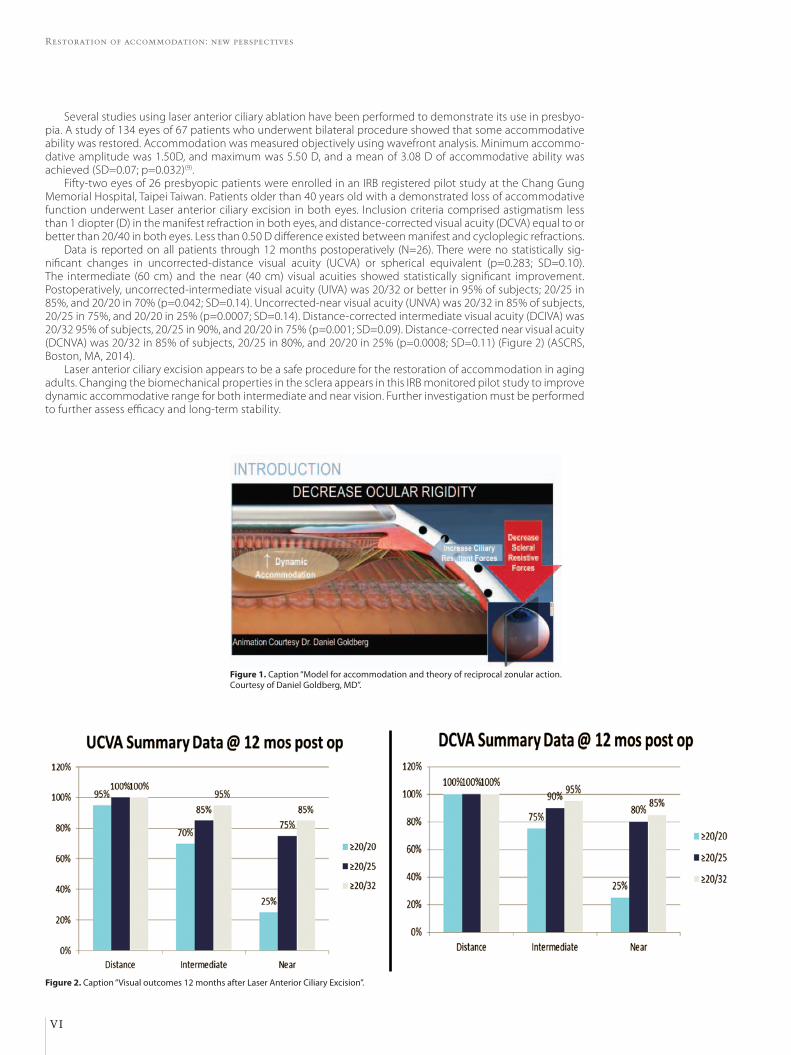
Several studies using laser anterior ciliary ablation have been performed to demonstrate its use in presbyo-pia. A study of 134 eyes of 67 patients who underwent bilateral procedure showed that some accommodative ability was restored. Accommodation was measured objectively using wavefront analysis. Minimum accommo-dative amplitude was 1.50D, and maximum was 5.50 D, and a mean of 3.08 D of accommodative ability was achieved (SD=0.07; p=0.032)(9).
Fifty-two eyes of 26 presbyopic patients were enrolled in an IRB registered pilot study at the Chang Gung Memorial Hospital, Taipei Taiwan. Patients older than 40 years old with a demonstrated loss of accommodative function underwent Laser anterior ciliary excision in both eyes. Inclusion criteria comprised astigmatism less than 1 diopter (D) in the manifest refraction in both eyes, and distance-corrected visual acuity (DCVA) equal to or better than 20/40 in both eyes. Less than 0.50 D difference existed between manifest and cycloplegic refractions.
Data is reported on all patients through 12 months postoperatively (N=26). There were no statistically sig -nificant changes in uncorrected-distance visual acuity (UCVA) or spherical equivalent (p=0.283; SD=0.10). The intermediate (60 cm) and the near (40 cm) visual acuities showed statistically significant improvement. Postoperatively, uncorrected-intermediate visual acuity (UIVA) was 20/32 or better in 95% of subjects; 20/25 in 85%, and 20/20 in 70% (p=0.042; SD=0.14). Uncorrected-near visual acuity (UNVA) was 20/32 in 85% of subjects, 20/25 in 75%, and 20/20 in 25% (p=0.0007; SD=0.14). Distance-corrected intermediate visual acuity (DCIVA) was 20/32 95% of subjects, 20/25 in 90%, and 20/20 in 75% (p=0.001; SD=0.09). Distance-corrected near visual acuity (DCNVA) was 20/32 in 85% of subjects, 20/25 in 80%, and 20/20 in 25% (p=0.0008; SD=0.11) (Figure 2) (ASCRS, Boston, MA, 2014).
Laser anterior ciliary excision appears to be a safe procedure for the restoration of accommodation in aging adults. Changing the biomechanical properties in the sclera appears in this IRB monitored pilot study to improve dynamic accommodative range for both intermediate and near vision. Further investigation must be performed to further assess efficacy and long-term stability.
Figure 1. Caption “Model for accommodation and theory of reciprocal zonular action. Courtesy of Daniel Goldberg, MD”.
Figure 2. Caption “Visual outcomes 12 months after Laser Anterior Ciliary Excision”.

Swartz TS, et al.
VII
ReFeRenCeS 1. Goldberg DB. Computer-animated model of accommodation and theory of recipro-
cal zonular action. Clin Ophthalmol. 2011;5:1599-66. 2. Croft MA, Nork TM, McDonald JP, Katz A, Lutjen-Drecoll E, Kaufman PL. Accommo-
dative movements of the vitreous membrane, choroid and sclera in young and presbyopic human and nonhuman primate eyes. Invest Ophthalmolo Vis Sci. 2013; 54(7):5049-58.
3. Lütjen-Drecoll E, Kaufman PL, Wasielewski R, Ting-Li L, Croft MA. Morphology and accommodative function of the vitreous zonule in human and monkey eyes. Invest Ophthalmol Vis Sci. 2010;51(3):1554-64.
4. Pallikaris IG, Kymionis GD, Ginis HS, Kounis GA, Tsilimbaris MK. Ocular rigidity in living human eyes. Invest Ophthalmol Vis Sci. 2005;46(2):409-14.
5. Pallikaris IG, Kymionis GD, Ginis HS, Kounis GA, Christodoulakis E, Tsilimbaris MK. Ocular rigidity in patients with age-related macular degeneration. Am J Ophthalmol.
2006;141(4):611-5. Comment in: Am J Ophthalmol. 2006;142(4):706-7; author reply 707; Am J Ophthalmol. 2006;141(4):731-2.
6. Dastiridou AI, Tsironi EE, Tsilimbaris MK, Ginis H, Karyotakis N, Cholevas P, et al. Ocular rigidity, outflow facility, ocular pulse amplitude, and pulsatile ocular blood flow in open-angle glaucoma: a manometric study. Invest Ophthalmol Vis Sci. 2013;54(7):4571-7.
7. Wilde GS. Measurement of human lens stiffness for modelling presbyopia. Treat-ments [Thesis]. Oxford: Brasenose College, University of Oxford; 2011.
8. Hipsley A, Waring GO, Wang J, Hsiao E. A novel method using collagen cross-linking to evaluate the ability of the LaserACE procedure to decrease ocular rigidity as it re-lates to the efficiency of intra ocular accommodative forces. Poster session presented at: Annual Meeting of the American Society of Cataract and Refractive Surgeons, 2013 Apr 19-23; San Francisco, CA.
9. Hipsley A. Compelling Findings for restoring natural dynamic accommodation using dynamic abberometry. Poster presented at: Annual Meeting of the American Society of Cataract and Refractive Surgeons 2011 Mar 25-29; San Diego, CA.

1Arq Bras Oftalmol. 2014;77(1):1-3
Original Article
InTRODUCTIOnAcute anterior uveitis (AAU) is the most common type of intrao-
cular inflammation, with varying incidence reported worldwide(1). Al-though, in general, it is a smaller threat to vision than posterior uveitis, it is an important cause of blindness and ocular morbidity in Brazil(1,2).
Most often, AAU manifests with varying degrees of pain and ocu-lar hyperemia, visual blurring, and inflammatory cells in the anterior chamber (AC). In severe cases, it can be associated with increased intraocular pressure (IOP)(1). Open-angle or closed-angle glaucoma have been described in 20% uveitis cases(3), and ocular hypertension is considered an important complication of uveitis, particularly when it involves the anterior ocular segment(4).
The corneal involvement during uveitis remains understudied, al-though the cornea is probably a target of intraocular inflammation(2). Inflammation of the anterior segment causes changes in the endo-thelium that, if severe, can compromise the integrity of the cornea; these changes have been observed in some studies using specular microscopy(5). Some authors have proposed that corneal thickness is
an indicator of endothelial function and suggested that this response can be clinically assessed via central pachymetry measurement(6).
Optical coherence tomography (OCT) is a noninvasive and non-contact method that provides information on corneal disorders that cannot be obtained by biomicroscopic examination(7). In addition, it is a high-resolution imaging method for the determination of the AC angle(8).
Therefore, this study aimed to analyze the corneal thickness and AC angle using Anterior Segment OCT (AS-OCT) in patients with AAU.
MeTHODSThis prospective study involved 22 patients (24 eyes) with AAU
admitted to the emergency service of Fundação Altino Ventura de Recife-Pernambuco (FAV); patients with chronic uveitis, panuveites, intermediate and posterior uveitis, other ocular comorbidities, or pre-vious history of eye surgery were excluded. The criteria defined by the Standardization of Uveitis Nomenclature (SUN) Working Group were
Anterior segment optical coherence tomography in acute anterior uveitisTomografia de coerência óptica do segmento anterior em uveíte anterior aguda
criSTiana aGra1, lydianne aGra1, Jeanine danTaS1, TiaGo euGênio Faria e aranTeS1, João linS de andrade neTo1
Submitted for publication: April 15, 2013 Accepted for publication: October 2, 2013
Study carried out at Fundação Altino Ventura, Recife (PE), Brazil.1 Fundação Altino Ventura, Recife (PE), Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: C.L.M. Agra, None; L. Agra, None; J. Dantas, None; T.E.F. Arantes, None; J.L. Andrade Neto, None.
Correspondence address: Cristiana Lumack do Monte Agra. Fundação Altino Ventura - FAV, Rua da Soledade, 170 - Recife (PE), Brazil - 50070-040 - E-mail: [email protected]
ABSTRACT Purpose: To analyze the corneal thickness and anterior chamber (AC) angle using anterior segment optical coherence tomography (AS-OCT) in patients with acute anterior uveitis (AAU). Methods: Twenty two patients (24 eyes) were included. All patients underwent complete ophthalmological examination, applanation tonometry and AS-OCT at diagnosis and fifteen days after treatment. Results: Average corneal thickness before treatment was 564.2 ± 44.2 µm, 580.0 ± 44.3 µm and 580.1 ± 2.9 µm, respectively in central, pericentral and paracentral cornea. Fifteen days after treatment a significant decrease of corneal thickness was observed, with 529.5 ± 33.1 µm (p=0.0091) and 542.6 ± 33.6 µm (p=0.0068), respectively in central and pericentral cornea; paracentral corneal thickness (557.8 ± 35.3 µm) thinning did not reach statistical significance (p=0.1253). There was no significant change in temporal AC angle between visits, 44.3 ± 14.4 degrees before treatment and 44.7 ± 14.7 degrees fifteen days after (p=0.9343), and mean intraocular pressure, 10.8 ± 4.5 mmHg before treatment and 12.3 ± 3.0 mmHg fifteen days after (p=0.1874). Conclusion: In the studied group, AS-OCT detected a decrease of corneal thickness after AAU treatment. Temporal AC angle and intraocular pressure did not change during the studied period.
Keywords: Uveitis, anterior/diagnosis; Tomography, optical coherence; Anterior eye segment; Inflammation; Corneal pachymetry
RESUMO Objetivo: Analisar a espessura corneal e ângulo da câmara anterior (CA) utilizando a tomografia de coerência óptica de segmento anterior (OCT-SA) em pacientes com uveíte anterior aguda (UAA). Métodos: Foram selecionados 24 olhos de 22 pacientes com UAA. Todos foram submetidos a exame oftalmológico completo, tonometria de aplanação e OCT-SA na consulta inicial e após 15 dias de início do tratamento. Resultados: Na visita inicial, as médias da espessura corneal foram de 564,2 ± 44,2 µm e 580,0 ± 44,3 µm e 580,1 ± 2,9 µm, respectivamente para as regiões central, pericentral e paracentral. Após 15 dias de tratamento, observou-se redução da espessura para 529,5 ± 33,1 µm (p=0,0091) e 542,6 ± 33,6 µm (p=0,0068), respectivamente para a córnea central e pericentral; e um valor de 557,8 ± 35,3 µm para a região paracentral, porém para um p não significante (p=0,1253). Não foi observada mudança estatisticamente significante nos valores da porção temporal do ângulo da CA; 44,3 ± 14,4 graus na visita inicial e de 44,7 ± 14,7 graus após 15 dias de tratamento (p=0,9343) e na média das pressões intraoculares (PIO), 10,8 ± 4,5 mmHg na visita inicial e 12,3 ± 3,0 mmHg após tratamento (p=0,1874). Conclusão: No grupo estudado, obteve-se uma redução dos valores da espessura corneal após início do tratamento da UAA. Os valores da porção temporal do ângulo da CA e PIO não sofreram mudanças significantes.
Descritores: Uveíte anterior/diagnóstico; Tomografia de coerência óptica; Segmento anterior do olho; Inflamação; Paquimetria corneana

Anterior segment optical coherence tomography in acute anterior uveitis
2 Arq Bras Oftalmol. 2014;77(1):1-3
used to select patients, and eye samples with scores ranging from +1 to +4 were included(9). The disease was diagnosed on the basis of clinical history and eye examination.
The subjects were invited to undergo the first OCT-SA at the time of the initial emergency visit and to return to the service for the second examination 15 days after treatment initiation. The procedure was performed before dilatation of the pupils in both situations. IOP was measured using Goldmann applanation tonometry on both con sultations.
Images of the anterior segment were obtained using the anterior segment module of the RTVue® Fourier-domain system (Optovue, Fremont, California, USA). The central thickness of the cornea and the trabecular temporal angle of AC were measured during the same consultation. During the exam, the central corneal thickness was measured using the pachymetry map obtained with the use of an optional attached lens (CAM-L) (8 × 1024 A-scans). The temporal angle of AC was obtained through the scan of AC angle provided by the same lens CAM-L (1 × 1024 A-scans). The pachymetry map was generated by the system from eight 6-mm-long meridional scans centralized in the pupil. Each 6-mm line consisted of 1.024 axial scans acquired in 0.04 s and the set of eight meridians was obtained in 0.31 s. Five consecutive sets were obtained in 1.55 s and the three most consistent were used to calculate corneal power. Thickness was analyzed in three sectors: central area (2 mm central diameter); pericentral area (ring between 2 and 5 mm), and paracentral area (ring between 5 and 6 mm)(10).
The Schwalbe line (SL), a visible anatomical structure with good image definition in the sections produced by the system, was consi-dered the reference to measure AC angle. The measure of the angle opening from SL is a method of quantifying AC angle opening in RTVue images. Transverse scans (6 × 2 mm) were performed and the temporal portion of AC angle was analyzed(10).
Statistical analysis was performed with the Epi Info (version 7) and the R-cran (version 15) software programs. The results of the quanti-tative variables were expressed as means ± standard deviation (SD), whereas the qualitative variables were expressed as absolute and relative frequencies. The Wilcoxon test was used to assess the mean difference, and the level of significance was set at 5%.
The study was approved by the Ethics Committee in Human Research (protocol No. 026/2011). All patients signed an informed consent and received ophthalmological follow-up care.
ReSULTSTwenty-two patients (24 eyes) participated in the study, inclu-
ding 15 women (68.2%) and 7 men (31.8%). The age of the parti-cipants ranged between 7 and 72 years (mean 42.8 ± 20.3 years). Seventeen patients had the first episode of AAU and 10 patients had recurrent AAU.
The results of the biomicroscopic examination of the anterior segment in the first consultation and 15 days after treatment are shown in Table 1.
Before the initiation of the treatment, the mean central corneal thickness of patients was 564.2 ± 44.2 µm; the thickness of the pe-ricentral and paracentral areas were 580.0 ± 44.3 µm and 580.1 ± 2.9 µm, respectively. Fifteen days after the initiation of treatment, there was a reduction in corneal thickness. The mean value of the patients’ central thickness was 529.5 ± 33.1 µm, the pericentral thickness was 542.6 ± 33.6 µm, and the paracentral thickness was 557.8 ± 35.3 µm. The central and pericentral corneal thickness was higher before the initiation of treatment, p = 0.0091 and 0.0068, respectively, whereas the paracentral thickness decreased; however, p was not significant (p=0.1253) (Figure 1).
The mean AC angles of participants was 44.3° ± 14.4° and the mean intraocular pressure was 10.8 ± 4.5 mmHg before treatment. After treatment, the mean AC angle were 44.7° ± 14.7° and the mean
intraocular pressure was 12.3 ± 3.0 mmHg (Figure 2). Tonometry values were not obtained for two patients because of their difficulty in participating in the study. No patient had IOP of >21 mmHg. The values of AC angle and IOP between the assessed periods were not significantly different (p=0.9343 and 0.1874, respectively) (Table 2).
DISCUSSIOnIn general, anterior uveitis (AU) is associated with fewer sequelae
than inflammation of the posterior segment, especially if it is treated early. However, its potential for severe ocular consequences is proba-bly underestimated if recurrent or poorly managed(1).
Endothelial anomalies have been observed in cases of AU and posterior uveitis. Some authors have studied these changes in several corneal disorders and uveitis, using specular microscopy(2). It is well known that endothelial anomalies occur in uveitis(5).
Polymorphism and polymegathism of the endothelial cells can occur in AU(5,7). Studies using specular microscopy have demonstra-
Figure 1. A) Pachymetry map before the start of the treatment. B) Pachymetry map 15 days after the start of the treatment.
A
B
Table 1. Results of the anterior segment biomicroscopy of the 24 eyes with acute anterior uveitis subjected to AS-OCT
Initial visit 15th day of treatment
Results n (%) n (%)
Keratic precipitates 06 (25.0) 01 (04.2)
Fibrin membrane 04 (16.7) 00 (00.0)
Posterior synechiae 07 (29.2) 03 (12.5)
Iris pigments in the lens 05 (20.8) 04 (16.7)
Anterior chamber cell core n (%) n (%)
+1 04 (16.7) 17 (70.8)
+2 11 (45.8) 04 (16.7)
+3 05 (20.8) 02 (08.3)
+4 04 (16.7) 01 (04.2)

Agra C, et al.
3Arq Bras Oftalmol. 2014;77(1):1-3
ted endothelial changes induced by inflammation, which include de-fects in the endothelium associated to the deposition of precipitates on the posterior surface of the cornea and other defects similar to guttata and not associated with the precipitates. Moreover, in most patients, these alterations tended to disappear completely, together with other signs of acute inflammation, without changes in cell count, and were significantly correlated with the increase in corneal thickness during the inflammatory period of the disease(11). Despite these anomalies, the majority of cases of uveitis did not progress to per-manent corneal decompensation(5,6) and pachymetry values returned to normal by the end of the inflammatory crisis(6).
Table 2. Comparison between the variables observed on AS-OCT regarding the assessment period
Variables
Assessment period(Mean ± SD) p
valuePretreatment Post-treatment
Central pachymetry (µm) 564.2 ± 44.2 529.50 ± 33.1 0.0091
Pericentral pachymetry (µm) 580.0 ± 44.3 542.59 ± 33.6 0.0068
Paracentral pachymetry (µm) 580.1 ± 02.9 557.77 ± 35.3 0.1253
Angle of the anterior chamber (o) 044.3 ± 14.4 044.73 ± 14.7 0.9343
Intraocular pressure (mmHg) 010.8 ± 04.5 012.27 ± 03.0 0.1874
Figure 2. A) Temporal portion of the AC angle viewed on SA-OC before the start of the treatment. B) Temporal portion of AC 15 days after the start of the treatment.
A
B
In a study conducted in patients with Behçet’s disease, the mean central pachymetry in patients with active disease was significantly higher than that in patients with inactive disease and in the control group. Some mechanisms have been proposed to explain the nega-tive effect of the inflammatory process on the endothelium. In this sense, several inflammatory mediators and cytokines have been found in the aqueous humor and cornea during inflammation and are probably responsible for cellular damage(6).
The patients in this study exhibited a significant reduction in mean central pachymetry between the initial period of the disease and following the control of ocular inflammation (564.2 ± 44.3 µm to 529.50 ± 33.1 µm, respectively). We would like to point out that no patient had edema of the cornea on clinical examination.
The patients in this study did not exhibit a significant change in IOP during the disease; however, inflammation of the anterior seg-ment, particularly in severe cases, can occur with the increase in IP(1). We observed an increase in pachymetry in the sample during the uveitis crisis. Thickening of the cornea caused by edema can lead to underes-timated IOP measurement by Goldmann applanation tonometry(12,13), which may interfere with the established approach.
In this study, the mean temporal AC angle was within normal values and the difference between the pretreatment and post-treat-ment periods was not statistically significant, probably because most of these patients exhibited mild to moderate ocular inflamma-tion, with low frequency of posterior synechiae. In addition, there were few cases of recurrent uveitis, and without sequelae from previous episodes.
COnCLUSIOnSAnterior segment optical tomography detected a reduction in
the corneal thickness 15 days after initiation of the acute anterior uveitis treatment. No alterations in the anterior chamber angle were observed.
ReFeRenCeS 1. Agrawal RV, Murthy S, Sangwan V, Biswas J. Current approach in diagnosis and mana-
gement of anterior uveitis. Indian J Ophthalmol. 2010;58(1):11-9. Review. 2. Oliveira F, Motta AC, Muccioli C. [Corneal specular microscopy in infectious and no-
nin fectious uveitis]. Arq Bras Oftalmol. 2009;72(4):457-61. Portuguese. 3. Bodh SA, Kumar V, Raina UK, Ghosh B, Thakar M. Inflammatory glaucoma. Oman J
Ophthalmol. 2011;4(1):3-9. 4. Pogorzalek N, de Monchy I, Gendron G, Labetoulle M. [Hypertony and uveitis: 103 cases
of uveitis]. J Fr Ophtalmol. 2011;34(3):157-63. French. 5. Pillai CT, Dua HS, Azuara-Blanco A, Sarhan AR. Evaluation of corneal endothelium and
keratic precipitates by specular microscopy in anterior uveitis. Br J Ophthalmol. 2000; 84(12):1367-71.
6. Ozdamar Y, Berker N, Ertugrul G, Gurlevik U, Karakaya J, Ozkan SS. Is there a change of corneal thickness in uveitis with Behçet disease? Cornea. 2010;29(11):1265-7.
7. Hirano K, Ito Y, Suzuki T, Kojima T, Kachi S, Miyake Y. Optical coherence tomography for the noninvasive evaluation of the cornea. Cornea. 2001;20(3):281-9.
8. Khor WB, Sakata LM, Friedman DS, Narayanaswamy A, Lavanya R, Perera SA, et al. Eva-luation of scanning protocols for imaging the anterior chamber angle with anterior segment-optical coherence tomography. J Glaucoma. 2010;19(6):365-8.
9. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509-16. Review.
10. Huang D. RTVue fourier-domain optical coherence tomography primer series. Vol. II Cornea and anterior segment. Fremont: Optovue Inc; 2009.
11. Olsen T. Transient changes in specular appearance of the corneal endothelium and in corneal thickness during anterior uveitis. Acta Ophthalmol (Copenh). 1981;59(1):100-9.
12. Heinz C, Taneri S, Roesel M, Heiligenhaus A. Influence of corneal thickness changes during active uveitis on Goldmann applanation and dynamic contour tonometry. Ophthalmic Res. 2012;48(1):38-42.
13. Ehlers N, Bramsen T, Sperling S. Applanation tonometry and central corneal thickness. Acta Ophthalmol (Copenh). 1975;53(1):34-43.

4 Arq Bras Oftalmol. 2014;77(1):4-7
Original Article
InTRODUCTIOnPterygium is characterized by the encroachment of a fleshy fi -
bro vascular tissue from the bulbar conjunctiva onto the cornea. Al-though historically described as a degenerative disorder, it is more closely associated with inflammation and progressive fibrovascular proliferation(1-3).
The pathogenesis of pterygium appears to be complex. Despite being historically described more as a degenerative process, inflam-mation and fibrovascular proliferation are currently proven to be im portant factors. Angiogenesis has also been demonstrated during pterygium formation and progression(4-5).
The current treatments for pterygium focus on surgical excision and prevention of recurrence. The extent and severity of the fibrovas-
cular growth of pterygium seem to comprise a reliable morphologi-cal index for predicting recurrence after surgery(6).
Recurrence of pterygium is the most common undesirable outco me after surgical excision. Recurrent pterygia are more hazardous than primary ones because the underlying cornea may be thinner. Exten-sive scarring from previous procedures can adversely affect visual acuity, and further recurrence is common(7).
Several studies have shown that the increased expression of basic fibroblast growth factor (bFGF), transforming growth factor (TGF-β), vascular endothelial growth factor (VEGF), and platelet-derived growth factor correlates with the formation and recurrence of pterygia(8-11).
Bevacizumab (Avastin®, Genentech, Inc., San Francisco, CA, USA) is a humanized monoclonal antibody to VEGF designed for intravenous (IV) administration and approved for the treatment of colorectal
Efficacy and safety of subconjunctival bevacizumab for recurrent pterygiumEficácia e segurança da aplicação subconjuntival de bevacizumabe em pterígio recidivado
lariSSa roSSana Souza STival1, aneliSe MedeiroS laGo1, MariSa novaeS Falleiro chaveS de FiGueiredo1, ricardo henrique GoularT biTTar1, Márcia leiTe Machado1, João JorGe naSSaralla Junior1,2
Submitted for publication: June 13, 2013 Accepted for publication: October 5, 2013
Study carried out at Instituto de Olhos de Goiânia.1 Goiânia Eye Institute, Goiânia, Goiás, Brazil.2 Department of Ophthalmology, Faculty of Health Sciences, Universidade de Brasília, UNb, Brasília
(DF), Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: L.R.S. Stival, None; A.M. Lago, None; M.N.F.C. Figueiredo, None; R.H.G. Bittar, None; M.L. Machado, None; J.J. Nassaralla Jr, None.
Correspondence address: Larissa Rossana Souza Stival. Rua 2, 708 - Apto. 701 - Ed. Thitara Park - Setor Oeste, Goiânia (GO) - 74110-130 - Brazil - E-mail: [email protected]
ClinicalTrials.gov ID- NCT01744756
Research Ethics Committee: Goiania Eye Institute, Goiania, Goiás, Brazil.
ABSTRACTPurpose: To evaluate the clinical outcome(s) and complication(s) of subcon-junctival bevacizumab treatment in patients with recurrent pterygium. Methods: This prospective case series included patients who had undergone pterygium surgery and were diagnosed with recurrent pterygium. All patients received one subconjunctival injection of 0.5 mL of bevacizumab (2.5 mg/0.1 mL). The main outcome was the change in size and clinical appearance. The clinical appearance of the pterygium was graded according to Tan and colleagues. The horizontal size of the pterygium (from limbus to apex) was recorded from baseline to 2 months after injection. Treatment-related complications and adverse events were reported. Results: We included 36 eyes of 36 patients (18 males) with a mean age of 58.75 ± 10.98 years. Totally, 30.6% patients developed recurrent pterygium in both eyes (only the worst eye was treated), with 47.2% developing it in the left eye and 22.2% in the right eye. More than half the patients (58.3%) had a family history of pterygium. There was a significant difference in the size of pterygium at different intervals (P<0.05). Approximately two-thirds (66.7%) of patients pre-sented with hyposphagma on the 2nd day after subconjunctival application; this value decreased to 30.6% by day 7 and to 0% at 1 month. Most patients (69.4%) ex hibited amelioration of irritative symptoms within 2 days, 88.9% after 7 days, and 97.2% after 1 month. Conclusions: Subconjunctival bevacizumab injection is useful for the manage-ment of patients with recurrent pterygium, with no significant local or systemic adverse effects.
Keywords: Pterygium; Recurrence; Antibodies, monoclonal/therapeutic use; Angio -genesis inhibitors/administration & dosage; Injections
RESUMOObjetivo: Avaliar os resultados e complicações da injeção subconjuntival de bevaci-zumabe em pacientes com pterígio recidivado.Métodos: Série de casos prospectiva envolvendo pacientes submetidos à exérese de pterígio que foram diagnosticados com pterígio recidivado. Todos pacientes receberam uma aplicação subconjuntival 0,5 ml de bevacizumabe (2,5 mg/0,1 ml). O principal resultado foi a mudança no tamanho dos pterígios. A aparência clínica do pterígio foi graduada de acordo com os critérios de Tan et al. O tamanho horizontal do pterígio (do limbo ao ápice) foi observado até 60 dias semanas após a injeção. Os efeitos adversos e as complicações do tratamento foram descritos.Resultados: Foram incluídos 36 olhos de 36 pacientes (18 masculinos) com média de idade de 58,75 ± 10,98 anos. 30,6% dos pacientes tinham pterígio recidivado em ambos os olhos (apenas o pior olho foi tratado), 47,2% no olho esquerdo e 22,2% no olho direito. Mais da metade dos pacientes (58,3%) possuíam história familiar de pterígio. Houve uma diferença estatisticamente significante no tamanho do pterígio em diferentes intervalos (P<0,05). 66,7% dos pacientes apresentaram hemorragia subconjuntival no segundo dia após a aplicação, diminuindo para 30,6% no sétimo dia e nenhum paciente após um mês. A maioria dos pacientes (69,4%) teve melhora dos sintomas irritativos após dois dias, 88,9% após 7 dias e 97,2% após um mês.Conclusão: A injeção subconjuntival de bevacizumabe é uma alternativa válida na condução de pacientes com pterígio recidivado, não apresentando efeitos locais e sistêmicos significantes.
Descritores: Pterígio; Recidiva; Anticorpos monoclonais/uso terapêutico; Inibidores de angiogênese/administração & dosagem; Injeções

Stival LRS, et al.
5Arq Bras Oftalmol. 2014;77(1):4-7
cancer(11). Various clinical trials have shown that intravitreal admi-nistration is well tolerated and associated with an improvement in visual acuity, decrease in central retinal thickness, and decrease in angiographic leakage(12,13).
Pterygia are composed of proliferating fibrovascular tissue, and pterygium formation and progression require new blood vessel formation(14). Prominent regression of limbal-conjunctival neovascu-larization and delayed recurrence have been reported with the use of topical bevacizumab in patients with impending recurrent pterygium(15-16).
Anti-VEGF therapy may potentially suppress neovascularization in pterygium, preventing or retarding the progression of recurren-ce(17-19). This study aimed to determine the clinical effectiveness and safety of subconjunctival injection of bevacizumab for recurrent pterygium.
MeTHODSThis was a prospective, single-dosing, interventional case series
conducted at Instituto de Olhos de Goiânia (Goiânia Eye Institute), a hospital in Goiânia (Brazil), from March 2012 to December 2012 in patients with recurrent pterygium. Recurrent pterygium was defined as the growth of fibrovascular tissue over the limbus onto the clear cornea in the area of previous pterygium excision.
The pterygia were graded according to the system used by Tan et al.(6): grade I (atrophic), in which the episcleral vessels under the body of the pterygium are not obscured and clearly distinguished; grade II (intermediate); and grade III (fleshy), in which the episcleral vessels are totally obscured. Exclusion criteria included any condition for which bevacizumab was contraindicated (allergy to bevacizumab, proteinuria, bleeding tendencies, previous myocardial infarction or stroke, pregnancy, and lactation), evidence of other ocular diseases except refraction errors, use of topical medications for pterygium, presence of other complaints not attributable to pterygium, prior ocular trauma, more than one recurrent pterygia, and the inability to follow-up for the entire duration of the study.
Patients were interviewed before injection using a questionnaire to obtain information such as general data, contact number, demo-graphic factors, and medical, surgical, and ocular history.
Informed consent was obtained from all patients after the nature and possible consequences of the study were explained. The study was approved by the Institutional Research Ethics Committee. In cases of bilateral recurrent pterygium, only the worst eye was treated.
All injections were administered by a single investigator in an operating room. Eyes were anesthetized with topical proparacaine hydrochloride drops. A subconjunctival injection of 0.5 mL of bevaci-zumab (Avastin® 2.5 mg/0.1 mL, F. Hoffmann-La Roche, Basel, Switzer-land) was administered at the limbus, adjacent to the pathological blood vessels growing/sprouting into the cornea. Using an eyelid speculum, injections were administered at the slit lamp following appli-cation of topical anesthetic eyedrops. After surgery, patients were treated with topical Cilodex® (ciprofloxacyn and dexamethasone, Alcon Laboratories Ltd.) eye drops 4 times daily for 15 days.
As per our protocol, all eyes received a single bevacizumab in-jection. All eyes were biomicroscopically examined before surgery, 2 and 7 days after surgery, and 1 and 2 months after surgery. Complete opthalmological evaluation was performed for each patient. This included visual acuity determination, applanation tonometry, slit-lamp examination, and anterior segment photography. At each visit, 2 di-gital corneal photographs were obtained using a digital camera. The size of pterygium was measured horizontally from the limbus to the apex and graded according to the system used by Tan et al. using the slit-lamp microscope(6).
Any complications and adverse events were noted. The same pho -tographer captured images of the anterior segment using the same camera at every follow-up visit. Postinjection complications such as
ocular surface toxicity, corneal abrasion, persistent epithelial defect, subconjunctival hemorrhage, and infection were noted, as was any change in the size and vascularity of pterygium.
Statistical analyses were performed using SPSS version 18.0 (SPSS, Chicago, IL). The paired t test was used to compare changes in the size of pterygia, and the Friedman test was used to determine the significance of changes after treatment. Probabilities of less than 5% were considered statistically significant.
ReSULTSThe study group comprised 36 eyes of 36 patients with recurrent
pterygium. These included 18 males (50%) and 18 females (50%) with a mean age of 58.75 years (SD, 10.98 years). Close to one-third (30.6%) of the patients had recurrent pterygia in both eyes. The left and right eyes were affected in 47.2% and 22.2% patients, respectively. Appro-ximately 44.4% patients were from Goiânia (Brazil), while 55.6% were from other cities. More than half the patients (58.3%) had a family history of pterygium.
According to the results of graph 1 (paired-samples test), there was a significant difference in the size (in mm) of pterygium at diffe-rent intervals (P<0.05) after the injection of bevacizumab.
Table 1 represents the distribution of patients according to the classification of Tan et al.(6) before and 60 days after one injection of 0.5 mL of bevacizumab (2.5 mg/0.1 mL). There was a difference in the gradation of pterygium before and after application.
The mean surface area was decreased. There was a significant diffe-rence in the gradation according to the system used by Tan et al.(6) at different intervals (P<0.05), particularly 30 days after injection.
Approximately two-thirds (66.7%) of the patients presented with hyposphagma on the 2nd day after subconjunctival injection; this decreased to 30.6% by day 7 and to 0% at 1 month. Most pa-tients (69.4%) exhibited amelioration of irritative symptoms within 2 days, 88.9% patients after 7 days, and 97.2% after 1 month. The aspect of the recurrent pterygium after injection did not change conside-rably (Figure 1).
Graph 1. There was a significant change in the size of pterygium at different intervals (P<0.05; paired t-test) after the injection of bevacizumab. The mean pterygium size ranged from 2.37 mm to 1.61 mm. These patients were only the treated ones.
Table 1. Distribution of patients according to the classification of Tan et al.(6) before and 60 days after one application of 0.5 ml of bevacizumab (2.5 mg/0.1 ml)
Pre 60-day visit Total
Grade I 06 (16.7%) 15 (41.7%) 21
Grade II 20 (55.6%) 17 (47.2%) 37
Grade III 10 (27.8%) 04 (11.1%) 14
Total 36 36 72

Efficacy and safety of subconjunctival bevacizumab for recurrent pterygium
6 Arq Bras Oftalmol. 2014;77(1):4-7
DISCUSSIOnIn recent years, anti-VEGF agents such as bevacizumab and rani-
bizumab have been evaluated as an adjunctive therapy for pterygium along with surgical excision or as a nonsurgical therapy(20).
Recent studies have reported successful outcomes after the ad-ministration of bevacizumab for the treatment of corneal neovas-cularization. Erdurmus and Totan(21-22) evaluated the efficacy of sub -conjunctival bevacizumab injection (2.5 mg/0.1 mL) in 2 patients with corneal neovascularization along with the associated etiologies. One patient had dry eye and exhibited significantly regression of ve ssels a week after injection, while the other patient had a failed graft and exhibited only minor vessel regression. Awadein(23) descri bed 3 pa-tients with corneal neovascularization after keratoplasty who were trea-ted with a single subconjunctival injection of 2.5 mg bevacizumab. In all patients, the number and caliber of blood vessels decreased after injection. The regression of the corneal new vessels was more marked in patients with smaller and/or fewer blood vessels. However, in patients with old and rejected vascularized grafts, there was little change in the number and caliber of blood vessels(21).
Recently, several studies have been conducted to evaluate the effects of local therapy with bevacizumab on both primary and recur-rent pterygium(24-27). Bevacizumab has been used at various doses at various times by different routes of administration. Nonetheless, the results remain limited and controversial, and there is no clear rando-mized controlled trial that has studied the efficacy of subconjunctival bevacizumab in patients with impending recurrent pterygium(28-30).
A single administration of an arbitrary dose based on the intravi-treal preparation of bevacizumab may be inadequate. A single dose of 1.25 mg of intravitreal bevacizumab has been reported to provide complete intravitreal VEGF blockade for a minimum of 4 weeks, with an intravitreal bevacizumab half-life of approximately 3 days(28). Ho-wever, the conjunctival half-life of the drug may be shorter than the vitreous half-life because of the higher systemic absorption through the abundant conjunctival vessels(24). Repeat injections or higher doses of bevacizumab may be required to achieve better outcomes. Nevertheless, increased or multiple doses may be accompanied by significant side effects.
Our study illustrated that a single subconjunctival dose of beva-cizumab dose is partly efficacious in decreasing conjunctival vascu-larization in the impending recurrent pterygium compared with that at baseline. Nevertheless, the favorable effect was incomplete and temporary, similar to that reported by Leippi et al.(25).
Previous reports suggesting the effective role of subconjunctival bevacizumab were noncomparative case reports(25,28,31). Corneal neo-vascularization was inhibited or regressed, but not completely elimi-
Figure 1. A and C) Before subconjuntival application of bevacizumab in recurrent pte-rygium. B and D) 60 days after de application.
A B
C D
nated. Delayed recurrence was observed in a study by Fallah et al., who used topical bevacizumab to inhibit the growth of impending recurrent pterygium in 26 eyes, although the pterygia eventually ex-tended onto the cornea(17).
Other factors such as tumor necrosis factor alpha, bFGF, TGF-β, and platelet-derived growth factor (PDGF) have been shown to correlate with the formation and recurrence of pterygium. Immuno reactivity for these growth factors was located in epithelial cells, en dothelial cells of vessels, basement membranes of vessels, and the epithelium, fibroblasts, and infiltrating inflammatory cells in pterygium(28,29).
COnCLUSIOnSThe limitations of this study include the short duration of follow-up,
the lack of a control group, the limited number of patients, and the difficulty in objectively measuring the size of recurrent pterygia be-fore and after injection.
Further studies with larger sample sizes will be required to deter-mine the appropriate dosing schedule, efficacy, and safety profile. In addition, anti-VEGF treatment may have a greater synergistic effect when combined with treatment targeting alternate cytokines and growth factors and should be investigated in future studies. New an -tiangiogenic therapies will hopefully focus more on facilitating deli-very into tissue, increasing the duration of effect while continuing to minimize adverse side effects.
In summary, a single administration of subconjunctival bevaci-zumab to recurrent pterygium was well tolerated and decreased irritation and vascularization for a short term. The transient effect was likely related to the limited bioavailability of the drug in the setting of continued VEGF expression.
ReFeRenCeS 1. Hill JC, Maske R. Pathogenesis of pterygium. Eye (Lond). 1989;3(Pt 2):218-26. 2. Cameron ME. Histology of pterygium: An electron microscopic study. Br J Ophthalmol.
1983;67(9):604-8. 3. Cilova-Atanasova B. On the pathogenesis of pterygium. Folia Med (Plovdiv). 1971;
13(2):67-74. 4. Mauro J, Foster CS. Pterygia: pathogenesis and the role of subconjunctival bevacizu-
mab in treatment. Semin Ophthalmol. 2009;24(3):130-4. 5. Hosseini H, Nejabat M, Khalili MR. Bevacizumab (Avastin) as a potentialnovel adjunct
in the management of pterygia. Med Hypotheses. 2007;69(4):925-7. 6. Tan DT, Chee SP, Dear KB, Lim AS. Effect of pterygium morphology on pterygium
recurrence in a controlled trial comparing conjunctival autografting with bare sclera excision. Arch Ophthalmol. 1997;115(10):1235-40. Erratum in: Arch Ophthalmol. 1998; 116(4):552.
7. Busin M, Halliday BL, Arffa RC, McDonald MB, Kaufman HE. Precarved lyophilized tissue for lamellar keratoplasty in recurrent pterygium. Am J Ophthalmol. 1986;102(2):222-7.
8. Kria L, Ohira A, Amemiya T. Immunohistochemical localization of basic fibroblast growth factor, platelet derived growth factor, transforming growth factor-beta and tumor necrosis factor-alpha in the pterygium. Acta Histochem. 1996;98(2):195-201.
9. Kria L, Ohira A, Amemiya T. Growth factors in cultured pterygium fibroblasts: immuno-histochemical and ELISA analysis. Graefes Arch Clin Exp Ophthalmol. 1998;236(9):702-8.
10. Lee JK, Song YS, Ha HS, Park JH, Kim MK, Park AJ, et al. Endothelial progenitor cells in pterygium pathogenesis. Eye (Lond). 2007;21(9):1186-93.
11. Jin J, Guan M, Sima J, Gao G, Zhang M, Liu Z, et al. Decreased pigment epithelium- derived factor and increased vascular endothelial growth factor levels in pterygia. Cornea. 2003;22(5):473-7.
12. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, Bevaci-zumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335-42. Comment in: N Engl J Med. 2004;350(23):2406-8; Nat Clin Pract Gastroenterol Hepatol. 2004;1(2):72-3; Cancer Treat Rev. 2004;30(8):715-7; N Engl J Med. 2004;351(16):1690-1; author reply 1690-1.
13. Rosenfeld PJ, Moshfeghi AA, Puliafito CA. Optical coherence tomography findings after an intravitreal injection of bevacizumab (Avastin) for neovascular age related macular degeneration. Ophthalmic Surg Laser Imaging. 2005;36(4):331-5. Comment in: Ophthalmic Surg Lasers Imaging. 2005;36(4):270-1.
14. Avery RL, Pieramici DJ, Rabena MD, Castellarin AA, Nasir MA, Giust MJ. Intravitreal beva-cizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology. 2006;113(3):363-72. Comment in: Ophthalmology. 2007;114(2):400; author reply 400-1.
15. Wu PC, Kuo HK, Tai MH, Shin SJ. Topical bevacizumab eye drops for limbal: conjunc-tival neovascularization in impending recurrent pterygium. Cornea. 2009;28(1):103-4.

Stival LRS, et al.
7Arq Bras Oftalmol. 2014;77(1):4-7
16. Di Girolamo N, Coroneo MT, Wakefield D. Active matrilysin (MMP-7) in human pterygia: potential role in angiogenesis. Invest Ophthalmol Vis Sci. 2001;42(9):1963-8.
17. Fallah MR, Khosravi K, Hashemian MN, Beheshtnezhad AH, Rajabi MT, Gohari M. Efficacy of topical bevacizumab for inhibiting growth of impending recurrent pterygium. Curr Eye Res. 2010;35(1):17-22.
18. Shenasi A, Mousavi F, Shoa-Ahari S, Rahimi-Ardabili B, Fouladi RF. Subconjunctival bevacizumab immediately after excision of primary pterygium: the first clinical trial. Cornea. 2011;30(11):1219-22.
19. Lekhanont K, Patarakittam T, Thongphiew P, Suwan-apichon O, Hanutsaha P. Ran-domized controlled trial of subconjunctival bevacizumab injection in impending recurrent Pterygium: a pilot study. Cornea. 2012;31(12):155-61.
20. Ozgurhan EB, Alper A, Kara N, Yuksel K, Dermican A, Demirok A. Topical application of bevacizumab as an adjunct to recurrent pterygium surgery. Cornea. 2013;32(6):835-8.
21. Fallah T, Tafti MR, Khosravifard K, Mohammadpour M, Hashemian M, Kiarudi M. Effica cy of intralesional bevacizumab injection in decreasing pterygium size. Cornea. 2011;30(2):127-9.
22. Erdurmus M, Totan Y. Subconjunctival bevacizumab for corneal neovascularization. Graefes Arch Clin Exp Ophthalmol. 2007;245(10):1577-9.
23. Awadein, A. Subconjunctival bevacizumab for vascularized rejected corneal grafts. J Cataract Refract Surg. 2007;33(11):1991-3.
24. Spaide RF, Fisher YL. Intravitreal bevacizumab (Avastin) treatment of proliferative diabetic retinopathy complicated by vitreous hemorrhage. Retina. 2006;26(3):275-8.
25. Leippi S, Grehn F, Geerling G. [Antiangiogenic therapy for pterygium recurrence]. Oph thalmologe. 2009;106(5):413-9. German.
26. Wu PC, Kuo HK, Tai MH, Shin SJ. Topical bevacizumab eyedrops for limbalconjunctival neovascularization in impending recurrent pterygium. Cornea. 2009; 28(1):103-4.
27. Bahar I, Kaiserman I, McAllum P, Rootman D, Slomovic A. Subconjunctival bevacizu-mab injection for corneal neovascularization in recurrent pterygium. Curr Eye Res. 2008; 33(1):23-8.
28. Beer PM, Wong SJ, Hammad AM, Falk NS, O´Malley MR, Khan S. Vitreous levels of un-bound bevacizumab and unbound vascular endothelial growth factor in two patients. Retina. 2006;26(8):871-6.
29. Mansour AM. Treatment of infl amed pterygia or residual pterygial bed. Br J Ophthal-mol. 2009;93(7):864-5.
30. Enkvetchakul O, Thanathanee O, Rangsin R, Lekhanont K, Suwan-Apichon O. A rando-mized controlled trial of intralesional bevacizumab injection on primary pterygium: preliminary results. Cornea. 2011;30(11):1213-8.
31. Shahin MM, Elbendary AM, Elwan MM. Intraoperative subconjunctival bevacizumab as an adjunctive treatment in primary pterygium: a preliminary report. Ophthalmic Surg Lasers Imaging. 2012;43(6):459-66.
XXI Congresso Brasileiro de Prevenção da Cegueira e Reabilitação Visual
II Congresso de Oftalmologia de Língua Portuguesa
3 a 6 de setembro de 2014 Centro de Convenções de Pernambuco
Recife (PE)
informações: ASSESSOR - Assessoria e Marketing
Tels.: (81) 3423-1300 / 9172-7580 E-mail: [email protected]
MAIS EventosTels.: (81) 3033-5147 / 81 8129-4354 E-mail: [email protected]
Site: http://www.congressocbo.com.br/cbo2014/

8 Arq Bras Oftalmol. 2014;77(1):8-11
Original Article
InTRODUCTIOnVision is a complex process. It allows individuals the experience
of shapes and colors as well as the perception of the surrounding environment. It allows an immediate assessment of the elements that stimulate the curiosity and interest of children and plays an important role in image synthesis and formation(1). Vision is not an isolated pro-cess. It is integrated with a child’s neuropsychomotor development, which includes the development of head posture(2).
For an effective eye gaze, the visual fixation of an object should be sustained on the foveal zone for at least 3 s. Visual fixation is the result of a series of movements, such as saccades, which focus the object of interest in the fovea and move the eyes from one object to another. Fixation can occur either voluntarily or as a reflex, similar to visual pursuit, which is characterized by slow and smooth ocular movements. The main function of visual pursuit is to track the visual stimulus and maintain it near the fovea(3).
Effective visual fixation is necessary for good visual acuity. Visual acuity is a quantitative assessment of the ability of the human sensory system to discriminate detail in objects(4).
The close association between visual acuity and nystagmus has been reported in the literature(5-9). Nystagmus comprises involuntary ocular oscillations that prevent the adequate projection of the image on the retina(5). In nystagmus, saccadic movements hinder foveal fixation, leading to the impairment of visual acuity(6,7).
In congenital nystagmus, which has its onset between either 2 and 3 months or 6 and 12 months of age, visual fixation is possible with a head posture that minimizes nystagmus. At this stage, compensatory movements of the head in the so-called “null position” can occur(10).
Abnormal head positioning implies that this posture is adopted to achieve visual adaptation. In addition, the null position is a habit, and not the cause of nystagmus. It promotes ocular stability and is naturally adopted by children with visual impairment(11).
Influence of head posture on the visual acuity of children with nystagmusInfluência da postura da cabeça na acuidade visual de crianças com nistagmo
ana carla raMoS vieira da coSTa1, Márcia caireS beSTilleiro lopeS2, célia reGina naKanaMi3
Submitted for publication: January 30, 2013 Accepted for publication: October 9, 2013
Study carried out at Departamento de Oftalmologia da Universidade Federal de São Paulo/Unifesp - Setor de Baixa Visão e Reabilitação Visual-Ambulatório de Estimulação Visual Precoce em parceria com a Universidade de Santo Amaro.
1 Ambulatório de Estimulação Visual Precoce, Universidade Federal de São Paulo, UNIFESP, São Paulo (SP), Brazil.
2 Universidade Federal de São Paulo, UNIFESP, São Paulo (SP), Brazil.3 Setor de Baixa Visão e Reabilitação Visual, Universidade Federal de São Paulo, UNIFESP, São
Paulo (SP), Brazil.
Funding: This study was supported by Bolsa de Iniciação Científica da Universidade de Santo Amaro.
Disclosure of potential conflicts of interest: A.C.R.V. Costa, None; M.C.B. Lopes, None; C.R. Nakanami, None.
Correspondence address: Ana Carla Ramos Vieira da Costa. Avenida Interlagos, 871/44 - Bloco 11 - São Paulo (SP) - 04661-100 - Brazil - E-mail: [email protected]
Comitê de Ética em Pesquisa: Registro CEP-UNISA No 82/10.
RESUMOObjetivo: Avaliar a relação entre o alinhamento postural da cabeça e a possível interferência na visão de crianças. Métodos: Foram avaliadas 11 crianças, entre 2 e 7 anos de idade de ambos os sexos, com o diagnóstico de deficiência visual, que apresentavam nistagmo e posição de bloqueio de cabeça. O teste Lea Grating Acuity Test® foi utilizado para coletar medidas de acuidade visual. Este aplicado em dois momentos: sem e com o alinhamento postural da cabeça. Para confiabilidade do alinhamento postural da cabeça, as inclinações foram medidas pelo software Fisiologic®. Resultados: As crianças apresentaram pior desempenho após o alinhamento postural fisiológico. Este pior desempenho é possível devido à perda da posição de bloqueio do nistagmo para ganho do alinhamento postural, dito como ideal. Foram observadas compensações posturais e maior esforço visual. Conclusão: A busca do alinhamento postural tradicional prejudica a resposta visual de criança com deficiência visual.
Descritores: Postura; Cabeça; Transtornos da motilidade ocular; Nistagmo fisiológico; Acuidade visual
ABSTRACTPurpose: Evaluate the relationship between the postural alignment of the head and possible interference in the view of children.Methods: We evaluated 11 children between 2 and 7 years of age of both sexes, with the visually impaired, who had nystagmus and head lock position. The test Lea Grating Acuity Test® was used to collect measurements of visual acuity. This applied on two occasions: with and without postural alignment of the head. For reliability of the postural alignment of the head, the slopes were measured by Fisiologic® software. Results: The children had a poorer performance after physiological postural align-ment. This poor performance is possible due to loss of position lock nystagmus to gain postural alignment, said to be ideal. Postural compensations were observed, and sharply increased eyestrain. Conclusion: The pursuit of traditional postural alignment affect the visual response of children with visual impairments.
Keywords: Posture; Head; Ocular motility disorders; Nystagmus, physiologic; Visual acuity

Costa ACRV, et al.
9Arq Bras Oftalmol. 2014;77(1):8-11
There is no scientific evidence that the correct postural alignment of the head in children with nystagmus can improve visual acuity. Most physical therapists believe that the alignment of the head in a position perpendicular to the ground is more important than the compensatory null position adopted by children with nystagmus. Professionals who specialize in visual impairment believe that reco-vered vision can improve the child’s functional performance, conse-quently improving the quality of life(12).
MeTHODSThis prospective, cross-sectional study was conducted between
May and November 2010 at the Department of Ophthalmology of the Federal University of São Paulo, Sector of Low Vision and Visual Rehabilitation–Outpatient clinic for Early Visual Stimulation, in colla-boration with the University of Santo Amaro.
Eleven male and female children with nystagmus and null head positions were evaluated. The subjects were aged between 2 and 7 years (mean 4.3 ± 1.4), did not exhibit delayed neuropsychomotor development and/or other associated systemic diseases. In addition, some had developed the ability to speak and could maintain the standing position required to perform the Lea Grating Acuity Test®.
The psychophysical Lea Grating Acuity Test® Model 251300 (Figure 1) was used. In this test, the child detects and directs the gaze toward discs with or without a high visual contrast. The equipment includes four discs with plain gray color on one side and black and white pa-rallel lines on the other, which had the following spatial frequencies: 0.5 cycle per degree of visual angle (cpd), 2 cpd, 4 cpd, and 8 cpd. The discs are 20 cm in diameter and both the patterned and the gray side are shown simultaneously to the children. The aim of the test is to determine the number of discs the child is able to identify(13). The assessment of visual acuity and head posture was performed on the same day and on two separate occasions, with and without the correct postural alignment of the head.
Children stood 30 cm away from the plumb line, with the ear lo-bes and the right and left acromion visible. The discs were maintained at a distance of 50 cm from the child. The camera was placed on a tripod, at a height of 80 cm and a distance of 80 cm from the plumb line, for the recording of measurements (Figure 2). Using the anterior view, we recorded the head position that blocked nystagmus and the subsequent inclination angles of the head during the performance of the Lea Grating Acuity Test®.
The test was performed on a second occasion, after postural alig n ment of the head (by vertically aligning the child’s head); the head posture was aligned manually by the physical therapist and the child’s caregiver, and the distance parameters applied were the same as those used during the test performed without the correct postural alignment of the head.
For quantitative analysis of the head posture, the images were analy zed using the Fisiologic® software; the highlighted points were defined and the angles formed between the anatomical points on the trunk and the vertical position of the head were recorded for comparison between the two test situations, and therefore impro-ving data validity (Figure 3).
ReSULTSThree of the 11 children detected all four discs in the nystagmus
null position. However, these children detected only two discs after the correct postural alignment of the head. In addition, three children detected three discs in the nystagmus null position, but only one disc after the correct postural alignment of the head.
Figure 1. Lea Grating Acuity Test® Model 251300(13).
Figure 2. Scheme of the positioning of the equipment and measurements for test pre sentation.
Figure 3. Example of evaluation and variability of postural alignment.

Influence of head posture on the visual acuity of children with nystagmus
10 Arq Bras Oftalmol. 2014;77(1):8-11
Three children detected three discs in the null position and later detected only two discs after the correct postural alignment of the head.
Two children detected the same number of discs in the nystag-mus null position and following the postural alignment of the head. One child detected all four discs in both head postures and another detected two discs in both postures.
These data were used to determine the ideal head posture to be adopted during rehabilitation treatment. According to the results ob-tained, the children had worse performance after the correct postural alignment of the head, as shown in graph 1.
Table 1 shows the number of discs detected per child in the null position and in the correct postural alignment of the head. There was a significant difference between the two conditions, with a Z score of -2.76 and a p value of 0.006* (p<0.05), indicating that the children detected more discs in the null position than in the correct postural alignment of the head.
Table 2 shows the variations in postural alignment the head and scapular waist in both conditions. Six children exhibited significantly poorer alignment of the scapular waist after postural alignment of the head. Five children exhibited improved alignment of the scapular waist following postural alignment of the head. Notably, alignment improvement was subtle in most children.
DISCUSSIOnSeveral studies on nystagmus and visual acuity(5-9,14-17) and head
posture(7,11,18) have been conducted. However, the relationship be-tween head posture and visual acuity has not been fully explored(7-9,11).
The alignment of head posture in children with nystagmus grea-tly influences visual acuity. In the nystagmus null position, ocular mo-vements are blocked or minimized, allowing the object to be directly focused on the foveal center, consequently improving visual acuity. In the correct postural alignment of the head, nystagmus is neither blocked nor minimized, resulting in an increase in the frequency and amplitude of ocular movement, leading to lower visual acuity(5-7,10).
According to the results obtained in this study, nine children de-tected more discs in the nystagmus null position than in the aligned head posture. This better performance is probably the result of image fixation at the foveal center for a longer period in the null position, thereby promoting better visual acuity(6).
On the other hand, in the correct postural alignment of the head, images are not directed to the foveal center, resulting in low visual acuity(6,7). We observed that the nystagmus worsened in seven chil-dren under these conditions.
Two children could detect the same number of discs in both head pos tures; however, during the test, one of the children made a greater effort to focus on the discs, with increased eyelid aperture.
Vision was compromised in most children when the scapular waist was compensated. Therefore, physiological postural alignment of the head through traditional physical therapy not only hinders visual performance but also causes skeletal muscle compensation in more stable areas of the body (e.g., the scapular waist), considering that the head is part of the axial skeleton, although very mobile.
Conditions such as neck deformities by muscle shortening can occur over time, through sustained null position for long periods. In su ch situations, the term torticollis is more appropriate; however, it is a consequence and not the cause of the null position(11).
Several surgical procedures are available for nystagmus treat ment, with a view for eliminating the abnormal head posture. If nys tag mus is accompanied with strabismus, surgery should simultaneously correct both the abnormal head posture and ocular deviation. We believe that surgical procedures intended to maintain the rotation angle of the head between the postural deviation of the head and the null area, can both eliminate the incorrect head posture and restore visual acuity at the correct ocular position(8,9).
Other treatment options for nystagmus include injections of bo tulinum toxin in the extraocular muscles or the retrobulbar space. Moreover, electro-optical devices are currently being developed as a no ninvasive method to eliminate the visual consequences of nys-tagmus. In this sense, the subject looks through a telescope associa-ted with a sensor that detects ocular movements. The sensor sends a signal to a servomotor that moves the telescope lenses and thereby
Table 2. Description of the variation in postural alignment of the head and nystagmus null position
Child
Head tilt Scapular waist
null position Aligned position null position Aligned position
01 -6.4° -2.7° -5.4° 0.2°
02 -6.1° 3.4° -5.5° -3.2°
03 15.6° -3.3° -3.1° -5.0°
04 3.9° -2.0° -6.6° -11.7°
05 -13.0° -2.9° 0.5° -8.9°
06 -17.9° -1.8° -5.4° 5.2°
07 16.7° 1.3° 8.2° 0.8°
08 5.6° -2.8° -4.5° -3.6°
09 3.9° -0.9° -12.2° -7.3°
10 4.2° -0.5° -5.3° -9.0°
11 -4.6° 0.0° 12.7° -6.7°
Table 1. Results of the Lea Grating Acuity Test® in two situations: null position and head alignment
Children null position Aligned position*
01 4 2
02 4 2
03 4 4
04 3 2
05 3 1
06 4 2
07 3 1
08 3 1
09 2 2
10 3 2
11 3 2
Graph 1. Representation of the visual performance on the two occasions: null and aligned positions.
Costa ACRV, et al.
11Arq Bras Oftalmol. 2014;77(1):8-11
abolishes the visual limitation of nystagmus. However, such electro- optical devices are not yet commercially available(9).
Families of children with nystagmus should be advised to find outpatient care centers specializing in low vision to correct the null position, which interferes with child development, and to prevent the impairment of visual performance. Therefore, specialists in visual impairment should manage both head posture conditions to ensure that the child is not adversely affected.
In the opinion of physical therapists specialized in visual impair-ment, a better visual acuity leads to improved functional performan-ce of the child, consequently providing an improved quality of life(12). In this study, we suggest that visual performance should be contem-plated in the rehabilitation of children with visual impairment with an aim to assess better head postures and to avoid the adoption of a stable head posture, thereby preventing muscle shortening and body compensations and improving visual acuity.
COnCLUSIOnThis study assessed the influence of the postural alignment of the
head on visual acuity in children with nystagmus. We observed that postural alignment of the head had a positive effect on the control of nystagmus. On the other hand, the physiological alignment in children with nystagmus did not result in good visual performance.
ReFeRenCeS 1. Padula WV, Spungin SS. A criança visualmente incapacitada, do nascimento até a idade
pré-escolar: a importância da estimulação visual. Rev Benjamin Constant. 2000;6(16):10-3. 2. Bower TG. The visual world of infants. Sci Am. 1966;215(6):80-92. 3. Kanski JJ. Oftalmologia Clínica: uma abordagem sistemática. 6a ed. Rio de Janeiro:
Elsevier; 2008.
4. Bicas HE. Acuidade visual: medidas e notações. Arq Bras Oftalmol. 2002;65(3):375-84. 5. Weiss HA, Kelly PJ. Acuity development in infantile nystagmus. Invest Ophthalmol Vis
Sci. 2007;48(9):4093-9. 6. Vaunghan D, Asbury T, Riodan-Eva P. Oftalmologia Geral. 15a ed. São Paulo: Atheneu;
2008. 7. Caovilla HH, Ganança MM, Munhoz MS, Silva MG, Frazza MM. O equilíbrio corporal e
os seus distúrbios. Parte I: noções de neuroanatomofisiologia do sistema vestibular. Rev Bras Med Otorrinolaringol. 1997;4(1):11-9.
8. Wang P, Lou L, Song L. Design and efficacy of surgery for horizontal idiopathic nys-tagmus with abnormal head posture and strabismus. J Huazhong Univ Sci Technolog Med Sci. 2011;31(5):678-81.
9. Thurtell MJ, Leigh RJ. Treatment of nystagmus. Curr Treat Options Neurol. 2012; 14(1):60-72.
10. Cullom DR, Chang B. Manual das doenças oculares “Wills Eye Hospital”: diagnóstico e tratamento no consultório e na emergência. 2a ed. Rio de Janeiro: Cultura Médica; 1998.
11. Bicas HE. Torcicolo posição viciosa de cabeça. Medicina (Ribeirão Preto). 2000; 33(1):64-72.
12. Lopes MC, Salomão SR, Berezovsky A, Tartarella MB. [Assessing vision-related qua-lity of life in children with bilateral congenital cataracts]. Arq Bras Oftalmol. 2009; 72(4):467-80. Portuguese.
13. Hyvarinen L. Instruções para o Sistema de Testes Lea. Helsinki, Finland; Goog-Lite; 2012 [cited 2012 Oct 20]. Available from: http://www.lea-test.fi
14. Felius J. Fu VL, Birch EE, Hertle RW, Jost RM, Subramanian V. Quantifying nystagmus in infants and young children: relation between foveation and visual acuity deficit. Invest Ophthalmol Vis Sci. 2011;52(12):8724-31.
15. Han SB, Yang HK, Hyon JK, Seo JM, Lee JH, Lee IB, et al. Efficacy of a computerized optokinetic nystagmus test in prediction of visual acuity of better than 20/200. Invest Ophthalmol Vis Sci. 2011;52(10):7492-7.
16. Han SB, Han ER, Hyon JY, Seo JM, Lee JH, Hwang JM. Measurement of distance ob-jective visual acuity with the computerized optokinetic nystagmus test in patients with ocular diseases. Graefes Arch Clin Exp Ophthalmol. 2011;249(9):1379-85.
17. Weiss AH, Kelly JP, Phillips JO. Relationship of slow-phase velocity to visual acuity in infantile nystagmus associated with albinism. J AAPOS. 2011;15(1):33-9. Comment in: J AAPOS. 2011;15(1):1-2.
18. Bunnell WP. Selective screening for scoliosis. Clin Orthop Relat Res. 2005;(434):40-5.
39o Congresso da Associação Paranaense de Oftalmologia
22 a 25 de maio de 2014Centro de Eventos
Londrina - PR
informações: Site: www.congressoapo.com.br

12 Arq Bras Oftalmol. 2014;77(1):12-6
Original Article
InTRODUCTIOnA cataract is characterized by clouding that develops in the crys-
talline lens of the eye or its envelope and varies from a slight to a complete opacity that can obstruct the passage of light. Cataracts are specifically defined as any opacification in one or more layers of the crystalline lens that diffracts light and causes impaired vision(1). Cata-ract is the main cause of curable blindness and represents a public health problem that negatively affects patient quality of life(2,3). The blindness caused by cataract incapacitates the individual, increases dependency, decreases the patient’s social condition, and results in early professional retirement(4). Vision recovery facilitated by cataract
surgery results in social and economic benefits to the individual, their family, and the community as a whole(5,6).
In the United States, approximately 1.5 million individuals undergo surgery for cataracts every year(7). According to the Brazilian Council of Ophthalmology (CBO), approximately 2% of the Brazilian population aged 60 years is affected by impaired vision due to cataracts(8).
Assessing the quality of life after public health procedures is important. In the field of ophthalmology, maximum emphasis is pla ced on visual improvement in patients who have undergone ca-taract surgery using instruments for measuring the quality of life and visual function. Packer et al.(9) described the term visual function as
Life quality assessment of patients after phacoemulsification or extracapsular cataract extractionAvaliação da qualidade de vida de pacientes submetidos à facoemulsificação ou extração extracapsular de catarata
paula Teixeira de Mendonça1, leonardo Teixeira de Mendonça2, alexandre anTônio MarqueS roSa2, luiz carloS de liMa Silveira3
Submitted for publication: October 23, 2012 Accepted for publication: October 9, 2013
Study carried out at Universidade Federal do Pará.1 Hospital Universitário Bettina Ferro de Souza, Universidade Federal do Pará, Belém (PA), Brazil.2 Faculdade de Medicina, Instituto de Ciências da Saúde, Universidade Federal do Pará, Belém (PA),
Brazil.3 Núcleo de Medicina Tropical, Universidade Federal do Pará, Belém (PA), Brazil.
Funding: This study was supported by the following grants: FINEP IBN-Net; CNPq-PRONEX/FAPESPA #2268 and 316799/2009; and CNPq #620248/2006-8, #620037/2008-3, and 476744/2009-1. LCLS is a CNPq research fellow.
Disclosure of potential conflicts of interest: P.T. Mendonça, None; L.T. Mendonça, None; A.A.M. Rosa, None; L.C.L. Silveira, None.
Correspondence address: Luiz Carlos de Lima Silveira. Núcleo de Medicina Tropical. Av. Genera-líssimo Deodoro, 92 (Umarizal), 66055-240 - Belém (PA) - 66055-240 - Brazil
E-mail: [email protected]
ABSTRACTPurpose: To study the quality of life, treatment outcomes, and satisfaction in pa-tients who have undergone cataract surgeryMethods: This comparative case series study was conducted at the Ophthalmo-logy Service of the Bettina Ferro de Souza University Hospital, Belém, Pará, Brazil. Totally, 60 patients with cataract were included; 50% underwent conventional extracapsular cataract extraction (ECEE) and 50% underwent cataract extraction by phacoemulsification (PHACO). Patients were interviewed using the Visual Function 14 (VF-14) questionnaire to determine the quality of life before and 30 days after surgery. The results of ophthalmological examination were recorded in the patients’ files and were available throughout this study. One-way ANOVA, Tukey’s post-hoc comparison, and the sign test were used for statistical analyses.Results: The mean VF-14 satisfaction index was 38.0 and 89.4 before and after surgery, respectively, for the ECEE group and 47.0 and 94.1, respectively, for the PHACO group. The improvement in patient quality of life after surgery was significant in both groups (p<0.0001), with a similar amount of improvement in both groups.Conclusions: The observed improvement in quality of life was significant (p<0.0001) and directly related to patient satisfaction with surgical outcomes, which was also significant (p<0.0001) as assessed using the VF-14. Satisfaction and quality of life are individual factors; consequently, patient responses to questions regarding improvements in the ability to perform each activity are subjective and depend uniquely on individual perception.
Keywords: Cataract; Cataract extraction; Quality of life; VF-14 questionnaire; Eye surgery
RESUMOObjetivo: Estudar a qualidade de vida, resultados e satisfação em pacientes que se submeteram à cirurgia de catarata.Métodos: O trabalho foi realizado no Serviço de Oftalmologia do Hospital Universi-tário Bettina Ferro de Souza, Belém, Pará, Brasil. O desenho experimental consistiu em séries de casos comparados. O estudo incluiu 60 indivíduos com catarata. Metade dos pacientes foi submetida à extração de catarata extracapsular convencional (ECEE) e a outra metade à extração de catarata por facoemulsificação (PHACO). Os pacientes foram entrevistados usando-se o questionário Visual Function 14 (VF-14) para deter-minar a qualidade de vida antes e 30 dias depois da cirurgia. Os resultados do exame oftalmológico foram registrados no arquivo de cada paciente e disponibilizados ao longo do trabalho. Foram usados análise de variância simples e comparação post-hoc com teste de Tukey e teste dos sinais para a análise estatística dos resultados.Resultados: O índice de satisfação médio VF-14 foi 38,0 e 89,4 antes e após a cirurgia, respectivamente, para o grupo ECEE, sendo 47,0 e 94,1 para o grupo PHACO. A melhora na qualidade de vida após a cirurgia foi significativa em ambos os grupos de pacientes (p<0,0001), tendo sido semelhante em ambos os grupos.Conclusão: A melhora observada na qualidade de vida avaliada foi significativa e diretamente relacionada à satisfação dos pacientes com os resultados da cirurgia, a qual também foi significativa (p<0,0001). A satisfação e a qualidade de vida são fatores individuais. Consequentemente, as respostas dos pacientes relativas à melhoria em cada atividade são subjetivas e dependem unicamente da percepção individual.
Descritores: Catarata; Extração de catarata; Qualidade de vida; Questionário VF-14; Cirurgia dos olhos

Mendonça PT, et al.
13Arq Bras Oftalmol. 2014;77(1):12-6
the impact of vision on the quality of life or the capacity to realize everyday activities directly related to visual usefulness(9). Quality of life has different aspects, and because health is not only defined as the lack of disease but also as physical, mental, and social welfare, the term quality of life is considered more often(10,11).
Developed in the United States, the Visual Function 14 (VF-14) questionnaire measures functional capacity related to the vision of patients who have undergone cataract surgery. The VF-14 is based on 14 daily activities that can be affected by ocular diseases. Implanta-tion of an intraocular lens (IOL) is currently one of the most common surgical procedures for cataracts because of the benefits to pa-tients(12,13). The techniques used in cataract surgery are extracapsular cataract extraction (ECEE) and phacoemulsification (PHACO)(14). PHACO is currently the most used technique in the majority of developed countries because of the fast visual recovery and decreased pre- and postsurgical complications(15). The present study aimed to evaluate the quality of life, treatment outcomes, and satisfaction in patients who underwent cataract surgery in Belém, State of Pará, Brazil.
MeTHODSThe present study is an interventionist study performed at the
University Hospital Bettina Franco de Souza (HUBFS). The patients sig-ned a written informed consent form, and the research was approved by the Committee of Ethics and Research with Human Beings of the Núcleo de Medicina Tropical da Universidade Federal do Pará under number 005/2007-CEP/NMT. All the rules of resolution 196/1996 of the National Council of Health were followed. The study was com-pliant with the Declaration of Helsinki for studies involving humans.
Sixty individuals with senile cataract indicated for surgery and attended to at the Ophthalmology Service of the HUBFS were se-lected. The patients were divided into 2 groups; 30 underwent ECEE and 30 underwent PHACO. All surgeries were performed by the same surgeon.
Patients completed the VF-14 in the waiting room of the Ophthal-mology ambulatory clinic of the HUBFS or in one of the patient assis-tance offices. A similar questionnaire was administered to patients in a population study of corneal transplantation in Brazil(16). The VF-14 comprises 14 questions, each of which can have 5 answers (0 = im-possible to realize, 1 = intense difficulty, 2 = moderate difficulty, 3 = minimal difficulty, 4 = without difficulty). The corresponding number is multiplied by 25 to obtain the final score, which varies from 0 (worst index of visual function) to 100 (best index of visual function)(17).
To characterize the sample, the following variables were se-lected: sex, age, schooling, occupation, and visual acuity. Quality of life variables included physical domains (near vision and far vision) and the level of independence (daily activities, social activities, physical activities, and capacity to drive an automobile). Visual acuity is presented as logMAR (Snellen equivalent). The results of the questionnaire before and after surgery were compared, taking into consideration evident improvements in the ability to perform daily tasks after surgery as reported by the patients, using ANOVA and the sign test.
ReSULTSThe average age of the study population was 68 ± 8.4 years (mean
± standard deviation) in the PHACO group and 67 ± 8.0 years in the ECEE group. With regard to schooling, 16 patients (53.3%) in the PHACO group had completed primary and secondary school, 8 (26.7%) had completed high school, 4 (13.3%) had a college degree, and 2 (6.7%) had no school background. In the ECEE group, 24 patients (80%) had completed primary and secondary school, 3 (10%) had received high school level education, and 3 (10%) had no schooling background.
With regard to occupation, 7 patients (23.3%) in the ECEE group worked in rural areas and 7 (23.3%) patients were maids. In the PHACO
group, 8 patients (26.7%) were maids and 6 patients (20%) were reti-red. The average VF-14 score was 47.0 before and 94.1 after PHACO, while it was 38.0 before and 89.4 after ECEE. Significant differences were found between the averages calculated before and after sur-gery in both groups (Figures 1 and 2).
The visual acuity before surgery was considerably low, mainly in patients who underwent ECEE, 30% of whom had an visual acuity of 1.2 logMAR (20/400). The acuities of patients in the PHACO group varied greatly before surgery, with a predominant acuity of 0.6 (20/80) in 26.7% patients. After surgery, an improvement was observed in 83.3% patients, with an acuity of >0.3 logMAR (20/40). A number of ECEE
Figure 1. Average VF-14 score per question before and after surgery among patients who underwent extracapsular cataract extraction.
Figure 2. Average VF-14 score per question before and after surgery among patients who underwent phacoemulsification.

Life quality assessment of patients after phacoemulsification or extracapsular cataract extraction
14 Arq Bras Oftalmol. 2014;77(1):12-6
patients had a visual acuity of 0.0 logMAR (20/20), corresponding to 43.3% of the total sample (Table 1).
With regard to satisfaction, graphic analysis using the sign test (Figures 3 and 4) and ANOVA revealed significant satisfaction in both surgical groups (p<0.0001), which resulted in an improved quality of life (Figures 5 and 6).
DISCUSSIOnIn a study by McKee et al.(18), the average patient age was 75 years
for men and 77 years for women. In the present study, the proportion of patients aged 61-70 years was high at 36.7% and 43.3% in the PHACO and ECEE groups, respectively, probably because patients visit ophthalmological centers earlier because of the lack of visual function or increased awareness about cataracts and their surgical treatment.
With regard to patient occupations, we found no data in the literature. However, although the majority of patients were elderly, 77% were still working, increasing the importance of vision recovery for the continuity of professional activities. The high proportion of working patients reflects the reality of the studied population that, despite being of retirement age, still needed to work to make a living.
Twenty-two (37%) of the 60 patients presented with a postsur-gical visual acuity of 0.0 (20/20), indicating a total recovery of visual acuity. Nevertheless, 27% patients (n = 16) had a visual acuity of <0.7 (20/100). Norregaard et al. considered 0.3 to be the optimal visual acuity after surgery(19). We can conclude that a significant proportion of patients did not achieve the desired acuity. However, on the basis of the results obtained in the visual function test, even though the visual acuity of some patients remained low, surgery clearly enabled them to perform daily activities. Therefore, the association of both methods, objective and subjective, is important to the final evalua-tion of surgical outcomes.
After surgery, considerable improvement was observed in the ability to perform all activities, with an improvement of approxima-tely 40 points for each activity. Some activities such as reading the
Table 1. Patient visual acuity before and after cataract surgery accor-ding to surgical procedure
Visual acuity Phacoemulsificationextracapsular
extraction
Snellen logMAR (n) % (n) %
Beforesurgery
<20/400 >1.3 5 16.7 9 30.0
20/400 >1.3 3 10.0 7 23.3
20/200 >1.0 6 20.0 4 13.3
20/125 >0.8 1 03.3 0 0
20/100 >0.7 7 23.3 8 26.7
20/80 >0.6 8 26.7 2 06.7
Total 30 100 30 100
Aftersurgery
20/20 0 9 30.0 13 43.3
20/25 0.10 6 20.0 02 06.7
20/30 0.20 7 23.3 02 06.7
20/40 0.30 3 10.0 05 16.7
20/50 0.40 0 0 02 06.7
20/60 0.50 3 10.0 01 03.3
20/70 0.55 0 0 02 06.7
20/100 0.70 2 06.7 03 10.0
Total 30 100 30 100
Figure 3. Satisfaction analysis using the sign test among patients who underwent extracapsular cataract extraction. Horizontal bars represent the median, first, and third quartiles. Vertical bars represent the standard deviation from the mean.
Figure 4. Satisfaction analysis among patients who underwent phacoemulsification. Ho-rizontal bars represent the median, first, and third quartiles. Vertical bars represent the standard deviation from the mean.
newspaper and reading small print still remained below the 95 points set by Norregaard et al.(19), even with the significant improvement in outcome. In that previous study, a VF-14 score of 95 was used as an indicator of success or optimum visual function after surgery.
The results obtained before and after surgery are of great im-portance in complementing the current literature. In the study by Friedman et al.(20), approximately 50% patients interviewed before surgery reported difficulty or inability to drive at night or read small print, consistent with the major difficulties reported by patients in the present study.
Friedman et al. disagreed with some questions included in the VF-14 that inform little about the functional status of most patients(20). For example, 4 out of 5 patients did not practice sports, indicating that this issue did not contribute to the VF-14 score. A similar situation was observed in the current study, not only with practicing sports but also with car driving and playing games such as dominoes and cards. Therefore, the test should be adapted to activities related to the culture of each region, with an increased focus on the elderly.
In general, the average VF-14 score among patients who under-went PHACO was 47 points before and 94.1 points after surgery, indicating an improvement of 47.1 points. In the ECEE group, the ave-rage VF-14 score was 38 points before and 89.4 points after surgery, indicating an improvement of 51.4 points. These results are similar to those of other studies in which the average VF-14 score was 82.6 before and 94.8 after surgery(18).

Mendonça PT, et al.
15Arq Bras Oftalmol. 2014;77(1):12-6
The results after surgery were like other results observed around the world. Several conclusions concerning patients who used the service in the city of Belém can be made. First, patients who visited the service usually had poor visual function; the difficulties these patients faced in everyday life were so grave that they preferred sur-gical correction. In developed countries, patients with an average of more than 70 points before surgery usually do not exhibit an obvious improvement after surgery, which directly influences patient satisfac-tion with the surgical outcome.
The visual acuity of patients demonstrated a good improvement after surgery. Reading the newspaper, performing manual tasks, reading at night, and reading texts with small letters were the daily activities that most often impaired the existence of the cataract. Acti-vities such as playing games (cards, dominoes, etc.), practicing sports, and driving were associated with low scores in the satisfaction and quality of life analysis of patients; 75% patients did not play games,
68% did not practice sports, and 87% did not drive. However, after surgery, a considerable improvement was observed in the ability to perform all these activities.
The observed improvement in the quality of life was significant (p<0.0001) and directly related to patient satisfaction with surgical outcomes, which was also significant (p<0.0001), as assesse using the VF-14. Satisfaction and quality of life are individual factors; con-sequently, patient responses to questions regarding improvements in the ability to perform each activity are subjective and depend uniquely on individual perception.
COnCLUSIOnSWhat is knoWn
Developed in the United States, the VF-14 questionnaire measu-res functional capacity related to the vision of patients who have un-
Figure 5. Satisfaction analysis among patients who underwent extracapsular cataract extraction. Improved quality of life was observed (ANOVA, p<0.0001).
Figure 6. Satisfaction analysis among patients who underwent phacoemulsification. Improved quality of life was observed (ANOVA, p<0.0001).

Life quality assessment of patients after phacoemulsification or extracapsular cataract extraction
16 Arq Bras Oftalmol. 2014;77(1):12-6
dergone cataract surgery. The VF-14 is based on 14 daily activities that can be affected by ocular diseases. Implantation of an IOL is currently one of the most common surgical procedures for cataract because of the benefits to patients. The techniques used in cataract surgery are ECEE and PHACO, the latter being the most used technique in the majority of developed countries because of the fast visual recovery and decreased pre- and postsurgical complications. The VF-14 has been widely used, particularly in advanced countries, and has vali-dated the use of both ECEE and PHACO; however, it determines that PHACO results in the best outcome in terms of patient quality of life. No other study has evaluated the outcomes of ECEE and PHACO in cataract patients living in remote areas such as the Amazon region.
What this paper adds
The VF-14 was used, for the first time as per our knowledge, to evaluate patients in the Amazon Region and validated the use of both ECEE and PHACO as surgical procedures that considerably improve the quality of life of patients after surgery. The observed improve-ment in quality of life was significant and directly related to patient satisfaction with surgical outcomes, which was also significant, as assessed using the VF-14. Satisfaction and quality of life are individual factors; consequently, patient responses to questions about impro-vements in the ability to perform each activity are subjective and depend uniquely on individual perception.
ACKnOWLeDGeMenTSThis research was supported by the following grants: FINEP IBN-Net;
CNPq-PRONEX/FAPESPA #2268 and 316799/2009; CNPq #620248/2006-8, #620037/2008-3, and 476744/2009-1. LCLS is a CNPq research fellow.
ReFeRenCeS 1. Ferraz EVAP, Lima CA, Cella W, Arieta CEL. Adaptação de questionário de avaliação da
qualidade de vida e percepção relativa à doença, aplicado a indivíduos portadores de catarata senil. Arq Bras Oftalmol. 2002;65:293-8.
2. Michon JJ, Lau J, Chan WS, Ellwein LB. Prevalence of visual impairment, blindness, and cataract surgery in the Hong Kong elderly. Br J Ophthalmol. 2002;86:133-9.
3. Nirmalan PK, Thulasiraj RD, Maneksha V, Rahmathullah R, Ramakrishnan R, Padma-
vathi A, Munoz SR, Ellwein LB. A population based eye survey of older adults in Tirunelveli district of South India: blindness, cataract surgery, and visual outcomes. Br J Ophthalmol. 2002;86:505-12.
4. Alves MR, Kara-José N. Catarata: um problema de saúde pública. In: Kara-Jose N, Delgado AMN, Arieta CEL, Rodrigues MLV, Alves MR (eds.). Prevenção da Cegueira por Catarata. Campinas, São Paulo, Brazil: UNICAMP, 1996; p.11-18.
5. Kara-José N, Barbosa E, Fonseca-Neto JC, Oura MH, Martins WH. Considerações sobre aspectos sociais do atendimento clínico e cirúrgico de pacientes portadores de ca-tarata senil. Arq Brasil Oftalmol. 1982;45:115-8.
6. Temporini ER, Kara-Júnior N, Holzchuh N, Kara-José N. Popular beliefs regarding the treatment of senile cataract. Rev Saúde Pública. 2002;36:343-9.
7. Hammond CJ, Duncan DD, Snieder H, de Lange M, West SK, Spector TD, Gilbert CE. The heritability of age-related cortical cataract: the twin eye study. Invest Ophthalmol Vis Sci. 2001;42-3:601-5.
8. Mello PAA, Araújo Filho A. Atualização na cirurgia da catarata. Rev Bras Med. 1993;50: 92-132.
9. Packer M, Fine IH, Hoffman RS. Functional vision, contrast sensitivity, and optical aberrations. Int Ophthalmol Clin. 2003;43:1-3.
10. Gill TM, Feinstein AR. A critical appraisal of the quality of life. JAMA 1994; 272:619-26. 11. Testa MA, Simonson DC. Assessment of quality of life outcomes. N Engl Med J. 1996;
334:835-40. 12. Ohrloff C, Zubcov AA. Comparasion of phacoemulsification and planned extracap-
sular extraction. Ophthalmologica. 1997;211:8-12. 13. Leinoken J, Laatikainen L. Changes in visual acuity of patients undergoing cataract
surgery during the last two decades. Acta Ophthalmol Scand. 2002;80:506-11. 14. Kara-José Júnior N, Avakian A, Lower LMT, Rocha AM, Cursino M, Alves RM. Facoe-
mulsificação versus extração extracapsular manual do cristalino: análise de custos. Arq Brasil Oftalmol. 2004;67:481-9.
15. Leaming DV. Practice styles and preferences of ASCRS members-1998 survey. J Cata-ract Refract Surgery. 1999;25:851-9.
16. Atique D, Goulart DG, Lake JC, Lima FA,Felberg S, Dantas MAN. Qualidade de vida após transplante penetrante de córnea. Arq Bras Oftalmol. 2002;65:371-4.
17. Alonso J, Espallargues M, Andersen TF, Cassard SD, Dunn E, Bernth-Petersen P et al. International applicability of the VF-14. An index of visual function in patients with cataracts. Ophthalmology. 1997;104:799-807.
18. Mckee M, Whatling JM, WilsonJ L and Owen AV. Comparing outcomes of cataract surgery: challenges and opportunities. J Public Health. 2005;27:348-52.
19. Norregaard JC, Petersen PB, Alonso J, Dunn E, Black C, Tavs Folmer Espallargues AM, Bellan L, Anderson GF. Variation in indications for cataract surgery in the United Sta tes, Denmark, Canada, and Spain: results from the International Cataract Surgery Out co-mes Study. Br J Ophthalmol. 1998;82:1107-11.
20. Friedman DS, Tielsch JM, Vitale S, Bass EB, Schein OD, Steinberg EP. VF-14 item specific responses in patients undergoing first eye cataract surgery: can the length of the VF-14 be reduced? Br J Ophthalmol. 2002;86:885-91.
17Arq Bras Oftalmol. 2014;77(1):17-20
Original Article
InTRODUCTIOnCorneal laser surgery is currently the most widely used surgical
method for correcting refractive errors. Measurement of the corneal curvature, thickness, and elevation are important for the preopera-tive assessment of patients requiring refractive surgery and for the diagnosis of corneal ectasias like keratoconus and pellucid marginal degeneration. Historically, a simple Placido-based corneal topography was considered the norm for screening the cornea for topographic anomalies. Currently, Scheimpflug and Placido systems are being used to provide information on the anterior and posterior corneal sur faces. Currently, 2 such systems are widely used: the Galilei Dual Scheimp flug Analyzer (Ziemer, SIS, Port, Switzerland) and the Pentacam (OCULUS Optikgeräte GmbH, Germany) single Scheimpflug analyzer.
The present study aims to evaluate the agreement in measure-ments obtained by these 2 systems. Previous studies have evaluated
the agreement between Scheimpflug devices; however, different best-fit sphere (BFS) diameters were used in both devices(1) or only elevation data were compared between the Dual Scheimpflug Ana -lyzer and a Scanning Slit-beam imaging system(2). Comparisons using different BFS would alter the elevation data obtained by the single Scheimpflug system (compared with the dual Scheimpflug system) because the reference is flatter. Now that the pre-set BFS diameter in the single Scheimpflug system is universally set to 8.0 mm, we attempted a comparison with equal BFS diameters in both systems. Our aim was not to demonstrate the superiority of one system over the other, but to discuss the similarities between both systems.
MeTHODSThis prospective, noninterventional, diagnostic study comprised
60 eyes of normal candidates for refractive surgery. Patients who had
Assessment of anterior and posterior corneal indices using two Scheimpflug analyzers Índices da córnea anterior e posterior com dois analisadores Scheimpflug
daoud charbel Fahd1, carole GeorGe cherFan1, claudia raad2, Marc aSouad2, Shady TanuS awwad1
Submitted for publication: August 2, 2013 Accepted for publication: August 26, 2013
Study carried out at Department of Ophthalmology in the American University of Beirut Medical Centre, Beirut, Lebanon. Presented in 2010 ASCRS meeting in Boston
1 Department of Ophthalmology in the American University of Beirut Medical Centre, Beirut, Lebanon.2 LaserVision Inc, Beirut, Lebanon.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: D.C. Fahd, None; C.G. Cherfan, None; C. Raad, None; M. Asouad, None; S.T. Awwad, None.
Correspondence address: Shady T. Awwad. Director of Laser and Refractive Surgery Division - De-partment of Ophthalmology - American University of Beirut Medical Centre, Beirut, Lebanon
E-mail: [email protected]
ABSTRACT Purpose: To assess the agreement between the elevation and curvature measu-rements of the anterior and posterior corneal surfaces obtained using the Gali-lei Dual Scheimpflug Analyzer and those obtained using the Pentacam single Scheim pflug system.Methods: This prospective, noninterventional, diagnostic study was conducted at the Department of Ophthalmology at the American University of Beirut (Medical Center) and included 60 eyes of 60 consecutive patients. Measurements were obtained using 2 different Scheimpflug analyzers (Galilei and Pentacam). The best-fit sphere was set at 8 mm in both machines. Pachymetry (CCT), anterior elevation (AE) and posterior elevation (PE), and curvature were assessed. Pearson’s correlation coefficients, comparison of means, and Bland-Altman plots were used to evaluate agreement between the 2 systems. Results: The average CCT (at the corneal apex) was 533 ± 35 μm and 532 ± 37 μm (p=0.980), the average central AE was 1.25 ± 3.95 μm and 2.29 ± 5.28 μm (p=0.964), and the average central PE was 4.19 ± 8.18 μm and 5.42 ± 14.05 (p=0.956) μm with the Galilei and Pentacam, respectively. Conclusion: The Scheimpflug analyzers correlated well in the assessment of pa -chymetry, elevation, and curvature.
Keywords: Cornea/pathology; Cornea/anatomy & histology; Corneal topography; Corneal pachymetry; Photography/instrumentation
RESUMO Objetivo: Avaliar a concordância entre as medidas de elevação e curvatura das superfícies anterior e posterior da córnea obtidos pelos analisadores de Scheimpflug Galilei e Pentacam. Método: Estudo de teste diagnóstico, prospectivo, não-intervencional realizado no Departamento de Oftalmologia do Centro Médico da Universidade Americana de Bei rute. Sessenta olhos de 60 pacientes consecutivos. As medições foram feitas usando dois analisadores Scheimpflug diferentes (Galilei e Pentacam). A esfera de melhor ajuste foi fixada em 8 mm para ambos equipamentos. Paquimetria (CCT ), elevação anterior (AE) e elevação posterior (PE), e curvatura foram avaliados. Coeficientes de correlação de Pearson, comparação das médias, e gráficos de Bland-Altman foram utilizados para avaliar a correlação. Resultados: A média de CCT (no ápice da córnea) foi 533 ± 35 μm usando o Galilei e 532 ± 37 μm usando o Pentacam (p=0,980). As médias centrais de AE foram de 1,25 ± 3,95 μm e 2,29 ± e 5,28 μm com o Galilei e Pentacam, respectivamente (p=0,964). As médias de centrais de PE foram 4,19 ± 8,18 μm e 5,42 ± 14,05 μm com a Galilei e Pentacam, respectivamente (p=0,956). Conclusões: Os analisadores de Scheimpflug avaliados correlacionam bem em termos de paquimetria, elevação e curvatura.
Descritores: Córnea/patologia; Córnea/anatomia e histologia; Topografia da córnea; paquimetria corneana; Fotografia/instrumentação.

Assessment of anterior and posterior corneal indices using two Scheimpflug analyzers
18 Arq Bras Oftalmol. 2014;77(1):17-20
undergone previous ocular surgeries, those with any systemic disea-se (including diabetes mellitus, connective tissue disease, hyperten-sion, and collagen vascular diseases), and/or those who had worn rigid contact lenses in the past 6 months were excluded. Soft contact lens wearers were asked to discontinue wearing their contact lenses for at least 14 days prior to measurements(3). The study received the approval of the Institutional Review Board of the American University of Beirut and complied with the Health Insurance Portability and Accountability Act (HIPAA) recommendations. Informed consent was obtained from all patients. All subjects underwent corneal topogra-phy using the Galilei (dual Scheimpflug system) followed by corneal topography using the Pentacam (single Scheimpflug system) by the same trained ophthalmic technician who was blinded to the study protocol.
pentacam (single scheimpflug system)The Pentacam system uses a single rotating Scheimpflug camera
(180°) and a monochromatic slit-light source [blue light-emitting diode (LED) at 475 nm] that rotate together around the optical axis of the eye to calculate a 3-dimensional (3D) model of the anterior segment. The 3D, high-resolution, cornea-scanning mode obtains 50 images of the eye in 1 second. Overall, 138,000 true elevation points were recorded.
galilei (dual scheimpflug system)The Galilei Dual Scheimpflug Analyzer uses two rotating
Scheimpflug cameras integrated with a Placido topographer. The light source is also monochromatic (blue LED at 475 nm). The 122,000 data points are analyzed per scan. The system used Scheimpflug images of all anterior segment structures (cornea, iris, pupil, anterior chamber, and lens) to evaluate and analyze the corneal shape and thickness, pupil size, and anterior chamber parameters (size, volume, and angle). The presence of two Scheimpflug camera devices that obtain images of the same part of the eye simultaneously decreases movement artifacts and increases image accuracy by superimposing the two images. The presence of the Placido improves the accuracy of calculation of the anterior corneal curvature.
measurement technique
Measurements were obtained in a semi-lit room. To standardize the tear film meniscus and account for tear film abnormalities that may influence Placido measurements, a drop of carboxymethyl ce llulose artificial tears was instilled in the fornix of each eye, and measurements were obtained 3 min later to ensure that the tear film meniscus was back to its normal thickness(4). Both eyes were measu-red. Measurements were obtained using an 8.0-mm diameter BFS, which was fitted in float. Central elevations and maximum/minimum elevations in the central 8 mm of the cornea were recorded with both the dual and single Scheimpflug systems. Pachymetry measurements were internally calculated by the individual machines by subtracting the anterior and posterior corneal elevations. In patients with a nor-mal topography, only one eye was considered for analysis (60 eyes of 60 patients). Data from the right eyes of the first, third, and fifth 10 patients and data from the left eyes of the second, fourth, and sixth 10 patients were used for further analysis.
intraclass correlation coefficients (iccs)For each system and for a defined subset of apparently healthy
eyes, measurements were obtained 3 times and the data were avera-ged. One eye of each subject was selected. Ten right eyes were selec-ted from the first 10 subjects and 10 left eyes were chosen from the second 10 subjects. The internal repeatability of each machine was analyzed by calculating the ICC, which was defined as the ratio of the between-subjects variance to the sum of the pooled within-subject variance and between-subjects variance. The ICC, which approached
1.0 when there was no variance between repeated measurements, was automatically calculated using PASW Statistics software (SPSS version 18.0, SPSS Inc. Chicago, IL, USA). The ICCs ranged from 0 to 1 and were commonly classified as follows: ICC <0.75, poor agreement; 0.75-<0.90, moderate agreement; and >0.90, high agreement(5).
statistical analysis
Statistical analysis was performed using the Statistical Program for Social Sciences v18.0 (SPSS v18.0, SPSS Inc. Chicago, IL, USA). A paired t-test was used to compare the instruments in each elevation parameter. Mean algebraic and mean absolute differences were calculated. Results are expressed as means ± standard deviations. In addition, Pearson’s correlation coefficients (PCCs) were calculated to assess the correlation between the anatomical parameters measured by each imaging technique. All tests were 2-tailed. A p-value of <0.05 was considered statistically significant. Bland-Altman plots were used to assess the interchangeability (agreement) of the 2 imaging systems for measuring elevation parameters. These plots show the differences between the methods plotted against the mean of the methods. They provided a graphical method to assess the presence of an agreement between the 2 clinical techniques.
ReSULTSpatient characteristics
Sixty eyes of 60 subjects (25 males, 35 females) were included in the study. The mean age of the participants was 27.0 ± 4.1 years. All eyes had a normal topography, with no evidence of curvature abnormalities.
machine characteristics
Each measurement was obtained 3 times, and only the findings with the highest quality (as determined by the machine) were inclu-ded for analysis. The ICC was calculated for each machine on the basis of 3 measurements. The ICC for the dual Scheimpflug system was as follows: 0.999 for pachymetry (CCT), 0.998 for SimK, 0.998 for anterior BFS, and 0.993 for posterior BFS. The ICC for the single Scheimpflug system was as follows: 0.994 for CCT, 0.986 for SimK, 0.996 for anterior BFS, and 0.991 for posterior BFS.
Pachymetry
Pachymetry measurements are summarized in table 1. The mean difference between the dual Scheimpflug and single Scheimpflug systems in central pachymetry measurements was 0.7 ± 8.2 µm. The mean absolute difference between the two machines in central pachy-metry measurements was 6.7 ± 4.6 µm. Figure 1 shows a Bland-Altman plot of central pachymetry. The dual Scheimpflug system exhibited a
Table 1. Correlation of pachymetry measurements between the dual Scheimpflug system (Galilei) and the single Scheimpflug system (Pentacam)
(μm)Galilei (μm)
Pentacam (μm)
Pearson’s correlation coefficient
Central pachymetry 535 ± 35 534 ± 37 0.977
Thinnest point 531 ± 37 528 ± 43 0.982
Superior 2 mm 574 ± 33 590 ± 33 0.864
Inferior 2 mm 568 ± 38 559 ± 43 0.949
Nasal 2 mm 578 ± 32 579 ± 34 0.897
Temporal 2 mm 549 ± 33 553 ± 34 0.904
Superior 3 mm 612 ± 35 649 ± 37 0.889
Inferior 3 mm 613 ± 35 613 ± 39 0.865
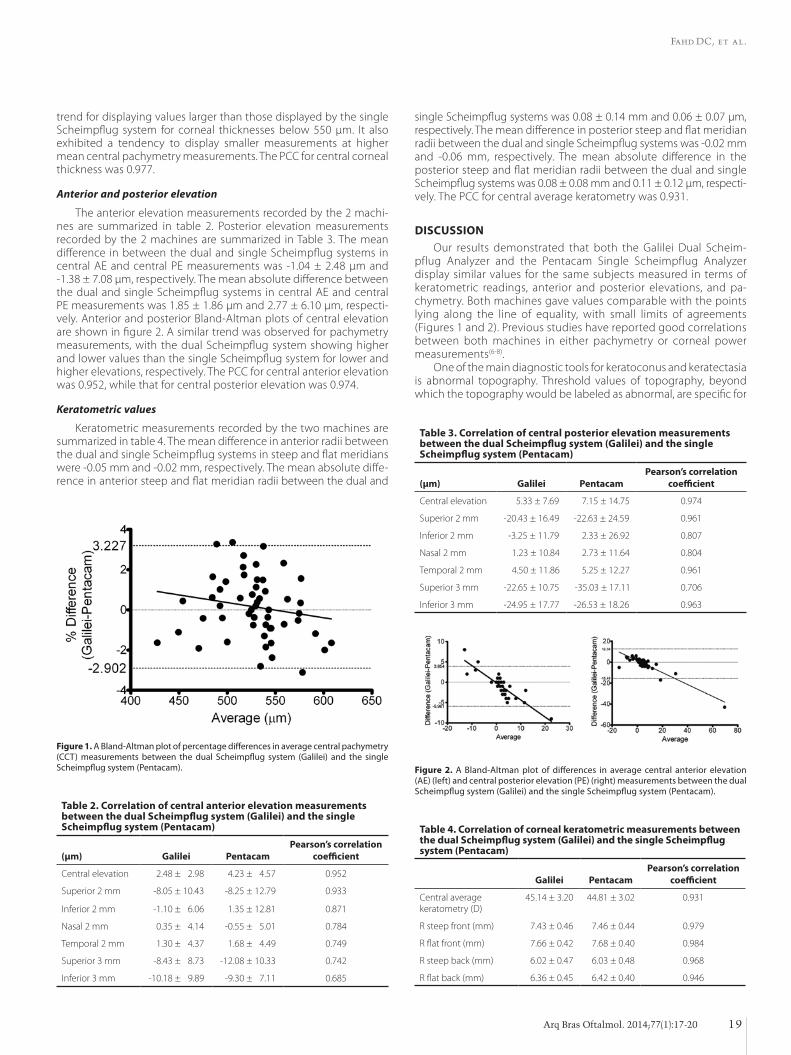
Fahd DC, et al.
19Arq Bras Oftalmol. 2014;77(1):17-20
trend for displaying values larger than those displayed by the single Scheimpflug system for corneal thicknesses below 550 μm. It also exhibited a tendency to display smaller measurements at higher mean central pachymetry measurements. The PCC for central corneal thi ckness was 0.977.
Anterior and posterior elevation
The anterior elevation measurements recorded by the 2 machi-nes are summarized in table 2. Posterior elevation measurements recorded by the 2 machines are summarized in Table 3. The mean difference in between the dual and single Scheimpflug systems in central AE and central PE measurements was -1.04 ± 2.48 µm and -1.38 ± 7.08 µm, respectively. The mean absolute difference between the dual and single Scheimpflug systems in central AE and central PE measurements was 1.85 ± 1.86 µm and 2.77 ± 6.10 µm, respecti-vely. Anterior and posterior Bland-Altman plots of central elevation are shown in figure 2. A similar trend was observed for pachymetry measurements, with the dual Scheimpflug system showing higher and lower values than the single Scheimpflug system for lower and higher elevations, respectively. The PCC for central anterior elevation was 0.952, while that for central posterior elevation was 0.974.
Keratometric values
Keratometric measurements recorded by the two machines are summarized in table 4. The mean difference in anterior radii between the dual and single Scheimpflug systems in steep and flat meridians were -0.05 mm and -0.02 mm, respectively. The mean absolute diffe-rence in anterior steep and flat meridian radii between the dual and
single Scheimpflug systems was 0.08 ± 0.14 mm and 0.06 ± 0.07 µm, respectively. The mean difference in posterior steep and flat meridian radii between the dual and single Scheimpflug systems was -0.02 mm and -0.06 mm, respectively. The mean absolute difference in the posterior steep and flat meridian radii between the dual and single Scheimpflug systems was 0.08 ± 0.08 mm and 0.11 ± 0.12 µm, respecti-vely. The PCC for central average keratometry was 0.931.
DISCUSSIOnOur results demonstrated that both the Galilei Dual Scheim-
pflug Analyzer and the Pentacam Single Scheimpflug Analyzer display similar values for the same subjects measured in terms of keratometric readings, anterior and posterior elevations, and pa-chymetry. Both machines gave values comparable with the points lying along the line of equality, with small limits of agreements (Figures 1 and 2). Previous studies have reported good correlations between both machines in either pachymetry or corneal power measurements(6-8).
One of the main diagnostic tools for keratoconus and keratectasia is abnormal topography. Threshold values of topography, beyond which the topography would be labeled as abnormal, are specific for
Figure 1. A Bland-Altman plot of percentage differences in average central pachymetry (CCT) measurements between the dual Scheimpflug system (Galilei) and the single Scheimpflug system (Pentacam). Figure 2. A Bland-Altman plot of differences in average central anterior elevation
(AE) (left) and central posterior elevation (PE) (right) measurements between the dual Scheimpflug system (Galilei) and the single Scheimpflug system (Pentacam).
Table 2. Correlation of central anterior elevation measurements between the dual Scheimpflug system (Galilei) and the single Scheimpflug system (Pentacam)
(μm) Galilei PentacamPearson’s correlation
coefficient
Central elevation -02.48 ± 02.98 -04.23 ± 04.57 0.952
Superior 2 mm 0-8.05 ± 10.43 0-8.25 ± 12.79 0.933
Inferior 2 mm 0-1.10 ± 06.06 -01.35 ± 12.81 0.871
Nasal 2 mm -10.35 ± 04.14 0-0.55 ± 05.01 0.784
Temporal 2 mm -01.30 ± 04.37 -01.68 ± 04.49 0.749
Superior 3 mm 0-8.43 ± 08.73 -12.08 ± 10.33 0.742
Inferior 3 mm -10.18 ± 09.89 0-9.30 ± 07.11 0.685
Table 3. Correlation of central posterior elevation measurements between the dual Scheimpflug system (Galilei) and the single Scheimpflug system (Pentacam)
(μm) Galilei PentacamPearson’s correlation
coefficient
Central elevation -2 5.33 ± 7.69 7.15 ± 14.75 0.974
Superior 2 mm -20.43 ± 16.49 -22.63 ± 24.59 0.961
Inferior 2 mm -3.25 ± 11.79 2.33 ± 26.92 0.807
Nasal 2 mm 1.23 ± 10.84 2.73 ± 11.64 0.804
Temporal 2 mm 4.50 ± 11.86 5.25 ± 12.27 0.961
Superior 3 mm -22.65 ± 10.75 -35.03 ± 17.11 0.706
Inferior 3 mm -24.95 ± 17.77 -26.53 ± 18.26 0.963
Table 4. Correlation of corneal keratometric measurements between the dual Scheimpflug system (Galilei) and the single Scheimpflug system (Pentacam)
Galilei Pentacam
Pearson’s correlation coefficient
Central average keratometry (D)
45.14 ± 3.20 44.81 ± 3.02 0.931
R steep front (mm) 07.43 ± 0.46 07.46 ± 0.44 0.979
R flat front (mm) 07.66 ± 0.42 07.68 ± 0.40 0.984
R steep back (mm) 06.02 ± 0.47 06.03 ± 0.48 0.968
R flat back (mm) 06.36 ± 0.45 06.42 ± 0.40 0.946

Assessment of anterior and posterior corneal indices using two Scheimpflug analyzers
20 Arq Bras Oftalmol. 2014;77(1):17-20
each machine. Problems with the existence of 2 systems will make it more difficult to set common standard cut-off values. In addition, refractive surgery physicians who have access to both systems may be faced with the need to compare serial images of the same patient using 2 different machines. Machine threshold values were first studied on the Orbscan (Bausch and Lomb)(2,9-11) and later on the Pentacam(12,13). With the availability of the Galilei Dual Scheimpflug Analyzer, the primary concern was whether values obtained using the dual Scheimpflug system correlated with those obtained using the single Scheimpflug system and whether images captured by both systems can be safely compared. Our study showed that the 2 systems were strongly correlated in terms of keratometry, anterior and posterior elevation, and pachymetry measurements. Therefore, a conclusion or a trend in values in a specific patient can be gene-ralized from the single Scheimpflug system and applied to the dual Scheimpflug system when considering threshold values and overall patterns. Our results, in terms of pachymetry, were in agreement with those published by Jahadi-Hoseini et al.(6).
The central keratometric, curvature, and pachymetric values sho wed a high correlation (and high agreement) and were not very different between both systems. As we moved peripherally, the correlation remained high, albeit not as strong as that in the central area. Similarly, other authors have reported an increase in variability in corneal pachymetry measurements from the center to the peri-phery, particularly in the superior cornea(4,14-17). They attributed this variability to the effects of the superior eyelid(4). We believe that the differences observed in paracentral (peripheral) values were very pre dictable because small decentration in the BFS would lead to a false high value, considering that the peripheral cornea is farther away from the BFS because of its prolate shape. Even within the same system, small decentrations in BFS can manifest as large deviations in peripheral elevation. The effects of contact lenses on corneal eleva-tion and curvature have been eliminated from the equation because all subjects were advised to stop wearing soft contact lenses for at least 2 weeks(3); furthermore, all subjects that had worn rigid contact lenses in the past 6 months were excluded from the study. The ima-ges were obtained on the same day, thus decreasing any additional confounding factors.
Keratometric values in both machines, despite the fact that they were obtained in a different manner, showed a high degree of cor-relation between both systems; keratometric values with the dual Scheim pflug system were obtained mainly from the Placido image and were only complemented by the rotating Scheimpflug cameras, while keratometry using the single Scheimpflug system relied solely on information from the Scheimpflug images.
The objective of our paper was not to show the advantage of one system over the other, but to assess the degree of correlation. A previously published study showed a difference between the single and dual Scheimpflug systems, with values obtained by the former system (Pentacam) being higher than those obtained by the latter (Galilei)(1). We believe that the difference was primarily due to the diff erent BFS diameters pre-set for each system: 9 mm in the single Scheimpflug system and 8 mm in the dual Scheimpflug system. Current versions of the Pentacam software, similar to the software used in our study, have adopted the 8-mm pre-set BFS diameter. The fact that both machines showed similar results for all indices made it possible to compare the follow-up findings of patients obtained with these two systems, provided the radius of the BFS was set to 8 mm in both machines.
The reason for incorporating two Scheimpflug cameras may solely be patency issues. The strong correlation between measurements obtained by both systems does not preclude the potential ad-van tages offered by the dual Scheimpflug system over the single Scheim pflug system; in theory, the former should be less sensitive to eye movements while obtaining pachymetry measurements. This theoretical advantage could be translated into a clinical one only in a small subset of patients with eye movements beyond a certain critical threshold. Therefore, potential advantages of the dual Scheimpflug system observed in some patients would be easily diluted while evaluating aggregate results. Further studies with the objective of testing the theoretical advantages of the dual Scheimpflug system and com paring them with those of a gold standard system are required.
Our study was limited by the small sample size.In conclusion, the single and dual Scheimpflug analyzers correla-
ted well in terms of pachymetry, anterior and posterior elevation, and curvature measurements.
ReFeRenCeS 1. Salouti R, Nowroozzadeh MH, Zamani M, Fard AH, Niknam S. Comparison of anterior
and posterior elevation map measurements between 2 Scheimpflug imaging sys-tems. J Cataract Refract Surg. 2009;35(5):856-62.
2. Sy ME, Ramirez-Miranda A, Zarei-Ghanavati S, Engle J, Danesh J, Hamilton DR. Comparison of posterior corneal imaging before and after LASIK using dual rotating scheimpflug and scanning slit-beam corneal tomography systems. J Refract Surg. 2013;29(2):96-101.
3. Hashemi H, Firoozabadi MR, Mehravaran S, Gorouhi F. Corneal stability after discon-tinued soft contact lens wear. Cont Lens Anterior Eye. 2008;31(3):122-5.
4. Miranda MA, Radhakrishnan H, O’Donnell C. Repeatability of oculus pentacam me-trics derived from corneal topography. Cornea. 2009;28(6):657-66.
5. McGraw KO, Wong S.P. Forming inferences about some intraclass correlation coeffi-cients. Psychological Methods. 1996;1:30-46.
6. Jahadi Hosseini HR, Katbab A, Khalili MR, Abtahi MB. Comparison of corneal thickness measurements using Galilei, HR Pentacam, and ultrasound. Cornea. 2010;29(10): 1091-5.
7. Oliveira CM, Ribeiro C, Franco S. Corneal imaging with slit-scanning and Scheimpflug imaging techniques. Clin Exp Optom. 2011;94(1):33-42.
8. Shirayama M, Wang L, Weikert MP, Koch DD. Comparison of corneal powers obtained from 4 different devices. Am J Ophthalmol. 2009;148(4):528-35 e1.
9. Cairns G, McGhee CN. Orbscan computerized topography: attributes, applications, and limitations. J Cataract Refract Surg. 2005;31(1):205-20.
10. Rainer G, Findl O, Petternel V, Kiss B, Drexler W, Skorpik C, et al. Central corneal thi-ckness measurements with partial coherence interferometry, ultrasound, and the Orbscan system. Ophthalmology. 2004;111(5):875-9.
11. Karimian F, Feizi S, Doozandeh A, Faramarzi A, Yaseri M. Comparison of corneal tomo-graphy measurements using Galilei, Orbscan II, and Placido disk-based topographer systems. J Refract Surg. 2011;27(7):502-8.
12. Lackner B, Schmidinger G, Pieh S, Funovics MA, Skorpik C. Repeatability and repro-ducibility of central corneal thickness measurement with Pentacam, Orbscan, and ultrasound. Optom Vis Sci. 2005;82(10):892-9.
13. O’Donnell C, Maldonado-Codina C. Agreement and repeatability of central thickness measurement in normal corneas using ultrasound pachymetry and the OCULUS Pen tacam. Cornea. 2005;24(8):920-4.
14. Miranda MA, Radhakrishnan H, O’Donnell C. Repeatability of corneal thickness mea-sured using an Oculus Pentacam. Optom Vis Sci. 2009;86(3):266-72.
15. Bullimore MA, Fusaro RE, Adams CW. The repeatability of automated and clinician refraction. Optom Vis Sci. 1998;75(8):617-22.
16. Lam AK, Chen D. Pentacam pachometry: comparison with non-contact specular microscopy on the central cornea and inter-session repeatability on the peripheral cornea. Clin Exp Optom. 2007;90(2):108-14.
17. Buehl W, Stojanac D, Sacu S, Drexler W, Findl O. Comparison of three methods of measuring corneal thickness and anterior chamber depth. Am J Ophthalmol. 2006; 141(1):7-12.

21Arq Bras Oftalmol. 2014;77(1):21-4
Original Article
InTRODUCTIOnSurveys represent one of the most common types of research
in the health, social, and human sciences. Particularly in the health sciences, the prospect of studying the evolution of a specific disorder and monitoring the efficacy of a specific treatment based on assess-ment surveys has been considered a great advantage, because they are easily accessible and inexpensive(1).
The increasing use of surveys to assess the quality of life, quantify symptoms, and evaluate attitudes and behaviors in studies from dis-tinct countries warrants the translation and adaptation of previously validated questionnaires to different languages and cultures. To fa-cilitate and expedite this task, guidelines on the translation process aiming to ensure the equivalence between the original and the translated versions have been published(1-3).
The literature has several validated surveys that are useful for measuring the symptoms associated with visual discomfort, such as those developed by Conlon et al.(4), the Convergence Insufficiency
Symptom Survey (CISS)(5), and the CDQOVL visual quality of life survey(6).
The CISS survey addresses the most common issues regarding near vision problems and has been subjected to numerous stu-dies to determine its validity, reproducibility, and effectiveness in identifying and monitoring the treatment evolution in individuals with convergence insufficiency(5,7-9). Initially developed by the CIRS (Convergence Insufficiency and Reading Study) group, it was later modified to include near vision activities for adults (e.g., video games, hobbies, reading, and leisure activities)(5,7,8). This questionnaire, valida-ted in schoolchildren aged between 9 and 18 years(5) and in young adults aged between 19 and 30 years(8), is a reproducible and valid instrument, with high internal consistency and capable of addressing clinical changes during the treatment of convergence insufficiency(9). In addition, it has proven to be an added value in the diagnosis of other nonstrabismic binocular disorders with symptoms similar to those of convergence insufficiency, particularly the accommoda-
Translation and validation of Convergence Insufficiency Symptom Survey (CISS) to Portuguese - psychometric resultsTradução e validação do CISS para a língua portuguesa - resultados psicométricos
caTarina TavareS1, aMélia Maria MonTeiro FernandeS nuneS2, anTónio João SanToS nuneS3, Maria vaz paTo4, pedro MiGuel lourenço MonTeiro2
Submitted for publication: August 2, 2013 Accepted for publication: August 25, 2013
Study carried out at Laboratório de Ciências da Visão, University of Beira Interior.1 Health Sciences Faculty, University of Beira Interior, Covilhã, Portugal.2 Department of Physics, University of Beira Interior, Covilhã, Portugal.3 Research Center, Management and Economics Department, University of Beira Interior, Covilhã,
Portugal. 4 Health Science Research Centre, FCS-UBI. Portugal; ULS Guarda, Hospital Sousa Martins.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: C. Tavares, None; A.M.M.F Nunes, None; A.J.S. Nunes, None; M. Vaz Pato, None; P.M.L. Monteiro, None.
Correspondence address: Amélia Maria Monteiro Fernandes Nunes. Avenida Marques d’Avila e Bolama - Universidade da Beira Interior - Departamento de Física, 6200 - Covilhã - Portugal
E-mail: [email protected]
Projecto no CE-FCS-2012-027 - Faculdade Ciências da Saúde - UBI.
ABSTRACTPurpose: Translate and adapt the Convergence Insuficiency Symptom Survey (CISS) questionnaire to the Portuguese language and culture and assess the psychometric properties of the translated questionnaire (CISSvp). Methods: The CISS questionnaire was adapted according to the methodology recommended by some authors. The process involved two translations and back- translations performed by independent evaluators, evaluation of these versions, preparation of a synthesis version and its pre-test. The final version (CISSvp) was applied in 70 patients (21.79 ± 2.42 years) students in higher education, and at two different times, by two observers, to assess its reliability. Results: The results showed good internal consistency of the CISSvp (Cronbach’s alpha - α=0.893). The test re-test revealed an average of the differences between the first and second evaluation of 0.75 points (SD ± 3.53), which indicates a mi-nimum bias between the two administrations. The interrater reliability assessed by intraclass correlation coefficient ranged from 0.880 to 0.952, revealing that the CISSvp represents an appropriate tool for measuring the visual discomfort associated with near vision tasks with a high level of reproducibility. Conclusions: The CISS Portuguese version, showed good psychometric pro-perties and has been sown to be applicable to the Portuguese population, to quantify the visual discomfort associated with near vision, in higher education students.Keywords: Translations; Questionnaires; Language; Convergence, ocular; Asthe-nopia; Psychometrics
RESUMOObjetivo: Traduzir e adaptar transculturalmente o questionário Convergence Insu-ficiency Symptom Survey (CISS) para a língua portuguesa e avaliar as propriedades psicométricas do questionário traduzido (CISSvp). Métodos: O questionário CISS foi adaptado segundo metodologia recomendada por alguns autores. O processo envolveu duas traduções e retrotraduções realizadas por avaliadores independentes, avaliação das versões seguida da elaboração de uma versão síntese e pré-teste comentado. A versão final (CISSvp) foi aplicada em 70 indivíduos (21,79 ± 2,42 anos) estudantes do ensino superior, em dois momentos distintos e por dois observadores, para avaliar a confiabilidade do mesmo. Resultados: Os resultados evidenciaram boa consistência interna do CISSvp (alfa de Cronbach - α=0,893). O teste re-teste revelou uma media das diferenças entre a primeira e a segunda avaliação de 0,75 pontos (SD=±3,53) o que indica um viés mínimo entre as duas administrações. A confiabilidade inter-examinadores avaliada pelo coeficiente de correlação intraclasse variou de 0,880 e 0,952, revelando que o CISSvp representa uma ferramenta de medida do desconforto visual associado a tarefas em visão próxima com um nível de reprodutibilidade elevado. Conclusões: O CISS versão portuguesa apresentou boas propriedades psicométricas e demonstrou ser aplicável na população portuguesa, para quantificar a o desconforto visual associado à visão de perto, em estudantes do ensino superior.
Descritores: Traduções; Questionários; Linguagem; Convergência ocular; Astenopia; Psicometria

Translation and validation of Convergence Insufficiency Symptom Survey (CISS) to Portuguese - psychometric results
22 Arq Bras Oftalmol. 2014;77(1):21-4
tive insufficiency(10). It has also contributed to the quantification of symptoms of visual discomfort in students(11), and the identification of individuals susceptible to visual complaints associated with visual discomfort from 3D displays(12).
In Portugal, no easy-to-apply, self-administered instruments with good reproducibility rates are able to assess the visual discomfort associated with near vision tasks. Therefore, the present study aimed to adapt the CISS survey both transculturally and linguistically into Portuguese.
MeTHODSThe study was conducted in the Laboratory of Vision Sciences of
the University of Beira Interior, with the approval of the Ethics Com-mittee of the Faculty of Health Sciences of the same university (pro-cess CE-FCS-2012-027). The research comprised two phases: the pha-se of translation and transcultural adaptation to the target language and the phase of psychometric validation of the questionnaire.
The translation and transcultural adaptation process was based on the guidelines proposed by the Beaton and Gjersing teams(2,3).
The psychometric validation of the translated survey was per-formed via interitem internal consistency analysis using Cronbach’s alpha, and via temporal stability and reproducibility assessment using the test-retest analysis. These analyses are able to assess the validity and the reliability of the adapted instrument(13,14). To achieve the de-sired results, the translated questionnaire was applied twice by two separate researchers. The interval between the applications of the two questionnaires was 1 week, which was sufficient to ensure that no significant changes would occur in the general behavior of the participants and that they would not remember the answers given in the previous questionnaire. This interval corresponds to the period necessary to analyze the reliability of measurements of the health status using the test-retest reliability test(14).
participants
The number of participants in the process of translation and adap tation of the survey (pretest) amounted to 20 students. Seven ty students aged between 18 and 30 years participated in the psy -cho metric validation phase. Of these, 30 were from the Faculty of Health Sciences and the remaining 40 were from the Department of Sciences and Engineering of the University of Beira Interior. All par-ticipants were duly informed about the aim of the study and signed an informed consent form.
survey
The object of study was the Convergence Insufficiency Symptom Sur vey (CISS), which comprised 15 items and assessed the presence and frequency of symptoms typical of convergence insufficiency. In each question the subject indicates the frequency of each symptom on a Likert scale with scores ranging from 0 to 4, according to the following frequencies: never (0), infrequently (1), sometimes (2), often (3), and always (4). The points of all 15 items were added to determine the final score, which ranged from 0 to 60(11).
procedures
Before the translation and validation, we requested the question-naire in digital form and a written authorization from one of the au-thors of the original survey(1).
After obtaining the authorization and the approval of the ethics committee to conduct the study with students of the University of Beira Interior, the work instrument described below was performed.
translation and transcultural adaptation process
To obtain a scientifically based translation and transcultural va -li dation of the survey from its original language (English) into the
target language (Portuguese), we adopted the methods proposed by Beaton (2000) and Gjersing (2010)(2,3). The process involved three steps, from the initial translation to the final version of the CISS (de-signated CISSvp), as summarized in table 1.
First step - Initial translation: two independent translations (de-signated T1 and T2) were performed by two bilingual translators working in completely different areas of expertise. A first assessment meeting was conducted, when a panel composed of two visual health professionals, one social sciences professor, one neurologist, and two independent translators analyzed T1 and T2 in depth, com-paring them with the original questionnaire. This assessment resulted in the establishment of the third translated version of the question-naire after consensus among all parties involved (T3 version).
Second step - Back-translation: The T3 version of the questionnai-re translated into Portuguese was translated back into English by a professional translator, who did not know the original version, resul-ting in a back-translated version (Tr-t). A second assessment meeting ensued, with the presence of the same panel that attended the first meeting and the professional translator. In this meeting, the original questionnaire, the T3 version, and the Tr-t version, were analyzed, compared, and rated. Small changes were made to the syntax, resul-ting in the fourth version of the questionnaire (T4 version).
Third step - Final revision: in this phase a pretest was conducted through the assessment of the T4 version of the translated questionnaire by 20 university students to determine inconsistencies and interpret the content of the various items. At this point, the option “I do not understand the question” was added to the answer options for each item. In addition, the assessors were asked to comment on the ques-tions that raised doubts. Following the analysis of the pretest results, the final format of the Portuguese version of the questionnaire was prepared (CISSvp).
psychometric validation of the scale Psychometric validation of the scale was performed according to the
guidelines proposed in previous studies(15). The following ana lyses were performed: interitem internal consistency, temporal stability, and interobserver reproducibility.
The analysis of internal consistency aimed to determine whether the questionnaire items were correlated with each other. The internal consistency coefficient provided an estimate of measurement relia-bility, on the basis of the assumption that items that assess the same constructs must be correlated.
Stability of the instrument, or test-retest reliability, was assessed using Spearman’s coefficient to determine the correlation or the as-sociation strength between the two instances of the administration of the survey. The intraclass correlation coefficient (ICC) was used to determine the degree of concordance between the measurements taken by different respondents(16).
STATISTICAL AnALySISAll statistical analyses were performed using the IBM SPSS Statis-
tics software, version 20.
Table 1. Summary of CISS (convergence insufficiency symptom sur-vey) questionnaire translation and adaptation process to portuguese
Phase Action Result
Initial translation Independent translation Translated version T3
1st meeting
Back-translation Back-translation Translated version T4
2nd meeting
Final review VersionT4 pre-test Final version CISSvp
3rd meeting

Tavares C, et al.
23Arq Bras Oftalmol. 2014;77(1):21-4
The reliability of a Likert-type scale was assessed using Cronbach’s α coefficient. This coefficient assesses the internal consistency of a set of items, i.e., it evaluates the degree of coherence (relatedness), with an aim to determine whether those items measure the same parameter and whether they can be summed into a single score. The values >0.7 were considered acceptable(13).
The reliability of the instrument was assessed using the following tests: Spearman’s correlation coefficient, to determine the association of CISSvp survey score between the two assessment instances and to determine temporal stability, and the intraclass correlation coeffi-cient (ICC), to evaluate the degree of concordance between the me-asurements taken by distinct assessors. The degree of concordance of ICC values was determined as proposed by Bland, i.e., acceptable: <0.4, good: 0.41-0.6, very good: 0.61-0.80, and excellent: 0.81-1.0(16).
ReSULTS
survey translation and adaptation During the first step of the translation and adaptation into Portu-
guese, difficulties emerged when translating and adapting questions 10 and 11. Question 10 was translated in a similar fashion by the two translators: “sente dor nos olhos.” Question 11 was translated diffe-rently by the same translators: “sente os olhos doloridos” and “sente os olhos inflamados,” and these versions raised controversies among the panel members. Therefore, a separate interview with 10 students was proposed, when they were asked to opine on the interpretation of the two questions. They concluded that the translation of question 11, “sente os olhos inflamados,” was the most adequate.
The remaining steps of the process did not raise any controversy.In the third step of the process, the result of the pretest did not
indicate any inconsistencies in the interpretation of the items of the translated survey. The overall result of this entire process, which is presented in Annex A, is the draft of the final Portuguese version of the CISS survey.
psychometric validation of the survey
The answers of the survey administered to both groups of stu-dents, one group from the Department of Health Sciences (FCS) and the other from other departments of the University of Beira Interior, were analyzed to validate the translation of the instrument. The mean score differences between the two groups of students were analyzed using the Mann-Whitney test, which indicated that the survey score of FCS students and the score of students from other departments were not significantly different (Table 1).
The internal consistency of the scale was determined for the sample evaluated by FCS students and that evaluated by students from other departments, and for the total sample of respondents. This assessment indicated moderate to high reliability for all groups (Table 2).
The analysis of the overall total internal consistency, and the in-ternal consistency when one item was eliminated (Table 3), in both the test and retest, revealed that all items contributed to a higher consistency. However, the exclusion of item 6 neither decreased the overall consistency nor contributed to a significant increase in inter-nal consistency. The Cronbach’s alpha obtained in the retest (0.918) was slightly higher than that obtained in the test (0.893). Moreover, as this was a translation and adaptation of an instrument into another language, it would be useful to compare this data with those from other populations and cultures.
cissvp survey reliability analysis
The temporal stability was assessed via the test-retest reliability analysis, by interpreting the Spearman’s correlation coefficient bet-ween the score of each item in each evaluation. Table 4 shows the Spearman’s rho coefficient for each item and for the overall score.
The correlations between the answers from the first and the se -cond survey assessments varied between 0.504 (item 5) and 0.844 (item 3). Using the scores proposed by Maroco, correlations were high for items 1, 3, 8, 11, and 13 (scores between 0.70 and 0.89), and moderate for items 2, 4, 6, 7, 9, 10, 12, 14, and 15 (scores between 0.40 and 0.69)(17). The overall scores obtained on the two instances of the survey assessment exhibited an excellent correlation, which led us to conclude that CISSvp had a good temporal stability.
ICC between the two assessment instances was 0.924 (95% CI: 0.880 and 0.952). The mean difference between the survey’s overall score of the first and second assessments was 0.75 ± 3.53 points, indica-ting minimum bias between the two evaluations (sign test: Z score, -1.162; p, 0.245).
Table 2. Descriptive statistics, test of differences and internal consis-tency of the Portuguese version of the CISS (convergence insuffi-ciency symptom survey) questionnaire (CISSvp) score
Sample (n)Age
mean ± SDTotal score mean ± SD
Mann-Withneyp-value
Cronbach’s Alpha
Total sample (70) 21.79 ± 2.42 15.56 ± 8.86 – 0.893
CHSS (30) 21.33 ± 1.47 15.03 ± 8.380.656
0.901
Other (40) 21.13 ± 2.91 15.95 ± 9.20 0.892
SD= standard deviation; CHSS= College of Health Sciences Students; Other= college of sciences and college of engineering students.
Table 3. Reliability: Internal consistency of the portuguese version of CISS (convergence insufficiency symptom survey) questionnaire (CISSvp)
Item
Correlation total corrected
Cronbach’s Alpha if the item is excluded
Test Re-test Test Re-test
11 0.709 0.721 0.880 0.909
12 0.713 0.746 0.879 0.908
13 0.642 0.625 0.883 0.912
14 0.521 0.569 0.888 0.914
15 0.463 0.553 0.890 0.914
16 0.336 0.425 0.895 0.919
17 0.498 0.529 0.889 0.915
18 0.353 0.542 0.894 0.915
19 0.488 0.641 0.889 0.912
10 0.709 0.749 0.880 0.908
11 0.609 0.661 0.884 0.911
12 0.557 0.597 0.886 0.913
13 0.675 0.718 0.881 0.909
14 0.489 0.565 0.889 0.914
15 0.640 0.714 0.883 0.909
Total 0.893 0.918
Table 4. Spearman correlation coefficient between test and re-test of the CISSvp questionnaire (convergence insufficiency symptom survey – portuguese version)
Item 1 2 3 4 5 6 7 8
Rho 0.802 0.691 0.840 0.640 0.504 0.668 0.688 0.823
Item 9 10 11 12 13 14 15 Total score
Rho 0.685 0.697 0.782 0.638 0.719 0.565 0.686 0.910

Translation and validation of Convergence Insufficiency Symptom Survey (CISS) to Portuguese - psychometric results
24 Arq Bras Oftalmol. 2014;77(1):21-4
DISCUSSIOnThe results of the present study indicate that the translation and
adaptation of the CISS survey into Portuguese, which resulted in the CISSvp version, is a reliable outcome measurement instrument for uni-versity students. The high internal consistency of the answers obtained in the survey (α = 0.893) and the high intraclass correlation (ICC=0.924) indicate that CISSvp exhibited a high degree of reliability.
The translation and adaptation process was scientifically rigorous and followed the guidelines used in similar studies(2,3). Moreover, the use of two independent translators was very useful, because it allo-wed the comparison and discussion of the two distinct versions and the preparation of a final translation, after initial discrepancies were re solved. The inclusion of members with distinct areas of expertise in the assessment panel allowed the comparison of different view-points from professionals in health and social sciences. The discus-sions that unfolded to solve those discrepancies and the search for a consensus were essential to the entire process of semantic equiva-lence. The pretest applied during step 3 of the process indicated that all participants understood the questions from the CISSvp survey.
In the psychometric validation of the scale, the sample of res-pondents was classified according to the University the students belonged to. The aim of this classification was to investigate whether familiarity with the terms used in the translated survey affected the way the questions were answered. The mean score of the survey was similar for both groups of students, 15.03 and 15.95, and the Mann-Whitney test indicated that the scores obtained for the two student groups were not significantly different. The scores of the interitem internal consistency analysis using Cronbach’s alpha coe-fficient were 0.901 and 0.892, indicating that the internal consistency of CISSvp was high for both groups of students(13). Using data from all participants, Cronbach’s alpha was 0.893, and all items contributed to the increase in the overall internal consistency. These results indicate that the internal consistency of CISSvp was high and similar to the results obtained by Rouse during the validation of the original survey (CISS) using a sample of adult respondents(8).
ICC was 0.924, which indicates an excellent reproducibility for CISSvp(16). The mean difference (0.75 ± 3.528) and the analysis of va rian-ce between the two assessment instances (sign test Z score, -1.162; p, 0.245) suggest minimum bias between the two evaluations applied in a 1-week interval. These data are in line with the results of other studies in which CISS was used(5,8).
COnCLUSIOnThe aim of this study was to translate the CISS survey into Portu-
guese (CISSvp). Both the translation and the psychometric characte-ristics of the survey application were very satisfactory. The outcome
mea surement instrument exhibited very good to excellent levels of internal reliability (Cronbach’s alpha) and temporal stability (test-re-test analysis), indicating that CISSvp is a reliable and reproducible instrument for university students.
ReFeRenCeS 1. Acquadro C, Conway K, Hareendran A, Aaronson N; European Regulatory Issues and
Quality of Life Assessment (ERIQA) Group. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials. Value Health. 2008;11(3):509-21.
2. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of crosscul -tural adaptation of self-report measures. Spine (Phila Pa 1976). 2000;25(24):3186-91.
3. Gjersing L, Caplehorn, J R, Clausen T. Cross-cultural adaptation of research instruments: Language, setting, time and statistical considerations. BMC Med Res Me thodol. 2010:10-3.
4. Conlon E, Lovegrove W, Chekaluk E, Pattison P. Measuring visual discomfort. Vis Cogn. 1999;6:637-66.
5. Borsting E, Rouse MW, Mitchel GL, Scheiman M, Cotter SA, Cooper J, Kulp MT, London R; Coonverge Insufficiency Treatment Trial Group. Validity and reliability of the revised convergence insufficiency symptom survey in children aged 9 to 18 years. Optom Vis Sci. 2003;80(12):832-8. Optom Vis Sci. 2004 Jul; 81(7):489; author reply 489-90. Optom Vis Sci. 2004 Jul; 81(7):489; author reply 489-90. Optom Vis Sci. 2004 Jul; 81(7):489; author reply 489-90. Comment in: Optom Vis Sci. 2004;81(7):489; author reply 489-90.
6. Mozlin R. Quality-of-life outcomes assessment. J Optom Vis Dev. 1995;26:194-9. 7. Borsting E, Rouse MW, De Land PN, Convergence Insufficiency and Reading Study
(CIRS) group. Prospective comparison of convergence insufficiency and normal binocular children on CIRS symptom surveys. Optom Vis Sci. 1999;76(4):221-8.
8. Rouse MW, Borsting E, Mitchel GL, Scheiman M, Cotter SA, Cooper J, Kulp MT, London R, Wensveen J; Convergence Insufficiency Treatment Trial Group. Validity and reliabi-lity of the revised convergence insufficiency symptom survey in adults. Ophthalmic Physiol Opt. 2004;24(5):384-90.
9. The Convergence Insufficiency Treatment Trial (CITT) Study Group. The convergence insufficiency treatment trial: design, methods and baseline data. Ophthalmic Epide-miol. 2008;15(1):24-36.
10. Marran, LF, De Land PN, Nguyen AL. Accommodative insufficiency is the primary source of symptoms in children diagnosed with convergence insufficiency. Optom Vis Sci. 2006;83 (5):281-9. Comment in: Optom Vis Sci. 2006;83(11):857-8; author reply 858-9.
11. Borsting E, Chase C, Tosha C, Ridder WH 3rd. Longitudinal study of visual discomfort symptoms in college students. Optom Vis Sci. 2008;85(10):992-8.
12. Lambooij MT, Ijsselsteijn WA, Fortuin M, Evans BJ, Heynderickx I. Susceptibility to visual discomfort of 3-D displays by visual performance measures. IEEE Trans Circuit Syst Video Technol. 2011;21(12):1913-23.
13. Cortina JM. What is coefficient alpha? an examination of theory and applications. J Applied Psychol. 1993;78:98-104.
14. Marx RG, Menezes A, Horovitz L, Jones EC, Warren RF. A comparison of two time intervals for test-retest reliability of health status instruments. J Clin Epidemiol. 2003; 56(8):730-5.
15. Kimberlin CL, Winsterstein AG. Validity and reliability of measurement instruments used in research. Am J Health Syst Pharm. 2008;65(23):2276-84.
16. Bland JM, Altman DG. A note on the use of the intraclass correlation coefficient in the evaluation of agreement between two methods of measurement. Comput Biol Med. 1990;20(5):337-40.
17. Maroco J. Análise estatística com utilização do SPSS. 3a ed. Lisboa: Edições Sílabo; 2007.

25Arq Bras Oftalmol. 2014;77(1):25-9
Original Article
InTRODUCTIOnCataract surgery is the most commonly performed surgery world -
wide and one of the most cost-effective interventions(1,2). Yet, in ma-ny developing countries, millions of individuals are still blind from cataract and have not undergone surgery. There are 2 indicators of cataract surgical services: cataract surgical rate (CSR) and cataract sur-gical coverage (CSC). CSR is the annual number of cataract surgeries performed per 1 million population. CSC is the annual proportion of
cataract cases completed in a given population, thereby demonstra-ting the distribution and equity of services across different regions and populations.
To calculate cataract surgery needs, the number of individuals who are blind or visually impaired because of cataract (based on preo-perative visual acuity) should first be estimated in each country. This estimate is projected as 5-10 years by modeling(3). Furthermore, the size of a country and geographically disparate data with regard to
Complexities and challenges of surgical data collection from cataract patients: comparison of cataract surgery rates between 2001 and 2008 in all provinces of ArgentinaComplexidades e desafios da coleta de dados cirúrgicos de catarata: comparação das taxas de cirurgia de catarata em todas as províncias da Argentina de 2001 em relação a 2008
van c. lanSinGh1, Maria e. nano2, MariSSa J. carTer3, naTalia záraTe2, SerGe reSniKoFF 4, KriSTen a. ecKerT3
Submitted for publication: May 29, 2013 Accepted for publication: August 25, 2013
Study was conducted at the International Agency for the Prevention of Blindness/VISION 2020 Latin America.
1 International Agency for the Prevention of Blindness/VISION 2020 Latin America, Weston, FL 33331, USA.
2 Fundación Oftalmológica Hugo D. Nano, Buenos Aires, Argentina.3 Strategic Solutions, Inc., Cody, WY 82414, USA.4 International Health and Development, Geneva, Switzerland.
Financial support: This study was funded by ORBIS and the International Agency for the Prevention of Blindness.
Disclosure of potential conflicts of interest: V.C. Lansingh is employed by the IAPB; M.E. Nano is employed by Fundación Hugo Nano; M.J. Carter is employed by Strategic Solutions and is a paid consultant to ORBIS and the IAPB; N. Zárate is employed by Fundación Hugo Nano; S. Resnikoff, None; K.A. Eckert is a paid consultant to Strategic Solutions.
Correspondence address: Van C. Lansingh. International Agency for the Prevention of Blindness/VISION 2020 Latin America, 3720 San Simeon Cr. Weston, FL 33331, USA - Email: [email protected]
Institution responsible for the approval of the research ethics committee: Fundación Oftalmológica Hugo D. Nano.
Project number: 4013.
ABSTRACT Purpose: To compare the cataract surgical rate (CSR) in 2001 with that in 2008 in all Argentinean provinces using current reporting methods and verify the accuracy of CSRs by cross-checking these methods with the number of sold intraocular lenses (IOLs) within the country.Methods: A longitudinal study including public and private set-ups was conducted, and it included 40 ophthalmologists from 22 provinces who provided cataract surgery data for 2001 and 2008. Other data were obtained from the Ministry of Health. Estimates were cross-checked against the market data for sold intraocular lens (IOLs) in 2008 and 2010. Results: The number of cataract surgeries increased 2.7-fold, from 62,739 in 2001 to 169,762 in 2008, with increases in every province except Mendoza. Although the population also increased by 9.4% during the same time period, the apparent CSR jumped from 1,744 to 4,313 per million population. The number of IOLs sold in Argentina in 2008 was 186,652, suggesting that the number of cataract sur-geries performed was slightly greater than anticipated. Cross-checks with other countries using IOL sales data did not show discrepancies when compared with previously reported CSRs.Conclusions: Although the CSR in Argentina increased considerably from 2001 to 2008 for several reasons, the main reason was that thorough cross-checking between the number of surgeries reported and the number of IOLs sold revealed that the number of surgeries performed annually were being underestimated as a result of incomplete reporting by private practitioners. Furthermore, the presence of multiple societies of ophthalmology in the country complicated the process of obtaining accurate data.
Keywords: Cataract/epidemiology; Argentina; Health services research/statistics & numerical data
RESUMOObjetivo: Comparar a taxa de cirurgia de catarata (TCC) em todas as províncias da Argentina entre 2001 e 2008, utilizando métodos de relatórios convencionais e verificar a precisão da TCC por meio do cruzamento desses métodos com o número de lentes intraoculares (LIOs) vendidas no país.Métodos: Estudo longitudinal realizado em clínicas públicas e privadas, com a participação de 40 oftalmologistas de 22 províncias, que forneceram dados sobre cirurgias de catarata para 2001 e 2008. Outros dados foram obtidos a partir do Ministério da Saúde. As obser-vações foram cruzadas com os dados de mercado para LIOs no período de 2008 a 2010.Resultados: O número de cirurgias de catarata aumentaram 2,7 vezes, de 62.739 em 2001 para 169.762 em 2008, com aumentos em todas as províncias, exceto Mendoza. Embora a população também tenha aumentado 9,4 % durante o mesmo período de tempo, a aparente TCC saltou de 1.744 para 4.313 por milhão de população. O número de LIOs vendidas na Argentina em 2008 foi de 186.652, o que pode significar que tenham sido realizadas um pouco mais de cirurgias de catarata do que o estimado. Verificações cruzadas com outros países que utilizam dados de vendas de LIOs não apresentam discrepâncias quando comparado a TCC anteriormente relatadas.Conclusões: De 2001 a 2008, a TCC na Argentina aumentou consideravelmente por várias razões mas, principalmente, porque foi revelada, por meio do cruzamento de dados sobre cirurgias relatadas com o número de LIOs vendidas, que o número de cirurgias realizadas anualmente foi hipoestimado no passado, como resultado de relatórios incompletos feitos por médicos privados. Há também várias sociedades de oftalmologia no país, o que dificulta a obtenção de dados precisos.
Descritores: Catarata/epidemiologia; Argentina; Pesquisa sobre serviços de saúde/estatística & dados numéricos

Complexities and challenges of surgical data collection from cataract patients: comparison of cataract surgery rates between 2001 and 2008 in all provinces of Argentina
26 Arq Bras Oftalmol. 2014;77(1):25-9
visual impairment are also factors that must be considered. Next, the number of cataract surgeries performed on an annual basis and the country’s capacity for surgeries have to be determined on the basis of the number of surgically active ophthalmologists in each district or province. Finally, postoperative visual acuities and sight restoration rates should be reported to assess whether outcomes are satisfactory. Epidemiological data are usually obtained from regional or national surveys using population sampling designs, such as the rapid assess-ment of cataract surgical services (RACSS)(4) or the rapid assessment of avoidable blindness (RAAB)(5) studies. The number of surgeries and outcomes is estimated from governmental or institutional records. Such data are often incomplete because of resource limitations or the lack of a mandate to collect surgical operation statistics. Conse-quently, the resulting situation can hamper the evaluation of whether needs and supplies are balanced and whether services are meeting future needs.
Most national surveys that cover entire countries are based on sam pling strategies; consequently, they do not cover all surgeries(6-9). In Argentina, although 2 RACSS studies have been conducted(10,11), no data have been published on the number of cataract surgeries by province, except for brief details for 2001 (Nano ME, Nano H; available from: http://boletinocular.bvsalud.org/boletim.php?lang=es&visionId=10192450200311&unitId=10192449200351&style=homepage).
To determine the reliability of the national reported CSRs, we as-sessed the reliability of current traditional sources using Argentina as an example of a well-developed country with many kinds of providers and major government activity. Therefore, the current study aimed to compare the CSR in 2001 with that in 2008 in all Argentinean pro-vinces using a methodology used to report data to the World Health Organization (WHO) for the last several years. Then, the study verified this data by cross-checking the number of intraocular lenses (IOLs) sold within the country. The timing of this study was in line with the recent approval of the updated WHO Action Plan for the prevention of avoidable blindness and visual impairment 2014-19 (EB132/9), which now has mandated that CSRs be reported by governments.
MeTHODSThe study adhered to the tenets of the Declaration of Helsinki.
The institutional review board of the Fundación Oftalmológica Hugo D. Nano determined that the study was exempt from formal review because it evaluated retrospective cataract surgical data and requi-red no patient intervention.
The head and deputy head of each provincial society of ophthal-mology were asked to recommend several high-volume surgeons who had performed the greatest number of surgeries and had best access to other provincial surgical and related data for participation in this study. The nominated ophthalmologists were contacted by phone or e-mail and invited to participate as local investigators. Par -ticipants were asked to obtain standardized data on cataract surge-ries performed within each province, including population data, num ber of surgical centers, number of cataract surgeries performed in the public and private health sectors, number of ophthalmolo-gists, and economic information. This information came from local provincial government sources such as the departments of health, industry representatives, and private clinics with high surgical volu-mes. Several follow-up calls were made in cases of non-response. Monthly information on the number of surgeries was requested for 12 months. Population information and economic data were verified and supplemented with National Census data from the Institute of Statistics and Census in Argentina. The number of ophthalmologists was estimated on the basis of data provided by various sources, inclu-ding participating ophthalmologists, societies, and large commercial houses. Data on the number of IOLs sold in Argentina were obtained from suppliers to verify the number of cataract surgeries performed in 2008 through 2010. Although there is reason to believe that supplier
data would be accurate (from all known suppliers with sales fi gures), this may not fully equate to the number of IOLs exactly used in a gi-ven year because of stockpiling, purchases by large institutions, and purchases by individuals that bypass customs.
Data collection issues meant that there were incomplete figures in Cordoba in 2008 and that data were not available for the private sector in Entre Ríos. For the private sector of Buenos Aires, the figure was calculated on the basis of the number of IOLs sold. Meanwhile, the Ministry of Health (MOH) provided input on public sector num-bers. Although this method has its limitations, it has worked for other provinces with complete data. This method has also been used in other countries, and similar data has been presented and analyzed from neighboring countries of Argentina in the Discussion to further validate this method.
ReSULTSIn 2001 and 2008, data were collected from a total of 40 ophthal-
mologists (1-3 per province) in 22 provinces. Between 2001 and 2008, the population of Argentina increased by 9.6% to 39.4 million (Table 1), but the most important statistic was the nearly one-third increase in the population aged ≥50 years (from 130,403 in 2001 to 172,154 in 2008), which is the age group at the greater risk of cataracts. During this same time period, the number of ophthalmologists was estimated to have increased from 3,417 to 4,079 (19.4%). The number of ophthal-mologists per million population increased from 95 to 104 (8.9%).
While the number of cataract surgeries increased from 62,739 in 2001 to 169,762 in 2008 (2.7-fold increase), the change varied con siderably by province (provincial geography: Figure 1). The majo-rity of provinces experienced a 26% to 100% increase in surgeries (Figure 2). Only one province, Mendoza, experienced a decline in the total number of surgeries (Table 1); however, the proportion of public surgeries increased from 2001 to 2008 (Figure 3). In Cordoba, despite repeated attempts, we did not receive full cooperation from local ophthalmologists and local authorities; therefore, the data were incomplete. Most likely, there was no decline in the number of surgeries, but this could not be verified. Formosa, which reported no surgeries in 2001 despite having 15 ophthalmologists, reported 1,680 surgeries in 2008. The number of surgeries increased by more than 2-fold in 6 other provinces.
CSR increased in all but 2 provinces: Cordoba (as explained abo-ve) and Río Negro (Table 1). Río Negro exhibited a very small decline (approximately 3%). The increases were impressive in Neuquen, La Rioja, Chaco, and Formosa. Overall, the national CSR increased from 1,744 to 4,313 per million.
The number of public surgeries-i.e., surgeries paid for by the go -vernment-increased from 5,762 to 14,614 (2.5-fold increase in abso -lute numbers); however, it decreased from 9.2% to 8.7% when con-sidered as a percentage of the total number of surgeries. Fourteen provinces experienced an increase in the number of public surgeries while 8 experienced a decrease (Figure 3). In Entre Ríos, the local so-ciety of ophthalmology did not provide surgical data for either time period (Figure 3). The largest absolute increase occurred in Misiones (3.3-fold increase in absolute numbers), where the number of public surgeries in 2008 was relatively small (164). While the percentage of public surgeries also increased in the greater Buenos Aires metropoli-tan area (5.7% to 8.3%; 10.259 surgeries in 2008), there was a decrease in San Juan (30.4% to 7.2%), San Luis (16.7% to 3.7%), and Tucumán (16.3% to 2.8%).
The number of IOLs sold in Argentina was 186,652 in 2008, of which 59,500 were paid for by the government under a private insurance scheme known as PAMI [Programa de Atención Médica Integral] and 127,152 were public/private sector surgeries. PAMI is considered a private provider that primarily offers health coverage to employees, who contribute a portion of their salary in each paycheck to the go-vernment fund, which then reimburses the PAMI insurance scheme.

Lansingh VC, et al.
27Arq Bras Oftalmol. 2014;77(1):25-9
PAMI additionally offers coverage to other vulnerable social groups, including veterans, the disabled, and widows. While 186,652 IOLs were sold in 2008, 169,762 surgeries were reported. Therefore, 16,890 surgeries were not accounted for, although it is likely that some of the IOLs imported in 2008 may not have been used for cataract surgeries
Table 1. Data on population, number of ophthalmologists and cataract surgeries, and cataract surgical rate in 2001 and 2008
Province
Population 2001 Population 2008 Ophthalmologists Surgeries CSR*
Total ≥50 years Total ≥50 years 2001 2008 2001 2008 2001 2008
BA† CABA‡ 16,587,449 4,262,528 17,952,101 4,416,742 2,023 2,242 35,000 123,288 2,110 6,868
Catamarca 333,661 58,800 380,612 70,658 2,013 2,016 420 123, 704 1,259 1,850
Chaco 967,396 157,117 1,042,881 183,328 2,048 2,056 600 2,706 620 2,595
Chubut 413,240 74,224 455,607 91,116 2,022 2,046 400 1,343 968 2,948
Cordoba 3,061,611 744,025 3,340,041 844,794 2,214 342 7,657 3,322§ 2,501 995§
Corrientes 929,236 160,954 1,002,416 183,487 2,055 2,084 600 1,110 646 1,107
Entre Ríos 1,156,799 256,988 1,242,547 293,570 2,077 2,091 1,625 2,146 1,405 1,727
Formosa 439,136 72,944 532,238 88,597 2,015 2,020 0 1,680 0 3,156
Jujuy 611,484 98,485 670,766 118,883 2,028 2,031 580 956 949 1,425
La Rioja 289,280 48,376 334,235 59,595 2,016 2,024 198 1,040 684 3,112
La Pampa 298,460 70,184 329,576 82,190 2,013 2,019 500 1,558 1,675 4,727
Mendoza 1,576,585 352,146 1,711,416 406,554 2,122 141 3,740 3,136 2,372 1,832
Misiones 963,869 130,403 1,061,590 172,154 2,030 2,033 250 304 259 286
Neuquen 473,315 73,542 538,952 98,054 2,028 2,067 860 3,342 1,817 6,201
Río Negro 552,677 105,259 594,189 128,206 2,041 2,047 750 785 1,357 1,321
Salta 1,079,420 171,078 1,202,753 203,523 2,056 2,064 1,220 1,521 1,130 1,265
San Juan 622,094 125,088 685,883 146,326 2,048 2,0 52 1,150 1,551 1,849 2,261
San Luis 366,900 72,468 428,025 88,304 2,037 2,0 46 600 1,558 1,635 3,640
Santa Cruz 197,000 30,770 221,871 38,934 2,023 2,031 219 463 1,112 2,087
Santa Fe 2,997,376 753,313 3,242,551 835,283 354 458 3,760 4,555 1,254 1,405
Santiago del Estero 806,347 145,009 856,739 156,774 2,044 2,053 840 1,881 1,042 2,196
Tierra del Fuego 100,960 11,466 126,212 17,759 2,010 2,011 170 223 1,684 1,767
Tucumán 1,142,105 246,927 1,457,357 293,785 100 123 1,600 6,790 1,401 4,659
Total 35,966,400 8,222,094 39,410,558 9,018,616 3,417 4,079 62,739 169,762 1,744|| 4,313||
*CSR= cataract surgical rate; †BA= Buenos Aires; ‡CABA= greater metropolitan area of Buenos Aires; §= data are incomplete, resulting in much lower estimates than expected ||= mean.
Figure 1. Map of Argentinean provinces.
Figure 2. Percentage changes in the number of cataract surgeries categorized by value.

Complexities and challenges of surgical data collection from cataract patients: comparison of cataract surgery rates between 2001 and 2008 in all provinces of Argentina
28 Arq Bras Oftalmol. 2014;77(1):25-9
in that year. The numbers of IOLs sold in 2009 and 2010 were 173,395 and 233,498, respectively.
DISCUSSIOnThis study represents the first national longitudinal survey of
ca taract surgery in a country (by province) of Latin America. Overall, the results demonstrated a large increase in the number of surgeries, particularly government-financed surgeries (from 5,762 to 14,006). The CSR increased from 2001 to 2008. However, this study highlights the difficulties in obtaining an accurate count of surgeries and, con-sequently, the CSR in some countries. This is important because the CSR is 1 of 3 components used to define the progress in national plans related to cataract blindness (the others are CSC and cataract surgical outcomes). Often, inaccurate CSRs are reported to be lower than the actual rate, so the situation appears worse than it actually is.
When CSR data for Argentina was published in 2010(12), IOL ma-nufacturers were contacted to assure that the data presented were reasonably accurate. Indeed, data were in good agreement with IOL sales data. However, when an update was recently requested, it was a surprise to find that figures from 2008 onward in Argentina had been enormously revised upward, largely because some sources had not been included. These revised figures suggested that approximately 52% IOLs were not accounted for in the actual number of surgeries reported in the initial 2008 survey. That is to say, more surgeries were performed than reported. The new IOL sales figures appear to be accurate because the 2008-2011 IOL sales data are all roughly in the same range, with some year-to-year fluctuations. Moreover, the data for PAMI is validated because PAMI manages cataract surgeries financed by the government on a contract basis to ophthalmologists, who cannot be paid without reporting surgeries directly to PAMI.
In 2008, it was estimated that Argentina had 128 ophthalmolo-gists per million population (approximately 5,400 in total for a popu-lation of 39.4 million) and a CSR of approximately 2,350 per million population(12). The more refined data presented in this study suggest that the number of ophthalmologists was considerably inflated; a more accurate total would be 4,100 (104 ophthalmologists per million population). Nevertheless, the trend toward an increased
number of ophthalmologists continues, and Argentina has one of the highest number of ophthalmologists per capita in Latin Ameri ca. Many ophthalmologists in Argentina do not perform cataract sur -gery. Many residencies are located in the private sector, where the majority of surgeries are performed by consultants nominated by patients and supported by insurance companies. Therefore, many residents work as clinical ophthalmologists rather than surgeons.
Using the revised IOL sales data, the true CSR for Argentina in 2008 was probably around 4,700, rather than the originally reported 2,350(12). On the basis of the most recent IOL sales report, it can be as-sumed that today’s CSR is approximately 5,000, which would actual ly place Argentina among the top CSR countries in Latin America.
This new method of CSR data collection was further validated by cross-checking CSR data with IOL inventories in Brazil, Peru, and Chile. According to industry reports, in Brazil, approximately 540,000 IOLs were imported by suppliers in 2011. In Peru, the reported number of IOLs sold in the country in 2010 was 45,500. In Chile, the estimated number of IOLs sold in the country was 65,000 in 2010. Therefore, working with an estimated population of 199.7 million in Brazil in 2011(13), the calculated CSR based on IOL sales would be 2,704 or almost exactly the same as that (2,700) reported recently to the WHO. Likewise, in Peru, the calculated rate based on a population of 29.4 million(13) would be 1,548 or close to the 1,400 reported that year. Fi-nally, in Chile, the calculated CSR would be 3,720 versus the reported 3,450, indicating a discrepancy of 7.8%. We therefore believe that the figures presented in this study were reasonably accurate. CSR accuracy depends on the number of surgeries reported and the po-pulation for a given year, which can vary considerably. For example, the Brazilian government’s estimate was approximately 191 million in 2011, while the UN’s estimate was near 200 million, which equates to a CSR difference of 123 (approximately a 4.5% variance).
Although it appears that the CSR in Argentina is much higher than believed, high CSR figures do not guarantee that individuals who need surgery actually undergo it because this metric is just a measure of cataract surgery consumption(12). Moreover, surgical outcomes have to be considered. For example, if 25% surgeries are not meeting the WHO criteria, then the CSR should be discounted accordingly. To some extent, CSC data can provide snapshots in time
Figure 3. The number of public surgeries as a percentage of the total number of surgeries performed in 2001 and 2008 by province.

Lansingh VC, et al.
29Arq Bras Oftalmol. 2014;77(1):25-9
of how many individuals are blind or visually impaired because of ca taract. In Argentina, many regions have not yet been surveyed.
There was a large increase in the number of IOLs sold in Argentina between 2001 and 2008, from approximately 80,000 to 187,000, but this increase likely occurred after the results of the first RACCS study(10) published in 2006 caused considerable alarm in the MOH. The MOH and PAMI then established a Prevention of Blindness Committee with a focus on cataract surgery. Based on recent IOL sales and data from PAMI, PAMI now finances up to 80,000 cataract surgeries per year. The MOH also supports public surgeries in provinces that do not have any kind of coverage. Both these developments highlight the importance of MOH involvement in developing countries to increase the number of cataract surgeries.
There are several potential reasons why the initial survey method used in Argentina underestimated the number of surgeries. First, the presence of multiple ophthalmological societies in the country com-plicated the process of obtaining accurate data, particularly in the greater Buenos Aires area. For example, the number of ophthalmo-logists may be double-counted, and some ophthalmologists do not belong to either organization or are not board-certified. Second, and perhaps most importantly, private practitioners in ophthalmology may be afraid to fully report the number of cataract surgeries perfor-med for various reasons such as taxation.
Therefore, a complete survey of Argentina by province demons-trated that the CSR increased impressively between 2001 and 2008. However, cross-checks with in-country IOL sales and PAMI data in -di cated that our previous reporting system was considerably unde-restimating the number of cataract surgeries. The method used in this study is now more aligned with the system successfully used in other Latin American countries and is more accurate because the number of surgeries reported can be validated with the number of IOLs sold. The findings of this study are being released simultaneously with the recent WHO mandate for governments to report CSRs. While this will facilitate future data collection in the public sector, it is necessary to note that in many countries such as Argentina, the ma jority of cata-ract surgeries are conducted in the private sector. As such, a reporting mechanism for private practitioners needs to be developed so that they are motivated to contribute their surgical data to the national statistics.
ACKnOWLeDGeMenTSThe authors would like to thank Nora Luedicke and Rosario Bar-
renechea of the Programa Nacional de Salud Ocular y Prevención de la Ceguera, Ministerio de Salud de la Nación, Buenos Aires, Argentina for help in collecting data on public surgeries. The authors would also like to thank all the ophthalmologists who helped in collecting
data: Dr. Carlos Laje, Dr. Carlos Alberto Carranza, Dr. Emma Sonzini, Dr. Victor Forcada, Dr. Hernan Gras, Dr. Juliet Gras, Dr. Maria Alejandra Carrasco, Dr. Oscar Moretti, Dr. Christian Larrañaga, Dr. Osvaldo Roux, Dr. Cristina Aguado Casal, Dr. Manuel Flores, Dr. Raúl Ruffa, Dr. Nélida Rosso Nano, Dr. Ignacio Lichinsky, Dr. Jorge Lichinsky, Dr. Diana G. De Waisman, Dr. Myriam Berman, Dr. Isabel F. Roman, Dr. Elbio Her-nández, Dr. Juan Carlos Casanovas, Dr. Joaquín Baffaluy, Dr. García Castellanos, Dr. Alberto Cruz, Dr. Richard Rubens Cárdenas, Dr. Jorge Echeverría, Dr. Pablo Emilio Passone, Dr. Patricia Larcher, Dr. Teresa Airasca, Dr. Fernando Suárez, Dr. Carlos Zarif, Dr. Ernesto Ferrer, Dr. Antonio Anzalaz, Dr. Héctor Vega Fernández, Dr. Bárbara Ventura, Dr. Gustavo Alarcón, Dr. Jorge Kleisinger, Dr. Horacio Martínez, and Dr. Italo Horacio Di Biase. Finally, the authors thank ORBIS for their financial support.
ReFeRenCeS 1. Pesudovs K. Patient-centred measurement in ophthalmology-a paradigm shift. BMC
Ophthalmol. 2006;6:25. Review. 2. Lansingh VC, Carter MJ, Martens M. Global cost-effectiveness of cataract surgery.
Ophthalmology. 2007;114(9):1670-8. 3. Lewallen S, Williams TD, Dray A, Stock BC, Mathenge W, Oye J, et al. Estimating in cidence
of vision-reducing cataract in Africa: a new model with implications for program tar-gets. Arch Ophthalmol. 2010;128(12):1584-9.
4. World Health Organization. Estimating cataract surgical services in national programs. Version 1.02, December 2001. [Programmed by Hans Limburg]. Geneva: World Health Organization. 2001 [cited 2013 May 2]. Available from: http://www.who.int/ncd/vision2020_actionplan/documents/raccs/manuals/RACSSDOSManuaEngl.pdf
5. Kuper H, Polack S, Limburg H. Rapid assessment of avoidable blindness. Community Eye Health. 2006;19(60):68-9.
6. Lundström M, Stenevi U, Thorburn W. The Swedish National Cataract Register: A 9-year review. Acta Ophthalmol Scand. 2002;80(3):248-57.
7. Johnston RL, Sparrow JM, Canning CR, Tole D, Price NC. Pilot National Electronic Ca-taract Surgery Survey: I. Method, descriptive, and process features. Eye (Lond). 2005; 19(7):788-94.
8. Jaycock P, Johnston RL, Taylor H, Adams M, Tole DM, Galloway P, Canning C, Sparrow JM; UK EPR user group. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye (Lond). 2009;23(1):38-49.
9. Murthy G, Gupta SK, John N, Vashist P. Current status of cataract blindness and Vision 2020: the right to sight initiative in India. Indian J Ophthalmol. 2008;56(6):489-94.
10. Nano ME, Nano HD, Mugica JM, Silva JC, Montaña G, Limburg H. Rapid assessment of visual impairment due to cataract and cataract surgical services in urban Argentina. Oph thalmic Epidemiol. 2006;13(3):191-7.
11. Kleisinger JE, Nano ME, Lansingh VC, et al. Estimating the number of cataract sur-geries needed in the Chaco province of Argentina using various visual acuity (VA) thresholds and CSC. Ophthalmol Clin Exp. 2010;4(2):61-3.
12. Lansingh VC, Resnikoff S, Tingley-Kelley K, Nano ME, Martens M, Silva JC, et al. Cata ract surgery rates in latin america: a four-year longitudinal study of 19 countries. Oph thalmic Epidemiol. 2010;17(2):75-81.
13. United Nations Department of Economic and Social Affairs. World population pros-pects: the 2010 revision. United Nations. 2010 [cited 2013 May 2]. Available from: http://esa.un.org/unpd/wpp/Excel-Data/population.htm.

30 Arq Bras Oftalmol. 2014;77(1):30-3
Original Article
InTRODUCTIOnPotential sight-threatening complications may occur if ocular in -
flam mation is not diagnosed and treated early in the course of disea-se(1-5). However, initial evaluation of patients with uveitis is frequently conducted in nonspecialized centers because intraocular inflamma-tion usually produces nonspecific symptoms such as pain, photopho-bia, redness, blurred vision, and floaters, which may easily be confused with other disorders(2,6). In Brazil, uveitis is one of the main diagnoses in patients who attend institutions for visual rehabilitation(7) and accounts for up to 7.4% visits to emergency eye care units.(8-11).
The etiology of uveitis can be broadly categorized into infectious and noninfectious, and it is frequently associated with systemic disea-se(12). Several studies have investigated the epidemiology of uveitis, showing variations in etiology according to geographical region, gender, ethnicity, age, social aspects, and immunological factors. However, most of these studies have included patients from tertiary
uveitis centers and may have been influenced by selection bias(1,4,13-18). Globally, anterior uveitis accounts for the majority of cases(1,4,17,18). Ho-wever, posterior uveitis is the most common presentation in Brazilian patients, with toxoplasmic retinochoroiditis being the most frequent identifiable cause(14-16).
Identification of clinical and epidemiological patterns of uveitis is crucial to devise strategies for preventing late diagnosis and facili-tating prompt treatment. Therefore, this study aimed to analyze the clinical and epidemiological characteristics of patients with uveitis who visited an emergency eye care center.
MeTHODSThis prospective study included patients with a clinical diagnosis
of active uveitis who were treated between May 2012 and July 2012 in the emergency eye care center of Fundação Altino Ventura, a reference eye hospital for patients from the public health system of
Clinical and epidemiological characteristics of patients with uveitis in an emergency eye care center in BrazilCaracterísticas clínicas e epidemiológicas das uveítes em um serviço de urgência oftalmológica no Brasil
eduardo nery roSSi caMilo1, GuilherMe lucena Moura1, TiaGo euGênio Faria e aranTeS1,2
Submitted for publication: June 13, 2013 Accepted for publication: October 02, 2013
Study was carried out at Fundação Altino Ventura. 1 Fundação Altino Ventura, Recife, PE, Brazil.2 Hospital de Olhos de Pernambuco, Recife, PE, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: E.N.R. Camilo, None; G.L. Moura, None; T.E. Faria e Arantes, None.
Correspondence address: Eduardo Nery Rossi Camilo. Fundação Altino Ventura, 170 - Recife (PE) - 50070-040 - Brazil - E-mail: [email protected]
The study was approved by Institutional Ethics Committee (Fundação Altino Ventura, no 053/2011).
ABSTRACTPurpose: To analyze the clinical and epidemiological characteristics of patients with uveitis in an emergency eye care center.Methods: We conducted a prospective, observational study of patients with active uveitis admitted between May 2012 and July 2012 to an emergency eye care center.Results: The majority of patients were male (63.2%), with a mean age of 43.2 years; 66.2% patients were of mixed ethnicity, 22.5% were Caucasian, and 11.3% were black. Anterior uveitis was observed in 70.1% patients, posterior uveitis in 26.5%, and panuveitis in 3.4%; no patient was diagnosed with intermediate uveitis. All patients had a sudden and acute presentation. The most frequent symptoms were ocular pain (76.9%), redness (59.8%), and visual blurring (46.2%). The majority of patients had unilateral disease (94.9%) with a mean symptom duration of 6.2 days. Diffuse and anterior uveitis were associated with ocular pain (p<0.001). Scotomata and floaters were more frequent in patients with posterior uveitis (p=0.003 and p=0.016, respectively). Patients with anterior uveitis presented with better visual acuity (p=0.025). Granulomatous keratotic precipitates were more frequent in patients with posterior uveitis (p=0.038). An etiological diagnosis based on the evaluation at the emergency center was made in 45 patients (38.5%). Conclusions: Acute anterior uveitis was the most frequent form of uveitis. Initial patient evaluation provided sufficient information for deciding primary therapy and aided in arriving at an etiological diagnosis in a considerable number of patients.
Keywords: Uveitis/etiology; Uveitis/epidemiology; Uveitis/diagnosis; Uveitis/clas-sification; Emergencies
RESUMOObjetivo: Analisar as características clínicas e epidemiológicas das uveítes em um serviço de atendimento oftalmológico de urgência.Métodos: Estudo prospectivo, observacional de pacientes com uveíte ativa admitido entre maio e julho de 2012, em um serviço de atendimento oftalmológico de emergência.Resultados: A maioria dos pacientes eram do sexo masculino (63,2%) e a média de idade foi de 43,2 anos; 66,2% dos pacientes tinham etnia mista, 22,5% eram brancos e 11,3% negros. Uveíte anterior foi observada em 70,1% dos pacientes, uveíte posterior em 26,5%, e panuveíte em 3,4%, nenhum foi diagnosticado com uveíte intermediária. Todos os pacientes tiveram apresentação súbita e aguda. Os sintomas mais frequentes foram: dor ocular (76,9%), hiperemia conjuntival (59,8%) e baixa visual (46,2%). A maio-ria dos pacientes tinha doença unilateral (94,9%), com duração média dos sintomas de 6,2 dias. Uveítes anteriores e difusas foram associadas com dor ocular (p<0,001). Escotomas e a “floaters” foram mais frequentes na uveíte posterior (p=0,003 e p=0,016, respectivamente). Pacientes com uveíte anterior apresentaram melhor acuidade visual (p=0,025). Precipitados ceráticos granulomatosos foram mais frequentes em pacientes com uveíte posterior (p=0,038). Um diagnóstico etiológico com base na avaliação inicial no serviço de emergência foi possível em 45 pacientes (38,5%).Conclusão: A uveíte anterior aguda foi a uveíte mais frequentemente encontrada no serviço de urgência oftalmológica. A avaliação inicial do paciente forneceu informações suficientes para a conduta terapêutica primária, e possibilitou diagnóstico etiológico em um número considerável de pacientes.
Descritores: Uveíte/etiologia; Uveíte/epidemiologia; Uveíte/diagnóstico; Uveíte/ clas -sificação; Emergência

Camilo ENR, et al.
31Arq Bras Oftalmol. 2014;77(1):30-3
the state of Pernambuco, Brazil, which admits self-referred and pro-fessionally referred patients in all levels of care. Disease activity was defined by the presence of anterior chamber reaction, retinal or cho-roidal inflammation, and/or vitreous inflammation (if associated with macular edema or vasculitis). Patients with no signs of inflammatory activity of uveitis, those who had visited an outpatient uveitis clinic in the 3 months prior to consultation in the emergency department, those with a history of ocular trauma, and those with an uncertain diagnosis of uveitis were excluded.
The demographic and ophthalmological variables evaluated in -cluded age, gender, race, residence, symptoms, duration of symptoms, number of previous episodes, and clinical data from the ocular examination. Physical examination included presenting visual acuity (VA) measurement, external eye examination, slit-lamp biomicrosco-py, indirect ophthalmoscopy, and applanation tonometry. Ancillary investigations were requested at the discretion of the examiners. Specific etiological diagnoses, when available, were based on the clinical data collected and tests requested at the initial consultation.
Anatomical and clinical classifications were determined accor-ding to established standard classification systems(12,19). Only one eye of each patient was included in the analysis; in cases of bilateral invol-vement, the eye with more severe disease (higher grade of anterior chamber reaction or worse VA if the inflammation was symmetrical) was analyzed.
Statistical analysis was performed using SPSS 16.0 for Windows (SPSS Inc, Chicago, Illinois, USA). Continuous variables are expressed as means ± standard deviations, while categorical data are presen-ted as frequencies. Relationships between categorical variables were assessed using Fisher’s exact test. Analysis of variance (ANOVA) and Student’s t test were used for the analysis of continuous va -ria bles. A P-value of <0.05 was considered statistically significant. The study was approved by the Institutional Review Board of Funda-ção Altino Ventura (#053/2011). All patients signed a written informed consent form for this research.
ReSULTSDuring the period from May 2012 to July 2012, 480 patients with
uveitis were examined in the emergency eye care center of Fundação Altino Ventura. Among these, 117 who had active uveitis and fulfilled the study requirements were included in the analysis. The mean age of the evaluated patients was 43.2 ± 18.3 years, and 74 (63.2%) were male. Demographic data are shown in Table 1. There were no diffe-rences in the distribution of gender, race, and residence in relation to the anatomical classification of uveitis (p>0.05).
Anterior uveitis was observed in 82 patients (70.1%), posterior uveitis in 31 (26.5%), and diffuse uveitis in 4 (3.4%); none of the pa-tients were diagnosed with intermediate uveitis (Table 2). All patients presented with sudden and acute symptoms (less than 3 months du-ration). Patients with posterior uveitis were younger than those with either anterior uveitis or diffuse uveitis (47.6 ± 17.0 years, 31.3 ± 16.1 years, and 46.0 ± 24.2 years, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p<0.001).
The most common symptoms observed were eye pain (n=90, 76.9%), redness (n=70, 59.8%), and visual blurring (n=54, 46.2%). The majority of patients had unilateral disease (n=111, 94.9%), with a mean symptom duration of 6.2 ± 6.3 days. Eleven patients (9.4%) had a previous diagnosis of uveitis and reported 1 to 5 previous epi-sodes. None of the patients was being treated for uveitis at the time of evaluation; however, one patient was being treated for iatrogenic conjunctivitis.
The clinical characteristics of the patients and the physical exami-nation findings are presented in Tables 3 and 4, respectively. Anterior and diffuse uveitis were associated with complaints of eye pain (86.6%, 48.4%, and 100.0%, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p<0.001). Scotomata were more frequent
in patients with posterior uveitis (1.2%, 19.4%, and 0.0%, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p=0.003). Com -plaints about floaters were associated with posterior uveitis (1.2%, 16.1%, and 0.0%, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p=0.016). Blurred vision was uncommon in patients with anterior uveitis when compared with inflammation at other sites (30.5%, 80.6%, 100.0%, respectively, for anterior uveitis, posterior uvei-tis, and diffuse uveitis; p<0.001). There was no significant association between the frequency of redness, photophobia, and photopsia with the anatomical classification of uveitis (p>0.05).
Patients with anterior uveitis showed better presenting VA (VA >20/63 in 57.0%, 38.7%, and 0.0%, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p=0.025). Conjunctival hype-remia was more common in patients with anterior uveitis (91.5%, 64.5%, and 75.0%, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p=0.003). Patients with granulomatous keratotic precipitates were most often diagnosed with posterior uveitis (3.7%, 19.4%, and 0.0%, respectively, for anterior uveitis, posterior uveitis, and diffuse uveitis; p=0.038). There was no association of the fre-quency of posterior synechiae, fine keratotic precipitates, iris nodules, and anterior chamber cells grade with the anatomical classification of uveitis (p>0.05). The mean intraocular pressure at presentation was 13.9 ± 7.2 mmHg (range, 2.0 to 40.0 mmHg), and there was no sta-tistical association between intraocular pressure and the anatomical classification of uveitis (p=0.598).
Table 1. Demographic characteristics of patients with active uveitis treated at the emergency eye care center of Fundação Altino Ventu-ra, Recife, Brazil, between March and July 2012 (n=117)
Age (years)
Mean ± standard deviation, (range) 43.2 ± 18.3 (8 - 89)
Gender [n (%)]
Female 43 (36.8)
Male 74 (63.2)
Ethnicity [n (%)]†
Caucasian 16 (22.5)
Black 08 (11.3)
Mixed race 47 (66.2)
Place of residence [n (%)]†
Recife 24 (33.8)
Other cities in the metropolitan region 27 (38.0)
Other cities in states 19 (26.8)
Other states 01 (01.4)†= data on ethnicity and residence were not collected for 46 patients (n =71).
Table 2. Anatomical classification and frequency of determination of a cause or clinical syndrome on the basis of initial evaluation of 117 patients with active uveitis treated at the emergency eye care center of Fundação Altino Ventura, Recife, Brazil between March and July 2012 [n (%)]
Anatomical classificationTotal patients
n (%) Patients with specific diagnoses
n (%)
Anterior uveitis 082 (070.1) 14 (017.1)
Intermediate uveitis 000 (000.0) 00 (000.0)
Posterior uveitis 031 (026.5) 27 (087.1)
Panuveitis 004 (003.4) 04 (100.0)
Total 117 (100.0) 45 (038.5)

Clinical and epidemiological characteristics of patients with uveitis in an emergency eye care center in Brazil
32 Arq Bras Oftalmol. 2014;77(1):30-3
Etiological diagnosis was established in 45 patients (38.5%) on the basis of the clinical evaluation and ancillary laboratory tests re quested at the initial visit. Among the 82 patients with anterior uveitis, 68 (82.9%) had an unknown etiology (of these, 63 had their first episode of anterior uveitis and were not investigated), 8 (9.8%) had uveitis associated with rheumatological disease, and 6 (7.3%) had a herpetic etiology. Among the 31 patients with posterior uveitis, 26 (87.1%) had an etiological diagnosis established during the initial visit, 25 (83.9% of posterior uveitis) had toxoplasmic retinochoroidits, and 1 (3.2%) patient had herpetic retinitis (acute retinal necrosis). Among the 4 patients with diffuse uveitis, 2 (50%) were diagnosed with Vogt-Koyanagi-Harada disease, 1 (25%) with fungal endophthal-mitis, and 1 (25%) with hypersensitivity uveitis caused by a corneal bee sting (Table 2).
DISCUSSIOnThis study prospectively evaluated patients from an emergency
eye care center, in contrast to most uveitis epidemiological studies that have been conducted retrospectively in tertiary specialized cen-ters(1,4). In previous studies from referring uveitis centers in Brazil, in-cluding our institution, posterior uveitis accounted for the majority of cases, particularly toxoplasmosis(14-16). In contrast, anterior uveitis was responsible for 70.1% patients in our study. This can be explained by the fact that our sample mostly included individuals with first-epi sode anterior uveitis; these patients are typically not referred to specialized centers for investigation. The high frequency of anterior uveitis was in accordance with that reported in studies conducted in specialized uveitis centers in other countries(1,4,17) and studies conduc-ted in community-based eye care centers(18).
The mean age of patients in this study (42.6 years) was higher than that reported in a previous study conducted at our institution betwe-en 1998 and 1999 (32.1 years)(14) and in studies conducted in re ferring centers in Colombia and Tunisia (31.7 and 34.0 years, respectively)(13,17). Nevertheless, the mean age of patients in the present study was similar to that in studies from North America (45 years)(18) and Sou-theastern Brazil (41 years)(16). Most patients in our study were working adults, similar to the patients in the previous studies. The incidence of uveitic entities has been associated with ethnicity(1,4); however, we could not find such an association, possibly because of the mixed race background of the Brazilian population.
The most frequently reported symptoms were pain, redness, blur-red vision, and photophobia. Such symptoms are nonspecific and can be easily misdiagnosed as other conditions, including conjuncti vitis and keratitis(6). Anterior uveitis was associated with a higher fre quen-cy of redness and pain, while posterior uveitis was greatly associated with blurred vision and scotomata. Granulomatous keratotic precipi-tates were most common in patients with the primary site of inflam-mation in the posterior segment. Therefore, an accurate medical his tory and physical examination are imperative for establishing a diag nosis in patients with uveitis.
Determination of a cause or clinical syndrome on the basis of cli-nical presentation and ancillary examination requested at the initial visit was possible in 38.5% patients, a diagnostic rate lower than that observed in community-based, comprehensive ophthalmological units and uveitis referral centers (46% to 79.4%)(1,4,13,17,18). In this study, first-episode acute anterior uveitis accounted for the majority of cases. It should be noted that further investigations are usually not per-formed in patients presenting with the first episode of uncomplica-ted anterior uveitis(20), which explains the high frequency of uveitis of unknown etiology.
This research mostly included patients who were visiting the hos-pital for the first time, and the onset and course of disease were based on symptomatology, which can lead to misclassification. For example, a patient with an exacerbation of undiagnosed chronic uveitis could have been incorrectly diagnosed with sudden-onset acute uveitis(18). Another limitation of this study was the small sample size, which may have restricted the inclusion of less common uveitic entities.
Table 3. Clinical characteristics of patients with active uveitis treated at the emergency eye care center of Fundação Altino Ventura, Recife, Brazil between March and July 2012 (n=117)
Laterality [n(%)]
Unilateral 111 (94.9)
Bilateral 006 (05.1)
Duration of symptoms (days)
Mean ± standard deviation, (range) 6.2 ± 6.3 (1 - 30)
Symptoms [n (%)]
Blurred vision 054 (46.2)
Redness 070 (59.8)
Pain 090 (76.9)
Photophobia 031 (26.5)
Scotomas 007 (06.0)
Floaters 006 (05.1)
Fotopsias 002 (01.7)
Previous diagnosis of uveitis [n (%)] 011 (09.4)
Table 4. Ocular examination findings of the patients with active uveitis treated at the emergency eye care center of Fundação Altino Ventura, Recife, Brazil between March and July 2012 (n=117)
Visual acuity [n (%)]†
>20/63 57 (50.0)
20/63 to 20/200 29 (25.4)
<20/200 28 (24.6)
Anterior segment [n (%)]
Conjunctival hyperemia 98 (83.8)
Fine keratic precipitates 48 (41.0)
Granulomatous keratic precipitates 09 (07.7)
Corneal edema 19 (16.2)
Keratitis 10 (08.5)
Posterior synechiae 24 (20.5)
<180o 15 (12.8)
>180o 09 (07.7)
Iris nodules 01 (00.9)
Anterior chamber cell reaction‡
0+ cells 10 (08.8)
0.5 to 2+ cells 63 (55.3)
>2+ cells 41 (36.0)
Hypopyon 03 (02.6)
Posterior segment [n (%)]§
Vitreous opacity 24 (21.6)
Retinochoroiditis 24 (21.6)
Retinitis 01 (00.9)
Exudative retinal detachment 02 (01.8)
Intraocular pressure (mmHg)¶
Mean ± standard deviation, (range) 13.9 ± 7.2 (2.0 - 40.0)†= visual acuity measurement was not possible in 3 patients (n=114); ‡= evaluation of anterior chamber reactions was not possible in 3 patients (n=114); §= evaluation of pos-terior segment was not possible in 6 patients (n=111); ¶= applanation tonometry was not possible in 18 patients (n=99).
Camilo ENR, et al.
33Arq Bras Oftalmol. 2014;77(1):30-3
In conclusion, this study shows that anterior uveitis is observed more frequently in primary health care centers than in tertiary referral centers. Initial evaluation of the patient in the emergency room pro-vided sufficient information for deciding primary therapy and aided in arriving at an etiological diagnosis in a considerable number of patients. These findings are important for prioritization of education and training for general ophthalmologists.
ReFeRenCeS 1. Chang JH, Wakefield D. Uveitis: a global perspective. Ocul Immunol Inflamm. 2002;
10(4):263-79. Review. 2. Gutteridge IF, Hall AJ. Acute anterior uveitis in primary care. Clin Exp Optom. 2007;
90(5):390; author reply 390. 3. Prieto-del-Cura M, González-Guijarro J. [Complications of uveitis: prevalence and risk
factors in a series of 398 cases]. Arch Soc Esp Oftalmol. 2009;84(10):523-8. Spanish. 4. Rathinam SR, Namperumalsamy P. Global variation and pattern changes in epidemio-
logy of uveitis. Indian J Ophthalmol. 2007;55(3):173-83. Review. 5. Durrani OM, Meads CA, Murray PI. Uveitis: a potentially blinding disease. Ophthalmo-
logica. 2004;218(4):223-36. Review. 6. Mahmood AR, Narang AT. Diagnosis and management of the acute red eye. Emerg
Med Clin North Am. 2008;26(1):35-55, vi. Review. 7. Kara-José N, Carvalho KM, Pereira VL, Venturini NH, Gasparetto ME, Gushiken MT.
[Retrospective study of first 140 cases attended the Clinica de Visäo Sub-Nor mal of the Hospital de Clínicas da Unicamp]. Arq Bras Oftalmol. 1988;51(2):65-9. Portuguese.
8. Carvalho Rde S, José NK. Ophthalmology emergency room at the University of São Paulo General Hospital: a tertiary hospital providing primary and secondary level care. Clinics (Sao Paulo). 2007;62(3):301-8.
9. Campos Júnior JC. [Profile of ophthamological attendance of emergency]. Rev Bras Oftalmol. 2004;63(2):89-91. Portuguese.
10. Kumar NL, Black D, McClellan K. Daytime presentations to a metropolitan ophthalmic emergency department. Clin Experiment Ophthalmol. 2005;33(6):586-92.
11. Pierre Filho PT, Gomes PR, Pierre ET, Pinheiro Neto FB. [Profile of ocular emergencies in a tertiary hospital from Northeast of Brazil]. Rev Bras Oftalmol. 2010;69(1):12-7. Por-tuguese.
12. Deschenes J, Murray PI, Rao NA, Nussenblatt RB; International Uveitis Study Group. International Uveitis Study Group (IUSG): clinical classification of uveitis. Ocul Immu-nol Inflamm. 2008;16(1):1-2.
13. de-la-Torre A, López-Castillo CA, Rueda JC, Mantilla RD, Gómez-Marín JE, Anaya JM. Clinical patterns of uveitis in two ophthalmology centres in Bogota, Colombia. Clin Experiment Ophthalmol. 2009;37(5):458-66.
14. Diniz JR, Toscano JL, Campelo DE, Delgado AC, Leal SD. [Occurency of uveitis in Per -nambuco state, Brazil]. Rev Bras Ciênc Saúde. 2001;5(1):59-64. Portuguese.
15. Gehlen ML, Dabul VM, Obara SS, Grebos SP, Moreira CA. [Incidence and etiology of uveitis in Curitiba]. Arq Bras Oftalmol. 1999;62(5):622-6. Portuguese.
16. Gouveia EB, Yamamoto JH, Abdalla M, Hirata CE, Kubo P, Olivalves E. [Causes of uveitis in a tertiary center in São Paulo city, Brazil]. Arq Bras Oftalmol. 2004;67(1):139-45. Portuguese.
17. Khairallah M, Yahia SB, Ladjimi A, Messaoud R, Zaouali S, Attia S, et al. Pattern of uveitis in a referral centre in Tunisia, North Africa. Eye (Lond). 2007;21(1):33-9.
18. McCannel CA, Holland GN, Helm CJ, Cornell PJ, Winston JV, Rimmer TG. Causes of uveitis in the general practice of ophthalmology. UCLA Community-Based Uveitis Study Group. Am J Ophthalmol. 1996;121(1):35-46.
19. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Re-sults of the First International Workshop. Am J Ophthalmol. 2005;140(3):509-16. Review.
20. Forooghian F, Gupta R, Wong DT, Derzko-Dzulynsky L. Anterior uveitis investigation by Canadian ophthalmologists: insights from the Canadian National Uveitis Survey. Can J Ophthalmol. 2006;41(5):576-83.
XXI Simpósio Internacional de Atualização em Oftalmologia da Santa Casa de São Paulo
28 a 31 de maio de 2014Centro de Convenções do Clube A Hebraica
São Paulo - SP
informações: E-mail: [email protected]
JDE Eventos - Tels.: (11) 5084-5284 / 508 4-9174Site: http://www.oftalmosantacasa.com.br
34 Arq Bras Oftalmol. 2014;77(1):34-9
Original Article
InTRODUCTIOnFor many decades, researchers worldwide have been investiga-
ting the causes of retinopathy of prematurity (ROP) and the best method to identify the preterm children that are at risk of developing this disease(1-9). In 2007, one ROP research group in Brazil published the criteria for se lecting premature children for examination and ROP treatment, following the assessment of regional characteristics of the disease in Brazil(10).
At present, the analysis of the results of visual functions (VF) of pre -mature infants, i.e., visual acuity, chromatic and contrast discrimination, visual field, stereopsis, and ocular motility, has contributed to unravel the influence of ROP and its treatment on these functions. The effects of developmental conditions during the neonatal period (ROP deve-lopment, low birth weight, gestational weight and age above the ex-pected for ROP development, presence of neonatal complications, and brain damage) on visual functions have not yet been elucidated(11-16).
Comparative study of visual functions in premature pre-school children with and without retinopathy of prematurity Estudo comparativo das funções visuais em pré-escolares nascidos prematuros com e sem retinopatia da prematuridade
líGia beaTriz bonoTTo1, ana Tereza raMoS Moreira2, Silvia chuFFi3, SuSana Maria biTTencourT ScKudlareK3
Submitted for publication: August 21, 2012 Accepted for publication: October 2, 2013
Study carried out at Hospital de Olhos Sadalla Amin Ghanem, Joinville - Santa Catarina (SC), Brazil.1 Hospital de Olhos Sadalla Amin Ghanem; UTI Neonatal da UNIMED, Joinville, Santa Catarina,
(SC), Brazil.2 Universidade Federal do Paraná, PR, Brazil; Hospital de Olhos do Paraná, Curitiba (PR), Brazil.3 Hospital de Olhos Sadalla Amin Ghanem, Joinville, Santa Catarina (SC), Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: L.B. Bonotto, None; A.T.R. Moreira, None; S. Chuffi, None; S.M.B. Sckudlarek, None.
Correspondence address: Lígia Beatriz Bonotto. Rua Abdon Batista, 146 - Joinville (SC) - 89201-010 - Brazil - E-mail: [email protected] ou [email protected]
Projeto aprovado pelo CEP do Hospital São José, Joinville - S/C.
ABSTRACTPurpose: Observe whether there are differences in visual functions among pre -mature infants with treated retinopathy of prematurity (ROP) in relation to preterm infants with ROP and spontaneous regression; and among these two groups with ROP and the control group without ROP. Methods: Cross-sectional observational no blind study. Premature infants were born between 06/1992-06/2006 and were exam between 06/2009-12/2010; re-gistered in data of Hospital de Olhos Sandalla Amin Ghanem; with gestational age less than or equal to 32 weeks and 1,599 g born weigh; without ROP and ROP stages II or III, in one of the eyes, with spontaneous regression or with treatment; at least three visits during the se lection period at maximum 6 months in the first exam and minimum 4 years of age in reassessment (chronological age) were in-clude. Premature that did not respond or were not located for reassessment and those that did not have conditions to do the exams were exclude. Study’s groups: G1- ROP post-treatment; G2-ROP post-spontaneous regression; G3- without ROP (control). Visual function evaluated with visual acuity (VA), contrast sensitivity test (CST), color test (CT), eye movement, stereopsis. Results: Overall, there were 24 premature infants and 48 eyes. Normal VA: 64.28% (G1), 87.5% (G2) and 100% (G3); Normal CST: 66.67% (G1), 100% (G2) and 55.56% (G3); Normal Ishihara CT: 100% (G1 and G2) and 86% (G3); Normal Farnsworth CT: 20% (G1), 75% (G2) and 50% (G3). Normal stereoacuity: 0.00% (G1); 25% (G2) and 3.5% (G3). Strabismus: 37% (G2), 0.00% (G1 and G3). The prevalent tendency for lower response in CST and CT between the premature children in group G3 and Farnsworth color test in G1 is a curious result of this work and more study is necessary about these visual functions in older premature children. Conclusion: The visual functions showed no statistically significant difference among the groups studied.
Keywords: Infant, premature; Infant, premature, diseases; Retinopathy of prema-turity; Visual acuity; Child, preschool
RESUMOObjetivo: Observar se há diferença nas funções visuais entre os prematuros com retinopatia da prematuridade (ROP) pós-tratamento em relação aos prematuros com retinopatia da prematuridade pós-regressão espontânea. E entre cada um destes grupos com o controle sem ROP. Métodos: Estudo transversal, observacional, não cego. Incluídas crianças prematuras nascidas entre 06/1992-06/2006 e examinadas entre 06/2009 e 12/2010; idade gestacional menor ou igual a 32 semanas e peso ao nascimento menor ou igual a 1.599 g; cadastrados no banco de dados do Hospital de Olhos Sandalla Amin Ghanem; com diagnóstico de retinopatia estágio II ou III em pelo menos um dos olhos com regressão espontânea ou por tratamento da ROP e sem retinopatia da prematuridade; mínimo de três consultas no período de seleção; máximo de seis meses de idade cronológica para o primeiro exame no HOSAG; idade cronológica mínima de quatro anos no período da reavaliação. Foram excluídas crianças prematuras que não responderam ou não foram localizados para os exames de reavaliação; e que não ofereciam condições de realização dos exames, por apresentarem comprometimento seve ro do sistema nervoso central ou síndromes impeditivas. Os prematuros foram divididos em três grupos: G1- prematuros com ROP pós-tratamento; G2- com ROP pós-regressão espontânea; e G3- sem ROP. Função visual avaliada por meio da acuidade visual (AV), teste de sensibilidade ao contrate (TSC), teste de cores (TC), exame de motricidade ocular e estereopsia. Resultados: Foram examinados 24 prematuros (48 olhos). No grupo G1 formado por 7 prematuros; G2, 8 prematuros e G3, 9 prematuros. AV normal: 64,28% (G1), 87,5% (G2) e 100% (G3); TSC normal: 66,67% (G1), 100% (G2) e 55,56% (G3); TC de Ishihara normal, 100% (G1 e G2) e 86% (G3); TC de Farnsworth normal: 20% (G1), 75% (G2) e 50% (G3). Estereopsia normal: 0,00% (G1), 25% (G2) e 3,5% (G3). Estrabismo: 37% (G2), 0,00% (G1 e G3). A prevalente tendência de respostas abaixo do esperado no TSC e TC entre os prematuros do grupo G3 exige novos estudos sobre o assunto em prematuros com maior idade. Conclusão: As funções visuais não apresentaram diferença entre os três grupos de prematuros estudados.
Descritores: Prematuro; Doenças do prematuro; Retinopatia da prematuridade; Acuidade visual; Pré-escolar

Bonotto LB, et al.
35Arq Bras Oftalmol. 2014;77(1):34-9
The knowledge of the risk factors for VF among premature infants is important for the selection of those who need to be followed up after the neonatal period.
This study aimed to determine possible differences in VF between premature infants at ROP stages II and III and premature infants with spontaneous remission of ROP stages II and III, and compare each of these groups with a group without ROP.
MeTHODS This was an observational, nonblinded, cross-sectional study
of the VF responses of premature infants registered in the database of the Hospital de Olhos Sadalla Amin Ghanem (HOSAG). HOSAG da tabase comprised children born before 36 weeks of gestation, ac-cording to the definition of prematurity of the World Health Organi-zation(17). The premature infants were selected from the Darcy Vargas Maternity, in Joinville, and from other regions in the state of Santa Catarina, for follow-up after being discharged from the institution where their delivery was conducted. They were classified and treated for ROP according to the International Committees in force during the selection period (06/1992 - 06/2006)(7-9). During the re-evaluation period (06/2009 - 12/2010), the infants who fulfilled the criteria of the study underwent eye examinations at HOSAG. The following in-clusion criteria were used: premature infants born between 06/1992 and 06/2006, gestational age ≤32 weeks and birth weight ≤1,599 g, absence of ROP, occurrence of ROP in stages II or III with spontaneous remission or remission by cryotherapy or laser treat ment in at least one eye, minimum of three medical consultations during the selec-tion period, maximum chronological age of 6 months at the time of the first examination at HOSAG (selection period), and minimum chronological age of 4 years during the re-evaluation period. The exclusion criteria were: infants who did not respond or were not followed up for the re-evaluation tests, and those who did not fulfill the criteria for VF assessment because of severe impairment of the central nervous system or syndromes that hindered the performance of the tests.
Infants were divided into three groups: G1, premature infants with ROP, stages II and III, treated by laser or cryotherapy; G2, prema-ture infants with ROP, stages II and III, with spontaneous remission; and G3, premature infants without ROP (control).
Re-eVALUATIOn TeSTS
distance visual acuity (va)After appropriate optical correction, each eye was separately exa mi-
ned according to a multiethnic pediatric eye disease study (MEPEDS) with preschool children, published in 2009, in which VA better or equal to 20/30 Snellen (or 0.67 in decimal or 0.18 in logMAR) was con -sidered normal(18,19). Infants with VA values lower than normal for med a distinct group and were used for comparison purposes. The letter E on the Snellen chart was used for children aged <7 years or illiterate, and letters of the alphabet were used for children aged >7 years and literate. Each line had five letters (ETDRS table), and two mistakes were tolerated for the last line visualized on the chart. Visual acuity was assessed at a distance of 4 m. The optotypes were generated using the Opto Magis 2nd generation software and transmitted via a flat screen monitor (Phillips) that complied with the specifications re-quired by the software (15-22-inch liquid-crystal display, backlighting of 200 cd/m2, and working distance of 3.0-9.5 m). The optotypes were configured by the system software according to the distance used in the test. This system also provided the sensitivity contrast and the Ishihara color tests.
The Teller VA cards test was exceptionally used. Children with neurological and psychomotor development (NPMD) were excluded,
particularly those with intellectual or postural and motor stability impairments that precluded the performance of >2 of the proposed tests.
contrast sensitivity test (cst) CST was separately performed on each eye. In this test, gray on
white saturation followed a 5% increment scale until 100% black was reached. Values of 5% - 10% were considered normal (NL), values >10% were considered altered (ALT), and the NU category comprised premature infants not submitted to the examination (for statistical purposes). The test was performed at a distance of 4 m, in a dark room, and the only light visible was that from the display. CST was assessed with the optotypes placed two to three lines above the best visual acuity measured (e.g., in VA 20/20, CST was assessed at 20/40).
An optimal contrast test for preschool children does not exist(20,21). This system was selected because the Opto Magis visual acuity equipment allows this test to be applied in any optotype, which is appropriate for use with children.
farnsWorth and ishihara color tests
The Farnsworth D-15 test was performed with natural light and both eyes open. Considering that the children examined were aged <12 years, large charts were used (in subnormal vision) to facilitate the test. The software analyzed the results and generated a graph with the score values.
The Ishihara color test was separately applied to each eye and was performed with the child standing at a distance of 4 m in a dark room. The same software described above generated a sequence of plates with a pattern of colored dots, so that the numbers on each plate could be identified by people without chromatic visual impair-ments but could not be distinguished by people with abnormal color vision. A total of 38 plates were used, and among them, 13 exhibited a linear pattern that was appropriate for illiterate children, and 25 had a numerical pattern (four of the latter were blind). Children who had difficulty undergoing this test or did not recognize numbers were tested using the Ishihara color test in a booklet format, wherein the plates were shown from a 40-cm distance. Children who did not recognize the numbers were asked to follow with the finger the “little road” in a different color in the “pool of dots.”
The children who performed the test without making mistakes were classified as normal (NL), the children who did not perform the test or the test was not conclusive were classified as NU, and the children unable to identify more than three numbers in the Ishihara color test were classified as altered (ALT).
static refraction (under cycloplegia)In children aged <7 years, one drop of cyclopentolate 1% and
one drop of tropicamide 1% were instilled in each eye 30 min before the refraction test. In children aged >7 years of age, one drop of tropicamide 1% was instilled in each eye thrice, with an interval of 5 min, and the test was performed 30 min after instillation of the first drop(22). Retinoscopy was performed with trial frame lenses and was confirmed using a skiascopy rack. For statistical analysis, the spherical equivalent was used both for myopia and hyperopia with astig-matism. The spherical equivalent corresponded to the sum of the spherical degree and 50% of the value of astigmatism. Astigmatism was considered significant when ≥1.50 negative diopters and the percentage difference between the groups was calculated.
motility test
Eye motility was assessed using the Hirschberg, Krimsky, and the eye cover ocular tests, by observing fixation in the nine positions of gaze. Versions and ductions were tested. The groups were compared for the presence or absence of strabismus.

Comparative study of visual functions in premature pre-school children with and without retinopathy of prematurity
36 Arq Bras Oftalmol. 2014;77(1):34-9
stereopsis
Stereoscopic assessment was performed using the Titmus test. The following classification was used: normal (NL): 40 arcseconds, altered (ALT): >40 arcseconds, and NRT: those who were unable to perform the Titmus test. To facilitate the calculation of the statistical difference, two distinct groups were considered: the group of pre-mature infants with normal stereopsis (40 arcseconds) and the group with stereopsis above this value.
binocular indirect ophthalmoscopy (bio)The BIO test was used for the assessment of the anatomical retinal
appearance of premature infants in the three groups. The test was filmed and recorded in DVD.
The pediatric ophthalmologist who performed the BIO, VA, CST, and color tests and the orthoptist who performed the eye motility and stereopsis tests followed up the children at HOSAG after the selection period.
STATISTICAL AnALySIS The Fisher’s exact test was used to evaluate the association bet-
ween the dichotomous variables. The nonparametric Mann-Whitney test was used to compare the quantitative variables between the groups. Values of p<0.05 indicated significance difference. Data were analyzed using the Statistica software, version 8.0.
ReSULTSThe HOSAG database (TASY) included 432 premature infants
examined for the risk of developing ROP during the selection period. More details are shown in table 1.
Twenty-four premature infants were selected and divided into three groups: G1-7 premature infants after ROP treatment; G2-8 pre-mature infants after spontaneous ROP remission; and G3-9 premature infants without ROP.
The results of the comparison between the groups with regard to VA, SCT, chromatic sensitivity test, presence of strabismus, and stereopsis are shown in tables 2-7.
Demographic data and the refraction test and indirect ophthal-moscopy data are shown in tables 1 and 2.
DISCUSSIOnWeight at birth and gestational age above those required to
participate in the study were the most important factors for exclu-ding premature infants from the study (Table 1). This reflects the comprehensive approach to the management of ROP in Brazil until the publication of the guidelines for treating ROP in the country, in 2007 (9). This study was the result of several meetings of the ROP group in Brazil, where studies from various regions of the country were analyzed and discussed(23). Outside Brazil, the definition of the limits of weight and gestational age that indicate risk of ROP and blindness was established by the 1984 and 1987 International Committees(7,8). Other authors observed that the lack of cooperation in answering the repeated calls to participate in the visual assessment tests after the selection period was the factor that most contributed to the co-hort reduction (176/505 premature infants)(15). In the present study, this factor was included in the result specified as “other factors” and represented <10% of the reduction (Table 1).
The good visual functions (FV) results obtained for group G1 were not in line with the findings of a study on VA and strabismus in preschool children published in 1999, wherein the authors observed worse VA among premature infants after ROP treatment(24). Other au-thors have indicated low birth weight and ROP (mainly stages III and IV) negatively affect the response to VA, static refraction, chromatic and contrast sensitivity tests(13-15).
VA was slightly better in group G2, considering that ROP, gestatio-nal age, birth weight, and age group at the time of the re-evaluation examination were similar among groups (Table 2). The high frequency of normal VA among premature infants with postremission ROP and those without ROP was also observed by other researchers(15).
Previous studies suggested that the exclusion of premature in-fants with neuropsychomotor development problems and the type of treatment performed led to better visual acuity even in premature infants after ROP treatment. Moreover, ROP laser treatment had a positive effect on these results(24-26). In the present study, only one
Table 1. Premature children selected and examined between 06/1992 and 06/2006 at HOSAG: reasons for excluding subjects from the study on visual function assessment
Motive of exclusion
Total number of premature children 432
%100
Gestational weight and age above required 266 61.0
<3 visits during the selection period 039 09.0
Impossible to contact 022 05.0
Children aged <4 years on re-evaluation 011 02.5
Chronological age >6 months on first test 011 02.5
ROP stage higher or lower than required 011 02.5
Subnormal vision or severe neuropsychomotor impairment
009 02.0
Informed deaths 003 00.6
Children were followed up by another service 003 00.6
Other factors 033 07.6
Total number of premature children per study 024 06.0
Source: HOSAG records (2012).ROP= retinopathy of prematurity; Other factors= did not agree to participate in the study or withdrawal from the study.
Table 2. Visual acuity Snellen test (OD and OS): Comparison between premature children after ROP treatment (G1) and premature children after ROP remission (G2) and between each group with ROP and the control group (G3)
Groups nnormal VA
%Low VA
% p value
G1 OD 7 071.43 28.57 0.569
G2 OD 8 087.50 12.50
G1 OS 7* 057.14 42.84 0.282
G2 OS 8 087.50 12.50
G1 OD 7 071.43 28.57 0.175
G3 OD 9 100.00 00.00
G1 OS 7* 057.14 42.84 0.282
G3 OS 9 100.00 00.00
G2 OD 8 087.50 12.50 0.471
G3 OD 9 100.00 00.00
G2 OS 8 087.50 12.50 0.471
G3 OS 9 100.00 00.00
Source: HOSAG records (2012).OD= right eye; OS= left eye; VA= visual acuity; *= one premature child with amaurosis in the left eye, after 6 years of age, secondary to total late retinal detachment. Normal= visual acuity considered as normal (20/30 or better). Nonparametric Mann-Whitney test for p<0.05.

Bonotto LB, et al.
37Arq Bras Oftalmol. 2014;77(1):34-9
premature infant in group G1 underwent cryotherapy; this fact and the exclusion of premature infants with severe development impair-ment may have contributed to good VA performance in the three groups under study.
With regard to contrast visual sensitivity, the group of premature infants after ROP treatment exhibited lower contrast sensitivity than the remaining groups (Table 3). On the other hand, in 2001 the Cryotherapy for ROP Cooperative Group observed a better contrast sensitivity among treated premature infants(20). The difficulty in cor-relating low contrast sensitivity with ROP severity was also observed by other authors(15,21).
The result obtained for group G2 was slightly better than that obtained for group G3 (without ROP). This unexpected finding may be explained by the early age of the premature children in group G3 (mean age of 5 years, whereas the mean age of the remaining groups was 6 years), and was not in line with the findings of the Cryotherapy for ROP Cooperative Group, who studied 10-year-old children in 2001. According to a 1981 study conducted with preschool children and their mothers, the factor that affected the responses was the difference in associative knowledge and not necessarily the age difference between the two groups(27).
In group G1, the different CST results obtained for the right and left eyes may be explained by the difference in disease severity bet-ween the eyes.
Other reasons for excluding G1 and G2 groups from the test were the difficulty in communicating verbally, overall developmental and learning disability (inability to understand the test), and total retinal detachment in one eye (Table 3).
The three groups under study exhibited good performance in the Ishihara color test (Table 4). However, there was a large percen-tage of unfavorable responses in G1 using the Farnsworth D-15 test.
Table 3. Contrast sensitivity test (OD and OS): Comparison between premature infants after ROP treatment (G1) and after ROP remission (G2) and between each group with ROP and the control group (G3)
Groups nnL TSC
%ALT TSC
% p value
G1 OD 6* 066.67 33.33 0.192
G2 OD 7*** 100.00 00.00
G1 OS 5** 060.00 40.00 0.523
G2 OS 7*** 085.71 14.29
G1 OD 6 066.67 33.33 1
G3 OD 9 055.56 44.44
G1 OS 5 060.00 40.00 1
G3 OS 9 055.56 44.44
G2 OD 7 100.00 00.00 0.088
G3 OD 9 055.56 44.44
G2 OS 7 085.71 14.29 0.308
G3 OS 9 055.56 44.44
Source: HOSAG records (2012).OD= right eye; OS= left eye; NL TSC= normal contrast sensitivity test; ALT TSC= altered con-trast sensitivity test; G1(*): one premature infant in G1 did not undergo the test on both eyes; 1 (**): another premature infant in G1 did not undergo the CST test on the left eye (total retinal detachment); G2 (***): one premature infant in G2 did not undergo the CST test. Nonparametric Mann-Whitney test for p<0.05.
Table 4. Ishihara color test: Comparison between groups G1 and G3 (OU) and G2 and G3 (OU)
Groups nCT IHnL
%CT IHALT
% p value
G1 OU 5 100.00 0.00 1
G3 OU 7 85.71 14.29
G2 OU 6 100.00 0.00 1
G3 OS 7 85.71 14.29
Source: HOSAG records (2012).OU= both eyes; OS= left eye; CT IHNL= normal Ishihara color test; CT IHALT= altered Ishihara color test; N= number of premature infants who underwent the test in each group (total pre mature infants per group: G1=7, G2=8, and G3=9). Nonparametric Mann-Whitney test for p<0.05.
Table 5. Farnsworth D-15 AO color test: comparison between groups G1 and G2
Groups nCT FW-D15 nL
%CT FW-D15 ALT
% p value
G1 OU 5 20.00 80.00 0.206
G2 OU 4 75.00 25.00
G1 OU 5 20.00 80.00 0.524
G3 OU 4 50.00 50.00
G2 OU 4 75.00 25.00 1
G3 OU 4 50.00 50.00
Source: HOSAG records (2012).OU= both eyes; CT FW-D15 NL= normal Farnsworth D-15 color test; CT FW-D15 ALT= altered Farnsworth D-15 color test. N= number of premature infants that underwent the test in each group (total premature infants per group: G1=7, G2=8, G3=9). Nonparametric Mann-Whitney test for p<0.05.
Table 6. Strabismus: Comparison between premature infants after ROP treatment (G1) and after remission of ROP Stages II and III (G2)
Groups nStrabismus
yes (%)Strabismus
no (%) p value
G1 OU 7 00.00 100.00 0.200
G2 OU 8 37.50 062.50
G1 OU 7 00.00 100.00 –
G3 OU 9 00.00 100.00
G2 OU 8 37.50 062.50 0.082
G3 OU 9 00.00 100.00
Source: HOSAG records (2012). OU= both eyes. Nonparametric Mann-Whitney test for p<0.05.
Table 7. Stereopsis: Comparison between premature infants with after treat-ment RO (G1) and after remission of ROP Stages II and III (G2)
Groups nStereopsis
nL (%)Stereopsis
ALT (%) p value
G1 OU 7 00.00 100.00 p: 0.467
G2 OU 8 25.00 075.00
G1 OU 7 00.00 100.00 p: 0.200
G3 OU* 8 37.50 062.50
G2 OU 8 25.00 075.00 P:1
G3 OU 8 37.50 062.50
Source: HOSAG records (2012).OU= both eyes; NL= normal Titmus test; ALT= altered, >40 arcseconds; NRT= those who were unable to perform the Titmus test. *= one premature infant did not undergo the Titmus test. Nonparametric Mann-Whitney test for p<0.05.

Comparative study of visual functions in premature pre-school children with and without retinopathy of prematurity
38 Arq Bras Oftalmol. 2014;77(1):34-9
This percentage was significantly higher than that observed by the CRYO-ROP study group (80% in G1 vs. 2.8% in the CRYO-ROP study). According to these authors, this deficiency was related to low visual acuity and not to possible alterations inherent to prematurity itself or to ROP severity(28). However, in the present study, 64.28% premature infants in group G1 exhibited good visual acuity.
In the three groups under study, the reason for excluding prema-ture infants from this test was their difficulty in understanding the color test (TC), which was in agreement with the findings of other authors who observed that, after excluding the children unable to perform the color test, the responses of premature children were very similar to those of full-term children(29).
Chart 2. Distribution of static refraction and VA data in groups G1, G2, and G3
Right eye Left eye
Spherical Cylinder Axis Acuity Spherical Cylinder Axis Acuity
G1- laser
1 +0.50 -0.50 180 20/20 0.00 -0.50 180 20/20
2 +2.00 0.00 0 20/20 +1.50 0.00 0 20/30
3 -5.50 -3.00 105 20/30 -4.25 0.00 0 20/25
4 -4.25 -0.75 125 20/60 0.00 0.00 0 20/20
5 +0.50 -1.75 180 20/30 -0.50 -3.00 180 20/40
6 -6.50 -2.00 170 20/30 * **
7 -2.75 -0.50 180 20/63 -2.75 -0.50 180 20/63
G2- without laser
8 +4.50 -1.25 10 20/20 +4.75 -1.50 170 20/20
9 +2.25 0.00 0 20/20 +2.50 0.00 0 20/20
10 +2.00 -0.50 165 20/20 +2.25 0.00 0 20/20
11 +2.00 -0.50 180 20/20 +2.00 -0.50 165 20/20
12 +0.25 -0.25 90 20/20 +0.25 0.00 0 20/20
13 +1.50 -0.25 90 20/20 +1.50 -0.25 5 20/20
14 +1.75 -1.25 15 20/50 +1.75 -1.50 180 20/50
15 +2.00 -0.50 90 20/20 +1.50 0.00 0 20/20
G3- without ROP
16 -0.25 0.00 0 20/20 0.00 0.00 0 20/20
17 +2.50 0.00 0 20/20 +2.50 0.00 0 20/20
18 +1.50 -0.75 180 20/20 +1.50 -1.00 180 20/20
19 +1.00 -0.50 180 20/20 +1.00 -0.50 180 20/20
20 +1.75 0.00 0 20/20 +2.00 -0.50 180 20/20
21 +3.00 -0.25 90 20/20 +2.50 0.00 0 20/20
22 +1.50 0.00 0 20/20 +1.50 -0.50 90 20/20
23 +1.00 0.00 0 20/20 +1.00 0.00 0 20/20
24 +1.25 -0.50 170 20/20 +1.50 0.00 0 20/20
G1= after treatment ROP stages II and III; G2= ROP stages II and III in remission; G3= without ROP; *= refraction impossible, total retinal detachment; **= amaurosis.
Chart 1. Demographic data for the three groups of premature preschool children classified into three groups of retinopathy of prematurity (G1, G2, and G3), considering the variables gender, chronological age on re-evaluation (CRA), gestational age (GA), birth weight (BW), and number of medical consultations between the selection and re-evaluation periods
Groups GenderCRA
(years)GA
(weeks)WB
(grams)number of
Visits
n M (%) F (%) mean DP mean DP mean DP mean DP
G 1 7 71 29 6.1 1.6 28.1 1.9 1.015 123.5 24.4 20.5
G 2 8 25 75 6.5 1.9 27.2 1.6 963.7 123.0 19.8 13.9
G 3 9 78 22 5.1 0.9 28.4 2.5 991.1 258.4 9.7 4.2
G1= group after treatment of ROP stages II and III; G2= groups at ROP stages II and III in remission; G3= group without ROP; M= male; F= female; CRA= chronological age on re-evaluation; GA= gestational age; BW= birth weight. SD= standard deviation; N= total number.

Bonotto LB, et al.
39Arq Bras Oftalmol. 2014;77(1):34-9
The absence of cases of strabismus in group G1 contradicted the findings of other authors in similar studies, which indicated the occurrence of strabismus in 26%-44% of premature infants after ROP treatment, and this proportion was dependent on the type of treatment (laser or cryotherapy)(14,24,25,30). In the present study, the study sample was small and the possibility that the exclusion criteria selected premature infants without strabismus in group G1 cannot be discarded. The ideal would be to assess the presence of strabismus in premature children excluded for other reasons; however, such evaluation was not the aim of this study.
A 37% incidence of convergent strabismus in group G2 was in accordance with the results obtained by other authors, who found a similar frequency and a higher percentage of convergent strabismus among premature infants after spontaneous ROP remission(24,31).
Of the four infants in G2 with neuropsychomotor development problems, three presented with strabismus. Therefore, the pro-portion of infants with neurological problems was relevant in this group and may explain the higher percentage of strabismus in the group with spontaneous remission, as was also observed by other authors(11,14,24,30,31).
Stereopsis was present in 57% the premature infants in group G1. A similar result was observed in a study published in 2005, wherein 66.6% premature infants with ROP treated with laser exhibited ste-reopsis(24). However, no premature infants exhibited normal stereop-sis. Strabismus was not among the causes of the low performance of G1 with regard to stereopsis. On the other hand, low unilateral or bilateral VA was responsible for this result. The lower stereoscopic resolution observed among premature infants after ROP treatment was in line with other studies that associated stereoscopic resolution with ROP severity(14,30). In group G2, the nonrecognition of the Titmus test and the suppression caused by strabismus represented 37% of the 75% change in this test. In addition, age contributed to the low frequency of normal stereopsis among the groups G2 and G3.
In this study there was no difference between premature children after ROP treatment and those after spontaneous ROP remission with regard to the visual functions assessed. In addition, there was no difference between the groups with ROP and the control (Tables 2-7).
The limitations of the present study include sample size, which may have contributed to the nonsignificant differences between the groups. Therefore, additional studies from other institutions that study ROP in Brazil are necessary.
The lack of standardization of the chromatic and contrast sensiti-vity tests precludes the comparison of results across studies. Further studies using tests performed in computers and high-definition monitors may help solve these limitations.
The results of VA and the presence of strabismus in the groups with ROP highlight the risks of low vision and amblyopia and suggest the need for close follow-up of preschool and school children.
COnCLUSIOnThere was no significant difference in visual functions between
premature infants after ROP treatment and those after spontaneous remission, and between premature infants with ROP and without ROP.
ReFeRenCeS 1. Terry TL. Extreme prematurity and fibroblastic over-growth of persistent vascular
sheath behind each crystalline lens. Am J Ophthalmol. 1942;25:203-4. 2. Owens WC, Owens EU. Retrolental fibroplasia in premature infants. Am J Ophthalmol.
1949;32(1):1-21. 3. Reese AB. Persistence and hyperplasia of primary vitreous; retrolental fibroplasia; two
entities. Arch Ophthal. 1949;41(5):527-52. 4. Kinsey VE. Retrolental fibroplasia; cooperative study of retrolental fibroplasia and the
use of oxygen. AMA Arch Ophthalmol. 1956;56(4):481-543. 5. Kinsey VE, Arnold HJ, Kalina RE, Stern L, Stahlman M, Odell G, et al. PaO2 levels and
retrolental fibroplasia: a report of the cooperative study. Pediatrics. 1977;60(5):655-68.
6. Flynn JT, Bancalari E, Bachynski BN, Buckley EB, Bawol R, Goldberg R, et al. Retinopa thy of prematurity. Diagnosis, severity, and natural history. Ophthalmology. 1987;94(6): 620-9.
7. An international classification of retinopathy of prematurity. The Committee for the Classification of Retinopathy of Prematurity. Arch Ophthalmol. 1984;102(8):1130-4.
8. An international classification of retinopathy of prematurity. II. The classification of retinal detachment. The International Committee for the Classification of the Late Stages of Retinopathy of Prematurity. Arch Ophthalmol. 1987;105(7):906-12. Erratum in: Arch Ophthalmol 1987;105(11):1498.
9. International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity revisited. Arch Ophthalmol. 2005;123(7):991-9. Review.
10. Zin A, Florêncio T, Fortes Filho JB, Nakanami CR, Gianini N, Graziano RM, Moraes N; Brazilian Society of Pediatrics, Brazilian Council of Ophthalmology and Brazilian Society of Pediatric Ophthalmology. [Brazilian guidelines proposal for screening and treatment of retinopathy of prematurity (ROP)]. Arq Bras Oftalmol. 2007;70(5):875-83. Portuguese.
11. Holmström G, Larsson E. Long-term follow-up of visual functions in prematurely born children-a prospective population-based study up to 10 years of age. J AAPOS. 2008;12(2):157-62.
12. Mirabella G, Kjaer PK, Norcia AM, Good WV, Madan A. Visual development in very low birth weight infants. Pediatr Res. 2006;60(4):435-9.
13. O’Connor AR, Stephenson TJ, Johnson A, Tobin MJ, Ratib S, Moseley M, et al. Visual function in low birthweight children. Br J Ophthalmol. 2004;88(9):1149-53.
14. O’Connor AR, Fielder AR. Visual outcomes and perinatal adversity. Semin Fetal Neo-natal Med. 2007;12(5):408-14.
15. O’Connor AR, Stephenson T, Johnson A, Tobin MJ, Moseley MJ, Ratib S, et al. Long-term ophthalmic outcome of low birth weight children with and without retinopathy of prematurity. Pediatrics. 2002;109(1):12-8.
16. Robaei D, Kifley A, Gole GA, Mitchell P. The impact of modest prematurity on visual function at age 6 years: findings from a population-based study. Arch Ophthalmol. 2006;124(6):871-7.
17. World Health Organization. Weekly epidemiological record relevé épidémiologique hebdomaire. Wkly Epidem Rec. 1984;59:205-12.
18. Pan Y, Tarczy-Hornoch K, Cotter SA, Wen G, Borchert MS, Azen SP, Varma R; Multi-Ethnic Pediatric Eye Disease Study Group. Visual acuity norms in pre-school children: the Multi-Ethnic Pediatric Eye Disease Study. Optom Vis Sci. 2009;86(6):607-12.
19. Holladay J. Proper method for calculating average visual acuity. J Refract Surg. 1997; 13:388-91.
20. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Contrast sensitivity at age 10 years in children who had threshold retinopathy of prematurity. Arch Oph-thalmol. 2001;119(8):1129-33.
21. Larsson E, Rydberg A, Holmström G. Contrast sensitivity in 10 year old preterm and full term children: a population based study. Br J Ophthalmol. 2006;90(1):87-90.
22. Bicas HE. Sociedade Brasileira de Oftalmologia Pediátrica. Prescrição de óculos na infância [Internet]. São Paulo: Sociedade Brasileira de Oftalmologia Pediátrica; s.d. p. 1-21. [citado 2014 Jan 17]. Disponível em: http://www.cbo.com.br/cbo/sociedades/pediatria/artigos/prescricoes_oculos_infancia.pdf
23. Sociedade Brasileira de Oftalmologia Pediátrica. Projeto ROP Brasil: na prevenção da cegueira por retinopatia da prematuridade [Internet]. São Paulo:CBO; 2006. [citado 2014 Jan 17]. Disponível em: http://dnanet.dna.com.br/sbop/site/interna.asp?campo=119&secao_id=6
24. Holmström G, el Azazi M, Kugelberg U. Ophthalmological follow up of preterm infants: a population based, prospective study of visual acuity and strabismus. Br J Oph thalmol. 1999;83(2):143-50.
25. Ospina LH, Lyons CJ, Matsuba C, Jan J, McCormick AQ. Argon laser photocoagulation for retinopathy of prematurity: long-term outcome. Eye (Lond). 2005;19(11):1213-8.
26. Sahni J, Subhedar NV, Clark D. Treated threshold stage 3 versus spontaneously regres-sed subthreshold stage 3 retinopathy of prematurity: a study of motility, refractive, and anatomical outcomes at 6 months and 36 months. Br J Ophthalmol. 2005;89(2):154-9.
27. Atkinson J, French J, Braddick O. Contrast sensitivity function of preschool children. Br J Ophthalmol. 1981;65(8):525-9.
28. Dobson V, Quinn GE, Abramov I, Hardy RJ, Tung B, Siatkowski RM, et al. Color vision measured with pseudoisochromatic plates at five-and-a-half years in eyes of children from the CRYO-ROP study. Invest Ophthalmol Vis Sci. 1996;37(12):2467-74.
29. Jackson TL, Ong GL, McIndoe MA, Ripley LG. Monocular chromatic contrast threshold and achromatic contrast sensitivity in children born prematurely. Am J Ophthalmol. 2003;136(4):710-9.
30. VanderVeen DK, Coats DK, Dobson V, Fredrick D, Gordon RA, Hardy RJ, Neely DE, Pal-mer EA, Steidl SM, Tung B, Good WV; Early Treatment for Retinopathy of Prematurity Cooperative Group. Prevalence and course of strabismus in the first year of life for infants with prethreshold retinopathy of prematurity: findings from the Early Treat-ment for Retinopathy of Prematurity study. Arch Ophthalmol. 2006;124(6):766-73.
31. Bremer DL, Palmer EA, Fellows RR, Baker JD, Hardy RJ, Tung B, et al. Strabismus in premature infants in the first year of life. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Arch Ophthalmol. 1998;116(3):329-33.
40 Arq Bras Oftalmol. 2014;77(1):40-6
Original Article
InTRODUCTIOnAstigmatism is a visually disabling refractive error, and at least
15%-20% cataract patients have corneal astigmatism of ≥1.50 diop-ters (D)(1).
One way to correct astigmatism simultaneously during cataract surgery is to place limbal relaxing incisions (LRIs)(2,3). It is possible,
however, that late corneal biomechanics may play an unfavorable role in refractive outcomes over time(4). Toric intraocular lens (IOL) implantation is another valuable option for astigmatism correction in cataract patients. Undesired rotation of the toric IOL is the main pro-blem associated with this method. Approximately 1 degree of off-axis rotation results in a loss of up to 3.3% in expected cylinder correction(5).
Treatment of astigmatism during phacoemulsificationTratamento do astigmatismo durante a facoemulsificação
Giuliano oliveira FreiTaS1,2, Joel edMur boTeon1, Mario JoSé carvalho2, roGerio Melo coSTa pinTo3
Submitted for publication: May 29, 2013 Accepted for publication: September 2, 2013
Study was carried out at Center of postgraduate Faculdade de Medicina, Universidade Federal de Minas Gerais - UFMG, Belo Horizonte, (MG); Instituto de Saúde Ocular ISO-Olhos, Uberlândia, (MG).
1 Universidade Federal de Minas Gerais, Belo Horizonte (MG), Brazil.2 Cataract Surgery Department at ISO - Olhos - Instituto de Saúde Ocular, Uberlândia (MG), Brazil.3 Universidade Federal de Uberlândia, Uberlândia (MG), Brazil.
Financial contributors: Private: Alcon Labs. Brazil Sao Paulo (SP), provided all intraocular lenses at no cost for scientific purposes. Public: Municipal Health Authority of Uberlândia funded surgical procedures as part of a regular governmental assistance policy.
Disclosure of potential conflicts of interest: G.O. Freitas, None; J.E. Boteon, None; M.J. Carvalho, None; R.M.C. Pinto, None.
Correspondence address: Giuliano Oliveira Freitas. ISO Olhos - Rua Eduardo Marquez, 50 - Uberlân-dia (MG) - 38400-442 - Brazil - E-mail: [email protected]
ABSTRACTPurpose: To compare the effectiveness of limbal relaxing incisions (LRI) with that of toric intraocular lens (IOL) implantation for the treatment of astigmatism during phacoemulsification using nonvectorial (predictability, safety, and efficacy) and vectorial analyses.Methods: This longitudinal observational case series assessed 62 eyes of 31 consecutive cataract patients with preoperative corneal astigmatism of 0.75-2.50 diopters (D) in both eyes. Patients were randomly assigned to 2 groups: a toric IOL group, which received toric IOLs in both eyes, and an LRI group, which received spherical IOLs associated with LRI placement in both eyes. All patients were eva-luated at 1, 3, and 6 months after surgery, when refractive astigmatism analysis was performed using both nonvectorial and Alpins vectorial methods. Outcomes were assessed within each group and compared between groups. Results: The proportion of eyes within ±0.50 D of the intended correction at 3 and 6 months after surgery was 75% and 71.88%, respectively, in the LRI group and 40% and 66.67%, respectively, in the toric IOL group. In the remaining period, the proportion was greater in the toric IOL group. The safety index showed no difference at any time point. The efficacy index at 1 and 3 months after surgery was significantly higher in the toric IOL group (0.43 and 0.44, respectively) than in the LRI group (0.31 and 0.36, respectively). At 6 months after surgery, the status of eyes in the LRI group was as follows: 53.13% were undercorrected, 43.74% achieved the intended correction, and 3.13% were overcorrected. In the toric IOL group, 16.76% eyes were undercorrected, 76.67% achieved the intended correction, and 6.67% were overcorrected. The success rates for astigmatic surgery, astigmatism reduction at the intended axis, and astigmatism corrected were 43%, 62%, and 64%, respectively, in the LRI group and 57%, 81%, and 94%, respectively, in the toric IOL group. Conclusions: Our results suggest that the use of toric IOLs may be advantageous over the use of LRIs for the treatment of astigmatism during phacoemulsification. Although such advantages seem subtle in nonvectorial analyses, they are highli-ghted in vectorial analyses.
Keywords: Astigmatism/physiopathology; Lens implantation, intraocular; pha-coemulsification/methods; Limbus cornea/surgery; Evaluation of the efficacy/effec tiveness of interventions.
RESUMOObjetivo: Comparar incisões relaxantes limbares (IRL) e lentes intraoculares (LIO) tóricas tanto em termos não-vetoriais (efetividade, segurança e eficácia), quanto vetoriais no tratamento do astigmatismo por ocasião da facoemulsificação. Métodos: Estudo observacional longitudinal (série de casos) no qual foram avaliados 62 olhos de 31 pacientes consecutivos de catarata com astigmatismo corneano pré-operatório entre 0,75 e 2,50 dioptrias (D) para ambos os olhos. Os pacientes foram aleatoriamente distribuídos entre 2 grupos: “1” submetido a implante de lentes intraoculares AcrySof ToricTM em ambos os olhos e “2” com implante bilateral de lentes intraoculares tóricas AcrySof NaturalTM complementada por incisões relaxantes limbares. Todos os pacientes foram reavaliados com 1, 3 e 6 meses de pós-operatório, sendo feitas análises do astigmatismo refracional por métodos não-vetoriais, como pela análise vetorial de Alpins, interessando os resultados dentro de cada grupo e entre os grupos. Resultados: O porcentual de olhos entre ±0,50 D da correção pretendida no grupo incisões relaxantes limbares foi de 75 e 71,88%, respectivamente, em comparação aos 40 e 66,67% do grupo lentes intraoculares tóricas aos 3 e 6 meses de pós-operatório. Nos outros períodos avaliados, os porcentuais foram favoráveis ao grupo lentes intraoculares tóricas. O índice de segurança não demonstrou diferença em nenhum dos períodos. O índice de eficácia foi estatisticamente maior para o grupo lentes intraoculares tórica com 1 e 3 meses de pós-operatório (0,43 e 0,44), em comparação ao grupo incisões relaxantes limbares (0,31 e 0,36). Aos 6 meses, o porcentual de olhos, para o grupo incisões relaxantes limbares, foi: hipocorreção em 53,13%; 43,74% alcançaram a correção pretendida e 3,13% ficaram hipercorrigidos; no grupo lentes intraoculares tóricas, a hipocorreção ocorreu em 16,76%; 76,67% alcançaram a correção pretendida e 6,67% ficaram hipercorrigidos. Os porcentuais de sucesso da cirurgia astigmática, da redução do astigmatismo no eixo pretendido e do astigmatismo corrigido foram, respectivamente, para o grupo IRL: 43%, 62% e 64%; para o grupo lentes intraoculares tóricas: 57%, 81% e 94%. Conclusões: Nossos resultados sugerem que o uso de lentes intraoculares tóricas é vantajoso ao de incisões relaxantes limbares no tratamento do astigmatismo por ocasião da facoemulsificação. Apesar de que tais vantagens mostraram-se sutis na análise não-vetorial, elas foram consistentes na perspectiva vetorial.
Descritores: Astigmatismo/fisiopatologia; Implante de lente intraocular; Facoe-mulsificação/métodos; Limbo da córnea/cirurgia; Avaliação de eficácia-efetividade de intervenções.

Freitas GO, et al.
41Arq Bras Oftalmol. 2014;77(1):40-6
Vectors are mathematical expressions that combine values for magnitude and direction. Astigmatism, with cylinder power and axis (refractive) or magnitude and meridian (corneal), fits such a description(6,7). The Alpins method is a vectorial analysis method that allows determination of the effectiveness of a specific treatment for astigmatism. Such methods have been used by several authors to analyze astigmatic changes induced by different surgical approa-ches such as excimer laser refractive surgery, LRI(3,8-11), and toric IOL implantation(1,12,13).
In light of the advantages and limitations of each approach, de-termination of the more superior treatment remains controversial(14). This study compared LRI placement and toric IOL implantation for the treatment of preoperative astigmatism during phacoemulsification using both nonvectorial (predictability, safety, and efficacy indices(15) and vectorial analyses.
MeTHODSThis longitudinal, observational case series assessed 31 consecu-
tive cataract patients with preoperative corneal astigmatism of 0.75 D-2.50 D in both eyes. Patients were randomly assigned using the Microsoft ExcelTM “=RANDBETWEEN(1;2)” function into two phacoe-mulsification groups: a toric IOL group, which received toric IOLs in both eyes (model AcrySof ToricTM, AlconTM, Inc.), and an LRI group, which received spherical IOLs (AcrySof NaturalTM, AlconTM, Inc.) asso-ciated with LRI placement in both eyes. All patients provided written informed consent after they were provided with an explanation about the nature of the study and its potential complications, in ac-cordance with the tenets of the Declaration of Helsinki. All surgeries were performed between May 2010 and June 2012.
Inclusion criteria were age >40 years; visually significant cataract, defined as spectacle distance corrected visual acuity (SDCVA) worse than Snellen 20/40 (LogMAR scale of 0.3); regular corneal astigmatism ranging from 0.75 D to 2.50 D; and pharmacological mydriasis of at least 6.0 mm (measured at the slit lamp) to facilitate proper intrao-perative visualization of axis marks on the surface of the toric IOL.
Affected eyes with a history of previous surgery, pterygium, ocu-lar disease that would lead to poor postoperative corrected visual acuity (corneal scarring, uveitis, advanced glaucoma, neuroophthal-mic disease, and significant macular disease or other retinopathy), and/or zonule or pupil abnormalities were excluded.
Before surgery, all patients underwent complete ophthalmologi-cal evaluation by an examiner other than the surgeon (G.F.), including manifest refraction and SDCVA, slit lamp examination, applanation tonometry, and fundoscopy under pharmacological mydriasis in addition to corneal topography (OrbscanII™, Bausch&Lomb™, Inc.) and ultrasound immersion biometry (OcuScan™, Alcon™, Inc.). The Hoffer Q formula was used in eyes with an axial length shorter than 22 mm, and the SRK/T formula was used for all other eyes.
Toric IOL cylinder power and axis placement were determined using the IOL manufacturer’s online calculator (www.acrysoftoriccal-culator.com). The size and location of LRIs were also determined via an online open source application (www.lricalculator.com), accor-ding to Donnenfeld’s nomogram. For both groups, data such as bio metry, keratometry, main incision location, and default surgically induced astigmatism (set at -0.50 D) were entered into the calculators with the final aim of achieving postoperative zero sphere and the smallest residual cylinder possible(16,17).
surgical technique
The same surgeon (M.C.) performed all surgeries under mild sedation and topical anesthesia. Just before surgery, a sterile ink pen was used to place two marks on the corneal limbus at the 0-degree and 180-degree positions with the patient sitting upright at the slit lamp to avoid ocular torsion. In both groups, phacoemulsification followed by IOL implantation was performed through a 2.75-mm,
single-plane, temporal incision at the corneal limbus; a Mendez ring was used to mark the steepest meridian. In the toric IOL group, the IOL was rotated to align with the intended axis. In the LRI group, LRIs were placed inside the limbus using a calibrated diamond knife with a preset blade depth of 600 μm.
postoperative folloW-up
All patients were evaluated at 1, 3, and 6 months after surgery (G.F.).The postoperative manifest refraction, uncorrected distance visu-
al acuity (UDVA), and SDCVA were measured. Spherical equivalent re-fraction (SE), predictability, and safety and efficacy indices were then calculated. Predictability was expressed as the proportion of eyes within ±1.00 D of the intended SE or the proportion of eyes within an even more strict limit of ±0.50 D of the intended SE. The intended SE was calculated from the difference between the postoperative SE and target SE. The target SE was defined as half of the goal residual cylinder. The safety index (SI) was calculated from the ratio between the postoperative SDCVA and preoperative SDCVA. The efficacy index (EI) was calculated from the ratio between postoperative UDVA and preoperative SDCVA.
The Alpins vectorial method of astigmatism analysis is based on three elementary vectors: target-induced astigmatism (TIA), surgi-cally-induced astigmatism (SIA), and the difference vector (DV). In an ideal scenario, TIA equals SIA, while DV is null. Several relationships between these vectors, such as the magnitude of error (ME= SIA - TIA), index of success (IoS= DV/TIA), and correction index (CI= SIA/TIA) are capable of fully describing the surgical astigmatic change if analyzed together(6). The Alpins vectorial parameters for refractive astigmatism were calculated using Microsoft™ Excel™ for MacIntosh™ spreadsheets (version 12.2.7, Microsoft™ Corp.).
The Shapiro-Wilk normality tests for data sets were performed using IBM™ SPSS™ for Microsoft™ Windows™ software (version 20.0.0). A P-value of ≤0.05 was considered statistically significant(18). Pearson’s coefficient of determination (R2) was used as necessary(19); bootstrapping (95% confidence interval) was performed in such cases(20). The Wilco-xon test was used to analyze statistical nonparametric differences within the same group throughout the follow-up period, and the Mann-Whitney U test was used to determine differences between the toric IOL and LRI groups at each evaluation(3).
ReSULTSThe study enrolled 62 eyes of 31 consecutive eligible patients.
Patient demographics and preoperative data are presented in Table 1. The mean age of patients in the LRI group was 71.75 years, which was significantly higher than that (65.67 years) of patients in the toric IOL group. Accordingly, the number of patients with rule astigmatism was 3 times lower in the LRI group (8 eyes) than in the toric IOL group (24 eyes).
All surgeries were uneventful. None of the eyes required a second intervention. No potentially sight-threatening complications such as persistent corneal edema, pupillary block, retinal detachment, or endophthalmitis were observed.
All patients completed the follow-up period of 6 months.Table 2 shows the preoperative intended astigmatic correction
based on topographic astigmatism and the 1-, 3-, and 6-month postoperative astigmatic corrections based on manifest refractive astigmatism during each follow-up period in both groups. There was no statistical difference in the preoperative intended astigmatic correction between groups: -1.32 D in the LRI group and -1.41 D in the toric IOL group. The manifest refractive astigmatism at 6 months after surgery was -0.74 D in the LRI group and -0.62 D in the toric IOL group; these values were close to statistical significance (P=0.06).
At 6 months after surgery, the manifest refraction, as SE (means ± standard deviation), was -0.20 ± 0.42 in the LRI group and -0.21 ± 0.49 in the toric IOL group, with no significant difference between groups (P=0.84).

Treatment of astigmatism during phacoemulsification
42 Arq Bras Oftalmol. 2014;77(1):40-6
Figure 1A compares the mean preoperative and 1-, 3-, and 6-month postoperative SDCVAs between the LRI and toric IOL groups. The preoperative mean SDCVA was significantly lower in the toric IOL group than in the LRI group (Mann–Whitney U test, P=0.01). There was no significant difference in the mean SDCVA during the remaining period between groups (Mann–Whitney U test, P>0.05). Within each group, the postoperative SDCVAs were statistically lower than the preoperative corrected acuity and remained stable thereaf-ter (Wilcoxon test; P=0.00). Figure 1B compares the mean 1-, 3-, and 6-month postoperative UCVAs between the LRI and toric IOL groups. The mean postoperative UDVA was comparable between groups throughout the follow-up period (Mann-Whitney U test; P>0.05).
Table 3 shows the proportion of eyes within ±1.00 D and within ±0.50 D of the intended spherical equivalent refraction at 1, 3, and 6 months after surgery in both groups. The proportion of eyes within ±0.50 D at 3 months and 6 months after surgery was greater in the LRI group (75% and 71.88%, respectively) than in the toric IOL group (40% and 66.67%, respectively). In the remaining period, the proportion was greater in the toric IOL group.
Table 4 shows the safety and efficacy indices in both groups at 1, 3, and 6 months after surgery.
SI showed no difference at any time point between groups. EI at 1 and 3 months after surgery was significantly higher in the toric IOL group (0.43 and 0.44, respectively) than in the LRI group (0.31 and 0.36, respectively).
Figure 2A compares the mean TIAs at 1, 3, and 6months after sur-gery with the mean SIAs at the same time points between the LRI and toric IOL groups. There was no significant difference in the mean TIAs between groups (Mann-Whitney U test, P>0.05), while the mean SIAs were significantly lower in the LRI group than in the toric IOL group (Mann-Whitney U test; P<0.05). However, within each group, there were no differences in the mean SIAs throughout the follow-up period (Wilcoxon test; P>0.05). The mean SIAs were significantly lower than the mean TIAs in the LRI group (Wilcoxon test; P<0.05), while there were no significant differences in mean TIAs and SIAs in the toric IOL group (Wilcoxon test; P>0.05). Figure 2B compares the postoperative 1-, 3-, and 6-month mean DVs between the LRI and toric IOL groups. The mean DVs were significantly higher in the LRI group than in the toric IOL group throughout the follow-up period (Mann-Whitney U test; P<0.05). There were no significant differences within the same group over time (Wilcoxon test; P>0.05).
Figure 3 compares the attempted versus achieved astigmatism 6 months after surgery in the LRI and toric IOL groups. Pearson’s coe-fficient of determination (R2) for each group was 0.50 and 0.89 in the LRI and toric IOL groups, respectively (Figure 3).
Figure 4 shows the percentage distribution of astigmatic correc-tion based on ME at 6 months after surgery in both groups. In the LRI group, 53.13% eyes were undercorrected, 43.74% eyes achieved the intended correction, and 3.13% eyes were over-corrected. In the toric IOL group, 16.76% eyes were undercorrected, 76.67% eyes reached the intended correction, and 6.67% eyes were overcorrected.
Table 1. Patient demographics and preoperative data
Group
LRI Toric IOL P-value*
Patients (n) 16 15 -
Eyes (n) 32 30 -
Sex (F/M) 8/8 11/4 -
Age (years)
Range 51 to 84 52 to 80 -
Mean ± SD 71.75 ± 8.87 65.67 ± 6.28 0.01
Topographic astigmatism (D)
Range 0.75 to 2.40 0.80 to 2.50 -
Mean ± SD 1.32 ± 0.47 1.41 ± 0.54 0.60
Steepest topographic 180°-semimeridian angle (n)
0° to 30° or 151° to 180° 18 5 -
61° to 120° 8 24 -
31° to 60° or 121° to 150° 6 1 -
Axial length (mm)
Range 21.40 to 24.33 21.75 to 25.93 -
Mean ± SD 23.05 ± 0.63 23.33 ± 0.92 0.25
Biometric formulae (n)
SRK/T 30 28 -
Hoffer Q 2 2 -
Spherical IOL power (D)
Range 18.50 to 27.00 13.50 to 24.50 -
Mean ± SD 21.50 ± 1.87 21.38 ± 2.58 0.61
Toric IOL model (n)
T3 - 14 -
T4 - 7 -
T5 - 9 -
LRI= limbal relaxing incisions; IOL= intraocular lens; n= number; F= females; M= males; SD= standard deviation; D= diopters; mm= millimeters; T3= AcrySof ToricTM T3 IOL; T4= AcrySof ToricTM T4 IOL; T5= AcrySof ToricTM T5 IOL.(*) Mann-Whitney U test.
Table 2. Preoperative intended astigmatism and achieved astigmatism at 1, 3, and 6 months after surgery
Group
Cylinder diopters LRI Toric IOL P-value*
Preoperative intended astigmatism
Range -2.40 to -0.75 -2.50 to -0.80 -
Mean ± SD -1.32 ± 0.47 -1.41 ± 0.54 0.60
1-month postoperative achieved astigmatism
Range -1.25 to 0.00 -1.00 to 0.00 -
Mean ± SD -0.66 ± 0.30 -0.58 ± 0.24 0.25
P-value† 0.00 0.00 -
Achieved astigmatism 3 months after surgery
Range -1.00 to 0.00 -1.00 to -0.25
Mean ± SD -0.70 ± 0.21 -0.63 ± 0.20
P-value†† 0.00 0.00 -
Achieved astigmatism 6 months after surgery
Range -1.25 to -0.25 -1.00 to -0.25 -
Mean ± SD -0.74 ± 0.26 -0.62 ± 0.17 06
P-value††† 0.00 0.00 -
LRI= limbal relaxing incisions; IOL= intraocular lens; SD= standard deviation.(*) Mann-Whitney U test. (†,††,†††) Wilcoxon test; preoperative intended astigmatism vs. achieved astigmatism at 1, 3, and 6 months, respectively, after surgery.

Freitas GO, et al.
43Arq Bras Oftalmol. 2014;77(1):40-6
Figure 5 shows the success rates for astigmatic surgery, astigma-tism reduction at the intended axis, and percentage of astigmatism corrected at 6 months after surgery in both groups. The success rates were 43%, 62%, and 64%, respectively, in the LRI group and 57%, 81%, and 94%, respectively, in the toric IOL group.
DISCUSSIOnIn our study, both the LRI and toric IOL groups presented similar
preoperative characteristics in most aspects of interest, as shown in Table 1, in accordance with the randomization design. However, one difference was remarkable; in the toric IOL group, the mean age of patients was significantly lower than that of patients in the LRI group. The incidence of both oblique and against the rule astigma-tism increases with age(21). Both these forms of corneal astigmatism seem to respond somewhat poorly to LRI(10,22). Therefore, it may be expected that the overall capacity of LRI for treating pre-existing
corneal astigmatism may have been underestimated and that the overall outcomes could possibly be different, if there were no such discrepancies in mean age between groups.
The postoperative manifest cylinder refraction at 6 months (me-ans ± standard deviation) was -0.74 D ± 0.26 D in the LRI group and -0.62 D ± 0.17 D in the toric IOL group, values consistent with those re-ported in the current literature (-0.71 D ± 0.42 D(13) and -0.94 D ± 0.40 D(23)). These refractions were consistently lower than the intended astigmatism within each group and showed comparable outcomes between groups (Table 2). One factor should be considered here; the differences between groups were close to the cut-off value at the 6-month re-evaluation. The postoperative spherical equivalents exhibited consistent homogeneity between groups throughout the follow-up period.
The mean visual acuity for both groups is shown in Figure 1. Fi -gu re 1A shows the pre- and postoperative SDCVA. Figure 1B shows the postoperative UDVA (preoperative UDVA was not analyzed in our stu dy). The preoperative SCDVA was slightly better in the toric IOL group. There was no significant difference between groups during the remaining period.
The mean predictability values are shown in Table 3. Predictability oscillated widely within and between groups throughout the follow--up period. We hypothesized that such variations arise from the sub-jective nature of manifest refraction. The mean ∆SE was significantly
Figure 1. A) Preoperative, 1-m., 3-m. and 6-m. postoperative mean SDCVA (logMAR scale). B) One-month, 3-m. and 6-m. postoperative mean UDVA (logMAR scale). (IOL= intraocular lens; LRI= limbal relaxing incisions; m.= n-month postoperative; Preop.= preoperative period; SDCVA= spectacle distance corrected visual acuity; UDVA= uncorrected distance visual acuity).
Table 3. Refractive predictability at 1, 3, and 6 months after surgery
Group
LRI Toric IOL
P-value*Fraction (%) Fraction (%)
1 month after surgery 0.05
∆SE1 ± 1.00 D 27/32 (84.38) 28/30 (93.33) -
∆SE1 ± 0.50 D 17/32 (53.13) 18/30 (60.00) -
3 months after surgery 0.09
∆SE3 ± 1.00 D 30/32 (93.75) 24/30 (80.00) -
∆SE3 ± 0.50 D 24/32 (75.00) 12/30 (40.00) -
P-value† 0.10 0.00
6 months after surgery 0.77
∆SE6 ± 1.00 D 31/32; (96.88) 30/30; (100) -
∆SE6 ± 0.50 D 23/32; (71.88) 18/30; (66.67) -
P value†† 0.02 0.71
D= diopters; IOL= intraocular lens; LRI = limbal relaxing incisions; SD= standard deviation; ∆SE
1= 1-month postoperative spherical equivalent minus preoperative target spherical
equivalent; ∆SE3= 3-month postoperative target spherical equivalent minus preoperative
target spherical equivalent; ∆SE6= 6-month postoperative target spherical equivalent
minus preoperative target spherical equivalent.(*) Mann-Whitney U test for mean ∆SEs between groups at 1, 3, and 6 months after surgery.(†) Wilcoxon test; ∆SE1
(1 month after surgery) vs. ∆SE
3 (3 months after surgery).
(††) Wilcoxon test; ∆SE1 (1 month after surgery)
vs. ∆SE
6 (6 months after surgery).
Table 4. Safety and efficacy indices at 1, 3, and 6 months after surgery
Group
LRI Toric IOL P-value*
1-month postoperative SI
Range 0.00 to 0.60 0.00 to 0.60 -
Mean ± SD 0.11 ± 0.14 0.13 ± 0.20 0.94
3-month postoperative SI
Range 0.00 to 0.33 0.00 to 0.60 -
Mean ± SD 0.10 ± 0.13 0.18 ± 0.21 0.27
P value† 0.92 0.13 -
6-month postoperative SI
Range 0.00 to 0.38 0.00 to 0.60 -
Mean ± SD 0.09 ± 0.12 0.12 ± 0.18 0.81
P value†† 0.66 0.68 -
1-month postoperative EI
Range 0.00 to 1.00 0.00 to 1.00 -
Mean ± SD 0.31 ± 0.18 0.43 ± 0.23 0.01
3-month postoperative EI
Range 0.17 to 1.00 0.00 to 1.00 -
Mean ± SD 0.36 ± 0.18 0.44 ± 0.25 0.04
P value‡ 0.04 0.32 -
6-month postoperative EI
Range 0.17 to 1.00 0.00 to 1.00 -
Mean ± SD 0.37 ± 0.19 0.42 ± 0.27 0.23
P value‡ ‡ 0.03 0.72 -
EI = efficacy index; LRI = limbal relaxing incisions; SD = standard deviation; SI = safety index.(*) Mann-Whitney U test. (†) Wilcoxon test; SI at 1 months vs. SI at 3 months.(††) Wilcoxon test; SI at 1 month vs. SI at 6 months.(‡) Wilcoxon test; EI at 1 month vs. EI at 3 months.(‡ ‡) Wilcoxon test; EI at 1 month vs. EI at 6 months.

Treatment of astigmatism during phacoemulsification
44 Arq Bras Oftalmol. 2014;77(1):40-6
constitutes an advantage of toric IOL implantation over LRI place-ment for the treatment of astigmatism during phacoemulsification.
Figure 2A provides information concerning TIA and SIA trends over time within and between groups; the mean TIAs were com-parable between groups (Mann-Whitney U test; P=0.62); however, the mean SIAs were significantly lower in the LRI group than in the toric IOL group (Mann-Whitney U test; P≤0.01). In addition, the mean SIAs were significantly lower than the mean TIAs in the LRI group (Wilcoxon test P=0.00); this was in accordance with values reported in the current literature, which documents that LRI most often un-dercorrects astigmatism(2,3,10). In both the LRI and toric IOL groups, there were no significant differences in the mean SIAs throughout the follow-up period (Wilcoxon test; P≥0.25). The trend for mean DVs between and within groups over time is presented in Figure 2B. The mean DV was always higher in the LRI group than in the toric IOL group (Mann-Whitney U test; P≤0.03); these differences were signifi-cant. Within each group, the variations over time were statistically in-significant (Wilcoxon test; P≥0.17). Consequently, the toric IOL group outcomes exhibited greater consistency with surgical planning; the mean SIAs were closer to the mean TIAs and lower mean DVs.
Scatterplots of attempted (TIA) versus achieved (SIA) astigmatic changes are shown for the LRI (Figure 3A) and toric IOL groups (Figu-re 3B). For each group, a trendline correlating TIA and SIA has been drawn. The points distributed along the trendline indicate eyes that achieved the desired correction (TIA= SIA). Eyes that were undercor-rected (TIA> SIA) or overcorrected (TIA< SIA) were represented by points under and above the trendline, respectively(12). The strength of such correlations was assessed by Pearson’s R2 to determine the group with the more accurate correction of astigmatism(19). The coe-fficient of determination was greater in the toric IOL group (R2=0.89) than in the LRI group (R2=0.50).
Figure 2. A) Comparison of TIA and SIA means, over time, between LRI and toric IOL groups and within each group. B) Comparison of DV means, over time, between LRI and toric IOL groups. (DV = difference vector; IOL intraocular lens; LRI = limbal relaxing incisions; SIA = surgically induced astigmatism vector; TIA = target induced astigmatism vector; m. = n-month postoperative)
A
B
Figure 3. Scatterplots of attempted astigmatic correction and achieved astigmatic change at 6 months after surgery. A) LRI group. B) Toric IOL group. D= diopters; LRI= limbal relaxing incisions; SIA= surgically induced astigmatism; R2= Pearson’s coefficient of determination; TIA= target induced astigmatism; 6-m PO= 6-month postoperative period
A
B
different between groups only at 1 month after surgery (better in the toric IOL group). In both groups, a considerable number of eyes achie-ved a refraction within 1.00 D (nearly 97% in the LRI group and 100% in the toric IOL group) or within 0.50 D of the goal refraction (nearly 72% in the LRI group and 67% in the toric IOL group); this was in accordance with the values reported in the current literature, which demonstrates that almost 90% patients are within 1.00 D of the goal refraction(24).
The mean SI, as shown in Table 4, remained stable throughout the follow-up period and exhibited no major differences between groups during any follow-up period. The mean EI, also shown in Table 4, increased over time in the LRI group (statistically significant), while they remained stable throughout the follow-up period in the toric IOL group. The EI exhibited lower values at 1 and 3 months after sur-gery, although this difference was no longer important by 6 months after surgery. We believed that the EI trend in the LRI group may be related to cicatricial demands associated with this technique(4); once the cicatricial process of incisions reached completion, the outcomes in the LRI and toric IOL groups became comparable.
Several studies have shown that both LRI and toric IOL implanta-tion provide good safety, predictability, and efficacy associated with a postoperative improvement in visual acuity(3,22,25-36). Such studies, however, made comparisons with control groups. A straightforward comparison between LRI and toric IOL in terms of predictability, sa fety and efficacy is one of the original contributions of our study.
We believe that predictability, safety, and efficacy should be in ter -preted in a complementary fashion, rather than as discrete parame -ters. Our results suggest that both LRI and toric IOL implantation are predictable, safe, and efficient treatment options. Statistically signifi-cant differences, whenever present, are subtle, although they should be taken into account during surgical planning. A slightly greater stability in outcomes over time was found in the toric IOL group; this

Freitas GO, et al.
45Arq Bras Oftalmol. 2014;77(1):40-6
Figure 4. Histogram of the proportion of achieved astigmatic correction at 6 months after surgery. IOL= intraocular lens; ME= magnitude of error; LRI= limbal relaxing incisions; 6-m.= 6-month postoperative period
Alternatively, eyes that achieved the intended astigmatic correc-tion and the under- or overcorrected eyes can be assessed by analy -zing a parameter termed ME. The proportion of eyes that achieved the intended correction and that of under- and overcorrected eyes, determined on the basis of ME, in both groups are shown in Figure 4. Nearly 77% and 44% eyes achieved the intended correction in the toric IOL and LRI groups, respectively. Undercorrection was observed in 17% eyes in the toric IOL group and 53% eyes in the LRI group. Overcorrection was observed in approximately 7% eyes in the toric IOL group and 3% eyes in the LRI group. In our study, the greater number of patients with against the rule and oblique astigmatisms in the LRI group may have induced some bias because such categories of astigmatism are somewhat less responsive to LRI(2,3,10). The propor-tion of eyes that achieved the intended correction in the toric IOL group is remarkable compared with that in the LRI group. Although over-correction occurred in both groups, it was more frequent in the toric IOL group.
Figure 5 depicts 3 indices that, if examined together, enable complete assessment of any astigmatic change: the success of astig-matic surgery, calculated from the index of success (Figure 5A) and indicating a relative measure of success; the flattening index (FI; Figure 5B), related to the proportion of SIA at the TIA axis and suggestive of treatment effectiveness; and the correction index (CI; Figure 5C), the overall astigmatism correction achieved by SIA, representing treat-ment efficacy(7). These indices were better in the toric IOL group than in the LRI group: 57% vs. 43% for the success of astigmatic surgery, 81% vs. 62% for FI, and 94% vs. 64% for CI.
COnCLUSIOnSFrom both nonvectorial and vectorial perspectives, our results
sug gested that toric IOL implantation was advantageous over LRI placement for the treatment of astigmatism during phacoemulsifi-cation. Although such advantages often seem subtle in nonvectorial analysis, their importance is highlighted by the vectorial approach. The main limitation of our study was the considerable proportion of against the rule and oblique astigmatisms found in the LRI group, which introduced some bias of an uncertain extent.
ReFeRenCeS 1. Alió JL, Agdeppa MC, Pongo VC, El Kady B. Microincision cataract surgery with toric
intraocular lens implantation for correcting moderate and high astigmatism: pilot study. J Cataract Refract Surg. 2010;36(1):44-52.
2. Muftuoglu O, Dao L, Cavanagh HD, McCulley JP, Bowman RW. Limbal relaxing incisions at the time of apodized diffractive multifocal intraocular lens implantation to reduce astigmatism with or without subsequent laser in situ keratomileusis. J Cataract Refract Surg. 2010;36(3):456-64.
3. Carvalho MJ, Suzuki SH, Freitas LL, Branco BC, Schor P, Lima AL. Limbal relaxing incisions to correct corneal astigmatism during phacoemulsification. J Refract Surg. 2007;23(5):499-504. Comment in: J Refract Surg. 2008;24(6):562-3.
4. Kamiya K, Shimizu K, Ohmoto F, Amano R. Evaluation of corneal biomechanical pa-rameters after simultaneous phacoemulsification with intraocular lens implantation and limbal relaxing incisions. J Cataract Refract Surg. 2011;37(2):265-70.
5. Mendicute J, Irigoyen C, Aramberri J, Ondarra A, Montés-Micó R. Foldable toric in-traocular lens for astigmatism correction in cataract patients. J Cataract Refract Surg. 2008;34(4):601-7.
6. Alpins N. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19(4):524-33.
7. Alpins N, Goggin M. Practical astigmatism analysis for refractive outcomes in cataract and refractive surgery. Surv Ophthalmol. 2004;49(1):109-22.
8. Geggel HS. Arcuate relaxing incisions guided by corneal topography for postkerato-plasty astigmatism: vector and topographic analysis. Cornea. 2006;25(5):545-57.
9. Kaufmann C, Krishnan A, Landers J, Esterman A, Thiel MA, Goggin M. Astigmatic neutra-lity in biaxial microincision cataract surgery. J Cataract Refract Surg. 2009;35(9):1555-62.
10. Silva EF, Trindade FC. [Surgical correction of astigmatism during cataract surgery]. Arq Bras Oftalmol. 2007;70(4):609-14. Portuguese.
11. Wang L, Misra M, Koch DD. Peripheral corneal relaxing incisions combined with cataract surgery. J Cataract Refract Surg. 2003;29(4):712-22.
12. Hoffmann PC, Auel S, Hütz WW. Results of higher power toric intraocular lens implan-tation. J Cataract Refract Surg. 2011;37(8):1411-8.
Figure 5. Histograms of the success rates at 6 months after surgery. A) Success of as -tig matism surgery 6 months. B) Achieved astigmatic correction at the intended axisC) Percentage of astigmatism corrected. CI × 100= percentage of astigmatism corrected; FI × 100= astigmatism reduction at the intended axis; IOL= intraocular lens; LRI= limbal relaxing incisions; 6-m.= 6-month postoperative period Mann-Whitney U test ≤0.01 for all patients

Treatment of astigmatism during phacoemulsification
46 Arq Bras Oftalmol. 2014;77(1):40-6
13. Visser N, Nuijts RM, deVries NE, Bauer NJ. Visual outcomes and patient satisfaction after cataract surgery with toric multifocal intraocular lens implantation. J Cataract Refract Surg. 2011;37(11):2034-42.
14. Mingo-Botín D, Muñoz-Negrete FJ, Won Kim HR, Morcillo-Laiz R, Rebolleda G, Oblanca N. Comparison of toric intraocular lenses and peripheral corneal relaxing incisions to treat astigmatism during cataract surgery. J Cataract Refract Surg. 2010;36(10):1700-8.
15. Ferrer-Blasco T, García-Lázaro S, Albarrán-Diego C, Belda-Salmerón L, Montés-Micó R. Refractive lens exchange with a multifocal diffractive aspheric intraocular lens. Arq Bras Oftalmol. 2012;75(3):192-6.
16. Behndig A, Montan P, Stenevi U, Kugelberg M, Zetterström C, Lundström M. Aiming for emmetropia after cataract surgery: Swedish National Cataract Register Study. J Cataract Refract Surg. 2012;38(7):1181-6.
17. Goggin M, Moore S, Esterman A. Outcome of toric intraocular lens implantation after adjusting for anterior chamber depth and intraocular lens sphere equivalent power effects. Arch Ophthalmol. 2011;129(8):998-1003. Comment in: Arch Ophthalmol. 2012;130(7):947-8; author reply 948-9. Arch Ophthalmol. 2012;130(7):945-6; author reply 948-9.
18. Razali NM, Wah Y. Power comparisons of Shapiro-Wilk, Kolmogorov-Smirnov, Lilliefors and Anderson-Darling tests. J Statistical Model Analyt [Internet]. 2011[cited 2013 Jan 21];2(1):21-33. Available from: http://instatmy.org.my/downloads/e-jurnal%202/3.pdf
19. Shi R, Conrad S. Correlation and regression analysis. Ann Allergy Asthma Immunol. 2009;103(4):S35-41.
20. Carpenter J, Bithell J. Bootstrap confidence intervals: when, which, what? A practical guide for medical statisticians. Stat Med. 2000;19(9):1141-64.
21. Gudmundsdottir E, Jonasson F, Jonsson V, Stefánsson E, Sasaki H, Sasaki K. “With the rule” astigmatism is not the rule in the elderly - Reykjavik Eye Study: a population based study of refraction and visual acuity in citizens of Reykjavik 50 years and older. Iceland-Japan Co-working Study Group. Acta Ophthalmol Scand. 2000;78(6):642-6.
22. Ganekal S, Dorairaj S, Jhanji V. Limbal relaxing incisions during phacoemulsification: 6-month results. J Cataract Refract Surg. 2011;37(11):2081-2.
23. Alió JL, Piñero DP, Tomás J, Alesón A. Vector analysis of astigmatic changes after cataract surgery with toric intraocular lens implantation. J Cataract Refract Surg. 2011;37(6):1038-49. Comment in: J Cataract Refract Surg. 2011;37(12):2234-5; author reply 2235.
24. Goggin M, Moore S, Esterman A. Toric intraocular lens outcome using the manufac-
tu rer’s prediction of corneal plane equivalent intraocular lens cylinder power. Arch Ophthalmol. 2011;129(8):1004-8. Comment in: Arch Ophthalmol. 2012;130(7):946-7; author reply 948-9; Arch Ophthalmol. 2012;130(7):945-6; author reply 948-9.
25. Arraes JC, Cunha F, Arraes TA, Cavalcanti R, Ventura M. [Limbal relaxing incisions during cataract surgery: one-year follow-up]. Arq Bras Oftalmol. 2006;69(3):361-4. Portugue se.
26. Coloma-Gonzáles I, Gonzáles-Herrera M, Megual-Verdú E, Hueso-Abancens JR. [Lim-bal relaxing incisions and cataract surgery: our experience]. Arch Soc Esp Oftalmol. 2007;82(9):551-4. Spanish.
27. Cristóbal JA, del Buey M, Ascaso FJ, Lanchares E, Calvo B, Doblare M. Effect of limbal relaxing incisions during phacoemulsification surgery based on nomogram review and numerical simulation. Cornea. 2009;28(9):1042-9.
28. Gills JP, Wallace R, Miller K, Fine HI, Friedlander M, McFarland M, et al. Reducing pre-existing astigmatism with limbal relaxing incisions. In: Henderson BA, Gills JP. A complete guide for correcting astigmatism. Thorofare, NJ; Slack: 2003. p.99-119.
29. Ahmed II, Rocha G, Slomovic AR, Climenhaga H, Gohill J, Greagore A, Ma J; Canadian Toric Study Group. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cataract Refract Surg. 2010;36(4):609-16.
30. Bauer NJ, deVries NE, Webers CA, Hendrikse F, Nuijts RM. Astigmatism management in cataract surgery with the AcrySof toric intraocular lens. J Cataract Refract Surg. 2008; 34(9):1483-8.
31. Buckhurst PJ, Wolffsohn JS, Naroo SA, Davies LN. Rotational and centration stability of an aspheric intraocular lens with a simulated toric design. J Cataract Refract Surg. 2010;36(9):1523-8.
32. Correia RJ, Moreira H, Lago-Netto SU, Pantaleão GR. Visual performance after toric IOL implantation in patients with corneal astigmatism. Arq Bras Oftalmol. 2009;72(5):636-40.
33. Debois A, Nochez Y, Bezo C, Bellicaud D, Pisella PJ. [Refractive precision and objective quality of vision after toric lens implantation in cataract surgery]. J Fr Ophthalmol. 2012;35(8):580-6. French.
34. Ernest P, Potvin R. Effects of preoperative corneal astigmatism orientation on results with a low-cylinder-power toric intraocular lens. J Cataract Refract Surg. 2011;37(4):727-32.
35. Forseto AS, Nosé RM, Nosé W. Toric intraocular lens misalignment inducing astigma-tism after refractive surgery. J Refract Surg. 2011;27(9):691-3.
36. Koshy JJ, Nishi Y, Hirnschall N, Crnej A, Gangwani V, Maurino V, et al. Rotational stability of a single-piece toric acrylic intraocular lens. J Cataract Refract Surg. 2010;36(10):1665-70.
XVIII Congresso Internacional da Sociedade Brasileira de Oftalmologia
24 a 26 de julhoHotel Windsor Barra
Rio de Janeiro - RJ
informações: Site: www.congressosbo.com.br

47Arq Bras Oftalmol. 2014;77(1):47-9
Case Report
InTRODUCTIOnIncontinentia pigmenti (IP), also known as Bloch-Suzlberger syn-
drome, is a rare familial disorder affecting the ectodermal structures, with various dermatological, dental, ocular, and neurological features. It is inherited as an X-linked dominant condition and is fatal in males(1).
Diagnosis is made on the basis of skin biopsy. According to Car-ney(2), dental abnormalities occur in 65% patients, neurological ab-nor malities in 30%, and ocular manifestations in 35%. Retinal le sions such as ischemia and new vessel proliferation are the most cha -racteristic ocular findings(3).
This paper describes the cases of two young girls with inconti-nentia pigmenti who were histopathologically diagnosed via skin bio psy and were followed-up for 5 years and >20 years, respectively.
CASe RePORTScase 1
A 4-year-old female presented with total hyphema in the right eye following unsuccessful cataract surgery in 1990. Ultrasound re -vealed complete retinal detachment. Pars plana vitrectomy was performed, albeit with little success, and phthisis developed within a few months. Upon examination, her other eye exhibited lens opacity, an attached retina with some pigment clumping, and a small amount of fibrosis over the macula (Figure 1). The best-corrected visual acuity was 20/400. Her past medical history revealed a cutaneous rash du-ring the neonatal period and 3 seizures in the past year. She was also being treated for dental abnormalities. A clinical diagnosis of inconti-nentia pigmenti was confirmed by skin biopsy. During the follow-up period, myopia increased to -9.00 in the left eye. In 2007, at the age of 21, she developed a cataract and underwent phacoemulsification
and IOL implantation. Her best-corrected visual acuity was restored to 20/400 and has been maintained since then.
case 2A 5-year-old girl presented with pain, hyperemia, and no light
perception in the left eye in 2008. The intraocular pressure (IOP) in the affected eye was 47 mmHg. Ultrasound examination revealed fibrotic tissue extending from the posterior aspect of the lens to the optic nerve. The initial diagnosis was persistent hyper-plastic primary vitreous (PHPV), although closed funnel retinal detachment could not be ruled out. The patient received medical treatment for the increased IOP and developed total hyphema 2 months later. The IOP decreased dramatically to 4 mmHg, and the condition of her left eye progressed to phthisis within a month. The best-corrected visual acuity in the fellow eye was 20/25. In 2010, her myopia increased to -4.00, and during retinal examina-tion, an area of nonperfusion with new vessels was observed in the temporal peripheral retina (Figure 2). Her past medical history revealed a cutaneous rash during the neonatal period, which left pigmented lesions on the abdomen. Dental abnormalities were observed, including 12 missing teeth. Skin biopsy revealed an epidermis with hypopigmentation and a decrea sed melanocyte count, necrotic keratinocytes, and acanthosis. The dermis appe-ared thickened with a discrete inflammatory infiltrate and mela-nophages. Focal areas of degeneration of the basal lamina were present.
The non-perfused retina of the left eye was subjected to laser the-rapy. Six months later, fluorescein angiography revealed only a few leaking vessels and a stable retina (Figure 3). Her best-corrected visual acuity at the last follow-up in April 2013 was 20/20 in the left eye.
Ophthalmic evaluation, treatment, and follow-up of two cases of incontinentia pigmentiAvaliação oftalmológica, tratamento e seguimento de dois casos de incontinentia pigmenti
carloS auGuSTo Moreira neTo1, ana Tereza raMoS Moreira2, carloS auGuSTo Moreira Jr.2
Submitted for publication: June 6, 2013 Accepted for publication: October 24, 2013
Study carried out at Hospital de Olhos do Paraná, Curitiba, Paraná, Brazil.1 Eye Hospital of Paraná, Curitiba, Paraná, Brazil.2 Universidade Federal do Paraná, Curitiba, Paraná, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: C.A. Moreira Neto, None; A.T.R. Moreira, None; C.A. Moreira Jr, None.
Correspondence address: Carlos A. Moreira Neto. Rua Fernando Simas, 1.010 - Curitiba (PR) - 80710-660 - Brazil - E-mail: [email protected]
Número do Projeto: 002/13 – Hospital de Olhos do Paraná
ABSTRACTIncontinentia pigmenti (IP) is an X-linked dominant disorder affecting the skin, teeth, eyes, and central nervous system. Ocular changes are common and may lead to severe vision loss. We report on the ocular manifestations in two young girls with IP, with emphasis on the asymmetry of this condition in both eyes and associated retinal problems. The outcomes of laser treatment of the ischemic peripheral retina were good and resulted in stability of vision.
Keywords: Incontinentia pigmenti/diagnosis; Incontinentia pigmenti/therapy; Laser therapy; Case reports
RESUMOIncontinentia pigmenti (IP) é uma desordem ligada ao X dominante afetando a pele, dentes, olhos e sistema nervoso central. Alterações oculares são comuns e podem levar a severa perda visual. Nós relatamos manifestações oculares de duas jovens pacientes com IP, enfatizando a assimetria da condição em cada olho e também alterações retinianas que possam ocorrer. Tratamento a laser na periferia isquêmica da retina gera bons resultados e estabiliza a visão.
Descritores: Incontinência pigmentar/diagnóstico; Incontinência pigmentar/terapia; Terapia a laser; Relatos de casos
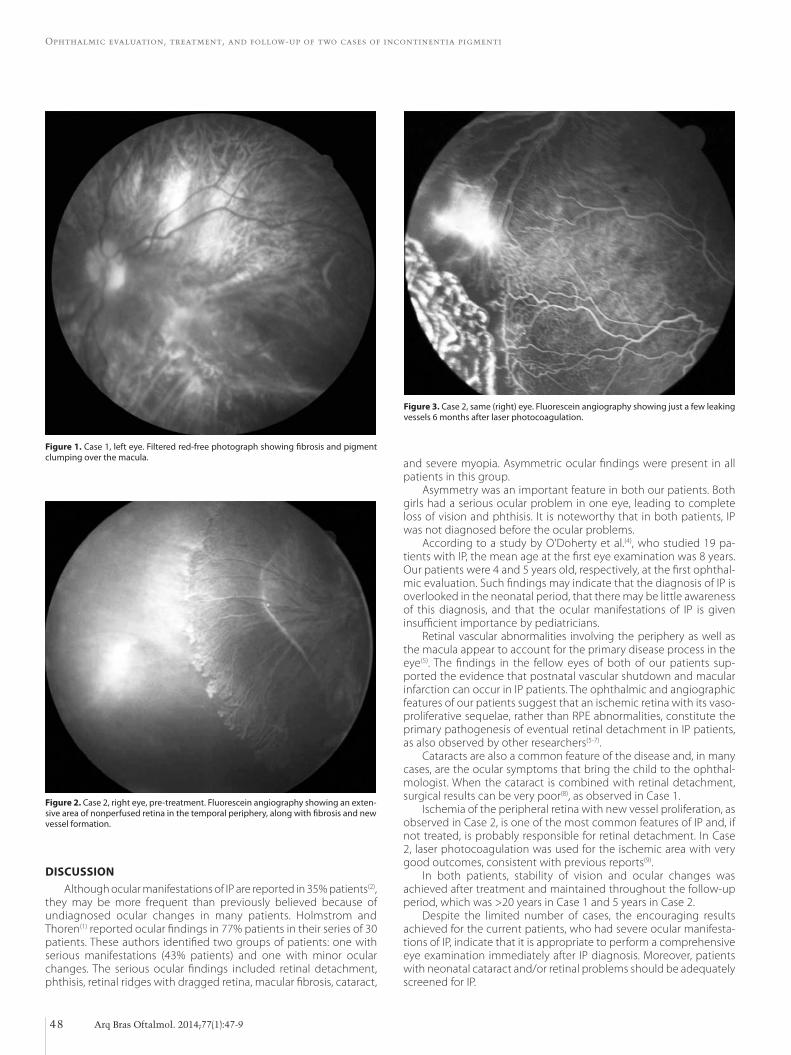
Ophthalmic evaluation, treatment, and follow-up of two cases of incontinentia pigmenti
48 Arq Bras Oftalmol. 2014;77(1):47-9
DISCUSSIOnAlthough ocular manifestations of IP are reported in 35% patients(2),
they may be more frequent than previously believed because of undiagnosed ocular changes in many patients. Holmstrom and Thoren(1) reported ocular findings in 77% patients in their series of 30 patients. These authors identified two groups of patients: one with serious manifestations (43% patients) and one with minor ocular changes. The serious ocular findings included retinal detachment, phthisis, retinal ridges with dragged retina, macular fibrosis, cataract,
Figure 1. Case 1, left eye. Filtered red-free photograph showing fibrosis and pigment clumping over the macula.
Figure 2. Case 2, right eye, pre-treatment. Fluorescein angiography showing an exten-sive area of nonperfused retina in the temporal periphery, along with fibrosis and new vessel formation.
Figure 3. Case 2, same (right) eye. Fluorescein angiography showing just a few leaking vessels 6 months after laser photocoagulation.
and severe myopia. Asymmetric ocular findings were present in all patients in this group.
Asymmetry was an important feature in both our patients. Both girls had a serious ocular problem in one eye, leading to complete loss of vision and phthisis. It is noteworthy that in both patients, IP was not diagnosed before the ocular problems.
According to a study by O’Doherty et al.(4), who studied 19 pa-tients with IP, the mean age at the first eye examination was 8 years. Our patients were 4 and 5 years old, respectively, at the first ophthal-mic evaluation. Such findings may indicate that the diagnosis of IP is overlooked in the neonatal period, that there may be little awareness of this diagnosis, and that the ocular manifestations of IP is given insufficient importance by pediatricians.
Retinal vascular abnormalities involving the periphery as well as the macula appear to account for the primary disease process in the eye(5). The findings in the fellow eyes of both of our patients sup-ported the evidence that postnatal vascular shutdown and macular infarction can occur in IP patients. The ophthalmic and angiographic features of our patients suggest that an ischemic retina with its vaso-proliferative sequelae, rather than RPE abnormalities, constitute the primary pathogenesis of eventual retinal detachment in IP patients, as also observed by other researchers(5-7).
Cataracts are also a common feature of the disease and, in many cases, are the ocular symptoms that bring the child to the ophthal-mologist. When the cataract is combined with retinal detachment, surgical results can be very poor(8), as observed in Case 1.
Ischemia of the peripheral retina with new vessel proliferation, as observed in Case 2, is one of the most common features of IP and, if not treated, is probably responsible for retinal detachment. In Case 2, laser photocoagulation was used for the ischemic area with very good outcomes, consistent with previous reports(9).
In both patients, stability of vision and ocular changes was achieved after treatment and maintained throughout the follow-up period, which was >20 years in Case 1 and 5 years in Case 2.
Despite the limited number of cases, the encouraging results achieved for the current patients, who had severe ocular manifesta-tions of IP, indicate that it is appropriate to perform a comprehensive eye examination immediately after IP diagnosis. Moreover, patients with neonatal cataract and/or retinal problems should be adequately screened for IP.

Moreira Neto CA, et al.
49Arq Bras Oftalmol. 2014;77(1):47-9
ReFeRenCeS 1. Holmström G, Thorén K. Ocular manifestations of incontinentia pigmenti. Acta
Ophthalmol Scand. 2000;78(3):348-53. 2. Carney RG. Incontinentia pigmenti. A world statistical analysis. Arch Dermatol. 1976;
112(4):535-42. 3. Goldberg MF, Custis PH. Retinal and other manifestations of incontinentia pigmenti
(Bloch-Sulzberger syndrome). Ophthalmology. 1993;100(11):1645-54. 4. O’Doherty M, Mc Creery K, Green AJ, Tuwir I, Brosnahan D. Incontinentia pigmenti-
ophthalmological observation of a series of cases and review of the literature. Br J Ophthalmol. 2011;95(1):11-6. Review.
5. Goldberg MF. The blinding mechanisms of incontinentia pigmenti. Trans Am Oph-thalmol Soc. 1994;92:167-76; discussion 176-9.
6. François J. Incontinentia pigmenti (Bloch-Sulzberger syndrome) and retinal changes. Br J Ophthalmol. 1984;68(1):19-25.
7. Spallone A. Incontinentia pigmenti (Bloch-Sulzberger syndrome): seven case reports from one family. Br J Ophthalmol. 1987;71(8):629-34.
8. Wald KJ, Mehta MC, Katsumi O, Sabates NR, Hirose T. Retinal detachments in incon-tinentia pigmenti. Arch Ophthalmol. 1993;111(5):614-7.
9. Nguyen JK, Brady-Mccreery KM. Laser photocoagulation in preproliferative retinopathy of incontinentia pigmenti. J AAPOS. 2001;5(4):258-9.
10o Simpósio Internacional de Glaucoma da UnICAMP
23 e 24 de maioHotel Maksoud Plaza
São Paulo - SP
informações: E-mail: [email protected]

50 Arq Bras Oftalmol. 2014;77(1):50-3
Case Report
InTRODUCTIOn Cyclodialysis clefts are areas of disinsertion of the meridional ci -
liary muscle fibers from their attachment at the scleral spur, allowing direct communication between the anterior chamber and the cilio-choroidal space. Previously, cyclodialysis was intentionally caused during an obsolete surgical technique for treating glaucoma(1,2). No -wadays, it is mainly caused by severe blunt ocular trauma(3,4), which cau ses momentary axial compression and a rapid compensatory equa torial expansion that stretches the ocular tissue, resulting in separation and tearing of the tissue. Intraocular surgeries that mani-pulate the iris were also reported to be important causes of iatrogenic cyclodialysis(1,3,5), which became less common with the development of better intraocular surgical techniques.
Cyclodialysis is a rare condition(3,6) and results in a shallow anterior chamber, ciliochoroidal detachment, ocular hypotony, and hypotony maculopathy with loss of vision(5,7,8).
Gonioscopy is the best way to examine the structures of the angle(9), but in some eyes with shallow anterior chambers, hyphema, and corneal opacity, a cyclodialysis cleft may not be visible on clinical examination(3,4,6). To diagnose these clefts and evaluate the location and extent of the cyclodialysis and suprachoroidal effusion, ultra-sound biomicroscopy (UBM) is of particular importance(3,5,7,10).
Several modalities for surgical and nonsurgical treatment of hypotony maculopathy have been proposed(6): medical treatment(10) (long-acting cycloplegic agents such as 1% atropine sulfate), argon laser cleft photocoagulation, ciliochoroidal diathermy, anterior scleral buckle, transscleral Nd:YAG laser cyclophotocoagulation, transscleral diode laser therapy, direct cyclopexy(1,11), vitrectomy, transscleral cryo therapy with or without gas endotamponade, endoscopic sur-gery, indirect cyclopexy, and other surgical techniques. The best treat-ment for these cases remains controversial, although recent publica-tions show better results with direct cyclopexy surgery(4).
Here we present a case of traumatic cyclodialysis not identified by gonioscopy and associated with hypotony maculopathy, which was evaluated by UBM before and after direct cyclopexy surgery.
case reportA 41-year-old male Caucasian presented with a complaint of
pro gressive blurred vision in his left eye after suffering blunt ocular trauma 2 months back.
At the time of presentation, he was undergoing medical treat-ment for hypotony (cycloplegic and steroid drops), and his Snellen best-corrected visual acuity (BCVA) was 20/20 in the right eye (OD) and counting fingers in the left eye (OS). Slit-lamp examination
Direct cyclopexy surgery for post-traumatic cyclodialysis with persistent hypotony: ultrasound biomicroscopic evaluationCiclopexia direta em ciclodiálise pós-traumática com hipotonia ocular persistente - acompanhamento por biomicroscopia ultrassônica (UBM)
Fabiola MurTa1, SoMaia MiTne1,2, norMa alleMann2, auGuSTo paranhoS Junior3
Submitted for publication: November 4, 2013 Accepted for publication: November 18, 2013
Study carried out at Universidade Federal de São Paulo.1 Department of Ophthalmology, Ocular Trauma section, Universidade Federal de São Paulo, UNIFESP,
São Paulo (SP), Brazil.2 Department of Ophthalmology, Ultrasound section, Universidade Federal de São Paulo, UNIFESP,
São Paulo (SP), Brazil. 3 Department of Ophthalmology, Glaucoma section, Universidade Federal de São Paulo, UNIFESP,
São Paulo (SP), Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: F. Murta, None; S. Mitne, None; N. Allemann, None; A. Paranhos Jr, None.
Correspondence address: Norma Allemann. Rua Olimpíadas, 134 - Conj. 51 - São Paulo (SP) - 04551-000 - Brazil - E-mail: [email protected]
ABSTRACTCyclodialysis is a relatively rare condition usually caused by ocular injury; however, it can also be caused iatrogenically during intraocular surgery. Hypotony maculo-pathy is the most important complication and the primary reason for visual loss. Clinical diagnosis using gonioscopy may be difficult, and ultrasound biomicroscopy (UBM) can be an alternative. There are different kinds of treatments, and the opti-mal one remains controversial. Here we describe a case of traumatic cyclodialysis with persistent ocular hypotony treated by direct cyclopexy, as illustrated by UBM performed before and after surgery.
Keywords: Refractive errors/surgery; Eye injuries/complications; Eye injuries/ultrasonography; Ocular hypotension/etiology; Ciliary body/injuries; Gonioscopy; Tomography, optical coherence/methods; Microscopy/methods; Visual acuity; Case reports; Humans; Male; Adult
RESUMOCiclodiálise é uma condição relativamente rara, geralmente devido a um trauma ocular, mas também pode ser causada iatrogenicamente como consequência de cirurgia intraocular. A maculopatia hipotônica é a complicação mais importante e a principal razão para a perda visual nessa situação. O diagnóstico clínico por gonioscopia pode ser difícil e a biomicroscopia ultrassônica (UBM) pode ser uma alternativa. Existem diferentes tipos de tratamentos e algumas controvérsias sobre a melhor opção. Neste relato, nós descrevemos um caso de ciclodiálise traumática com hipotonia ocular persistente tratado por cyclopexia direta avaliado por UBM antes e depois da cirurgia.
Descritores: Erros de refração/cirurgia; Lesão nos olhos/complicações; Lesão nos olhos/ultrassonografia; Hipotensão ocular/etiologia; Corpo ciliar/lesões; Gonioscopia; Tomografia de coerência óptica/métodos; Microscopia/métodos; Acuidade visual; Relato de caso; Humanos; Masculino; Adulto

Murta F, et al.
51Arq Bras Oftalmol. 2014;77(1):50-3
revealed a normal right eye and inferior corectopia; a hemorrhagic, prolapsed vitreous body into the anterior chamber; phacodonesis; iridodonesis; and mild cataract in the left eye. The intraocular pressure (IOP) was 18 mmHg in OD and 0 mmHg in OS. Gonioscopy of OS revealed inferior angle recession. Fundus examination revealed optic disc edema, chorioretinal folds radiating around the macula, tortuosity and dilatation of the retinal vessels (Figure 1A), and a nasal choroidal rupture.
B-scan, 10-MHz ultrasonography revealed superior peripheral cho roidal detachment (10 o’clock to 2 o’clock position), an attached retina, optic disc edema, and choroidal thickening (Figure 1B). UBM (50-MHz immersion technique) revealed an anterior chamber depth of 3.0 mm, vitreous herniation into the anterior chamber (Figure 2A), inferior corectopia, apposition of the peripheral iris to the posterior surface of the cornea (Figure 2B), a suspected cyclodialysis cleft at the 7 o’clock position (Figure 2C), and a 360° ciliary body detachment showing a cavernous pattern of the suprachoroidal space (Figure 2D).
Because of the extensive ciliary body detachment, persistent hypotony with important visual impairment, and the failure of clinical treatment, surgical intervention was indicated. Direct cyclopexy was performed for the 4 quadrants, as described in figures 3 A-C. Four days after surgery, the BCVA was 20/200, IOP was 14 mmHg, the an-terior chamber depth was restored, and fundus examination revealed complete resolution of the retinal folds and no optic disc edema (Fi-gure 1C), as confirmed by B-scan ultrasound (Figure 1D). On the 14th day, the postoperative IOP increased to 40 mmHg and was controlled with oral acetazolamide, topical apraclonidine, and timolol, following which it decreased to 19 mmHg without medication after 45 days of surgery, when the BCVA was 20/50. At 5 months, the BCVA was 20/40, the IOP was 18 mmHg, there was a +1/+4 nuclear cataract, and some residual inferior corectopia with a scar on the scleral flaps sites. There were no signs of maculopathy on ophthalmoscopy. Three years after surgery, the BCVA was 20/50 with a potential acuity meter result of 20/40 and the IOP was 18 mmHg. UBM revealed a +2/+4 nuclear ca-taract, while gonioscopy revealed a residual cyclodialysis cleft at the 7 o’clock position with residual angle recession. Fundus examination
showed a discreet pigment irregularity in the macula and a nasal cho-roidal rupture scar. UBM revealed complete ciliary body attachment, residual inferior corectopia, a residual cyclodialysis cleft inferiorly (from the 5 o’clock position to the 8 o’clock position, probably not observed on gonioscopy because of anterior synechiae), and angle recession at the 9-10 o’clock position (Figures 4A-C).
discussionThe term hypotony maculopathy indicates the inward collapse of
the scleral wall caused by ocular hypotony. Severe persistent ocular hypotony leads to progressive cataract, chronic inflammation, cilio-choroidal effusion, and hypotony maculopathy with marked vision loss(1,8). The primary decrease in vision can be related to chorioretinal folds in the macular area, with distortion and malalignment of the retinal photoreceptors. Once the IOP returns to normal, the folds may disappear completely(8). In cases of prolonged hypotony, pigmented lines resulting from changes in the retinal pigment epithelium (RPE) may persist and decrease the final visual acuity(9). Another primary cause of visual decrease in severe hypotony is the decrease in the an teroposterior diameter, which induces relative hyperopia(3).
Hypotony in patients with traumatic ciliary body detachment is caused by a combination of increased uveoscleral outflow via the ciliochoroidal space and a decrease in aqueous production(2,4,5,10), thus decreasing the IOP to levels usually lower than 5 mmHg. Although some points on the physiopathology of ocular hypotony caused by cyclodialysis, such as the lack of association between the size of the cleft and the degree of hypotony(2,4,5,9), remain to be clarified, the extent of ciliary body detachment does not seem to be connected to the intensity of hypotony.
UBM is a useful tool for imaging the anterior segment, allowing the visualization of its structures even in the presence of media opa-cities(4,5,9,10). It can be used as an aid in the diagnosis of cyclodialysis undetectable by gonioscopy(5,11). Although gonioscopy is the gold
A B
C D
Figure 1. Color images obtained and 10-MHz ultrasound performed before and after surgery. A) A preoperative color image obtained 2 months after blunt ocular trauma shows retinal folds with peripapillary heaping of the disc margins and tortuosity and dilatation of the retinal vessels. B) Preoperative 10-MHz ultrasound performed 2 months after blunt trauma shows optic disc edema and choroidal thickening. C) A color image obtained 4 days after surgery for direct cycloplegy shows total resolution of the retinal folds and heaping of the disc margins. D) 10-MHz ultrasound performed 4 days after direct cyclopexy shows resolution of optic disc edema.
Figure 2. Ultrasound biomicroscopy (UBM) performed at 50 MHz using the immersion technique after blunt trauma. A) Anterior chamber depth of 3.0 mm, vitreous herniation into the anterior chamber (arrow). B) Inferior angle demonstrating apposition of the peripheral iris (black arrow) to the posterior surface of the cornea associated with vitreous prolapse through the pupil (white arrow). C) A suspected cyclodialysis cleft (black arrow) at the 7 o’clock position. D) Ciliary body detachment (cavernous pattern of the suprachoroidal space; black arrow) in 360°.
A B
C D
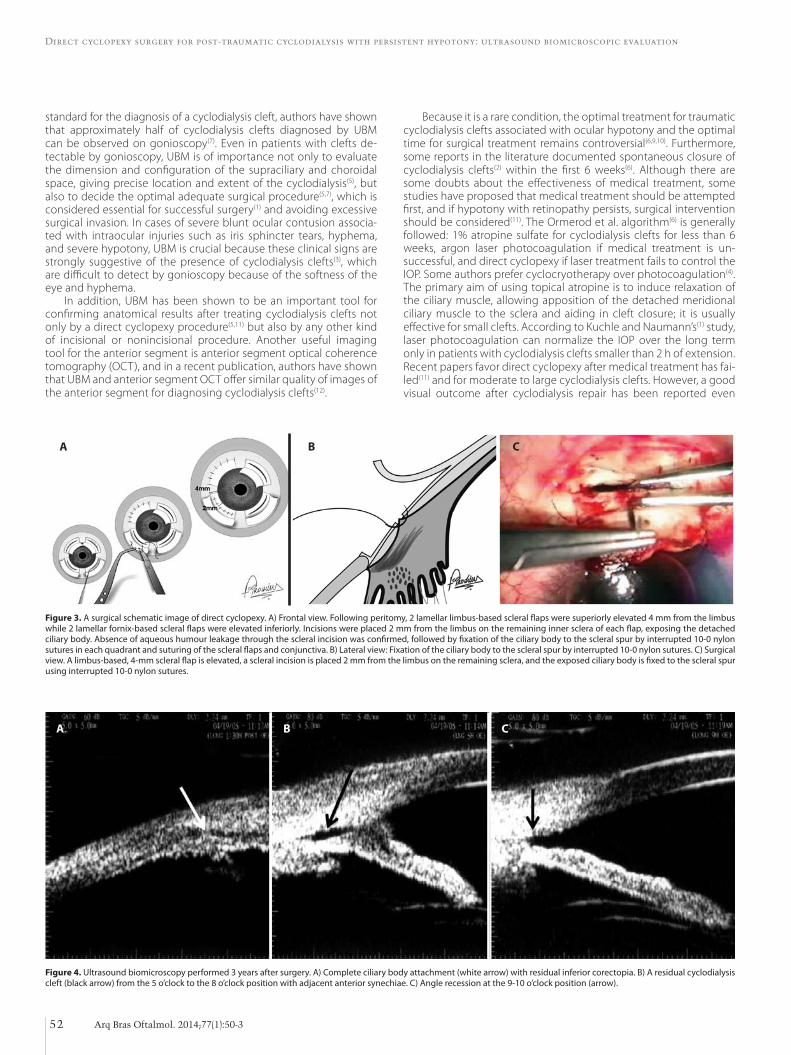
Direct cyclopexy surgery for post-traumatic cyclodialysis with persistent hypotony: ultrasound biomicroscopic evaluation
52 Arq Bras Oftalmol. 2014;77(1):50-3
Figure 4. Ultrasound biomicroscopy performed 3 years after surgery. A) Complete ciliary body attachment (white arrow) with residual inferior corectopia. B) A residual cyclodialysis cleft (black arrow) from the 5 o’clock to the 8 o’clock position with adjacent anterior synechiae. C) Angle recession at the 9-10 o’clock position (arrow).
A B C
standard for the diagnosis of a cyclodialysis cleft, authors have shown that approximately half of cyclodialysis clefts diagnosed by UBM can be observed on gonioscopy(7). Even in patients with clefts de-tectable by gonioscopy, UBM is of importance not only to evaluate the dimension and configuration of the supraciliary and choroidal space, giving precise location and extent of the cyclodialysis(5), but also to decide the optimal adequate surgical procedure(5,7), which is considered essential for successful surgery(1) and avoiding excessive surgical invasion. In cases of severe blunt ocular contusion associa-ted with intraocular injuries such as iris sphincter tears, hyphema, and severe hypotony, UBM is crucial because these clinical signs are strongly suggestive of the presence of cyclodialysis clefts(3), which are difficult to detect by gonioscopy because of the softness of the eye and hyphema.
In addition, UBM has been shown to be an important tool for confirming anatomical results after treating cyclodialysis clefts not only by a direct cyclopexy procedure(5,11) but also by any other kind of incisional or nonincisional procedure. Another useful imaging tool for the anterior segment is anterior segment optical coherence tomography (OCT), and in a recent publication, authors have shown that UBM and anterior segment OCT offer similar quality of images of the anterior segment for diagnosing cyclodialysis clefts(12).
Because it is a rare condition, the optimal treatment for traumatic cyclodialysis clefts associated with ocular hypotony and the optimal time for surgical treatment remains controversial(6,9,10). Furthermore, some reports in the literature documented spontaneous closure of cyclodialysis clefts(2) within the first 6 weeks(6). Although there are some doubts about the effectiveness of medical treatment, some studies have proposed that medical treatment should be attempted first, and if hypotony with retinopathy persists, surgical intervention should be considered(11). The Ormerod et al. algorithm(6) is generally followed: 1% atropine sulfate for cyclodialysis clefts for less than 6 weeks, argon laser photocoagulation if medical treatment is un-successful, and direct cyclopexy if laser treatment fails to control the IOP. Some authors prefer cyclocryotherapy over photocoagulation(4). The primary aim of using topical atropine is to induce relaxation of the ciliary muscle, allowing apposition of the detached meridional ciliary muscle to the sclera and aiding in cleft closure; it is usually effective for small clefts. According to Kuchle and Naumann’s(1) study, laser photocoagulation can normalize the IOP over the long term only in patients with cyclodialysis clefts smaller than 2 h of extension. Recent papers favor direct cyclopexy after medical treatment has fai-led(11) and for moderate to large cyclodialysis clefts. However, a good visual outcome after cyclodialysis repair has been reported even
Figure 3. A surgical schematic image of direct cyclopexy. A) Frontal view. Following peritomy, 2 lamellar limbus-based scleral flaps were superiorly elevated 4 mm from the limbus while 2 lamellar fornix-based scleral flaps were elevated inferiorly. Incisions were placed 2 mm from the limbus on the remaining inner sclera of each flap, exposing the detached ciliary body. Absence of aqueous humour leakage through the scleral incision was confirmed, followed by fixation of the ciliary body to the scleral spur by interrupted 10-0 nylon sutures in each quadrant and suturing of the scleral flaps and conjunctiva. B) Lateral view: Fixation of the ciliary body to the scleral spur by interrupted 10-0 nylon sutures. C) Surgical view. A limbus-based, 4-mm scleral flap is elevated, a scleral incision is placed 2 mm from the limbus on the remaining sclera, and the exposed ciliary body is fixed to the scleral spur using interrupted 10-0 nylon sutures.
A B C

Murta F, et al.
53Arq Bras Oftalmol. 2014;77(1):50-3
after several years of severe ocular hypotony(1,4,6,11), and some authors found no correlation between the duration of hypotony and final visual acuity(1,2,4,11). Furthermore, there appears to be no connection between the cleft extent and the final visual outcome; instead, the pe riod required for IOP normalization after direct cyclopexy seems to be correlated to the final visual acuity(11).
Despite this controversy, a majority of authors agree that treat-ment should not be postponed because of the possibility of perma-nent vision loss by retinal damage. We believe that while deciding the optimal therapy for cyclodialysis, not only the duration of hypotony but also the extent of cyclodialysis and degree of visual impairment should be taken into account.
Direct cyclopexy is a well-known and effective approach(1,11); it allows the treatment of large areas of cyclodialysis and is an alterna-tive therapy for phakic patients. Direct cyclopexy was the first choice in the present phakic patient because of the large extent of ciliocho-roidal detachment, evident hypotony maculopathy, and important visual impairment.
Possible complications of direct cyclopexy include intraocular he morrhage, endophthalmitis, cataract, vitreous loss, retinal detach-ment, wound dehiscence, anterior segment ischemia, and secondary glaucoma due to peripheral anterior synechiae. Reversible pressure spikes in the early postoperative course of direct cyclodialysis have been reported after successful closure of the cyclodialysis cleft(1,4,8), a condition that can occur in association with other treatment moda-lities for cyclodialysis(6,9,10), even after spontaneous cleft closure(2). A transient increase in the IOP may assist the resolution of retinal folds and facilitate the adhesion of the ciliary body and sclera(1). Authors have commented that this transient and early IOP spike has no corre-lation with residual anatomical angle damage(4). Although our patient had a residual cleft after surgery, no clinical effect on the IOP was observed on long-term follow-up, probably because the cleft may have closed at its posterior site. It has been reported that small clefts remaining after treatment do not influence the IOP(1,2,6).
In conclusion, cyclodialysis can lead to persistent hypotony, thus increasing the possibility of permanent visual loss. Subsidiary exami-nations such as UBM aids in diagnosis and treatment of cyclodialysis by determining its real dimensions and location, thus guiding the surgeon during surgical repair. In addition, it aids in the evaluation of anatomical surgical success. Cyclopexy can be an effective treat-ment, particularly in patients with extensive cyclodialysis leading to hypotony maculopathy.
ReFeRenCeS 1. Kuchle M, Naumann GO. Direct cyclopexy for traumatic cyclodialysis with persisting
hypotony. Report in 29 consecutive patients. Ophthalmology. 1995;102(2):322-33. Comment in: Ophthalmology. 1995;102(10):1413.
2. Chandler PA, Maumenee AE. A major cause of hypotony. Am J Ophthalmol. 1961; 52:609-18.
3. Ioannidis AS, Barton K. Cyclodialysis cleft: causes and repair. Curr Opin Ophthalmic. 2010;21(2):150-4.
4. Agrawal P, Shah P. Long-term outcomes following the surgical repair of traumatic cyc lodialysis clefts. Eye (Lond). 2013. [Epub ahead of print].
5. Gentile RC, Pavlin CJ, Liebmann JM, Easterbrook M, Tello C, Foster FS, et al. Diagnosis of traumatic cyclodialysis by ultrasound biomicroscopy. Ophthalmic Surg Lasers. 1996; 27(2):97-105.
6. Ormerod LD, Baerveldt G, Sunalp MA, Riekhof FT. Management of the hypotonus cyclodialysis cleft. Ophthalmology. 1991;98(9):1384-93.
7. Roters S, Engels BF, Szurman P, Krieglstein GK. Typical ultrasound biomicroscopic findings seen in ocular hypotony. Ophthalmologica. 2002;216(2):90-5.
8. Demeler U. Surgical management of ocular hypotony. Eye (Lond). 1988;2(Pt 1):77-9. 9. Lopes Filho JG, Costa VP, Goldbaum M. Hipotonia ocular secundária à ciclodiálise:
des crição de 4 casos e revisão de literatura. Arq Bras Oftalmol. 1997;60(6):626-30. 10. Kamei C, Kato T, Tsukamoto H, Mishima HK. A case of traumatic cyclodialysis followed
by ultrasound biomicroscopy. Hiroshima J Med Sci. 2002;51(3);81-4. 11. Hwang JM, Ahn K, Kim C, Park KA, Kee C. Ultrasonic biomicroscopic evaluation
of cyclodialysis before and after direct cyclopexy. Arch Ophthalmol. 2008;126(9): 1222-5.
12. Mateo-Montoya A, Dreifuss S. Anterior segment optical coherence tomography as a diagnostic tool for cyclodialysis clefts. Arch Ophthalmol. 2009;127(1):109-10.
IV Simpósio de Atualização em Oftalmologia
7 de junho de 2014Hospital Banco de Olhos de Porto Alegre
Porto Alegre - RS
informações: Tel.: (51) 3018-3123

54 Arq Bras Oftalmol. 2014;77(1):54-6
Case Report
InTRODUCTIOnMultiple primary tumors (MPT) are rare and have different clinical
presentations. Historically, Warren and Gates defined MPT as tumors that are histologically confirmed as malignant, separated by at least 2 cm of normal mucosa, and/or chronologically separated by at least 5 years, excluding metastatic tumors. When tumors develop simul-taneously or within 6 months after discovery of the primary tumor, they are considered to be synchronous tumors. If this period exceeds 6 months, they are defined as metachronous tumors(1). The most common findings are related to the presence of 2 tumors, and the gastrointestinal tract, breast, and skin are the most commonly invol-ved primary sites. In the scientific literature, there are few descriptions of lymphoma as one of the primary types of MPT, and an association with the mantle cell lymphoma subtype is even more infrequent and results in a worse prognosis(1,2).
The term mantle cell lymphoma was first used in 1993 to describe the specific subtype of non-Hodgkin B-cell lymphoma with specific clinical and histopathological characteristics(3). It accounts for 3%-7% of all non-Hodgkin lymphomas and 1%-9% of all lymphomas in the periocular region(3-5). This disease primarily affects men aged over 60 years and is usually a widespread and aggressive tumor(3,4). Because of its rarity, most of the descriptions in the literature are case reports, with some cases described in a large case series of lymphoma(4,6).
Here we present an atypical case of metachronous MPT associa-ted with basal cell carcinoma of the skin, intestinal adenocarcinoma
with regional lymph node metastasis, and non-Hodgkin B-cell mantle cell lymphoma of the bilateral orbits with systemic findings.
CASe RePORTA 73-year-old man who was retired and born and raised in São
Bernardo do Campo, São Paulo, presented with a complaint of bilate-ral eyelid edema with low visual acuity since 1 year and 6 months. The symptoms had first appeared on the left and progressed to the right. His family history included a brother who died of an abdominal tumor (exact type unknown). His ophthalmological history included bilate-ral cataract surgery performed 5 years back. His past medical history included non-Hodgkin B-cell small cell lymphoma diagnosed in the first semester of 2010 through pleural biopsy and cervical lymph node involvement (Figure 1A and 1B); basal cell carcinoma diagnosed in the second semester of 2010 through biopsy of the skin over the right and left scapular area, left forehead, and chin (Figure 1C and 1D); and intestinal adenocarcinoma diagnosed in January 2011 through histopathological analysis of a piece of intestine removed during emergency surgery (right hemicolectomy and bowel resection for perforated acute abdomen), with regional lymph node metastases (Figure 1 e and 1F).
Ectoscopy revealed bilateral proptosis, bilateral bulging in the upper and lower eyelid regions, which was more prominent on the left, and the presence of a solid lesion that was adherent to the deep planes and painless after significant reduction of the palpebral fissure
Case report of a metachronous multiple tumor: Mantle cell lymphoma in the orbital region associated with epithelial malignancies at other sitesTumor múltiplo metacrônico: linfoma do manto na região orbital associado a neoplasias malignas epiteliais em outros sítios - relato de caso
Juliana S. F. Medrado1, MirTha raMírez diTTrich1, Jacqueline M. SouSa1, luiz F. Teixeira1, paulo GóiS ManSo1
Submitted for publication: August 27, 2013 Accepted for publication: October 07, 2013
Study carried out at Orbital Disorders Service, Department of Ophthalmology, Universidade Federal de São Paulo.
1 Orbital Disorders Service, Department of Ophthalmology, Universidade Federal de São Paulo, SP, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: J.S.F. Medrado, None; M.R. Dittrich, None; J.M. Sousa, None; L.F. Teixeira, None; P.G. Manso, None.
Correspondence address: Jacqueline M. Sousa. Rua Botucatu, 821 - São Paulo (SP) - 04023-062 - Brazil - E-mail: [email protected]
ABSTRACTHere we report the case of a 73-year-old man who was diagnosed with metachro-nous, multiple primary tumors with non-Hodgkin B-cell mantle cell lymphoma involving the orbit on the basis of biopsy and immunohistochemistry in 2012. The patient had been diagnosed with non-Hodgkin small cell lymphoma and basal cell skin carcinoma in 2010 and intestinal adenocarcinoma with metastasis to the regional lymph nodes in 2011, thus representing a typical case of metachronous, multiple primary tumors. Mantle cell lymphoma is a rare disease and its prog-nosis is quite poor, particularly when it is associated with other metachronous malignancies. Therefore, physicians should consider mantle cell lymphoma as a differential diagnosis for neoplasms of the orbit.
Keywords: Lymphoma, mantle cell/diagnosis; Orbital neoplasms/diagnosis; Lym-phoma, non-Hodgkin; Case report
RESUMORelatamos um caso de linfoma não-Hodgkin de células B subtipo células do manto acometendo região orbital, com o diagnóstico confirmado pela biópsia e testes imuno- -histoquímicos em 2012. O paciente apresentava história de linfoma não-Hodgkin de pequenas células em 2010, carcinoma basocelular de pele no mesmo ano e adenocar-cinoma intestinal com metástase para linfonodos regionais em 2011; caracterizando um caso de tumor primário múltiplo metacrônico. O linfoma de células do manto é uma doença rara, ainda mais quando associado a outras neoplasias metacrônicas, apresentando prognóstico bastante reservado. Dessa forma, deve estar entre os diag -nósticos diferenciais de neoplasias da órbita.
Descritores: Linfoma de células do manto/diagnóstico; Neoplasias orbitárias; Linfoma não Hodgkin; Relato de caso
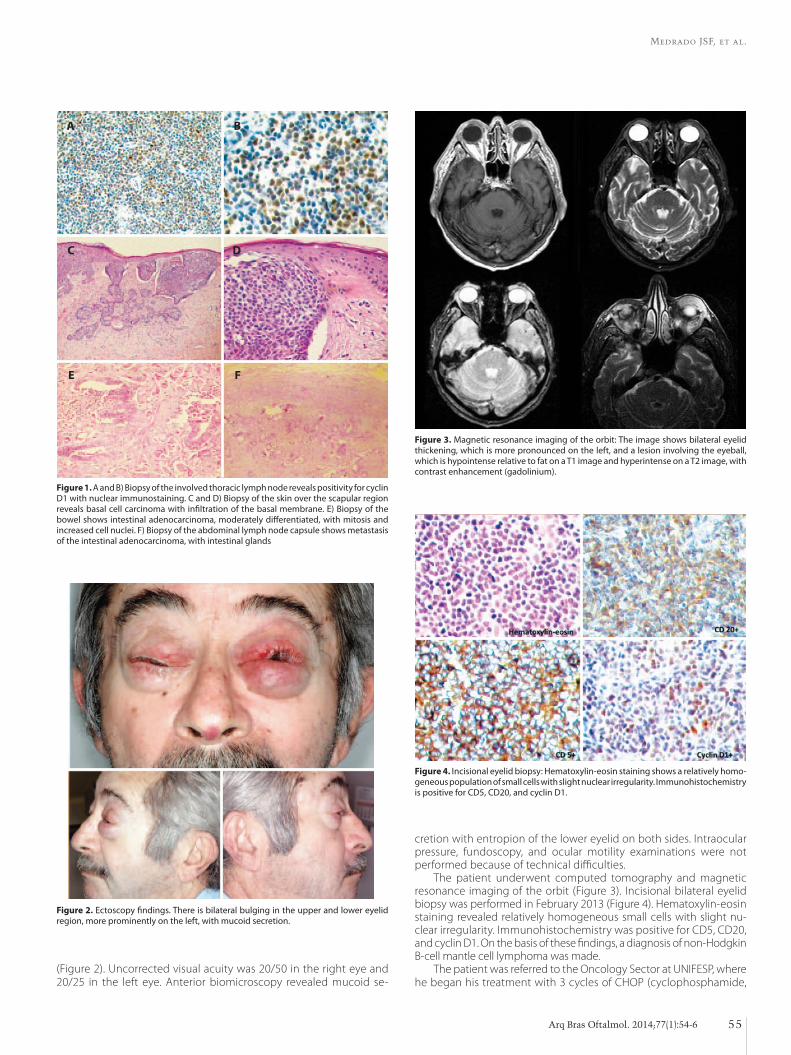
Medrado JSF, et al.
55Arq Bras Oftalmol. 2014;77(1):54-6
cretion with entropion of the lower eyelid on both sides. Intraocular pressure, fundoscopy, and ocular motility examinations were not performed because of technical difficulties.
The patient underwent computed tomography and magnetic resonance imaging of the orbit (Figure 3). Incisional bilateral eyelid biopsy was performed in February 2013 (Figure 4). Hematoxylin-eosin staining revealed relatively homogeneous small cells with slight nu-clear irregularity. Immunohistochemistry was positive for CD5, CD20, and cyclin D1. On the basis of these findings, a diagnosis of non-Hodgkin B-cell mantle cell lymphoma was made.
The patient was referred to the Oncology Sector at UNIFESP, where he began his treatment with 3 cycles of CHOP (cyclophosphamide,
Figure 1. A and B) Biopsy of the involved thoracic lymph node reveals positivity for cyclin D1 with nuclear immunostaining. C and D) Biopsy of the skin over the scapular region reveals basal cell carcinoma with infiltration of the basal membrane. E) Biopsy of the bowel shows intestinal adenocarcinoma, moderately differentiated, with mitosis and increased cell nuclei. F) Biopsy of the abdominal lymph node capsule shows metastasis of the intestinal adenocarcinoma, with intestinal glands
A B
C D
e F
Figure 2. Ectoscopy findings. There is bilateral bulging in the upper and lower eyelid region, more prominently on the left, with mucoid secretion.
Figure 3. Magnetic resonance imaging of the orbit: The image shows bilateral eyelid thickening, which is more pronounced on the left, and a lesion involving the eyeball, which is hypointense relative to fat on a T1 image and hyperintense on a T2 image, with contrast enhancement (gadolinium).
Figure 4. Incisional eyelid biopsy: Hematoxylin-eosin staining shows a relatively homo-geneous population of small cells with slight nuclear irregularity. Immunohistochemistry is positive for CD5, CD20, and cyclin D1.
(Figure 2). Uncorrected visual acuity was 20/50 in the right eye and 20/25 in the left eye. Anterior biomicroscopy revealed mucoid se-

Case report of a metachronous multiple tumor: Mantle cell lymphoma in the orbital region associated with epithelial malignancies at other sites
56 Arq Bras Oftalmol. 2014;77(1):54-6
doxorubicin, vincristine, and prednisone), 6 cycles of FCR (fludarabi-ne, cyclophosphamide, and rituximab), and radiotherapy The patient is being followed-up by a multidisciplinary team.
DISCUSSIOnMPT affects approximately 1.3%-2.5% patients diagnosed with
malignancy, and patients with ≥3 MPTs account for 0.16%-0.26% of this total(1,7). Although the lesions described in the literature primarily involved the gastrointestinal tract, breast, and skin (non-melanoma), other sites can also be affected. Pandurengan et al.(8) described a case of gastrointestinal stromal tumor associated with gastric lymphoma, while Troyanova et al.(9) described an increased risk of MPT in Bulga-rian patients diagnosed with malignant non-melanoma of the skin, primarily affecting the head and neck, thyroid, lung, larynx, bladder, colon, melanoma, and non-Hodgkin lymphoma. Dasanu et al.(2) repor-ted a case of pancreatic adenocarcinoma associated with mantle cell lymphoma; this was the only case we found in PubMed and Bireme describing MPT involving the specific subtype of mantle cell lym-phoma, similar to the present case. Our first tentative diagnosis was based on the patient’s personal history and was orbital metastasis. In our patient, any of the malignancies could be the origin of metastasis, indicating the importance of biopsy for histological confirmation.
Systemic lymphomas (nodal and extranodal) can spread to the ocular adnexa. When there is ocular involvement secondary to a systemic lymphoma, the uvea is almost exclusively the affected site (choroid, ciliary body, and iris)(5). However, ocular adnexal lymphomas have not been associated with intraocular lymphomas. They are ge-nerally indolent, painless, and well tolerated and mold to the adjacent structures without bone destruction in imaging studies(5). Rasmussen et al.(4) related the most common symptoms of mantle cell lymphoma in the orbital and adnexal region: irritation, pain, and epiphora. They also referred to eyelid masses, conjunctival swelling, and proptosis as the most frequent signs. Our patient complained of bilateral eyelid swelling, low visual acuity, and an orbital mass. Because this was a specific subtype of lymphoma, we believed that the orbital tumor in our patient was a metastasis of non-Hodgkin B-cell small cell lympho-ma of the cervical lymph nodes. A factor in favor of this hypothesis is the rarity of the presence of two primary malignant tumors in the orbit; however, we have to remember that the primary sites for or-bital metastasis are the breasts, lungs, and prostate. Our patient also presented with intestinal adenocarcinoma, which can metastasize to the orbit; however, this type of involvement is very rare. In such cases, imaging findings have been related to osseous changes such as hypo- or hyperostosis primarily located intra- or extraconally and occasionally involving the extraocular muscles. These characteristics were not found in the case presented(10).
Mantle cell lymphoma is a distinct subtype of non-Hodgkin B-cell tumors that primarily affect elderly men, unlike the majority of pe-riocular lymphomas, which are more common in older women(4,6). As observed in our case, approximately one- to two-thirds of patients report a previous diagnosis of systemic lymphoma at diagnosis; for the remaining third, the diagnosis is made when the disease is alrea-dy widespread. This characteristic also differentiates it from other orbital lymphomas(4). Approximately 32%-71% of these tumors are bilateral, and the eyelid, orbit, and conjunctiva are the most involved regions(3-5). The bone marrow is involved in 50%-70% cases at diag-nosis(4). In most cases, there is involvement of more than one site in the orbital region or the ocular adnexa(4). The most frequent signs and symptoms are irritation, ptosis, eyelid edema or mass, proptosis, pain, and diplopia; other less common findings include a mass in
the region of the lacrimal gland, chemosis, conjunctival hyperemia, ocular motility alteration, tearing, and malalignment of the eyeball(3,4). Only 50% patients have a survival rate of >5 years(3,4).
There are some characteristic immunohistochemical markers (CD5+, CD20+, bcl-2+, CD21+ dendritic form, CD43+, CD23-, CD10, CD11c-, and CD25-) and genetic patterns characterized by the trans-location t(11;14)(q13,q32), which causes overexpression of the CCND1 gene and the protein cyclin D1(3-5). However, some authors have described atypical cases that were immunohistochemically negative for CD5(3). Coupland et al. showed p16 expression in 2 patients.6 Histo-logically, this lymphoma is characterized by small cells with irregular and hyperchromatic nuclei and scant cytoplasm(6).
The European Task Force on Lymphoma has defined 3 types of mantle cell lymphoma growth patterns: diffuse (most common), no dular, and marginal zone(3,4). Some studies have shown that the mar ginal zone pattern is related to better prognosis, while others have demonstrated that all patterns have a similar prognosis(3). In fact, the prognosis is usually poor, with poor response to treatment, bone marrow involvement, and short survival duration. The poor prognosis is associated with increased mitotic activity (>20 mitoses/10x field), blastic morphology, peripheral involvement (atypical cells in the pe ripheral blood), and increased p53 expression(3,5). A few years ago, it was considered an untreatable disease with only palliative care options available, but nowadays, several types of treatments are being studied. Recently, some studies showed a response to combined the-rapy with multiple chemotherapy regimens and rituximab (anti-CD20) in patients with an early diagnosis; other researchers have seen good results with bone marrow transplantation(3,4).
In conclusion, mantle cell lymphoma is a rare disease, usually wi-despread, and carries a poor prognosis. Physicians should consider this malignancy as a differential diagnosis for neoplasms of the orbit. Rapid and accurate diagnosis by clinical and immunohistochemical tests is essential before referral of the patient for systemic evaluation and treat-ment. This case report described an extremely rare occurrence, and in our knowledge, it represents the first case described in the scientific literature on metachronous MPT with bilateral non-Hodgkin B-cell mantle cell lymphoma of the orbit in a Brazilian patient.
ReFeRenCeS 1. Santander G, Lombardo K, Rodríguez R. Tumores multiples. Análisis de 25 casos. Salud
Militar. 2006;28(1):73-80. 2. Dasanu CA, Shimanovsky A, Rotundo EK, Posteraro AF, Cooper DL, Atienza JA.
Collision tumors: pancreatic adenocarcinoma and mantle cell lymphoma. JOP. 2013; 14(4):458-62.
3. Looi A, Gascoyne RD, Chhanabhai M, Connors JM, Rootman J, White VA. Mantle cell lymphoma in the ocular adnexal region. Ophthalmology. 2005;112(1):114-9.
4. Rasmussen P, Sjo LD, Prause JU, Ralfkiaer E, Heegaard S. Mantle cell lymphoma in the orbital and adnexal regional. Br J Ophthalmol. 2009;93:1047-51.
5. Jakobiec FA. Ocular adnexal lymphoid tumors: progress in need of clarification. Am J Ophthalmol. 2008;145:941-50.
6. Coupland SE, Hellmich M, Auw-Haedrich C, Lee WR, Stein H. Prognostic value of cell-cy cle markers in ocular adnexal lymphoma: an assessment of 230 cases. Arch Clin Exp Ophthalmol. 2004;242:130-45.
7. Salem A, Abu-Hijlih R, Abdelrahman F, Turfa R, Amarin R, Farah N, et al. Multiple pri-mary malignancies: Analysis of 23 patients with at least three tumors. J Gastrointest Cancer. 2012;43(3):437-43.
8. Pandurengan RK, Dumont AG, Araujo DM, Ludwig JA, Ravi V, Patel S, et al. Survival of patients with multiple primary malignancies: a study of 783 patients with gastroin-testinal stromal tumor. Ann Oncol. 2010;21(10):2107-11.
9. Troyanova P, Danen S, Ivanona T. Nonmelanoma skin cancers and risk of subsequent malignancies: a cancer registry-based study in Bulgaria. Neoplasma. 2002;49(2): 81-5.
10. Borota OC, Kloster R, Lindal S. Carcinoid tumour metastatic to the orbit with infiltra-tion to the extraocular orbital muscle. APMIS. 2005;113(2):135-9.
57Arq Bras Oftalmol. 2014;77(1):57-9
Case Report
InTRODUCTIOnConjunctival melanoma shows considerable clinical variability.
This lesion usually presents as a pigmented or tan elevated lesion that can be located in any area of the conjunctiva. It may arise spon-taneously (de novo), in a pre-existent nevus, or in association with primary acquired melanosis (PAM) with atypia(1). Melanoma can ex-tend from the conjunctiva onto the cornea or can be displaced and limited over the cornea without evidence of conjunctival tumors. The latter lesions comprise 5% of all conjunctival melanomas and are called corneally displaced malignant conjunctival melanomas to describe their supposed conjunctival origin and actual corneal location(2).
The degree of pigmentation in melanomas depends on the amount of melanin in the tumor cells, macrophages, or extracellular matrix(3). The corneally displaced melanoma is a rare disease, and the complete absence of intrinsic pigmentation is even more rare(2).
CASe RePORTThe authors describe the case of a 65-year-old Caucasian female
from Curitiba (Parana, Brazil). In June 2013, she was referred to one of the authors (M.M.) in São Paulo because of unresponsiveness to topical steroid treatment for a nonpigmented lesion located over her left cornea since 1 year. Although the lesion disturbed her blinking reflex, her vision remained unchanged because her left eye had am-blyopia secondary to an untreated congenital cataract. She reported a history of Herpes simplex keratitis of the same eye since 2005, which had recurred several times, with the last episode in December 2012. On examination, the visual acuity of her left eye was count fingers. On examination, a fleshy, white, vascularized nodule with indistinct but well-outlined edges was observed on the temporal quadrant of the cornea (Figure 1A). Corneal opacities were observed in the inferior and nasal quadrants (Figure 1B). The nodule was surrounded by a margin of clear cornea and connected with superficial neovascular
Amelanotic corneally displaced malignant conjunctival melanoma: a case report evaluated with impression cytologyMelanoma amelanótico conjuntival maligno deslocado sobre a córnea com citologia de impressão: relato de caso
JeiSon de nadai barroS1, Márcia MoTono2,3, Felipe d’alMeida coSTa3, Marcelo carvalho da cunha2, MarTha MoTono choJniaK3
Submitted for publication: August 21, 2013 Accepted for publication: October 24, 2013
Study carried out at Clínica de Olhos Dr. Moacir Cunha - São Paulo - SP (Brasil) and A.C. Camargo Cancer Center - São Paulo - SP, Brasil.
1 Laboratório de Citologia de Impressão, Clínica de Olhos Dr. Moacir Cunha - São Paulo (SP) - Brasil. 2 Clínica de Olhos Dr. Moacir Cunha.3 A.C. Camargo Cancer Center - São Paulo (SP) - Brasil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: J.N. Barros, None; M. Motono, None; F.D´A. Costa, None; M.C. Cunha, None; M.M. Chojniak, None.
Correspondence address: Jeison de Nadai Barros. Al. Gabriel Monteiro da Silva, 1.000 - São Paulo (SP) - 01442-000 - Brazil - E-mail: [email protected]
ABSTRACTHere we describe the case of a 65-year-old Caucasian female who presented with an amelanotic malignant conjunctival melanoma and highlight the clinical and pathological features of this rare entity that displayed exclusive corneal invasive growth without evidence of conjunctival tumors other than primary acquired me-lanosis. Impression cytology aided in the initial diagnosis. The patient underwent surgical treatment. Histopathology and immunohistochemistry revealed an invasive amelanotic melanoma limited to the cornea and exhibiting S-100, Melan A, and HMB-45 positivity. The absence of pigmentation delayed early clinical detection and treatment. Awareness of this nonpigmented melanoma is important for early recognition and appropriate management.
Keywords: Melanoma/pathology; Conjunctival neoplasms; Eye neoplasms; Cy-to logical techniques; Diagnostic techniques, Ophthalmological; Humans; Female; Aged; Case report
RESUMOOs autores descrevem o caso de uma mulher branca de 65 anos que apresentava um melanoma amelanótico maligno conjuntival e destacam as características clínicas e patológicas desta entidade rara com crescimento invasivo exclusivo na córnea sem evidência de tumores na conjuntiva além de melanose adquirida primária sem pigmento. A citologia de impressão auxiliou no diagnóstico inicial. A paciente foi submetida a tratamento cirúrgico. A histopatologia e a imuno-histoquímica revelaram um melanoma amelanótico invasivo limitado sobre a córnea exibindo positividade para proteína S-100, Melan A e HMB-45. A ausência de pigmentação retardou sua identificação clínica e seu tratamento precoce. O conhecimento deste melanoma não pigmentado é importante para o reconhecimento precoce e a conduta apropriada.
Descritores: Melanoma/patologia; Neoplasias da túnica conjuntiva; Neoplasias ocu -lares; Técnicas citológicas; Técnicas de diagnóstico oftalmológico; Humanos; Feminino; Idoso; Relato de caso
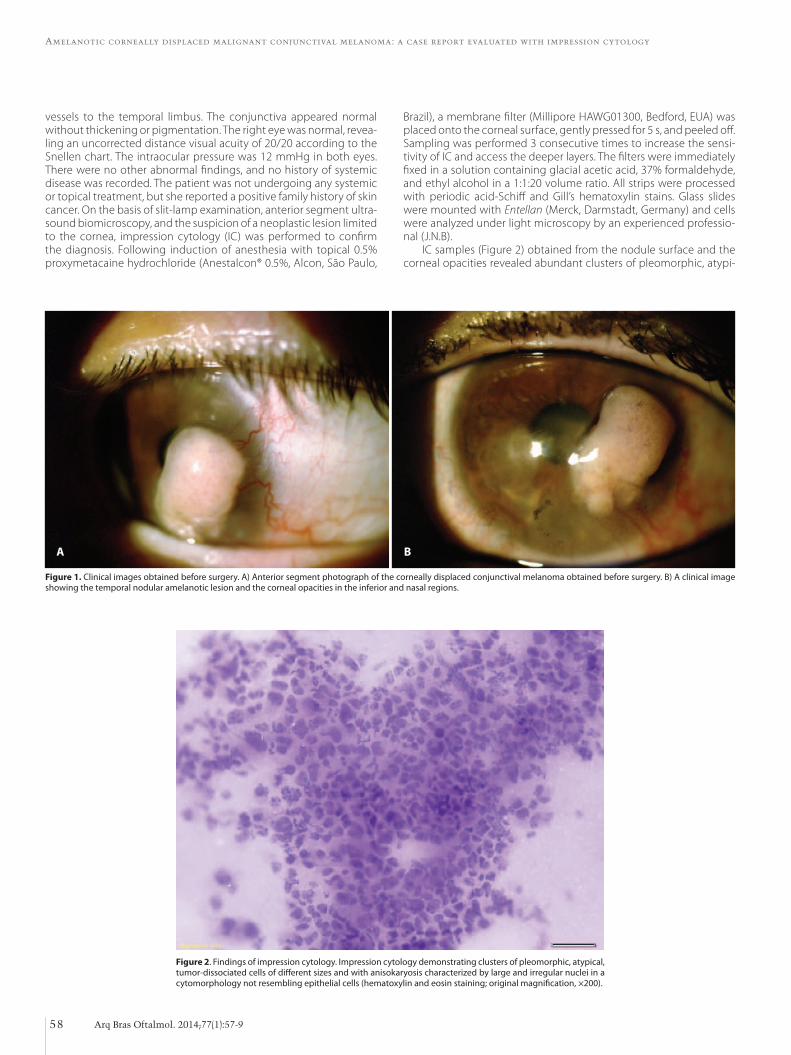
Amelanotic corneally displaced malignant conjunctival melanoma: a case report evaluated with impression cytology
58 Arq Bras Oftalmol. 2014;77(1):57-9
A B
Figure 1. Clinical images obtained before surgery. A) Anterior segment photograph of the corneally displaced conjunctival melanoma obtained before surgery. B) A clinical image showing the temporal nodular amelanotic lesion and the corneal opacities in the inferior and nasal regions.
Figure 2. Findings of impression cytology. Impression cytology demonstrating clusters of pleomorphic, atypical, tumor-dissociated cells of different sizes and with anisokaryosis characterized by large and irregular nuclei in a cytomorphology not resembling epithelial cells (hematoxylin and eosin staining; original magnification, ×200).
vessels to the temporal limbus. The conjunctiva appeared normal without thickening or pigmentation. The right eye was normal, revea-ling an uncorrected distance visual acuity of 20/20 according to the Snellen chart. The intraocular pressure was 12 mmHg in both eyes. There were no other abnormal findings, and no history of systemic disease was recorded. The patient was not undergoing any systemic or topical treatment, but she reported a positive family history of skin cancer. On the basis of slit-lamp examination, anterior segment ultra-sound biomicroscopy, and the suspicion of a neoplastic lesion limited to the cornea, impression cytology (IC) was performed to confirm the diagnosis. Following induction of anesthesia with topical 0.5% proxymetacaine hydrochloride (Anestalcon® 0.5%, Alcon, São Paulo,
Brazil), a membrane filter (Millipore HAWG01300, Bedford, EUA) was placed onto the corneal surface, gently pressed for 5 s, and peeled off. Sampling was performed 3 consecutive times to increase the sensi-tivity of IC and access the deeper layers. The filters were immediately fixed in a solution containing glacial acetic acid, 37% formaldehyde, and ethyl alcohol in a 1:1:20 volume ratio. All strips were processed with periodic acid-Schiff and Gill’s hematoxylin stains. Glass slides were mounted with Entellan (Merck, Darmstadt, Germany) and cells were analyzed under light microscopy by an experienced professio-nal (J.N.B).
IC samples (Figure 2) obtained from the nodule surface and the corneal opacities revealed abundant clusters of pleomorphic, atypi-
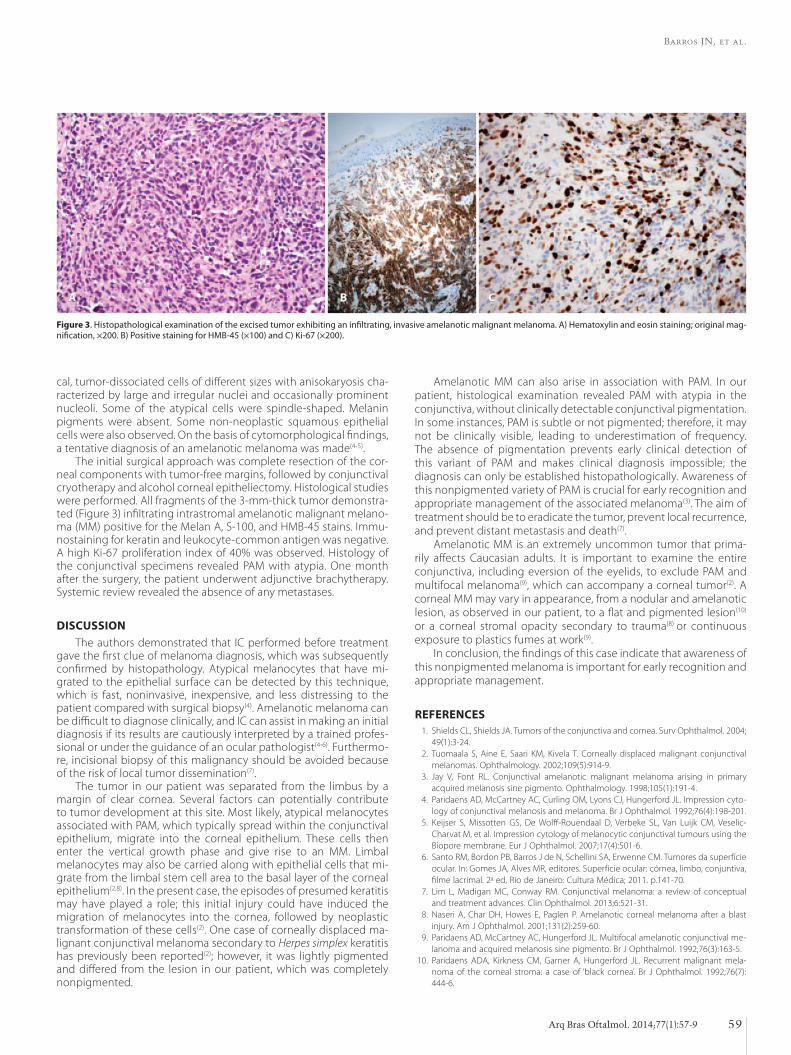
Barros JN, et al.
59Arq Bras Oftalmol. 2014;77(1):57-9
cal, tumor-dissociated cells of different sizes with anisokaryosis cha-racterized by large and irregular nuclei and occasionally prominent nucleoli. Some of the atypical cells were spindle-shaped. Melanin pigments were absent. Some non-neoplastic squamous epithelial cells were also observed. On the basis of cytomorphological findings, a tentative diagnosis of an amelanotic melanoma was made(4-5).
The initial surgical approach was complete resection of the cor-neal components with tumor-free margins, followed by conjunctival cryotherapy and alcohol corneal epitheliectomy. Histological studies were performed. All fragments of the 3-mm-thick tumor demonstra-ted (Figure 3) infiltrating intrastromal amelanotic malignant melano-ma (MM) positive for the Melan A, S-100, and HMB-45 stains. Immu-nostaining for keratin and leukocyte-common antigen was negative. A high Ki-67 proliferation index of 40% was observed. Histology of the conjunctival specimens revealed PAM with atypia. One month after the surgery, the patient underwent adjunctive brachytherapy. Systemic review revealed the absence of any metastases.
DISCUSSIOnThe authors demonstrated that IC performed before treatment
gave the first clue of melanoma diagnosis, which was subsequently confirmed by histopathology. Atypical melanocytes that have mi-grated to the epithelial surface can be detected by this technique, which is fast, noninvasive, inexpensive, and less distressing to the patient compared with surgical biopsy(4). Amelanotic melanoma can be difficult to diagnose clinically, and IC can assist in making an initial diagnosis if its results are cautiously interpreted by a trained profes-sional or under the guidance of an ocular pathologist(4-6). Furthermo-re, incisional biopsy of this malignancy should be avoided because of the risk of local tumor dissemination(7).
The tumor in our patient was separated from the limbus by a margin of clear cornea. Several factors can potentially contribute to tumor development at this site. Most likely, atypical melanocytes as sociated with PAM, which typically spread within the conjunctival epithelium, migrate into the corneal epithelium. These cells then enter the vertical growth phase and give rise to an MM. Limbal melanocytes may also be carried along with epithelial cells that mi-grate from the limbal stem cell area to the basal layer of the corneal epithelium(2,8). In the present case, the episodes of presumed keratitis may have played a role; this initial injury could have induced the migration of melanocytes into the cornea, followed by neoplastic transformation of these cells(2). One case of corneally displaced ma-lignant conjunctival melanoma secondary to Herpes simplex keratitis has previously been reported(2); however, it was lightly pigmented and differed from the lesion in our patient, which was completely nonpigmented.
Amelanotic MM can also arise in association with PAM. In our pa tient, histological examination revealed PAM with atypia in the conjunctiva, without clinically detectable conjunctival pigmentation. In some instances, PAM is subtle or not pigmented; therefore, it may not be clinically visible, leading to underestimation of frequen cy. The absence of pigmentation prevents early clinical detection of this variant of PAM and makes clinical diagnosis impossible; the diag nosis can only be established histopathologically. Awareness of this nonpigmented variety of PAM is crucial for early recognition and appropriate management of the associated melanoma(3). The aim of treatment should be to eradicate the tumor, prevent local recurrence, and prevent distant metastasis and death(7).
Amelanotic MM is an extremely uncommon tumor that prima-rily affects Caucasian adults. It is important to examine the entire conjunctiva, including eversion of the eyelids, to exclude PAM and multifocal melanoma(9), which can accompany a corneal tumor(2). A corneal MM may vary in appearance, from a nodular and amelanotic lesion, as observed in our patient, to a flat and pigmented lesion(10) or a corneal stromal opacity secondary to trauma(8) or continuous exposure to plastics fumes at work(9).
In conclusion, the findings of this case indicate that awareness of this nonpigmented melanoma is important for early recognition and appropriate management.
ReFeRenCeS 1. Shields CL, Shields JA. Tumors of the conjunctiva and cornea. Surv Ophthalmol. 2004;
49(1):3-24. 2. Tuomaala S, Aine E, Saari KM, Kivela T. Corneally displaced malignant conjunctival
melanomas. Ophthalmology. 2002;109(5):914-9. 3. Jay V, Font RL. Conjunctival amelanotic malignant melanoma arising in primary
acqui red melanosis sine pigmento. Ophthalmology. 1998;105(1):191-4. 4. Paridaens AD, McCartney AC, Curling OM, Lyons CJ, Hungerford JL. Impression cyto-
logy of conjunctival melanosis and melanoma. Br J Ophthalmol. 1992;76(4):198-201. 5. Keijser S, Missotten GS, De Wolff-Rouendaal D, Verbeke SL, Van Luijk CM, Veselic-
Char vat M, et al. Impression cytology of melanocytic conjunctival tumours using the Biopore membrane. Eur J Ophthalmol. 2007;17(4):501-6.
6. Santo RM, Bordon PB, Barros J de N, Schellini SA, Erwenne CM. Tumores da superfície ocular. In: Gomes JA, Alves MR, editores. Superfície ocular: córnea, limbo, conjuntiva, filme lacrimal. 2a ed, Rio de Janeiro: Cultura Médica; 2011. p.141-70.
7. Lim L, Madigan MC, Conway RM. Conjunctival melanoma: a review of conceptual and treatment advances. Clin Ophthalmol. 2013;6:521-31.
8. Naseri A, Char DH, Howes E, Paglen P. Amelanotic corneal melanoma after a blast injury. Am J Ophthalmol. 2001;131(2):259-60.
9. Paridaens AD, McCartney AC, Hungerford JL. Multifocal amelanotic conjunctival me-lanoma and acquired melanosis sine pigmento. Br J Ophthalmol. 1992;76(3):163-5.
10. Paridaens ADA, Kirkness CM, Garner A, Hungerford JL. Recurrent malignant mela-noma of the corneal stroma: a case of ‘black cornea’. Br J Ophthalmol. 1992;76(7): 444-6.
A B C
Figure 3. Histopathological examination of the excised tumor exhibiting an infiltrating, invasive amelanotic malignant melanoma. A) Hematoxylin and eosin staining; original mag-nification, ×200. B) Positive staining for HMB-45 (×100) and C) Ki-67 (×200).

60 Arq Bras Oftalmol. 2014;77(1):60-5
Review Article
InTRODUCTIOnThe cornea is the transparent, anterior part of the eye that refracts
light onto the lens and is essential to vision. The curvature and thickness of the cornea play an important role in focusing the light to the lens; therefore, they are largely responsible for its optical powers(1).
In humans and many other mammals, the cornea consists of five layers: the epithelium, Bowman’s membrane, the stroma, Descemet’s membrane, and the endothelium(2). Of these, the middle layer, the stroma, accounts for 90% of the corneal thickness in humans and is the major layer contributing to the mechanical strength and stiffness of the cornea(3).
The stroma is a composite material comprising matrix embedded with a complex network of collagen fibers. The matrix is a viscoelastic and nearly incompressible material(2). The collagen fibrils are bundled together to form fibers(4), which are stacked in parallel layers called lamellae(5). In the human cornea, the stroma consists of approxima-tely 300 lamellae at the center and approximately 500 lamellae at the limbus(6). The fibers reinforce the tissue and give it mechanical strength along their orientation. The arrangement of collagen fibrils is important to determine the mechanical strength of the cornea. X-ray scatter intensity distribution data has indicated two preferred directions of collagen orientation at the center of the cornea: along the nasal-temporal and superior-inferior meridians(7-8). Closer to the limbus, the fibers tend to run in a circumferential direction(8). Appro-
ximately two-thirds of the fibrils are preferentially oriented in the cor nea, with the remaining third exhibiting a more or less random orientation(9-10). This arrangement of collagen fibrils results in aniso-tropy of the corneal material.
Biomechanical experiments on corneal tissue have been perfor-med in both in vitro and in vivo studies. Recently, the use of com-putational models based on the finite element method has proven to be an effective way for studying corneal mechanics and related diseases(2,6,11-12). These models have been successful in predicting the pre- and postoperative response to eye surgery for myopia, hypero-pia, as tigma tism, and keratoconus(5,13-16).
The finite element method (FEM) is a numerical technique to obtain approximate solutions for partial differential equations invol-ving physical, thermal, chemical, and other phenomena. Generally, these differential equations are impossible to solve analytically because of the complex geometries and properties of the materials. The approach for solving the equations is to simplify the form of the equation using simple interpolation functions and integrate the en-tire solution to obtain the final results. This method is very useful for solving problems involving complex material properties and irregular geometries.
To conduct a finite element analysis (FEA), a given body or system is divided into small units called elements, which are interconnected at points called nodes. The nodes and elements create a network
Finite element modelling of cornea mechanics: a reviewModelagem de elementos finitos da mecânica da córnea: uma revisão
TaliSa MohaMMad neJad1, craiG FoSTer1, dipiKa GonGal2
Submitted for publication: October 24, 2013 Accepted for publication: October 25, 2013
Study carried out at University of Illinois at Chicago.1 Department of Civil and Materials Engineering, University of Illinois at Chicago, Chicago, IL 60607 USA.2 Foster Wheeler North America, Hampton, NJ 08827.
Funding: This work was partially supported by NIH grant 1R21EY020946- 01 and University of Illinois at Chicago Chancellor’s Discovery Fund for Multidisciplinary Pilot Research.
Disclosure of potential conflicts of interest: T.M. Nejad, grant from National Institutes of Health; C. Foster, grant from National Institutes of Health; D. Gongal, None
Correspondence address: Craig Foster. Department of Civil and Materials Engineering. University of Illinois at Chicago. MC 246, 3085 Engineering Research Facility - 842 W. Taylor St. - Chicago, IL 60607 - USA - E-mail: [email protected]
ABSTRACTThe cornea is a transparent tissue in front of the eye that refracts light and faci-litates vision. A slight change in the geometry of the cornea remarkably affects the optical power. Because of this sensitivity, biomechanical study of the cornea can reveal much about its performance and function. In vivo and in vitro studies have been conducted to investigate the mechanics of the cornea and determine its characteristics. Numerical techniques such as the finite element method (FEM) have been extensively implemented as effective and noninvasive methods for analyzing corneal mechanics and possible disorders. This article reviews the use of FEM for assessing the mechanical behavior of the cornea. Different applications of FEM in corneal disease studies, surgical predictions, impact simulations, and clinical applications have been reviewed. Some suggestions for the future of this type of modeling in the area of corneal mechanics are also discussed.
Keywords: Finite element analysis; Cornea/physiology; Cornea/ultrastructure; Cornea/surgery; Biomechanics/methods; Models, biological
RESUMOA córnea é um tecido transparente na parte frontal do olho, que refrata a luz e torna a visão possível. Uma ligeira alteração na geometria da córnea notavelmente afeta a sua potência óptica. Devido a essa sensibilidade, o estudo biomecânico da córnea pode revelar muito sobre o seu desempenho e funcionalidade. Estudos in vivo e in vitro foram realizados para investigar a mecânica da córnea e para determinar suas características. Técnicas numéricas como o método dos elementos finitos (FEM) fo-ram amplamente implementadas como métodos eficazes e não invasivos de análise mecânica da córnea e seus possíveis transtornos. Este artigo analisa o uso de FEM para avaliar o comportamento mecânico da córnea. Diferentes aplicações da FEM no estudo de doenças da córnea, previsões cirúrgicas, simulações de impacto e aplicações clínicas foram revistos. São discutidas algumas sugestões para o futuro deste tipo de modelagem na área de mecânica de córnea.
Descritores: Análise de elementos finitos; Córnea/fisiologia; Córnea/ultraestrutura; Córnea/cirurgia; Biomecânica/métodos; Modelos biológicos

Nejad TM, et al.
61Arq Bras Oftalmol. 2014;77(1):60-5
referred to as a mesh. Each element is assigned specific material and structural properties and the body is analyzed under certain bounda-ry conditions. These boundary conditions can include forces, displa-cements, and temperatures. The analyzed solution of each element is assembled together to give the global response of the system.
The accuracy of this method, in general, depends upon the num-ber of elements used for analysis. A larger number leads to a more pre-cise solution. However, over-refinement of the mesh can lead to longer computational time and memory use in the computer. The element shape and type also play an important role in the accuracy of analysis.
The focus of this article will be the use of FEA for mechanical analysis of the cornea. We will review how this method has been applied to examine the cornea under different loads such as intraocular pres-sure (IOP), impact from a foreign object, or incisions. The method can also be used to examine how the shape is affected by changes in material properties, such as those occurring during keratoconus. It is worth mentioning briefly, though, that the method can be applied to a wide variety of problems. It has been used to study thermal, electri-cal, and other physical responses as well as ionic transport. Shafahi and Vafai(17) used a thermal finite element model of the eye to study its response to thermal disturbances. Papaioannou and Samaras(18) used a rabbit eye model to simulate the temperature distribution and velocity field generated under exposure to millimeter wave radiation. Jo and Aksan(19) performed a simulation of conductive keratoplasty, a thermal treatment for hyperopia and presbyopia, to predict thermal damage to the corneal tissue. Mandel et al.(20) used a three-dimen-sional cornea model exposed to an electrical field to evaluate the electrical properties of the endothelial layer. Guimera et al.(21) also developed a noninvasive FEM to predict the electrical properties of the endothelium and study variations in epithelial permeability. Li and Pinsky(22) created a multiphasic mathematical model describing the transport of ionic solution and ionic species in human corneal tissue. We refer the reader to those papers and references therein for further details on these topics of study.
Section 2 discusses the modeling assumptions made in many finite element models of the cornea. The purpose of this section is to give modelers an understanding of the different assumptions that have been used, so that they may choose an appropriate model for their application of interest. Section 3 discusses different applications in corneal mechanics. Finite elements have been used to model the response to corneal surgery, disease, and treatments such as collagen cross-linking (CXL); trauma; and basic research applications. Section 4 summarizes the work and gives some suggestions on the future of such modeling in the practice of ophthalmology and eye research.
modeling basics
The structural model of the cornea can be approached by crea-ting a continuum model or shell model. Continuum models expli-citly model the geometry of the cornea in three dimensions, although two-di mensional (2D) approximations are sometimes used. Shell-based models use the theory of thin shell behavior to decrease the geo-metrical complexity. The modeled geometry is a surface, with the thickness of the shell as a defined parameter. Tensile and bending loads on the shell create deformations in the shell in accordance with shell theory. While this approach decreases geometrical complexity and increases efficiency of the formulation, it is difficult to extend to complex constitutive models. Anderson et al.(23) proposed a corneal model by using shell analysis to develop a nonlinear finite element model to study the mechanical behavior of the cornea. Howland et al.(24), Pinsky and Datye(25), Li and Tighe(26), and Elsheikh and Wang(27)
also based their models on this method.
Geometry
The structure of the human cornea has a nonuniform curvature with variable thickness throughout(27). It is thinner at the center and thickens towards the edges. Dubbelman et al.(28) recorded the corneal
geometry for the internal and external surfaces of the human cornea using Scheimpflug photography. Roy et al.(14) used magnetic resonan-ce imaging to determine the geometric profile of the eye.
Some early models of the cornea, e.g.(29), use a 2D axisymmetric approximation of the cornea. This models the geometry as a surface of revolution and is efficient compared with three-dimensional models (3D). However, it cannot capture the subtle variations in the geometry of the cornea from a surface of revolution, prevalent anisotropies in the material, or any loads that occur off-center, such as an impact or incision. Figure 1 illustrates common shell elements and 3D elements used for FEA of the cornea.
Pandolfi and Holzapfel(2) used the corneal geometry data publi-shed by Dubbelman et al.(28) to create biconic interior and exterior surfaces for a 3D corneal model. Pandolfi and Manganiello(10) used an ellipsoidal shape to define the anterior and posterior corneal surfa-ces. Nguyen et al.(30) and Nguyen and Boyce(31) also approximated the corneal surface to be ellipsoidal according to digital image correla-tion (DIC) measurements of the corneal surface profile. Buzard(32) and Howland et al.(24) used axisymmetry to create their corneal models.
Salimi et al.(33) meshed the corneal model into triangular shell elements. For 3D models, hexahedral elements are more commonly used(2,6), although tetrahedral elements may also be used. Linear te-trahedrals and standard trilinear hexahedrals are known to perform poorly for nearly incompressible materials such as soft tissues. Trili-near hexahedral elements can be modified using techniques such as selective reduced integration(34); alternatively, higher order elements may be employed. Figure 2 shows an example of an FE mesh of the cornea.
Boundary conditions
The viscous fluid filled inside the anterior chamber of the eye exerts pressure known as IOP on the cornea. Under physiological conditions, the IOP inflates the cornea and gives it shape. A model developed for the cornea using the entire eyeball allows appropriate realistic displacement at the limbus. Uchio et al.(35) and Amini and Barocas(36) modeled the entire eye globe for the analysis. However, the whole eye model may not be efficient because it is highly time consuming and not economical for development and analysis.
A
C
B
D
Figure 1. Common shell and solid elements used for finite element analysis (FEA) of the cornea. A) Triangle and B) quadrilateral are common shell elements. Each shell element node has 5 degrees of freedom (DOF): 3 translational and 2 rotations (approximately 2 orthogonal axes on the shell surface). C) Tetrahedral and D) hexahedral are common 3D elements. Each element node has 3 translational DOF.

Finite element modelling of cornea mechanics: a review
62 Arq Bras Oftalmol. 2014;77(1):60-5
Alastrue et al.(5) analyzed the corneal model with the limbus cons-trained against displacement. Anderson et al.(23) compared the de-formation pattern of the entire eye model to the rigid cornea-limbus boundary. They proposed an approximate boundary condition, with roller support at the edges inclined at 40° with respect to the horizontal axis, to represent the cornea-limbus behavior. The results obtained from their boundary assumption were similar to the results obtained for the whole eye. Other studies(11,37,38) adopted similar boundary conditions for their corneal models. Roy et al.(14) created the whole eye model and compared the displacement results with those for the corneal model with fixed sclera to show that the cor-neoscleral limbus plays an important part in predicting the response to refractive surgery. Pandolfi and Holzap fel(2) proposed a corneal model allowing rotation at the limbus and restricting displacement at the edges. Rotation at the limbus plays a role in changing the cur-vature of the cornea. Figure 3 illustrates these boundary conditions.
Figure 4 illustrates displacement results of FE simulation of a cornea subjected to IOP, with rotation at the limbus.
Material models
For creating a material model, the corneal material is often appro-ximated as the stroma, which is the major contributor to mechanical strength(2,6,31). The stromal layer may be modeled as a nonlinear, aniso-tropic, viscoelastic material that undergoes large deformation. Finite deformation theory is incorporated in the corneal model, which suc-cessfully captures its true nonlinear response under deformation(2,31).
Earlier finite element models were simple linear elastic models. One of the earlier models developed by Vito et al.(39) considered the stroma as a linear, elastic, homogeneous, and isotropic material. Si milarly, Bryant et al.(40), Hanna et al.(41), Gefen et al.(12), and Velinsky and Bryant(42) also assumed that the cornea would undergo a small deformation and used linear elasticity for their analysis. Pinsky and Datye(25) developed a linear material corneal model based on the anisotropic constitutive model using the predominant fiber directions in the cornea.
The first geometrically nonlinear models represented the stro-ma as a nearly incompressible, isotropic, hyperelastic material. The Neo-Hookean model is widely used for modeling tissues(2,6). Other hy perelastic models have also been used. Niroomandi et al.(43) used a simpler Saint Venant-Kirchhoff hyperelastic model. Bryant and McDonnell(44) created a 2D axisymmetric model to compare various isotropic and a couple of transversely isotropic constitutive models of the cornea. Of the models they compared, an exponential nonlinear model best fit the inflation experiments.
Many researchers used a base isotropic model for the matrix of the stroma and additional terms for the effects of the fibers, as discussed below. Alastrue et al.(5), Hanna et al.(41), and Pandolfi et al.(13) considered the matrix as a Mooney-Rivlin model. Nguyen et al.(30) and Pinsky et al.(6) used a Neo-Hookean model as their matrix model.
Anisotropic nonlinear hyperelastic models with embedded colla-gen fibers have been frequently used in recent corneal models(2,5,6,31). Alastrue et al.(5) used a discrete fiber model with embedded collagen fibers in two preferred orientations, the nasal-temporal and supe-rior-inferior directions. Most other recent models do not simulate each fiber explicitly, which can be computationally expensive; however, they include a smeared effect of oriented fibers. Cristobal et al.(45) and Pandolfi and Manganiello(10) developed their models with two preferred directions at the center and circumferential at the limbus region. Pan-dolfi and Holzapfel(2) used a distributed model with two preferred orien tations. Pinsky et al.(6) and Nguyen et al.(30) developed a continuous distributed fiber model with preferred orientation.
Nguyen et al.(30) created an anisotropic corneal model, taking into consideration the viscoelastic properties. Yoo et al.(46) also used a vis -coelastic ocular tissue model for their study.
Parameter measurement and optimization
Corneal tissue material properties are determined by various laboratory tests of corneal specimens. The material parameters used for the cornea model are based on these studies. Wollensak et al.(47), Hoeltzel et al.(29), and Zeng et al.(48) performed uniaxial tension tests on corneal tissue to record stress-strain relation. Kohlhaas et al.(49) and Wollensak et al.(47) extended these tests to study the effects of CXL on the mechanical response of the cornea. Bryant et al.(44), Elsheikh et al.(50), and Anderson et al.(23) conducted inflation tests on the entire cornea to determine the apical displacement at different pressure values. Petsche et al.(51) examined the depth-dependent material properties of the stroma. However, further experimental work to completely determine the mechanical behavior of the cornea, parti-cularly in vivo, is required.
Inverse simulation is a mathematical approach to determine unknown model parameters to match observed or assumed physical responses. In inverse FEM, an optimization algorithm is coupled with
Figure 2. An example of a finite element (FE) mesh of the cornea using hexahedral elements.
Figure 4. An example of vertical displacement mapping of a mouse cornea subjected to intraocular pressure (IOP) obtained from finite element (FE) simulations is shown in the cross-section. The wireframe on the bottom is the undeformed mesh, and vertical displacement colored by magnitude is shown on top. The corneal displacement, but not rotation, is restricted along the limbus.
Figure 3. Schematic of boundary conditions at the limbus used by researchers. A) The cornea is constrained against displacement and rotation, as proposed in(5). B) The cornea is fixed against displacement, but may rotate at the edges, as in(2). C) Springs normal to the cross-section. Researchers in(13) investigated boundary conditions (a), (b), and (c). D) The cornea is allowed to expand along a given surface, as in(11, 23, 37, 38). Forty degrees from horizontal is taken as a typical angle.
A B C D

Nejad TM, et al.
63Arq Bras Oftalmol. 2014;77(1):60-5
an FEM to find a set of optimal parameters for a given model to be used in the FE simulation. Such methods are important for determi-ning the physical properties of actual corneas.
Nguyen and Boyce(31) presented an inverse FEM to estimate bovi-ne corneal material properties using an in vitro inflation experiment and investigate the influence of variations in these properties on the bovine inflation response. They determined a set of anisotropic material properties, minimizing the error between simulation results and experimental measurements of the surface displacement field.
Summary of finite element modeling choices
Different choices in finite element models of the cornea can change the results. 2D or shell models are efficient, but they may not be able to accurately capture the complex material behavior of some applications. While modeling the entire eye may avoid approximate boundary conditions at the limbus, the computational time increa-ses significantly. However, modeling the changes in IOP during an impact may be difficult without a full model of the eye.
Material models are also increasingly accurate and, at the same time, computationally more expensive. While linear models are very efficient, they may be inaccurate over large changes in deformation. Isotropic models may not accurately capture the behavior of the complex material in the stroma, but they may be adequate for pro-blems that only require a rough idea of the displacements. The depth of knowledge of the properties of corneal tissue is improving. In applications with rapid load, the viscoelastic and dynamic properties of the cornea may be important. For other analyses, such as those of the long-term results of surgery, a quasistatic model is acceptable. It is important to select a model that can simulate an application with the necessary accuracy. However, a model with too much detail may computationally become very expensive.
APPLICATIOnSFEA is a useful tool for studying corneal mechanical behavior and
the mechanisms underlying its functions. FEA has been widely used for modeling surgical effects on the cornea and for studying corneal diseases and eye trauma. In this section, different applications of FEA in simulation of corneal surgery, disorder, and impact, among others, are discussed.
surgery
The curvature of the internal and external surfaces of the cornea significantly affect its refractive power. Refractive eye surgery can im-prove the visual acuity in patients with common refractive maladies such as astigmatism, hyperopia, and myopia. In several surgical te-chniques, the dioptric power of the cornea is improved by removing thin layers of biological tissues and adjusting the curvature of the cornea using excimer lasers(13). Laser-assisted in-situ keratomileusis (LASIK), photorefractive keratectomy (PRK), and intrastromal photo-refractive keratectomy (ISPRK) are the 3 main types of refractive sur-geries. Refractive surgeries on the periphery of the cornea, such as conductive keratoplasty (CK) and intracorneal rings (ICR), have recen-tly attracted more interest. These surgeries are primarily performed on hyperopic eyes that require steepening rather than flattening of the corneal surface(38).
FEA has potential usefulness as a simulation tool for refractive surgery planning using accurate in vivo corneal material properties and geometry data(14). FEA has been extensively used to model de-formation of the cornea for corneal surgery simulation and predict mechanical and refractive effects of surgery(24).
Pandolfi et al.(13) implemented an FEM in astigmatic and myopic corneas to evaluate the mechanical and refractive outcomes of laser refractive surgery. They computed the change in the curvature and thickness of the human cornea exposed to laser ablation and evalua-ted the corrected dioptric power in individual patients.
Roy et al.(14) proposed an FE model of the whole eye to give insight into refractive surgery planning. They later presented an inverse FEM to determine the undeformed state of the cornea(16). They also deve-loped a 3D, patient-specific, corneoscleral FE model to estimate the surgical impact on corneal shape variations and changes in corneal elastic properties.
Niroomandi et al.(43) presented a novel numerical technique for actual surgery simulation using an extended FEM (X-FEM). The X-FEM enhances standard FE by defining additional degrees of freedom, in this case, for fracture opening (those interested in further theory of the X-FEM can refer to the work of Belytschko et al.(52), among others). In their model, fracture opening induced by the incision pla ced during refractive surgery was reproduced using the X-FEM method. Their presented FEM was able to simulate the complex constitutive model of the cornea and reproduce the discontinuities of the scalpel incision for actual surgery simulations.
Nomograms in ophthalmology are sets of tables of corrected values or graphics used to plan the surgical procedure, particularly in-cisional surgeries for astigmatism and similar diseases(45). Nomograms can manage the incision effect by revising the cut parameters such as depth, length, and optical zone in incisional surgery. Cristóbal et al.(45) proposed an FE model of a limbal incision to predict patient-specific optical power that can be induced during surgery. The nomogram outcomes were compared to simulation results, and, in some cases, the nomograms were revised accordingly.
CK is a subablative thermal treatment wherein thin electrodes are inserted into the stroma to apply radiofrequency (RF) heating. The heat causes the peripheral corneal tissue to shrink. Jo et al.(19)
developed a 3D FE model, including the cornea, aqueous humor, and RF electrodes, to investigate the resultant thermal damage during RF heating in the CK procedure. Fraldi et al.(38) also presented a viscoe-lastic FEA to study the mechanical response of the hyperopic cornea to CK and assess the postsurgical stability of the applied refractive correction. Hameed et al.(53) created a 3D FE model to simulate the ISPRK technique for correcting myopic corneas and predicting treat-ment outcomes. The simulation outcomes were compared with the results from an earlier 2D FE model developed by Bryant et al.(40) for the same purpose. The model outputs were more strongly correlated with the clinical data when the 3D model was used than when the 2-D model was used.
corneal diseases
Finite element analysis has been widely used to study biomecha-nical interactions in corneal maladies (e.g. keratoconus) and better understand the etiology and treatment of the diseases. FEM can be used to investigate the effects of variations in corneal material pro-perties on vision power in patients with corneal diseases.
Keratoconus is a degenerative corneal disease characterized by irregular thinning and bulging of the corneal structure and progressi-ve topographic irregularities in the cornea. This shape distortion leads to an optical aberration that can be corrected with the use of hard contact lenses or glasses in mild cases or corneal transplantation in more severe cases(12). CXL is a new method for treating keratoconus. In this technique, the epithelium is usually removed from the central zone of the cornea, and riboflavin is absorbed into the stroma(16). Under ultraviolet (UV) radiation, the riboflavin creates additional cross-linking in the collagen fibrils, stiffening the cornea.
Gefen et al.(12) presented a 3D linear anisotropic FE model of nor-mal and keratoconic corneas to investigate the mechanical behavior and optical performance. The results of analysis revealed that IOP had a considerable influence on the optical power of the keratoco-nic cornea, while having little effect on the refractive power of the normal cornea. Roy et al.(16) presented a 3D patient-specific FE model of the whole eye to study keratoconus progression. The model was able to demonstrate a patient-specific procedure for investigating

Finite element modelling of cornea mechanics: a review
64 Arq Bras Oftalmol. 2014;77(1):60-5
the locally decreased corneal elastic properties during keratoconus development.
Carvalho et al.(11) presented an FEM of a keratoconic cornea to predict the biomechanical behavior and evolution of the cornea in keratoconus. Using shell elements, they investigated how variations in IOP and material properties of the cornea (i.e., decrease in rigidity of the cornea) can lead to a localized increase in corneal curvature. Foster et al.(54) examined the stiffening effect of CXL in corneal tissue, fitting the material parameters to experiments on corneal strips.
impact and trauma
Ocular trauma can cause long-term vision disorders and can be expensive to treat(55). FEM is a useful tool for simulating ocular trau-ma. It may offer possible solutions for decreasing eye impact injuries and designing protective tools against globe trauma. The impact of different projectiles on the eye has been simulated using FEA to investigate the injury potential.
Stitzel et al.(55) offered a nonlinear FEM of the human eye to pre dict eye rupture injuries caused by high-speed blunt impact. The numerical model was verified with experiments to predict the injury due to different types of impacting projectiles and loading conditions.
Weaver et al.(56) implemented a numerical model of eye impact that considered a variety of blunt projectiles and loading conditions and was based on many experimental impact tests. They investigated the effects of different projectile mass, size, material properties, and velocity on the response of the eye to impact. The study results gave insights for predicting eye rupture in various loading conditions and designing eye safety equipment.
Gray et al.(57) studied the impact of paintballs on the cornea, with the aim of designing safer paintballs. To this end, they implemented a numerical model of the human eye, orbit, and paintball into the CTH computer code (a 3D, finite-volume, and large deformation nu-merical hydrocode developed by Sandia National Laboratory) to study the physical mechanisms causing impact eye injuries. By varying material properties, they concluded that paintballs with less mass can be safer for the eye.
Uchio et al.(35) also presented a 3D FEA supercomputer simu-lation of traumatic impacts on the eyeball. They investigated the threshold of impact eye injuries caused by bodies of different sizes and velocities.
other applications
FEM can be used as a potential noninvasive tool in clinical appli-cations for investigating the biomechanical behavior of the cornea and obtaining characteristic measurements of the tissue. FEM may be a critical method for assessing corneal mechanical and electrical properties and for obtaining IOP measurements.
Applanation tonometry is among the most widely used contact tonometry techniques for IOP measurement. FEM has been used to examine applanation tonometry for measuring IOP(33). Ghaboussi et al.(58) developed a computationally efficient numerical method to accurately measure IOP in the cornea using a modified applanation tonometer. They used the combination of a neural network and ge-netic algorithm to fit clinical applanation tonometry outcomes (force and displacement history data) to the outcomes achieved from the FE model.
As the heart beats, IOP behind the cornea changes; the vibration characteristics of the eye also vary with IOP. Salimi et al.(33) developed a coupled fluid-structure FEM of the eye and investigated the dynamic response of the eye to changing IOPs. They validated the vibrational characteristics from the simulation model with experimental modal analysis (EMA) of a water-filled spherical shell.
Rhee et al.(59) developed a nonlinear, anisotropic FE model of the mouse cornea to study the formation of spiral patterns on the epi-
thelium. They compared the obtained numerical curves of maximum shear strain with actual spiral patterns observed on X-ray images of mouse cornea. The presented work helped in providing insight into the possible development of the cornea.
conclusionsFEA is a powerful numerical technique for finding approximate
solutions to partial differential equations in complex structures. FEA may be used to simulate a wide range of biological structures and body organs. In this work, the different applications of FEA in studying mechanical behavior of the cornea were reviewed. This review inclu-ded information about a wide variety of applications, ranging from surgery to disease and impact simulation.
On the basis of the articles reviewed, FEA has been used to deve-lop a better understanding of the mechanics of the cornea in a variety of settings. It can be a noninvasive, predictive method for assessing corneal function and properties and studying related diseases. The FE models can be used in clinical applications to investigate corneal malfunctions and present possible treatments. FEA can predict the pre- and postoperative responses of the cornea to refractive surge-ries and may be used as a patient-specific simulation tool in clinical applications for surgical planning.
In the future, FE models may become important tools for plan-ning treatments. Initially, the models will be used to improve proce-dural parameters such as incision locations and depths. However, it will soon be possible to provide patient-specific corneal models that can be used to plan individual surgeries and predict outcomes, such as optimal treatment times and concentrations for CXL.
Obtaining the parameters for the stiffness of individual corneas, par ticularly in vivo, remains a challenge. A combination of investi-gations of excised corneas and simple tests of in vivo corneas will provide reasonable data to approximate patient-specific corneal properties. Ongoing investigations on the complex mechanical properties of the cornea will continue to create more realistic and accurate models for all these applications.
ACKnOWLeDGeMenTSThis work was partially supported by an NIH grant 1R21EY020946-01
and the University of Illinois at Chicago Chancellor’s Discovery Fund for Multidisciplinary Pilot Research. We gratefully acknowledge this support.
ReFeRenCeS 1. Albanese A, Urso R, Bianciardi L, Rigato M, Battisti E. Keratoconus, cross-link-induction,
comparison between fitting exponential function and a fitting equation obtained by a mathematical model. Biomed Pharmacotherapy. 2009;63(9):693-6.
2. Pandolfi A, Holzapfel GA. Three-dimensional modeling and computational analysis of the human cornea considering distributed collagen fibril orientations. J Biomech Eng. 2008;130(6):061006.
3. Maurice, DM. The Cornea and Sclera. The Eye, 2nd ed., H. Davison, ed., Academic, New York. 1969;489-600.
4. Graham JS, Vomund AN, Philips CL, Grandbois M. Structural change in human type I collagen fibrils investigated by force spectroscopy. Exp Cell Res. 2004;299:335-42.
5. Alastrué V, Calvo B, Peña EM, Doblaré M. Biomechanical modeling of refractive cor-neal surgery. J Biomech Eng. 2006;128:150-60.
6. Pinsky PM, Van der Heide D, Chernyak D. Computational modeling of mechanical anisotropy in the cornea and sclera. J Cataract Refract Surg. 2005;31(1):136-45.
7. Meek KM, Blamires T, Elliott GF, Gyi, TJ, Nave C. The organisation of collagen fibrils in the human corneal stroma: A synchrotron X-ray diffraction study. Curr Eye Res. 1987; 6(7):841-6.
8. Meek KM, Newton RH. Organization of collagen fibrils in the corneal stroma in rela-tion to mechanical properties and surgical practice. J Refract Surg. 1999;15(6):695-9.
9. Daxer A, Fratzl P. Collagen fibril orientation in the human corneal stroma and its im -plication in keratoconus. Invest Ophthalmol Visual Sci. 1997;38(1):121-9.
10. Pandolfi A, Manganiell F. A model for the human cornea: constitutive formulation and numerical analysis. Biomech Model Mechanobiol. 2006;5(4):237-46.

Nejad TM, et al.
65Arq Bras Oftalmol. 2014;77(1):60-5
11. Caravalho LA, Prado M, Cunha RH, Costa Neto A, Paranhos A, Schor P, et al. Keratoco-nus prediction using a finite element model of the cornea with local biomechanical properties. Arq Bras Oftalmol. 2009;72(2):139-45.
12. Gefen A, Shalom R, Elad D, Mandel Y. Biomechanical analysis of the keratoconic cornea. J Mech Behav Biomed Mater. 2009;2(3):224-36.
13. Pandolfi A, Fotia G, Manganiello F. Finite element simulations of laser refractive cor-neal Surgery. Eng Comput. 2009;25:15-24.
14. Roy AS, Dupps WJ Jr. Effects of altered corneal stiffness on native and postoperative LASIK corneal biomechanical behavior: a whole-eye finite element analysis. J Refract Surg. 2009;25(10):875-87.
15. Mousavi SJ, Nassiri N, Masoumi N, Nassiri N, Majdi-N, Farzaneh S, et al. finite Element Analysis of Blunt Foreign Body Impact on the Cornea After PRK and LASIK. J Refract Surg. 2012;28(1):59-64.
16. Roy AS, Dupps WJ Jr. Patient-specific modeling of corneal refractive surgery outcomes and inverse estimation of elastic property changes. J Biomech Eng. 2011;113(1):011002.
17. Shafahi M, Vafai K. Human eye response to the thermal disturbances. J Heat Transfer. 2011;113:011009.
18. Papaioannou A, Samaras T. Numerical model of heat transfer in the rabbit eye expo-sed to 60-GHz millimeter wave radiation. IEEE Trans Biomed Eng. 2011;58(9):2582-8.
19. Jo B, Aksan A. Prediction of the extent of thermal damage in the cornea during conductive keratoplasty. J Therm Biol. 2010;35:167-74.
20. Mandel Y, Laufer S, Rubinsky B. Measurement of corneal endothelial impedance with non-invasive external electrodes - A theoretical study. Med Eng Phys. 2012;34(2): 195-201.
21. Guimera A, Ivorra A, Gabriel G, Villa R. Non-invasive assessment of corneal endothe-lial permeability by means of electrical impedance measurements. Med Eng Phys. 2010;32(10):1107-15.
22. Li L, Pinsky PM. A nonlinear macroscopic multi-phasic model for describing in-teractions between solid, fluid and ionic species in biological tissue materials. Philosophical Magazine. 2011;91(2):300-14.
23. Anderson K, El-Sheikh A, Newson T. Application of structural analysis to the mecha-nical behaviour of the cornea. J R Soc Interface. 2004;1(1):3-15.
24. Howland HC, Rand RH, Lubkin SR. A thin-shell model of the cornea and its application to corneal surgery. Refract Corneal Surg. 1992;8(2):183-6.
25. Pinsky PM, Datye DV. A microstructurally-based finite element model of the incised human cornea. J Biomech. 1991;24(10):907-22.
26. Li LY, Tighe B. The anisotropic material constitutive models for the human cornea. J Struct Biol. 2006;153(3):223-30.
27. Elsheikh A, Wang D. Numerical modelling of corneal biomechanical behavior. Com-put Methods Biomech Biomed Engin. 2007;10(2):85-95.
28. Dubbelman M, Sicam VA, Van der Heijde GL. The shape of the anterior and posterior surface of the aging human cornea. Vision Res. 2006;46(6-7):993-1001.
29. Hoeltzel DA, Altman P, Buzard K, Choe K. Strip Extensiometry for Comparison of the Mechanical Response of Bovine, Rabbit, and Human Corneas. J Biomech Eng. 1992; 114(2):202-15.
30. Nguyen TD, Jones RE, Boyce BL. A nonlinear anisotropic viscoelastic model for the tensile behavior of the corneal stroma. J Biomech Eng. 2008;130(4):041020.
31. Nguyen TD, Boyce BL. An inverse finite element method for determining the aniso-tropic properties of the cornea. Biomech Model Mechanobiol. 2011;10(3):323-37.
32. Buzard KA. Introduction to Biomechanics of the Cornea. Refract Corneal Surg. 1992; 8:127-38.
33. Salimi S, Park SS, Freiheit T. Dynamic response of intraocular pressure and biomecha-nical effects of the eye considering fluid-structure interaction. J Biomech Eng. 2011; 133(9):091009.
34. Hughes TJ. Generalization of selective integration procedures to anisotropic and non linear media. Int J Numer Methods Eng. 1980;15(9):1413-8.
35. Uchio E, Ohno S, Kudoh J, Aoki K, Kisielewicz LT, Simulation model of an eyeball based on finite element analysis on a supercomputer. Br J Ophthalmol. 1999;83(10): 1106-11.
36. Amini R, Barocas VH. Anterior chamber angle opening during corneoscleral inden-tation: the mechanism of whole eye globe deformation and the importance of the limbus. Invest Ophthalmol Vis Sci. 2009;50(11):5288-94.
37. Elsheikh A, Geraghty B, Rama P, Campanelli M, Meek KM. Characterization of age-related variation in corneal biomechanical properties. J R Soc Interface. 2010;7(51):1475-85.
38. Fraldi M, Cutolo A, Esposito L, Guarracino F. The role of viscoelasticity and stress gradients on the outcome of conductive keratoplasty. Biomech Model Mechano-biol. 2011;10(3):397-412.
39. Vito RP, Shin TJ, McCarey BE. A mechanical model of the cornea: the effects of phy-siological and surgical factors on radial keratotomy surgery. Refract Corneal Surg. 1989;5(2):82-8.
40. Bryant MR, Velinsky SA, Plesha ME, Clarke GP. Computer aided surgical design in refractive keratotomy. CLAO J. 1987;13(4):238-42.
41. Hanna KD, Jouve FE, Waring GO. Preliminary computer simulation of the effects of radial keratotomy. Arch Ophthalmol. 1989;107(6):911-8.
42. Velinsky SA, Bryant MR. On the computer-aided and optimal design of keratorefrac-tive surgery. Refract Corneal Surg. 1992;8(2):173-82.
43. Niroomandi S, Alfaro I, González D, Cueto E, Chinesta F. Real-time simulation of surgery by reduced-order modeling and X-FEM techniques. Int J Numer Method Bio med Eng. 2012;28:574-88.
44. Bryant MR, McDonnell PJ. Constitutive laws for biomechanical modeling of refractive surgery. J Biomech Eng. 1996;118(4):473-81.
45. Cristóbal JA, del Buey MA, Ascaso FJ, Lanchares E, Calvo B, Doblaré M. Effect of limbal relaxing incisions during phacoemulsification surgery based on nomogram review and numerical simulation. Cornea. 2009;28(9):1042-9.
46. Yoo L, Reed J, Shin A, Kung J, Gimzewski JK, Poukens V, et al. Characterization of ocular tissues using microindentation and hertzian viscoelastic models. Invest Ophthalmol Vis Sci. 2011;52(6):3475-82.
47. Wollensak G, Spoerl E, Seiler T. Stress-Strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J. Cataract Refractive Surg. 2003;29(9):1780-5.
48. Zeng Y, Yang J, HuangK, Lee Z, Lee X. A comparison of biomechanical properties between human and porcine cornea. J Biomech. 2001;34(4):533-7.
49. Kohlhaas M, Spoerl E, Schilde T, Unger G, Wittig C, Pillunat LE. Biomechanical evidence of the distribution of cross-links in corneas treated with riboflavin and ultraviolet A light. J Cataract Refract Surg. 2006;32(2):279-83.
50. Elsheikh A, Wang D, Pye D. Determination of the modulus of elasticity of the human cornea. J Refract Surg. 2007;23(8):808-18.
51. Petsche SJ, Chernyak D, Martiz J, Levenston ME, Pinsky PM. Depth-dependent transverse shear properties of the human corneal stroma. Invest Ophthalmol Vis Sci. 2012;53(2):873-80.
52. Belytschko T, Chen H, Xu J, Zi G. Dynamic crack propagation based on loss of hyperbolicity and a new discontinuous enrichment. Int J Numer Methods Eng. 2003; 58(12):1873-905
53. Sayed AA, Solouma NH, El-berry AA, Kadah YM. Finite element models for computer simulation of intrastromal photorefractive keratectomy. J Mech Med Biol. 2011; 11(05):1255-70.
54. Foster CD, Gongal D, Begaj T, Luo M. Embedded collagen deformation models for computational modeling of healthy, keratoconic, and crosslinked corneas. J Mech Med Biol. 2013;13(03). [13 pages] DOI: 10.1142/S0219519413500243
55. Stitzel JD, Duma SM, Cormier JM, Herring IP. A nonlinear finite element model of the eye with experimental validation for the prediction of globe rupture. In: SAE Conference Proceedings; 2002SAE; 1999; 2002. p.81-102.
56. Weaver AA, Kennedy EA, Duma SM, Stitzel JD. Evaluation of different projectiles in mat-ched experimental eye impact simulations. J Biomech Eng. 2011;133(3):031002.
57. Gray W, Sponsel WE, Scribbick FW, Stern AR, Weiss CE, Groth SL, Walker JD. Numeri-cal modeling of paintball impact ocular trauma: Identification of progressive injury mechanisms. Invest Ophthalmol Vis Sci. 2011;52(10):7506-13.
58. Ghaboussi J, Kwon T, Pecknold DA, Hashash Y. Accurate intraocular pressure predic-tion from applanation response data using genetic algorithm and neural networks. J Biomech. 2009; 42(14):2301-6.
59. Rhee J, Mohammad Nejad T, Comets O, Flannery S, Gulsoy EB, Iannaccone P, Foster CD. The golden spiral in abduction of mouse corneal behaviors. Integrative Biology (Article in press).


67Arq Bras Oftalmol. 2014;77(1):67-70
Instructions Authors
INSTRUCTIONS TO AUTHORS
• Scope and policy• Methods• Types of Manuscripts• Editorial Process• Manuscript Preparation
ABO-ARQUIVOS BRASILeIROS De OFTALMOLOGIA (ABO, ISSN 0004-2749 - printed version and ISSN 1678-2925 - online version) is the official bimonthly publication of the Brazilian Council of Ophthal-mology (Conselho Brasileiro de Oftalmologia - CBO). The purpose of the journal is to publish scientific studies in Ophthalmology, Visual Sciences, and Public Health, encouraging research, as well as qualifi-cation and updating of the professionals involved in this field.
MeTHODSOriginal manuscripts are accepted in Portuguese or English. All
ma nuscripts submitted in Portuguese will be translated to English before publishing. Authors will cover translation costs. Manuscripts are grouped into one of the following categories based on the me-thodology used:
clinical studies
Descriptive or analytical studies involving humans or evaluating the literature relevant to humans.
epidemiological studies
Analytical studies involving results from human populations.
laboratory experimental studies
Descriptive or analytical studies involving animal models or other biological, physical or chemical techniques.
theoretical studies
Descriptive studies involving description and theoretical analysis of new hypotheses based on the knowledge available in the literatu-re. Theoretical results must add new information to literature.
TyPeS OF MAnUSCRIPTSManuscripts submitted to ABO should fit into one of the follo-
wing categories according to their format. The maximum number of words, figures, tables and, references for each type of manuscript are in parentheses at the end of the description for each category. The word count of the manuscript includes the text from the beginning of the introduction up to the end of the discussion; therefore, the following items are not included: title page, abstract, references, acknowledgments, tables and figures, including legends.
editorials
Editorials are contributed by invitation and should be related to to pics of current interest, preferentially related to articles published in the same issue of ABO (title, maximum of 1,000 words, 2 figures or tables, and 10 references).
original articles
Original articles present complete experiments with results that have never been published before (title, structured abstract, maxi-mum of 3,000 words, 7 figures or tables, and 30 references). The eva-luation of the manuscripts will be based on the following priorities:
1. New and relevant information confirmed in a study using appro-priate methodology.
2. Repetition of information available in the literature, but not previously confirmed locally, based on a study using appropriate methodology.
3. Repetition of information available in the literature and previously confirmed locally, based on a study using appropriate methodology.
* Manuscripts containing speculative conclusions, unsubstantiated by the results or based on a study with inappropriate methodology will not be accepted.
case reports and case series
Case reports or case series will be considered for publication when describing rare and original findings that have not been internatio-nally confirmed, or when presenting clinical or surgical responses that can contribute to elucidate the pathophysiology of a disease (ti tle, unstructured abstract, maximum of 1,000 words, 4 figures or tables, and 10 references).
letters to the editor
Letters to the editor are considered for publication if they contain comments related to manuscripts previously published in ABO or, exceptionally, the results of original studies with insufficient content to be submitted as Original Article. These letters should present new information or new interpretation of existing information. When the content of the letter refers to an article previously published in ABO, such article should be mentioned in the first paragraph of the letter and included in its reference list. In these cases, the letters will be linked to the article, and the authors of the article will have their right of reply guaranteed in the same issue. Congratulation letters will not be published (title, maximum of 700 words, 2 figures or tables, and 5 references).
revieW articles
Review articles follow the editorial line and are accepted only by invitation from the editor. Suggestions of topics for review articles should be sent directly to the editor, but manuscripts cannot be sent without an invitation (title, unstructured abstract, maximum of 4,000 words, 8 figures or tables, and 100 references).
eDITORIAL PROCeSSManuscripts will only be considered for publication if they meet
all the journal’s requirements. The editorial office will inform the authors if their manuscript fails to meet such requirements. Upon notification, the corresponding author will have 30 days to make the necessary changes in the manuscript. If the deadline is not met, the manuscript will be excluded from the editorial process.
The manuscripts submitted to ABO are initially evaluated by the editors to check for content compliance with the editorial line of the journal. After this assessment, all manuscripts are sent for peer review. The anonymity of reviewers is preserved throughout the whole process. However, the authors of manuscripts do not remain anonymous.
After the initial editorial evaluation, the reviewers’ comments can be sent to the authors to guide the changes to be implemented in the text. After implementing the changes suggested by the revie-wers, the revised manuscript should be resubmitted along with a letter (which is sent as a supplementary document) with specific in dications of all changes made to the manuscript or the reasons why the suggested changes were not made. Manuscripts that are resubmitted without a letter will be withheld until the editorial office receives the letter. The deadline to submit the new version of the ma-

68 Arq Bras Oftalmol. 2014;77(1):67-70
nuscript is 30 days after the authors are informed of the need to make changes in their manuscript. Manuscripts will be excluded from the process if authors fail to meet this deadline. The ultimate publication will be based on the final approval of the editors.
Manuscripts submitted to ABO should not be simultaneously considered for publication by other journals. In addition, total or par-tial publication or translation for publication in another language of the manuscripts submitted to ABO should not be considered without the permission of the editors of ABO.
AUTHORSHIPThe criteria for authorship of manuscripts in medical journals are
well established. Individuals who have contributed in a concrete way during the following three phases of manuscript preparation should be considered authors: I. Conception and design, acquisition of data, or analysis and
interpretation of data. II. Draft or critical revision of the article for important intellectual
content. III. Final approval of the version to be published.
The authors of manuscripts submitted to ABO should make sure that all authors meet the criteria mentioned above and that all per -sons who meet these criteria are listed. Individuals who hold head-ship positions cannot be considered authors of manuscripts based only on their positions. ABO does not accept the participation of honorary authors.
The corresponding author should complete and submit the Au-thor Contribution Statement as a supplementary document.
GUIDeLIneS FOR eXCeLLenT ReSeARCHIt is recommended that authors follow the appropriate guideline
bellow before submitting your work: • CONSORT (Controlled and randomized clinical trials) • STARD (Diagnostic instruments or techniques) • PRISMA (Systematic reviews and meta-analyses) • STROBE (Observational studies)
MAnUSCRIPT PRePARATIOnManuscripts should only be submitted online using the appro-
priate interface of ABO. The following guidelines were based on the format suggested by the International Committee of Medical Journal Editors (ICMJE) and published in the document: Uniform Require-ments for Manuscripts Submitted to Biomedical Journals.
Only the manuscripts complying with these guidelines will be considered for analysis.
The text should be sent as a digital file. Only the following formats are accepted: .doc or .rtf. The text should be typed double-spaced, in 12 point font. The pages should be numbered in Arabic numerals, starting each section on a new page.
The sections should be presented according to the following se-quence: Title page (as a separate document); Abstract and Keywords; Introduction; Methods; Results; Discussion; Acknowledgements (if any); References; Tables (optional) and Figures (optional) including legends.
1. Title Page. It should contain: a) title (no more than 135 characters with spaces); b) running title to be used as a page heading (no more than 60 characters with spaces); c) authors’ names as they should appear in print; d) each author’s affiliation* (city, state, country and, if applicable, department, school, university); e) corresponding author’s, name, address, phone number, and email; f ) sources of fi-
nancial support (if any); g) project number and institution responsible for the approval of the Research Ethics Committee; h) statement of conflicts of interests of all authors; i) clinical trial registration number on a public trials registry.* Professional or academic degrees, as well as job position will not be published.
Approval of the Institutional Review Board (IRB). All retrospec-tive, cross-sectional, or prospective studies involving primary data collection or clinical and surgical reports should include the project number and name of the institution that provided the approval of the IRB on the title page. Studies involving humans should be compliant with the Declaration of Helsinki, whereas studies involving animals should be in accordance with the principles suggested by the Asso-ciation for Research in Vision and Ophthalmology (ARVO).
As a supplementary document, the corresponding author should send the IRB approval or its report stating that the evaluation of the project by the Committee is not necessary. The author cannot decide on the need for evaluation by the Research Ethics Committee.
Statement of Conflicts of Interest. The title page should contain the statement of conflicts of interest of all authors (even if there is no conflict of interest). For more information about potential conflicts of interest, refer to: World Association of Medical Editors: Conflict of interest in peer-reviewed medical journals.
All authors should send the Form for Disclosure of Potential Con-flicts of Interest as supplementary documents.
Clinical Trials. All Clinical Trials shall include on the title page the registration number in an international registry that allows free ac-cess to trial information (examples: U.S. National Institutes of Health, Australian and New Zealand Clinical Trials Registry, International Standard Randomised Controlled Trial Number - ISRCTN, University Hospital Medical Information Network Clinical Trials Registry - UMIN CTR, Nederlands Trial Register).
2. Abstract and Keywords. Structured abstract (Objective, Metho-ds, Results, Conclusions) with no more than 300 words. Unstructured abstract with no more than 150 words. Five keywords in English listed by the National Library of Medicine (MeSH - Medical Subject Headings).
3. Abstract and Keywords in Portuguese. Structured abstract (Objective, Methods, Results, Conclusions) with no more than 300 words. Unstructured abstract with no more than 150 words. Five keywords in Portuguese listed by BIREME (DeCS - Descritores em Ciências da Saúde). Portuguese translation may be provided by ABO at publication.
4. Introduction, Methods, Results, and Discussion. Citations in the text should be numbered sequentially in superscript Arabic numerals and in parentheses. The names of the authors should not be cited in the text.
5. Acknowledgements. This section should include the colla-boration of people, groups or institutions that deserve to be ack-nowledged but do not meet the criteria for authorship. Statisticians and medical editors may meet the criteria for authorship and, in this case, should be acknowledged as authors. When they do not meet the criteria for authorship, they should be mentioned in this section. Writers who are not identified in the manuscript cannot be accepted as authors; therefore, professional writers should be acknowledged in this section.
6. References. Citations (references) of authors in the text should be numbered sequentially in the same order as they are cited and identified using superscript Arabic numerals. References should be in accordance with the format suggested by the International
69Arq Bras Oftalmol. 2014;77(1):67-70
Committee of Medical Journal Editors (ICMJE), based on the exam-ples below.
The titles of the journals should be abbreviated according to the style provided by the List of Journal Indexed in Index Medicus of the National Library of Medicine.
The names of all authors should be cited for references with up to six authors. For studies with seven or more authors, cite only the first six authors followed by et al.
Examples of references:
Journal ArticlesCosta VP, Vasconcellos JP, Comegno PEC, José NK. O uso da mitomi cina C em cirurgia combinada. Arq Bras Oftalmol. 1999;62(5):577-80.
BooksBicas HEA. Oftalmologia: fundamentos. São Paulo: Contexto; 1991.
Book ChaptersGómez de Liaño F, Gómez de Liaño P, Gómez de Liaño R. Exploración del niño estrábico. In: Horta-Barbosa P, editor. Estrabismo. Rio de Janeiro: Cultura Médica; 1997. p. 47-72.
AnnalsHöfling-Lima AL, Belfort R Jr. Infecção herpética do recém-nascido. In: IV Congresso Brasileiro de Prevenção da Cegueira; 1980 Jul 28-30, Belo Horizonte, Brasil. Anais. Belo Horizonte; 1980. v.2. p. 205-12.
DissertationsSchor P. Idealização, desenho, construção e teste de um ceratômetro cirúrgico quantitativo [dissertation]. São Paulo: Universidade Federal de São Paulo; 1997.
Electronic DocumentsMonteiro MLR, Scapolan HB. Constrição campimétrica causada por vigabatrin. Arq Bras Oftalmol. [online journal]. 2000 [cited 2005 Jan 31]; 63(5): [about 4 p.]. Available at:http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0004-27492000000500012&lng=pt&nrm=iso
7. Tables. Tables should be numbered sequentially using Arabic nu-merals in the order they are mentioned in the text. All tables should have a title and a heading for all columns. Their format should be simple, with no vertical lines or color in the background. All ab-breviations (even if previously defined in the text) and sta tistical tests should be explained below the table. The bibliographical source of the table should also be informed when the table is extracted from another study.Do not include tables in the main document of the manuscript, they should be uploaded as supplementary documents
8. Figures (graphs, photos, illustrations, charts). Figures should be numbered sequentially using Arabic numerals in the order they are mentioned in the text. ABO will publish the figures in black and white at no cost to the authors. Manuscripts with color figures will be published only after the authors pay a publication fee of R$ 500.00 per manuscript.
Graphs should preferably be in shades of gray, on a white background and without three-dimensional or depth effects. Instead of using pie charts, the data should be included in tables or described in the text.Photos and illustrations should have a minimum resolution of 300 DPI for the size of the publication (about 2,500 x 3,300 pixels for a full page). The quality of the images is considered in the evaluation of the manuscript.
The main document should contain all figure legends, typed dou ble-spaced and numbered using Arabic numerals.
Do not include figures in the main document of the manuscript; they should be uploaded as supplementary documents.
Supplemental files can have the following extensions: JPG, BMP, TIF, GIF, EPS, PSD, WMF, EMF or PDF.
9. Abbreviations and Acronyms. Abbreviations and acronyms should be preceded by the spelled-out abbreviation on first mention and in the legends of tables and figures (even if they have been pre-viously mentioned in the text). Titles and abstracts should not contain abbreviations and acronyms.
10. Units of Measurement: Values of physical quantities should be used in accordance with the standards of the International System of Units.
11. Language. Texts should be clear to be considered appropriate for publication in a scientific journal. Use short sentences, written in a direct and active voice. Foreign words should be in italics. Thera-peutic agents should be mentioned by their generic names with the following information in parentheses: trade name, manufacturer’s name, city, state and country of origin. All instruments or apparatus should be mentioned including their trade name, manufacturer’s name, city, state and country of origin. The superscript symbol of trademark ® or™ should be used in all names of instruments or trade names of drugs. Whenever there are doubts about style, terminology, units of measurement and related issues, refer to the AMA Manual of Style 10th edition.
12. Original Documents. Corresponding authors should keep the original documents and the letter of approval from the Research Ethics Committee for studies involving humans or animals, the con-sent form signed by all patients involved, the statement of agreement with the full content of the study signed by all authors and the state-ment of conflict of interest of all authors, as well as the records of the data collected for the study results.
13. Corrections and Retractions. Errors may be noted in published manuscripts that require the publication of a correction. However, some errors pointed out by any reader may invalidate the results or the authorship of a manuscript. If substantial doubt arises about the honesty or integrity of a submitted manuscript, it is the editor’s responsibility to exclude the possibility of fraud. In these situations, the editor will inform the institutions involved and the funding agen-cies about the suspicion and wait for their final decision. If there is confirmation of a fraudulent publication in ABO, the editor will act in compliance with the protocols suggested by the International Com-mittee of Medical Journal Editors (ICMJE) and by the Committee on Publication Ethics (COPE).
CHeCKLISTBefore submitting their manuscript, authors should make sure
that all the following items are available: □Manuscript prepared in accordance with the instructions to
authors. □Maximum number of words, tables, figures, and references
according to the type of manuscript. □ Title page including the clinical trial registration number is not
included in the main document □ No figures and tables are included in the main document of
the manuscript. □ All figures and tables were uploaded separately as supple-
mentary documents. □ Author Contribution Statement completed and saved as a
digital file to be sent as a supplementary document. □ Form for Disclosure of Potential Conflicts of Interest of all
authors completed and saved as digital files to be sent as supplementary documents.
□ Digital version of the report provided by the Institutional Re-view Board containing the approval of the project to be sent as a supplementary document.

70 Arq Bras Oftalmol. 2014;77(1):67-70
Chief Executive Officer: Fernando Steven Ullmann;Commercial Director: Helen Suzana Perlmann; Art Director: Elza Rudolf;
Publishing, Printing and CTP: Ipsis Gráfica e Editora S.A.Frequency of publication: Bimonthly; Circulation: 8.600 copies
Edited byiPSiS gRáFiCA E EDiTORA S.A.
Rua Vereador José Nanci, 151 - Parque Jaçatuba 09290-415 - Santo André - SP - Brazil
Phone: (5511) 2172-0511 - Fax (5511) 2273-1557
AdvertisingconSelho BraSileiro De
OFTAlMOlOgiA
R. Casa do Ator, 1.117 - 2nd Floor - São Paulo - SP - Brazil - 04546-004
Contact: Fabrício LacerdaPhone: (5511) 3266-4000 - Fax: (5511) 3171-0953E-mail: [email protected]
LIST OF WeBITeSOnline interface for submission of manuscripts to ABOhttp://www.scielo.br/ABO
Authors’ Participation Formhttp://www.cbo.com.br/site/files/Formulario Contribuicao dos Auto-res.pdf
International Committee of Medical Journal editors (ICMJe) http://www.icmje.org/
Uniform requirements for manuscripts submitted to biomedical journalshttp://www.icmje.org/urm_full.pdf
Declaration of Helsinkihttp://www.wma.net/en/30publications/10policies/b3/index.html
Principles of the Association for Research in Vision and Ophthalmology (ARVO)http://www.arvo.org/eweb/dynamicpage.aspx?site=arvo2&webcode=AnimalsResearch
World Association of Medical editors: Conflict of interest in peer-reviewed medical journals.http://www.wame.org/conflict-of-interest-in-peer-reviewed-medical-journals
Authorship Principles according to the ICMJehttp://www.icmje.org/ethical_1author.html
Form for Disclosure of Potential Conflicts of Interesthttp://www.icmje.org/coi_disclosure.pdf
COnSORT (Consolidated Standards of Reporting Trials)http://www.consort-statement.org/consort-statement/
STARD (Standards for the Reporting of Diagnostic accuracy studies)http://www.stard-statement.org/
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) http://www.prisma-statement.org/index.htm
STROBe (Strengthening the Reporting of Observational studies in epidemiology)http://www.strobe-statement.org/
U.S. national Institutes of Healthhttp://www.clinicaltrials.gov
Australian and new Zealand Clinical Trials Registryhttp://www.anzctr.org.au
International Standard Randomised Controlled Trial number - ISRCTnhttp://isrctn.org/
University Hospital Medical Information network Clinical Trials Registry - UMIn CTRhttp://www.umin.ac.jp/ctr/index/htm
nederlands Trial Registerhttp://www.trialregister.nl/trialreg/index.asp
MeSH - Medical Subject Headingshttp://www.ncbi.nlm.nih.gov/sites/entrez?db=mesh&term=
DeCS - Health Sciences Keywords in Portuguesehttp://decs.bvs.br/
Format suggested by the International Committee of Medical Journal editors (ICMJe)http://www.nlm.nih.gov/bsd/uniform_requirements.html
List of Journal Indexed in Index Medicushttp://www.ncbi.nlm.nih.gov/journals
AMA Manual of Style 10th editionhttp://www.amamanualofstyle.com/
Protocols of the International Committee of Medical Journal editors (ICMJe) http://www.icmje.org/publishing_2corrections.html
Protocols of the Committee on Publication ethics (COPe)http://publicationethics.org/flowcharts

Barreira microporosa1
Evita o uso de conservantesmemBrana filtrante de 0,2µ1
tuBo flexível e ergonômico1
gotas caliBradas (30µl)1
Doses precisas
Até 2 mesesde utilização após aberto2
Referências Bibliográficas: 1) Patente de Laboratoires Théa. 2) Bula do produto: Hyabak. Registro MS nº 8042140002.HYABAK®. Solução sem conservantes para hidratação e lubrificação dos olhos e lentes de contacto. Frasco ABAK®. COMPOSIÇÃO: Hialuronato de sódio 0,15g. Cloreto de sódio, trometamol, ácido clorídrico, água para preparações injetáveis q.b.p. 100 mL. NOME E MORADA DO FABRICANTE: Laboratoires Théa, 12 rue Louis Blériot, 63017 CLERMONT-FERRAND CEDEX 2 - França. QUANDO SE DEVE UTILIZAR ESTE DISPOSITIVO: HYABAK® contém uma solução destinada a ser administrada nos olhos ou nas lentes de contato. Foi concebido: • Para humedecimento e lubrificação dos olhos, em caso de sensações de secura ou de fadiga ocular induzidas por fatores exteriores, tais como, o vento, o fumo, a poluição, as poeiras, o calor seco, o ar condicionado, uma viagem de avião ou o trabalho prolongado à frente de um ecrã de computador. • Nos utilizadores de lentes de contato, permite a lubrificação e a hidratação da lente, com vista a facilitar a colocação e a retirada, e proporcionando um conforto imediato na utilização ao longo de todo o dia. Graças ao dispositivo ABAK®, HYABAK® permite fornecer gotas de solução sem conservantes. Pode, assim, ser utilizado com qualquer tipo de lente de contato. A ausência de conservantes permite igualmente respeitar os tecidos oculares. ADVERTÊNCIAS E PRECAUÇÕES ESPECIAIS DE UTILIZAÇÃO: • Evitar tocar nos olhos com a ponta do frasco. • Não injetar, não engolir. Não utilize o produto caso o invólucro de inviolabilidade esteja danificado. MANTER FORA DO ALCANCE DAS CRIANÇAS. INTERAÇÕES: É conveniente aguardar 10 minutos entre a administração de dois produtos oculares. COMO UTILIZAR ESTE DISPOSITIVO: POSOLOGIA: 1 gota em cada olho durante o dia, sempre que necessário. Nos utilizadores de lentes: uma gota em cada lente ao colocar e retirar as lentes e também sempre que necessário ao longo do dia. MODO E VIA DE ADMINISTRAÇÃO: INSTILAÇÃO OCULAR. STERILE A - Para uma utilização correta do produto é necessário ter em conta determinadas precauções: • Lavar cuidadosamente as mãos antes de proceder à aplicação. • Evitar o contato da extremidade do frasco com os olhos ou as pálpebras. Instilar 1 gota de produto no canto do saco lacrimal inferior, puxando ligeiramente a pálpebra inferior para baixo e dirigindo o olhar para cima. O tempo de aparição de uma gota é mais longo do que com um frasco clássico. Tapar o frasco após a utilização. Ao colocar as lentes de contato: instilar uma gota de HYABAK® na concavidade da lente. FREQUÊNCIA E MOMENTO EM QUE O PRODUTO DEVE SER ADMINISTRADO: Distribuir as instilações ao longo do dia, conforme necessário. EFEITOS NÃO PRETENDIDOS E INCÔMODOS (EFEITOS INDESEJÁVEIS): Rara possibilidade de ligeiras irritações oculares. CONSERVAÇÃO DE DISPOSITIVO: NÃO EXCEDER O PRAZO LIMITE DE UTILIZAÇÃO, INDICADO NA EMBALAGEM EXTERIOR. PRECAUÇÕES ESPECIAIS DE CONSERVAÇÃO: Conservar a uma temperatura inferior a 25ºC. Depois de aberto, o frasco não deve ser conservado mais de 8 semanas. DATA DE REVISÃO DESTE FOLHETO INFORMATIVO: 04/2009. Registro MS nº 80424140002.
Material dirigido exclusivamente a profissionais habilitados a prescrever e/ou dispensar medicamentos.
uso compátivel com lentes de contato2
facilita a colocaçãoe a retirada, e proporciona
conforto imediatoP
rodu
zido
em
: Fev
/201
4

38756004_21X28_B2B_2.indd 1 12/9/13 11:14 AM


















