Romildo Torres da Silva.pdf

If you can't read please download the document
Transcript of Romildo Torres da Silva.pdf
-
UNIVERSIDADE NOVE DE JULHO
Programa de Ps-Graduao em Biofotnica Aplicada s Cincias
da Sade
Romildo Torres da Silva
EFEITO DO LASER DE BAIXA POTNCIA (660NM) NA TENDINITE
INDUZIDA POR COLAGENASE EM TENDO CALCNEO DE RATOS
So Paulo, SP 2013
-
ROMILDO TORRES DA SILVA
EFEITO DO LASER DE BAIXA POTNCIA (660NM) NA TENDINITE
INDUZIDA POR COLAGENASE EM TENDO CALCNEO DE RATOS
Dissertao apresentada ao Programa de Ps-Graduao em Biofotnica Aplicada s Cincias da Sade da Universidade Nove de Julho, para obteno do Ttulo de Mestre em Cincias. rea de Concentrao: Sade Orientador: Prof. Dr. Rodrigo Labat Marcos
So Paulo, SP 2013
-
Torres-silva, R. Efeito do laser de baixa potncia (660nm) na tendinite induzida
por colagenase em tendo calcneo de ratos. / Romildo Torres da Silva 2013.
52 f.
Dissertao (mestrado) Universidade Nove de Julho - UNINOVE, So Paulo,
2013.
Orientador (a): Prof. Dr. Rodrigo Labat Marcos.
1. Tendinite. 2. Inflamao aguda. 3. Tendo calcneo. 4. Colagenase. I. Marcos, Rodrigues Labat. II. Titulo
CDU 615.831
-
Dedico este trabalho:
minha esposa, Ana Maria
Aos meus filhos Thiago, Reinaldo e Juliana
As minhas netas Milena e Alice.
-
AGRADECIMENTOS
A Deus, o nosso Grande Arquiteto do Universo, sem ele nada seria
possvel.
A minha famlia, em especial ao meu grande amor minha esposa Ana
Maria.
Ao meu orientador Prof. Dr. Rodrigo Labat Marcos, pela orientao
nos trabalhos desenvolvidos, dedicao apoio e amizade.
Ao Prof. Dr. Rodrigo lvaro Brando Lopes Martins, pela confiana,
oportunidade e pela amizade.
A todos os amigos de sala, em especial a Ana, Manolo e Elis.
A todos os Professores Doutores que contriburam direta e
indiretamente para a realizao do trabalho.
MUITO OBRIGADO!!!!!!!!!
-
O mundo de um cego definido pelo limite de seu tato. O de um
homem ignorante, pelos limites do seu conhecimento. J o mundo de um
grande homem definido pelo tamanho do seu conhecimento.
(Autor desconhecido)
-
RESUMO
TORRES-SILVA, R. Efeito do laser de baixa potncia (660nm) na tendinite
induzida por colagenase em tendo calcneo de ratos. 52f . Dissertao
(Mestrado em Biofotnica Aplicada a Cincias da Sade) Universidade UNINOVE,
So Paulo, 2013.
Tendinopatias so distrbios comuns com uma variedade de tratamentos e terapias
e a Laserterapia aparece como uma alternativa no tratamento destas doenas. Ns
investigamos os efeitos da irradiao laser no modelo de tendinite induzida por
colagenase, em tendes calcneo de ratos, verificando sua ao em importantes
marcadores inflamatrios. Mtodos: Foram utilizados ratos machos (Wistar) divididos
em grupos: Controle (C), Tendinite No Tratado (NT), Tratamento com Diclofenado
de Sdio (D) ou Laser (1J) e (3J). A tendinite foi induzida por colagenase
(100g/tendo) sobre o tendo calcneo que foi removido para anlises. Foi
verificado a expresso gnica de COX-2, TNF-, IL-6 e IL-10 (RT-PCR). Resultados
e discusso: A laserterapia (660nm, 100mW, 3J), utilizada no tratamento da tendinite
induzida por colagenase em tendo calcneo de ratos, foi eficaz na reduo de
importantes marcadores inflamatrios, tornando-se uma ferramenta promissora para
o tratamento de leses tendneas.
Palavras-chave: Tendinite. Inflamao Aguda. Tendo calcneo. Colagenase.
Laser de baixa potncia.
-
ABSTRACT
TORRES-SILVA, R. Effect of the low level laser therapy (660nm) in the induced
tendinitis by collagenase in aquilles tendon of rats. 52pg. Master in Applied
Biophotonics the Health Sciences - UNINOVE, So Paulo , 2013.
Tendinopathy is a common disease with a variety of treatments and therapies. Laser
therapy appears as a alternative treatment. We research the effects of the laser
irradiation in tendinitis model induced by collagenase injection on Achilles tendon
rats, verified its action in important inflammatory markers. Methods: The male rats
(Wistar) were used and divided in groups: Saline (C), Tendinitis (NT) and tendinitis
treated with Sodium diclofenac (D) or Laser (1J) and (3J). The tendinitis was induced
by collagenase (100g/tendon) on the Achilles tendon which was removed for
analyzes. The gene expression for COX-2; TNF-; il-6 and IL-10 (RT-PCR) was
measured. Results and discussion: The Laser therapy (660nm, 100mW, 3J) used
in the treatment of the tendinitis induced by collagenase in Achilles tendon in rats,
was effective in the reduction of important inflammatory markers, becoming a
promising tool for the treatment of tendon diseases.
Word-key: Tendinitis. Acute inflammation. Achilles tendon. Collagenase. Low
Intensity laser therapy.
-
SUMRIO
1- INTRODUO..............................................................................................11
1.1- Tendo...............................................................................................12
1.2- Arquitetura interna dos tendes..........................................................13
1.3- Tecido colgeno.................................................................................14
1.4- Processo Inflamatrio .......................................................................14
1.5- Inflamao do Tendo........................................................................15
1.5.1 Cicloxigenase 2 (COX-2)...................................................................16
1.5.2 Interleucinas IL-6 e IL-10...................................................................17
1.5.3 Fator de necrose tumoral TNF-........................................................18
1.6- Tratamentos......................................................................................18
1.7- Laserterapia.......................................................................................19
2- OBJETIVOS..................................................................................................22
3- MATERIAL E MTODOS.............................................................................23
3.1 Animais...............................................................................................23
3.2 Grupos Experimentais........................................................................23
3.3 Induo da tendinite............................................................................24
3.4 Aplicao da Terapia com Laser de Baixa Potncia (LBP)..............25
3.5 Anlises de expresso gnica por RT-PCR.....................................25
3.6 Anlise estatstica...............................................................................26
4- RESULTADOS................................................................................................27
4.1 Artigo submetido para publicao.......................................................27
5- CONSIDERAES FINAIS.............................................................................43
6- REFERNCIAS..............44
7- ANEXO 1 (Aprovao do comit de tica e pesquisa)....................................52
-
LISTA DE ABREVIAES
AP Fosfatase Alcalina
ATP Adenosina Trifosfato
-actina Anticorpo Policlonal
cDNA DNA Complementar
COX Ciclo-Oxigenase
DNAse Enzima catalizadora do cido Desoxirribonuclico
FP Fibrinognio Plasmtico
HILT - High Intensity Laser Treatment
IL Interleucina
JMT Juno Msculo-tendnea
JOT Juno steo-tendnea
LASER Light Amplification by Stimulated Emission of Radiation
LBP Laser de Baixa Potncia
LILT - Low Intensity Laser Treatment
MMP Metaloproteinase da Matriz
mW MiliWatt
nm Nanmetro
PMNs Polimorfonucleares
RNA cido Ribonuclico
RNAm cido Ribonuclico mensageiro
RT PCR reao de transcriptase reversa reao em cadeia da polimerase
TNF- Fator de Necrose Tumoral
-
LISTAS DE FIGURAS
Figura 1: Tendo Calcneo..............................................................................pag 12
Figura 2: Arquitetura interna dos tendes.........................................................pag 13
Figura 3: Esquema de grupos experimentais...................................................pag 23
Figura 4: Seqncia de Primers..................................................................pag 25-26
Figura 5: Tabela dos resultados......................................................................pag 44
-
11
1 INTRODUO
As doenas musculoesquelticas entre elas a tendinite, em virtude da sua
frequncia, do custo do tratamento, da reduo da funcionalidade laboral e do
desencadeamento de co-morbidades, necessitam de recursos financeiros
considerveis para o acompanhamento da sade dos indivduos vtimas destas
patologias, principalmente nos casos em que a incapacidade no trabalho persiste
alm do tempo mdio para o retorno s atividades laborativas (BERNARD B., 1997,
ARVIDSSON S. et al., 2008).
As tendinopatias so alteraes na sade do tendo, geralmente frequentes e
difceis de serem tratadas, incapacitando desde atletas profissionais e recreacionais
at pessoas comuns em seu local de trabalho. A tendinite tem um alto impacto na
qualidade de vida do indivduo que requer freqente atendimento mdico mesmo
nos casos simples, constituindo um desafio teraputico nos casos crnicos
(BARROS M. et al.; 2006; AITTOMAKI A. et al., 2006).
Sua ocorrncia alta, especialmente quando consideramos o tendo
calcneo, o patelar e o do cotovelo, onde a cronificao da doena comum
(LANGBERG e KONGS-GAARD, 2008), sendo objeto de preocupao entre as
classes de trabalhadores em diversas ocupaes, pela reduo da qualidade de vida
e pelo alto custo ao sistema de sade (LOISEL P., et al 2002). Quando a doena
cronifica, ocorre um aumento considervel dos recursos despendidos pelo
empregador, relacionados ao afastamento e a necessidade de relocao e
qualificao de outro para o exerccio desta funo (NGUYEN et al 2007).
Sua predominncia foi relatada entre 2% dos trabalhadores ativos e 55% dos
atletas (LIN et al, 2006). Nos Estados Unidos, foi observado um aumento de 39%
dos gastos com indenizaes e 62% com custos mdicos no perodo de 1991
2001. No Brasil, acidentes de trabalho e doenas ocupacionais somaram 509.062
dias de trabalho perdidos em 2000, responsvel por R$8.492.762,00 de gastos com
benefcios concedidos pelo INSS, apenas no estado da Bahia (SANTANA et al.,
2006).
Porm, a etiologia das tendinopatias ainda no foi totalmente explicada
(ALFREDSON e LORENTZON, 2000), mas sua ocorrncia elevada faz destas
doenas um grande problema scio-econmico onde as intervenes mdicas e
terapias para a reabilitao so ainda limitadas (LANGBERG e KONGS-GAARD,
-
12
2008). Sua preveno, a identificao das causas associadas e a promoo do
retorno seguro s atividades laborativas, portanto, tornaram-se tema de estudos no
campo da sade pblica (BARBE MF, 2006).
1.1 Tendo
Tendes saudveis apresentam colorao branca brilhante e textura
fibroelstica, mostrando grande resistncia a tenses mecnicas. Eles podem variar
muito quanto forma, e ainda quanto maneira como esto ligados ao osso. Alm
disso, a juno miotendnea (JMT) tambm mostra variaes anatmicas entre
diferentes msculos.
Figura 1. Tendo calcneo (Aquiles) de humano. (vista posterior). Fonte:
Wikipdia.org.
Tendes so estruturas anatmicas interpostas entre msculos e ossos
(figura 1), que transmitem a fora gerada no msculo para o osso, tornando possvel
o movimento articular (JZSA e KANNUS, 1997; KHAN et. al., 1999). Os elementos
bsicos dos tendes so fibras de colgeno e matriz extracelular rica em
proteoglicanas, formadas a partir de clulas denominadas tencitos. O colgeno
fornece a fora tnsil ao tendo, enquanto a matriz fornece suporte estrutural para
as fibras de colgeno e regula a transformao extracelular de pr-colgeno em
-
13
colgeno maduro (ASTROM, 1997). Os tenoblastos, clulas achatadas e distribudas
entre as fibras de colgeno sintetizam tanto a matriz extracelular, quanto o pr-
colgeno. O colgeno arranjado hierarquicamente em nveis de complexidade
crescente, comeando com protocolgeno, fibras, fascculos, bandas tercirias e
finalmente o tendo propriamente dito (JZSA e KANNUS, 1997; ASTROM, 1997;
KHAN et al., 1999).
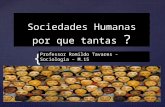
1.2 Arquitetura interna dos tendes
O tendo completamente coberto pelo epitendo, uma camada fina de
tecido conjuntivo contendo suprimentos nervosos, vasculares e linfticos. O
epitendo se estende profundamente no tendo, entre as bandas tercirias e o
endotendo (figura 2). Mais superficialmente, o epitendo envolvido pelo
paratendo, um tecido conjuntivo areolar contendo basicamente fibrilas de colgeno
(KVIST et al., 1985), algumas fibrilas elsticas e uma linha interna de clulas
sinoviais (WILLIANS, 1986).
Figura 2. Organizao hierrquica da estrutura do tendo (das fibrilas de colgeno
at o tendo propriamente dito). Fonte: KASTELIC et al. (1978).
1.3 Tecido Colgeno
-
14
As fibras formadas por colgeno representam dois dos trs principais tipos de
fibras do tecido conjuntivo, as fibras colgenas e as reticulares. As fibras elsticas
so formadas pela protena elastina.
O colgeno a protena mais abundante do organismo, representando cerca
de 30% do peso seco e pode ser classificado nos seguintes grupos: (1) colgenos
que formam longas fibrilas; (2) colgenos associados a fibrilas; (3) colgeno que
forma rede e (4) colgeno de ancoragem. O colgeno que forma os tendes, ossos,
dentina, derme e outros tecidos, est includo no 1o Grupo.
A sntese de colgeno foi primeiramente atribuda a uma variedade restrita de
tipos celulares como fibroblastos, osteoblastos e condroblastos. Atualmente, existem
evidncias convincentes de que outros tipos celulares so capazes de sintetizar o
colgeno (JUNQUEIRA e CARNEIRO, 2004).
O colgeno um dos principais componentes da matriz extracelular,
responsvel pela resistncia trao atuando tambm na estabilidade do tecido
conjuntivo (MOALI C, 2012, WIDMER, C, et al 2012 ). Esta integridade e
estabilidade do tecido so reguladas principalmente atravs de um equilbrio entre
produo, organizao e degradao do colgeno (HULMES DJ 2002). O colgeno
fibrilar mais abundante no tendo primeiramente o colgeno do tipo I, seguido pelo
colgeno tipo II e III, sintetizados a partir do pr colgeno (HULMES, 2008).
1.4 Processo Inflamatrio
A inflamao uma resposta biolgica complexa do tecido estmulos
nocivos como, clulas danificadas, ou irritantes (FERRERO- MILIANI L. et al., 2007)
sendo um dos mecanismos de proteo do organismo com a funo de neutralizar e
remover este estmulos nocivos, promovendo o reparo. A inflamao aguda um
processo de curta durao, aparecendo geralmente dentro de alguns minutos ou
horas (COTRAN et al., 1998).
O mecanismo fisiopatolgico da inflamao explicado por um conjunto de
reaes locais e gerais do organismo, compondo uma srie de fenmenos
complexos que se associam e se complementam, formando uma reao em
cascata, que envolve clulas inflamatrias, como: neutrfilos, linfcitos e moncitos/
macrfagos (TEDGUI e MALLAT, 2001).
-
15
Durante a resposta inflamatria aguda, ao libertar mediadores inflamatrios
responsveis pelos sinais de inflamao, ocorre a vasodilatao e consequente
aumento do fluxo sanguneo, apresentando na rea inflamada vermelhido e
aumento do calor. O aumento da permeabilidade dos vasos sanguneos resulta em
uma exsudao do plasma e protenas de fluidos para os tecidos, se manifestando
como inchao. Alguns mediadores inflamatrios liberados durante este processo
podem alterar determinadas molculas dos vasos sanguneos permitindo a migrao
de leuccitos, principalmente de neutrfilos provocando um infiltrado inflamatrio. Os
neutrfilos migram por quimiotaxia at o local da leso (COTRAN et al., 1998).
1.5 Inflamao do Tendo
Historicamente, tendes so conhecidos como partes vulnerveis do corpo
humano. Hipcrates reportou que se o tendo de Aquiles (calcneo) fosse lesado,
poderia causar febre aguda, convulses, inconscincia e finalmente a morte.
Felizmente, leses no calcneo nos dias de hoje no esto associadas com morte,
mas algumas vezes podem causar condies crnicas dolorosas e de difcil
tratamento.
No processo inflamatrio crnico, ocorre o remodelamento da bainha
tendnea e do tecido sinovial, aumentando a quantidade de clulas inflamatrias.
Estas alteraes no tecido tendneo conduzem a um distrbio com reduo de sua
funcionalidade. Outra complicao est no fato que os tendes usam suas
extremidades para se ligarem em outras estruturas, como ossos e cartilagens e uma
vez alterado, este processo inflamatrio pode migrar para outros tecidos iniciando
um quadro pr-artrtico. Esta pode ser a explicao sobre como os tendes so
afetados pela inflamao crnica e como a tendinite pode influenciar no
aparecimento e evoluo de doenas inflamatrias nos ossos e cartilagens (HAYER
et al., 2007).
De maneira Geral, o tendo humano tem uma alta capacidade de suportar
tenses. Medies diretas em calcneos humanos registraram foras de at 9 kN
(correspondente a 12,5 vezes o peso corporal) durante uma corrida em velocidade
de 6 m/s. Entretanto, hoje sabemos que a fora mxima suportada desse tendo
-
16
uma varivel bastante individual, indicando tambm uma faixa ampla de
suscetibilidade a sobrecargas.
Existe um grande nmero de sugestes quanto aos fatores etiolgicos da
tendinite, mas so poucas as comprovaes cientficas. A causa determinante mais
comum o esforo exagerado de extenso sobre os tendes, ocorrendo distenso
de suas fibras, que por no suportarem a trao mecnica, podem apresentar
rupturas parciais desenvolvendo intensa e dolorosa reao inflamatria local
(ALFREDSON e LORENTZON, 2000).
Alm da sobrecarga mecnica conhecida como o principal fator causador das
tendinopatias, existem processos lesivos repentinos e o envelhecimento que
tambm contribuem para a degenerao do tendo que pode ocorrer na ausncia
(tendinose) ou na presena (tendinite) de resposta inflamatria (SUN et al., 2008).
1.5.1 Cicloxigenase 2 (COX-2)
Aps a leso do tendo, o organismo inicia uma srie de eventos para a
promoo do reparo tecidual que pode ter como resultado a alterao do tecido e
formao de cicatriz (LIN al, 2006). A cicatriz inicialmente fornece a continuidade
fsica do tecido, porm pode provocar a formao de tecidos adjacentes
indesejveis, impedindo o mecanismo de deslizamento do tendo (BEREDJIKLIAN
et al., 2003). J a inflamao intensa, com grande migrao leucocitria e formao
de citocinas pr-inflamatrias partir da Ciclo-oxigenase, promove a alterao do
tecido, pelo aumento de fibroblastos e mudana da matriz extracelular (LIECHTY et
al., 2000).
A prostaglandina H2 sintase, tambm conhecida como cicloxigenase uma
enzima integral da membrana celular, participando da cascata inflamatria.
Geralmente so constitutivas, porm a COX-2 pode ser induzida durante a resposta
inflamatria, influenciando ainda a formao de mediadores inflamatrios tais como
interleucinas, prostaglandinas e tromboxanos (KOMOTO J. et al 2006). Algumas
destas citocinas, entre elas a IL-1, IL-6 e IL-12 e ainda o TNF- so reprimidas
drasticamente no final do processo inflamatrio, durante o reparo tecidual (RANG
and DALE, 2012).
A expresso de COX-2 pode ser tambm aumentada aps a induo do
processo inflamatrio em tendes calcneos de ratos (MARCOS et al, 2011). Ao
-
17
contrrio, sua reduo foi observada aps terapias farmacolgicas e no
farmacolgicas, como na utilizao da laserterapia de baixa potncia (WANG et al,
2003; XAVIER et al, 2010; MARCOS et al, 2011).
1.5.2 Interleucinas IL-6 e IL-10
Uma maneira de reduzir o processo inflamatrio no tecido lesionado seria
controlar o processo de cicatrizao pela modulao do processo inflamatrio e dos
nveis de citocinas anti e pr-inflamatrias envolvidas no reparo (RICCHETTI et al.,
2008). Entre estas citocinas, as interleucinas teriam um papel importante na
modulao da inflamao do tendo (LIN et al., 2006).
A IL-6, uma citocina com papel central na inflamao aps processos
lesivos (SKUTEK M, et al., 2001). No processo inflamatrio agudo do tendo
observado um aumento expressivo de granulcitos e neutrfilos na bainha sinovial,
geralmente ativados pelo aumento de IL1 e IL6. A presena destas duas citocinas
esta diretamente relacionada a progresso da tendinite (HAYER et al., 2007). Outros
estudos sugeriram que as citocinas inflamatrias pode desempenhar um papel
durante a progresso das condies das tendinopatias, uma vez que tambm foram
detectados no processo da dor e ruptura do tendo ([FU SC, et al., 2002, NAKAMA
K, et al. , 2006).
A IL-10 foi identificada inicialmente por MOSMANN et al. (1989), sendo
reconhecida por sua atividade antiimunolgica e antiinflamatria. Desde sua
descrio, a lista de clulas produtoras de IL-10 se expandiu rapidamente assim
como o nmero de clulas que so capazes de responder a essa citocina (MOSSER
et al., 2008). A IL-10 tambm conhecida por inibir a expresso de IL-6 e IL-8 e a
migrao de clulas inflamatrias no local da leso incluindo macrfagos e
moncitos (ALAM et al., 1994; RICCHETTI et al., 2008).
Durante o processo inflamatrio a interleucina IL-10 possui uma importante
funo biolgica de inibir a maturao e a diferenciao de clulas dendrtica em
moncitos e de inibir a produo de citocinas pr-inflamatrias exposio IL-10
que pode ainda inibir a inflamao, aumentando os receptores antagonistas de IL-1
pelos macrfagos (MOSSER et al., 2008).
-
18
1.5.3 Fator de necrose tumoral TNF-
O fator de necrose tumoral (TNF-) uma citocina pleitrpica, relacionada
tanto na sobrevivncia e proliferao celular como na morte celular no processo
apopttico. Esta citocina tambm distribuda e expressa em tencitos em
condies inflamatrias onde a apoptose e a proliferao celular acentuada
(HOSAKA et al., 2005).
O TNF- considerado uma citocina chave na origem de vrias doenas
osteomusculares, como Artrite Reumatide, Osteoartrite e Tendinite (HAYER et al.,
2007), porm, seu papel na doena do tendo ainda no foram bem determinada.
Sabe-se que em tendes de equinos, o TNF- pode apresentar aes anti-
apoptticas e apoptticas, controlando o nmero de clulas, sendo um fator
importante no progresso de degenerao do tecido tendneo (HOSAKA et al., 2005).
Os tendes so bastante afetados pela inflamao tambm por estarem
sujeitos a foras especficas e cargas mecnicas prolongadas (HAYER et al., 2007).
Nestas condies patolgicas, o tecido tendneo pode apresentar aumento dos
receptores de TNF- (R1 e R2) (HOSAKA et al., 2005).
Os nveis de TNF- so aumentados nos tecidos msculo-tendneos, em
situaes ps-traumticas (ELSAID et al., 2008). As cirurgias de tendo, cartilagem
e osso outro fator que pode dar incio a um processo inflamatrio. Aps uma leso,
sejam por um acidente ou por uma interveno mdica, os nveis de citocinas
inflamatrias como TNF- e IL so aumentados (AKESEN et al., 2009).
1.6 Tratamentos
Condies inflamatrias de tendes esto associadas a uma ampla variedade
de tratamentos propostos, algumas delas com poucas evidncias cientficas que
apoiem seu uso (KVIST, 1994; KHAN et al., 1999; ALFREDSON e LORENTZON,
2000; ANDRES et al., 2008; BJORDAL et al., 2008).
Os tratamentos da tendinite tm por finalidade a reduo da inflamao, que
se persistir, promove alteraes nos feixes das fibras de colgeno e aumento da
atividade de determinadas enzimas, prolongando-se assim as fases inflamatria e
proliferativa, favorecendo a deposio excessiva de tecido cicatricial, alterando
-
19
algumas caractersticas como a reduo da resistncia em comparao ao tendo
original (FERNANDES et al., 2003).
O tratamento mais comum o conservador, recomendado pela maioria dos
autores como estratgia inicial. Na maioria das vezes consiste em uma abordagem
multi-orientada, incluindo modelos de reabilitao combinada como repouso,
medicao a base de antiinflamatrios no esteroidais e corticides, crioterapia,
massagem, treinamento de fora.
A eficcia do tratamento aumenta com a determinao da fase em que o
processo inflamatrio no tendo se encontra. Na fase inicial do processo de
reparao, podem ser institudas prticas hidroterpicas frias, visando-se reduzir o
metabolismo na regio, e agentes antiinflamatrios esteroidais ou no-esteroidais
(ALVES e MIKAIL, 2006).
Os corticosterides so bem absorvidos em qualquer stio de administrao,
(tpica, oral, subcutnea, intramuscular, intralesional e intravenosa), porm podem
provocar efeitos deletrios no uso intralesional (POOL et al., 1980).
Os antiinflamatrios no esteroidais so as drogas utilizadas com mais
freqncia, como parte do tratamento inicial, principalmente na reduo da dor,
embora seja comum encontrarmos amostras de tendes durante a tendinopatia, com
ausncia de clulas inflamatrias que justifique esta preferncia (ALFREDSON et
al., 2003; ANDRES et al., 2008).
1.7 Laserterapia
Vrios trabalhos foram publicados para melhorar o entendimento dos efeitos
da terapia LASER no tratamento de doenas inflamatrias. Porm, apesar de todas
as investigaes realizadas e do importante uso clnico do laser de baixa potncia, o
conhecimento bsico de seus mecanismos de ao ainda muito deficiente.
O termo Laser um acrnimo para Light Amplification by emission of
radiation (amplificao da luz pela emisso estimulada da radiao). Embora Albert
Einstein originalmente tenha delineado os princpios subjacentes gerao deste
tipo de luz no incio deste sculo, foi somente em 1960 que Maiman produziu o
primeiro feixe de luz de laser e baseado neste prottipo surgiu vrios aparelhos. As
caractersticas que diferem a luz laser de uma lmpada so: monocromaticidade,
colimao e coerncia (SCHAWLOW,1995).
-
20
A coerncia uma das propriedades da luz laser, como citada acima, mas ao
penetrar no tecido, esta propriedade se perde nos primeiros extratos da pele. Isto
ocorre devido grande variedade de estruturas celulares que compe a pele
(Nomura et al, 1989). Segundo esses autores, apesar da perda da coerncia no
interior dos tecidos, a irradiao ainda absorvida pelas clulas, gerando alteraes
no seu metabolismo tanto em tecidos superficiais como profundos (SVAASAND,
1990).
Os lasers podem ser classificados em dois grandes grupos: os laseres
cirrgicos de alta intensidade (HILT High -Intensity Laser Treatment) e laseres no-
cirrgicos de baixa intensidade (LILT Low Intensity Laser Treatment).
Em geral, quase todas as aplicaes com HILT tomam por base os efeitos
fototrmicos e fotoablativos do laser no tecido, sendo usados para cortar, destruir,
soldar, remover tatuagens, entre outros efeitos. Em contraste, nas dcadas de 60 e
70 os pesquisadores voltaram-se para as aplicaes com LILT e essas se baseiam
nas interaes atrmicas da luz laser com o tecido, produzindo efeitos de
Biomodulao (KARU, 1998; BASFORD,1995).
A terapia com laser de baixa potncia (LBP), incide sobre as reaes
atrmicas da luz com o tecido, ocasionando efeitos fotoqumicos (SCHAFFER et al.,
2000; HONMURA et al.,1993), ou seja, radiaes com baixa densidade de potncia
(DP) 0,01 w/cm2 1 w/cm2 e tambm baixa densidade de energia (DE), de 1
10J/cm2 (SCHINDL et al., 2000). Nesses limites se produz uma pequeno e no
significante aumento de temperatura, o qual no ultrapassa 1 grau Celsius
(KARU,1987).
O Laser de baixa potncia parece agir sobre organelas celulares
(mitocndrias e membranas), gerando aumento da sntese de ATP e modificando o
transporte inico. Dessa forma o laser, em curto prazo, acelera a gliclise e a
oxidao fosforilativa e em longo prazo a transcrio e a replicao do DNA (KARU,
1987).
Acredita-se que a ao do laser de baixa potncia sobre o tecido est
relacionada possibilidade de inibio do aparecimento de fatores quimiotticos nos
estgios iniciais da inflamao; de interferir com o efeito dos mediadores qumicos
induzidos pela inflamao (CAMPANA et al., 1998; CAMPANA et al. ,1999); inibir a
sntese das prostaglandinas (SATTAYUT et al., 1999; BJORDAL et al., 2006) alm
de inibir o esfncter pr-capilar, atravs de mediadores qumicos.
-
21
Estudos adicionais sobre o efeito antiinflamatrio do laser de baixa potncia
ainda se fazem bastante necessrios e seu mecanismo de ao deve ser
investigado a fim de compreender suas aes nos diferentes modelos experimentais
em que vem sendo utilizados.
Campana et al. (1998) quantificaram o nvel de fibrinognio plasmtico (FP)
em modelo de leso tecidual induzida por laparotomia e tratada com LBP e
diclofenaco de sdio. Nesse modelo experimental os resultados mostraram que o
nvel de FP que se encontrava aumentado nos tecidos lesados retornaram a nveis
normais aps o tratamento com LBP sendo semelhante ao tratamento com
diclofenaco de sdio. Esses resultados sugerem que a resposta inflamatria pode
ser normalizada ou reduzida pela ao fotoqumica do LBP, sugerindo uma ao
seletiva da COX-2, visto que a reduo do FP obtida com LBP foi semelhante ao
tratamento farmacolgico.
SATTAYUT et al. (1999), investigaram o efeito do laser As-Ga-Al (820nm)
com densidade de energia de 4J/cm2 e 19J/cm2 na produo de PGE2 em culturas de
clulas estimulada com IL-1 e observaram que a inibio da sntese de PGE2
ocorreu com 19J/cm2, sugerindo ser este o mecanismo analgsico para as dores
msculo - esquelticas.
O uso de lasers na prtica clnica objetivando o efeito antiinflamatrio em
diferentes doenas baseia-se em um nmero j razovel de publicaes de carter
cientfico.
Nos ltimos anos, inmeros estudos em diferentes situaes foram
realizados, fazendo com que a terapia laser j seja considerada como alternativa
teraputica para vrias doenas. (SALATE et al, 2005; FRIGO, 2009; CHOW, 2009;
CRESSONI ET AL, 2010; TUMILTY et al, 2012; ALFREDO et al, 2012; ALVES et al,
2013; BJORDAL et al, 2013; MARCOS et al, 2013; CASALECHI et al, 2013. partir
destes trabalhos, foi possvel entender parte do efeito da Terapia com Laser de
Baixa Potncia na reao inflamatria em cartilagem, na osteoartrite e tendinite, em
ratos e humanos. No entanto, importante ressaltar que pouco se conhece a
respeito do mecanismo de ao dos laseres no processo inflamatrio, onde os
estudos experimentais assumem grande relevncia.
-
22
2 OBJETIVOS
Estudar o efeito do laser de baixa potncia 660nm, 100mW na inflamao
aguda do tendo, investigando alteraes da expresso de enzimas e mediadores
inflamatrios como COX-2, IL-6, IL-10 e TNF-.
-
23
3 MATERIAL E MTODOS
3.1 Animais
Foram utilizados ratos Wistar machos pesando entre 200 e 250g (+/- 90 dias
de vida) com livre acesso a gua e rao, provenientes Biotrio do Instituto de
Cincias Biomdicas da Universidade de So Paulo.
Os animais foram mantidos em ambiente com temperatura controlada e ciclo
claro/escuro de 12 horas.
3.2 Grupos Experimentais
Os animais foram divididos em diferentes grupos conforme o esquema
abaixo:
Figura 3. Esquema dos grupos experimentais.
-
24
- Grupo 1: Controle (C) Tendes de animais que receberam injeo com soluo
salina 0,9% de NaCl (soro fisiolgico estril).
- Grupo 2: Tendinite no tratado (NT): Tendes de animais que receberam injeo
com soluo de colagenase.
- Grupo 3: Diclofenaco (D): Receberam injees de Colagenase e foram tratados
com Diclofenaco de Sdio (2,5mg/kg I.M., Voltaren, Novartis) imediatamente aps
a induo.
- Grupos 4: Irradiado (1J): Receberam injeo de colagenase e os tendes foram
irradiados, na regio da injeo, num nico ponto com Laser em 660nm na energia
de 1J e 100mW.
- Grupos 5: Irradiado (3J): Receberam injeo de colagenase e os tendes foram
irradiados, na regio da injeo, num nico ponto com Laser em 660nm na energia
de 3J e 100mW.
3.3 Induo da tendinite
Os animais foram anestesiados com injeo de cloridrato de ketamina
(90mg/Kg) e cloridrato de Xilazina (10mg/Kg). Depois de anestesiados, os animais
do grupo G2 ao G5 receberam 100 l de injeo transcutnea de colagenase (1
mg/ml; Sigma Chemical Co, Cat. C-6885) na regio posterior da pata direita do
Tendo calcneo. Animais do grupo controle receberam o mesmo volume de
soluo fisiolgica (NaCl 0,9%). A seguir, os animais retornaram para as caixas de
conteno separados em diferentes grupos experimentais. Aps 2 horas da induo
do processo inflamatrio pela injeo de colagenase, os animais foram
eutanasiados. A eutansia foi realizada atravs de overdose injetvel de
anestsico cloridrato de ketamina (180mg/Kg) e cloridrato de Xilazina (20mg/Kg). O
tecido tendneo foi removido para posteriores anlises.
-
25
3.4 Aplicao da Terapia com Laser de Baixa Potncia (LBP)
Os animais receberam o tratamento com laser de baixa potncia 660nm em
100mW de potncia (Thera Lase, DMC), 1 hora aps serem submetidos ao modelo
de inflamao aguda pela injeo de colagenase,
O tempo de Irradiao foi de 10 e 30 segundos, respectivamente para a
energia de 1J e 3J.
A aplicao do laser com um ponto por contato pontual, com dimetro de
0,028 cm.
3.5 Anlises de expresso gnica por RT-PCR
Os tendes removidos foram imediatamente armazenados -80 C para
anlise da expresso gnica dos compostos indicados na tabela abaixo, pela reao
em cadeia da polimerase reversa (PCR) em tempo real. O RNA total das amostras
foi extrado com o reagente Trizol (Gibco BRL, EUA), de acordo com instrues do
fabricante. Aps tratamento com DNAse, a sntese dos cDNAs foi feita pelo mtodo
da transcriptase reversa, empregando a enzima SuperScript (Invitrogen, 2g de RNA
total), na presena de mistura de primers randmicos e oligo dT. A anlise das
amostras em tempo real obedeceu um ciclo de desnaturao inicial (10min 95 C)
e quarenta ciclos de amplificao (30 seg de desnaturao 95 C e 1min de
anelamento e extenso 60 C).
As seqncias dos primers utilizados esto representadas na figura 4,
conforme Wang et al. (2004). Os resultados da expresso gnica foram
interpretados usando-se a frmula 2- Ct (Ct = nmero de ciclos necessrios para
atingir o limiar de fluorescncia acima do valor de fundo - background) que relaciona
a expresso do gene de interesse comparado quela do gene controle B-actina.
PRIMER SEQUNCIA
-ACTINA FOWARD: AAGATTTGGCACCACACTTTCTACA
REVERSE: CGGTGAGCAGCACAGGGT
COX-2 FOWARD: AGATCAGAAGCGAGGACCTG
REVERSE: CCATCCTGGAAAAGTCGAAG
-
26
IL-6
FOWARD: TGACCCAACCACAAATGC
REVERSE: CGAGCTCTGAAACAAAGGAT
IL-10 FOWARD: CATGGGTGTTGGGAAGAGAA
REVERSE: GCTTTCGAGACTGGAAGTGG
TNF- FOWARD: GGTGATCGGTCCCAACAAGGA
REVERSE: CACGCTGGCTCAGCCACT
Figura 4: Seqncia de Primers para anlise da expresso de mRNA, pela tcnica
de RT-PCR em tempo real.
3.6 Anlise estatstica
Os dados foram descritos em valores mdios seguidos dos respectivos
desvios padro. Todos os resultados foram submetidos anlise estatstica atravs
do teste de ANOVA com post-hoc de Tukey-Kramer para mltiplas comparaes.
Valores de p
-
27
4 RESULTADOS
4.1 Artigo submetido para publicao.
-
28
The Low Level Laser Therapy (LLLT) Operating in 660 nm Reduce Gene
Expression of Inflammatory Mediators in the Experimental Model of
Collagenase-induced Rat Tendinitis
Torres-Silva, R1; Lopes-Martins R.A.B.2, Bjordal J.M.3, Frigo L4, Rahouadj R.5, Arnold
G.6, Leal-Junior, E.C.P.1, Magdalou J.7, Pallota R.2, Marcos, R.L.1
1 - University of Nove de Julho, Biophotonics Applied to Health Sciences, So Paulo
01504-001, Brazil
2 - University of So Paulo (USP), Laboratory of Pharmacology and Experimental
Therapeutics, Institute of Biomedical Sciences (ICB), So Paulo 05508-900, Brazil
3 University of Bergen, Department of Global Health, Norway
4 Universidade Cruzeiro do Sul, Departamento de Cincias da Sade So Paulo
5 - Universit de Lorraine (UL), Laboratoire d'Energtique et de Mcanique
Thorique et Applique (LEMTA), UMR 7563 CNRS, F-54504 Vanduvre-ls-
Nancy, France
6 - Universit de Haute Alsace (UHA), Laboratoire Physique et Mcanique Textiles
(LPMT), F-68093 Mulhouse, France e Universit de Strasbourg (UdS), ICube, UMR
7357 CNRS, F-67411 Illkirch, France
7- Universit de Lorraine (UL), Ingnierie Molculaire, Physiopathologie Articulaire
(IMoPA), UMR 7365 CNRS, Biople, F-54505 Vanduvre-ls-Nancy, France
Correspondence Author
Rodrigo Labat Marcos
Programa de Ps-Graduao em Biofotnica Aplicada das Cincias da Sade
Universidade Nove de Julho
Rua Vergueiro 239-245
Email: [email protected]
ABSTRACT
-
29
Tendinopathy is a common disease with a variety of treatments and therapies. Laser
therapy appears as an alternative treatment. Here we investigate the effects of laser
irradiation in an experimental model of tendinitis induced by collagenase injection on
rat calcaneous tendon, verifying its action in important inflammatory markers.
Methods: Male Wistar rats were used and divided in five groups: Control Saline (C),
non-treated tendinitis (NT) and tendinitis treated with sodium diclofenac (D) or Laser
(1J) and (3J). The tendinitis was induced by collagenase (100g/tendon) on the
Achilles tendon which was removed for analyzes. The gene expression for COX-2;
TNF-; IL-6; IL-10; MMP-3, 9, 13 (RT-PCR) was measured. Results and discussion:
The Laser irradiation (660nm, 100mW, 3J) used in the treatment of the tendinitis
induced by collagenase in Achilles tendon in rats, was effective in the reduction of
important inflammatory markers, becoming a promising tool for the treatment of
tendon diseases.
Keywords: Tendinitis. LLLT, Laser therapy, Tendinitis, inflammation, tendon, rats.
INTRODUCTION
Tendinopathies are changes in the tendon health, which are frequent and
difficult to treat, because of the high impact on quality of life of individuals that require
frequent medical care even in simple cases, being a therapeutic challenge in chronic
situations [1,2]. This fact results in a significant increase of resources expended by
the employer relating to the sick leave and the need for relocation and qualifying new
employees [3].
The high incidence tendon diseases make it a social problem which medical
therapies and interventions for rehabilitation are limited [4]. Therefore, its prevention,
the identification of associated causes and also the promotion of safe return for
working activities became the subject of studies in public health [5].
Tendons are composed by tenocytes which are responsible for the synthesis
of specific extracellular matrix and collagen, arranged in hierarchical levels, forming a
complex anatomical structure transmitting the force generated from the muscle to the
bone, making possible the joint movement [6,7].
The tendon tissue is covered by epitendon which provides a poor blood supply
when compared to other tissues. This may compromise its repair process after a
-
30
lesion due to the difficulty in removing metabolites or even the low bioavailability of
drugs commonly used in conventional therapy [8,9].
The most abundant collagen found in tendon tissue is the type I collagen
followed by type II and III. These proteins are organized in long fibrils conferring
resistance to the tissue. A balance between production and degradation of collagen
regulates the tissue integrity. Thus, changes in this balance can interfere directly in
the mechanical properties of the tendon [10,11,12].
There are a number of etiologic factors that can be attributed as tendinitis
inductors. The most common cause is the overexertion of tendons extension
promoting distension of collagen fibers leading to partial ruptures, developing an
intense and painful inflammatory reaction [13]. In this context, the most common
treatment of the inflammatory reaction in tendon tissue are the NSAIDs. The use of
NSAIDs still controversial in tendon diseases. However, an alternative to way to
reduce the inflammatory process in tendon tissue could be controlling the wound
healing process by modulating the inflammation and levels of anti- and pro-
inflammatory cytokines involved in tissue repair [14]. The cyclooxygenase II, for
example, is an integral enzyme that can be induced during this inflammatory process,
influencing the formation of important inflammatory cytokines, including the
interleukins (IL-1, IL-6, IL-10) and tumor necrosis factor (TNF - ). These cytokines
have a major role in the modulation of tendon inflammation [15]. IL-6, for example, is
a cytokine with a central role in inflammation after injurious processes [16]. In acute
inflammation of tendon is commonly observed a significant increase of both
granulocytes and neutrophil in synovial sheath, usually activated by increasing IL-1
and IL-6. The presence of these cytokines is directly related to progression of
tendinitis in a painful process after tendon rupture [17,18,19].
In contrast, IL-10 is known for its anti-inflammatory activity. IL-10 inhibits both
the expression of the interleukins (IL-6; IL-8) and the migration of inflammatory cells
at the lesion site including macrophages and monocytes [14,20].
TNF- is a pleitropic cytokine related to cell survival and proliferation but also
to cell death in the apoptotic process expressed by tenocytes in inflammatory
conditions [21]. TNF- may be the key cytokine in the origin of several
musculoskeletal diseases such as Rheumatoid Arthritis, Osteoarthritis and tendinitis
[19], however, its role in tendon disease has not been well determined. It is known
-
31
that its expression is increased in tendons in traumatic situations or after surgery,
wherein there is a harmful process [21,22].
Thus, treatment of tendinitis aims to reduce inflammation, because its
persistence promotes alterations in collagen and an increase in specific activity of
certain enzymes fibers, extending the inflammatory and proliferative phases, favoring
the excess deposition of scar tissue, altering some characteristics as strength
reduction compared to the original tendon [23,24].
The most common treatment is still conservative and recommended by most
authors as the initial strategy. The NSAIDs are the drugs most commonly used as
part of initial treatment, especially in reducing pain [25,26]. However there are a few
scientific evidences to support its use [7,8,13,26,27].
In recent years, several studies have been performed in different situations,
leading laser therapy to be considered as a promising alternative therapy for a
numerous diseases, acting in the early stages of inflammation by inhibiting the onset
chemotactic factors through altering the presence of pro- and anti-inflammatory
mediators, modulating the inflammation [28,29,30,31].
From these studies, it was possible to understand part of the effect of therapy
using a Low Level Laser in inflammatory reaction of cartilage in osteoarthritis and
tendinitis of both rats and humans [9,24,26,28,32,33,34]
However, it is important to note that very few studies addresses the molecular
effects in gene expression over the lasers action in the inflammatory process,
specially in tendons.
This work aims to study the effect of low level laser 660nm, 100mW in acute
inflammation of tendon, investigating changes in the expression of enzymes and
inflammatory mediators such as COX-2, IL-6, IL-10 and TNF-.
MATERIALS AND METHODS:
All of the experimental procedures were submitted and approved by the
Ethical Committee of the University of Sao Paulo. Thirty male Wistar rats weighing
250 + 20 g were randomly divided and housed five per cage before the experimental
procedure. Food and water were provided ad libitum throughout the experiment. Rats
were anesthetized with xylazine and ketamine injection (90mg/Kg and 10mg/Kg,
respectively) before collagenase injection. All the necessary preoperative procedures
-
32
were performed in order to prevent discomfort and to avoid any infection. Skin was
surgically prepared and collagenase was injected in right leg (100 g/tendon)
percutaneously into the Achilles tendon, approximately 2 mm proximal to the
osteotendinous junction under anesthesia using a 30 G needle. The same volume of
PBS without collagenase was injected using the same procedure in a control group
(C). Thirty minutes after collagenase injection, one group (called D) was treated
using sodium diclofenac (Voltaren injectable Novartis 2.5 mg/kg) injected in the
gluteus muscle. Two other groups were treated by laser 1 h after collagenase
injection. A single LLLT was performed with an infrared laser unit (Thera Lase, DMC,
Brazil). The laser unit emitted a continuous optical radiation under a wavelength of
660 nm, with a power of 100 mW in a mean spot size area of 0.028 Cm2. Laser
irradiation was performed in skin contact at the site of collagenase injection with
doses of 1 J and 3 J, corresponding to irradiation times of 10 s and 30 s,
respectively. The laser energy doses were chosen according to previous studies [29].
The two groups were called L1J and L3J, for 1 and 3 J respectively. The last group
(called TEN) was not subjected to any treatment of tendinitis. Six animals of each
group were sacrificed with an overdose of xylazine and ketamine injection (270mg/Kg
and 30mg/Kg, respectively), 2 h after tendinitis induction for biochemical analysis.
After the removal of skin and connective tissue, Achilles tendons were dissected,
frozen in liquid nitrogen, and stored at 80 C for further analysis.
- RNA isolation and Real Time PCR analysis: At the Achilles tendons were dissected,
frozen in liquid nitrogen, and stored at 80C. Total RNA was isolated in the Trizol
reagent, according to the manufacturers instruction. DNase I was employed to digest
DNA to obtain RNA purification and the integrity of RNA was verified by agarose gel
electrophoresis. Total RNA (2 g) was used for first-strand cDNA synthesis (reverse
transcriptase [RT]) using SuperScript II. In addition, RNaseOUT was also added to
protect the RNA during this process. Three pooled RNA aliquots were routinely sham
reverse transcribed (i.e. RT omitted) to insure the absence of DNA contaminants.
Diluted RT samples (1:10) were submitted to real-time PCR amplification using
Platinum Sybr QPCR Supermix-UDG and specific oligonucleotides for COX-2
(forward: AGATCAGAAGCGAGGACCTG; reverse: CCATCCTGGAAAAGTCGAAG),
IL-6 (forward: TGACCCAACCACAAATGC; reverse: CGAGCTCTGAAACAAAGGAT),
IL-10 (forward: CATGGGTGTTGGGAAGAGAA; reverse:
GCTTTCGAGACTGGAAGTGG) and TNF- (forward:
-
33
GGTGATCGGTCCCAACAAGGA; reverse: CACGCTGGCTCAGCCACT). Beta-actin
was used as an internal control (forward: AAGATTTGGCACCACACTTTCTACA;
reverse: CGGTGAGCAGCACAGGGT). The conditions for PCR were as follows:
50C2 min; 95C2 min, followed by 30 cycles of 95C15 s; 60C1 min and
72C15 s. Ct values were recorded for each gene, and the results of genes of
interest were normalized to results obtained with the internal control gene. ddCT
were calculated and the results are expressed as fold increase. All oligonucleotides
and reagents utilized in this protocol were purchased from Invitrogen Co.
- Statistical analysis: Data are expressed as mean and standard error () of the
mean (SEM) and were analyzed using Student's t-test to evaluate the statistical
significance of the null hypothesis vs CTL and/or TEN. All data were statistically
evaluated by analysis of variance (ANOVA), followed by the Tukey test. Values with
P < 0.05 were considered to be statistically significant.
RESULTS
The figure 01 shows in the Panel A the COX-2 gene expression, 2 hours after
induction of tendinitis . We can observe that the tendinitis ( NT ) as well as the other
3 groups presented a significant increase in COX-2 gene expression when compared
to the control group after tendinitis induction (P < 0.001). However, none of the
groups were significantly inhibited by diclofenac or Laser treatments.
In Panel B we can observe the IL6 gene expression at 2 hours after induction
of tendinitis. We could observe that there was an increase in gene expression of IL-6
in tendinitis untreated group (NT), (p
-
34
group. The group treated with sodium diclofenac (D) and the irradiated group (1J)
showed increased expression of the same gene, when compared with (NT).
The figure 01 panel D shows the TNF- gene expression, two hours after
tendinitis induction. We can observe that the (NT) group showed a significant
increase in TNF- gene expression when compared to the control group (C). It was
also observed that both groups diclofenac and Laser 1J failed to reduce the
expression of TNF-. Only the group treated with laser irradiation at the energy of 3J
was able to significantly reduce the TNF- expression when compared to NT group
(p
-
35
DISCUSSION
Low level laser therapy has been studied since the 60s being considered as a
therapeutic alternative with good perspectives for use specially in musculo-skeletal
and inflammatory disorders. In our study, we investigated the effects of low level
laser therapy on important inflammatory mediators, involved in acute inflammation of
the tendon.
Recent studies have focused on the discovery of new therapies able to
promote cytokines inhibition, such as IL-1, TNF- as well as metalloproteinases in
tendon diseases. Thus, tendinitis appears as the target of concern, both in the sports
medicine and labor.
Here we employed the nonsteroidal anti-inflammatory drug Sodium Diclofenac
as a pharmacological reference therapy to be compared to Laser irradiation in tendon
inflammation induced by collagenase. The experimental model used was the
tendinitis induced in Achilles tendon of rats by collagenase injection. This
experimental model of tendon inflammation is well known in the study of tendinitis in
which edema and acute destruction of the extracellular matrix are similar to those
found in natural tendon injury, being considered an excellent model that allows to
investigate molecular and histological changes [35].
The development of inflammation during the injury is a beneficial event that
aims to restore tissue homeostasis. In this process the formation of chemical
mediators with pro-inflammatory or anti-inflammatory action are produced from
cyclooxygenase pathways that also increase in inflammatory processes.
In tendinitis model, due to low vascularity or to transitions between tendinitis
and tendinosis periods, this tissue has not always inflammatory infiltrate. However,
COX-2 increase was observed in both cases which indicates in some extent, a tissue
degeneration as a result of the inflammatory process [36].
Previous study from our group was the first to determine the time course of
COX-2 gene expression, and the peak time after 2 hours of tendinitis induction [29].
From these data, we choose the period of 2 hours, the same used previously, to
-
36
study the effects of Laser irradiation, this time operating in 660nm, in the
experimental model of collagenase-induced rat tendinitis.
In the present study it was observed that COX-2 gene expression increased in
non-treated group (NT). In the same way, non-treated group presented significant
increases in the other pro-inflammatory citokines, IL-6 and TNF-.
The treated group with sodium diclofenac (D) also presented increase in COX-
2 and TNF- expression, similar to NT group and more IL-6 expression compare to
NT. On the other hand, the irradiated groups, especially 3J showed a slight decrease
in COX-2, IL-6 and TNF-, compared to NT.
Cyclooxygenase-2 increased can directly interfere in the formation of specific
inflammatory mediators, such as interleukins and tumor necrosis factor, by changing
the tissue repair process. TNF- is another factor that can modulate this process.
Their levels are generally increased in the presence of musculoskeletal diseases like
tendinitis and could be important in degenerative process of the tissue by inducing an
increase in inflammatory cells [19]. Thus, the increase of TNF- gene expression
after tendinitis induced may represent an increase in the inflammatory process
triggering other important inflammatory mediators, such as matrix metalloproteinases
[37].
Changes in tendon repair can lead to scar formation with different
characteristics of the original tissue. The scar initially provides the physical continuity
of the tissue, but the proliferation of adjacent tissue can be undesirable and hinder
the sliding mechanism tendon [14]. One way to reduce these changes would be
control the healing process, modulating the inflammation by cytokines levels,
involved in the repair, such as IL-6 , IL-10 and TNF- , observed in this work and
associated with disease progression. IL-10 for instance, sharing functional activities
such as suppression of proinflammatory events by inhibition of inflammatory
cytokines such as IL-1, IL-6, TNF- and also inhibit some MMPs that could hamper
tissue repair [15].
In this work, the expression of pro-inflammatory cytokines (IL-6 and TNF-)
were increased not only in the NT group, but also in diclofenac group (D) and even in
the irradiated group (1J). Only the irradiated group (3J) was able to reduce
-
37
expression of these pro-inflammatory cytokines. On the other hand, the expression of
antiinflammatory cytokines (IL-10) was increased in all groups where tendinitis was
induced, probably a natural action of the body to reduce inflammation, but in the
treated groups D, 1J and 3J, this increase was even higher.
Thus, the relationship between the amounts of IL-6 and IL-10 show a positive
anti-inflammatory response, mainly in the irradiated group 3J. These results together
suggest that in the non-treated group (NT) the inflammation remained high and
probably the highest level of tissue injury, on account of increase of TNF- to be
associated with increased of matrix metalloproteinase enzymes.
Previous results demonstrated that treatment with sodium diclofenac reduces
prostaglandin E2 synthesis and NK1 neuropeptides expression, receptors likely to
pain. However, our results showed that sodium diclofenac treatment failed to reduce
the expression of citokines (IL6 and TNF-). Diclofenac treatment failure may be
related to dose and administration in rats or specific tendon characteristics that is
poorly vascularized.
The sum of these factors is a strong indication that low level laser therapy in
660nm - 100mW and 3 Joules can be effective in reducing the acute inflammatory
process induced by collagenase in Achilles tendons of rats. However, further analysis
are needed to determine this laser modulation operating in 660 nm on matrix
metalloproteinases in tendon tissues during the inflammatory process. The
investigation of biochemical factors as protein expression of inflammatory mediators,
enzyme dosage and morphological and functional factors such as histological and
mechanical properties analyzes are important to understanding of this inflammatory
event and the action mechanism involved at cellular and structural changes in
tendinitis.
-
38
CONCLUSION
We can conclude that the model of tendinitis by collagenase-induced in rats
increased the expression of important inflammatory mediators. Treatment with
sodium diclofenac was not effective in reducing inflammatory mediators. The low
level laser therapy (660nm - 100mW) at 3 Joules of energy was effective in reducing
the inflammation in this model.
REFERENCES
1 BARROS M, CSAR CLG, CARANDINA L, TORRE GD. Desigualdades sociais na
prevalncia das doenas crnicas no Brasil, PNAD 2003. Cienc Sade Coletiva. 11:
911-926. 2006.
2 AITTOMAKI A, LAHELMA E, RAHKONEN O, LEINO-ARJAS AMN, OLSEN J. The
contribution of musculoskeletal disorders and physical workload to socioeconomic
inequalities in health. Eur J Public Health 2006; 2: 145-150.
3 NGUYEN TH, RANDOLPH DC. Nonspecific low back pain and return to work. Am
Fam Physician. 10: 1497-502. 2007.
4 Kjaer M, Langberg H, Bojsen-Mller J, Koskinen SO, Mackey A, Heinemeier
K,Holm L, Skovgaard D, Dssing S, Hansen M,Hansen P, Haraldsson B, Care
I,Magnusson SP. Novel methods for tendon investigations. Disabil
Rehabil.2008;30(20-22):1514-22.
5 BARBE MF, BARR AE. Inflammation and the pathophysiology of work-related
musculoskeletal disorders. Brain Behav Immun. 5: 423-429. 2006.
6 JZSA, L.; KANNUS, P. Histopathological findings in spontaneous tendon
ruptures. Scand. J. Med. Sci. Sports, v. 7, n. 2, p. 113-118, 1997.
7 KHAN, K. M.; COOK, J. L.; BONAR, F.; HARCOUT, P.; ASTROM, M. (1999).
Hystopathology of common tendinopathies. Update and implications for clinical
management. Sports Med., v. 27, n. 6, p. 393-408, 1999.
-
39
8 KVIST, M.; JOZSA, L.; JARVINEN, M. Fine structural alterations in chronic Achilles
paratenonitis in athletes. Path. Res. Pract., v. 180, p. 416-423, 1985.
9 MARCOS RL, ARNOLD G, MAGNENET V, RAHOUADJ R, MAGDALOU J,
LOPES-MARTINS RA. Biomechanical and biochemical protective effect of low-level
laser therapy for Achilles tendinitis. J Mech Behav Biomed Mater. 9; 29C, 272-285.
2013.
10 HULMES DJ. Building collagen molecules, fibrils and suprafibrillar structures.
Struct J Biol. 137. (1-2), 2-10. 2002.
11 MOALI C, HULMES DJS. Extracellular Matrix: Pathobiology and Signaling.In:
Karamanos M, editor. Roles and Regulation of BMP-1/Tolloid-Like Proteinases:
Collagen/Matrix Assembly, Growth Factor Activation and Beyond. Berlin: De Gruyter;
2012.
12 WIDMER, C, et al Molecular basis for the action of the collagen-specific
chaperone Hsp47/SERPINH1 and its structure-specific client recognition. Proc Natl
Acad Sci USA. 109 (33):1324313247. 2012.
13 ALFREDSON, H.; LORENTZON, R. Chronic Achilles tendinosis.
Recommendations for treatment and prevention. Sports Med., v. 29, n. 2, p. 135-146,
2000.
14 RICCHETTI, E. T.; REDDY, S. C.; ANSORGE, H. L.; ZGONIS, M. H.; VAN
KLEUNEN, J. P.; LIECHTY, K. W.; SOSLOWSKY, L. J.; BEREDJIKLIAN, P. K. Effect
of interleukin-10 overexpression on the properties of healing tendon in a murine
patellar tendon model. J. Hand Surg. Eur., v. 33A, p. 1843-1852, 2008.
15 LIN, T. W.; CARDENAS, L.; GLASER, D. L.; SOSLOWSKY, L. J. Tendon healing
in interleukin-4 and interleukin-6 knockout mice. J. Biomech., v. 39, p. 61-69, 2006.
16 SKUTEK M, VAN GRIENSVEN M, ZEICHEN J et al. Cyclic mechanical stretching
enhances secretion of interleukin 6 in human tendon fibroblasts. Knee Surg Sports
Traumatol Arthrosc. 9:322-6. 2001.
http://www.ncbi.nlm.nih.gov/pubmed?term=Marcos%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=24126100http://www.ncbi.nlm.nih.gov/pubmed?term=Arnold%20G%5BAuthor%5D&cauthor=true&cauthor_uid=24126100http://www.ncbi.nlm.nih.gov/pubmed?term=Magnenet%20V%5BAuthor%5D&cauthor=true&cauthor_uid=24126100http://www.ncbi.nlm.nih.gov/pubmed?term=Rahouadj%20R%5BAuthor%5D&cauthor=true&cauthor_uid=24126100http://www.ncbi.nlm.nih.gov/pubmed?term=Magdalou%20J%5BAuthor%5D&cauthor=true&cauthor_uid=24126100http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes-Martins%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=24126100http://www.ncbi.nlm.nih.gov/pubmed/24126100
-
40
17 FU SC, WANG W, PAU HM ET AL. Increased expression of transforming growth
factor-beta1 in patellar tendinosis. Clin Orthop Relat Res. 400:174-83. 2002.
18 NAKAMA K, GOTOH M, YAMADA T et al. Interleukin-6-induced activation of
signal transducer and activator of transcription-3 in ruptured rotator cuff tendon.
19 HAYER, S.; REDLICH, K.; KORB, A.; HERMANN, S.; SMOLEN, J.; SCHETT, G.
Tenosynovitis and osteoclast formation as the initial preclinical changes in a murine
model of inflammatory arthritis. Arthritis Rheum., v. 56, n.1, p. 79-88, 2007.
20 ALAM, R.; KUMAR, D.; ANDERSON-WALTERS, D.; FORSYTHE, P. A.
Macrophage inflammatory protein-1 alpha and monocyte chemoattractant peptide-1
elicit immediate and late cutaneous reactions and activate murine mast cells in vivo.
J. Immunol., v. 2, p. 1298-1303, 1994.
21 HOSAKA, Y.; KIRISAWA, R.; UEDA, H.; YAMAGUCHI, M.; TAKEHANA, K.
Differences in tumor necrosis factor (TNF)alpha and TNF receptor-1-mediated
intracellular signaling factors in normal, inflamed and scar-formed horse tendons. J.
Vet. Med. Sci., v. 67, n. 10, p. 985-991, 2005.
22 AKESEN, B.; DEMIRAG, B.; BUDAK, F. Evaluation of intra-articular collagenase,
TIMP-1, and TNF-lpha levels before and after anterior cruciate ligament
reconstruction. Acta Orthop. Traumatol. Turc., v. 43, n. 3, p. 214-218, 2009.
23 FERNANDES, M. A. L.; ALVES, G. E. S.; SOUZA, J. C. A. Efeito do ultra-som
teraputico em tendinite experimental de eqinos: estudo clnico, ultra-sonogrfico e
histopatolgico de dois protocolos. Arq. B. Med. Vet. Zoot., v. 55, n. 1, p. 27-34,
2003.
24 ALVES AC, ALBERTINI R, DOS SANTOS SA, LEAL-JUNIOR EC, SANTANA E,
SERRA AJ, SILVA JA JR, DE CARVALHO PD. Effect of low-level laser therapy on
metalloproteinase MMP-2 and MMP-9 production and percentage of collagen types I
and III in a papain cartilage injury model. Lasers Med Sci. 29. 2013.
25 ALFREDSON, H.; OHBERG, L.; FORSGREN, S. Is vasculo-neural ingrowth the
cause of pain in chronic Achilles tendinosis? An investigation using ultrasonography
http://www.ncbi.nlm.nih.gov/pubmed?term=Alves%20AC%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Albertini%20R%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Dos%20Santos%20SA%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Leal-Junior%20EC%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Santana%20E%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Serra%20AJ%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Silva%20JA%20Jr%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Carvalho%20PD%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed/23990219
-
41
and colour Doppler, immunohistochemistry, and diagnostic injections. Knee Surg.
Sports Traumatol. Arthrosc., v. 11, n. 5, p. 334-338, 2003.
26 ANDRES, B. M.; MURRELL, G. A. Treatment of tendinopathy: what works, what
does not, and what is on the horizon. Clin. Orthop. Relat. Res., v. 466, n. 7, p. 1539-
1554, 2008.
27 BJORDAL, J. M.; KLOVNING, A.; LOPES-MARTINS, R. A.; ROLAND, P. D.;
JOENSEN, J.; SLRDAL, L. Overviews and systematic reviews on low back pain.
Ann. Intern. Med., v. 10 n. 148, p. 789-790, 2008.
28 BJORDAL JM, LOPES-MARTINS RA. Lack of adherence to the laser dosage
recommendations from the World Association for Laser Therapy in Achilles study.
Arch Phys Med Rehabil. 94(2), 408. 2013.
29 MARCOS RL, LEAL JUNIOR EC, et al. Infrared (810 nm) low-level laser therapy
in rat achilles tendinitis: a consistent alternative to drugs. Photochem Photobiol.
87(6):1447-52. 2011.
30 ALFREDO PP, BJORDAL JM, DREYER SH, MENESES SR, ZAGUETTI G,
OVANESSIAN V, FUKUDA TY, JUNIOR WS, LOPES MARTINS R, CASAROTTO
RA, MARQUES AP. Efficacy of low level laser therapy associated with exercises in
knee osteoarthritis: a randomized double-blind study. Clin Rehabil. 26(6), 523-33.
2012.
31 DE ALMEIDA P, TOMAZONI SS, FRIGO L, DE CARVALHO PD, VANIN AA,
SANTOS LA, ALBUQUERQUE-PONTES GM, DE MARCHI T, TAIROVA O,
MARCOS RL, LOPES-MARTINS RA, LEAL-JUNIOR EC. What is the best treatment
to decrease pro-inflammatory cytokine release in acute skeletal muscle injury
induced by trauma in rats: low-level laser therapy, diclofenac, or cryotherapy? Lasers
Med Sci. 30. 2013
32 FRIGO, L.; LUPPI, J. S.; FAVERO, G. M.; PENNA, S. C.; BJORDAL, J. M.;
BENSADOUN, R. J.; LOPES-MARTINS, R. A. The effect of low-level laser irradiation
(In-Ga-Al-AsP - 660 nm) on melanoma in vitro and in vivo. BMC Cancer, v. 20, n. 9,
p. 404, 2009.
http://www.ncbi.nlm.nih.gov/pubmed?term=Bjordal%20JM%5BAuthor%5D&cauthor=true&cauthor_uid=23351679http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes-Martins%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=23351679http://www.ncbi.nlm.nih.gov/pubmed/23351679http://www.ncbi.nlm.nih.gov/pubmed?term=Marcos%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=21910734http://www.ncbi.nlm.nih.gov/pubmed?term=Leal%20Junior%20EC%5BAuthor%5D&cauthor=true&cauthor_uid=21910734http://www.ncbi.nlm.nih.gov/pubmed/21910734http://www.ncbi.nlm.nih.gov/pubmed?term=Alfredo%20PP%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Bjordal%20JM%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Dreyer%20SH%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Meneses%20SR%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Zaguetti%20G%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Ovanessian%20V%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Fukuda%20TY%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Junior%20WS%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes%20Martins%20R%C3%81%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Casarotto%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Casarotto%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Marques%20AP%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed/22169831http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Almeida%20P%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Tomazoni%20SS%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Frigo%20L%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Carvalho%20PD%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Vanin%20AA%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Santos%20LA%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Albuquerque-Pontes%20GM%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=De%20Marchi%20T%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Tairova%20O%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Marcos%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes-Martins%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed?term=Leal-Junior%20EC%5BAuthor%5D&cauthor=true&cauthor_uid=23812849http://www.ncbi.nlm.nih.gov/pubmed/23812849http://www.ncbi.nlm.nih.gov/pubmed/23812849
-
42
33 CHOW, R. T.; JOHNSON, M. I.; LOPES-MARTINS, R. A.; BJORDAL, J. M.
Efficacy of low-level laser therapy in the management of neck pain: a systematic
review and meta-analysis of randomised placebo or active-treatment controlled trials.
Lancet, v. 374, n. 9705, p. 1897-1908, 2009.
34 CASALECHI HL, DE FARIAS MARQUES AC, DA SILVA EA, AIMBIRE F,
MARCOS RL, LOPES-MARTINS RA, DE CARVALHO PD, ALBERTINI R. Analysis
of the effect of phototherapy in model with traumatic Achilles tendon injury in rats.
Lasers Med Sci. Nov 2. 2013.
35 WARDEN, S. J. Animal models for the study of tendinopathy. Br. J. Sports Med.,
v.41, n.4, p. 232-240, 2007.
36 QUEIROZ-JUNIOR, C. M.; PACHECO, C. M. F.; MALTOS, K. L. M.; CALIARI, M.
V.; DUARTE, I. D. G; FRANCISCHI, J. N. Role of systemic and local administration
of selective inhibitors of cyclo-oxygenase 1 and 2 in an experimental model of
periodontal disease in rats. J. Periodontal Res., v. 44, n. 2, p. 153-160, 2009.
37 DEMOS, M.; JOOSTEN, L. A.; OPPERS-WALGREEN, B.; VAN SCHIE, J. T.;
JAHR, H.; VAN OSCH, G. J.; VERHAAR, J. A. Tendon degeneration is not mediated
by regulation of Toll-like receptors 2 and 4 in human tenocytes. J. Orthop. Res., v. 27
, p. 1043-1047, 2009.
http://www.ncbi.nlm.nih.gov/pubmed?term=Casalechi%20HL%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Farias%20Marques%20AC%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=da%20Silva%20EA%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Aimbire%20F%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Marcos%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes-Martins%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Carvalho%20PD%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Albertini%20R%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed/24186775
-
43
5 CONSIDERAES FINAIS
O modelo de tendinite induzida por colagenase em ratos aumentou a
expresso de importantes mediadores inflamatrios relacionados tambm com a
degradao de colgeno. O tratamento com diclofenaco de sdio no foi eficaz na
reduo de mediadores inflamatrios. O laser de baixa potncia (660nm 110mW)
na energia de 3 Joules foi eficaz na reduo do processo inflamatrio neste modelo
de tendinite.
Figura 5: Tabela dos resultados; os valores do grupo NT foram comparados com o
grupo C, e os grupos tratados com D, 1J e 3J, com valores comparados com o grupo
NT.
-
44
6 REFERNCIAS
ALFREDO PP, BJORDAL JM, DREYER SH, MENESES SR, ZAGUETTI G,
OVANESSIAN V, FUKUDA TY, JUNIOR WS, LOPES MARTINS R, CASAROTTO
RA, MARQUES AP. Efficacy of low level laser therapy associated with exercises in
knee osteoarthritis: a randomized double-blind study. Clin Rehabil. 26(6), 523-33.
2012.
ALFREDSON, H.; LORENTZON, R. Chronic Achilles tendinosis. Recommendations
for treatment and prevention. Sports Med., v. 29, n. 2, p. 135-146, 2000.
ALFREDSON, H.; OHBERG, L.; FORSGREN, S. Is vasculo-neural ingrowth the
cause of pain in chronic Achilles tendinosis? An investigation using ultrasonography
and colour Doppler, immunohistochemistry, and diagnostic injections. Knee Surg.
Sports Traumatol. Arthrosc., v. 11, n. 5, p. 334-338, 2003.
ALVES AC, ALBERTINI R, DOS SANTOS SA, LEAL-JUNIOR EC, SANTANA E,
SERRA AJ, SILVA JA JR, DE CARVALHO PD. Effect of low-level laser therapy on
metalloproteinase MMP-2 and MMP-9 production and percentage of collagen types I
and III in a papain cartilage injury model. Lasers Med Sci. 29. 2013.
ALAM, R.; KUMAR, D.; ANDERSON-WALTERS, D.; FORSYTHE, P. A. Macrophage
inflammatory protein-1 alpha and monocyte chemoattractant peptide-1 elicit
immediate and late cutaneous reactions and activate murine mast cells in vivo. J.
Immunol., v. 2, p. 1298-1303, 1994.
ANDRES, B. M.; MURRELL, G. A. Treatment of tendinopathy: what works, what
does not, and what is on the horizon. Clin. Orthop. Relat. Res., v. 466, n. 7, p. 1539-
1554, 2008.
AITTOMAKI A, LAHELMA E, RAHKONEN O, LEINO-ARJAS AMN, OLSEN J. The
contribution of musculoskeletal disorders and physical workload to socioeconomic
inequalities in health. Eur J Public Health 2006; 2: 145-150.
AKESEN, B.; DEMIRAG, B.; BUDAK, F. Evaluation of intra-articular collagenase,
TIMP-1, and TNF-lpha levels before and after anterior cruciate ligament
reconstruction. Acta Orthop. Traumatol. Turc., v. 43, n. 3, p. 214-218, 2009.
ARVIDSSON S, ARVIDSSON B, FRIDLUND B, BERGMAN S. Health predicting
factors in a general population over an eight-year pe riod in subjects with and without
chronic musculoskeletal pain. Health Qual Life Outcomes. 6: 98. 2008.
ASTROM, M. On the Nat. and etiology of chronic achilles tendinopathy. Ph. D. Thesis
- Lund University, 1997.
http://www.ncbi.nlm.nih.gov/pubmed?term=Alfredo%20PP%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Bjordal%20JM%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Dreyer%20SH%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Meneses%20SR%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Zaguetti%20G%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Ovanessian%20V%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Fukuda%20TY%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Junior%20WS%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes%20Martins%20R%C3%81%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Casarotto%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Casarotto%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Marques%20AP%5BAuthor%5D&cauthor=true&cauthor_uid=22169831http://www.ncbi.nlm.nih.gov/pubmed/22169831http://www.ncbi.nlm.nih.gov/pubmed?term=Alves%20AC%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Albertini%20R%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Dos%20Santos%20SA%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Leal-Junior%20EC%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Santana%20E%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Serra%20AJ%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=Silva%20JA%20Jr%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Carvalho%20PD%5BAuthor%5D&cauthor=true&cauthor_uid=23990219http://www.ncbi.nlm.nih.gov/pubmed/23990219
-
45
BARBE MF, BARR AE. Inflammation and the pathophysiology of work-related
musculoskeletal disorders. Brain Behav Immun. 5: 423-429. 2006.
BARROS M, CSAR CLG, CARANDINA L, TORRE GD. Desigualdades sociais na
prevalncia das doenas crnicas no Brasil, PNAD 2003. Cienc Sade Coletiva. 11:
911-926. 2006.
BASFORD, J.R. Low intensity laser therapy still not na established clinical tool.
Lasers Surg. Med., v. 16, n. 4, p. 331-342, 1995.
BEREDJIKLIAN PK. Biologic aspects of flexor tendon laceration and repair. J Bone
Joint Surg Am. 85-A(3). 539-50. 2003.
BERNARD B. Musculoskeletal disorders and workplace factors: a critical review of
epidemiologic evidence for work-related musculoskeletal disorders of the neck, upper
extremity and low back. Cincinnati: NIOSH. 573. 1997.
BJORDAL, J. M.; JOHNSON, M. I.; LOPES-MARTINS, R. A.; BOGEN, B.; CHOW,
R.; LJUNGGREN, A. E. Short-term efficacy of physical interventions in osteoarthritic
knee pain. A systematic review and meta-analysis of randomised placebo-controlled
trials. BMC Musculoskelet. Disord., v. 8, n. 22, p. 51, 2007.
BJORDAL, J. M.; KLOVNING, A.; LOPES-MARTINS, R. A.; ROLAND, P. D.;
JOENSEN, J.; SLRDAL, L. Overviews and systematic reviews on low back pain.
Ann. Intern. Med., v. 10 n. 148, p. 789-790, 2008.
BJORDAL JM, LOPES-MARTINS RA. Lack of adherence to the laser dosage
recommendations from the World Association for Laser Therapy in Achilles study.
Arch Phys Med Rehabil. 94(2), 408. 2013.
CAMPANA, V. R.; MOYA, M.; GAVOTTO, A.; SORIANO, F.; JURI, H. O.; SPITALE,
L. S.; SIMES, J. C.; PALMA, J. A. The relative effects of He-Ne laser and meloxicam
on experimentaly induced inflammation Laser Therapy. Lasers Med. Surg., v. 11, n.
2, p. 6-10, 1999.
CAMPANA, V.; MOYA, M.; GAVOTO, A.; JURI, H.; PALMA, J. A. Effects of
diclofenac sodium and HeNe laser irradiation on plasmatic fibrinogen levels in
inflammatory processes. Lasers Med. Surg., v. 16, n. 6, p. 317-320, 1998.
CASALECHI HL, DE FARIAS MARQUES AC, DA SILVA EA, AIMBIRE F, MARCOS
RL, LOPES-MARTINS RA, DE CARVALHO PD, ALBERTINI R. Analysis of the effect
of phototherapy in model with traumatic Achilles tendon injury in rats. Lasers Med
Sci. Nov 2. 2013.
http://www.ncbi.nlm.nih.gov/pubmed?term=Beredjiklian%20PK%5BAuthor%5D&cauthor=true&cauthor_uid=12637445http://www.ncbi.nlm.nih.gov/pubmed/12637445http://www.ncbi.nlm.nih.gov/pubmed/12637445http://www.ncbi.nlm.nih.gov/pubmed?term=Bjordal%20JM%5BAuthor%5D&cauthor=true&cauthor_uid=23351679http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes-Martins%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=23351679http://www.ncbi.nlm.nih.gov/pubmed/23351679http://www.ncbi.nlm.nih.gov/pubmed?term=Casalechi%20HL%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Farias%20Marques%20AC%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=da%20Silva%20EA%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Aimbire%20F%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Marcos%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Marcos%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Lopes-Martins%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Carvalho%20PD%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed?term=Albertini%20R%5BAuthor%5D&cauthor=true&cauthor_uid=24186775http://www.ncbi.nlm.nih.gov/pubmed/24186775http://www.ncbi.nlm.nih.gov/pubmed/24186775
-
46
CHEN, Y. J.; WANG, C. J.; YANG, K. D.; KUO, Y. R.; HUANG, H. C.; HUANG, Y. T.;
SUN, Y. C.; WANG, F. S. Extracorporeal shock waves promote healing of
collagenase-induced Achilles tendinitis and increase TGF-eta1 and IGF-I
expression. J. Orthop. Res., v. 22, p. 854-861, 2004.
CHOW, R. T.; JOHNSON, M. I.; LOPES-MARTINS, R. A.; BJORDAL, J. M. Efficacy
of low-level laser therapy in the management of neck pain: a systematic review and
meta-analysis of randomised placebo or active-treatment controlled trials. Lancet, v.
374, n. 9705, p. 1897-1908, 2009.
COTRAN KUMAR, COLLINS ROBBINS. Pathologic Basis of Disease. Philadelphia:
W.B Saunders Company. 1998.
CRESSONI MD, GIUSTI HH, PIO AC, DE PAIVA CARVALHO RL, ANARUMA CA,
CASAROTTO RA. Effect of GaAlAs laser irradiation on the epiphyseal cartilage of
rats. Photomed Laser Surg. 28(4):527-32. 2010.
DEMOS, M.; JOOSTEN, L. A.; OPPERS-WALGREEN, B.; VAN SCHIE, J. T.; JAHR,
H.; VAN OSCH, G. J.; VERHAAR, J. A. Tendon degeneration is not mediated by
regulation of Toll-like receptors 2 and 4 in human tenocytes. J. Orthop. Res., v. 27 ,
p. 1043-1047, 2009.
ELSAID KA, FLEMING BC, OKSENDAHL HL, MACHAN JT, FADALE PD, HULSTYN
MJ, SHALVOY R, JAY GD. Decreased lubricin concentrations and markers of joint
inflammation in the synovial fluid of patients with anterior cruciate ligament injury.
Arthritis Rheum. 58(6). 1707-15. 2008.
FERNANDES, M. A. L.; ALVES, G. E. S.; SOUZA, J. C. A. Effect of therapeutic
ultrasound on experimental tendinitis in horses: clinical, sonographic and
histopathologic two protocols. Arq. B. Med. Vet. Zoot., v. 55, n. 1, p. 27-34, 2003.
FELSON DT, LAWRENCE RC, DIEPPE PA, HIRSCH R, et al. Osteoarthritis: new
insights. Part 1: the disease and its risk factors. Ann Intern Med. 17;133(8):635-46.
2000.
FRIGO, L.; LUPPI, J. S.; FAVERO, G. M.; PENNA, S. C.; BJORDAL, J. M.;
BENSADOUN, R. J.; LOPES-MARTINS, R. A. The effect of low-level laser irradiation
(In-Ga-Al-AsP - 660 nm) on melanoma in vitro and in vivo. BMC Cancer, v. 20, n. 9,
p. 404, 2009.
FU SC, WANG W, PAU HM ET AL. Increased expression of transforming growth
factor-beta1 in patellar tendinosis. Clin Orthop Relat Res. 400:174-83. 2002.
http://www.ncbi.nlm.nih.gov/pubmed?term=Cressoni%20MD%5BAuthor%5D&cauthor=true&cauthor_uid=20201664http://www.ncbi.nlm.nih.gov/pubmed?term=Giusti%20HH%5BAuthor%5D&cauthor=true&cauthor_uid=20201664http://www.ncbi.nlm.nih.gov/pubmed?term=Pi%C3%A3o%20AC%5BAuthor%5D&cauthor=true&cauthor_uid=20201664http://www.ncbi.nlm.nih.gov/pubmed?term=de%20Paiva%20Carvalho%20RL%5BAuthor%5D&cauthor=true&cauthor_uid=20201664http://www.ncbi.nlm.nih.gov/pubmed?term=Anaruma%20CA%5BAuthor%5D&cauthor=true&cauthor_uid=20201664http://www.ncbi.nlm.nih.gov/pubmed?term=Casarotto%20RA%5BAuthor%5D&cauthor=true&cauthor_uid=20201664http://www.ncbi.nlm.nih.gov/pubmed/20201664http://www.ncbi.nlm.nih.gov/pubmed?term=Elsaid%20KA%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Fleming%20BC%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Oksendahl%20HL%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Machan%20JT%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Fadale%20PD%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Hulstyn%20MJ%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Hulstyn%20MJ%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Shalvoy%20R%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Jay%20GD%5BAuthor%5D&cauthor=true&cauthor_uid=18512776http://www.ncbi.nlm.nih.gov/pubmed/18512776http://www.ncbi.nlm.nih.gov/pubmed?term=Felson%20DT%5BAuthor%5D&cauthor=true&cauthor_uid=11033593http://www.ncbi.nlm.nih.gov/pubmed?term=Lawrence%20RC%5BAuthor%5D&cauthor=true&cauthor_uid=11033593http://www.ncbi.nlm.nih.gov/pubmed?term=Dieppe%20PA%5BAuthor%5D&cauthor=true&cauthor_uid=11033593http://www.ncbi.nlm.nih.gov/pubmed?term=Hirsch%20R%5BAuthor%5D&cauthor=true&cauthor_uid=11033593http://www.ncbi.nlm.nih.gov/pubmed/11033593
-
47
HAYER, S.; REDLICH, K.; KORB, A.; HERMANN, S.; SMOLEN, J.; SCHETT, G.
Tenosynovitis and osteoclast formation as the initial preclinical changes in a murine
model of inflammatory arthritis. Arthritis Rheum., v. 56, n.1, p. 79-88, 2007.
HONMURA, A.; ISHII, A. Analgesic effect of GaAlAs diode laser irradiation on
hyperalgesia in carrageenin-induced inflammation. Lasers Surg Med., v. 13, p. 463-
469, 1993.
HOSAKA, Y.; KIRISAWA, R.; UEDA, H.; YAMAGUCHI, M.; TAKEHANA, K.
Differences in tumor necrosis factor (TNF)alpha and TNF receptor-1-mediated
intracellular signaling factors in normal, inflamed and scar-formed horse tendons. J.
Vet. Med.