SYMPTOMATIC THORACIC SPINAL CORD COMPRESSION … · A abordagem cirúrgica mostrou fechamento dural...
4
Arq Neuropsiquiatr 2007;65(2-A):279-282 Hospital São José / Complexo Hospitalar Santa Casa de Porto Alegre RS, Brazil: 1 Medical, Resident in Neurosurgery at Hospital São José - Complexo Hospitalar Santa Casa (HSJ/CHSC). 2 Neurosurgeon at Hospital Tacchini - Bento Gonçalves, RS. 3 Medical Student, Complexo Hospitalar Santa Casa / Fundação Faculdade Federal de Ciências Médicas de Porto Alegre (FFFCMPA). 4 N e u ro s u rgeon at HSJ-CHSC. Received 2 August 2006, received in final form 27 October 2006. Accepted 18 December 2006. Dr. Arthur de Azambuja Pereira Filho - Avenida Oscar Pereira 3008 - 91710-000 Porto Alegre RS - Brasil. E-mail: arthurpereirafilho@ gmail.com SYMPTOMATIC THORACIC SPINAL CORD COMPRESSION CAUSED BY POSTSURGICAL PSEUDOMENINGOCELE Arthur de Azambuja Pereira Filho 1 , Gustavo de David 2 , Gustavo de Azambuja Pereira Filho 3 , Albert Vincent Berthier Brasil 4 ABSTRACT - We report the first case of symptomatic thoracic spinal cord compression caused by postsur- gical pseudomeningocele. A 49-year-old man sought treatment for pro g ressive loss of strength in the low- er extremities ten months after full neurological re c o v e ry for a thoracic (T11) intradural-extramedullary schwannoma. Magnetic resonance imaging revealed a postsurgical thoracic (T11-T12) pseudomeningo- cele. The surgical approach showed an inadequate dural closure with spontaneous cere b rospinal fluid fis- tula. The defect was sealed with suture, muscle and biological glue covering. The patient had a good recov- ery. Pseudomeningocel e must take part of the diff e rential diagnosis of myelopathy after thoracic spine surgery. KEY WORDS: pseudomeningocele, spinal cord compression, myelopathy. Compressão medular torácica sintomática causada por pseudomeningocele pós-operatória RESUMO - Relatamos o primeiro caso de compressão medular torácica sintomática causada por pseudo- meningocele pós-operatória. Paciente masculino, 49 anos, apresentou perda pro g ressiva de força nas extremidades inferiores dez meses após recuperação neurológica completa de ciru rgia para remoção de schwannoma intradural-extramedular torácico. A ressonância magnética dorsal revelou pseudomeningo- cele (T11-T12). A abordagem cirúrgica mostrou fechamento dural inadequado com fistula liquórica espon- tânea. O defeito foi corrigido com sutura, músculo e cola biológica. O paciente teve boa evolução pós- operatória. Pseudomeningocele deve fazer parte do diagnóstico diferencial de mielopatia surgida após cirurgia na coluna dorsal. PALAVRAS-CHAVE: pseudomeningocele, compressão medular, mielopatia. Pseudomeningoceles are defined as extradural collections of cere b rospinal fluid (CSF) with no dural covering, which usually result from an inadvertent me- ningeal tear or inadequate closure during spinal sur- gery 1-4 . Most pseudomeningoceles remain embed- ded in the paraspinal soft tissue and cause no symp- toms 5 . Pseudomeningocele is an extremely rare cause of spinal cord compression. Few cases have been re- p o rted in the literature and in all of them the spinal cord compression was located in the cervical region 6-9 . We describe a case of symptomatic thoracic spinal c o rdcompression caused by postsurgical pseudome- ningocele. To our knowledge, this is the first re p o rt- ed case of a thoracic postsurgical pseudomeningo- cele causing symptomatic spinal cord compression. CASE History and examination – A 49-year-old Caucasian man sought treatment after experiencing the development of p ro g ressive motor loss in the lower extremities for the last t h ree months. The patient had undertaken a previous neu- ro s u rgical approach for a thoracic schwannoma ten months earlier, with a history of full neurological recovering after the surgery. The patient’s neurological examination showed de- creased strength in both the lower limbs (he could walk with aid), with bilateral Babinsky sign, without sensory, bowel or bladder findings. All other aspects of neurologi- cal examination were intact. The palpation of the operative wound showed no abnormality. Neuroimaging investigation – Magnetic resonance imag-
Transcript of SYMPTOMATIC THORACIC SPINAL CORD COMPRESSION … · A abordagem cirúrgica mostrou fechamento dural...

Arq Neuropsiquiatr 2007;65(2-A):279-282
Hospital São José / Complexo Hospitalar Santa Casa de Porto Alegre RS, Brazil: 1Medical, Resident in Neurosurgery at Hospital SãoJosé - Complexo Hospitalar Santa Casa (HSJ/CHSC). 2N e u ro s u rgeon at Hospital Tacchini - Bento Gonçalves, RS. 3Medical Student,Complexo Hospitalar Santa Casa / Fundação Faculdade Federal de Ciências Médicas de Porto Alegre (FFFCMPA). 4N e u ro s u rgeon atHSJ-CHSC.
Received 2 August 2006, received in final form 27 October 2006. Accepted 18 December 2006.
D r. Arthur de Azambuja Pereira Filho - Avenida Oscar Pereira 3008 - 91710-000 Porto Alegre RS - Brasil. E-mail: art h u r p e re i r a f i l h o @gmail.com
SYMPTOMATIC THORACIC SPINAL CORD COMPRESSION CAUSED BY POSTSURGICALPSEUDOMENINGOCELE
Arthur de Azambuja Pereira Filho1, Gustavo de David2,Gustavo de Azambuja Pereira Filho3, Albert Vincent Berthier Brasil4
ABSTRACT - We re p o rt the first case of symptomatic thoracic spinal cord compression caused by postsur-gical pseudomeningocele. A 49-year-old man sought treatment for pro g ressive loss of strength in the low-er extremities ten months after full neurological re c o v e ryfor a thoracic (T11) intradural-extramedullaryschwannoma. Magnetic resonance imaging revealed a postsurgical thoracic (T11-T12) pseudomeningo-cele. The surgical approach showed an inadequate dural closure with spontaneous cere b rospinal fluid fis-tula. The defect was sealed with suture, muscle and biological glue covering. The patient had a good re c o v-e ry. Pseudomeningocele must take part of the diff e rential diagnosis of myelopathy after thoracic spinesurgery.
KEY WORDS: pseudomeningocele, spinal cord compression, myelopathy.
Compressão medular torácica sintomática causada por pseudomeningocele pós-operatória
RESUMO - Relatamos o primeiro caso de compressão medular torácica sintomática causada por pseudo-meningocele pós-operatória. Paciente masculino, 49 anos, apresentou perda pro g ressiva de força nase x t remidades inferiores dez meses após recuperação neurológica completa de ciru rgia para remoção deschwannoma intradural-extramedular torácico. A ressonância magnética dorsal revelou pseudomeningo-cele (T11-T12). A abordagem cirúrgica mostrou fechamento dural inadequado com fistula liquórica espon-tânea. O defeito foi corrigido com sutura, músculo e cola biológica. O paciente teve boa evolução pós-operatória. Pseudomeningocele deve fazer parte do diagnóstico diferencial de mielopatia surgida apóscirurgia na coluna dorsal.
PALAVRAS-CHAVE: pseudomeningocele, compressão medular, mielopatia.
Pseudomeningoceles are defined as extraduralcollections of cere b rospinal fluid (CSF) with no duralcovering, which usually result from an inadvertent me-ningeal tear or inadequate closure during spinal sur-g e ry1 - 4. Most pseudomeningoceles remain embed-ded in the paraspinal soft tissue and cause no symp-t o m s5. Pseudomeningocele is an extremely rare causeof spinal cord compression. Few cases have been re-p o rted in the literature and in all of them the spinalc o rd compression was located in the cervical re g i o n6 - 9.
We describe a case of symptomatic thoracic spinalc o rdcompression caused by postsurgical pseudome-ningocele. To our knowledge, this is the first re p o rt-ed case of a thoracic postsurgical pseudomeningo-cele causing symptomatic spinal cord compression.
CASEH i s t o ry and examination – A 49-year-old Caucasian man
sought treatment after experiencing the development ofp ro g ressive motor loss in the lower extremities for the lastt h ree months. The patient had undertaken a previous neu-ro s u rgical approach for a thoracic schwannoma ten monthsearlier, with a history of full neurological recovering afterthe surgery.
The patient’s neurological examination showed de-c reased strength in both the lower limbs (he could walkwith aid), with bilateral Babinsky sign, without sensory,bowel or bladder findings. All other aspects of neurologi-cal examination were intact.
The palpation of the operative wound showed noabnormality.
N e u roimaging investigation – Magnetic resonance imag-

280 Arq Neuropsiquiatr 2007;65(2-A)
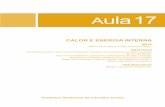
ing (MRI) revealed a postsurgical thoracic pseudomeningo-cele extending from T11 to T12 (Fig 1).
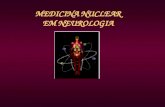
S u rgical treatment – An external cere b rospinal fluidlumbar drain was placed preoperatively and kept closedduring all the surgical pro c e d u re. The previous wound wasreopened and a high tension encapsulated cere b ro s p i n a lfluid collection was identified. The pseudomeningocele wasincised and the defect in the dural closure was seen withthe aid of a Valsalva maneuver (Fig 2). The defect wassealed with suture and muscle with biological glue cover-ing. Continuous CSF drainage was perf o rmed for five days.
Postoperative course – The patient had a good postop-erative re c o v e ry. The lower limbs` strength had a mildi m p rovement immediately. The patient was discharged 4days after the surgery.
At a 6-months re v i e w, the patient’s neurological exam-ination was normal and the postoperative MRI showed re s-olution of the pseudomeningocele (Fig 3).
The patient agreed with the publication of his case.
DISCUSSION
The most common causes of spinal cord compre s-sion are: trauma, neoplasia, degenerative disease,epidural or subdural spinal hematoma, inflammato-ry disease and infection1 0 - 1 7. Postoperative peudo-meningocele is an extremely rare cause of spinal cord
Fig 1. T2-weighted sagittal spinal MRI demonstrates large CSF
collection at T11-T12 levels.
Fig 2. Transoperative photography demonstrates the pseudomeningocele`s cavity and the defect in the dur -
al closure (arrow).

Arq Neuropsiquiatr 2007;65(2-A) 281
c o m p re s s i o n6 - 9. A postlaminectomy pseudomeningo-cele was re p o rted first in 1946 by Hyndman and Ger-ber in a review of extradural cysts1 8. In 1947, Swan-son and Fincher1 9 re p o rted the first three cases ofpseudomeningocele after a lumbar discectomy. Wi n-kler and Powers2 0 re p o rted two additional cases ofpseudomeningocele after a lumbar discectomy andt reated both patients with an excision of the menin-gocele and spinal fusion. Myelopathy due to pseudo-meningocele was only re p o rted four times, but in allcases the spinal cord compression was located in thecervical region6-9.
The incidence of a postsurgical pseudomeningo-cele is unknown as many cases probably are asymp-t o m a t i c2 1. Swanson and Fincher1 9 re p o rted a 0.068%incidence of pseudomeningoceles in 1700 explorato-ry laminectomies. Teplick et al.2 noted that 2% of 400laminectomy patients who underwent postoperativeCT scanning had a pseudomeningocele.
The term pseudomeningocele reflects the absenceof a true meningeal layer lining the cyst wall2 1. Thef o rmation of a pseudomeningocele begins with atear in the dura that is closed incompletely or goesunnoticed at the time of a laminectomy. If the arach-noid remains intact, there may be herniation of thearachnoid through the dural opening resulting in anarachnoid-lined cyst2 , 2 0 , 2 2 , 2 3. More commonly, the duraand arachnoid are lacerated, and the CSF pours into
the paraspinal soft tissue. The CSF may be absorbedi n i t i a l l y, but the CSF collection eventually becomesencapsulated by fibrous tissue1,2,24,25.
The optimal selection of diagnostic imaging tech-niques is debated in the literature. CT scanning hasbeen considered in the diagnosis of postoperativepseudomeningocele. Identification of the neck of thepseudomeningocele is improved with the intrathe-cal administration of water-soluble contrast2 , 2 6 , 2 7.Although myelography demonstrates the pseudo-meningocele, the communication between themeningocele sac and the thecal sac usually is not wellvisualized. The use of MRI in the evaluation of post-operative pseudomeningoceles has been re p o rt e dsince 19882 7 , 2 8. MRI studies can provide excellent def-inition of the meningocele and its communicationwith the dural sac. It is considered the g o l d - s t a n d a rdmethod in diagnosing postoperative pseudomeningo-c e l e s2 8. Digital subtraction myelography is also re p o rt-ed in the literature with good results29.
Pseudomeningoceles can be either symptomaticor not. According to Lee et al.2 1, it may be diff i c u l tto determine the real source of symptoms in patientswith a history of local surg e ry and radiological evi-dence of a pseudomeningocele. Tension of the cystagainst the spinal cord or the nerve roots, entrap-ment of nerve roots into the dural defect, or peri-radicular fibrosis can be responsible for the patient’scomplaints21,26.
The treatment of a postoperative pseudomenin-gocele is somewhat controversial. Asymptomaticpseudomeningoceles may be left untreated; howev-e r, it may be difficult to confirm that the pseudo-meningocele is truly asymptomatic. The definitivet reatment of a symptomatic postoperative pseudo-meningocele is surgical and re q u i res adequate expo-s u rein order to localize the dural defect2 6. The durashould be closed primarily, if at all possible. Fibringlue along the suture line may be helpful1 , 2 6. Theremoval of the entire pseudomeningocele sac is un-n e c e s s a ryaccording to the literature2 6. Some authorsrefer other options for the treatment of pseudome-ningoceles, such as peritoneal shunt3 0 and mechani-cal compre s s i o n3 1, but we consider these techniquesas alternative treatments and our pre f e rence is almostalways for the aggressive surgical repair.
Lumbar spinal fluid drainage is a common pro c e-d u re to reduce the risks of CSF fistula after varioustransdural neuro s u rgical pro c e d u re s3 2. Although it isan effective pro c e d u re, some serious complicationsmay ensue. Common adverse events observed with
Fig 3. Postoperative T1-weighted sagittal spinal MRI shows the
resolution of the pseudomeningocele.

282 Arq Neuropsiquiatr 2007;65(2-A)
lumbar spinal fluid drainage are infections, pneumo-cephalus, hematoma, and CSF overd r a i n a g e3 2. In thep resent case, we decided to maintain the lumbardrainage for five days, and no complication occurre d .No evidence of treatment failure was observed sixmonths after the procedure.
In conclusion, pseudomeningocele must take partof the diff e rential diagnosis of pro g ressive myelopa-thy after thoracic spine surg e ry. Surgical tre a t m e n tof this entity seems to be effective.
REFERENCES1. B a r ron JT. Lumbar pseudomeningocele. Orthopedics 1990;11 3 : 6 0 8 - 6 1 0 .
2. Teplick JG, Peyster RG, Teplick SK, et al. CT identification of post-laminectomy pseudomeningocele. AJNR 1983;4:179-182.
3. D ̀ A n d rea F, Maiuri F, Corriero G, et al. Postoperative lumbar arach-noidal diverticula. Surg Neurol 1985;23:287-290.
4. Kim Y W, Unger JD, Grinsell PJ. Postoperative pseudodiverticular (spu-rious meningoceles) of the cervical subarachnoid space. Acta RadiolDiagn 1974;15:16-20.
5. Paolini S, Ciappetta P, Piattella MC. Intraspinous postlaminectomypseudomeningocele. Eur Spine J 2003;12:325-327.
6. Hosono N, Yonenobu K, Ono K. Postoperative cervical pseudomeningo-cele with herniation of the spinal cord. Spine 1995;20:2147-2150.
7. Hanakita J, Kinuta Y, Suzuki T. Spinal cord compression due to post-operative cervical pseudomeningocele. Neuro s u rgery 1985;17:317-319.
8. Helle TL, Conley FK. Postoperative cervical pseudomeningocele as acause of delayed myelopathy. Neurosurgery 1981;9:314-316.
9. B u r res KP, Conley FK. Pro g ressive neurological dysfunction second-ary to postoperative cervical pseudomeningocele in a C-4 quadriple-gic: case report. J Neurosurg 1978;48:289-291.
10. Held JL, Peahota A. Nursing care of the patient with spinal cord com-pression. Oncol Nursing Forum 1993;20:1507-1516.
11. Bucholtz JD. Metastatic epidural spinal cord compression. Sem OncolNursing 1999;15:150-159.
12. Quinn JA, DeAngelis LM. Neurological emergencies in the cancerpatient. Sem Oncol 2000;27:311-321.
13. Bucholtz JD. Central nervous system metastases. Sem Oncol Nursing1999;14:61-72.
14. Abraham J. Management of pain and spinal cord compression inpatients with advanced cancer. Ann Intern Med 1999;131:37-46.
15. Gleave JRW, MacFarlane R. Cauda equina syndrome: what is the re l a-tionship between timing of surgery and outcome? Br J Neuro s u rg2002;16:325-328.
16. Healey J H, Brown H K. Complications of bone metastases. Cancer2000;88:2940-2951.
17. Markman N. Early recognition of spinal cord compression in cancerpatients. Cleve Clin Med J 1999;66:629-631.
18. Hyndman OR, Gerber WF. Spinal extradural cysts, congenital andacquired: report of cases. J Neurosurg 1946;3:474-486.
19. Swanson HS, Fincher EF. Extradural arachnoidal cysts of traumatic ori-gin. J Neurosurg 1947;4:530-538.
20. Winckler H, Powers JA. Meningocele following hemilaminectomy. NC Med J 1950;11:292-294.
21. Lee KS, Hardy IM. Postlaminectomy lumbar pseudomeningocele: re p o r tof four cases. Neurosurgery 1992;30:111-114.
22. Rinaldi I, Hodges TO. Iatrogenic lumbar meningocele: report of threecases. J Neurol Neurosurg Psychiatry 1970;33:484-492.
23. Rinaldi I, Peach WF. Postoperative lumbar meningocele: report of twocases. J Neurosurg 1969;30:504-507.
24. Miller PR, Elder FW. Meningeal pseudocysts (meningocele spurius)following laminectomy. Report of ten cases. J Bone Joint Surg 1968;50:268-276.
25. Pagni CA, Cassinari V, Bernasconi V. Meningocele spurius followinghemilaminectomy in a case of lumbar discal hernia. J Neuro s u rg 1961;18:709-710.
26. Hadani M, Findler G, Knoler N, et al. Entrapped lumbar nerve root inpseudomeningocele after laminectomy: report of three cases. Neuro-surgery 1986;19:405-407.
27. Schumacher H-W, Wassman H, Podlinski C. Pseudomeningocele ofthe lumbar spine. Surg Neurol 1988;29:77-78.
28. Murayama S, Numaguchi Y, Whitecloud TS, et al. Magnetic re s o n a n c eimaging of postsurgical pseudomeningocele. Comput Med ImagingGraph 1989;13:335-339.
29. Phillips CD, Kaptain GJ, Razack N. Depiction of a postoperative pseudo-meningocele with Digital Subtraction Myelography. Am J Neuro r a d i o l2002;23:337-338.
30. A n d rew SA, Sidhu KS. Cervical-peritonial shunt placement for post-operative cervical pseudomeningocele. J Spinal Disord Tech 2005;18:290-292.
31. Leis AA, Leis JM, Leis JR. Pseudomeningoceles: a role for mechanicalc o m p ression in the treatment of dural tears. Neurology 2001;56:111 6 -1117.
32. Bloch J, Regli L. Brain stem and cerebellar dysfunction after lumbarspinal fluid drainage: case report. J Neurol Neuro s u rg Psychiatry 2003;74:992-994.








![Marcos Cezar dos Santos Biologia Geraleducacaonaopara.com/.../uploads/...REINO-ANIMAL-1.pdf · Reino Metazoa Filo nome em português Poriferos ou espon]as Celenterados Platelmlntos](https://static.fdocumentos.com/doc/165x107/6075f797267867789c7c0c9b/marcos-cezar-dos-santos-biologia-reino-metazoa-filo-nome-em-portugus-poriferos.jpg)