UNIVERSIDADE FEDERAL DE PERNAMBUCO … · examinador as medidas foram realizadas por dois...
92
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP UNIVERSIDADE FEDERAL DE PERNAMBUCO CENTRO DE CIÊNCIAS DA SAÚDE DEPARTAMENTO DE FISIOTERAPIA PROGRAMA DE PÓS-GRADUAÇÃO EM FISIOTERAPIA PEDRO OLAVO DE PAULA LIMA PROPRIEDADES CLINIMÉTRICAS DA UNIDADE DE BIOFEEDBACK PRESSÓRICO NA AVALIAÇÃO DA ATIVIDADE MUSCULAR DO TRANSVERSO ABDOMINAL EM PACIENTES COM DOR LOMBAR CRÔNICA INESPECÍFICA. RECIFE 2010
Transcript of UNIVERSIDADE FEDERAL DE PERNAMBUCO … · examinador as medidas foram realizadas por dois...

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
UNIVERSIDADE FEDERAL DE PERNAMBUCO
CENTRO DE CIÊNCIAS DA SAÚDE
DEPARTAMENTO DE FISIOTERAPIA
PROGRAMA DE PÓS-GRADUAÇÃO EM FISIOTERAPIA
PEDRO OLAVO DE PAULA LIMA
PROPRIEDADES CLINIMÉTRICAS DA UNIDADE DE BIOFEEDBACK
PRESSÓRICO NA AVALIAÇÃO DA ATIVIDADE MUSCULAR DO TRANSVERSO
ABDOMINAL EM PACIENTES COM DOR LOMBAR CRÔNICA INESPECÍFICA.
RECIFE
2010

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
PEDRO OLAVO DE PAULA LIMA
PROPRIEDADES CLINIMÉTRICAS DA UNIDADE DE BIOFEEDBACK
PRESSÓRICO NA AVALIAÇÃO DA ATIVIDADE MUSCULAR DO TRANSVERSO
ABDOMINAL EM PACIENTES COM DOR LOMBAR CRÔNICA INESPECÍFICA.
Dissertação apresentada ao Programa de Pós-Graduação em Fisioterapia do Centro de Ciências da Saúde da Universidade Federal de Pernambuco, para obtenção do Grau de Mestre em Fisioterapia.
Linha de Pesquisa: Instrumentação e Intervenção Fisioterapêutica - Aplicabilidade e confiabilidade de métodos de avaliação em Fisioterapia.
Orientadora: Glória Elizabeth Carneiro Laurentino.
Co-orientadora: Maria Cristina Falcão Raposo.
RECIFE
2010

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Lima, Pedro Olavo de Paula
Propriedades clinimétricas da unidade de biofeedback pressórico na avaliação da atividade muscular do transverso abdominal em pacientes com dor lombar crônica inespecífica / Pedro Olavo de Paula Lima. – Recife: O Autor, 2010.
91 folhas: il., fig., tab.
Dissertação (mestrado) – Universidade Federal de Pernambuco. CCS. Fisioterapia, 2010.
Inclui bibliografia, anexos e apêndice.
1. Unidade de biofeedback pressórico. 2. Dor lombar. 3. Músculo transverso abdominal. 4. Reprodutibilidade. 5. Validade. I. Título.
615.8-7 CDU (2.ed.) UFPE 615.82 CDD (20.ed.) CCS2010-142

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ORIENTADORA
Glória Elizabeth Carneiro Laurentino
Professora Adjunto do Departamento de Fisioterapia do Centro de Ciências da Saúde da
Universidade Federal de Pernambuco
Doutora em Nutrição pela Universidade Federal de Pernambuco
CO-ORIENTADORA
Maria Cristina Falcão Raposo
Professora Adjunto do Departamento de Estatística do Centro de Ciências Exatas e da
Natureza da Universidade Federal de Pernambuco
Doutora em Economia pela Universidade Federal de Pernambuco

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
DEDICATÓRIA
Ao Senhor: Deus
À minha Mãe: Idée Maria
Ao meu pai: Pedro Olegário
À minha noiva: Flávia Botelho
Aos meus irmãos: Lílian, Jonathan, Ronaldo e Maria Clara
Ao meu sobrinho: Davi Lima Maia
Às minhas avós: Margarida e Carmelita
Aos meus avôs: Olavo e Moiséis “In Memoriam”

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
AGRADECIMENTOS ESPECIAIS
À Profª. Drª. Glória Elizabeth Carneiro Laurentino,
que aceitou a orientação deste trabalho e sempre se conduziu de maneira dedicada e
competente durante toda sua elaboração. Muito obrigado por sua dedicação e apoio em todos
os momentos, sempre disponível quando precisava.
À Profª. Drª. Maria Cristina Falcão Raposo,
pelo empenho na elaboração deste trabalho, supervisão estatística detalhada e tranquilidade
nas explicações;
Ao amigo e colega de trabalho, Rodrigo Ribeiro de Oliveira,
pela valiosa participação na coleta de dados e elaboração deste trabalho, seu apoio foi
fundamental;
Ao Prof°. Dr. Leonardo Oliveira Pena Costa
pela disponibilidade e atenção que sempre me dispensou, apesar da distância, em responder
dúvidas e revisar os manuscritos deste trabalho com máxima prontidão.

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
AGRADECIMENTOS
• Ao Departamento de Fisioterapia da UFPE, especialmente ao Laboratório de
Cinesiologia e Avaliação Funcional, pela acolhida e pelo apoio desde o início das
atividades do mestrado;
• Aos meus companheiros de moradia, Thales Henrique de Araújo Sales e Rodrigo
Ribeiro de Oliveira, pela parceira/companheirismo e por toda paciência com minha
pessoa durante o período do mestrado;
• A todos os meus colegas de mestrado, Alana Elza; Thaysa Oliveira; Emanuela
Cavalcante; Leila Barbosa; Antônio Francisco; João Danyell; Jacqueline Barcelar;
Silvana Uchôa; Dinalva Lacerda; Roberta Machado e Adriana Sarmento, pelos
estudos e debates que tanto promoveram o conhecimento da primeira turma do curso
(2009), assim como pelos encontros sociais realizados;
• Ao Prof°. Dr. Alberto Galvão de Moura Filho, pela acolhida no laboratório e
disponibilização da sala de eletromiografia para as coletas de dados;
• A todos os professores que participaram de minha formação profissional no mestrado.
Aos funcionários do Departamento de Fisioterapia pela atenção e ajuda;
• Aos sujeitos, que participaram de forma voluntária das avaliações, pela paciência e
pela disponibilização de tempo para contribuir nesse estudo;
• À amiga Elda Madruga e família, pela acolhida calorosa em seu lar e por todo apoio
despendido durante minha estadia em Recife-PE;

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
• Ao meu amigo de infância de Belém-PA, Bruno Brasil e a toda sua família, por me
receberem tão bem em sua cidade;
• À tia Anália Paranhos e a toda sua família por me receberem em sua casa tão bem;
• Agradeço a toda minha família e aos meus amigos pela torcida, constantes incentivos e
orações. Obrigado por acreditarem no meu esforço.

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
LISTA DE ABREVEATURAS, SIGLAS E SÍMBOLOS
DP Desvio Padrão
SD Standard Deviation
p Probabilidade de significância estatística
ICC Intraclass Correlation Coeficient
IC Intervalo de Confiança
CI Confidence Interval
r Coeficiente de Correlação de Pearson
CV Coeficiente de Variação
SEM Standard Error of the Measurement
SDC Smallest Detectable Change
LOA Limits of Agreement
PPV Positive Predictive Value
NPV Negative Predictive Value
SPSS Statistical Package for Social Sciences
UFPE Universidade Federal de Pernambuco
UFC Universidade Federal do Ceará
UNICID Universidade Cidade de são Paulo
CINAHL Cumulative Index to Nursing and Allied Health Literature
PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
UBP Unidade de Biofeedback Pressórico
PBU Pressure Biofeedback Unit
EMG Eletromiografia (Electromyography)
SENIAM Surface Electromyography for Non Invasive Assessment of Muscles

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
CIVM Contração Isométrica Voluntária Máxima
MVIC Maximal Voluntary Isometric Contraction
RMS Root Means Square
Ag/AgCl Cloreto de Prata
TrA Transverso Abdominal [Transversus Abdominis]
OI Oblíquo Interno [Internal Oblique]
LBP Low Back Pain
IMC Índice de Massa Corpórea
BMI Body Mass Index
JCR Journal Citation Reports

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
LISTA DE TABELAS
Referentes ao primeiro artigo - Measurement properties of the pressure biofeedback unit in
the evaluation of transversus abdominis muscle activity: a
systematic review.
Tabela 1. Checklist used to evaluate the clinimetric properties of the studies included in
the review. (p.32)
Tabela 2. Description of eligible studies. (p.34)
Tabela 3. Results and limitations of the studies included in the review. (p.36)
Tabela 4. Summary of assessment of the quality criteria of studies included in the review.
(p.37)
Referentes ao segundo artigo - Reproducibility of pressure biofeedback unit in the transversus
abdominis muscle activity in patients with chronic
nonspecific low back pain.
Tabela 1. Sample characteristics. (p.52)
Tabela 2. Reliability and agreement for pressure measures. (p.53)

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Referentes ao terceiro artigo - Validity of pressure biofeedback unit in the transversus
abdominis muscle activity in patients with chronic
nonspecific low back pain.
Tabela 1. Sample characteristics. (p.70)
Tabela 2. Description of the pressure measures and electromyographic measures in the
transversus abdominis muscle activity. (p.71)
Tabela 3. 2x2 Table between the pressure biofeedback unit ratings and the surface
electromyography ratings. (p.72)

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
LISTA DE FIGURAS
Referentes ao primeiro artigo - Measurement properties of the pressure biofeedback unit in
the evaluation of transversus abdominis muscle activity: a
systematic review.
Figura 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-
Analyses) flow diagram of the literature search. (p.33)
Referentes ao segundo artigo - Reproducibility of pressure biofeedback unit in the transversus
abdominis muscle activity in patients with chronic
nonspecific low back pain.
Figura 1. Pressure Biofeedback Unit (STABILIZER®). (p.50)
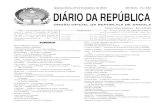
Figura 2. Bland and Altman plots for pressure measures of Examiner A (test 1 – test 2).
(p.53)
Figura 3. Bland and Altman plots for pressure measures of Examiner A and Examiner B.
(p.54)

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Referentes ao terceiro artigo - Validity of pressure biofeedback unit in the transversus
abdominis muscle activity in patients with chronic
nonspecific low back pain.
Figura 1. Pressure Biofeedback Unit (STABILIZER®). (p.69)

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
SUMÁRIO
LISTA DE ABREVEATURAS, SIGLAS E SÍMBOLOS
LISTA DE TABELAS
LISTA DE FIGURAS
RESUMO 18
ABSTRACT 19
1. APRESENTAÇÃO................................................................................................ 20
INTRODUÇÃO 23
2. PRIMEIRO ARTIGO…………………………….………………………....... 24
ABSTRACT 26
INTRODUCTION 28
METHODS 29
Data Sources and Searches 29
Study Selection and Eligibility Criteria 30
Data Extraction and Quality Assessment 30
RESULTS 31

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
DISCUSSION 37
REFERENCES 41
3. SEGUNDO ARTIGO…………………………………………………………… 43
ABSTRACT 45
INTRODUCTION 47
METHODS 48
RESULTS 51
DISCUSSION 54
CONCLUSION 58
REFERENCES 59
4. TERCEIRO ARTIGO………………………...………………………………… 61
ABSTRACT 63
INTRODUCTION 64
METHODS 66
RESULTS 70
DISCUSSION 72
CONCLUSION 75

_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
REFERENCES 76
5. CONCLUSÕES……………………………..…………………………………… 79
APÊNDICE 81
APÊNDICE A: Termo de Consentimento Livre e Esclarecido 82
ANEXOS 84
ANEXO 1: Termo de Submissão para a Physiotherapy 85
ANEXO 2: Termo de Submissão para a Physiotherapy Research
International
86
ANEXO 3: Termo de Submissão para a Physiotherapy Theory and Practice 87
ANEXO 4: Pain Numerical Rating Scale 88
ANEXO 5: Roland Morris Disability Questionnaire 89
ANEXO 6: Aprovação do Comitê de Ética em Pesquisa 91

18
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
RESUMO
Introdução: A Unidade de Biofeedback Pressórico (UBP) é, frequentemente, usada por
clínicos e pesquisadores para avaliar a atividade muscular do transverso abdominal (TrA) em
pacientes com dor lombar crônica inespecífica, entretanto pouco se sabe sobre suas
propriedades clinimétricas. Objetivos: Avaliar a reprodutibilidade e a validade da UBP na
atividade do músculo TrA em pacientes com dor lombar crônica inespecífica. Métodos: A
amostra foi composta por cinquenta participantes. Para testar a reprodutibilidade inter-
examinador as medidas foram realizadas por dois fisioterapeutas e para testar a
reprodutibilidade intra-examinador, um deles realizou duas medidas em ocasiões diferentes
com um intervalo de sete dias entre os testes. Para testar a validade foram correlacionadas as
medidas da UBP (teste índice) e da eletromiografia de superfície (teste padrão-referência).
Resultados: Foram observados valores do coeficiente de correlação intraclasse de 0,74 e 0,76
para a reprodutibilidade intra e inter-examinador, respectivamente. A concordância intra-
examinador e inter-examinador estiveram dentro dos limites de concordância em 95% das
ocasiões. Foi observado fraco valor do coeficiente de correlação de Pearson (r=0,2; p<0,20)
para a validade. Os testes diagnósticos mostraram baixa sensibilidade (60%) e especificidade
(40%) da UBP. O valor preditivo positivo foi igual a 0,8 e o valor preditivo negativo igual a
0,2. Conclusões: A reprodutibilidade da UBP variou de satisfatória a excelente e a validade
apresentou baixa correlação entre os dados pressóricos e eletromiográficos. Conclui-se que
um paciente com dor lombar crônica inespecífica pode ser avaliado por um único
fisioterapeuta em momentos distintos, assim como, esse mesmo paciente pode ser avaliado
por fisioterapeutas diferentes e obter o mesmo diagnóstico cinesiológico. Entretanto, os
achados eletromiográficos sugerem que a aplicabilidade clínica da UBP em pacientes com dor
lombar crônica inespecífica não é indicada.
Palavras-chave: unidade de biofeedback pressórico, dor lombar, músculo transverso
abdominal, reprodutibilidade, confiabilidade, concordância, validade.

19
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ABSTRACT
Introduction: Pressure Biofeedback Unit (PBU) is often used by clinicians and researchers to
evaluate the muscular activity of transversus abdominis (TrA) in patients with chronic
nonspecific low back pain, however little is known about its clinimetric properties.
Objectives: To assess the reliability and validity of PBU in the TrA muscle activity in patients
with chronic nonspecific low back pain. Methods: The sample consisted of fifty participants.
To test the inter-examiner reliability measurements were performed by two physiotherapists
and to test the intra-examiner reliability, one of them performed two measures on different
occasions with an interval of seven days between the tests. To test the validity were correlated
PBU (index test) measures and surface electromyography (reference-standard test) measures.
Results: We observed values of the intraclass correlation coefficient of 0.74 and 0.76 for
intra-examiner reproducibility and inter-examiner, respectively. Intra-examiner and inter-
examiner agremeent were within the limits of agreement in 95% of occasions. We observed
low value of the Pearson correlation coefficient (r = 0.2, p <0.20) for validity. Diagnostic
tests showed low sensitivity (60%) and specificity (40%) of the PBU. The positive predictive
value was equal to 0.8 and negative predictive value equal to 0.2. Conclusions: The
reproducibility of PBU ranged from satisfactory to excellent and the validity shown poor
correlation between pressure data and electromyographic data. We conclude that a patient
with chronic nonspecific low back pain can be assessed by a single physiotherapist at
different times and, that same patient can be evaluated by different physiotherapists and get
the same kinesiology diagnostic. However, electromyographic findings suggest that the
clinical applicability of the PBU in patients with chronic nonspecific low back pain is not
indicated.
Keywords: pressure biofeedback unit, low back pain, transversus abdominis muscle,
reproducibility, reliability, agreement, validity.

20
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
1. APRESENTAÇÃO
A maioria dos estudos sobre propriedades clinimétricas da unidade de
biofeedback pressórico (UBP) enfoca, em geral, indivíduos saudáveis, sendo escassos os
estudos objetivando testar clinimetricamente o instrumento em uma amostra relevante para a
prática clínica, isto é, composta por pacientes com dor lombar crônica inespecífica.
Para o desenvolvimento do estudo, inicialmente, foi realizada uma revisão
sistemática com o intuito de se fazer um levantando crítico da literatura. A partir das
conclusões extraídas dessa revisão, foram realizados ajustes no projeto de pesquisa inicial
com o objetivo de se reduzir possíveis vieses metodológicos no transcorrer da coleta e
análises dos dados. As etapas pré-definidas, dentro da metodologia estabelecida, foram
obedecidas e seguidas rigorosamente e, por fim, os resultados obtidos geraram dois artigos
originais, de acordo com seus principais desfechos. Um artigo teve como objeto principal
investigar a reprodutibilidade da UBP, enquanto o outro abordou a sua validade.
Com base na literatura especializada e após reflexão sobre o tema, foram
construídas as seguintes hipóteses:
• A UBP apresenta valores aceitáveis de reprodutibilidade intra-examinador da
atividade do músculo TrA em pacientes com dor lombar crônica inespecífica;
• A UBP apresenta valores aceitáveis de reprodutibilidade inter-examinador da
atividade do músculo TrA em pacientes com dor lombar crônica inespecífica;
• A UBP apresenta valores aceitáveis de validade da atividade do músculo TrA em
pacientes com dor lombar crônica inespecífica quando comparada a eletromiografia de
superfície;

21
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Para consecução da proposta e, como forma de aceitar ou rejeitar as hipóteses
formuladas, foram definidos os seguintes objetivos:
• Avaliar a confiabilidade intra-examinador da UBP, por intermédio de medidas
repetidas da atividade do músculo transverso abdominal em pacientes com dor lombar
crônica inespecífica;
• Avaliar a confiabilidade inter-examinador da UBP, por intermédio de medidas
repetidas da atividade do músculo transverso abdominal em pacientes com dor lombar
crônica inespecífica;
• Avaliar a concordância intra-examinador da UBP, por intermédio de medidas
repetidas da atividade do músculo transverso abdominal em pacientes com dor lombar
crônica inespecífica;
• Avaliar a concordância inter-examinador da UBP, por intermédio de medidas
repetidas da atividade do músculo transverso abdominal em pacientes com dor lombar
crônica inespecífica;
• Avaliar a validade da UBP, por intermédio de análise comparativa com a
eletromiografia de superfície em pacientes com dor lombar crônica inespecífica.
Seguindo recomendações do Programa de Pós-graduação em Fisioterapia da
UFPE, o trabalho de dissertação, aqui apresentado, inclui na sua estruturação três artigos
científicos enviados para publicação em revistas especializadas e, por esta razão, seguem as
normas dessas revistas no que diz respeito à formatação e escrita do manuscrito.
O primeiro artigo, intitulado – Measurement properties of the pressure
biofeedback unit in the evaluation of transversus abdominis muscle activity: a systematic

22
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
review – constitui uma revisão sistemática da literatura sobre propriedades clinimétricas da
UBP. Esse manuscrito foi submetido para publicação no periódico Physiotherapy (conceito
B1 na área 21 da CAPES, com fator de impacto igual a 0,773 JCR-2009) no dia 21 de Janeiro
de 2010 (ANEXO 1) e foi aceito para publicação no dia 27 de Julho de 2010.
Este artigo, por constituir uma revisão da literatura sobre o tema central aqui
abordado, está sendo usado como a introdução desta dissertação e os principais tópicos
abordados foram: propriedades clinimétricas (reprodutibilidade e validade); unidade de
biofeedback pressórico; músculo transverso abdominal e dor lombar crônica inespecífica.
O segundo artigo, intitulado – Reproducibility of pressure biofeedback unit in
the transversus abdominis muscle activity in patients with chronic nonspecific low back
pain – foi submetido ao periódico Physiotherapy Research International (conceito B1 na área
21 da CAPES) no dia 15 de Julho de 2010 (ANEXO 2), na qualidade de artigo original. Este
artigo enfoca, principalmente, a reprodutibilidade da UBP em pacientes com dor lombar
crônica inespecífica. Como desfechos primários foram abordadas a confiabilidade e
concordância intra-examinador e inter-examinador.
O terceiro artigo, intitulado – Validity of pressure biofeedback unit in the
transversus abdominis muscle activity in patients with chronic nonspecific low back pain –
foi submetido à Physiotherapy Theory and Practice (conceito B1 na área 21 da CAPES) no
dia 15 de Julho de 2010 (ANEXO 3), na qualidade de artigo original. O principal objeto desse
estudo foi investigar a validade da UBP em pacientes com dor lombar crônica inespecífica.
Como desfechos primários foram abordados a correlação entre dados pressóricos e
eletromiográficos, assim como análise de testes diagnósticos.

23
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
INTRODUÇÃO

24
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
2. PRIMEIRO ARTIGO
MEASUREMENT PROPERTIES OF THE PRESSURE BIOFEEDBACK UNIT IN THE
EVALUATION OF TRANSVERSUS ABDOMINIS MUSCLE ACTIVITY: A
SYSTEMATIC REVIEW.
Revisão sistemática submetida para publicação na Physiotherapy (ANEXO 1).

25
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
MEASUREMENT PROPERTIES OF THE PRESSURE BIOFEEDBACK UNIT IN
THE EVALUATION OF TRANSVERSUS ABDOMINIS MUSCLE ACTIVITY: A
SYSTEMATIC REVIEW.
Pedro Olavo de Paula Limaa*, Rodrigo Ribeiro de Oliveiraa, Leonardo Oliveira Pena Costab, Glória Elizabeth
Carneiro Laurentinoc.
a Master's Program in Physical Therapy, Universidade Federal de Pernambuco, Brazil
b Master's Program in Physical Therapy, Universidade Cidade de São Paulo, Brazil
c Department of Physical Therapy, Universidade Federal de Pernambuco, Brazil
* Corresponding Author: Laboratory of Kinesiology and Functional Assessment.
Address: Anibal Fernandes Street, Recife, PE, 50740-560, Brazil.
Telephone: +55 81 21268811 Facsimile: +55 81 21268491
Email: [email protected]

26
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ABSTRACT
Background: Measurements of pressure biofeedback unit (PBU) are used to indirectly
evaluate the activity of the transversus abdominis (TrA) muscle. These measures can be used
to classify patients or to monitor progress of treatment programs for people with low back
pain.
Objective: The purpose of this study was to systematically review studies on the
measurement properties of the PBU for the activity of the TrA muscle.
Data Sources: Eligible studies were identified through searches on PUBMED, CINAHL and
BIREME (1990-2009). Additionally, hand searches of journals and citation tracking were
performed.
Study Selection: Studies published in full text involving any type of clinimetric tests of the
PBU measurement for TrA muscle were selected.
Data Extraction: Two independent reviewers selected the studies, extracted the data and
assessed the methodological quality.
Data Synthesis: Due to the heterogeneity of study designs and statistical analysis, pooling the
data for a meta-analysis was not possible. Six studies met our inclusion criteria. These studies
were of low quality and recruited healthy subjects rather than patients with low back pain.
Results:The studies found moderate to good reproducibility with ICC values ranging from
0.47 to 0.82 and acceptable construct validity with correlations values ranging from 0.48 to
0.90.
Conclusions: The current evidence of the measurement properties of the PBU for evaluating
the muscle activity of TrA is mainly based on studies with suboptimal designs and the
findings from these studies are likely to be overly optimistic. The most important clinical

27
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
questions about the measurement properties of the PBU on the TrA muscle are yet to be
answered.
Key-words: pressure biofeedback unit, transversus abdominis, reproducibility, validity
systematic review.

28
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
INTRODUCTION
Specific stabilization exercises (also known as motor control exercises) in treatment programs
for patients with low back pain (LBP) have become increasingly popular in clinical practice.
The biological rationale for use of these exercises is that stability and control of the spine is
altered in patients with low back pain. Previous studies have also demonstrated that patients
who recovered from a period of acute low back pain are more vulnerable to recurrence and
chronicity if these changes on the deep abdominal wall muscles, were not treated with motor
control exercise.[1-3] Most researchers have assessed the activity of the transversus abdominis
(TrA) through direct and indirect measures such as fine wire electromyography and
rehabilitative ultrasound imaging. However, these methods have limitations such as high cost
and have the risk of being painful or causing infection which limits the use these equipments
in clinical practice.[4-6] An alternative approach may be the use of an indirect measurement of
muscle activity of TrA by measuring the abdominal wall pressure changes using a specific
instrument known as the pressure biofeedback unit (Stabilizer®, Chattanooga Group Inc.,
Hixson, USA).[7]
It is important that clinical measurements should have acceptable measurement properties.[8]
The most important measurement properties are criterion validity, construct validity,
reproducibility and responsiveness. Criterion validity refers to the extent that scores on an
instrument relate to a gold standard. Construct validity refers to the extent that scores on a
particular instrument relate to other measures that measure the same construct; regardless the
comparator is not a gold standard.[9] Reproducibility could be defined as the degree to which
repeated measurements can provide similar results, and thus is a broad term that includes two
properties: agreement and reliability. Agreement can be defined as the degree to which scores
on repeated measurements are close to each other (absolute measurement error) and reliability

29
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
can be defined as the degree to which individuals can be distinguished from each other,
despite the measurement error (relative measurement error). Reproducibility can be further
divided into two types: intra-examiner which is associated with repeated measurements taken
by the same examiner at different time points and inter-examiner which evaluates the
repetitive measurements taken by different examiners.[9, 10] Finally responsiveness refers to the
ability of an instrument to detect clinically important changes over time, even if these changes
are small.[11]
Although there are some studies[12-17] evaluating the clinimetric properties of measures of
PBU in the muscle activity of the TrA, there is no comprehensive systematic review
summarizing this. The aim of this study was to systematically review studies that evaluated
the measurement properties of the PBU in the activity of the TrA muscle.
METHODS
Data Sources and Searches
We performed systematic searches on PUBMED, CINAHL and BIREME (a comprehensive
database of medical journals published in Portuguese and Spanish languages) over the period
from January 1990 to July 2009. Additionally, hand searches of journals and citation tracking
of reference lists related to PBU were performed. There were no language restrictions and
when necessary non-English papers were translated. The last search was performed on 31st of
July 2009.
The search terms used are described as it follows:

30
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
1. Reliability OR agreement OR validity OR test-retest OR assessment OR evaluation
OR examination OR activation OR contraction OR responsiveness OR sensitivity to
change;
2. Pressure biofeedback unit OR pressure biofeedback OR clinical tests;
3. Transversus abdominis OR abdominal muscle$;
4. 1 AND 2 AND 3.
Study Selection and Eligibility Criteria
Studies were considered eligible for inclusion if they met the following criteria:
1. Used the PBU as a tool for evaluation of muscle activity;
2. Evaluated the activity of the transversus abdominal muscle;
3. Analyzed measurement properties of the PBU;
4. Described the characteristics of the sample;
5. Published in full text in a peer-reviewed journal.
We excluded studies that used the PBU as visual feedback to patients (i.e. we only included
studies that used the PBU as a testing/screening instrument).
Data Extraction and Quality Assessment
The selection of studies, data extraction and quality assessment were performed by two
independent reviewers (P.O.P.L. and R.R.O.), disagreements between reviewers were
resolved by a third reviewer (G.E.C.L.). The items that were extracted from eligible studies
were: (1) description of the sample, (2) presence of LBP, (3) study design, (4) description of
the examiners, (5) the time interval between tests, (6) assessment measures, (7) results and (8)
limitations of the studies. The measurement properties were extracted from the measures of
activity of the TrA muscle.

31
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
The quality of the studies was classified by the items 3, 4 and 5 of the Quality Criteria for
Measurement Properties of Health Status Questionnaires (Table 1).[9] These items evaluate
the study design, as well as the measurement properties values. Although this quality criterion
was developed for the evaluation of measurement properties of questionnaires we considered
it applicable to be used for the current study. This approach has been used in previous reviews
that analyzed not only measurement properties of questionnaires[18, 19], but it was also used by
studies that analyzed the clinimetric properties of measurement instruments such as
rehabilitative ultrasound imaging[20, 21]. We are unaware of a better criterion to evaluate
measurement properties of instruments such as the PBU.
RESULTS
From the search strategy, 193 potentially relevant studies were found. Of these, only 6 studies
were eligible for data analysis (Figure 1).[12-17] Five studies calculated the intra-examiner
reliability,[13-17] two also calculated the inter-examiner reliability,[16, 17] one estimated the
construct validity[13] and one study calculated the criterion validity.[12] It is noteworthy that
one of the studies, in addition to assessing the intra and inter-examiner reliability, also
calculated agreement.[16] Important measurement properties such as responsiveness and
ceiling and floor effects were not evaluated in any study. Due to the heterogeneity of the
eligible studies with regards to the study design and statistical analysis, the pooling of data in
a meta-analysis was not possible. Thus, the results are presented descriptively.

32
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 1: Checklist used to evaluate the clinimetric properties the studies included in the review (adapted from Costa et al. [6] and de Koning et al. [22]).
Clinimetric Properties Definition Quality Criteriaa,b
Reproducibility
(Intra-examiner agreement)
The extent to which the scores on repeated measures are
close to each other (absolute measurement error).
Repeated measures performed by the same examiner.
+ MIC** < SDC OR MIC outside the LOA OR convincing arguments that agreement is acceptable;
? Doubtful design or method OR (MIC not defined AND no convincing arguments that agreement is acceptable);
− MIC > SDC OR MIC equals or inside LOA, despite adequate design and method;
0 No information found on agreement.
Reproducibility
(Inter-examiner agreement)
The extent to which the scores on repeated measures are
close to each other (absolute measurement error).
Repeated measures performed by two or more
examiners.
Reproducibility
(Intra-examiner reliability)
Repeated measures made by the same examiner at
different times, ie refers to the ability of the examiner to
measure the same construct repeatedly.
+ ICC or weighted Kappa > 0.70; ? Doubtful design or method (eg, interval between tests not given,
inadequate description of the ICC); − ICC or weighted Kappa < 0.70, despite adequate design and
method; 0 No information found on reliability.
Reproducibility
(Inter-examiner reliability)
Repeated measures made by different examiners, ie, the
ability of different examiners measuring the same
construct repeatedly.
Criterion Validity The extent to which scores on a particular instrument
relate to a gold standard
+ Convincing arguments that gold standard is ‘‘gold’’ AND correlation with gold standard >0.70;
? No convincing arguments that gold standard is ‘‘gold’’ OR doubtful design or method;
− Correlation with gold standard < 0.70, despite adequate design and method;
0 No information found on criterion validity.
Construct Validity
The extent to which scores on a particular instrument relate to other measures in a manner that is consistent with theoretically derived hypotheses concerning the
concepts that are being measured
+ Specific hypotheses were formulated AND at least 75% of the results are in accordance with these hypotheses;
? Doubtful design or method (e.g., no hypotheses); − Less than 75% of hypotheses were confirmed, despite adequate
design and methods; 0 No information found on construct validity.
a + positive rating, ? indeterminate rating, - negative rating e 0 no information available. b MIC = minimal important change; SDC = smallest detectable change; LOA = limits of agreement; ICC = intraclass correlation coefficient; kappa = kappa coefficient. ** MIC was not considered in the ratings of agreement as MIC is more related to self-report patient outcome measures than physiological measures as PBU.

33
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 2 describes the data that were extracted from eligible studies.
Screening
Included
Eligibility
Iden
tification
Records identified through database searching: PUBMED (n=137), CINAHL
(n=41) and BIREME (n=14)
Additional records identified through other sources
(n=1)
Records after duplicates removed (n=6)
Records screened (n=187)
Records excluded, title (n=173) and abstract (n=5)
Full-text articles assessed for eligibility (n =9)
Full-text articles excluded, because used the PBU as a
feedback tool (n=3)
Studies included in qualitative synthesis
(n =6)
Figure 1: PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of the literature search.

34
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 2: Description of eligible studies.
Eligible studies Description of the sample Presence of low
back pain Clinimetric properties
tested Description of examiners
Time interval between tests
Assessment measures
Hodges et al., 1996 [12]
15 subjects (age 20-24 years, height 1.58-1.91 m, weight 58-85 kg. 9 men and 6
women)
6 subjects with LBP and 9 without LBP
Criterion validity No information No
information
EMG (measured latency TrA-DAa and
peak in 10 sec.) PBU (abdominal
hollowingb
maintained for 10 sec.)
Storheim et al., 2002 [15]
15 subjects (age 22.1 ± 2.45 years and body mass index 22.12 ± 2.1 kg/m2. 7 men
and 8 women)
No Reproducibility (intra-examiner reliability)
A single trained investigator blinded
to the previous measures
7 days Abdominal hollowing (maintained for 8-10
sec.)
Costa et al., 2004 [13] 29 subjects (age 22.7 ± 1.64 years and body mass index
22.82 ± 2.61 kg/m2) No
Reproducibility (intra-examiner reliability) and
Construct Validity
A single trained investigator blinded
to the previous measures
7 days
PBU (Abdominal hollowing maintained
for 8-10 sec.) Palpation test (deep tension maintained
for 10 sec.)
Figueiredo et al., 2005 [17]
31 subjects (age 23 ± 2.87 years, height 1.69 ± 10.4 m and weight 62.5 ± 13 kg)
No Reproducibility (intra and inter-examiner reliability)
2 trained examiners blinded to the
previous measures 7 days
Abdominal hollowing (reference value was obtained at the peak of contraction for 10
sec.)
Costa et al., 2006 [14]
29 subjects (age 22.7 ± 1.64 years, height 1.72 ± 0.09 m and weight 68.09 ± 1.13 kg)
No Reproducibility (intra-examiner reliability)
A single trained examiners blinded to
the previous measures
7 days Abdominal hollowing (maintained for 8-10
sec.)
von Garnier et al., 2009 [16]
40 subjects (age 44 ranging 24-62 years and body mass index 26 ranging 19-45
kg/m2)
Group with individuals who have had LBP
Reproducibility (intra and inter-examiner reliability
and agreement)
3 trained examiners, which are blind to the previous measures
Unclear
Abdominal hollowing (decrease of at least 1 mmHg maintained
for 4-10 sec.) a TrA-AD = transversus abdominal and anterior deltoid muscles; b Abdominal hollowing = voluntary contraction of the TrA muscle in the prone position.

35
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
The results and considerations differed among the eligible studies (Table 3). The ICC
(intraclass correlation coefficient), the kappa (coefficient) and the coefficient of variation
(CV%) were used to analyze the intra and inter-examiner reliability. Agreement was analyzed
by calculating the limits of agreement through Bland and Altman plots. Pearson’s r and
Spearman’s correlation coefficients were used to assess construct and criterion validity. In
regards to intra-examiner reliability, the ICC values ranged from 0.50 to 0.81 and the ICC
values to inter-examiner reliability ranged from 0.47 to 0.82. Correlation values assessing
validity ranged from 0.48 to 0.90.[12, 16] All studies used small sample sizes (ranging from 15
to 40 subjects) and only a pilot study was conducted prior to the main study for the sample
size calculation.[16]

36
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 3: Results and limitations of the studies included in the review.
Eligible studies Results Limitations
Hodges et al., 1996 [12] Spearman's coefficient (r = 0.48 / p <0.07) Fisher's exact test (p <0.006)
Underpowered.
Storheim et al., 2002 [15]
Wilcoxon test (p <0.09) Coefficient of variation (21%) Spearman's coefficient (r = 0.59)
Underpowered.
Costa et al., 2004 [13]
Intra-examiner reliability: ICC2,1 = 0.5 Pearson correlation coefficient (r = 0.5 / p <0.01) Adjusted correlation (r = 0.9 / p <0.01)
The categorizations of the palpation test and of the PBU were not
referenced. Underpowered.
Figueiredo et al., 2005 [17] Intra-examiner reliability: ICC2,1 = 0.71 Inter-examiner reliability: ICC2,1 = 0.82
Lack of CI (95%) for the ICC values Underpowered.
Costa et al., 2006 [14] Intra-examiner reliability: ICC2,1 = 0.58 (95% CI 0.28 to 0.78)
Underpowered.
von Garnier et al., 2009 [16]
Intra-examiner reliability: ICC = 0.81 (95% CI 0.67 to 0.90) and kappa = 0.68 (95% CI 0.35 to 1.00) Inter-examiner reliability: ICC = 0.47 (95% CI 0.20 to 0.68) and kappa = 0.38 (95% CI 0.03 to 0.73) Intra-examiner agreement: no statistical analysis Inter-examiner agreement: differences within the limits of agreement (95% CI)
Underpowered.
* ICC = intraclass correlation coefficient; kappa = kappa coefficient; PBU = pressure biofeedback unit; CI = confidence interval.
Table 4 shows the quality assessment of the 6 eligible studies, summarizing each
as positive; indeterminate; negative or no information. Most of the studies were classified as
negative or indeterminate. All studies classified as negative had insufficient statistical power
(i.e. sample sizes smaller than 50 participants[11, 23]) or had some important methodological
limitations (e.g., inclusion of healthy participants and lack description about examiners).[9, 24]

37
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 4: Summary of assessment of the quality criteria of studies included in the review.a
Eligible studies Intra-examiner Agreement
Inter-examiner Agreement
Intra-examiner Reliability
Inter-examiner Reliability
Criterion Validity
Construct Validity
Hodges et al., 1996
[12]
0 0 0 0 - 0
Storheim et al., 2002 [15]
0 0 - 0 0 0
Costa et al., 2004 [13]
0 0 - 0 0 +
Figueiredo et al., 2005 [17]
0 0 ? ? 0 0
Costa et al., 2006 [14]
0 0 - 0 0 0
von Garnier et al., 2009 [16]
? ? - - 0 0 a + = positive rating, ? = indeterminate rating, - = negative rating, 0 = no information available.
DISCUSSION
This review emphasizes the limitations of existing studies that analyzed the measurement
properties of the PBU as a measurement of the activity of the TrA muscle. Most studies have
assessed the intra-examiner reliability and few have evaluated the inter-examiner reliability
and agreement. This scenario is similar for validity studies; where there are only 2 published
articles: one comparing the PBU with fine wire electromyography and other with palpation
tests.[12, 13] No studies examined responsiveness or ceiling and floor effects.
In general, the quality assessments of the studies were classified as negative, since the
statistical values pre-established as criteria were not met. In relation to methodological

38
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
quality, can be highlighted as weaknesses the inclusion of healthy subjects in most of the
studies and small sample sizes.
The complete process of evaluation of the muscle activity of TrA muscle with the PBU has
several sources of error such as proper positioning of the patient in a prone position on a hard
surface (to minimize deformation of the mattress), the correct positioning of the PBU in the
lower abdomen, the uniform distribution of air in the 3 inflatable bags of the PBU and the
standardization of the verbal command to request the voluntary contraction of the TrA
muscle. It is also questioned whether the material of the bag would be totally inelastic and the
connection between the valve and the bag would be fully adequate to maintain an even
pressure without leakage. Furthermore, it should be acknowledged that normal variations in
the test and retest process can influence the performance of evaluation of muscle activity.
Because of this, it would be useful to examine whether changes in the assessment protocol
could increase the levels of reproducibility of pressure measurements of the PBU. Previous
studies on the reproducibility of measurement instruments for LBP patients have shown that
standardization of the protocol is likely to improve the reliability. [25, 26]
Methodological limitations in the studies may be focused in the sample and the evaluation
protocol. The studies used very small samples and only one study had performed a previous
pilot study.[16] To analyze the clinimetric properties of assessment tools, it is recommended
that a sample of at least 50 individuals[23] or carrying out a pilot study for posterior sample
size calculation.[9] The generalization of the findings from the study samples included in this
systematic review is critically limited because most studies recruited healthy subjects and

39
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
only one selected a mixed sample of patients with LBP and asymptomatic subjects.[12] Future
studies must attempt to these issues rather than testing an equipment in healthy
participants.[27]
The time interval between tests was mentioned in 4 studies as 7 days.[13-15, 17] The time period
between repetitions of the measures should be long enough to avoid the memorization of data
by examiners, but short enough to ensure that there were no clinical changes in the
participants. It is recommended that one or two weeks would be ideal, but there may be
reasons for the choice of another interval.[9]
The most used statistical test for reliability was the Intraclass Correlation Coefficient (ICC) (4
in 6 studies), which is the most appropriate choice to analyze the reliability for continuous
scales.[28] Choosing the best type of ICC depends on several factors, for example, if the
authors want to generalize their results to different examiners or not.[29] Only three studies
described the type of ICC used (type 2,1)[13, 14, 17] One of the studies did not provided the 95%
confidence intervals.[17] Another study used the coefficient of variation (CV%) to assess
reliability,[15] however, this statistical calculation is likely to provide overly optimistic
estimates for reliability, since it does not consider all aspects of the variance.[28, 29]
One study[16] evaluating agreement used Bland and Altman plots, and it was classified as
doubtful because lack of statistical power.[9, 10] The differences between the means of the
examiners were within the limits of agreement in 95% of cases, but as the differences between
repeated measurements (test-retest) were not normally distributed, the limits of agreement
could not be calculated.

40
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
One question that needs to be discussed is that many of the studies reported the reliability of
the average of repeated measurements. Even being an acceptable way to evaluate the
reliability of a measure, ultimately makes the measuring protocol longer. Similarly, it is worth
remembering that some studies used trained examiners, strict control of patient positioning
and selective isolation of the TrA muscle contraction. Although these elements are justifiable
and necessary for the purposes of scientific research, they limit the generalization of data for
clinical practice.[27]
This systematic review provided valuable information for researchers and clinicians on the
use of the PBU as a tool for assessing the activity of the TrA muscle. It is important to
clinicians understand that the current evidence of reproducibility and validity of
measurements taken from the PBU is limited. In addition, researchers must acknowledge that
the most important clinical questions about the measurement properties of the PBU for the
TrA muscle are yet to be answered, and further studies are needed.
Ethical Approval: Not applicable
Conflict of Interest: There are not conflicts of interests.

41
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
REFERENCES
1. O'Sullivan P. Diagnosis and classification of chronic low back pain disorders: maladaptive movement
and motor control impairments as underlying mechanism. Man Ther. 2005 Nov;10(4):242-55.
2. Hodges PW, Richardson CA. Feedforward contraction of transversus abdominis is not influenced by the
direction of arm movement. Exp Brain Res. 1997 Apr;114(2):362-70.
3. Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exercises for first-episode low
back pain. Spine. 2001;26(11):E243-8.
4. Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain with upper
limb movement at different speeds. Arch Phys Med Rehabil. 1999 Sep;80(9):1005-12.
5. Tsao H, Hodges PW. Persistence of improvements in postural strategies following motor control
training in people with recurrent low back pain. J Electromyogr Kinesiol. 2008 Aug;18(4):559-67.
6. Costa LOP, Maher CG, Latimer J, Hodges PW, Shirley D. An investigation of the reproducibility of
ultrasound measures of abdominal muscle activation in patients with chronic non-specific low back pain. Eur
Spine J. 2009 Jul;18(7):1059-65.
7. Chattanooga G, editor. Stabilizer pressure bio-feedback. Operating instructions. Hixson: Chattanooga
Group, Inc.; 2001.
8. May S, Littlewood C, Bishop A. Reliability of procedures used in the physical examination of non-
specific low back pain: a systematic review. Aust J Physiother. 2006;52(2):91-102.
9. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were
proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007 Jan;60(1):34-42.
10. de Vet HC, Terwee CB, Knol DL, Bouter LM. When to use agreement versus reliability measures. J Clin
Epidemiol. 2006 Oct;59(10):1033-9.
11. Terwee CB, Bot SDM, Boer MR, van der Windta DAWM, Knola DL, Dekkera J, et al. Quality criteria were
proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34-42.
12. Hodges P, Richardson C, Jull G. Evaluation of the relationship between laboratory and clinical tests of
transversus abdominis function. Physiother Res Int. 1996;1(1):30-40.
13. Costa LOP, Costa LCM, Cançado RL, Oliveira WM, Ferreira PH. Confiabilidade do teste palpatório e da
unidade de biofeedback pressórico na ativação do músculo transverso abdominal em indivíduos normais. Acta
Fisiatr. 2004;11(3):101-5.
14. Costa LOP, Costa Lda C, Cancado RL, Oliveira Wde M, Ferreira PH. Short report: intra-tester reliability
of two clinical tests of transversus abdominis muscle recruitment. Physiother Res Int. 2006 Mar;11(1):48-50.
15. Storheim K, Bo K, Pederstad O, Jahnsen R. Intra-tester reproducibility of pressure biofeedback in
measurement of transversus abdominis function. Physiother Res Int. 2002;7(4):239-49.
16. von Garnier K, Koveker K, Rackwitz B, Kober U, Wilke S, Ewert T, et al. Reliability of a test measuring
transversus abdominis muscle recruitment with a pressure biofeedback unit. Physiotherapy. 2009 Mar;95(1):8-
14.
17. Figueiredo MK, Chaves Júnior IP, Figueiredo VGC, Costa LOP, Costa LCM. Estudo da confiabilidade intra
e entre-examinadores da unidade de biofeedback pressórico na medida da contração do músculo transverso
abdominal. Rev Bras Cienc Mov. 2005;13(4):93-100.
18. Costa LCM, Maher CG, McAuley J, Costa LOP. Systematic review of cross-cultural adaptations of McGill
pain questionnaire reveals a paucity of clinimetric testing. J Clin Epidemiol. 2009;62(9):934-43.
19. Costa LOP, Maher CG, Latimer J. Self-report outcome measures for low back pain - Searching for
international cross-cultural adaptations. Spine. 2007;32(9):1028-37.
20. Costa LOP, Maher CG, Latimer J, Smeets RJEM. Reproducibility of rehabilitative ultrasound imaging for
the measurement of abdominal muscle activity: a systematic review. Phys Ther. 2009;89(8):756-69.
21. Costa LOP, Maher CG, Latimer J, Hodges PW, Shirley D. An investigation of the reproducibility of
ultrasound measures of abdominal muscle activation in patients with chronic non-specific low back pain. Eur
Spine J. 2009;18(7):1059-65.
22. Altman DG. Practical statistics for medical research. London: Chapman and Hall; 1991.
23. Altman DG, editor. Practical statistics for medical researched. London: Chapman and Hall; 1991.
24. Chiradejnant A, Maher CG, Latimer J. Objective manual assessment of lumbar posteroanterior stiffness
is now possible. J Manipulative Physiol Ther. 2003 Jan;26(1):34-9.

42
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
25. Maher CG, Latimer J, Adams R. An investigation of the reliability and validity of posteroanterior spinal
stiffness judgments made using a reference-based protocol. Phys Ther. 1998 Aug;78(8):829-37.
26. Costa LOP, Maher CG, Latimer J, Smeets RJ. Reproducibility of rehabilitative ultrasound imaging for the
measurement of abdominal muscle activity: a systematic review. Phys Ther. 2009 Aug;89(8):756-69.
27. Fleiss J. Design and Analysis of Clinical Experiments. Inc JWS, editor. New York, NY1986.
28. Armstrong GD. The intraclass correlation as a measure of interrater reliability of subjective judgments.
Nurs Res. 1981 Sep-Oct;30(5):314-5, 20A.
29. de Koning CH, van den Heuvel SP, Staal JB, Smits-Engelsman BC, Hendriks EJ. Clinimetric evaluation of
methods to measure muscle functioning in patients with non-specific neck pain: a systematic review. BMC
Musculoskelet Disord. 2008;9:142.

43
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
3. SEGUNDO ARTIGO
REPRODUCIBILITY OF PRESSURE BIOFEEDBACK UNIT IN THE TRANSVERSUS
ABDOMINIS MUSCLE ACTIVITY IN PATIENTS WITH CHRONIC NONSPECIFIC
LOW BACK PAIN
Artigo original foi submetido para publicação na Physiotherapy Research International
(ANEXO 2).

44
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
REPRODUCIBILITY OF PRESSURE BIOFEEDBACK UNIT IN THE
TRANSVERSUS ABDOMINIS MUSCLE ACTIVITY IN PATIENTS WITH
CHRONIC NONSPECIFIC LOW BACK PAIN
Pedro Olavo de Paula Limaa*, Rodrigo Ribeiro de Oliveiraa, Alberto Galvão de Moura Filhob, Maria Cristina
Falcão Raposoc, Leonardo Oliveira Pena Costad, Glória Elizabeth Carneiro Laurentinob.
a Master's Program in Physical Therapy, Federal University of Pernambuco and Department of
Physiotherapy, Federal University of Ceará, Brazil
b Department of Physiotherapy, Federal University of Pernambuco, Brazil
c Department of Statistic, Federal University of Pernambuco, Brazil
d Master's Program in Physiotherapy, University City of São Paulo, Brazil
* Corresponding Author: Laboratory of Kinesiology and Functional Assessment.
Address: Anibal Fernandes Street, Recife, PE, 50740-560, Brazil.
Telephone: +55 81 21268811 Facsimile: +55 81 21268491
Email: [email protected]
Short title: Reproducibility of pressure biofeedback unit.
Word count: 3.238

45
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ABSTRACT
Background: Pressure Biofeedback Units (PBU) are often used by clinicians and researchers
to indirectly evaluate the transversus abdominis (TrA) muscle activity in patients with low
back pain. Previous studies evaluating the reproducibility of PBU have provided important
information, however some clinically relevant questions have not been fully clarified. Little is
known about the reproducibility of PBU in a clinically relevant sample, with an adequate
sample size and using a standardized assessment protocol.
Objectives: The purpose of this study was to evaluate the reproducibility of PBU in the TrA
muscle activity in patients with chronic nonspecific low back pain.
Methods: Fifty patients with chronic nonspecific low back pain were recruited for this study.
Participants were on average 22 years old, weighed 63.7 kilos, 1.70 meters height and mean
low back pain duration was 1.9 years. To test the inter-examiner reproducibility,
measurements were performed by two physiotherapists and to test the intra-examiner
reproducibility, one of them performed two measures of the TrA muscle activity on two
different occasions with a seven-day interval between tests.
Results: It was observed a Intraclass Correlation Coefficients (ICC2,1) of 0.74 (95%
Confidence Intervals - CI 0.54 to 0.85) and 0.76 (95% CI 0.58 to 0.86) for the intra and inter-
examiner reproducibility, respectively. The intra-examiner agreement (Limits of Agreement -
LOA = 2.1 to -1.8 mmHg) and the inter-examiner agreement (LOA = 2.0 to -1.9 mmHg) were
within the limits of agreement in 95% of occasions. The standard error of measurement
(SEM) was 1.62 mmHg and smallest detectable change (SDC) was 4.49 mmHg.

46
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Conclusion: The reproducibility of PBU in the TrA muscle activity in patients with chronic
nonspecific low back pain ranged from satisfactory to excellent. Other clinimetric properties
(such as validity) of PBU should be an important topic for future investigations
Keywords: pressure biofeedback unit, transversus abdominis muscle, reproducibility,
reliability, agreement.

47
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
INTRODUCTION
The use of motor control exercises (also known as specific stabilization exercises)
has became very popular in clinical practice for the treatment of nonspecific low back pain(1-
4). The rationale for the use of motor control exercises is that the deep muscles of the
abdominal wall have a key role in dynamic control of the lumbar spine(5,6), being observed a
delay in onset of activation of the transversus abdominis (TrA) muscle in patients with
recurrent low back pain compared to asymptomatic controls(5,7).
Most studies that measured the muscle activity of the deep abdominal wall
muscles used fine-wire electromyography(8). However, this type of exam is invasive, painful,
uncomfortable, expensive and may present risks of infection(9,10). Thus, the pressure
biofeedback unit (PBU) has been used as an alternative approach to indirectly measure the
muscle activity(9,11,12). In physiotherapy, PBU is usually used to evaluate the activity of the
abdominal and neck muscles as well as serves as biofeedback tool for patients undertaking
motor control exercise interventions(13).
In order to be useful, PBU measures need to have acceptable clinimetric
properties such as reproducibility. Reproducibility is the degree to which repeated
measurements provide similar results in clinically stable patients and serves as an umbrella
term for reliability and agreement(14). Agreement can be defined as the degree to which scores
on repeated measurements are close to each other (absolute measurement error). Reliability
can be defined as the degree to which individuals can be distinguished from each other,
despite the measurement error (relative measurement error)(14,15).
Previous studies(8,9,16-19) that evaluated the reproducibility of PBU in the TrA
muscle activity answered some, but not all questions about the use of this test to guide the

48
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
clinical management of low back pain, being most of them sampled solely healthy
individuals(9,16-18). Only the studies conducted by Hodges; Richardson and Jull(8) and von
Garnier(19) recruited volunteers with a previous history of back pain. Although some authors
have concluded that PBU provides reproducible measures of the TrA muscle activity, their
results are questionable due to the suboptimal methodological quality, such as small sample
sizes; lack of standardization of the assessment protocol; recruitment of healthy subjects and
insufficient statistical power(9,16-19). Despite the reproducibility of PBU has already been
evaluated in previous studies, lack of consensus among several authors does not allow us to
consider the results as conclusive. Moreover, just few studies sampled participants with low
back pain, which is one of the target conditions for the use of PBU.
Therefore, this study aimed to evaluate the intra and inter-examiner
reproducibility of PBU in the TrA muscle activity in patients with chronic nonspecific low
back pain.
METHODS
This study was performed in a test-retest design(20), and it was carried out at the
Laboratory of Kinesiology and Functional Assessment of the Department of Physiotherapy of
Federal University of Pernambuco, Brazil in 2009.
The sample was selected among students of Federal University of Pernambuco
with chronic nonspecific low back pain. The sample size was estimated based on the
recommendations of specific guidelines on clinimetric properties that suggest a sample of at
least 50 individuals for reproducibility studies(14).

49
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
We included participants with chronic nonspecific low back pain for more than
three months. We excluded participants who had acute low back pain (i.e., an episode of low
back pain of less than 6 weeks), were pregnant, previous abdominal wall or spine surgery,
body mass index (BMI) over 25, were menstruation during the tests and suspected or
confirmed neurological and musculoskeletal pathologies in the pelvis and/or spine.
Participants who missed consecutive tests were also excluded.
Measurements were performed by two physiotherapists in order to test the inter-
examiner reproducibility of PBU. In order to avoid exchanging of information between the
examiners, none of them was present during measurements performed by the other examiner.
For the study of intra-examiner reproducibility, one of examiners conducted two
measurements of the TrA muscle activity on two different occasions, with an interval of seven
days between tests to reduce recall. The examiners were previously trained and were blind to
the measures collected from each other(14).
All participants received basic information about anatomy, biomechanics and
functions of the TrA muscle, as well as on the procedure of testing and training of the TrA
muscle contraction. Selected subjects were previously scheduled to the following instructions:
fasting for 2 hours prior to testing (including water), emptying the bladder immediately before
test and not performing abdominal exercises prior to the tests(9). In both tests, participants and
examiners have adopted the same clinical, environmental and temporal conditions to avoid
external influences or internal errors during data collection. Participants were positioned on
prone position on a hard surface, with lower limbs positioned with feet off the plinth and with
the upper limbs along the body.
Thereafter, the inflatable bag was placed between the anterior superior iliac spine
and navel. Before starting of contraction, the bag was inflated to a pressure of 70 mmHg with

50
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
the valve closed. Participants were instructed to make some deep breaths using mainly the
abdominal wall, then the inflatable bag was adjusted to 70 mmHg again. Patients were
requested to perform three TrA muscle contractions with the following verbal commands
standardized by examiner: "Draw in your abdomen without moving the spine or pelvis".
These contractions were maintained for ten seconds(9) According to the manufacturer of PBU
(Stabilizer®, Chattanooga Group Inc., Hixson, TN, USA), the ability to contract the TrA
muscle results in a pressure reduction from 4 to 10 mmHg, which was recorded by the
pressure gauge of PBU(12) (Figure 1). Thus, based on this information and previous research
on the subject a pressure reduction of at least 4 mmHg was defined as a positive result
(success)(8,9).
Figure 1: Pressure Biofeedback Unit (STABILIZER®).

51
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
All information were recorded using a digital evaluation form provided by
specific software (Miograph®). Pain intensity was measured by the Pain Numerical Rating
Scale and disability was measured by the Roland Morris Disability Questionnaire, both
adapted and clinimetrically tested for Brazilian-Portuguese speakers(21-23).
The sample characteristics was described by using descriptive statistics(24). To
describe the reliability, we used the Intraclass Correlation Coefficient (ICC2,1), ICC values
lower than 0.4 can be classified as poor, values between 0.4 and 0.7 are classified as
satisfactory and over 0.7 are classified as excellent(15). We used three measures of agreement:
Bland and Altman plots(25), Standard Error of the Measurement (SEM) and Smallest
Detectable Change (SDC). The SEM was calculated by dividing the standard deviation of the
mean differences between two measurements by the square root of 2 (SD differences/√2) and
the SDC was calculated using the formula SDC = 1.96 x √2 x SEM. The SEM reflects the
error of the instrument itself and the SDC reflects the smallest within person change in a score
that can be interpreted as a ‘‘real’’ change, above measurement error one of an individual(15).
Data were analyzed with SPSS software (Statistical Package for Social Sciences) version
15.0.
This study was approved by the Research Ethics Committee (# 00490236000-09).
RESULTS
In total, 57 participants were evaluated, of whom seven were excluded for not
attending on second test day, therefore 50 individuals were analyzed.

52
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Sample characteristics are presented in Table 1.
Table 1. Sample characteristics.
VARIABLES Mean (SD)
Gender (N, %) Female 38 (76%)
Male 12 (24%)
Age (years) 22 (2.3)
Low back pain duration (years) 1.9 (3.4)
Weight (kg) 62.7 (12)
Height (m) 1.7 (0.1)
Pain Intensity Numerical Rating Scale (0-10) 5.1 (1.8)
Roland Morris Disability Questionnaire (0-24) 9.1 (5.9)
Examiner A obtained mean pressure values of -4.1 (2.4) mmHg and -4.9 (2.9)
mmHg on first test day (Test 1) and second test day (Test 2), respectively. Examiner B
obtained a mean of -4.7 (3.1) mmHg. The difference between the means of Examiner A (Test
1 - Test 2) was 0.79 (2.3) mmHg with a ICC2,1 = 0.74 (95% CI 0.54 to 0.85). The difference
between the means of two examiners (Examiner A - Examiner B) was -0.14 (2.6) mmHg with
a ICC2,1 = 0.76 (95% CI 0.58 to 0.86). The SEM was 1.62 mmHg and SDC = 4.49 mmHg
(Table 2).

53
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 2. Reliability and agreement for pressure measures.
Measures Mean (SD)
mmHg ICC (95% CI)
SEM
mmHg
SDC
mmHg
PBU Examiner A (Test 1) -4.1 (2.4) -
PBU Examiner A (Test 2) -4.9 (2.9) -
PBU Examiner B -4.7 (3.1) -
Examiner A (Test 1 – Test 2) 0.79 (2.3) 0.74 (0.54 to 0.85) 1.62 4.49
Examiner A – Examiner B -0.14 (2.6) 0.76 (0.58 to 0.86)
* SD= standard deviation; ICC= intraclass correlation coefficient; SEM= standard error of the measurement; SDC= smallest detectable change.
Bland and Altman plots for intra-examiner agreement of Examiner A (test 1 - test
2) showed limits of agreement ranging between 2.1 and -1.8 mmHg (Figure 2). In the case of
inter-examiner agreement for pressure changes, limits of agreement ranged between 2.0 and -
1.9 mmHg, as shown by the Bland and Altman plots (Figure 3).
Figure 2. Bland and Altman plots for pressure measures of Examiner A (test 1 – test 2).

54
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Figure 3. Bland and Altman plots for pressure measures of Examiner A and Examiner B.
DISCUSSION
In this study, the results of measurements of PBU in the TrA muscle activity
during voluntary contraction maneuver in patients with chronic nonspecific low back pain
showed reproducibility indices that ranged from satisfactory to excellent for both the intra-
examiner and inter-examiner.
The use of PBU by physiotherapists as a feedback tool for the evaluation of
patients with chronic nonspecific low back pain has increased over the last decade. In clinical
practice, it is common that a patient is evaluated several times by the same examiner or by
different professionals. Therefore, it is important that measures and instruments used by the
same examiner on different occasions and by different examiners are reproducible(26).
With regards to intra-examiner reliability, the ICC2,1=0.74 reflected an excellent
reliability of the measures of the TrA muscle, similar results were found in most studies in

55
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
literature about the topic(9,17-19). However, this finding was not consensual, given the results
obtained by Storheim et al.(16) which the intra-examiner reliability was considered poor. This
discrepancy may be related to differences in some methodological aspects used in both
studies, as sample size and sample subjects, standardization of breathing during the
assessment protocol and methods of statistical analysis. Storheim et al.(16) recruited a sample
of 15 healthy subjects, did not standardized the breathing during the assessment protocol and
data analysis was performed by the coefficient of variation, unlike the present study that used
the Intraclass Correlation Coefficient.
Likewise, the inter-examiner reliability of PBU achieved excellent results (ICC2,1
= 0.76), corroborating with findings obtained by Figueireiro et al.(17) that found an ICC of
0.82. However, our results were different with the ones obtained by von Garnier et al.(19) with
ICCs ranging from 0.20 to 0.68 (poor to satisfactory).
Although some precautions have been taken in order to reduce the error of
measurements of PBU (extensive training of examiners and the use of the same equipment in
all measurements), different results were observed when compared with some previously
published studies. Perhaps these differences regarding to the reliability of PBU were related to
the different criteria adopted in each study to define how the pressure data would be collected
in evaluation test with the PBU. While Richardson; Hodges and Hides(27) collected a pressure
reduction of 4 to 10 mmHg for 10 seconds, Costa et al.(18) collected only the peak of pressure
reduction maintained for 2 seconds within a period of 10 seconds. Storheim et al.(16) also
recorded the maximum pressure reduction of at least 2 seconds within a period of 8 to 10
seconds. In contrast, von Garnier et al.(19) performed in their data collection a set of four
criteria that participants would have to fulfill for the correct TrA muscle contraction:
continuous breathing, absence of muscle substitution maneuvers, appropriate muscle

56
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
contraction checked by palpation test and pressure reduction of at least 1 mmHg for 4 seconds
within a period of 10 seconds. In summary, it was observed that some authors collected only
peak of muscle contraction while others have collected the most stable values for a certain
time. The results of this study showed that approximately 40% of participants were not able to
achieve positive results, similar to previous studies where it was found that people with a
history of chronic nonspecific low back pain have difficulty to perform a correct contraction
of the TrA muscle(28-30). Cairns et al.(31) evaluating two groups (symptomatic and healthy
subjects) with the PBU noted that pressure results obtained for group of patients with low
back pain were different from those obtained for the group with healthy subjects, confirming
the importance of checking clinimetric properties of PBU in a homogeneous sample
composed of patients with chronic nonspecific low back pain.
Adoption of different criteria for pressure data collection in some studies might
cause a tendency to reduce the reliability of PBU. Considering the information provided by
manufacturer of PBU, the literature and different criteria used in previous studies, the most
appropriate criteria to determine success of this test remain unclear. Furthermore, another fact
to consider is the standardization in the assessment protocol, which has shown to improve the
reproducibility of other processes of evaluation in patients with low back pain(32-34).
Most studies about reproducibility of PBU used seven days as interval period
between tests(9,16-18), same time used in our study. Time periods between the repeated
measurements should be long enough to avoid recall of data by the investigators, but short
enough to ensure there are no clinical changes in the participants(14). However, in all analysis
of assessment instruments it is possible that learning effects influence the results on the
second day of tests. The time interval between the first and second test is also an attempt to
limit this bias in this type of research(35).

57
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
In order to facilitate the comparison of results of this study with the majority of
investigations about clinimetric properties, we decided to estimate the reliability from the
average of three measures. This fact could constitute a potential difficulty in generalizing our
findings because, in clinical practice, is usual to consider simple measures to evaluate with the
PBU. However there is evidence that use of repeated measures is the best way to reduce error
and consequently increase the reproducibility(10,34).
The findings of Bland and Altman plots showed excellent intra-examiner
agreement (Limits of Agreement - LOA = 2.1 to -1.8 mmHg), indicating that measures related
to the first test were in agreement with the second test in 95% of occasions. Similarly, we
found excellent inter-examiner agreement (LOA = 2.0 to -1.9 mmHg), which means that
measures relating to Examiner A were in agreement with the Examiner B in 95% of
occasions. Results showed a SEM of 1.62 mmHg and a SDC of 4.49 mmHg, which means
that the absolute measurement error of PBU is around 1.62 mmHg, and there would need to
be at least an 4.49 mmHg improvement in the TrA muscle activity to make sure that a true
change has occurred(10,15). Although considering agreement values (SEM and SDC) for
pressure measurements, it is important to consider that there is no normative data in the
literature that could allow the determination of the minimal important change (MIC). Ideally
would be that the SDC is smaller than MIC(15), however these values are not available in the
literature.
Influence of breathing in the evaluation of patients with chronic nonspecific low
back pain with PBU was unknown until recently. Lafond et al.(36) investigated this influence
for the clinical assessment of lumbar postural control and concluded that there are significant
differences between pressure measurements collected during breathing and apnea, with higher
values during breathing. They also found that in order to ensure acceptable reliability during

58
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
apnea with ICC=0.8, this requires at least three repeated measures. Thus, how the breathing
might lead to misinterpretation of performance during the test with the PBU, clinicians should
be alert to standardization of assessment protocol during collections. There is a tendency that
participants without guidance as to breathing correctly, to make a TrA muscle contraction
associated with apnea(31). However, it has been demonstrated that data collection performed at
the end of expiratory time, could reduce contamination of results(37).
CONCLUSION
The intra and inter-examiner reproducibility of measures of PBU in the TrA
muscle activity, during voluntary contraction maneuver in patients with chronic nonspecific
low back pain ranged from satisfactory to excellent. It is suggested that other clinimetric
properties (such as validity) of PBU should be an important topic for future investigations.
Conflict of Interest: There are no conflicts of interests.

59
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
REFERENCES
1. Macedo LG, Maher CG, Latimer J, McAuley JH. Motor control exercise for persistent, nonspecific low
back pain: a systematic review. Phys Ther. 2009; 89(1):9-25.
2. Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD, et al. Comparison of general
exercise, motor control exercise and spinal manipulative therapy for chronic low back pain: A randomized trial.
Pain. 2007; 131(1-2):31-7.
3. Ferreira PH, Ferreira ML, Maher CG, Herbert RD, Refshauge K. Specific stabilisation exercise for spinal
and pelvic pain: a systematic review. Aust J Physiother. 2006; 52(2):79-88.
4. Macedo LG, Latimer J, Maher CG, Hodges PW, Nicholas M, Tonkin L, et al. Motor control or graded
activity exercises for chronic low back pain? A randomised controlled trial. BMC Musculoskelet Disord. 2008;
9:65.
5. Hodges PW, Richardson CA. Delayed postural contraction of transversus abdominis in low back pain
associated with movement of the lower limb. J Spinal Disord. 1998; 11(1):46-56.
6. Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low
back pain. A motor control evaluation of transversus abdominis. Spine. 1996; 21(22):2640-50.
7. Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain with upper
limb movement at different speeds. Arch Phys Med Rehabil. 1999; 80(9):1005-12.
8. Hodges P, Richardson C, Jull G. Evaluation of the relationship between laboratory and clinical tests of
transversus abdominis function. Physiother Res Int. 1996; 1(1):30-40.
9. Costa LOP, Costa LCM, Cançado RL, Oliveira WM, Ferreira PH. Confiabilidade do teste palpatório e da
unidade de biofeedback pressórico na ativação do músculo transverso abdominal em indivíduos normais. Acta
Fisiatr. 2004; 11(3):101-5.
10. Costa LOP, Maher CG, Latimer J, Hodges PW, Shirley D. An investigation of the reproducibility of
ultrasound measures of abdominal muscle activation in patients with chronic non-specific low back pain. Eur
Spine J. 2009; 18(7):1059-65.
11. Hodges PW, Pengel LH, Herbert RD, Gandevia SC. Measurement of muscle contraction with ultrasound
imaging. Muscle Nerve. 2003; 27(6):682-92.
12. Chattanooga G, editor. Stabilizer pressure bio-feedback. Operating instructions. Hixson: Chattanooga
Group Inc.; 2005.
13. Cynn HS, Oh JS, Kwon OY, Yi CH. Effects of lumbar stabilization using a pressure biofeedback unit on
muscle activity and lateral pelvic tilt during hip abduction in sidelying. Arch Phys Med Rehabil. 2006;
87(11):1454-8.
14. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were
proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007; 60(1):34-42.
15. de Vet HC, Terwee CB, Knol DL, Bouter LM. When to use agreement versus reliability measures. J Clin
Epidemiol. 2006; 59(10):1033-9.
16. Storheim K, Bo K, Pederstad O, Jahnsen R. Intra-tester reproducibility of pressure biofeedback in
measurement of transversus abdominis function. Physiother Res Int. 2002; 7(4):239-49.
17. Figueiredo MK, Chaves Júnior IP, Figueiredo VGC, Costa LOP, Costa LCM. Estudo da confiabilidade intra
e entre-examinadores da unidade de biofeedback pressórico na medida da contração do músculo transverso
abdominal. Rev Bras Cienc Mov. 2005; 13(4):93-100.
18. Costa LOP, Costa Lda C, Cancado RL, Oliveira Wde M, Ferreira PH. Short report: intra-tester reliability
of two clinical tests of transversus abdominis muscle recruitment. Physiother Res Int. 2006; 11(1):48-50.
19. von Garnier K, Koveker K, Rackwitz B, Kober U, Wilke S, Ewert T, et al. Reliability of a test measuring
transversus abdominis muscle recruitment with a pressure biofeedback unit. Physiotherapy. 2009; 95(1):8-14.
20. Hulley SB, Cumming SR, Browner WS, Grady DG, Newman TB. Delineando a pesquisa científica. Uma
abordagem epidemiológica. 3rd ed. Porto Alegre: Artmed; 2008.
21. Costa LOP, Maher CG, Latimer J. Self-report outcome measures for low back pain: searching for
international cross-cultural adaptations. Spine. 2007; 32(9):1028-37.
22. Maher CG, Latimer J, Costa LOP. The relevance of cross-cultural adaptation and clinimetrics for
physical therapy instruments. Braz J Phys. 2007; 11(4):245-52.

60
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
23. Costa LOP, Maher CG, Latimer J, Ferreira PH, Ferreira ML, Pozzi GC, et al. Clinimetric testing of three
self-report outcome measures for low back pain patients in Brazil: which one is the best? Spine. 2008;
33(22):2459-63.
24. Soares JF, Siqueira AL. Introdução à estatística médica. 2nd ed. Belo Horizonte: Coopmed; 2002.
25. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical
measurement. Lancet. 1986; 1(8476):307-10.
26. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. 3rd ed. Upper
Saddle River: Prentice Hall; 2008.
27. Richardson CA, Hodges PW, Hides JA. Therapeutic exercises for lumbopelvic stabilization. A motor
control approach for the treatment and prevention of low back pain. 2nd ed. Edinburgh: Churchill Livingstone;
2004.
28. Richardson CA, Jull GA. Muscle control-pain control. What exercises would you prescribe? Man Ther.
1995; 1(1):2-10.
29. Hodges PW. Is there a role for transversus abdominis in lumbo-pelvic stability? Man Ther. 1999;
4(2):74-86.
30. Gouveia KMC, Gouveia EC. O músculo transverso abdominal e sua função de estabilização da coluna
lombar. Fisioter Mov. 2008; 21(3):45-50.
31. Cairns MC, Harrison K, Wright C. Pressure biofeedback: a useful tool in the quantification of abdominal
muscular dysfunction? Physiotherapy. 2000; 86(3):127-38.
32. Maher C, Adams R. Reliability of pain and stiffness assessments in clinical manual lumbar spine
examination. Phys Ther. 1994; 74(9):801-9.
33. Maher CG, Latimer J, Adams R. An investigation of the reliability and validity of posteroanterior spinal
stiffness judgments made using a reference-based protocol. Phys Ther. 1998; 78(8):829-37.
34. Chiradejnant A, Maher CG, Latimer J. Objective manual assessment of lumbar posteroanterior stiffness
is now possible. J Manipulative Physiol Ther. 2003; 26(1):34-9.
35. Thomas JR, Nelson JK, Silverman SJ. Research Methods in Physical Activity. 5th ed. Champaign: Human
Kinetics; 2005.
36. Lafond D, Dimmock M, Champagne A, Descarreaux M. Intrasession reliability and influence of
breathing during clinical assessment of lumbar spine postural control. Physiother Theory Pract. 2009;
25(3):218-27.
37. Hodges PW, Richardson CA. Contraction of the abdominal muscles associated with movement of the
lower limb. Phys Ther. 1997; 77(2):132-42.

61
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
4. TERCEIRO ARTIGO
VALIDITY OF PRESSURE BIOFEEDBACK UNIT IN THE TRANSVERSUS
ABDOMINIS MUSCLE ACTIVITY IN PATIENTS WITH CHRONIC NONSPECIFIC
LOW BACK PAIN
Artigo original foi submetido para publicação na Physiotherapy Theory and Practice
(ANEXO 3).

62
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
VALIDITY OF PRESSURE BIOFEEDBACK UNIT IN THE TRANSVERSUS
ABDOMINIS MUSCLE ACTIVITY IN PATIENTS WITH CHRONIC NONSPECIFIC
LOW BACK PAIN
Pedro Olavo de Paula Limaa*, Rodrigo Ribeiro de Oliveiraa, Alberto Galvão de Moura Filhob, Maria Cristina
Falcão Raposoc, Leonardo Oliveira Pena Costad, Glória Elizabeth Carneiro Laurentinob.
a Master's Program in Physical Therapy, Federal University of Pernambuco and Department of
Physiotherapy, Federal University of Ceará, Brazil
b Department of Physiotherapy, Federal University of Pernambuco, Brazil
c Department of Statistic, Federal University of Pernambuco, Brazil
d Master's Program in Physiotherapy, University City of São Paulo, Brazil
* Corresponding Author: Laboratory of Kinesiology and Functional Assessment.
Address: Anibal Fernandes Street, Recife, PE, 50740-560, Brazil.
Telephone: +55 81 21268811 Facsimile: +55 81 21268491
Email: [email protected]

63
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ABSTRACT
Background: Pressure biofeedback unit (PBU) is an assessment tool used in clinical practice
and research to indirectly analyze the transversus abdominis (TrA) muscle activity in patients
with low back pain. Studies investigating the validity of PBU are very scarce. The validity of
PBU in a clinically relevant sample is still unclear.
Objectives: To evaluate the validity of PBU in the TrA muscle activity in patients with
chronic nonspecific low back pain.
Methods: Fifty patients with chronic nonspecific low back pain were recruited for this study.
To test the validity both pressure measures (index test) and superficial electromyographic
measures (reference-standard test) were collected by a physiotherapist from a voluntary
contraction maneuver of TrA muscle.
Results: Participants were on average 22 years old, weighed 63.7 kilos, 1.70 meters height
and mean low back pain duration was 1.9 years. It was observed a weak and non-significant
Pearson correlation coefficient (r=0.2, p<0.20) for the validity. With regards to diagnostic
tests, results suggest a low sensitivity (60%) and specificity (40%) of PBU. The positive
predictive value was high (0.8) and negative predictive value was low (0.2).
Conclusion: The validity of PBU in the TrA muscle activity in patients with chronic
nonspecific low back pain is poor, considering that there is no statistically significant
correlation between pressure data and electromyographic data.
Keywords: pressure biofeedback unit, transversus abdominis, diagnostic tests, validity.

64
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
INTRODUCTION
Low back pain is considered as a major public health problems and is associated
with high socioeconomic costs, work absenteeism and disability(1,2). Usually, acute low back
pain presents a satisfactory outcome and most patients return to their activities between 4-8
weeks, although recurrence is a common finding(3). Approximately 10-40% of cases of low
back pain become chronic and, despite several etiologic factors, most of them (85%) are
classified as nonspecific. Patients who develop chronic nonspecific low back pain (i.e.,
persistent pain and disability for more than three months) are responsible for more than 80%
of health care that are spent for spinal problem(4,5). European guidelines recommend motor
control exercises and spinal manipulative therapy as possible choices for the clinical
management of chronic nonspecific low back pain(6-8).
A delay in the onset of activation of the transversus abdominis (TrA) muscle has
been observed in patients with recurrent low back pain compared to asymptomatic
controls(9,10). In general, one of most used methods for measuring muscle activity of the deep
abdominal wall is fine-wire electromyography. However, some factors such as high cost,
pain, discomfort and risk of infection make the use of this method less accessible in clinical
practice. Thus, other valid instruments that are noninvasive and low cost could be useful to
measure the TrA muscle activity favoring the clinical management of the patients with
chronic nonspecific low back pain(11,12). Accordingly, pressure biofeedback unit (PBU) could
be considered as an alternative approach to indirectly measure the TrA muscle activity(13-15).
It is necessary that pressure measures of the abdominal muscle activity have
minimum validity indices to be useful. Validity is the degree to which the measure represents
the phenomenon of interest, and refers to how much an instrument measures what it would be
supposed to measure(16). Thus, when an instrument undergoes a validation process, in fact is

65
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
not the instrument itself that is being validated, but the purpose for which the instrument is
being used(17). There are four types of validity described in the literature: face, content,
construct and criterion validity. Validity is observed when it evaluates to how much the score
of a particular instrument correlates to other instrument for the same purpose(17-19).
Clinimetric properties of PBU in the TrA muscle activity have been discussed in
previous studies(13,20-24), but most of them sampled solely healthy individuals(13,21-23). Only the
studies conducted by Hodges; Richardson; Jull(20) and von Garnier(24) recruited subjects with a
history of low back pain. Of the six studies, only one(20) investigated the validity and, despite
the authors have concluded that PBU provides valid measures, their findings are questionable
due to the suboptimal methodological quality, such as small sample size (n=15), use of
different motor tasks to assess the TrA muscle activity and insufficient statistical power(20).
Findings from scientific research are more accepted when different studies investigate
the effects of an intervention or test, obtain similar conclusions(25). Thus, clinimetric
properties of the measures should be studied and presented for that the quality of the results
can be evaluated.
Therefore, considering the importance of the use of validated measures that can
support clinical practice and considering the scarce of studies concerning to validation of the
PBU in a clinically relevant sample, the purpose of this study was to evaluate the validity of
PBU in the TrA muscle activity in patients with chronic nonspecific low back pain.

66
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
METHODS
This study was performed as a validation design(26), and it was carried out at the
Laboratory of Kinesiology and Functional Assessment of the Department of Physiotherapy of
Federal University of Pernambuco, Brazil in 2009.
The sample was selected among students of Federal University of Pernambuco
with chronic nonspecific low back pain. The sample size was estimated based on the
recommendations of specific guidelines on clinimetric properties that suggest a sample of at
least 50 individuals for validation studies(18).
We included participants with chronic nonspecific low back pain for more than
three months. We excluded participants who had acute low back pain (i.e., an episode of low
back pain of less than 6 weeks), were pregnant, previous abdominal wall or spine surgery,
body mass index (BMI) over 25, were menstruation during the tests and suspected or
confirmed neurological and musculoskeletal pathologies in the pelvis and/or spine.
All participants received basic information about anatomy, biomechanics and
functions of the TrA muscle, as well as on the procedure of testing and training of TrA muscle
contraction. Selected subjects were previously scheduled to the following instructions: fasting
for 2 hours prior to testing (including water), emptying the bladder immediately before test
and not performing abdominal exercises prior to the tests(13). In both tests, participants and
examiners have adopted the same clinical conditions, environmental and temporal to avoid
external influences or internal errors during data collection. Participants were positioned on
prone position on a hard surface to minimize deformation of the foam.
To test the validity of PBU, surface electromyography (EMG) was considered as
the reference-standard test, based on the findings of previous studies on the topic(27-29) and

67
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
considering the questions of the ethics committees. For all patients, was initially performed
the surface EMG (Miotec® Miotool 400) under the conditions described below. Before
placing the electrodes, detection surfaces were properly cleaned, exfoliated and, when
necessary, a trichotomy was performed following the recommendations of SENIAM (Surface
Electromyography for Non Invasive Assessment of Muscles)(30) to allow a low impedance
between the skin and the electrodes. The bipolar surface electrodes (Ag/AgCl - Meditrace®)
were placed with a distance of 20 mm between their centers, and placed at right side in the
area corresponding to the TrA/OI (transversus abdominis/internal oblique) muscles, located 2
cm the anterior superior iliac spine, following the instructions established by Hodges;
Gandevia; Richardson(29) and adapted by Chanthapetch et al.(28). The reference electrode was
placed in the right lateral epicondyle. Participants were positioned on supine position with
knees flexed to 90°.
The first step was a recording of 30 seconds at rest to detect the parameters of
electromyographic silence (basal tonus). Then, it was performed the protocol of maximal
voluntary isometric contraction (MVIC) in agreement with the standards of SENIAM(30):
three contractions of 5 seconds with intervals of 3 seconds between each contraction, with
three replications (i.e., total of nine contractions). Each individual had one minute of rest
between repetitions. To finish the electromyographic collection was requested a TrA muscle
contraction maintained for 10 seconds. Overall, there were five electromyographic records.
The signs of electrical activity of TrA muscle were collected and transmitted to a monitor that
was connected to the EMG equipment. EMG data were sampled at 1000 Hz over a bandwidth
of 20-450 Hz (band-pass filter). The raw EMG signals generated were analyzed using the root
mean square (RMS). EMG data were normalized by the percentage of MVIC and significant

68
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
electromyographic activity (positive result - success) was defined as an activity at least 10%
of the MVIC(31,32).
After obtaining EMG recordings and respecting an interval of 15 minutes, was
initiated to measure of the TrA muscle activity through the PBU. Participants were positioned
on prone position and the inflatable bag was placed between the anterior superior iliac spine
and navel. Before starting the contraction, the bag was inflated to a pressure of 70 mmHg with
the valve closed. Participants were instructed to breathe deeply using mainly abdominal wall,
then the inflatable bag was adjusted to 70 mmHg again. Patients were requested to perform
three TrA muscle contractions with following verbal commands standardized by examiner:
"Draw in your abdomen without moving the spine or pelvis". These contractions were
maintained for ten seconds(13). According to manufacturer of PBU (Stabilizer®, Chattanooga
Group Inc., Hixson, USA), the ability to contract the TrA muscle results in a pressure
reduction from 4 to 10 mmHg, which was recorded by pressure gauge of PBU(15). Thus, based
on this information and previous research on the subject was defined as a positive result
(success) a pressure reduction of at least 4 mmHg (Figure 1).

69
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Figure1: Pressure Biofeedback Unit (STABILIZER®).
All information was recorded using a digital evaluation form provided by specific
software (Miograph®). Pain intensity was measured by the Numerical Pain Rating Scale and
disability was measured by the Roland Morris Disability Questionnaire, both adapted and
clinimetric tested for Brazilian-Portuguese speakers(33-35).
Description of sample characteristics was performed by using descriptive
statistics(36). To analyze the validity, we used the Pearson Correlation Coefficient, whose
values range from -1 to 1 and if it lower than 0.5 can be classified as weak, values between
0.5 and 0.7 are classified as moderate and over 0.7 are classified as strong correlation(37). The
relationship between the TrA muscle contraction maintained for 10 seconds measured by the
surface EMG (%MVIC) and the scores of pressure reduction measured by the PBU (mmHg)
was the specific hypothesis formulated to analyze the validity. We hypothesized that the PBU
(index test) would have a moderate and positive correlation with the surface EMG (reference-

70
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
standard test)(18,38). Furthermore, we calculated the values of diagnostic tests, such as
sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
Data were analyzed with software SPSS (Statistical Package for Social Sciences) version
15.0, considering the significance level of p<0.05 in all calculations.
This study was approved by the Research Ethics Committee (# 00490236000-09).
RESULTS
Sample characteristics are presented in Table 1.
Table 1. Sample characteristics.
VARIABLES*
Gender (N, %) Female 38 (76%)
Male 12 (24%)
Age (years) 22 (2.3)
Low back pain duration (years) 1.9 (3.4)
Weight (kg) 62.7 (12)
Height (m) 1.7 (0.1)
Pain Intensity Numerical Rating Scale (0-10) 5.1 (1.8)
Roland Morris Disability Questionnaire (0-24) 9.1 (5.9)
* Continuous data are mean (SD).

71
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
The measures performed through the surface EMG and the PBU are presented in
Table 2.
Table 2. Description of the pressure measures and electromyographic measures in the TrA muscle activity.
VARIABLES Mean (SD)
Pressure Measures
PBU (mmHg) - 4.1 (2.4)
Electromyographic Measures
MVIC* (µV) 127.1 (95.5)
MVIC (%) 100
Rest (µV) 2.3 (1.9)
Rest (%) 2.9
Contraction maintained for 10 seconds (µV) 29.6 (21.8)
Contraction maintained for 10 seconds (%) 24.4 * MVIC: maximal voluntary isometric contraction.
According to predetermined criteria to characterize the results as positive
(success), 31 (62%) patients received similar ratings by the two assessment instruments, but
19 (38%) were classified as false-positive (8%) and false-negative (30%), which shows a
weak and non-significant correlation of r=0.2 (p<0.20) between the ratings of PBU and
surface EMG (Table 3).

72
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Table 3. 2x2 Table between the PBU ratings and the surface EMG ratings.
EMG
(reference-standard test)
Positive Negative Total
PBU
(index test)
Positive 25 (50%) 4 (8%) 29 (58%)
Negative 15 (30%) 6 (12%) 21 (42%)
Total 40 (80%) 10 (20%) 50 (100%)*
* Pearson Correlation Coefficient (r=0.2, p<0.20).
Regarding to the diagnostic tests, the results showed low sensitivity (60%), low
specificity (40%), a high PPV (0.8) and a low NPV (0.2) of the PBU.
DISCUSSION
The findings showed a poor validity of PBU in the TrA muscle activity during
voluntary contraction maneuver in patients with nonspecific chronic low back pain. In
scientific research or clinical practice the usefulness of a measure depends on how much we
can rely on the accuracy of your data as indicators of the behavior or the phenomenon
assessed. Ideally, any measurement should be practical, easy to obtain and able to produce
reliable and valid data, since no consistent measures produce unreliable results, leading to
erroneous conclusions(39).
With regards to the correlation between the ratings of PBU and surface EMG, the
high disagreement of 38% showed that the pressure data are not statistically correlated to the
EMG data (r=0.2, p<0.20)(37). Similar results were found by Hodges; Richardson and Jull(20),

73
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
who preliminarily found a no significant correlation between the absolute magnitudes of PBU
and fine-wire EMG (r=0.48, p<0.07) but subsequently showed that the same data, when
converted into an ordinal scale to classify the two measures had high probability of being
correlated. Methodological differences can be used as a possible explanation for these
conflicting results, since in the study by Hodges; Richardson and Jull(20), while the PBU was
used to evaluate the presence of the TrA muscle activity, EMG was used to evaluate the
latency period between the onset of contraction of the TrA and anterior deltoid muscles (i.e.,
the instruments evaluated distinct phenomena). In this study, the two instruments (PBU and
surface EMG) were used to evaluate the same phenomenon (presence of the TrA muscle
activity).
The scarcity of studies investigating the validity of PBU makes it harder to
perform a detailed analysis of our results. Besides the study of Hodges; Richardson and
Jull(20) other research conducted by Costa et al.(13) tried to estimate the construct validity of
PBU in relation to a palpation test, and showed a positive and significant correlation between
the two tests (r=0.99, p<0.01). However, it is observed that their study compared two clinical
tests and did not take into account any laboratory finding, and its results are questioned by
Richardson et al.(40). In 2003, Falla and other researchers(41) found a correlation of 0.56
(p<0.001) between pressure data and electromyographic data (contact electrodes attached to a
suction catheter), but this study was conducted in individuals with chronic nonspecific neck
pain, unlike our sample of chronic low back pain participants.
The possibility of existence of the phenomenon of cross-talk would be a likely
explanation for the weak correlation observed between the instruments, however the
SENIAM(30) assumes that the placement of the surface electrodes could collect the
electromyographic signals from the TrA and OI muscles.

74
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
Among the many factors that can affect the outcome measure, the lack of
standardization of methodology is often referred to as an important source of error. In this
sense, the definition of certain criteria, which may be adopted as a benchmark to be followed,
is essential for a critical assessment as the best evidence available when different studies
investigating the effects of a test(17,25,26). One finding during the development of this study
was the absence of a benchmark for defining what would be considered "positive result" and
"negative result" of the PBU. There is no guidance in the literature in this direction, so that
different criteria were used by several authors(13,20-24,42). This fact may explain, at least as
likely hypothesis, this lack of consensus among studies on the validity of PBU. Considering
the information provided by manufacturer of PBU, the literature and different criteria used in
previous studies, the most appropriate criteria to determine success of this test remain unclear.
Accordingly, it is necessary to establish the criterion of pressure reduction more appropriately
to standardize the PBU test results(17,26,43,44).
Regarding to the diagnostic tests, the results showed a low sensitivity (60%) with
small ability of PBU detecting the TrA muscle activity when it is present, also showed a low
specificity (40%) with small ability of PBU to rule out the TrA muscle activity when it is
absent. Based on these results we can infer that the pressure measures were not sensitive to
discriminate the presence of the TrA muscle activity and were not specific to identify the
absence of the same muscle activity, making questionable the usefulness of PBU to evaluate
the TrA muscle activity in patients with chronic nonspecific low back pain(44,45). With regards
to diagnostic tests, the high PPV (0.8) found, ensures that if result of PBU is positive, the
chance to be a real TrA muscle activity is 80%. While the low NPV (0.2) does not assume
that the negative tests of PBU represent absence of the TrA muscle activity, since if results of
PBU are negative, the chance that there is no TrA muscle activity is only 20%.

75
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
CONCLUSION
Therefore, based on the results observed and the literature, it is emphasized that
there was no evidence sufficient to support the validity of PBU in the TrA muscle activity in
patients with chronic nonspecific low back pain.
Conflict of Interest: There are no conflicts of interests.

76
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
REFERENCES
1. Chou R, Qaseem A, Snow V, Casey D, Cross JT, Jr., Shekelle P, et al. Diagnosis and treatment
of low back pain: a joint clinical practice guideline from the American College of Physicians and the
American Pain Society. Ann Intern Med. 2007; 147(7):478-91.
2. Chou R, Huffman LH. Nonpharmacologic therapies for acute and chronic low back pain: a
review of the evidence for an American Pain Society/American College of Physicians clinical practice
guideline. Ann Intern Med. 2007; 147(7):492-504.
3. Swinkels-Meewisse EJ, Swinkels RA, Verbeek AL, Vlaeyen JW, Oostendorp RA. Psychometric
properties of the Tampa Scale for kinesiophobia and the fear-avoidance beliefs questionnaire in
acute low back pain. Man Ther. 2003; 8(1):29-36.
4. Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD, et al. Comparison
of general exercise, motor control exercise and spinal manipulative therapy for chronic low back
pain: A randomized trial. Pain. 2007; 131(1-2):31-7.
5. Macedo LG, Maher CG, Latimer J, McAuley JH. Motor control exercise for persistent,
nonspecific low back pain: a systematic review. Phys Ther. 2009; 89(1):9-25.
6. Ferreira ML, Ferreira PH, Latimer J, Herbert R, Maher CG. Does spinal manipulative therapy
help people with chronic low back pain? Aust J Physiother. 2002; 48(4):277-84.
7. Macedo LG, Latimer J, Maher CG, Hodges PW, Nicholas M, Tonkin L, et al. Motor control or
graded activity exercises for chronic low back pain? A randomised controlled trial. BMC
Musculoskelet Disord. 2008; 9:65.
8. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al. Chapter 4.
European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006; 15
Suppl 2:S192-300.
9. Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain
with upper limb movement at different speeds. Arch Phys Med Rehabil. 1999; 80(9):1005-12.
10. Hodges PW, Richardson CA. Delayed postural contraction of transversus abdominis in low
back pain associated with movement of the lower limb. J Spinal Disord. 1998; 11(1):46-56.
11. Critchley DJC, F.J. Abdominal muscle function in chronic low-back pain patients:
measurements with real-time ultrasound scanning. Physiotherapy. 2002; 86:322–32.
12. McMeeken JM, Beith ID, Newham DJ, Milligan P, Critchley DJ. The relationship between EMG
and change in thickness of transversus abdominis. Clin Biomech. 2004; 19(4):337-42.
13. Costa LOP, Costa LCM, Cançado RL, Oliveira WM, Ferreira PH. Confiabilidade do teste
palpatório e da unidade de biofeedback pressórico na ativação do músculo transverso abdominal em
indivíduos normais. Acta Fisiatr. 2004; 11(3):101-5.
14. Hodges PW, Pengel LH, Herbert RD, Gandevia SC. Measurement of muscle contraction with
ultrasound imaging. Muscle Nerve. 2003; 27(6):682-92.
15. Chattanooga G, editor. Stabilizer pressure bio-feedback. Operating instructions. Hixson:
Chattanooga Group Inc.; 2005.
16. Fletcher RH, Fletcher SW. Epidemiologia Clínica: elementos essenciais. 4th ed. Porto Alegre:
Artmed; 2006.
17. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. 3rd ed.
Upper Saddle River: Prentice Hall; 2008.
18. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria
were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;
60(1):34-42.
19. Johnston MVK, R. A.; Hinderer, S. R. Measurement Standards for interdisciplinary medical
rehabilitation. Arch Phys Med Rehabil. 1992; 73(12).
20. Hodges P, Richardson C, Jull G. Evaluation of the relationship between laboratory and clinical
tests of transversus abdominis function. Physiother Res Int. 1996; 1(1):30-40.

77
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
21. Storheim K, Bo K, Pederstad O, Jahnsen R. Intra-tester reproducibility of pressure
biofeedback in measurement of transversus abdominis function. Physiother Res Int. 2002; 7(4):239-
49.
22. Costa LOP, Costa Lda C, Cancado RL, Oliveira Wde M, Ferreira PH. Short report: intra-tester
reliability of two clinical tests of transversus abdominis muscle recruitment. Physiother Res Int. 2006;
11(1):48-50.
23. Figueiredo MK, Chaves Júnior IP, Figueiredo VGC, Costa LOP, Costa LCM. Estudo da
confiabilidade intra e entre-examinadores da unidade de biofeedback pressórico na medida da
contração do músculo transverso abdominal. Rev Bras Cienc Mov. 2005; 13(4):93-100.
24. von Garnier K, Koveker K, Rackwitz B, Kober U, Wilke S, Ewert T, et al. Reliability of a test
measuring transversus abdominis muscle recruitment with a pressure biofeedback unit.
Physiotherapy. 2009; 95(1):8-14.
25. Sampaio RF, Mancini MC. Estudos de revisão sistemática: um guia para síntese criteriosa da
evidência científica. Braz J Phys. 2007; 11(1):83-98.
26. Hulley SB, Cumming SR, Browner WS, Grady DG, Newman TB. Delineando a pesquisa
científica. Uma abordagem epidemiológica. 3rd ed. Porto Alegre: Artmed; 2008.
27. Marshall P, Murphy B. The validity and reliability of surface EMG to assess the neuromuscular
response of the abdominal muscles to rapid limb movement. J Electromyogr Kinesiol. 2003;
13(5):477-89.
28. Hodges PWG, S. C.; Richardson, C. A. . Contractions of specific abdominal muscles in postural
tasks are affected by respiratory maneuvers. J Appl Physiol. 1997; 83(3):753-60.
29. Chanthapetch PK, R.; Gaogasigam, C.; Chiradejnant, A. Abdominal muscle activity during
abdominal hollowing in four starting positions. Man Ther. 2009; 14(6):642-6.
30. Hermens HJ, Freiks B. Development of recommendetions for SEMG sensors and sensors
placement procedures. J Electromyogr Kinesiol. 2000; 10(5):361-74.
31. Vasseljen OF, A.; Westad, C.; Torp, H. Onset in abdominal muscles recorded simultaneously
by ultrasound imaging and intramuscular electromyography. J Electromyogr Kinesiol. 2009; 19(2):23-
31.
32. Yang YSK, A.; Triolo, R.; Mercer, J.; Boninger, M. Surface electromyography activity of trunk
muscles during wheelchair propulsion. Clin Biomech. 2006; 21(10):1032-41.
33. Costa LOP, Maher CG, Latimer J. Self-report outcome measures for low back pain: searching
for international cross-cultural adaptations. Spine. 2007; 32(9):1028-37.
34. Maher CG, Latimer J, Costa LOP. The relevance of cross-cultural adaptation and clinimetrics
for physical therapy instruments. Braz J Phys. 2007; 11(4):245-52.
35. Costa LOP, Maher CG, Latimer J, Ferreira PH, Ferreira ML, Pozzi GC, et al. Clinimetric testing
of three self-report outcome measures for low back pain patients in Brazil: which one is the best?
Spine. 2008; 33(22):2459-63.
36. Soares JF, Siqueira AL. Introdução à estatística médica. 2nd ed. Belo Horizonte: Coopmed;
2002.
37. Santos C. Estatística Descritiva: manual de auto-aprendizagem. Lisboa: Sílabo; 2007.
38. Munro H. Statistical Methods for Health Care Research. 5th ed. Philadelphia, PA: Lippincott
Williams & Wilkins; 2005.
39. Gadotti IC, Vieira RR, Magee DJ. Importance and clarification of measurement properties in
rehabilitation. Braz J Phys. 2006; 10(2):137-46.
40. Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation between the
transversus abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine. 2002; 27(4):399-
405.
41. Falla D, Jull G, Dall'Alba P, Rainoldi A, Merletti R. An electromyographic analysis of the deep
cervical flexor muscles in performance of craniocervical flexion. Phys Ther. 2003; 83(10):899-906.

78
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
42. Richardson CA, Hodges PW, Hides JA. Therapeutic exercises for lumbopelvic stabilisation. A
motor control approach for the treatment and prevention of low back pain. 2nd ed. Edinburgh:
Churchill Livingstone; 2004.
43. Rothstein JM. Measurement in Physical Therapy. New York: Churchil Livingstone; 1985.
44. Finch E, Brooks D, Stratford PW, Mayo N. Physical Rehabilitation Outcome Measures. 2nd ed.
Hamilton, Ontario: BC Decker Inc; 2002.
45. Fleiss J, Levin B, Paik M. Statistical methods for rates and proportions. 3rd ed. New York: John
Wiley & Sons; 2003.

79
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
5. CONCLUSÕES
As evidências encontradas, até a realização da revisão sistemática, sobre as
propriedades clinimétricas da UBP na atividade do músculo TrA eram limitadas. Abordagens
metodológicas questionáveis não permitiam que os achados da literatura fossem considerados
conclusivos. As principais restrições para generalização dos resultados observados eram:
tamanho amostral reduzido, falta de padronização do protocolo de avaliação, recrutamento de
indivíduos saudáveis e poder estatístico insuficiente. Estudos avaliando as propriedades
clinimétricas da UBP têm fornecido informações importantes, entretanto algumas questões
clinicamente relevantes ainda não foram totalmente esclarecidas. Pouco se sabe sobre a
reprodutibilidade e validade da UBP em uma amostra de pacientes com dor lombar crônica
inespecífica, com tamanho adequado e protocolo de avaliação padronizado.
As medidas da UBP na atividade do músculo TrA, durante a manobra de
contração voluntária em pacientes com dor lombar crônica inespecífica, apresentaram
reprodutibilidade intra-examinador e inter-examinador variando de satisfatória a excelente.
Na prática clínica, isso significa que um paciente com dor lombar crônica inespecífica pode
ser avaliado por um único fisioterapeuta em momentos distintos. Assim como, esse mesmo
paciente pode ser avaliado por fisioterapeutas diferentes e obter o mesmo diagnóstico
cinesiológico.
As medidas da UBP na atividade do músculo TrA, mediante comparação com os
dados eletromiográficos em pacientes com dor lombar crônica inespecífica, não apresentaram
evidências suficientes que possam comprovar sua validade. Esse achado sugere que a
aplicabilidade clínica da UBP em pacientes com dor lombar crônica inespecífica não é

80
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
indicada. Os critérios de redução pressórica mais adequados para determinar o sucesso
(resultado positivo) do teste com a UBP permanecem obscuros.
Sugere-se para futuras investigações, a determinação de um ponto de corte mais
adequado para avaliar e classificar os resultados obtidos pela UBP.

81
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
APÊNDICE

82
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
APÊNCIDE A
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO.
TÍTULO: PROPRIEDADES CLINIMÉTRICAS DA UNIDADE DE BIOFEEDBACK PRESSÓRICO NA AVALIAÇÃO DA ATIVIDADE MUSCULAR DO TRANSVERSO ABDOMINAL EM PACIENTES COM DOR LOMBAR CRÔNICA INESPECÍFICA.
INVESTIGADOR: Drª. Glória Elizabeth Carneiro Laurentino.
Nome completo do local de estudo: Laboratório de Cinesiologia e Avaliação Funcional / Departamento de Fisioterapia / Universidade Federal de Pernambuco - UFPE.
OBS: Este termo de consentimento pode conter palavras que você não entenda. Por favor, pergunte à equipe que o acompanha no estudo a respeito de quaisquer palavras ou informação que você não entenda claramente. Você receberá uma cópia deste termo de consentimento para seu registro.
INTRODUÇÃO: O (A) Senhor (a) está sendo convidado a participar de um estudo de pesquisa, “PROPRIEDADES CLINIMÉTRICAS DA UNIDADE DE BIOFEEDBACK PRESSÓRICO NA AVALIAÇÃO DA ATIVIDADE MUSCULAR DO TRANSVERSO ABDOMINAL EM PACIENTES COM DOR LOMBAR CRÔNICA INESPECÍFICA”.
OBJETIVOS DO ESTUDO: Durante a prática clínica da fisioterapia, a medida da ativação do músculo transverso abdominal, constitui um dos procedimentos mais utilizados, podendo ser aferida por diferentes métodos e instrumentos, não se observado, no entanto, consenso sobre qual deles seria mais confiável e viável ao mesmo tempo. Assim, este objetiva analisar a reprodutibilidade intra e inter-examinadores e a validade de um aparelho utilizado para medir a ativação dessa musculatura: a unidade de biofeedback pressórico e o eletromiógrafo de superfície.
DURAÇÃO DO ESTUDO: O estudo prevê um período de 2 anos para o desenvolvimento de todas as suas etapas.
DESCRIÇÃO DO ESTUDO: este estudo objetiva analisar a reprodutibilidade de medidas realizadas a partir dos seguintes equipamentos para medir a ativação do músculo transverso abdominal: unidade de biofeedback pressórico e eletromiógrafo de superfície. Poderão participar do estudo indivíduos de todas as idades e de ambos os sexos. As medidas serão feitas com os voluntários em decúbito dorsal e ventral. Na primeira etapa será feita a mensuração com a unidade de biofeedback pressórico e com o eletromiógrafo de superfície, e na segunda etapa repeti-se novamente a mensuração com a unidade de biofeedback pressórico.
RISCOS: Levando em consideração que os voluntários que farão parte da presente investigação não devem apresentar nenhuma anomalia ou descompensação grave; considerando que nenhum dos métodos de mensuração que serão investigados produz algum dano ou malefício ao organismo

83
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
humano e; considerando ainda, que todas as medidas serão feitas a partir de um movimento fisiológico, este trabalho conduz a riscos mínimos aos seus participantes.
BENEFÍCIOS: O fato da medida de ativação do músculo transverso abdominal constituir procedimento usual durante a prática clínica da fisioterapia, os resultados obtidos com a presente investigação poderão melhor nortear os profissionais e as pesquisas científicas na escolha do método ou instrumento a ser empregado.
CONFIDENCIALIDADE: As informações obtidas através desse estudo serão sigilosas, não daremos informações sobre o nome ou outros dados das pessoas que participarem e seus resultados serão divulgados publicamente, sem nenhuma identificação dos voluntários.
PARTICIPAÇÃO VOLUNTÁRIA/RETIRADA: A sua participação nesse estudo é voluntária. Você pode recusar-se a participar ou parar de participar a qualquer momento da pesquisa.
CONSENTIMENTO DO VOLUNTÁRIO: Li e entendi as informações procedentes descrevendo esse estudo, e todas as minhas dúvidas em relação ao estudo e a minha participação nele foram respondidas satisfatoriamente. Dou livremente meu consentimento em participar do estudo até que decida pelo contrário.
Assinando este termo de consentimento, concordo em participar desse estudo e não abro mão, na condição de participante de um estudo de pesquisa, de nenhum dos direitos legais que eu teria de outra forma.
NOME DO VOLUNTÁRIO ASSINATURA DATA
NOME DA TESTEMUNHA ASSINATURA DATA
NOME DA TESTEMUNHA ASSINATURA DATA
NOME DO PESQUISADOR ASSINATURA DATA
Telefones para contato:
Pedro Olavo de Paula Lima: (85) 8864-3219; (81) 9912-1592; (81) 2126-8811
Av: Profº. Moraes Rego, 1235, Cidade Universitária, Departamento de Fisioterapia, CEP: 50670-901
Recife-PE e-mail: [email protected]

84
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXOS

85
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXO 1
TERMO DE SUBMISSÃO PARA PUBLICAÇÃO NA PHYSIOTHERAPY.
Elsevier Editorial System(tm) for Physiotherapy
Manuscript Draft
Manuscript Number:
Title: MEASUREMENT PROPERTIES OF THE PRESSURE BIOFEEDBACK UNIT IN
THE EVALUATION OF TRANSVERSUS ABDOMINIS MUSCLE ACTIVITY: A
SYSTEMATIC REVIEW
Article Type: Systematic Review
Keywords: pressure biofeedback unit; transversus abdominis, reproducibility; validity;
measurement properties; systematic review
Corresponding Author: Dr Leonardo O P Costa, PhD
Corresponding Author's Institution: The George Institute for International Health
First Author: Pedro O Lima
Order of Authors: Pedro O Lima; Rodrigo R de Oliveira; Leonardo O P Costa, PhD; Glória E
Laurentino,PhD
Manuscript Region of Origin: BRAZIL

86
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXO 2
TERMO DE SUBMISSÃO PARA PUBLICAÇÃO NA PHYSIOTHERAPY RESEARCH
INTERNATIONAL.

87
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXO 3
TERMO DE SUBMISSÃO PARA PUBLICAÇÃO NA PHYSIOTHERAPY THEORY
AND PRACTICE.
For Peer Review Only
VALIDITY OF PRESSURE BIOFEEDBACK UNIT IN THE
TRANSVERSUS ABDOMINIS MUSCLE ACTIVITY IN PATIENTS
WITH CHRONIC NONSPECIFIC LOW BACK PAIN
Journal: Physiotherapy Theory and Practice
Manuscript ID: Draft
Manuscript Type: Research Report
Keywords:
pressure biofeedback unit, transversus abdominis muscle, validity,
diagnostic tests

88
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXO 4
ESCALA NUMÉRICA DE DOR (Pain Numerical Rating Scale)
Instruções: Eu gostaria que você desse uma nota para sua dor numa escala de 0 a 10 onde 0 é
nenhuma dor e 10 é a pior dor possível. Por favor, dê um número para descrever sua média de
dor.
0 1 2 3 4 5 6 7 8 9 10
Nenhuma Pior dor possível

89
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXO 5
BRASIL ROLAND MORRIS (Roland Morris Disability Questionnaire)
Instruções: Quando suas costas doem, você pode encontrar dificuldades em fazer algumas
coisas que normalmente faz. Esta lista possui algumas frases que as pessoas tem utilizado
para se descreverem quando sentem dores nas costas. Quando você ler (ou ouvir) estas frases
poderá notar que algumas se destacam por descrever você hoje. Ao ler (ou ouvir) a lista pense
em você hoje. Quando ler ou ouvir uma frase que descreve você hoje, responda sim. Se a
frase não descreve você, então responda não e siga para a próxima frase. Lembre-se, responda
sim apenas à frase que tiver certeza que descreve você hoje.
(sim) (não) 1. Fico em casa a maior parte do tempo por causa de minhas costas.
(sim) (não) 2. Mudo de posição freqüentemente tentando deixar minhas costas confortáveis.
(sim) (não) 3. Ando mais devagar que o habitual por causa de minhas costas.
(sim) (não) 4. Por causa de minhas costas eu não estou fazendo nenhum dos meus trabalhos que geralmente faço em casa.
(sim) (não) 5. Por causa de minhas costas, eu uso o corrimão para subir escadas.
(sim) (não) 6. Por causa de minhas costas, eu me deito para descansar freqüentemente.
(sim) (não) 7. Por causa de minhas costas, eu tenho que me apoiar em alguma coisa para me levantar de uma cadeira normal.

90
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
(sim) (não) 8. Por causa de minhas costas, tento conseguir com que outras pessoas façam as coisas por mim.
(sim) (não) 9. Eu me visto mais lentamente que o habitual por causa de minhas costas.
(sim) (não) 10. Eu somente fico de pé por períodos curtos de tempo por causa de minhas costas.
(sim) (não) 11. Por causa de minhas costas evito me abaixar ou me ajoelhar.
(sim) (não) 12. Encontro dificuldades em me levantar de uma cadeira por causa de minhas costas.
(sim) (não) 13. As minhas costas doem quase o tempo todo.
(sim) (não) 14. Tenho dificuldade em me virar na cama por causa de minhas costas.
(sim) (não) 15. Meu apetite não é muito bom por causa das dores em minhas costas.
(sim) (não) 16. Tenho problemas para colocar minhas meias (ou meia calça) por causa das dores em minhas costas.
(sim) (não) 17. Caminho apenas curtas distâncias por causa de minhas dores nas costas.
(sim) (não) 18. Não durmo tão bem por causa de minhas costas.
(sim) (não) 19. Por causa de minhas costas, eu me visto com ajuda de outras pessoas.
(sim) (não) 20. Fico sentado a maior parte do dia por causa de minhas costas.
(sim) (não) 21. Evito trabalhos pesados em casa por causa de minhas costas.
(sim) (não) 22. Por causa de minhas dores nas costas, fico mais irritado e mal humorado com as pessoas do que o habitual.
(sim) (não) 23. Por causa de minhas costas, eu subo escadas mais vagarosamente do que o habitual.
(sim) (não) 24. Fico na cama a maior parte do tempo por causa de minhas costas.

91
_________________________________________________________________________________________ LIMA, P.O.P. Propriedades Clinimétricas da UBP
ANEXO 6
APROVAÇÃO DO COMITÊ DE ÉTICA EM PESQUISA