VOLUME 70 N.1 JANEIRO/DEZEMBRO 2009 - … · The Hospital Naval Marcílio Dias contributes with a...
84
ARTIGO HISTÓRICO/HISTORICAL ARTICLE A hospitalização dos tuberculosos da Marinha Hospitalization of tuberculosis-infected Navy personnel MEDICINA OPERATIVA/OPERATIONAL MEDICINE A importância de um navio-hospital na MB The importance of a hospital ship at the Brazilian Navy Medicina Operativa: uma especialidade? Operational Medicine: a specialty? ARTIGOS ORIGINAIS/ORIGINAL ARTICLES Analgesia inalatória com óxido nitroso na Clínica de Cirurgia Buco-Maxilo-Facial da Policlínica Naval Nossa Senhora da Glória: análise de 260 casos Nitrous oxide inhalation analgesia at the Oral and Maxillofacial Surgical Clinics of the Policlínica Naval Nossa Senhora da Glória: analysis of 260 cases Avaliação do teor do produto de degradação dissulfeto de captopril em comprimidos de captopril 25mg Assessment study of the degradation product captopril disulfide in 25mg captopril tablets Relação entre esteatose hepática e hepatite C genótipo 3 The association between hepatic steatosis and hepatitis C virus genotype 3 ARTIGO DE REVISÃO/REVIEW ARTICLE Tratamento cirúrgico das complicações mecânicas do infarto agudo do miocárdio Surgical treatment of mechanical complications of acute myocardial infartion RELATO DE CASO/CASE REPORT Micobacteriose cutânea atípica, pós-mesoterapia: infecção por Mycobacterium arupense Atypical cutaneous mycobacteriosis post mesotherapy: infection caused by Mycobacterium arupense VOLUME 70 N.1 JANEIRO/DEZEMBRO 2009
Transcript of VOLUME 70 N.1 JANEIRO/DEZEMBRO 2009 - … · The Hospital Naval Marcílio Dias contributes with a...
Artigo Histórico/HistoricAl Article
A hospitalização dos tuberculosos da MarinhaHospitalization of tuberculosis-infected Navy personnelMedicinA operAtivA/operAtionAl Medicine
A importância de um navio-hospital na MBThe importance of a hospital ship at the Brazilian NavyMedicina Operativa: uma especialidade?Operational Medicine: a specialty?Artigos originAis/originAl Articles
Analgesia inalatória com óxido nitroso na Clínica de Cirurgia Buco-Maxilo-Facial da Policlínica Naval Nossa Senhora da Glória: análise de 260 casosNitrous oxide inhalation analgesia at the Oral and Maxillofacial Surgical Clinics of the Policlínica Naval Nossa Senhora da Glória: analysis of 260 casesAvaliação do teor do produto de degradação dissulfeto de captopril em comprimidos de captopril 25mgAssessment study of the degradation product captopril disulfide in 25mg captopril tabletsRelação entre esteatose hepática e hepatite C genótipo 3The association between hepatic steatosis and hepatitis C virus genotype 3Artigo de revisão/review Article
Tratamento cirúrgico das complicações mecânicas do infarto agudo do miocárdioSurgical treatment of mechanical complications of acute myocardial infartionrelAto de cAso/cAse report
Micobacteriose cutânea atípica, pós-mesoterapia: infecção por Mycobacterium arupenseAtypical cutaneous mycobacteriosis post mesotherapy: infection caused by Mycobacterium arupense
VOLUME 70 N.1 JANEIRO/DEZEMBRO 2009

Anos 30 – No final da década de 30, a revista científica foi criada pelo aviso n° 1.070, do Ministro da
Marinha, o Vice-Almirante Henrique Aristides Guilhem, em 19 de junho de 1939.
Anos 40 – É publicada a primeira edição com nove artigos e 145 páginas. A periodicidade é semestral.
Segunda metade do século XX
Fase da busca pela padronização no processo de editoração dos artigos científicos.
Anos 60 – Os artigos passam a aparecer com resumo, bibliografia consultada e o crédito dos autores.
Anos 70 – A revista passa a incluir introdução,
material & métodos, resultados, discussão e conclusão na sua estrutura. A periodicidade continua irregular.
Anos 80 – A periodicidade passa a ser regular e a revista adquire o formato tradicional - “in octavo”.
Meados de 80 e início de 90 A informatização torna necessária a indexação, para
facilitar a busca e recuperação de artigos.
Final de 90 – O novo padrão na publicação dos artigos científicos obedece aos avanços científicos e
tecnológicos provocados pela globalização.
Anos 2000 – A revista passa a ser editada em duas línguas: português e inglês, para alcançar a indexação
nas bases de dados no mundo científico.
In the 30’s – At the end of the 30’s, the scientific journal was created by Notice no. 1,070 of the Ministry of the Navy, Vice Admiral Henrique Aristides Guilhem, in June 19, 1939.
In the 40’s – The first issue is published with nine articles and 145 pages. It is published bi-annually.
In the second half of the 20th Century Intent to standardize the editing process of scientific articles.
In the 60’s – The articles begins to be published with an abstract, the references and giving credit to authors.
In the 70’s – The journal begins to include the following sections: Introduction, Material & Methods, Results, Discussion and Conclusion. It continues to be irregularly published.
In the 80’s – The journal is regularly published. It is printed in the octavo format.
In the middle of the 80’s and beginning of the 90’s With the use of information technology, indexing becomes vital for the research and retrieval of articles. At the end of the 90’s – The new publishing standard of scientific articles keeps up with the advances in science and technology due to globalization.
In the 2000’s – The journal begins to be published in two languages: Portuguese and English, for the purpose of indexing it in scientific databases.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1) - 3
Editorial
Este é o número especial que a revista Arquivos Bra-sileiros de Medicina Naval apresenta aos seus leito-res, em comemoração ao 160º aniversário do Corpo
de Saúde da Marinha. Compõe-se de um trabalho minucio-so do editor chefe, que selecionou artigos que focam as di-versas nuances das atividades do Corpo de Saúde.
Este ano um importante avanço, certamente decorren-te da maturidade alcançada ao completarmos 160 anos, constituiu-se na ativação de uma Organização Militar que veio representar a nossa atividade operativa, razão da exis-tência do Corpo de Saúde: o Centro de Medicina Operati-va da Marinha. Brindando o acontecimento, o editor chefe destacou dois excelentes artigos relacionados que, juntos a outros, formaram o magnífico conteúdo desta publicação.
Desta forma, agradeço aos autores todo o empenho ob-servado na produção científica colocada à disposição dos leitores, e ao editor chefe pela dedicação de grande parte do seu tempo no acompanhamento da construção deste número especial.
Cumprimento os componentes do Corpo de Saúde da Marinha pela marcante data e, por fim, desejo a todos uma boa leitura, numa profícua viagem pelo espaço de reflexão e conhecimento que é este periódico.
Edson Baltar da Silva
Vice-Almirante (Md)Diretor de Saúde da Marinha
T he journal Arquivos Brasileiros de Medicina Naval presents this commemorative volume in order to celebrate the 160th anniversary of the
Brazilian Navy Medical Corps. It is a detailed work of the chief editor who selected articles that highlight the several nuances of the activities developed by the Medical Corps.The launching this year of a Military Organization – the Centro de Medicina Operativa da Marinha – shows the maturity achieved through the 160 years of existence of the Medical Corps. As part of the celebration, the chief editor brings to our attention two special articles from the wonderful content of this publication.I would like to thank the authors who put their best effort in preparing these scientific articles for our readers, and I would also like to thank the chief editor for his time throughout the process. I congratulate the members of the Navy Medical Corps on this great celebration. Finally, I hope you enjoy the reading. It is intended to take you on a voyage of reflection and knowledge.
Edson Baltar da SilvaVice Admiral (Md)
Navy Health Care Director

4 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1)
Nota do Editor-Chefe
Para dar sequência à publicação da revista Arquivos Brasilei-
ros de Medicina Naval, criada em 1940 pelo Aviso Ministerial
nº 1.070, destacamos, no ano da ativação do Centro de Medi-
cina Operativa da Marinha (CMOpM), dois artigos afetos ao tema: no
primeiro é discutida a Medicina Operativa como uma especialidade
médica desde os primórdios da existência humana e no outro é de-
fendida a discussão da configuração adequada de um navio-hospital
que, efetivamente, seja capaz de apoiar a gama de atividades desen-
volvidas pela Marinha do Brasil.
A Policlínica Naval Nossa Senhora da Glória publica sua
experiência no controle da dor e da ansiedade que normalmente
são associadas ao tratamento odontológico. O Laboratório Far-
macêutico da Marinha discorre sobre a importância da técnica
correta utilizada no controle de qualidade de um medicamento.
O Hospital Naval de Brasília apresenta um caso de micobacterio-
se cutânea atípica, depois de sessão de mesoterapia. O Hospital
Naval Marcílio Dias contribui com um artigo de revisão da Clínica
de Cirurgia Cardíaca, que traz uma atualização sobre as compli-
cações mecânicas do infarto agudo do miocárdio, e a Clínica de
Gastroenterologia busca avaliar, com um artigo original, a asso-
ciação da hepatite C, genótipo 3, com a esteatose hepática atra-
vés de biópsia.
Desde os primórdios da história da Medicina Naval, a
busca em acompanhar a evolução da tecnologia na área da saú-
de foi um dos principais objetivos da Marinha do Brasil. Exemplo
disso é o Pavilhão Carlos Frederico (PCF), inaugurado em 1940,
com 150 leitos, que representava o estado da arte em instalações
destinadas ao tratamento de pacientes portadores de tubercu-
lose pulmonar, uma patologia desafiante para a época. Em vias
da reinauguração do PCF, republicamos um artigo histórico que
faz referência à sua inauguração, no qual são descritos aspectos
curiosos da sua construção diante dos conhecimentos da época.
Àqueles que desejarem, após essa leitura, convido a um passeio
pelo interior do Pavilhão Carlos Frederico para viajar pela história
da nossa Saúde Naval.
Boa leitura.
Roberto E. G. Casella Aversa
Capitão-de-Mar-e-Guerra (Md)
Editor-Chefe
Apresentação/Foreword
Note from the Chief Editor
F ollowing the publication of the journal Arquivos
Brasileiros de Med ic ina Nava l – created in 1940 by the
Ministerial Notice no. 1,070 – in the year in which the Centro
de Medicina Operativa da Marinha (CMOpM) was activated, we point
out two articles related to the theme: the first discusses the Operational
Medicine as a medical specialty since the beginning of human existence.
The other article discusses the appropriate configuration of a hospital
ship that, in fact, can provide support to a range of activities developed
by the Brazilian Navy.
The Policlínica Naval Nossa Senhora da Glória publishes its
experience in anxiety and in pain control in dentistry. The Laboratório
Farmacêutico da Marinha examines the importance of using the
correct technique in medication quality control. The Hospital Naval de
Brasília presents a case of atypical cutaneous mycobacteriosis after
mesotherapy treatment. The Hospital Naval Marcílio Dias contributes
with a review article of the Cardiac Surgery Clinic which brings the
latest on mechanical complications of the acute myocardium. Finally,
the Gastroenterology Clinic evaluates, with an original article, the
association of hepatitis C, genotype 3, with the hepatic steatosis
through biopsy.
Since the beginning of the Naval Medicine history, one of the main
objectives of the Brazilian Navy has been the pursuing of the latest
technology in the field of Health. An example of that is the Pavilhão
Carlos Frederico (PCF), inaugurated in 1940, with 150 beds, a state-
of-art facility designed to patients with pulmonary tuberculosis, a
challenging disease for that time. We here reprint a historical article
from the inauguration of the PCF that describes some interesting
aspects of its building from that time period. After this reading, I want to
invite you to a tour of the Pavilhão Carlos Frederico to a travel through
the history of the Brazilian Naval Health.
Enjoy the reading.
Roberto E. G. Casella Aversa
Captain (Md)
Chief Editor

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1) - 5
ARQUIVOS BRASILEIROS DE MEDICINA NAVALPUBLICAÇÃO SEMESTRAL DA DIRETORIA DE SAÚDE DA MARINHA
DIREÇÃOEDSON BALTAR DA SILVAVice-Almirante (Md) – Diretor de Saúde da MarinhaEditor-ChefeROBERTO EDUARDO GOMES CASELLA AVERSACapitão-de-Mar-e-Guerra (Md)SecretáriaCARLA CALLEGÁRIO REIS BASTOSCapitão-de-Fragata (S)BibliotecáriaJANE VITÓRIA QUEIRÓZ GUZMÁNServidora Civil
Criada pelo Aviso Ministerial nº 1.070, de 19 de junho de 1939, do Exmº Sr. Ministro da Marinha, Vice-Almirante Henrique Aristides Guilhem, sendo Diretor Geral de Saú-de Naval, o Contra-Almirante (Md) Otávio Joaquim Tosta da Silva.O Título desta revista foi registrado no Departamento Nacional de Propriedade In-dustrial do Ministério do Trabalho, Indústria e Comércio, conforme termo de depósito número 247.731, de 15 de junho de 1953, e no Registro Civil das Pessoas Jurídi-cas (Vara de Registro Público do Distrito Federal), sob o número 635, no livro “B”, número 1 de matrícula de oficinas impressas, jornais e outros periódicos, em 15 de junho de 1953.
Redação e AdministraçãoDIRETORIA DE SAÚDE DA MARINHAPraça Barão de Ladário – Complexo do 1ºDN S/NºCentro – Rio de Janeiro – Brasil – Tel: (21) 2253-6333
COMANDANTE DA MARINHAAlmirante-de-Esquadra JULIO SOARES DE MOURA NETO
DIRETOR–GERAL DO PESSOAL DA MARINHAAlmirante-de-Esquadra JOSÉ ANTONIO DE CASTRO LEAL
DIRETOR DE SAÚDE DA MARINHAVice-Almirante (Md) EDSON BALTAR DA SILVA
ARQUIVOS BRASILEIROS DE MEDICINA NAVALCONSELHO CONSULTIVOCELSO BARBOSA MONTENEGROContra-Almirante (Md) – Diretor do Hospital Naval Marcílio DiasPAULO CESAR DE ALMEIDA RODRIGUESContra-Almirante (Md) – Diretor do Centro de Medicina Assistencial da MarinhaJOÃO CARLOS GONÇALVES DA MOTTA FILHOContra-Almirante (Md) – Diretor do Centro de Perícias Médicas da MarinhaSÉRGIO PEREIRAContra-Almirante (Md) – Diretor do Centro de Medicina Operativa da Marinha
CONSELHO CIENTÍFICOContra-Almirante (Md-RM1) EIMAR DELLY DE ARAÚJOCapitão-de-Mar-e-Guerra (Md) WALMIR DE ALMEIDA AUGUSTOCapitão-de-Mar-e-Guerra (Md) BRUNO RIGUEIRA GEORGCapitão-de-Mar-e-Guerra (Md) ROSA REGINA SANNUTI PAIS Capitão-de-Mar-e-Guerra (Md) LUÍS FERNANDO LOPESCapitão-de-Mar-e-Guerra (Md) EDSON BENTO NASCIMENTO DA SILVA Capitão-de-Mar-e-Guerra (Md) HELDER MOREIRA FILHOCapitão-de-Mar-e-Guerra (Md) MARCO ANTONIO GOMES DE FREITASCapitão-de-Mar-e-Guerra (Md) CARLOS HENRIQUE F. RIBEIRO DA SILVACapitão-de-Fragata (Md) SÉRGIO ROBERTO FERNANDESCapitão-de-Fragata (Md) ANDRÉ GERMANO DE LORENZICapitão-de-Fragata (Md) CARLOS EDUARDO DE LOUREIRO ARAUJOCapitão-de-Fragata (Md) JOSÉ EDMILSON FERREIRA DA SILVA Capitão-de-Fragata (T) ROSANGELA COUTAS DE FIGUEIREDOCapitão-de-Fragata (S) LILA CARLA GOMES MARINS FÉRES
Produção gráfica: MP GRÁFICATel.: (21) 3411-2445
Diretor de Arte: Luiz Antonio
BRAZILIAN ARCHIVES OF NAVAL MEDICINEBIANNUAL PUBLICATION OF THE NAVY HEALTH CARE DIVISION
DIRECTOR’S OFFICEEDSON BALTAR DA SILVAVice Admiral (Md) – Navy Health Care DirectorChief EditorROBERTO EDUARDO GOMES CASELLA AVERSACaptain (Md)SecretaryCARLA CALLEGÁRIO REIS BASTOSCommander (S)LibrarianJANE VITÓRIA QUEIRÓZ GUZMÁNCivilian public servant
The Brazilian Archives of Naval Medicine was created on July 19th, 1939 by the Ministe-rial Notice no. 1.070 of the Brazilian Ministry of the Navy, Vice Admiral Henrique Aristides Guilhem, being Rear Admiral (Md) Otávio Joaquim Tosta da Silva the Navy Health Director.The title of this journal was registered with the National Department of Intellectual Property of the Ministry of Labor, Industry and Commerce, according to the filing term number 247.731, as of June 15th, 1953, and with the Civil Registry Office of Legal Entities (Public Court of Registry of the Federal District), under number 635, in book “B”, bearing the number 1 of enrollment for printed workshops, newspapers and other journals, on June 15th, 1953.
Press Office and AdministrationNAVY HEALTH DIRECTOR’S OFFICEPraça Barão de Ladário – Complexo do 1ºDN S/NºCentro – Rio de Janeiro – Brazil – Phone number: (55) (21) 22536333
COMMANDER OF THE BRAZILIAN NAVYAdmiral JULIO SOARES DE MOURA NETO
CHIEF OF THE NAVY STAFFAdmiral JOSÉ ANTONIO DE CASTRO LEAL
NAVY HEALTH CARE DIRECTORVice-Admiral (Md) EDSON BALTAR DA SILVA
BRAZILIAN ARCHIVES OF NAVAL MEDICINEADVISORY BOARDCELSO BARBOSA MONTENEGRORear Admiral (Md) – Director of the Hospital Naval Marcílio DiasPAULO CESAR DE ALMEIDA RODRIGUESRear Admiral (Md) – Director of the Navy Medical Care CenterJOÃO CARLOS GONÇALVES DA MOTTA FILHORear Admiral (Md) – Director of the Navy Medical Examination CenterSÉRGIO PEREIRARear Admiral (Md) – Director of the Naval Operational Medicine Center
SCIENTIFIC BOARDRear Admiral (Md-RM1) EIMAR DELLY DE ARAÚJOCaptain (Md) WALMIR DE ALMEIDA AUGUSTOCaptain (Md) BRUNO RIGUEIRA GEORGCaptain (Md) ROSA REGINA SANNUTI PAIS Captain (Md) LUIS FERNANDO LOPESCaptain (Md) EDSON BENTO NASCIMENTO DA SILVACaptain (Md) HELDER MOREIRA FILHOCaptain (Md) MARCO ANTONIO GOMES DE FREITASCaptain (Md) CARLOS HENRIQUE F. RIBEIRO DA SILVACommander (Md) SÉRGIO ROBERTO FERNANDESCommander (Md) ANDRÉ GERMANO DE LORENZICommander (Md) CARLOS EDUARDO DE LOUREIRO ARAUJOCommander (Md) JOSÉ EDMILSON FERREIRA DA SILVA Commander (T) ROSANGELA COUTAS DE FIGUEIREDOCommander (S) LILA CARLA GOMES MARINS FÉRES
Graphic production: MP GRÁFICAPhone number: (55) (21) 3411-2445
Art director: Luiz Antonio
Expediente Masthead

6 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1)
Sumário
Artigo Histórico
A hospitalização dos tuberculosos da Marinha 8
MedicinA operAtivA
Medicina Operativa: uma especialidade? 14CT (Md) Hemerson dos Santos Luz; CA (Md) Sérgio Pereira
A importância de um navio-hospital na MB 24CT (Md) Hemerson dos Santos Luz
Artigos originAis
Analgesia inalatória com óxido nitroso na Clínica de Cirurgia Buco-Maxilo-Facial da Policlínica Naval Nossa Senhora da Glória: análise de 260 casos 32CF (CD) Marcelo Rosado Botelho, M.D.; CMG (Md-RM1) Maryangela Foroni Monteiro; CT (CD) Guilherme Lima Pontes; 1ºT (CD) Sanny Alessandra Gonçalves de Noronha; 1ºT (CD) Emanuela Prado Ferraz; Lilia Regina Paiva
Avaliação do teor do produto de degradação dissulfeto de captopril em comprimidos de captopril 25mg 401ºT (S) Robson Marques Gouvêa; CC (S) Marco Antônio Arruda; CC (S) Ruben dos Santos; Armando Lucas Cherem da Cunha, M.D.
Relação entre esteatose hepática e hepatite C genótipo 3 54CT (Md) Priscila Pollo Flores, M.D.; CC (Md) Maria Fernanda Mascalubo Monteiro; CF (Md) Carlos Eduardo Ferreira Mesquita; CF (Md) José Edmilson Ferreira da Silva
Artigo de revisão
Tratamento cirúrgico das complicações mecânicas do infarto agudo do miocárdio 62CMG (Md-RM1) Hermes de Souza Felippe; CT (Md) Marcos Floripes da Silva; Eduardo Sérgio Bastos, M.D., Ph.D. relAto de cAso
Micobacteriose cutânea atípica, pós-mesoterapia: infecção por Mycobacterium arupense 761ºT (S-RM2) Fernanda Mendes Pereira Müller, M.D.; Maria Letícia dos Santos Cabral; CF (Md) Lásaro Pereira de Melo
norMAs pArA publicAção 82

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1) - 7
Table of contents
HistoricAl Article
Hospitalization of tuberculosis-infected Navy personnel 11
operAtionAl Medicine
Operational Medicine: a specialty? 19CT (Md) Hemerson dos Santos Luz; CA (Md) Sérgio Pereira
The importance of a hospital ship at the Brazilian Navy 28CT (Md) Hemerson dos Santos Luz
originAl Articles
Nitrous oxide inhalation analgesia at the Oral and Maxillofacial Surgical Clinics of the Policlínica Naval Nossa Senhora da Glória: analysis of 260 cases 36CF (CD) Marcelo Rosado Botelho, M.D.; CMG (Md-RM1) Maryangela Foroni Monteiro; CT (CD) Guilherme Lima Pontes; 1ºT (CD) Sanny Alessandra Gonçalves de Noronha; 1ºT (CD) Emanuela Prado Ferraz; Lilia Regina Paiva
Assessment study of the degradation product captopril disulfide in 25mg captopril tablets 471ºT (S) Robson Marques Gouvêa; CC (S) Marco Antônio Arruda; CC (S) Ruben dos Santos; Armando Lucas Cherem da Cunha, M.D.
The association between hepatic steatosis and hepatitis C virus genotype 3 58CT (Md) Priscila Pollo Flores, M.D.; CC (Md) Maria Fernanda Mascalubo Monteiro;CF (Md) Carlos Eduardo Ferreira Mesquita; CF (Md) José Edmilson Ferreira da Silva
review Article
Surgical treatment of mechanical complications of acute myocardial infartion 69CMG (Md-RM1) Hermes de Souza Felippe; CT (Md) Marcos Floripes da Silva; Eduardo Sérgio Bastos, M.D., Ph.D.
cAse report
Atypical cutaneous mycobacteriosis post mesotherapy: infection caused by Mycobacterium arupense 791ºT (S-RM2) Fernanda Mendes Pereira Müller, M.D.; Maria Letícia dos Santos Cabral; CF (Md) Lásaro Pereira de Melo
guidelines for publicAtion 82
8 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 8-10
O problema da hospitalização dos marinheiros tuberculo-sos tem sido motivo de sérias preocupações das altas autoridades navais, nos últimos anos. Localizados primi-tivamente na Enfermaria Auxiliar em Copacabana, a tí-
tulo provisório, ali foram eles ficando por muitos anos, por falta de um outro lugar apropriado para onde transferi-los, não obstante todos con-cordarem que aquela situação precária precisava ser resolvida com urgência. O local era impróprio e os barracões de madeira que ser-viam para abrigá-los, além dos inconvenientes naturais do material de construção, caminhavam aceleradamente para a ruína e ninguém se atrevia a repará-los, porque todos opinavam que era preciso retirar da-li os doentes o mais depressa possível. Faltava, porém, a iniciativa, o impulsionador da idéia.
Na administração do Vice-Almirante Protogenes Guimarães, nos terrenos do Sanatório Naval de Friburgo, foi construído um pavilhão para os tuberculosos que necessitassem de clima de altitude.
Copacabana, porém, continuou...Foi, então, que o atual Ministro Vice-Almirante Aristides Guilhem
resolveu dar o golpe decisivo. Comprou um terreno anexo ao Instituto Naval de Biologia e ali fez construir o
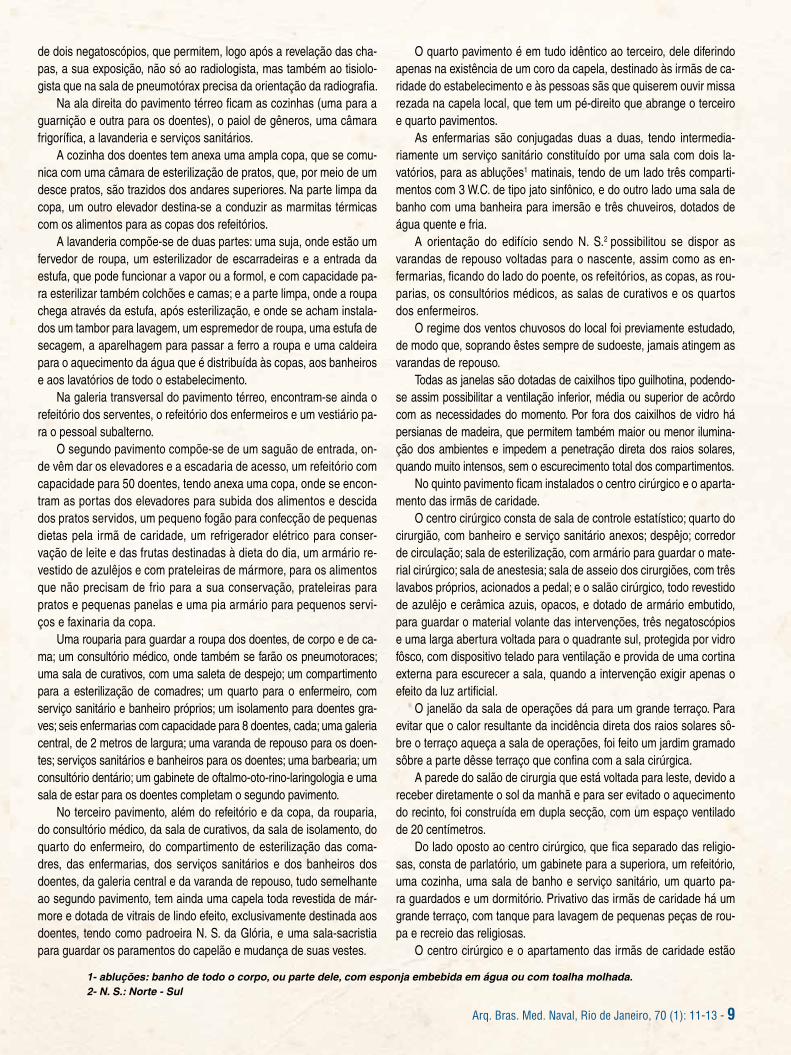
PAVILHÃO DR. CARLOS FREDERICOÉ um bloco de cimento armado e alvenaria, de cinco pavimen-
tos, dos quais três são destinados ao alojamento dos doentes (ex-clusivamente tuberculosos), um aos serviços auxiliares e outro ao centro cirúrgico e à residência das irmãs de caridade que servem no estabelecimento.
No pavimento térreo encontram-se o saguão de entrada, tendo à esquerda a sala do médico de serviço, em conexão com o refeitório, a sala de banho e o dormitório dos médicos; à direita a secretaria e o apartamento do enfermeiro-mor, constante de dormitório e serviço sa-nitário (W.C., lavatório e chuveiro, com água quente e fria).
De cada lado do saguão há um balcão de mármore, semi-circu-lar, com armários internos, destinados ao expediente do enfermeiro-mor e do enfermeiro de dia, que ali ficam em comunicação com todo o estabelecimento, pela sinalização luminosa e pela instalação inter-na de telefone.
O saguão de entrada comunica-se com uma galeria que corta o edifício no sentido transversal, cruzando-se com uma galeria longitudi-nal, exatamente no centro do bloco. Na galeria transversal encontram-se dois elevadores e uma escadaria de mármore, que conduzem aos pavimentos superiores.
Na ala esquerda do pavimento térreo ficam localizados os serviços de raios X e planigrafia, os aparelhos de fisioterapia, em sala própria, o ambulatório e a sala de pneumotórax controlado aos raios X, o ga-binete de interpretação do radiologista, uma sala de espera para os doentes e um serviço sanitário para os mesmos.
A secção de radiologia compreende uma sala de exame, com dois modernos aparelhos de radiodiagnóstico: para radiologia e radiografia para planigrafia. Anexos temos uma câmara escura, uma sala para de-pósito de material em uso e uma outra para arquivo. Todo o conjunto acha-se protegido por paredes forradas de chumbo e revestidas de madeira e a câmara escura é dotada de um sistema de sinalização e
A HOSPITALIZAÇÃO DOS TUBERCULOSOS DA MARINHA
Pavilhão Dr. Carlos Frederico - 1940
ARTIGO HISTÓRICO
Publicado inicialmente nos Arq. Bras. Med. Naval. Jul. 1940; 1 (3)
8 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 8-10
Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 11-13 - 9
de dois negatoscópios, que permitem, logo após a revelação das cha-pas, a sua exposição, não só ao radiologista, mas também ao tisiolo-gista que na sala de pneumotórax precisa da orientação da radiografia.
Na ala direita do pavimento térreo ficam as cozinhas (uma para a guarnição e outra para os doentes), o paiol de gêneros, uma câmara frigorífica, a lavanderia e serviços sanitários.
A cozinha dos doentes tem anexa uma ampla copa, que se comu-nica com uma câmara de esterilização de pratos, que, por meio de um desce pratos, são trazidos dos andares superiores. Na parte limpa da copa, um outro elevador destina-se a conduzir as marmitas térmicas com os alimentos para as copas dos refeitórios.
A lavanderia compõe-se de duas partes: uma suja, onde estão um fervedor de roupa, um esterilizador de escarradeiras e a entrada da estufa, que pode funcionar a vapor ou a formol, e com capacidade pa-ra esterilizar também colchões e camas; e a parte limpa, onde a roupa chega através da estufa, após esterilização, e onde se acham instala-dos um tambor para lavagem, um espremedor de roupa, uma estufa de secagem, a aparelhagem para passar a ferro a roupa e uma caldeira para o aquecimento da água que é distribuída às copas, aos banheiros e aos lavatórios de todo o estabelecimento.
Na galeria transversal do pavimento térreo, encontram-se ainda o refeitório dos serventes, o refeitório dos enfermeiros e um vestiário pa-ra o pessoal subalterno.
O segundo pavimento compõe-se de um saguão de entrada, on-de vêm dar os elevadores e a escadaria de acesso, um refeitório com capacidade para 50 doentes, tendo anexa uma copa, onde se encon-tram as portas dos elevadores para subida dos alimentos e descida dos pratos servidos, um pequeno fogão para confecção de pequenas dietas pela irmã de caridade, um refrigerador elétrico para conser-vação de leite e das frutas destinadas à dieta do dia, um armário re-vestido de azulêjos e com prateleiras de mármore, para os alimentos que não precisam de frio para a sua conservação, prateleiras para pratos e pequenas panelas e uma pia armário para pequenos servi-ços e faxinaria da copa.
Uma rouparia para guardar a roupa dos doentes, de corpo e de ca-ma; um consultório médico, onde também se farão os pneumotoraces; uma sala de curativos, com uma saleta de despejo; um compartimento para a esterilização de comadres; um quarto para o enfermeiro, com serviço sanitário e banheiro próprios; um isolamento para doentes gra-ves; seis enfermarias com capacidade para 8 doentes, cada; uma galeria central, de 2 metros de largura; uma varanda de repouso para os doen-tes; serviços sanitários e banheiros para os doentes; uma barbearia; um consultório dentário; um gabinete de oftalmo-oto-rino-laringologia e uma sala de estar para os doentes completam o segundo pavimento.
No terceiro pavimento, além do refeitório e da copa, da rouparia, do consultório médico, da sala de curativos, da sala de isolamento, do quarto do enfermeiro, do compartimento de esterilização das coma-dres, das enfermarias, dos serviços sanitários e dos banheiros dos doentes, da galeria central e da varanda de repouso, tudo semelhante ao segundo pavimento, tem ainda uma capela toda revestida de már-more e dotada de vitrais de lindo efeito, exclusivamente destinada aos doentes, tendo como padroeira N. S. da Glória, e uma sala-sacristia para guardar os paramentos do capelão e mudança de suas vestes.
O quarto pavimento é em tudo idêntico ao terceiro, dele diferindo apenas na existência de um coro da capela, destinado às irmãs de ca-ridade do estabelecimento e às pessoas sãs que quiserem ouvir missa rezada na capela local, que tem um pé-direito que abrange o terceiro e quarto pavimentos.
As enfermarias são conjugadas duas a duas, tendo intermedia-riamente um serviço sanitário constituído por uma sala com dois la-vatórios, para as abluções1 matinais, tendo de um lado três comparti-mentos com 3 W.C. de tipo jato sinfônico, e do outro lado uma sala de banho com uma banheira para imersão e três chuveiros, dotados de água quente e fria.
A orientação do edifício sendo N. S.2 possibilitou se dispor as varandas de repouso voltadas para o nascente, assim como as en-fermarias, ficando do lado do poente, os refeitórios, as copas, as rou-parias, os consultórios médicos, as salas de curativos e os quartos dos enfermeiros.
O regime dos ventos chuvosos do local foi previamente estudado, de modo que, soprando êstes sempre de sudoeste, jamais atingem as varandas de repouso.
Todas as janelas são dotadas de caixilhos tipo guilhotina, podendo-se assim possibilitar a ventilação inferior, média ou superior de acôrdo com as necessidades do momento. Por fora dos caixilhos de vidro há persianas de madeira, que permitem também maior ou menor ilumina-ção dos ambientes e impedem a penetração direta dos raios solares, quando muito intensos, sem o escurecimento total dos compartimentos.
No quinto pavimento ficam instalados o centro cirúrgico e o aparta-mento das irmãs de caridade.
O centro cirúrgico consta de sala de controle estatístico; quarto do cirurgião, com banheiro e serviço sanitário anexos; despêjo; corredor de circulação; sala de esterilização, com armário para guardar o mate-rial cirúrgico; sala de anestesia; sala de asseio dos cirurgiões, com três lavabos próprios, acionados a pedal; e o salão cirúrgico, todo revestido de azulêjo e cerâmica azuis, opacos, e dotado de armário embutido, para guardar o material volante das intervenções, três negatoscópios e uma larga abertura voltada para o quadrante sul, protegida por vidro fôsco, com dispositivo telado para ventilação e provida de uma cortina externa para escurecer a sala, quando a intervenção exigir apenas o efeito da luz artificial.
O janelão da sala de operações dá para um grande terraço. Para evitar que o calor resultante da incidência direta dos raios solares sô-bre o terraço aqueça a sala de operações, foi feito um jardim gramado sôbre a parte dêsse terraço que confina com a sala cirúrgica.
A parede do salão de cirurgia que está voltada para leste, devido a receber diretamente o sol da manhã e para ser evitado o aquecimento do recinto, foi construída em dupla secção, com um espaço ventilado de 20 centímetros.
Do lado oposto ao centro cirúrgico, que fica separado das religio-sas, consta de parlatório, um gabinete para a superiora, um refeitório, uma cozinha, uma sala de banho e serviço sanitário, um quarto pa-ra guardados e um dormitório. Privativo das irmãs de caridade há um grande terraço, com tanque para lavagem de pequenas peças de rou-pa e recreio das religiosas.
O centro cirúrgico e o apartamento das irmãs de caridade estão
1- abluções: banho de todo o corpo, ou parte dele, com esponja embebida em água ou com toalha molhada.2- N. S.: Norte - Sul

10 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 8-10
protegidos dos raios solares por uma cobertura de telhas francesas, tendo sido aproveitado o espaço situado entre a laje de cobertura e o telhado, para paiol de sobressalentes, caixa de distribuição de água e casa das máquinas dos elevadores.
Todas as lajes de cobertura estão isoladas contra o calor por es-pessa camada de cortiça.
O alojamento dos serventes está situado abaixo do primeiro pavi-mento, num local aproveitado do desnível do terreno, na porção norte da construção, e consta de um grande salão-dormitório, com escaninhos individuais para roupa, um serviço sanitário com 2 W.C., dois banheiros (chuveiros) e dois lavatórios. Todo o conjunto é muito bem iluminado e ventilado. Uma escadaria de mármore comunica o alojamento dos ser-ventes com os pavimentos superiores, permitindo que eles atendam aos chamados do serviço sem se exporem às intempéries.
A portaria está localizada junto ao portão de entrada do estabele-cimento, que dá acesso pela rua Maria Luzia. Consta de uma sala do porteiro, um dormitório e um serviço sanitário com chuveiro.
Todo piso do edifício é de cerâmica nacional, exceto o apartamento das irmãs de caridade e a sala de raios X, que são de taco, e os sa-guões, que são de mármore.
Todo o edifício foi pintado a óleo, em cor verde clara, para diminuir o excesso de luz existente e tornar ameno o ambiente à vista. As cozi-nhas foram pintadas de azul, a fim de afugentar as moscas.
Todas as paredes estão revestidas de azulêjo até 1,8m, exceto as paredes do saguão de entrada e da galeria transversal do pavimento térreo, que são revestidas de mármore.
Em cada galeria central há um relógio elétrico, pendente do teto, um quadro luminoso de sinalização, um telefone interno e um externo e um bebedouro higiênico, servido de água filtrada por uma instalação central. Para os serventes, no pavimento térreo, também foram coloca-dos dois bebedouros. Todos os bebedouros são de jato oblíquo e com os pontos de saída da água devidamente protegidos para não permitir o contacto com os lábios.
A sinalização luminosa e por meio de cigarras elétricas, surdas, é a mais perfeita possível, de modo a facilitar a assistência aos enfermos e permitir um controle completo dos serviços.
A rêde interna de telefone está ligada à rêde interna da parte baixa do Instituto Naval de Biologia.
Pela rua Maria Luiza penetra-se no terreno do pavilhão por uma avenida de concreto armado, tendo de um lado jardins e do outro arborização de arvores frutíferas. A avenida contorna um artístico
jardim que ocupa uma grande área na parte posterior do edifício, passa por um túnel de seis metros de largura (que é também a ga-rage do estabelecimento), ao lado da lavanderia, e permite o aces-so de automóveis ao páteo ajardinado da entrada principal.
Ao lado da portaria começa uma escadaria larga e bem lançada, que facilita o acesso dos pedestres ao páteo de entrada. Uma estra-da interna permite a livre comunicação com a parte baixa do I.N.B., facilitada por uma ponte de concreto armado construída sobre o Rio Cabuçú, que atravessa cascateando os terrenos do estabelecimento.
Um reservatório para 100.000 litros de água foi construído na parte baixa do I.N.B. D’aí a água é recalcada à caixa de distribuição, localizada acima da última laje do pavilhão, por meio de duas bom-bas propulsoras.
Interna e externamente o edifício é abundantemente iluminado. A instalação elétrica é feita em dois circuitos, de modo que permite, nas horas de silêncio da noite, uma iluminação de polícia, com lâmpadas fracas e de pequeno consumo.
Os laboratórios, o necrotério e a farmácia do Pavilhão Dr. Carlos Fre-derico são os já existentes no I.N.B., do qual ele é uma dependência.
Após a missa solene, celebrada em sua capela, no altar de Nossa Senhora da Glória, sua padroeira, a que assistiram o Sr. Presidente da República, Ministros de Estado, o Prefeito do Distrito Federal, outras altas autoridades civis e militares, oficiais do Instituto Naval de Biologia e Exmas Senhoras, o Pavilhão Dr. Carlos Frederico foi inaugurado pelo Sr. Presidente da República, que ali almoçou com os Srs. Ministros da Marinha, da Guerra, da Fazenda, da Viação, do Trabalho, da Educação, Chefe de Polícia, Chefe do Estado Maior da Armada, Diretor de Saú-de do Exército, Diretor Geral de Saúde Naval, Secretário de Saúde e Assistência do Distrito Federal, Reitor da Universidade do Brasil, En-genheiro Chefe da firma construtora do edifício e respectivas senhoras e, bem assim, o Diretor do Instituto Naval de Biologia, o Chefe do Ga-binete Militar e dois ajudantes de ordens do Presidente da República e dois oficiais do Estado Maior do Sr. Ministro da Marinha.
No dia 29 de Maio o Sr. Ministro da Marinha havia promovido, no Pavilhão Dr. Carlos Frederico, uma reunião de congraçamento e de ex-posição da nova realização da sua atividade na pasta que dirige, à qual compareceram oficiais da Marinha, acompanhados de suas famílias, médicos de destaque e convidados de projeção social.
O Pavilhão Dr. Carlos Frederico tem capacidade para 150 doentes e está convenientemente equipado para atendê-los com todos os re-cursos de que a moderna tisiologia se enriqueceu.
10 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 8-10

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 11-13 - 11
Over the past years, Navy authorities have been extremely concerned over the issue of the hospitalization of marines with tuberculosis. Patients had been initially and temporarily placed at the Nursing Auxiliary Ward in
Copacabana, but they remained there for many years due to lack of an appropriate place, despite the fact that everybody agreed that the situation could not be left to continue and that it required an urgent solution. The place was unsuitable and the wood barracks where patients were kept were not only inappropriate but were run down and nobody seemed to care to repair them because, in their opinion, patients should be placed at a different facility as soon as possible. But no initiative was taken to move ahead. During the administration of the Vice-Admiral Protogenes Guimarães, a pavilion building for tuberculosis patients who needed high altitude cold weather was built in the grounds of the Sanatório Naval de Friburgo.
But the Copacabana facilities were not closed down...Then the current Vice-Admiral Minister Aristides Guilhem made the
decisive move. He bought the land adjacent to the Instituto Naval de Biologia to build the
PAVILHÃO DR. CARLOS FREDERICO It is a reinforced concrete and masonry block, composed of five
floors, of which three are exclusively for the tuberculosis-infected patients; one is used for the ancillary services and the other holds the surgery center and the home of the charity sisters serving in the facility.
The entrance hall is on the ground (first) floor. Adjoining it to the left, are the room for the on-duty physician, connected to the dining room,
the bathroom and the dormitory of the physicians; to the right are the secretary’s office and the apartment of the senior nurse, consisting of sleeping quarters and toilet facilities (WC, lavatory and shower, with hot and cold water.).
On each side of the hall, there is a semicircular marble reception counter with internal cabinets, a nurse station for the files of the senior and day nurses, from whence they can communicate with the whole facility by means of light signals and the internal telephone system.
The entrance hall is connected to a wide corridor cutting the building transversally, crossing a longitudinal corridor, exactly at the center of the building. In the transversal corridor there are two elevators, as well as one marble staircase that lead to the upper floors.
In the west wing of the ground (first) floor, in a specially designated room, are the planigraphy, the X-ray and the physiotherapy equipment, as well as the clinic and the X-ray controlled pneumothorax room, the radiologist’s interpretation room, a waiting room and toilet facilities for the patients.
The radiology section consists of an examination room with two modern radiodiagnostic devices: for radiology, radiography and one for planigraphy. In addition to that, there is a dark chamber, a storage room and a file room. Walls encased in lead and covered with wood protect the entire set. The dark chamber has a signaling system, as well as two negatoscopes which help not only the radiologist but also the phthisiologist to define the diagnosis in the pneumothorax room.
In the east wing of the ground (first) floor are two kitchens (one for the garrison and another for patients), a dry goods storeroom, a
HOSPITALIZATION OF TUBERCULOSIS-INFECTED NAVY PERSONNEL
Pavilhão Dr. Carlos Frederico - 1940
Initially published in the Arq. Bras. Med. Naval. July 1940; 1 (3)
HISTORICAL ARTICLE

12 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 11-13
cold storage chamber, the laundry and the toilet facilities.The kitchen for the patients is adjoined to a wide pantry, which
is connected to a sterilization chamber for dishes that, through a descending (elevator-like) system, are brought down from the upper floors. In the clean part of the pantry, another elevator for transporting the thermal food cans to the pantries of the dining rooms.
The laundry consists of two sections: the dirty one, which includes the following: a clothes boiler, a spittoon sterilizer and the entrance of the heater, operated either by steam or by formalin, with further capacity to sterilize mattresses and beds. The clean section, where the clothes arrive through the heater after being sterilized, and where there is also a washing chamber, a squeezer for compressing clothes, a spin dryer, the clothes ironing apparatus and a boiler for heating the water distributed to the pantries, bathrooms and lavatories of the entire facility.
The dining room for the staff, another for the nurses and a dressing room for the subordinate personnel are located in the transversal corridor of the ground (first) floor.
The second floor consists of an entrance hall leading to the elevators and stairs, a dining room for 50 patients, adjoined to a pantry, in which are the elevators for sending food up and dishes to be served down, as well as a small stove used by the charity sisters for making light meals, an electrical refrigerator for storing milk and fruits for the daily diet, a cupboard covered with tiles, with marble shelves for storing food not requiring refrigeration, and shelves for dishes and small pans. There is also a kitchen sink cabinet for minor services and pantry cleaning.
On the second floor, there are also the following: a place for keeping both the patients’ clothes and bed linen; a medical office, where the pneumothoraxes shall be further performed; a bandage room and a small waste disposal room; a compartment for sterilizing bedpans; a dormitory for the nurse with toilet facilities and a private bathroom; an isolation area for severe patients; six wards which could accommodate 8 patients each ; a 2-m wide central corridor; a resting porch for the patients; toilet facilities and bathrooms for the patients; a barber’s; a dentist’s office; ophthalmology’s and otorhinolaryngology’s offices, as well as a sitting room for the patients.
On the third floor, in addition to the dining room and the pantry, there are the following: the place for keeping clothes, the medical office, the bandage room, the isolation room, the nurses’ room, the compartment for sterilizing bedpans, the wards, the toilet facilities and the bathrooms for patients, the central corridor and the resting porch – all of which similar to those of the second floor – there is a chapel entirely covered with marble, with beautiful stained glass windows, exclusively for the use of patients, having Our Lady of the Glory as patroness, with a sacristy room for the chaplain to keep his clergy vestments and for him to change his garments.
The fourth floor is totally identical to the third one, except for the chapel chorus for the charity sisters and the healthy people who would like to attend Masses at the local chapel, the height of which covers the third and fourth floors.
For every two wards, there is a toilet facility with two lavatories for morning ablutions. On one side, there are three compartments with three siphon jet type WCs and, on the other side, a bathroom with a bathtub for immersion and three showers with hot and cold water.
Being the building North-South oriented, it was possible to
dispose the resting porches towards the rising sun, as well as the wards, being the dining rooms, the pantries, the place to keep the clothes, the medical offices, the bandage rooms and the nurses’ rooms on the side of the setting sun.
The rainy winds – always blowing from the southwest – were considered when the facility was being built, so that they would never affect the resting porches.
All of the windows have sash frames, making it possible to have lower, medium or higher ventilation, according to the needs of the moment. Outside the glass frames, there are wooden blinds, which also allow for more or less indoor lighting, blocking the direct incidence of the Sun’s rays, when much intense, without completely darkening the compartments.
The surgery center and the apartment of the charity sisters are located on the fifth floor.
The surgery center comprises the following: a statistical control room; surgeons’ room with bathroom and toilet facilities; waste material room; circulation corridor; sterilization room with cabinet for keeping the surgical materials/instruments; anesthesia room; scrubbing room for the surgeons with three washbasins of their own activated by pedal. The large surgery room – finished with opaque blue tiles and ceramics – has built-in cabinets for storing surgical materials/instruments, three negatoscopes and a wide opening towards the south quarter, protected by an obscure glass, with a screen device for ventilation and an outdoor curtain for darkening the room when a surgery requires only artificial light.
The large window of the Operating Room (OR) faces a huge terrace. A grassy garden was created in the area of the terrace next to the operating room, so as to prevent the heat – as a result of the direct incidence of the Sun’s rays on the terrace – from affecting the temperature in the operating room.
The wall of the large operating room is turned to the East for directly receiving sunlight in the morning and to avoid the room to be heated, being a double section one, with a 20-cm ventilated space.
On the other side of the surgery center, which is separated from that of the religious women, there are the following: a parlor, the Mother Superior’s office, a dining room, a kitchen, a bathroom and toilet facilities, as well as a room for keeping personal effects and a dormitory room. There is a big terrace, which is used exclusively by the charity sisters as a recreation area, with a deep sink used for hand-washing clothes.
The surgery center and the apartment of the charity sisters are protected from the Sun’s rays by French roof tiles. A storehouse for spare parts, the water distribution box, as well as the elevator machine room are located in the space between the slab and the ceiling.
All of the covering slabs are insulated against heat by a thick cork layer.The quarters of the support service staff are located underground,
in an area used by taking advantage of the uneven terrain, at the North side of the facility, comprising a wide dormitory with individual compartments for clothes and a toilet facility with two WCs, two bathrooms (showers) and two lavatories. The whole area is very well illuminated and ventilated. A marble staircase connects these quarters to the upper floors, allowing them to attend to service calls without being exposed to bad weather
The janitor’s area is located next to the entrance gate, accessed via the Maria Luzia Street. Said area comprises a janitor’s office, a
12 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 11-13

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 11-13 - 13
dormitory and a toilet facility with a shower. The building’s flooring is finished with Brazilian made ceramic tiles,
except the floors of the apartment of the charity sisters and the X-ray room – made of wood – and those of the entrance halls – marble-made.
The entire building was oil painted in light green, so as to reduce excessive light and render the environment pleasant to the eyes. The kitchens were painted blue to drive the flies off.
All the walls are finished with tiles up to 1.8m, except for those of the entrance hall and the ones of the transversal corridor on the ground (first) floor, which are covered with marble.
On each central corridor, there is an electric clock, pending from the ceiling, a call signaling board, both internal and external telephone lines, as well as a drinking water fountain. Other two drinking fountains were placed on the ground (first) floor for the service support staff. All of the drinking fountains are of the oblique-jet type, with water outlet points duly protected, in order not to come into contact with people’s mouths.
The call signaling board – through muffled bells – is the most perfect one, facilitating the assistance of the patients and allowing the staff to have complete control of the services provided.
The internal telephone network is connected to the internal network of the lower part of the Instituto Naval de Biologia (I.N.B.).
Through the Maria Luiza Street, one gets into the land of the pavilion’s terrain via an avenue made of reinforced concrete. There are gardens on one side of it, and fruit trees planting on the other side. The avenue meanders through an artistic garden covering a large area in the rear part of the building, passing through a 6-m wide tunnel (that is also the facility’s garage), next to the laundry, giving vehicles access to the gardened yard of the main entrance.
Next to the janitor’s area begins a wide staircase, which facilitates the access of pedestrians into the entrance hall. An internal driveway allows for the free communication with the lower part of the I.N.B. A reinforced concrete bridge was built over the Cabuçú River, which runs across the lands of the facility.
A water reservoir with 10,000 liters of storage capacity was built in the lower part of the I.N.B. From there, the water is pumped to the distribution box, located above the last slab of the pavilion, through two pumps.
Both internally and externally, the building is abundantly illuminated. The electrical installation is a two-circuit one, so as to provide dimmer lighting, with energy-saving lamps in the late hours of the night.
The laboratories, morgue and pharmacy of the Pavilhão Dr. Carlos Frederico are those already existing in the I.N.B., of which this pavilion is an annex building.
A solemn Mass was celebrated before the inauguration of the Pavilhão Dr. Carlos Frederico, in its chapel at the altar of Our Lady of Glory, its patroness, to which attended the following authorities: Mr. President of the Republic of Brazil, the Ministers of State, the Mayor of the Federal District, as well as other civilian and military high authorities and officers of the Instituto Naval de Biologia and their spouses. Said Pavilion was inaugurated by Mr. President of the Republic of Brazil, who had lunch there with the Ministers of the Navy, War, Transports, Labor and Education, the Chief of Police, Chief of Staff of the Naval Forces, Health Officer of the Army, General Health Officer of the Navy, Health Secretary of the Federal District, Dean of the University of Brazil, Chief Engineer of the constructing firm of the building, accompanied by their respective spouses, in addition to the Director of the Instituto Naval de Biologia, the Chief of the Military Office and two assistants of the President of the Republic of Brazil, as well as two officers of the General Staff of Mr. Minister of the Navy.
On the 29th day of May, the Minister of the Navy held a celebration meeting, so as to show his recent accomplishments at his Ministry at the Pavilhão Dr. Carlos Frederico. Officers of the Navy accompanied by their families, renowned physicians and other renowned guests attended said meeting.
The Pavilhão Dr. Carlos Frederico was built to hold 150 beds and is conveniently equipped to assist and treat patients with all of the modern phthisiology resources available.

14 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 14-18
MEDICINA OPERATIVA: UMA ESPECIALIDADE?
AUTORES: CT (Md) HEMERSON DOS SANTOS LUZ Graduação em Medicina pela UFF.Especialização em Doenças Infecto-Contagiosas pela PUC-RJ.Especialização em Medicina Interna pela UFRJ.Aperfeiçoamento em Doenças Infecto-Contagiosas pelo HNMD.Estágio em Operações Ribeirinhas no Batalhão de Operações Ribeirinhas da Marinha do Brasil - Manaus.Estágio Básico de Combatente de Montanha no 11º BIMth - São João Del Rey.Surface Warfare Medical Department Officer (SWMDO) - a bordo do USNS Comfort.
CA (Md) SÉRGIO PEREIRA Graduação em Medicina pela Faculdade de Medicina de Itajubá.Residência em Medicina Interna (Título de Especialista em Clínica Médica) pelo Hospital Israel Pinheiro do IPSEMG.Especialização em Cardiologia pela Sociedade Brasileira de Cardiologia e pela Associação Médica Brasileira.Especialização em Terapia Intensiva pela Associação Brasileira de Terapia Intensiva e Associação Médica Brasileira.Master of Business Administration Executivo em Saúde pela COPPEAD - UFRJ.Curso de Política e Estratégia Marítimas - EGN (C-PEM).
RESUMOO presente estudo faz um resumo histórico da medicina de guerra e, paralelamente, ressalta as principais características desejáveis ao mé-
dico operativo, destacando, também, as qualidades inerentes aos militares que atuam em Medicina Operativa (MedOp).
Palavras-chave: medicina operativa; medicina militar.
INTRODUÇÃOA medicina de guerra evoluiu muito ao longo dos séculos, acompa-
nhando o desenvolvimento de novas técnicas e doutrinas empregadas em combate. A MedOp acompanha o desenvolvimento tecnológico e doutrinário inerente ao conhecimento militar.
Apesar das inovações e conquistas da ciência, algumas caracte-rísticas continuam a pontuar o perfil dos profissionais de saúde que atuam em MedOp, como, por exemplo, a capacidade de atuação em ambiente hostil e com limitação de recursos. O oficial médico ao in-gressar no Corpo de Saúde da Marinha não tem conhecimento de que, não raras vezes, deverá atuar em circunstâncias não habituais às de um hospital que disponha de recursos de alta complexidade. A vida do médico a bordo de um navio ou servindo em uma unidade de fuzilei-ros navais costuma ser muito diferente daquela que se vivencia em um hospital. Assim, seria importante a realização de uma formação orien-tada com foco nas atividades operativas da MB, para que não venha a
Figura 2: Réplica de
ambulância idealizada
por Dominique-
Jean Larrey, flying
ambulance.
ser desmotivador o fato de servir algum tempo embarcado ou em tropa. Diante da percepção do crescimento e da complexidade das ativi-
dades operativas perante múltiplas situações que envolvem o emprego de militares do Corpo de Saúde da Marinha (CSM) em ações a bor-do dos navios, unidades de fuzileiros navais e unidades aeronavais, a Alta Administração Naval decidiu pela criação do Centro de Medicina Operativa da Marinha (CMOpM), cuja ativação ocorreu em 15 de abril de 2009, marcando uma nova fase na história da medicina de guerra.
SÍNTESE HISTÓRICAO imperador romano Augustus, ao reorganizar as legiões romanas,
criou o primeiro corpo de saúde militar de que se tem conhecimento, com um médico para cada mil soldados. Esse corpo médico era alta-
Figura 1: Escultura da época da antiga Roma, com representação de legionários do corpo de saúde socorrendo seus camaradas feridos em batalha.
mente motivado e dispunha de uma tecnologia ímpar para a época co-mo instrumentais cirúrgicos específicos, fervidos antes de cada uso e o conhecimento de ervas com capacidades analgésicas.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 14-18 - 15
Na I Guerra Mundial, consolidou-se um ato médico que, até hoje, permanece em uso: a triagem, que, surgiu da preocupação com a me-lhor conservação dos efetivos, das dificuldades de apoio logístico e da inquietação humanitária dos médicos que atuavam no conflito.
Na II Guerra Mundial houve uma melhor coordenação do apoio das atividades médicas, existindo uma combinação de triagem no teatro de operações com uma cadeia de evacuação definida. No dia D, por exemplo, houve a presença de médicos nas vagas de desembarque anfíbio e nas tropas de paraquedistas, sendo que os mesmos organi-zavam os postos avançados de triagem e a evacuação dos feridos para os navios-hospital. Neste conflito iniciaram-se as primeiras atividades de coordenação e controle em atividades de saúde.
No conflito do Vietnã, com o advento das operações aerotranspor-tadas pelas forças norte-americanas, houve certa inércia do sistema de triagem ocasionado pelo amplo uso da evacuação aeromédica (EVAM); na verdade, era utilizado o sistema “pegar e correr” pelo exército ameri-
Na Idade Média, não houve desenvolvimento das ciências em ge-ral, ocorrendo o mesmo com a medicina de guerra.
Entretanto, nas campanhas napoleônicas, o barão Dominique-Je-an Larrey, respeitável cirurgião de Bonaparte, criou e coordenou o pri-meiro serviço de ambulâncias militares de que se tem conhecimento, com carroças preparadas para resgatar os soldados feridos em com-
bate. Além de salvarem incontáveis vidas, elas tornaram-se parte de um sistema bem organizado de evacuação de feridos e serviram de modelo para muitos outros exércitos.
Também nas guerras napoleônicas, os vasos de guerra ingleses, sob o comando do lendário almirante Nelson, já contavam com oficiais médicos em suas tripulações e os mesmos dispunham de canastras médicas para o seu trabalho.
A Guerra Civil americana acelerou o desenvolvimento da medici-na de guerra, seja pelos seus hospitais de campanha, com a presença marcante das enfermeiras no conflito, bem como pelas técnicas cirúrgi-cas de amputação amplamente utilizadas. Os cuidados médicos eram estendidos a todos os soldados que os necessitassem, independente-mente de qual lado pertencessem, prevalecendo assim a ética médica.
No Brasil destaca-se na história da medicina de guerra a obra do doutor Carlos Frederico dos Santos Xavier Azevedo intitulada História médico-cirúrgica da esquadra brasileira nas campanhas do Uruguay e Paraguay de 1864 a 1869, publicada em 1870. O autor foi promovido a Chefe da Saúde da Estação Naval do Rio do Prata em 1864, acompa-nhou muitos embates armados e administrou o Hospital de Marinha no Uruguai e, também, na Argentina. Desta maneira, suas experiências em guerra, tornam esta obra um relato muito valioso.
Figura 3: Hospital de campanha da Guerra Civil americana, preparativos para uma amputação de membro inferior.
Figura 4: Passagem de ferido entre navios durante a II Guerra Mundial.
Figura 5: Hospital de campanha vietnamita camuflado
com velame de paraquedas na
Guerra do Vietnã.
cano, com muito mais meios aéreos disponíveis para a evacuação dos feridos, enquanto os fuzileiros, com menos aeronaves, desenvolveram mais a triagem e a padronização das condutas de atendimento.
Figura 6: Oficial médico americano presta socorro a uma criança no Iraque.
Em certas regiões, os americanos detinham o controle total do es-paço aéreo e cada aeronave de asa rotativa de resgate, fazia em média quatro missões por dia, sendo, contudo, atingidas pelo fogo inimigo até três vezes mais do que os helicópteros de combate ou transporte que

16 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 14-18
não detinham a cruz vermelha na estrutura. Naquele conflito, tornaram-se claras as diferenças no atendimento
aos feridos, de acordo com o lado a que pertenciam. Por sua vez, a guerra de resistência começava a ser consolidada pelos vietnamitas.
Nas guerras do Golfo e do Iraque, o poderio econômico e mili-tar dos Estados Unidos determinou um novo conceito de medicina de guerra, com hospitais de campanha equipados com centro cirúrgico e CTI, muito mais próximos ao teatro de operações. Surgem as primei-ras Unidades Avançadas de Trauma. Inicia-se, também, a utilização de hospitais em países aliados, literalmente modernizados, com equipa-mentos de alta tecnologia. A medicina preventiva e a vigilância sanitá-ria ativa também passam a ser mais valorizadas.
No conflito do Iraque e Afeganistão surgem os conceitos de com-bat support hospital (CSH), aposentando-se o termo MASH (mobile army support hospital), utilizado desde o Vietnã e imortalizado em uma série de televisão norte-americana e o foward surgical team (FST), que se consolida como o padrão das unidades avançadas de trauma em uso. O sistema de evacuação aeromédica (EVAM) al-cança elevados índices de eficácia, fazendo com que um ferido em combate como em Fallujah – Iraque, por exemplo, consiga chegar na Alemanha em menos de 48 horas desde os primeiros socorros. Os protocolos de atendimentos de feridos em combate são amplamente utilizados pelos enfermeiros de combate.
CARACTERÍSTICAS DO MÉDICO OPERATIVOAlém do conhecimento científico inerente a todo médico, o mi-
litar deverá também estar apto a atuar e sobreviver em ambientes hostis. A selva, a montanha, a caatinga e o ambiente submerso são exemplos; nestes locais, os homens envolvidos no combate estão em luta contra um segundo inimigo, o próprio local da ope-ração. Aliás, historicamente foi o principal responsável pelas mor-tes ocorridas na Guerra da Tríplice Aliança. Quando embarcados em algum meio operativo de superfície, os oficiais médicos devem ter em mente que face à natureza do trabalho desenvolvido nos navios onde a tripulação executa rotineiramente atividades de tiro real, operação com aeronaves, controle de avarias e fainas mari-nheiras diversas caracterizadas por alto risco de acidentes pesso-ais, a insalubridade é fruto do cenário em que o navio opera e das condições de habitabilidade associadas às tensões, principalmente quando na iminência do combate.
O profissional de saúde deve estar preparado para atuar em situa-ções extremas, como o choque com novos ruídos, odores, cores, com a própria insegurança e, muitas vezes, com a hostilidade. Quando em-barcado em meios operativos de superfície deverá conhecer as limita-ções técnicas e logísticas envolvidas no apoio de saúde.
Em síntese, o médico operativo, além de tratar dos doentes e feri-dos, deve saber: • Sobreviver–estarvivoparaproversaúde• Orientar-se–usarcartasnáuticas,mapastopográficos,bússolase
instrumentos de posicionamento tais como o Global Position System (GPS)
• Ensinar–paraadestrarguarniçõesetripulaçõesemterraeabordo• Prevenir–atuardemodopreventivoemepidemiasesurtos• Reagir–reaçãorápidacontraataquescomusodearmamentosdi-
versos, em caso de ataque inimigo ou emboscadas
• Interagir–estarintegradoàtripulaçãodaorganizaçãomilitar(OM)em que serve, conhecendo bem o perfil físico e psicológico dos mili-tares e as características (recursos e limitações) do navio
• Liderar – equipes de saúde e, até mesmo, equipes em combatequando em situações de hostilidade.
Devido à crescente complexidade da atuação dos serviços de saúde em conflitos, todos os médicos, dentistas, farmacêuticos e en-fermeiros devem ter uma formação militar operativa genérica, mesmo que passem a atuar, grande parte de suas carreiras, em medicina as-sistencial. Por outro lado, aqueles que tiverem pendor ou uma maior vocação pela área operativa poderiam especializar-se com cursos específicos voltados à MedOp.
Há, no Exército Brasileiro, médicos, dentistas e farmacêuticos com curso de paraquedismo militar ou operações na selva que tra-balham, normalmente, em suas clínicas e serviços nos diversos hos-pitais militares. Na Força Aérea Brasileira, existem oficiais médicos com curso de PARA-SAR (especialização em paraquedismo e salva-mento), em bases aéreas ou hospitais. As tropas especializadas que operam em diferentes ambientes também lotam oficiais médicos em suas fileiras, como por exemplo, o 11º Batalhão de Infantaria de Mon-tanha do Exército Brasileiro ou o Batalhão de Operações Ribeirinhas dos fuzileiros navais. Habilitar militares para operar em atividades especiais e ambientes específicos não é tarefa fácil, entretanto, pas-sível de execução tendo em vista a existência de vários centros de formação nas Forças Armadas.
Quadro 1: Cursos operativos acessíveis a oficiais de saúde.
• Paraquedismomilitar
• Montanhismomilitar
• Operaçõesnaselva
• Comandosanfíbios
• Defesaquímicabiológicaenuclear(DQBN)
Quadro 2: Subsistemas de saúde da Marinha.
• Subsistemaassistencial
• Subsistemapericial
• Subsistemaoperativo
Não obstante, em tempos de paz, os militares do serviço de saúde com alguma formação específica operativa, entre as discri-minadas a seguir, poderão servir em qualquer organização mili-tar (OM), operativa ou hospitalar, permanecendo preparados para qualquer eventualidade.
Nesse contexto seria importante se os oficiais médicos ti-vessem uma formação específica em MedOp, com instruções abrangendo desde acidentes de múltiplas vítimas, ações de su-perfície, operações anfíbias, doenças tropicais, suporte avançado de vida, até apoio de saúde em ambientes especiais (montanha,
Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 14-18 - 17
selva, caatinga etc), num paralelo com os já estabelecidos cursos de medicina de submarino e escafandria e medicina de aviação, cujos médicos mantêm suas especialidades médicas de origem, podendo ser empregados em todos os subsistemas de medicina da MB. Recentemente um oficial médico da MB foi o primeiro es-trangeiro a completar o adestramento chamado Surface Warfa-re Medical Departament Officer (SWMDO), considerado uma es-pecialidade na Marinha americana valorizando as atividades de saúde nos meios de superfície. Ressalta-se também a presença atual de uma oficial do quadro de apoio à saúde realizando um curso de defesa química, biológica e nuclear, no Exército brasi-leiro, marcando a presença da primeira oficial do sexo feminino a realizar o referido curso.
A MEDICINA DE GUERRA NA MARINHA DO BRASIL (MEDICINA OPERATIVA)
A MB sempre se mostrou muito avançada em relação à medicina de guerra, seja pela experiência decorrente dos hospitais de campa-nha e navios-hospital desde a Guerra do Paraguai, passando pelas ex-periências no exterior em missões de paz, pela presença do médico no
Figura 7: Atendimento de urgência a civil ferida no Haiti.
continente antártico e pelas ações de atendimento ribeirinho na região amazônica (ASSHOP), além das atuações do hospital de campanha em missões de apoio humanitário ou em calamidades públicas.
Por sua vez, o apoio às operações aeronavais, de mergulho e submarino está fortemente alicerçado na MB, tratando-se de espe-cialidades médicas tradicionais, constantemente atualizadas e man-tidas no estado da arte.
Desde o ano 2000, os oficiais médicos do Corpo de Saúde da Mari-nha já podem ser voluntários para o curso de comandos anfíbios, porém permanece a saúde, nas áreas de ações de superfície e operações anfí-bias, no nosso entendimento, com necessidade de evoluir.
A presença de praças enfermeiros com inúmeros cursos operati-vos é marcante nas diferentes OM da MB.
Por fim, a criação de uma OM totalmente voltada para as ativida-des de MedOp, que disponha de uma tripulação de saúde marca-damente especializada em resposta médica militar em situações de desastres, em planejamento e controle das atividades de saúde opera-tiva e missões humanitárias, permitirá o melhor gerenciamento deste segmento do Sistema de Saúde da Marinha, além de contribuir com os meios operativos, no desenvolvimento e no contínuo aperfeiçoamento do apoio de saúde às operações navais.
PERSPECTIVAS PARA O FUTUROConsiderando especificamente a formação do médico operativo
na MB, já foi realizada a proposta de Diretoria da Saúde da Marinha (DSM) para a alta administração naval de um curso específico para essa formação, a ser realizado, inicialmente, nos Estados Unidos da América (EUA), provavelmente, no Army Medical Department Center (AMEDD) em San Antonio (Texas).
A criação de um curso especial de medicina operativa talvez se configure como um dos próximos passos na evolução da medicina de guerra na MB, a partir da formação inicial dos médicos no exterior.
Figura 8: NAe São Paulo – maior estrutura de saúde na esquadra.
• Açõesdesuperfície
• Açõesdemergulhoesubmarinos
• Aviaçãonaval
• Açõesemregiõesglaciais
• Operaçõesnaselva
• Operaçõesribeirinhas
• Operaçõesanfíbias
• Operaçõesespeciais
• Farmáciaoperativa
• Odontologiaoperativa
• Operaçõesdepaz
• DefesaQBN
• Salvamentoeresgate
Quadro 3: Segmentos da medicina operativa.

18 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 14-18
É possível ainda que, num futuro próximo, a MB tenha em seus quadros oficiais médicos, dentistas, enfermeiros e farmacêuticos com cursos de operações especiais, paraquedismo, operações na selva, montanha e DQBN embarcados em diversas OM de saúde, prontos para qualquer eventualidade.
CONSIDERAÇÕES FINAISA medicina sempre evoluiu em tempos de conflito, contudo, a
análise dessas descobertas não faz parte do escopo deste traba-lho. Trata-se sim, de um pequeno levantamento dos aspectos de um profissional de saúde que com dedicação e, muitas vezes, com sacrifício pessoal, busca a melhor capacidade de adaptação a si-tuações de conflito e, com isso, pretende contribuir para manter o potencial combativo dos militares componentes de uma força. Es-sa característica pouco mudou na história da humanidade pois es-ses profissionais continuam sempre empenhados em desempenhar uma medicina do melhor padrão desejável em situações não con-vencionais e, naturalmente, sem desconhecer as causas humanitá-rias e a ética profissional.
BIBLIOGRAFIA1. Ortiz JM. The revolutionary flying ambulance of Napoleon´s surge-
ons. [Acesso em: 27 jul. 2009]. Disponível em:http://napoleonicliterature.com/Flying_Ambulance.htm
2. Caring for the men: the history of Civil War Medicine. [Acesso em:
25 jul. 2009]. Disponível em:http://www.civilwarhome.com/civilwarmedi-cineintro.htm
3. Welsh WE. Napoleonic wars: battle of Trafalar: Vive-Admiral Hora-tio Nelson did his duty. [Acesso em: 27 jul. 2009]. Disponivel em: http://www.historynet.com/napoleonic-wars-battle-of-trafalgar-vice-admiral-horatio-nelson-did-his-duty.htm/3
4. Medical history: history of naval medicine- the development of pre-ventive medicine in the Royal Navy. [Acesso em: 25 jul. 2009]. Disponí-vel em: http://www.royalnavy.mod.uk/training-and-people/rn-life/medical-branch/medical-history/
5. Helicopter evacuation: Vietnam. [Acesso em: 19 jul. 2009]. Dispo-nível em: http://www.oliv drab.com/od_medical_evac_helio_vietnam.php
6. Definition of triage. [Acesso em: 25 jul.2009]. Disponível em: http://www.medterms.com/script/main/art.asp?articlekey=16736
7. World War II medical treatment. [Acesso em: 19 jul. 2009]. Dispo-nível em: http://www.olive-drab.com/od_history.php3
8. Smith AM: Bohman HR - Medical command and control in sea-based operations. Naval War Coll Rev. 2006; 59( 3).
9. Gawande A. Casualties of war-military care for the wounded from Iraq and Afghanistan. N Engl J Med. 2004; 351(24):2471-5. Available at: www.nejm.org
10. Sperandio GF; Neto JMA. A Marinha de Guerra do Brasil e sua atuação no conflito da tríplice aliança: condições sanitárias e cuidados médicos. Londrina: UEL-Universidade Estadual. Trabalho de Conclusão de Curso.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 19-23 - 19
OPERATIONAL MEDICINE: A SPECIALTY?
AUTHORS:CT (Md) HEMERSON DOS SANTOS LUZ Bachelor’s Degree in Medicine from UFF.Specialization in Infectious and Communicable Diseases from PUC-RJ.Specialization in Internal Medicine from UFRJ.Extended Training in Infectious and Communicable Diseases at HNMD. Internship in Riparian Operations at the Riparian Operations Battalion of the Brazilian Navy – Manaus.Basic Internship in Mountain Combat at the 11st BIMth - São João Del Rey.Surface Warfare Medical Department Officer (SWMDO) – on board the USNS Comfort.
CA (Md) SÉRGIO PEREIRA Bachelor’s Degree in Medicine from the Faculdade de Medicina de Itajubá.Medical Residency Training in Internal Medicine (Specialist in General Practice) at the Hospital Israel Pinheiro of IPSEMG.Specialization in Cardiology from the Brazilian Society of Cardiology and the Brazilian Medical Association.Specialization in Intensive Care from the Brazilian Intensive Care Association and the Brazilian Medical Association.Executive MBA in Health at COPPEAD - UFRJ.Course on Maritime Policy and Strategy - EGN (C-PEM).
ABSTRACTThe present study summarizes the historical background of war medicine and then discusses the major required features of a surgical
physician, highlighting the required features of militaries that operate in operational medicine.
Keywords: military medicine; war surgery.
INTRODUCTIONWar Medicine has greatly evolved along the centuries to
keep up with new combat developments and doctrines. Surgery has, likewise, evolved alongside technological and doctrinal developments that underlie military knowledge.
Despite scientific innovations and achievements, specific features are still required of medical staff with Surgery, like, for instance, the necessary skills to operate in hostile environments with limited resources. Medical officers that join the Brazilian Navy Medical Corps are not usually aware that often times they will have to operate in situations that are very diverse from the state-of-the-art resources available to a regular hospital. The daily life of on-board or marine-unit physicians is very unlike that of a hospital physician.
The former, therefore, poses the utmost need of surgical activity-focused training and qualification to prevent the demotivating feeling experienced by physicians who work on board or with troops.
Being aware of the expansion and increasing complexity of surgical activities in various situations that call for the employment of officers with the Brazilian Navy Medical Corps (BNMC) on board, with troops and with joint Air-Navy units, the High Navy Command decided to establish the Brazilian Navy Operational Medicine Center, whose operations started on April 15, 2009 and set forth a new phase in the history of Brazilian War Medicine.
BRIEF HISTORICAL BACKGROUNDWhen the Roman emperor Augustus decided to restructure the
Roman legions he created the first military medical corps known to man, Figure 1: Sculpture that dates back to Roman times, depicting the medical corps legion rescuing their battle-wounded comrade soldiers.
Figure 2: A replica
of the ambulance
designed by Dominique-
Jean Larrey, flying
ambulance.

20 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 19-23
with one physician for every one thousand soldiers. That highly motivated medical corps was provided with unmatched technology at the time and specific surgical devices that were boiled before each time they were used. They also had a body of knowledge about analgesic power herbs.
The Middle Ages did not promote any development of sciences in general, and war science was then no exception.
Figura 3: An American Civil War Camp Hospital – preparation for a lower limb amputation.
However, during Napoleon’s campaigns, the earl Dominique-Jean Larrey, one of Bonaparte’s renowned surgeons, established and coordinated the first military ambulance service heard about, with carts to rescue battle-wounded soldiers. Besides saving countless lives, these carts became a powerful component of a well-organized evacuation system that was referred to as a model for many other armies.
Still during Napoleon’s wars, the English war ships commanded by the legendary Admiral Nelson had medical officers in their crew as well as medical hampers to aid their work.
The American Civil War expedited the development of war medicine by setting up camp hospitals, employing a substantial number of female nurses, and widely using amputation surgical techniques. Medical care was made available to all soldiers, irrespective of what side of the war they were fighting with, and the medical ethics prevailed.
In the Brazilian history of war medicine it is worth mentioning Dr. Carlos Frederico dos Santos Xavier Azevedo’s book entitled História médico-cirúrgica da esquadra brasileira nas campanhas do Uruguay e Paraguay de 1864 a 1869 (‘The medical-surgical history of the Brazilian fleet in the Uruguay and Paraguay wars, from 1864 to 1869’), published in 1870. The author was promoted to Chief Medical Officer of the Prata River Medical Station in 1864, attended many armed combats and managed the Navy Hospital in Uruguay and in Argentina.
His war experiences make his book an invaluable historical account.World War I introduced a medical practice that has been used up
to now - screening, which resulted from the concern with the well-being of the war strength, the difficulties faced by logistics support and humanitarian views of the physicians that attended wounded soldiers.
During World War II, support to medical activities was better coordinated and there was a combined procedure of screening for operations with a well-designed evacuation chain. On D Day, for instance, there were physicians at the amphibious dock ships and with the parachute troops who organized the forward screening posts and the evacuation of the wounded to hospital ships. It was during this conflict that the first medical support coordination activities were implemented.
Figure 4: Moving a wounded soldier from one ship to another during World War II.
Figure 5: Vietnamese
Camp Hospital camouflaged
with parachute canvas during the
Vietnam War.
During the Vietnam War, with the advent of American airborne transportation systems, some inertia settled in the screening system due to the ample use of aeromedical evacuation. The American Army
actually used the “scoop-and-run” system which provided many more airborne means to evacuate wounded soldiers, while the marines, with fewer aircrafts, implemented more screening and medical care conduct standardization.
In certain regions, the Americans held total control of the air space and each rescue win rotation aircraft would perform an average of four missions per day; nevertheless, they were three times as much hit by
Figura 6: An American medical officer attending to a wounded child in Iraq.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 19-23 - 21
enemy artillery than combat helicopters or other transportation that did not bear the Red Cross in their fuselage.
This conflict evidenced the contrasting medical care provided to the wounded by either party. On the other hand, the Vietnamese started the consolidation of their resistance war.
During the Gulf and Iraq wars, the US economic and military power introduced a new concept of war medicine – their Camp Hospitals were equipped with a surgery unit and an ICU and were closer to the areas of operation. The first Forward Surgical Teams (FST) were implemented and allied countries offered their high-technology hospitals. Preventive medicine and sanitary surveillance were increasingly valued.
It was during the Iraq and Afghanistan conflicts that two concepts emerged: (1) combat support hospital (CSH), to replace the formerly used MASH (mobile army support hospital), which had emerged during the Vietnam war and was immortalized by the American TV series; and (2) forward surgical team (FST), which became the standard for forward trauma teams in force. The Aeromedical Evacuation System (AES) reached high effectiveness standards, allowing, for instance, a soldier that was wounded in combat in Fallujah, Iraq, to reach a German hospital in less than 48 hours after receiving first aid. Serious Injury Protocols (SIP) were widely used by combat nurses.
SPECIFIC FEATURES OF SURGICAL PHYSICIANSBesides the scientific knowledge that every physician must own,
medical officers must also be able to operate and survive hostile environments, like the jungle, the mountain, the caatinga (typical vegetation of stunted trees and spiky scrub in regions of small rainfall in Northeastern Brazil) and the underwater world. In such environments, combat men fight yet another enemy: the environment itself. It is worth noting that historically, the environment was accountable for most deaths during the Triple Alliance War. When on board a floating means of transportation, medical officers must bear in mind that given the nature of the routine work of the crew, life-fire exercises, damage control and several other sailing operations, there is always high risk of personal accidents, and that insalubrity results from the very environment where ships operate as well as from shipboard habitability associated to tension, especially when combat is imminent.
Medical professionals must be prepared to act in extreme situations and to overcome the shock caused by the inherent sense of insecurity, alien smells, colors, sounds, and last but not least, hostility. When on board a floating means of transportation, medical officers must be fully aware of the limited technical and logistics support to medical activities.
In a nutshell, surgical physicians, besides attending the sick and the wounded, must know how to:
• Survive–keepthemselvesalivetosupplymedicalservices
• Guide themselves – use nautical charts, topographic maps, acompass and location devices such as Global Position System (GPS)
• Teach–totrainthegarrisonsandcrewsbothonboardandinland
• Preventsituations–implementpreventiveactionsinthecaseofanepidemic or an outbreak
• React–quicklyrespondtoenemyorambushattackwithvariousweapons
• Interact– integratewith themilitarycrewtheyareservingwith,bybeing very familiar with the physical and psychological profile of militaries and with the ship features (resources and limitations)
• Lead – coordinate health teams, and even combat teams underhostile situations.
On account of the increasing complexity and scope of medical services in conflict situations, all military doctors, dentists, chemists and nurses must have undergone a general military operations training, even if they are supposed to work most of their lives in assistance medicine. Nevertheless, those that are willing to or have a vocation to work on board can specialize and take specific qualification and training in surgical medicine.
The Brazilian Army has a number of medical officers, dentists, and chemists who have undergone training in military parachuting or jungle operations who, nonetheless, work in various types of military clinics and hospitals. And the Brazilian Air Force counts several medical officers who have taken the PARA-SAR specialized training program (parachuting and life-saving and rescue) who work in air bases or hospitals. Special Forces Units have medical officers in their ranks, like for instance, the 11th Mountain Infantry Battalion of the Brazilian Army or still the River Operations Battalion of the Brazilian Marines. Although it is no easy task to qualify militaries in Special Forces activities and environments, this can be done in the various Armed Forces qualification and training centers.
Nevertheless, in times of peace, military medical professionals with surgical medicine qualification – amongst the scope describes below – can serve any military organization, be it on board or in hospitals, while on stand-by for any contingency operation.
Face to the above described context, it follows that medical officers should ideally be qualified in surgical medicine and trained in multiple-victim accidents, surface actions, amphibious operations, tropical diseases, forward life support, and even medical support in special environments (mountain, jungle, caatinga, etc), as parallel qualification
• Militaryparachuting
• Militarymountainclimbingandtraining
• Jungleoperations
• Amphibiouscommands
• NuclearBiologicalChemical(NBC)Defense
Chart 1: Surgical medicine qualification available to medical officers.
Chart 2: The Brazilian Navy Medical Support Subsystems.
• Medicalassistancesubsystem
• Forensicssubsystem
• Surgicalsubsystem

22 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 19-23
to the already established courses – submarine medicine, diving and undersea medicine, and aviation medicine, whose physicians have kept their original medical specialty, thus allowing for their employability in all the Brazilian Navy medicine subsystems. A recent example is a Brazilian Navy medical officer who became the first foreigner to complete the Surface Warfare Medical Department Officer (SWMDO) Program, which is considered a specialty by the American Navy and lends value to medical activities on floating means of transportation. It should also be noted that a female medical support officer is currently taking an NBC Defense course at the Brazilian Army – the first female officer ever to take the referred course.
Figure 7: Emergency assistance to a civilian wounded in Haiti.
Figure 8: NAe São Paulo – largest medical support sea craft in the Brazilian fleet.
• Surfaceactions
• Divingandsubmarineactions
• Navalaviation
• Actionsinglacialregions
• Jungleoperations
• Riveroperations
• Amphibiousoperations
• Specialoperations
• Surgicalpharmacy
• Surgicaldentistry
• Peaceoperations
• NBCdefense
• Life-savingandrescue
Chart 3: Operational medicine segments.
WAR MEDICINE (OPERATIONAL MEDICINE) IN THE BRAZILIAN NAVY
The Brazilian Navy has always had a forward stance towards war medicine, not only because of the accumulated experience
with camp hospitals and ship hospitals since the Paraguay War plus the overseas experience in peace missions, but also because of the experience in the Antarctic, in river medical assistance in the Amazon region, in the camp hospitals that joined humanitarian relief missions, and the support to disaster relief contingencies.
On the other hand, the support to joint Air-Navy operations, as well as to diving and submarine operations, is a bedrock in the Brazilian Navy, once they are traditional medical specialties that undergo constant updating to be kept in state-of-the-art standards.
Since 2000, the medical officers with the Navy Medical Corps have been allowed to apply as volunteers to the amphibious command course, although we understand it is the medical support system for surface and amphibious operations the area that needs further development.
Nurse officers qualified in a number of surgical medicine courses have a marking presence in the various types of military operations of the Brazilian Navy.
Finally, the establishment of military operations solely oriented towards medical surgery, composed of a medical crew notably specialized in military medical response to disasters, in the planning and control of operational medicine activities and in humanitarian missions, will foster more effective management of this Navy medical system segment, as well as contribute to the development and continuous improvement of medical support to naval operations.
FUTURE PERSPECTIVESWith specific regard to the qualification of the surgical physicians
at the Brazilian Navy, a request has already been submitted to the Higher Board of the Medical Division of the Brazilian Navy for a specific program for such qualification, to be initially conducted in the United States of America, most probably at the Army Medical

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 19-23 - 23
Department Center (AMEDD) in San Antonio (Texas).The development of a special surgical medicine course can
perhaps become one of the following steps in the evolution path of war medicine at the Brazilian Navy, following the initial qualification of surgical physicians overseas.
It is also possible that in the near future, the Brazilian Navy will have medical officers, dentists, nurses and chemists with special qualifications – parachuting, jungle and mountain operations, NBC defense - in several military medical operations, ready to operate in any contingency.
FINAL CONSIDERATIONSMedicine has always evolved in times of conflict. However, a
detailed analysis of such discoveries is beyond the scope of this work, which has aimed to present an overview of the required features of a medical professional who, upon personal sacrifice, seeks the best qualification to adapt to conflict situations in order to help the combat potential of the military corps. Such features have little changed throughout mankind history, since these professionals remain committed to practicing the highest standards of medicine in unconventional situations while keeping full consciousness of humanitarian causes and professional ethics.
BIBLIOGRAPHY1. Ortiz JM. The revolutionary flying ambulance of Napoleon´s
surgeons. [Accessed on: 27 jul. 2009]. Available at: http://napoleo ni-cliterature.com/Flying_Ambulance.htm
2. Caring for the men: the history of Civil War Medicine. [Accessed on: 25jul. 2009]. Available at: http://www.civilwarhome.com/civil warme-dicineintro.htm
3. Welsh WE. Napoleonic wars: battle of Trafalar: Vive-Admiral Horatio Nelson did his duty. [Accessed on: 27 jul. 2009]. Available at: http://www.historynet.com/napoleonic-wars-battle-of-trafalgar-vice-admiral-horatio-nelson-did-his-duty.htm/3
4. Medical history: history of naval medicine- the development of preventive medicine in the Royal Navy. [Accessed on: 25 jul. 2009]. Available at: http://www.royalnavy.mod.uk/training-and-people/rn-life/medical-branch/medical-history/
5. Helicopter evacuation: Vietnam. [Accessed on: 19 jul. 2009]. Available at: http://www.oliv drab.com/od_medical_evac_helio_vietnam.php
6. Definition of triage. [Accessed: 25 jul. 2009]. Available at: http://www.medterms.com/script/main/art.asp?articlekey=16736
7. World War II medical treatment. [Accessed on: 19 jul. 2009]. Available at: http://www.olive-drab.com/od_history.php3
8. Smith AM: Bohman HR - Medical command and control in sea-based operations. Naval War Coll Rev. 2006; 59( 3).
9. Gawande A. Casualties of war - military care for the wounded from Iraq and Afghanistan. N Engl J Med. 2004; 351(24):2471-5. Available at: www.nejm.org
10. Sperandio GF; Neto JMA. A Marinha de Guerra do Brasil e sua atuação no conflito da tríplice aliança: condições sanitárias e cuidados médicos. Londrina: UEL-Universidade Estadual. Trabalho de Conclusão de Curso .

24 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 24-27
INTRODUÇÃOPara que o emprego de uma força naval se realize com a eficácia dese-
jável, é fundamental que o seu apoio seja eficiente e compatível com a natu-reza, vulto, duração e espaço em que as operações se desenvolverão. Esse apoio é realizado pela logística, à qual cabe prover os recursos necessários para manter, e mesmo ampliar, a capacidade operativa das forças navais.
A função logística de saúde em operações navais (ON) é dotada de características especiais que a distingue daquela das demais forças sin-gulares pois exige uma preocupação constante com a manutenção do estado de higidez, com a capacidade de recuperação das baixas e com a estruturação de uma cadeia de evacuação, num ambiente caracteriza-do muitas vezes pelo isolamento, pela austeridade do clima, pelos espa-ços exíguos e pela limitação dos recursos de saúde disponíveis.
Por outro lado, o Brasil assistiu recentemente a sérios desastres naturais e antropogênicos, destacando-se as cheias em Santa Catari-na e a intervenção na saúde pública em Recife, em 2008. No presente ano as cheias no Norte e Nordeste, alcançaram a quantidade de mais de um milhão de atingidos. Estudos recentes indicam que o aqueci-mento global tende a piorar as situações de desequilíbrio na natureza, apresentando assim uma tendência a aumentar os desastres naturais.
Além disso, o incremento de algumas atividades econômicas, co-mo os cruzeiros turísticos e a exploração de petróleo, coloca a Amazô-nia Azul numa situação de cenário para possíveis sinistros.
Por fim, o Brasil tem aumentado as suas atividades militares pe-rante a Organização das Nações Unidas (ONU), tendo a Marinha do Brasil (MB) um papel de destaque nesse contexto, como integrante do Sistema de Pronto Emprego das Nações Unidas.
CADEIA DE EVACUAÇÃOA cadeia de evacuação é formada pelo conjunto de instalações de
saúde dispostas desde a frente de combate até a retaguarda, com a fi-nalidade de promover o tratamento das baixas com sua recuperação ou evacuação. As instalações de maior porte previstas atualmente na dou-trina de apoio de saúde em ON são o hospital de campanha (HCamp) e o navio de recebimento e tratamento de baixas (NRTB).
A IMPORTÂNCIA DE UM NAVIO-HOSPITAL NA MB
AUTOR: CT (Md) HEMERSON DOS SANTOS LUZGraduação em Medicina pela UFF.Especialização em Doenças Infecto-Contagiosas pela PUC-RJ.Especialização em Medicina Interna pela UFRJ.Aperfeiçoamento em Doenças Infecto-Contagiosas pelo HNMD.Estágio em Operações Ribeirinhas no Batalhão de Operações Ribeirinhas da Marinha do Brasil - Manaus.Estágio Básico de Combatente de Montanha no 11º BIMth - São João Del Rey.Surface Warfare Medical Department Officer (SWMDO) - a bordo do USNS Comfort.
RESUMOUm navio-hospital é uma estrutura hospitalar com capacidade de suporte de saúde avançado, com mobilidade e flexibilidade suficientes para apoiar
operações navais, desastres e missões humanitárias. Com o incremento das atividades econômicas no mar territorial brasileiro e também dos desastres nos últimos anos, destaca-se o nicho que poderia ser ocupado por esse meio de superfície especializado. É um importante instrumento de projeção do poder naval em tempo de paz, nas ações de assistência cívico-sociais (Aciso) e em apoio a exercícios e operações combinadas ou conjuntas.
Palavras-chave: navio-hospital; desastres; UNSA.
MEDICINA DE DESASTRES Compreende a área do conhecimento médico que se ocupa do
atendimento das vítimas com patologias adquiridas, em circunstâncias de desastre. A medicina de desastres possui alguns princípios doutri-nários básicos que são citados a seguir.
A MB evoluiu muito nos últimos anos no apoio de saúde em situações de desastres, como visto no HCamp do Campo de San-tana em 2005 (desastre por somação), no HCamp para o combate à dengue em Nova Iguaçu em 2008 (desastre antropogênico) e o apoio na região do 5˚ DN, após as inundações ocorridas em 2008 (desastre natural). O crescente emprego do pessoal do Corpo de
A) PRINCÍPIO DA PADRONIzAÇÃO DE CONDUTASEm situações de emergência há um incremento de demanda, porém não deve ocorrer a redução no pa-drão de qualidade dos atendimentos.
B) PRINCÍPIO DOS PRAzOS BIOLóGICOSO atendimento às emergências médicas e cirúrgicas depende de prazos biológicos impostergáveis. Com o passar do tempo, quadros clínicos, antes facilmente reversíveis, tendem a agravar-se e a apresentar níveis crescentes de complicação, evoluindo para situações de progressiva irreversibilidade, que poderiam ser pre-venidas, se oportunamente atendidas.
C) PRINCÍPIO DA TRIAGEMA triagem tem por finalidade identificar pacientes em risco de morte e que serão salvos caso recebam prioridade, que lhes assegure cuidados imediatos, preferenciais e oportunos. A utilização de um método padronizado de triagem visa à economia de tempo e dos recursos envolvidos, devendo ser realizada em todos os escalões da cadeia de evacuação, consti-tuindo um processo contínuo e flexível.
Quadro 1: Os princípios doutrinários da medicina de desastres.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 24-27 - 25
Saúde da Marinha nessas circunstâncias, em operações de paz da ONU e em outras situações consideradas operativas fez com que a Alta Administração Naval criasse na estrutura organizacional da MB o Centro de Medicina Operativa da Marinha (CMOpM) em 2009, organização militar (OM) que, entre as suas inúmeras atribui-ções, tem a capacidade de planejar, executar e controlar as ativida-des de resposta médica militar em desastres.
FATORES DE RISCO NA COSTA BRASILEIRAO impacto que o incremento das viagens de cruzeiro que transita-
ram nos portos brasileiros nos últimos anos e o aumento significativo das plataformas de petróleo, em operação no litoral brasileiro na Ama-zônia Azul, colocam a MB com uma responsabilidade ímpar perante eventuais eventos adversos.
Os 8.500 quilômetros da costa brasileira apresentam um movimen-to crescente de navios de cruzeiro de cabotagem, como pode ser ob-servado na Tabela 1.
Um acidente de grande porte em meio flutuante desse tipo, dadas as proporções envolvidas, poderia colapsar o sistema de atendimento de urgências de um grande centro, sem levar em conta a dificuldade da própria evacuação dos feridos até os hospitais de referência.
Tabela 1: Crescimento nos cruzeiros de cabotagem no Brasil
* Considerando que cada navio pode ter a capacidade de transportar de 700 a 2,8 mil passageiros, a média é estimada em 2 mil/navio. Isso totaliza aproximadamente mais de 100 mil passageiros transitando pela costa brasileira nos últimos anos.
Por sua vez, o grande número de plataformas de exploração de pe-tróleo na costa brasileira também chama a atenção, a despeito do exce-lente apoio de saúde que possuem. Essas plataformas possuem um mi-ni-hospital voltado para situações de emergência com múltiplas vítimas, geralmente com cinco leitos para suporte avançado de vida (Quadro 2).
Há um sistema de logística para dar suporte ao médico de plataforma. Um médico está disponível durante 24 horas para dis-cutir os casos complicados ou orientar os trâmites para a reali-zação de exames laboratoriais e radiológicos. Em casos graves realiza-se a remoção em um helicóptero UTI para um hospital predeterminado. Faz parte da rotina da tripulação treinar situa-ções de emergência como incêndio, vazamento de gás, explosão etc. A participação médica nos treinamentos é essencial e visa à capacitação do grupo de resgate para prestar os primeiros socor-ros às vítimas e auxiliar no atendimento médico.
Quadro 2: Material para suporte avançado de vida nas plataformas.
A MB E O SISTEMA DE PRONTO EMPREGO DAS NAÇÕES UNIDAS
Em janeiro de 1996 o Brasil aderiu ao sistema denominado United Nations Standby Arrangements (UNSA). No que concerne aos meios da MB, foi colocada à disposição, entre outras unidades, uma unidade médica nível dois (UMND). O comprometimento do Brasil com o UNSA não prevê, em princípio, a participação de forças navais. Entretanto, a convite das Nações Unidas e, após a devida autorização do Congres-so Nacional, a MB poderá ser incumbida de constituir forças navais, as quais, observando as limitações legais estabelecidas, poderão vir a realizar várias tarefas, entre as quais:• contribuirparaapoiohumanitário;• prestarassistênciaarefugiadosporviamarítima;• evacuarememergênciaosbrasileirosoumesmopessoasdeoutras
nacionalidades que se encontrem participando de operações de ma-nutenção da paz; e
• alojartemporariamentetropasdaONUourefugiados.
Temporada Cruzeiros (Navios Transatlânticos)
Média de passageiros *
2001/2002 6 12.000
2002/2003 5 10.000
2003/2004 7 14.000
2004/2005 6 12.000
2005/2006 9 18.000
2006/2007 11 22.000
2007/2008 14 28.000
Cardioversor automático
Material completo de assistência ventilatória (Ambu, oxigênio, tubos, laringoscópio e kit de traqueostomia)
Bandejas de sutura
Material para imobilização cervical e de membros
Kit de drenagem torácica
Medicamentos de emergência e de atendimento ambulatorial
Figura 1: NDCC Mattoso Maia em missão no Haiti.
A tripulação máxima é de 150 pessoas, sendo que o sistema na bacia marítima, saltou de 28 plataformas de exploração de pe-tróleo em 1997 para mais de 120 plataformas em 2008, algumas a mais de 200 km da costa. Assim, é nítida a necessidade de uma atenção maior para a possibilidade de sinistros, inclusive a even-tualidade de atentados terroristas contra esses meios. O quadro a seguir discrimina o material constante para suporte avançado de vida utilizado nas plataformas.
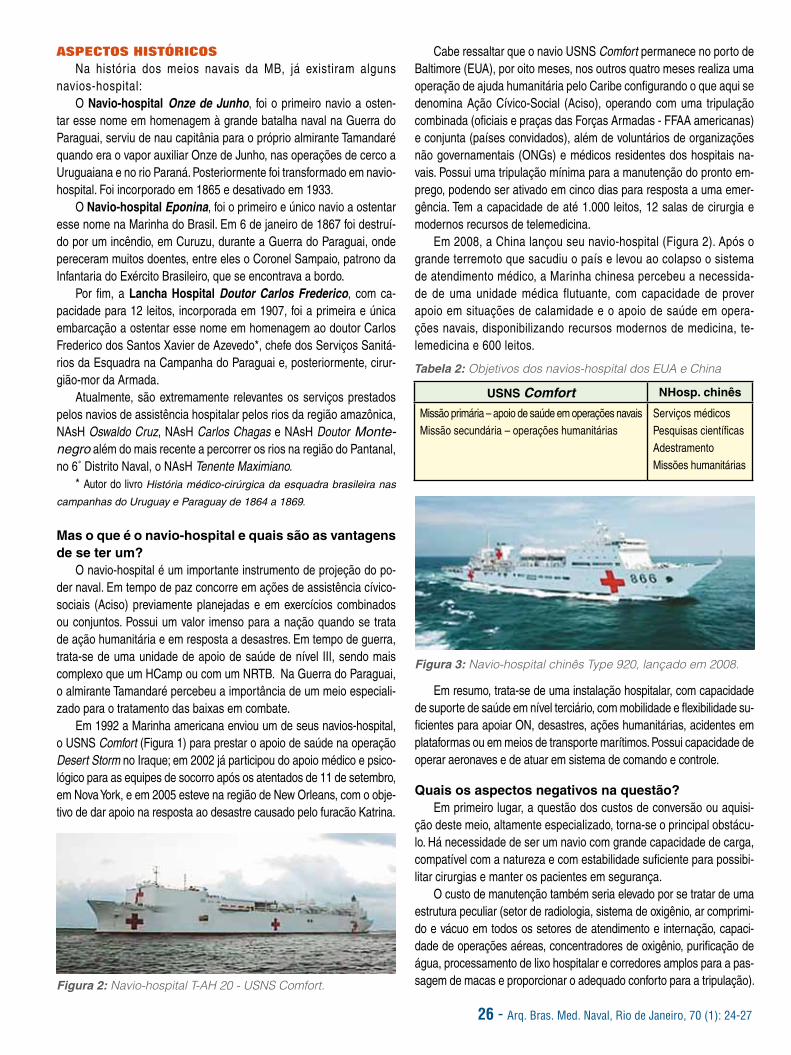
26 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 24-27
ASPECTOS HISTÓRICOSNa história dos meios navais da MB, já existiram alguns
navios-hospital:O Navio-hospital Onze de Junho, foi o primeiro navio a osten-
tar esse nome em homenagem à grande batalha naval na Guerra do Paraguai, serviu de nau capitânia para o próprio almirante Tamandaré quando era o vapor auxiliar Onze de Junho, nas operações de cerco a Uruguaiana e no rio Paraná. Posteriormente foi transformado em navio-hospital. Foi incorporado em 1865 e desativado em 1933.
O Navio-hospital Eponina, foi o primeiro e único navio a ostentar esse nome na Marinha do Brasil. Em 6 de janeiro de 1867 foi destruí-do por um incêndio, em Curuzu, durante a Guerra do Paraguai, onde pereceram muitos doentes, entre eles o Coronel Sampaio, patrono da Infantaria do Exército Brasileiro, que se encontrava a bordo.
Por fim, a Lancha Hospital Doutor Carlos Frederico, com ca-pacidade para 12 leitos, incorporada em 1907, foi a primeira e única embarcação a ostentar esse nome em homenagem ao doutor Carlos Frederico dos Santos Xavier de Azevedo*, chefe dos Serviços Sanitá-rios da Esquadra na Campanha do Paraguai e, posteriormente, cirur-gião-mor da Armada.
Atualmente, são extremamente relevantes os serviços prestados pelos navios de assistência hospitalar pelos rios da região amazônica, NAsH Oswaldo Cruz, NAsH Carlos Chagas e NAsH Doutor Monte-negro além do mais recente a percorrer os rios na região do Pantanal, no 6˚ Distrito Naval, o NAsH Tenente Maximiano.
* Autor do livro História médico-cirúrgica da esquadra brasileira nas
campanhas do Uruguay e Paraguay de 1864 a 1869.
Mas o que é o navio-hospital e quais são as vantagens de se ter um?
O navio-hospital é um importante instrumento de projeção do po-der naval. Em tempo de paz concorre em ações de assistência cívico-sociais (Aciso) previamente planejadas e em exercícios combinados ou conjuntos. Possui um valor imenso para a nação quando se trata de ação humanitária e em resposta a desastres. Em tempo de guerra, trata-se de uma unidade de apoio de saúde de nível III, sendo mais complexo que um HCamp ou com um NRTB. Na Guerra do Paraguai, o almirante Tamandaré percebeu a importância de um meio especiali-zado para o tratamento das baixas em combate.
Em 1992 a Marinha americana enviou um de seus navios-hospital, o USNS Comfort (Figura 1) para prestar o apoio de saúde na operação Desert Storm no Iraque; em 2002 já participou do apoio médico e psico-lógico para as equipes de socorro após os atentados de 11 de setembro, em Nova York, e em 2005 esteve na região de New Orleans, com o obje-tivo de dar apoio na resposta ao desastre causado pelo furacão Katrina.
Figura 2: Navio-hospital T-AH 20 - USNS Comfort.
Cabe ressaltar que o navio USNS Comfort permanece no porto de Baltimore (EUA), por oito meses, nos outros quatro meses realiza uma operação de ajuda humanitária pelo Caribe configurando o que aqui se denomina Ação Cívico-Social (Aciso), operando com uma tripulação combinada (oficiais e praças das Forças Armadas - FFAA americanas) e conjunta (países convidados), além de voluntários de organizações não governamentais (ONGs) e médicos residentes dos hospitais na-vais. Possui uma tripulação mínima para a manutenção do pronto em-prego, podendo ser ativado em cinco dias para resposta a uma emer-gência. Tem a capacidade de até 1.000 leitos, 12 salas de cirurgia e modernos recursos de telemedicina.
Em 2008, a China lançou seu navio-hospital (Figura 2). Após o grande terremoto que sacudiu o país e levou ao colapso o sistema de atendimento médico, a Marinha chinesa percebeu a necessida-de de uma unidade médica flutuante, com capacidade de prover apoio em situações de calamidade e o apoio de saúde em opera-ções navais, disponibilizando recursos modernos de medicina, te-lemedicina e 600 leitos.
USNS Comfort NHosp. chinês
Missão primária – apoio de saúde em operações navaisMissão secundária – operações humanitárias
Serviços médicosPesquisas científicasAdestramentoMissões humanitárias
Tabela 2: Objetivos dos navios-hospital dos EUA e China
Figura 3: Navio-hospital chinês Type 920, lançado em 2008.
Em resumo, trata-se de uma instalação hospitalar, com capacidade de suporte de saúde em nível terciário, com mobilidade e flexibilidade su-ficientes para apoiar ON, desastres, ações humanitárias, acidentes em plataformas ou em meios de transporte marítimos. Possui capacidade de operar aeronaves e de atuar em sistema de comando e controle.
Quais os aspectos negativos na questão?Em primeiro lugar, a questão dos custos de conversão ou aquisi-
ção deste meio, altamente especializado, torna-se o principal obstácu-lo. Há necessidade de ser um navio com grande capacidade de carga, compatível com a natureza e com estabilidade suficiente para possibi-litar cirurgias e manter os pacientes em segurança.
O custo de manutenção também seria elevado por se tratar de uma estrutura peculiar (setor de radiologia, sistema de oxigênio, ar comprimi-do e vácuo em todos os setores de atendimento e internação, capaci-dade de operações aéreas, concentradores de oxigênio, purificação de água, processamento de lixo hospitalar e corredores amplos para a pas-sagem de macas e proporcionar o adequado conforto para a tripulação).

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 24-27 - 27
Os equipamentos de saúde pertencendo ao navio elevariam o custo ain-da mais para a manutenção de sua capacidade operativa. O ideal seria deixar uma margem de operação satisfatória em tempo de paz e uma capacidade de expansão dependendo da mobilização de meios oriun-dos do Sistema de Saúde da Marinha (SSM) (por exemplo: quatro salas cirúrgicas, operando apenas uma em tempo de paz ou possuir 20 leitos de emergência, operando apenas cinco em tempo de paz).
Caso todo o pessoal de saúde seja oriundo de OM da Diretoria de Saúde da Marinha (DSM), isso poderia afetar a capacidade de atendi-mento do Subsistema Assistencial da Marinha.
CONCLUSÂOA MB não possui um navio-hospital de grande porte, pronto para
responder a um apoio de saúde de alta complexidade, em ON, desas-tres, acidentes e ações humanitárias.
Com um navio-hospital, a MB poderia responder, de uma forma ímpar, a esses chamados, aplicando os conceitos doutrinários da me-dicina de desastres e otimizando a cadeia de evacuação em ON, além de poder atuar em missões humanitárias proporcionando alívio ao so-frimento físico e psicológico dos desabrigados, deslocados e atingidos por desastres ou catástrofes.
O pessoal empregado nas operações do navio-hospital poderá ser oriundo, além da DSM, também das outras forças similares, operan-do com tripulações combinadas. O uso de tripulações combinadas em operações ou exercícios e em ações de resposta a desastres, já é uma realidade na MB.
O navio permaneceria com uma tripulação mínima para a prontifica-ção, e ativação em caso de necessidade, o que reduziria em muito o seu custo de operacional. Tal navio poderia complementar a capacidade de atendimento médico, quando atracado, na própria Base Naval do Mocan-guê, onde os profissionais de saúde poderiam utilizar as dependências do navio para atendimento aos militares pertencentes à esquadra.
Com o propósito de integrar o pessoal de saúde com a vida de bordo, tal navio poderia realizar uma viagem de instrução para os ofi-ciais alunos do Curso de Formação de Oficiais do Corpo de Saúde da Marinha, podendo ser uma viagem de 1 a 2 meses, com ênfase nas instruções de medicina operativa (MedOp) durante as travessias e com atendimento médico em localidades previamente planejadas (Aciso), principalmente em locais sujeitos a desastres ou com ca-rência de assistência médica (Santa Catarina e Nordeste). Médicos residentes e alunos do Curso de Aperfeiçoamente (C-Ap), também poderiam embarcar em caráter voluntário, sendo considerado como atividade extracurricular prevista no C-Ap.
É óbvio que a aquisição ou conversão de um meio assim tão espe-cializado demandaria estudos mais abrangentes e multidisciplinares en-volvendo outras OM. O futuro é construído em cada dia do presente e a presença de um navio-hospital na MB coaduna com a própria evolução vivenciada atualmente, tanto em relação à perspectiva dos meios opera-tivos (submarino nuclear brasileiro) como no SSM (criação do CMOpM).
A capacidade sugerida (Quadro 3) serve apenas como dado nu-mérico, baseado em experiências do CMOpM na operação do HCamp em operações humanitárias (Aciso, dengue).
- Setor de triagem e recebimento de pacientes (unidade de trauma com 20 leitos)
- Unidade de pacientes graves (no mínimo 10 leitos de UPG)
- UTI com 10 leitos (no mínimo)
- Unidade de Clínica Médica
- Unidade de Ortopedia
- Unidade de Ginecologia
- Chefia de Enfermagem
- Enfermarias com 120 leitos (no mínimo)
- Unidade de Odontologia até quatro consultórios
- Centro cirúrgico (no mínimo quatro mesas de cirurgia)
- Centro de esterilização e processamento de material
- Unidade de laboratório
- Farmácia/paiol
- Unidade de comando e controle médico
- Unidade de raio X com processadora automática
- Unidade de Oftalmologia
- Serviço de apoio psiquiátrico
- Banco de sangue
- Oficinas
- Paióis
- Setor de manutenção de aparelhos médicos
- Epidemiologia e controle das doenças
- Pré-operatório 10 leitos
- Pós-anestesia 10 leitos
- Paiol de equipamentos
- Fisioterapia
- 10 leitos de isolamento (risco NBQ, incluindo doenças contagiosas)
- Mais 30 macas de transporte para se converter outros compartimentos (academia, refeitório etc.) em enfermaria
- Total sugerido: 200 leitos
Quadro 3: Capacidade sugerida de um navio-hospital de médio porte.

28 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 28-31
THE IMPORTANCE OF A HOSPITAL SHIP AT THE BRAZILIAN NAVY
AUTHOR:CT (Md) HEMERSON DOS SANTOS LUZ Bachelor’s Degree in Medicine from UFF.Specialization in Infectious and Communicable Diseases from PUC-RJ.Specialization in Internal Medicine from UFRJ.Extended Training in Infectious and Communicable Diseases at HNMD. Internship in Riparian Operations at the Riparian Operations Battalion of the Brazilian Navy – Manaus.Basic Internship in Mountain Combat at the 11st BIMth - São João Del Rey.Surface Warfare Medical Department Officer (SWMDO) – on board the USNS Comfort.
ABSTRACTA hospital ship is a floating facility that supplies advanced medical support and whose mobility and flexibility allows for base aid to naval
operations, disasters and humanitarian relief missions. The increment of economic activities within Brazil’s territorial waters in recent years points to the advantageous usefulness of such facility. A hospital ship is also a major tool and attribute of the Navy powers in times of peace in what concerns civic social assistance and back up for combined or joint naval exercises and operations.
Keywords: hospital ship; disasters; UNSA.
INTRODUCTIONIn order to foster the optimal level of naval force effectiveness, efficient
and compatible support must comply with the nature, volume, length and space of naval operations development. Logistics is responsible for providing such support through the necessary resources to maintain and expand the naval force operating capacity.
The logistic function of medical naval operations holds distinguishing features from the function of other forces, given the constant concern about excellent medical conditions, the capacity for casualty rescue and recovery, and medical challenges in the evacuation chain within an environment characterized by isolation, inhospitable climate, restrained space and limited available medical resources.
It should be noted that there have been serious and anthropogenic disasters recently in Brazil, notably the floods in the state of Santa Catarina and the intervention in public health in the state capital city of Recife in 2008, in which year the floods in Northern and Northeastern states afflicted over one million people. On top of that, recent studies have concluded that global warming tends to aggravate nature’s unbalanced forces, potentially leading to more disasters.
In addition to that, the increment of certain sea-bound economic activities like tour cruises and oil exploration potentially places Blue Amazon at the radial point for possible catastrophes.
Finally, the Brazilian Navy plays a major role within the context of the country’s increased military activities with the UN, as an integral member of the United Nations Stand-by Arrangements System (UNSAS).
EVACUATION CHAINThe evacuation chain comprises a set of medical facilities that are
displaced from the war front to the war rearguard and holding, in order to implement the rescue, treatment, recovery and, if necessary, evacuation of casualties. The largest facilities currently planned for by medical naval
operations are a base camp hospital (CampHosp) and the Casualty Receiving and Treatment Ship (CRTS).
DISASTER MEDICINEThat is the area of medical specialization that provides medical care
to disaster-acquired pathology-bearers. Some of its basic underlying principles are discussed below.
The Brazilian Navy has considerably improved its medical support to disaster survivors in recent years. Examples are the 2005 CampHosp response to a somation-caused disaster in Campo de Santana, the
Principle 1. Standardization of proceduresEvery contingency results in increased demand. However, such si-tuation must not result in reduced quality standards for medical as-sistance.
Principle 2. Biological deadlinesEmergency assistance to medical and surgical contingencies de-pends on pressing biological deadlines. Delayed assistance can aggravate initially reversible clinical conditions and therefore, com-plications set down. Conditions can easily and progressively wor-sen until they become irreversible, whereas they could have been prevented if timely assisted.
Principle 3. ScreeningScreening is meant to identify at-risk patients who can be saved if given priority and therefore, immediate, preferential and timely medical assistance. A standardized screening method is time-saving as well as resource-saving, and must be implemented at all evacuation levels, thus constituting a continuous and flexible enough process.
Chart 1: Underlying principles of disaster medicine.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 28-31 - 29
CampHosp anthropogenic response to dengue combat in Nova Iguaçu in 2008, and the support provided to the 5th National District after the 2008 floods, a natural disaster response. The increasing use of the Navy’s Medical Staff in such situations, in UN peace operations and in other types of situations led the Higher Navy Management to establish the Centro de Medicina Operativa da Marinha (CMOpM) in 2009, a military organization whose main functions, among many, are the planning, execution and supervision of the military contingency medical response to disasters.
RISK FACTORS ALONG THE BRAZILIAN COASTThe impact generated by cruise tours along the Brazilian coast in
recent years and the significant increase of oil platforms in operation on the Brazilian coast of the Blue Amazon have conferred to the Brazilian Navy an unprecedented responsibility in what concerns response to adverse events.
Table 1 above shoes the increase in coastal navigation along the 8,500 kilometers along Brazilian coast.
A major accident with an ocean liner could result in a collapse of the contingency assistance system of a naval center, not to mention the hardships to be endured regarding the evacuation of victims to the nearest inland hospitals.
In addition to that, the increasing number of oil platforms in operation on the Brazilian coast is another issue to be addressed, despite the excellent medical assistance support they bear. The platforms usually have a mini-hospital to care for multiple victim contingencies with generally five beds for advanced life support (Chart 2).
The platform physicians can also count on a logistics system that provides 24-hour support to discuss the most challenging cases and provide guidance for procedures, laboratory and radiology exams. For the most serious cases an ICU-equipped helicopter is available to fly patients to a specific inland hospital. The platform crew regularly trains for contingencies like fire, gas leaks, explosions, etc. and medical staff participation is mandatory, for they must be trained
Season Cruisers(Ocean liners)
Average no. of pax *
2001/2002 6 12,000
2002/2003 5 10,000
2003/2004 7 14,000
2004/2005 6 12,000
2005/2006 9 18,000
2006/2007 11 22,000
2007/2008 14 28,000
Table 1: Increase in coastal navigation in Brazil
* Considering that each liner has a passenger capacity of 700 to 2.8 thousand, the estimated average is 2,000 pax/liner. That totals more than 100 thousand passengers sailing the Brazilian coast in recent years.
to aid the rescue team in delivering first aid assistance to the victims and start medical assistance.
The crew may consist of no more than 150 people. However, the number of oil platforms along the coast has jumped from 28 in 1997 to over 120 in 2008, some of which are more than 200 km offshore. This clearly points to the higher possibility of accidents, including terrorist attacks. The chart below lists the regular minimum required devices for advanced life support at platforms.
THE BRAZILIAN NAVY AND THE UNITED NATIONS STAND-BY ARRANGEMENTS SYSTEM (UNSAS)
In January 1996 Brazil joined the so-called United Nations Standby Arrangements System (UNSAS) and has made a number of the Brazilian Navy’s resources available to the UN, among which a Level 2 Medical Unit. However, Brazil’s commitment towards UNSAS did not initially comprise the participation of the country’s naval force. Nevertheless, upon invitation by the UN and after due authorization by the National
Automatic cardioverter
Complete set of ventilatory assistance devices (Ambu, oxygen, tubes, laryngoscope and tracheotomy kits)
Stitch set trays
Cervical and limb immobilization devices
Chest drainage kit
Emergency medication and ambulatory assistance devices
Chart 2: Advanced life support devices available at the platforms.
Congress, the Brazilian Navy may be convened to constitute a naval force that might eventually, in compliance with all the established legal constraints, perform a number of tasks, among which are the following:•Contributeforhumanitarianrelief;•Assistsurvivorsandrefugeesinmaritimecontexts;•EvacuateonacontingencybasisBraziliansandalsoforeignersthat are involved in peace negotiation operations; and•Host,onatemporarybasis,UNtroopsorrefugees.
Figure 1: NDCC (LST, or Landing Ship Tank) Mattoso Maia, on a mission in Haiti.

30 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 28-31
HISTORICAL BACKGROUNDThe history of the Brazilian Navy shows the existence of hospital
ships in the past:The Onze de Junho hospital ship was named after the great naval
battle in the Paraguay War. It served as admiral ship for Admiral Tamandaré when it was still an auxiliary steam ship used in the siege operations to Uruguaiana and in the Paraná River. It was later reshaped into a hospital ship, added to the naval force in 1865 and deactivated in 1933.
The Eponina hospital ship was the first and only ship to hold such name in the Brazilian Navy. On January 6 1867 it was destroyed by a fire in Curuzu, during the Paraguay War, and amongst the many casualties was Colonel Sampaio, the patron official for the Brazilian Army Infantry.
And lastly the Doutor Carlos Frederico hospital boat, with a capacity for 12 beds, added to the naval force in 1907, the first and only boat to hold this name as homage to Dr. Carlos Frederico dos Santos Xavier de Azevedo*, Chief of Squad for Sanitarian Services during the Paraguay War and later Chief Surgeon of the Brazilian Fleet.
The hospital ships that are currently operating in the rivers of the Amazon region - NAsH Oswaldo Cruz, NAsH Carlos Chagas, NAsH Doutor Montenegro, and the recently added NAsH Tenente Maximiano at the 6th Naval District, sailing along the Pantanal rivers – perform extremely relevant services.
* Author of the book História médico-cirúrgica da esquadra brasileira
nas campanhas do Uruguay e Paraguay de 1864 a 1869 (‘A medical-
surgical history of the Brazilian fleet in the Uruguay and Paraguay Wars,
from 1864 to 1869’).
WHAT EXACTLY IS A HOSPITAL SHIP AND WHAT ARE ITS ADVANTAGES FOR THE NAVAL FORCE?
The hospital ship is a major attribute of a country’s naval force. In times of peace it performs previously planned civic social assistance, as well as in combined or joint naval exercises. It is of great worth for a nation in what regards humanitarian relief action and response to disasters. And in times of war, it becomes a Level III medical support unit, as it is equipped with more complex facilities than a CampHosp or a Casualty Receiving and Treatment Ship (CRTS). During the Paraguay War, Admiral Tamandaré learned how relevant a CRTS was.
Figure 2: Hospital ship T-AH 20 - USNS Comfort.
In 1992 the American Navy sent one of its hospital ships, USNS Comfort (Fig. 1) to perform medical support services for the Desert Storm operation in Iraq. And in 2002 this ship provided medical and psychological services for the rescue teams who worked on the
September 11 terrorist attack to Nova York. Again in 2005 the ship went to New Orleans as a response measure to the disaster caused by the Katrina hurricane.
It should be noted that the USNS Comfort is docked at the Baltimore port eight months a year, and in the other four months it performs humanitarian relief services in the Caribbean through civic social actions. There is a mixed-force (US Armed Forces officers and soldiers) and joint-force (guest countries) crew, besides volunteers from non-governmental organizations (NGOs) and hospital ship resident physicians. It carries a minimum crew for stand-by arrangements and can be ready in five days for contingency response. Its capacity is for up to 1,000 beds, 12 surgery rooms and state-of-the-art telemedicine resources.
USNS Comfort Chinese Hospital ship
Primary Mission – medical support to naval ope-rationsSecondary Mission – humanitarian relief ope-rations
Medical servicesScientific researchTrainingHumanitarian relief missions
Table 2: Objectives of hospital ships in the US and China
In 2008 China launched its hospital ship (Fig. 2) after the earthquake that shook the country and caused the collapse of the medical system. The Chinese Navy realized the need for a permanent floating medical unit able to provide support to disasters and medical services for naval operations. This ship has a capacity of 600 beds and state-of-the-art telemedicine resources.
In conclusion, a hospital ship is a floating hospital facility able to provide III medical support, whose mobility and flexibility allows for support to naval operations and response to disasters, humanitarian relief actions, offshore platform accidents or even still maritime transportation accidents. It has the capabilities to operate aircraft and management and control systems.
WHAT POSSIBLE DISADVANTAGES ARE THERE?Firstly, the costs of converting or acquiring this highly specialized
ship constitute the major obstacle to its operation. It must have a large cargo capacity, be compatible with the nature of the operations, and stable enough to ensure surgery performance and patient total safety and security.
Maintenance costs would also be high because of its specialized infrastructure - radiology unit, oxygen system, compressed and vacuum air system in all the medical assistance units, capability for
Figure 3: Chinese hospital ship Type 920, launched in 2008.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 28-31 - 31
air operations, oxygen concentrators, water purification systems, hospital waste processing, and wide corridors to give way to stretch transportation and crew comfort. Health equipment would add to the ship operating capacity and maintenance costs. Ideally, a comfort margin for times of peace should be allocated, which could be expanded depending on the mobilization of funds by the Navy Health System – for instance, four surgery rooms, with only one of which operating in times of peace, or having 20 emergency beds, five of which operating in times of peace.
And last but not least, another consideration is that if all the staff came from the Healthcare Executive Board of the Brazilian Navy, this might affect the assistance capacity of the Navy Assistance Sub-system.
CONCLUSIONSThe Brazilian Navy does not own a large hospital ship that is able
to respond to naval operations, disasters, accidents and humanitarian relief situations with high-complexity medical services support.
However, if did, the Navy would provide unmatched response to such contingencies. It would also be able to practice the underlying principles of disaster medicine, to optimize the evacuation chain in naval operations, to act in humanitarian relied missions and to assist those in physical and psychological pain, homeless, and victims of disasters or catastrophes.
The crew could come from the Healthcare Executive Board of the Navy as well as from other similar forces and operate on a combined-force crew basis. The use of combined forces in disaster response exercises and operations is already in effect in the Brazilian Navy.
The ship would have a minimum crew for stand-by arrangements and could draft additional crew whenever necessary. This measure would
significantly reduce its operating costs. The complementary medical assistance capacity could be based where the ship would be docked, at Mocanguê Naval Base, where the health professionals would use the ship facilities to provide the local fleet militaries with medical assistance.
In order to integrate the medical staff to on-board routine, the ship could implement a one or two-month on-board instruction trip for the training officers of the Navy Healthcare Qualification Course. Such course would focus on operational medicine (OpMed) during offshore trips and on medical assistance at previously-planned onshore locations (civic social actions), mainly in those places that are commonly subject to disasters (Santa Catarina) or which lack medical assistance (Northeastern states). Resident physicians and students of the Medical Staff Development Course (C-Ap, from the original in Portuguese) would also be welcome on board to work on a volunteer basis and gain extracurricular credits as established by the C-Ap.
The acquisition or conversion of a ship of this type would naturally require more comprehensive and multidisciplinary studies involving other navy operations. However, the future is built every single day of the present and the Navy owning a hospital ship is consonant with the evolution pattern that has settled in this government institution recently, in what regards both the perspectives for new operating means (the Brazilian nuclear submarine) and the establishment of the Medicine Division of the Centro de Medicina Operativa da Marinha.
The suggested capacity (Chart 3) provides some numerical data base on the Centro de Medicina Operativa da Marinha experience in the operation of the CampHosp for humanitarian relief (civic social actions, dengue).
- Patient reception and screening Unit (Trauma unit with 20 beds)- Unit for seriously ill patients (with a minimum of 10 beds)
- ICT with 10 beds (minimum number)
- Medical Clinic Unit
- Orthopedics Unit
- Gynaecology Unit
- Chief Infirmary Room
- Infirmaries with 120 beds (minimum number)
- Dentistry Unit with up to four practice rooms
- Surgery room (a minimum of four surgery tables)
- Sterilization and material processing center
- Laboratory Unit
- Pharmacy / storeroom
- Medical command and control Unit
- X-ray Unit, with automatic processor
- Ophthalmology Unit
-Psychiatric support service
- Blood bank
- Workshops
- Storerooms
- Medical device maintenance room
- Epidemiology and disease control
- 10 pre-surgery beds
- 10 post-anesthesia beds
- Equipment storeroom
- Physiotherapy
- 10 isolation beds (for NBQ [nuclear, biological, and chemical] risk, including contagious diseases)
- More than 30 transport stretchers to help turn other ship compart-ments (gym, cafeteria, etc) into infirmaries
- Suggested total of: 200 beds
Chart 3: Suggested capacity for a middle-sized hospital ship.

32 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 32-35
ANALGESIA INALATÓRIA COM ÓXIDO NITROSO NA CLÍNICA DE CIRURGIA BUCO-MAXILO-FACIAL DA POLICLÍNICA NAVAL NOSSA SENHORA DA GLÓRIA: ANÁLISE DE 260 CASOS
AUTORESCF (CD) MARCELO ROSADO BOTELHO, M.D. Graduação em Odontologia pela UFF.Habilitação em Analgesia Inalatória pela PUC-RJ.Mestrado em Cirurgia Buco-Maxilo-Facial pela UNICAMP.Coordenador do Curso de Especialização em Cirurgia Buco-Maxilo-Facial da Marinha.Encarregado do Setor de Cirurgia Buco-Maxilo-Facial sob Analgesia Inalatória da PNNSG.
CMG (Md-RM1) MARYANGELA FORONI MONTEIRO Graduação em Medicina pela Escola de Ciências Médicas de Volta Redonda.Residência em Anestesiologia pela UERJ.CAT em Anestesiologia pelo HNMD.Anestesiologista do Centro Cirúrgico Ambulatorial da PNNSG.
CT (CD) GUILHERME LIMA PONTES Graduação em Odontologia pela Universidade Estácio de Sá.Especialização em Cirurgia Buco-Maxilo-Facial pela Marinha.Habilitação em Analgesia Inalatória pela PUC-RJ.Assistente do Serviço de Analgesia Inalatória da PNNSG.
1ºT (CD-RM2) SANNY NORONHA Graduação em Odontologia pela UGF.Especialização em Odontopediatria pela Universidade Estácio de Sá.Assistente do Serviço de Analgesia Inalatória da PNNSG.
1ºT (CD) EMANUELA PRADO FERRAZ Graduação em Odontologia pela Faculdade de Odontologia de Ribeirão Preto - USP.Especialização em Cirurgia Buco-Maxilo-Facial pela USP-RP.Habilitação em Sedação Inalatória pela UFRJ.Assistente do Serviço de Analgesia Inalatória da PNNSG.
LILIA REGINA PAIVAGraduação em Enfermagem pela Unirio.Especialização em Enfermagem Médico-cirúrgica e Enfermagem do Trabalho pela UGF.Enfermeira encarregada do Centro Cirúrgico Ambulatorial da PNNSG.
RESUMOApesar de todos os avanços científicos e tecnológicos, o tratamento odontológico continua sendo associado à dor, o que leva muitos pacientes a apre-
sentar diferentes graus de ansiedade, podendo desenvolver reações desagradáveis que podem inviabilizar a execução do procedimento cirúrgico. Desse modo, o controle da dor e da ansiedade é uma etapa fundamental que deve ser considerada na consulta inicial. Há uma série de mecanismos disponíveis para esse controle, que variam desde métodos não farmacológicos até a anestesia geral. Nos últimos anos, a utilização da sedação consciente com óxido nitroso vem sendo amplamente aplicada, por apresentar resultados eficazes, ter excelente aceitação pelos pacientes e ser uma técnica extremamente segura, quando comparada com outros métodos de sedação. Apresentaremos a nossa experiência com a técnica neste serviço.
Palavras-chave: sedação consciente; óxido nitroso.
INTRODUÇÃOOs conceitos de dor, medo e ansiedade sempre estiveram ligados
à prática odontológica, mais intimamente a procedimentos cirúrgicos, por serem normalmente mais invasivos e por muitas vezes traumáti-cos. Em um levantamento realizado com 1.000 adultos sobre os medos
mais comuns, a segunda resposta mais frequente foi “ir ao dentista” (Dental Health Advisor, 2003). Desse modo, um dos grandes desafios enfrentado pelos profissionais está relacionado ao controle da ansie-dade, que em muitos casos pode comprometer o atendimento.
Aspectos psicológicos têm grande influência na condição clínica

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 32-35 - 33
dos indivíduos, inclusive diminuindo o limiar de percepção dolorosa. Indivíduos ansiosos podem apresentar aumento da frequência cardía-ca e respiratória, aumento da pressão arterial sistêmica, transpiração excessiva, dilatação pupilar, tremores das extremidades, sensação de formigamento. Pacientes portadores de doenças cardiovasculares, res-piratórias, endócrinas entre outras, mesmo quando controladas, po-dem apresentar descompensação do quadro sistêmico, gerando uma emergência médica no consultório odontológico, como angina pecto-ris, infarto agudo do miocárdio, síncope (Andrade, 2006).
Malamed et al. (1993) realizaram um levantamento em um pe-ríodo de 10 anos, envolvendo mais de 4.000 dentistas que relatam mais de 30.000 episódios de emergências médicas em seus con-sultórios. Entre as complicações foram descritos 15.000 casos de lipotimia e síncope vasopressora, 1.300 casos de hiperventilação e cerca de 3.000 alterações cardiovasculares, todas as alterações relacionadas ao estresse. Nesse mesmo estudo também foi obser-vado que aproximadamente 55% das emergências médicas acon-teceram durante ou logo após a anestesia local, procedimento que gera dor e ansiedade nos pacientes.
Entre o armamentário que o cirurgião-dentista dispõe para minimi-zar essas situações, e evitar complicações, estão os métodos de con-trole de ansiedade. Há descrito na literatura uma série de alternativas, que variam desde métodos não farmacológicos onde está incluída a tranquilização verbal, até métodos farmacológicos de sedação cons-ciente ou anestesia geral.
A American Dental Association (2003) define sedação consciente co-mo “mínima depressão do nível de consciência do paciente, que não afeta a sua habilidade de respirar de forma automática e independente, e res-ponder de maneira apropriada à estimulação física e ao comando verbal”.
Entre os métodos farmacológicos de sedação consciente, os mais utilizados em odontologia são os benzodiazepínicos por via oral e a mistura de oxigênio e óxido nitroso, empregado por via inalatória.
Os benzodiazepínicos atuam ativando os receptores do ácido gama-aminobutírico (GABA), um neurotransmissor inibitório do sis-tema nervoso central, que induz a abertura dos canais de cloreto e promove o influxo desse ânion para o espaço intracelular, resul-tando, em última análise, na diminuição dos impulsos excitatórios e, desse modo, na redução da ansiedade. Além disso, também pro-movem diminuição do reflexo de vômito e de fluxo salivar, relaxam a musculatura esquelética, ajudam a manter a pressão arterial e glicemia em níveis aceitáveis e no caso do midazolam, produzem amnésia retrógrada (Andrade, 2006).
O óxido nitroso é um gás anestésico incolor, de odor agradável, não inflamável ou irritante, de baixa solubilidade no sangue, não se li-ga a nenhum elemento sanguíneo e não sofre metabolização. Assim, permite indução rápida, controle preciso da dose e apresenta rápida eliminação por expiração, com mínima depressão do centro respira-tório e baixa ação no córtex cerebral. Devido a essas características, os pacientes frequentemente relatam sensação de relaxamento total e bem-estar, formigamento dos lábios e extremidades, sonolência, enquanto mantêm os reflexos de deglutição e tosse intactos. A pres-são arterial, frequência cardíaca e respiratória e glicemia são man-tidas dentro dos níveis aceitáveis (Malamed, 2003; Falqueiro, 2005).
A mistura gasosa de oxigênio e óxido nitroso é o método de sedação consciente que vem sendo amplamente aplicado e divul-
gado no Brasil, através dos cursos de habilitação promovidos por instituições competentes. É uma técnica segura, que pode ser rea-lizada em consultório odontológico em pacientes previamente sele-cionados, altamente eficaz e aceita por grande parte dos pacientes.
HISTÓRICOPor volta de 1770, Joseph Priestley, descobre o óxido nitroso e o
oxigênio. No final do século XVIII, Humphrey Davy, sofrendo com uma odontalgia, inalou óxido nitroso a 100%, e verificou que o gás suprimiu a sensação de dor, além de determinar uma sensação agradável de euforia, aumento da acuidade auditiva e um desejo incontrolável de rir. Esse é o primeiro relato da utilização do gás no controle da dor.
Com o passar dos anos, uma série de outros indivíduos de vá-rias especialidades utilizaram o gás em diferentes experimentos. Até que em 1844 Horace Wells, um dentista americano, observou a reação de um indivíduo com um ferimento corto contuso na perna e sob o efeito do gás. Ao questioná-lo sobre a sensação dolorosa, obteve uma resposta negativa. Nesse momento, Wells vislumbra a possibilidade de utilizar o gás em procedimentos odontológicos e realiza uma exodontia utilizando óxido nitroso puro, classificando a técnica como a maior descoberta de todos os tempos. Infelizmente, durante uma demonstração pública dos efeitos do gás, um pacien-te passa a se comportar de maneira eufórica e a plateia conside-ra esta atitude como uma reação à dor, e o julga como charlatão. Somente anos mais tarde Horace Wells tem o reconhecimento da Associação Dental Americana e da Associação Médica Americana, recebendo o título de “descobridor da anestesia”.
Em 1868, Edmund Andrews passa a misturar 20% de oxigênio ao óxido nitroso, tornando uma mistura mais segura para ser aplicada aos pacientes. Na odontologia, próximo a 1860, a técnica passa a ser am-plamente utilizada.
No Brasil, em 1937, teve início o uso da analgesia inalatória com protóxido e oxigênio. A regulamentação definitiva da técnica de sedação inalatória ocorreu de acordo com o relatório final de dis-cussão do Fórum sobre o Uso da Analgesia em Odontologia, pro-movido pelo Conselho Federal de Odontologia em março de 2004, e encontra-se na Resolução n° 51/2004, de 12 de maio de 2004.
TÉCNICAPara o sucesso da técnica, é necessário que todos os pacientes
sejam inicialmente submetidos a rigorosa anamnese e exame físico. Alguns dados obtidos no exame clínico podem contraindicar relativa-mente o procedimento de analgesia com a mistura dos gases: des-vio de septo nasal, patologias dos seios paranasais (sinusite maxilar), cirurgia prévia em membrana timpânica, mulheres grávidas, crianças com sérios problemas de conduta, pacientes psiquiátricos ou paranoi-cos, e que apresentem fobia com o uso da máscara nasal. As contrain-dicações absolutas para o uso da técnica acontecem devido às altas tensões de O2 utilizadas: indivíduos com doença pulmonar obstrutiva crônica, que normalmente apresentam os quimiorreceptores respon-sáveis pelas trocas gasosas com alterações de sensibilidade, e altas concentrações de oxigênio podem ser interpretadas como um estímulo para reduzir a ventilação, resultando em hipóxia; pacientes com histó-ria de pneumotórax; pacientes submetidos à quimioterapia e que fize-ram uso de bleomicina há pelo menos um ano pela possibilidade de

34 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 32-35
apresentarem fibrose pulmonar (Haas, 1999). Se necessário, exames complementares, radiográficos ou laboratoriais serão solicitados.
Para a realização da técnica, é utilizado um equipamento es-pecífico, composto por: fluxômetro, engates específicos, máscara nasal, mangueiras, cilindros, manômetros e válvulas, balão reser-vatório, sistema de exaustão, oxímetro de pulso e esfignomanôme-tro e estetoscópio.
Antes de dar início à técnica propriamente dita, os pacientes de-vem ser submetidos a um teste psicomotor, sendo o mais comumen-te realizado, o teste desenvolvido por Norman Trieger, o teste de Trie-ger (Trieger et al., 1971). Em seguida, a máscara será selecionada, adaptada ao nariz do paciente devidamente monitorado, e então é iniciada a administração de oxigênio a 100% a 6l/min para adultos e 4l/min em crianças, aproximadamente, por no mínimo três minutos. Com o passar do tempo, e registrando os dados em um prontuário específico, inicia-se a administração do óxido nitroso, incrementan-do-se 10% à mistura a cada 10 minutos, e registrando os parâmetros de monitoramento e sensações descritas pelos pacientes. A concen-tração ideal depende de cada paciente, respeitando-se o limite de 70% de óxido nitroso.
A sedação ideal é atingida quando o paciente passa a relatar: rela-xamento, formigamento das extremidades, calor, analgesia dos tecidos moles, aumento da distância dos sons. Ainda é notado movimento dos membros e palpebrais reduzidos, lacrimejamento e o “sorriso de mo-nalisa” (Falqueiro, 2005).
Apesar de todos os cuidados, há relatos de casos de sobresseda-ção, nos quais os indivíduos passam a apresentar: sonolência, euforia, mal-estar, inquietação, perda de controle, risos, aumento da taxa res-piratória, náusea, tinitus. Nesses casos, ao reverter a sedação, com a administração de oxigênio a 100% por 10 minutos, os sinais e sintomas desaparecerão prontamente.
Após a realização do procedimento planejado, a sedação é rever-tida com a administração de oxigênio a 100% por 10 minutos. Os pa-cientes serão então novamente submetidos ao teste de Trieger para verificação da capacidade motora e somente então liberados.
EXPERIÊNCIA CLÍNICAO público-alvo é caracterizado por pacientes que apresentem du-
rante a anamnese algum tipo de fobia, medo ou ansiedade associado ao tratamento odontológico, pacientes pediátricos e aqueles que são enquadrados em ASA II, cuja manutenção dos níveis adequados de pressão arterial, pulso, frequência cardíaca e respiratória, além de níveis aceitáveis de glicemia são importantes para o sucesso do pro-cedimento. Inicialmente todos os pacientes são submetidos à rigoro-sa anamnese e exame físico e se necessário são solicitados exames complementares laboratoriais. Após a consulta inicial, se estiver in-dicada alguma técnica de sedação, esta é discutida individualmente com cada paciente. Se indicada outra técnica de sedação ou aneste-sia geral, o paciente é encaminhado para realização do pré-operató-rio e risco cirúrgico, para posterior avaliação com médico anestesis-ta que realizará o procedimento. Até o momento, aproximadamente 260 pacientes foram tratados sob sedação. Doze foram submetidos
à sedação oral com benzodiazepínicos (7,5mg de midazolam), 83 à sedação inalatória, 111 à técnica conjugada de ansiolíticos orais e óxido nitroso, 36 à sedação venosa e 18 à anestesia geral (Tabela 1).
Entre os pacientes submetidos à analgesia inalatória, a maioria começou a apresentar os sintomas de sedação a partir da adminis-tração de 30% de óxido nitroso; nenhum precisou de 70% de óxido nitroso para atingir os sintomas desejados (Tabela 2). Em pacientes submetidos à técnica de sedação inalatória associada a ansiolíticos, uma proporção maior apresentou início dos sintomas com a adminis-tração de 20% de óxido nitroso. Além disso, precisam de uma menor quantidade de protóxido para manter os níveis desejáveis de seda-ção durante o procedimento cirúrgico (Tabela 3).
Os sintomas mais comuns foram o formigamento das extremida-des (lábios, dedos das mãos e dos pés), sensação de peso do corpo e de embriaguez. Os sinais mais frequentes foram o sorriso de monalisa (Figura 1), olhar fixo e diminuição da frequência cardíaca.
Dos 194 pacientes submetidos à sedação inalatória associada ou não com midazolam, 13 apresentaram algum tipo de complicação relacionada à analgesia inalatória; cinco não suportaram ficar com a máscara, em dois não foi possível adaptar a máscara por razões ana-tômicas; seis manifestaram sinais de sobressedação: três pacientes tornaram-se eufóricos e inquietos e três referiram náusea. Os sinais e sintomas da sobressedação desapareceram após alguns minutos da administração de 100% de oxigênio (Tabela 4). Sete pacientes não manifestaram nenhum sinal ou sintoma.
A utilização desse tipo de tratamento diferenciado promove uma maior segurança durante o procedimento cirúrgico e aten-dimento odontopediátrico, além de inegável benefício, conforto e bem-estar aos usuários do Sistema de Saúde da Marinha do Brasil. A diminuição do estresse reduz, significativamente, a inci-dência de emergências médicas oriundas do atendimento odon-tológico e sem dúvida melhora a relação e imagem do cirurgião-dentista frente ao paciente.
REFERÊNCIAS1. Andrade ED. Terapêutica medicamentosa em odontologia. 2. ed.
São Paulo: Artes Médicas; 2006. 216p.2. American Dental Association. Guidelines for the use of conscious
sedation, deep sedation and General Anesthesia for Dentists. 2003. Disponível em: http://www.ada.org
3. Dental Health Advisor. Spring, In: Malamed, SF. Sedation: a guide to patient management. 4th ed. St. Louis: Mosby; 2003.
4. Falqueiro JM. Analgesia inalatória por óxido nitroso/oxigênio. 1. ed. São Paulo: Ed. Santos; 2005. 281p.
5. Haas DA. Oral and Inhalation conscious sedation. Dent Clin Nor-th Am. 1999; 73(2): 341.
6. Malamed SF. Managing medical emergencies. J Am Dent Assoc. 1993; 124:(8): 40-53.
7. Malamed SF. Sedation: a guide to patient management. 4th ed. St. Louis: Mosby; 2003.
8. Trieger N, et al. Nitrous oxide a study of physiological and psycho-motor effects. J Am Dent Assoc. 1971 Jan; 82(1):142-50.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 32-35 - 35
TABELAS
Tabela 1 Tabela 2
Tabela 3 Tabela 4
Figura 1 Figura

36 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 36-39
NITROUS OXIDE INHALATION ANALGESIA AT THE ORAL AND MAXILLOFACIAL SURGICAL CLINICS OF THE POLICLÍNICA NAVAL NOSSA SENHORA DA GLÓRIA: ANALYSIS OF 260 CASES
AUTHORS:CF (CD) MARCELO ROSADO BOTELHO, M.D. Bachelor’s Degree in Dentistry from UFF.Qualification in Inhalation Analgesia from PUC-RJ.Master’s Degree in Oral and Maxillofacial Surgery from UNICAMP.Coordinator of the Specialization Program in Oral and Maxillofacial Surgery, from the Brazilian Navy.Chief of the Division of Oral and Maxillofacial Surgery under Ihnalation Analgesia of PNNSG.
CMG (Md-RM1) MARYANGELA FORONI MONTEIRO Bachelor’s Degree in Medicine from the Escola de Ciências Médicas de Volta Redonda.Medical Residency Training in Anesthesiology at UERJ.CAT in Anesthesiology from HNMD.Anesthesiologist at the Ambulatory Surgical Center of PNNSG.
CT (CD) GUILHERME LIMA PONTES Bachelor’s Degree in Dentistry from Universidade Estácio de Sá.Specialization in Oral and Maxillofacial Surgery from the Brazilian Navy.Qualification in Inhalation Analgesia from PUC-RJ.Assistant Dentist at the Inhalation Analgesia Service of PNNSG.
1ºT (CD-RM2) SANNY NORONHA Bachelor’s Degree in Dentistry from UGF.Specialization in Pedodontics from the Universidade Estácio de Sá.Assistant Dentist at the Inhalation Analgesia Service of PNNSG.
1ºT (CD) EMANUELA PRADO FERRAZ Bachelor’s Degree in Dentistry from the Faculdade de Odontologia de Ribeirão Preto - USP.Specialization in Oral and Maxillofacial Surgery from USP-RP.Qualification in Inhalation Sedation from UFRJ.Assistant Dentist at the Inhalation Analgesia Service of PNNSG.
LILIA REGINA PAIVABachelor’s Degree in Nursery from Unirio.Specialization in Medical Surgery Nursing and Occupational Nursing from UGF.Head Nurse at the Ambulatory Surgical Center of PNNSG.
ABSTRACTDespite the advances of science and technology, dental treatment is still associated with pain. Patients show various degrees of anxiety
and they can experience unpleasant reactions, which could make the surgical procedure difficult to perform. Thus, pain and anxiety control is an essential aspect of dental care and the issue needs to be discussed with patients at their first visit to the dentist. There are several control management options available, ranging from non-pharmacological methods to general anesthesia. Over the past years, conscious sedation with nitrous oxide has been widely used due to its effective results, patients’ tolerance and for being an extremely safe technique when compared with other methods of sedation. We present our experience with this technique.
Keywords: conscious sedation; nitrous oxide.
INTRODUCTIONPain, fear and anxiety have always been related to dental
practice, more specifically to surgical procedures, which is usually more invasive and almost always traumatic. A survey conducted with 1,000 adults on some of their most common fears showed that “going
to the dentist” was the second most frequent answer. (Dental Health Advisor, 2003). Thus, anxiety control, which can adversely affect the treatment, is one of dentists’ great challenges.
Psychological aspects exert great influence upon patients’

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 36-39 - 37
clinical condition, including minimizing pain perception. Anxious individuals may show an increase in heart and respiratory rates, as well as in systemic blood pressure, excessive transpiration, dilated pupils, trembling and tingling sensations. Systemic decompensation may occur in patients with cardiovascular, respiratory and endocrine diseases, among others, even if their condition is under control, causing a medical emergency at the dentist’s office, such as angina pectoris, acute myocardial infarction and syncope (Andrade, 2006).
Over a ten-year period, Malamed et al. (1993) conducted a survey that involved more than 4,000 dentists who reported over 30,000 medical emergency situations at their offices. Among the complications surveyed were 15,000 cases of vasopressor syncope and sudden death, 1,300 cases of hyperventilation and about 3,000 cardiovascular complications, all of which are stress related. In the same study, it was also observed that about 55% of medical emergencies occurred during or soon after local anesthesia was administered, a procedure that causes pain and anxiety in patients.
In order to prevent complications and minimize theses situations, surgeon dentists may use, among others, the anxiety-control methods. Scientific literature presents a series of alternatives, ranging from non-pharmacological methods – including soothing words – to pharmacological methods of conscious sedation or general anesthesia.
The American Dental Association (2003) defines conscious sedation as the “minimally depressed level of consciousness that retains the patients’ ability to independently and continuously respond appropriately to physical stimulation or verbal command.”
Among the most used pharmacological methods of conscious sedation in dental care are the oral administration of benzodiazepines and the mixture of oxygen and nitrous oxide, administered via inhalation.
Benzodiazepines activate the receptors of gamma-amino butyric acid (GABA), a central nervous system inhibitory neurotransmitter that helps to open the chloride channels and increase the influx of this anion into the intracellular space. The effect is to reduce the excitatory impulses, thus reducing anxiety. The benzodiazepines also lead to a reduction of salivary flow and vomiting reflex, relax the skeletal musculature and help maintain blood pressure and glycemia at acceptable levels and, in the case of midazolam, cause retrograde amnesia (Andrade, 2006).
Nitrous oxide is an anesthetic colorless and non flammable gas, with a sweet-smelling odor and low solubility in blood; it does not link to blood elements and does not metabolize, thus allowing rapid induction and accurate control of the dose. It is also rapidly eliminated by expiration with minimum depression of the respiratory center and low effect on cerebral cortex. Due to these characteristics, patients often report a relaxing and well-being sensation, somnolence, tingling of the lips and extremities, while maintaining the swallowing and coughing reflexes. Blood pressure, respiratory and heart rates, as well as glycemia are maintained within acceptable levels (Malamed, 2003; Falqueiro, 2005).
The gaseous mixture of oxygen and nitrous oxide has been the most widely used conscious sedation method in Brazil, where it became known thanks to the training courses offered by important
academic institutions. It is a safe method of sedation that can be applied in certain cases at the dental office, being highly effective and well tolerated by the majority of patients.
BACKGROUNDAround 1770, Joseph Priestley identified and isolated nitrous
oxide and oxygen. At the end of the 18th Century, Humphrey Davy, suffering from toothache, inhaled 100 % nitrous oxide, and found that in addition to pain relief the gas produced a pleasant euphoric feeling, an increase in hearing acuity and an uncontrollable urge to laugh. This is the first report on the use of the gas in pain control.
Through the years, many other specialists from other areas have used the gas in different experiments. And then in 1844 Horace Wells – an American dentist – came across an individual who had suffered a contused wound on the leg and was under the effect of the gas. When asked about the level of pain, the individual said he felt none. At this moment, Dr. Wells became fascinated by the possibility of using this gas in dental procedures and went ahead and performed a dental extraction using pure nitrous oxide. He considered the technique a major finding of all times. Unfortunately, Dr. Wells was called a charlatan when, during a public demonstration, the patient became euphoric and agitated. The reaction of the patient led the public to believe that it was a reaction to the pain. It was not until years later that Horace Wells was recognized by the American Dental Association and the American Medical Association, being awarded the title of “pioneer in the use of anesthesia”.
In 1868, Edmund Andrews started using a mixture of 20% oxygen to nitrous oxide, making the procedure much safer for patients. Around 1860, the technique became widely used in dentistry.
Inhalation analgesia with protoxid and oxygen started being administered in Brazil in 1937. The technique of inhalation sedation was finally regulated in compliance with the final report from the Federal Council of Dentistry Forum on the Use of Analgesia in Dentistry, in March, 2004, as set forth in Resolution no. 51/2004, dated May 12, 2004.
TECHNIQUEAnamnesis and physical examination are essential for the
success of this technique. Data obtained from clinical examination can make the analgesia procedure with the mixture of the gases somehow not recommended for patients with these conditions: nasal septum deviation, paranasal sinus pathology (maxillary sinusitis), previous ear drum surgery, pregnant women, bad behaving children, psychiatric and paranoid patients, and those patients who do not tolerate the use of nasal masks. Due to the high rates of oxygen, this procedure should be completely avoided with the following patients: those with chronic obstructive lung disease because they usually have the chemoreceptors responsible for gas exchanges with sensitivity complications. A high concentration of oxygen can be interpreted as a stimulus for reducing ventilation, resulting in hypoxia. This procedure is also not recommended for patients with pneumothorax and those who received chemotherapy and bleomicine for at least a year for they can have pulmonary fibrosis (Haas, 1999). Further laboratory work and X-ray tests will be requested when necessary.

38 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 36-39
The technique involves using some specific equipment, such as the following: fluxmeter, nasal mask, couplings, hoses, cylinders, manometers and valves, reservoir balloon, exhaust system, pulse oxymeter, sphygmomanometer cuff and stethoscope.
Before being submitted to the technique, patients should be submitted to a psychomotor test. The most common one is the test developed by Norman Trieger, called “Trieger test” (Trieger et al., 1971). Next, the mask should be selected and adjusted to the patient’s nose. After that, the patient is administered with 100% oxygen – at 6 L/min in adults and 4 L/min in children – for at least three minutes. The patient should be monitored throughout the procedure and a written record should be made for data recording. Nitrous oxide is administered by adding 10% of it to the mixture for each 10 minutes. The monitoring parameters and the sensations described by the patient should also be recorded. The ideal concentration depends on the patient, but in all cases the limit of 70% of nitrous oxide must be taken into consideration.
Ideal sedation is achieved when the patient begins to report: relaxation, tingling of extremities, feeling warm, numbness of the soft tissues and an increase in hearing acuity. At this stage, patients still show some movement of the limbs and eyes, lacrimation and the “Gioconda smile” on their faces (Falqueiro, 2005).
Although all necessary precautions are taken, there are reports of cases of oversedation, in which patients developed the following signs or symptoms: somnolence, euphoria, indisposition, restlessness and loss of control, laughs, nausea, tinitus and an increase in the respiratory rate. The signs or symptoms will promptly disappear with the reversal of sedation with the administration of 100% oxygen for 10 minutes.
Upon completion of the planning procedure, patients are administered with 100% oxygen for 10 minutes to recover from sedation. Finally, patients are submitted to Trieger test again for checking their motor capacity and only then they can be discharged to go home.
CLINICAL EXPERIENCEThe target public are patients who during anamnesis show some
kind of phobia, fear or anxiety associated with dental treatment, as well as pediatrics patients and those who are ASA II (with mild systemic disease), whose blood pressure, pulse, heart and respiratory rates, and glycemia should be maintained at appropriate levels for the success of the procedure. First, all patients are submitted to strict physical examination and anamnesis and, when necessary, supplementary tests are requested. After the first visit, if the dentist deem necessary to use any sedation technique as part of the treatment, the issue should be discussed with the patient. If another method of sedation or general anesthesia is recommended, the patient should undergo preoperative care and surgical risk for future evaluation of the anesthetist who will perform the procedure. So far, about 260 patients were treated under sedation. Twelve were submitted to oral sedation with benzodiazepines (7.5 mg of
midazolam), 83 to inhalation sedation, 111 to a combined technique of oral anxiolytics and nitrous oxide, 36 to intra-venous sedation and 18 to general anesthesia (Table 1).
The majority of the patients submitted to inhalation analgesia started showing the signs of sedation when administered with 30% nitrous oxide. None of them needed 70% nitrous oxide to achieve the expected sedation (Table 2). In the case of patients submitted to the inhalation sedation technique associated to anxiolytics, a larger number started showing the signs of sedation when administered with 20% nitrous oxide. In addition, these patients needed a less amount of protoxid to maintain the expected levels of sedation during the surgical procedure (Table 3).
The most common symptoms were: tingling of the extremities (lips, fingers and toes), sensation of heaviness in the body, as well as a feeling like being drunk. The most frequent signs were the following: the Gioconda smile (Figure 1), fixed eyes and decreasing of heart rate.
From the 194 patients submitted to inhalation sedation, with or without midazolam, 13 presented some kind of complication related to inhalation analgesia. Five patients did not tolerate the mask and two of them could not use it due to adjusting anatomical reasons. Six patients expressed signs of oversedation: three of them became euphoric and restless; the other three reported nausea. The signs and symptoms of oversedation disappeared some minutes after the administration of 100% oxygen (Table 4). Seven patients reported no signs or symptoms.
This differentiated treatment makes surgical procedure and children’s dental treatment safer. Moreover, it provides benefit, comfort and well-being to the users of the Health System of the Brazilian Navy. The reduction of stress significantly decreases the incidence of medical emergencies in dental practice, improving the relationship between patients and surgeon dentists.
REFERENCES1. Andrade ED. Terapêutica medicamentosa em odontologia. 2. ed.
São Paulo: Artes Médicas; 2006. 216p.2. American Dental Association. Guidelines for the use of conscious
sedation, deep sedation and General Anesthesia for Dentists. 2003. Available at: http://www.ada.org
3. Dental Health Advisor. Spring, In: Malamed, SF. Sedation: a guide to patient management. 4th ed. St. Louis: Mosby; 2003.
4. Falqueiro JM. Analgesia inalatória por óxido nitroso/oxigênio. 1. ed. São Paulo: Ed. Santos; 2005. 281p.
5. Haas DA. Oral and Inhalation conscious sedation. Dent Clin North Am. 1999; 73(2): 341.
6. Malamed SF. Managing medical emergencies. J Am Dent Assoc. 1993; 124:(8): 40-53.
7. Malamed SF. Sedation: a guide to patient management. 4th ed. St. Louis: Mosby; 2003.
8. Trieger N, et al. Nitrous oxide a study of physiological and psychomotor effects. J Am Dent Assoc. 1971 Jan; 82(1):142-50.
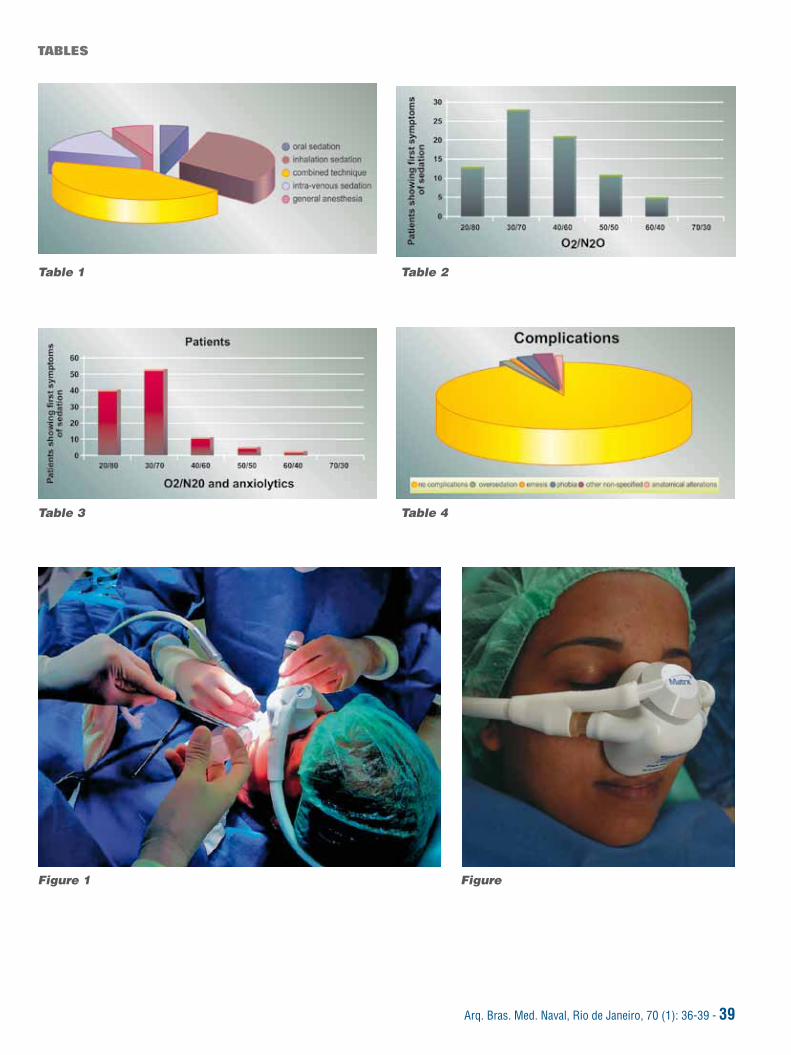
Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 36-39 - 39
Figure 1 Figure
TABLES
Table 1 Table 2
Table 3 Table 4

40 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 40-46
INTRODUÇÃOA promoção do uso racional dos medicamentos tem sido uma das
principais diretrizes preconizadas pela Organização Mundial da Saúde no sentido de orientar as políticas nacionais de medicamentos. Para alcançar esse objetivo, é fundamental a participação ativa e consciente dos profis-sionais responsáveis pela prescrição e dispensação dos medicamentos (médicos, odontólogos e farmacêuticos), além da ampla disseminação jun-to à população de informações corretas para a qual tem importância estra-tégica a participação de todos os profissionais da saúde (Azevedo, 2007).
A conscientização e assistência do profissional farmacêutico re-presentam uma melhoria significativa na atenção ao usuário do me-dicamento, com consequente melhoria na qualidade de vida da po-
AVALIAÇÃO DO TEOR DO PRODUTO DE DEGRADAÇÃO DISSULFETO DE CAPTOPRIL EM COMPRIMIDOS DE CAPTOPRIL 25MG
AUTORES:1ºT (S) ROBSON MARQUES GOUVÊAGraduação em Farmácia Industrial pela UFF.Especialização em Farmácia Industrial pela UFF.Ajudante da Seção de Desenvolvimento do LFM. CC (S) MARCO ANTONIO ARRUDAGraduação em Farmácia Industrial pela UFF.Aperfeiçoamento em Farmácia Industrial pelo LFM.Encarregado da Divisão de Pesquisa do LFM.
CC (S) RUBEN DOS SANTOSGraduação em Farmácia Industrial pela UFF.Aperfeiçoamento em Farmácia Industrial pelo LFM.Mestrado em Ciências pela Fiocruz.Responsável Técnico pelo LFM.
ARMANDO LUCAS CHEREM DA CUNHA. M.D.Graduação em Química Industrial pela UFRJ.Mestrado em Ciências pela UFRJ.Químico do LFM.
RESUMOAtualmente, quando todos os caminhos levam à busca da qualidade total devido à alta competitividade entre as empresas farmacêuticas,
torna-se indispensável conhecer perfeitamente cada fase de um processo de análise final de um produto antes de liberá-lo para o mercado. Por isso a importância das boas práticas de fabricação (BPF) durante a análise dos comprimidos de captopril em relação ao seu produto de degra-dação dissulfeto de captopril.
Deve-se ressaltar também a importância da técnica de análise para evitar que se coloque no mercado um produto com o teor acima ou abaixo do permitido, evitando assim a detecção de uma inconformidade em relação ao produto, com consequente constrangimento do laboratório produ-tor pela retirada do medicamento do mercado devido a uma interdição cautelar promovida pelos órgãos de vigilância sanitária. Os processos de recolhimento são desgastantes para a empresa e comprometem a sua imagem perante o público consumidor.
Ao se fazer uma avaliação do produto de degradação no captopril 25 mg produzido no Laboratório Farmacêutico da Marinha (LFM) e compa-rá-lo com os resultados de dois produtos existentes no mercado, pode-se verificar em que patamar se encontra o LFM, no que tange à qualidade do captopril em relação a tal produto de degradação.
Palavras-chave: captopril; dissulfeto de captopril.
pulação. Essa conscientização é capaz de auxiliar a saúde pública – que, aliás, é o objetivo existencial de todos os profissionais da área da saúde. Estes em ação conjunta, multiprofissional, têm como objeti-vo comum promover a saúde e a vida do ser humano (Azevedo, 2007).
O farmacêutico sempre exerceu, em todos os tempos, como ain-da exerce, uma importantíssima função social, principalmente no Brasil, onde nos velhos tempos, a farmácia foi um centro de irradiação cultural de destacada importância. As farmácias existiram por séculos e a indús-tria como é hoje, não tem mais do que cem anos. Com a implantação da indústria, a manipulação de medicamentos nas farmácias diminuiu, gradualmente (Thomaz, 2001).
O período de mudanças ocorreu, entre as décadas de 40 e 50, de-
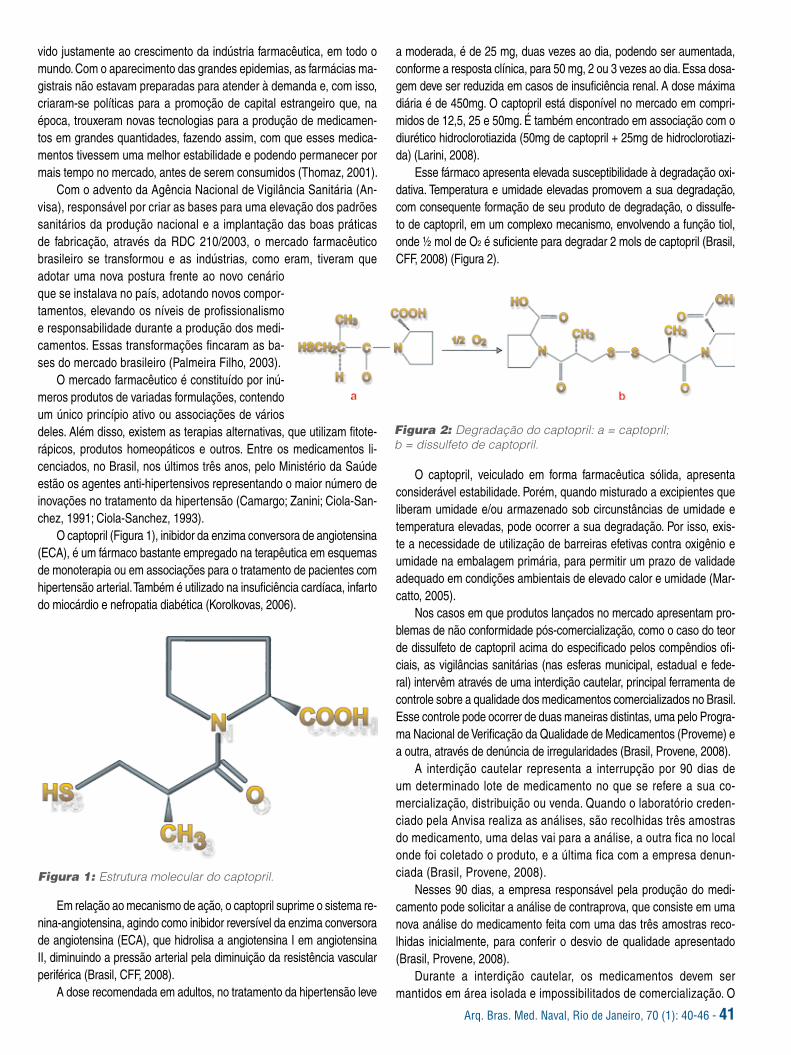
Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 40-46 - 41
vido justamente ao crescimento da indústria farmacêutica, em todo o mundo. Com o aparecimento das grandes epidemias, as farmácias ma-gistrais não estavam preparadas para atender à demanda e, com isso, criaram-se políticas para a promoção de capital estrangeiro que, na época, trouxeram novas tecnologias para a produção de medicamen-tos em grandes quantidades, fazendo assim, com que esses medica-mentos tivessem uma melhor estabilidade e podendo permanecer por mais tempo no mercado, antes de serem consumidos (Thomaz, 2001).
Com o advento da Agência Nacional de Vigilância Sanitária (An-visa), responsável por criar as bases para uma elevação dos padrões sanitários da produção nacional e a implantação das boas práticas de fabricação, através da RDC 210/2003, o mercado farmacêutico brasileiro se transformou e as indústrias, como eram, tiveram que adotar uma nova postura frente ao novo cenário que se instalava no país, adotando novos compor-tamentos, elevando os níveis de profissionalismo e responsabilidade durante a produção dos medi-camentos. Essas transformações fincaram as ba-ses do mercado brasileiro (Palmeira Filho, 2003).
O mercado farmacêutico é constituído por inú-meros produtos de variadas formulações, contendo um único princípio ativo ou associações de vários deles. Além disso, existem as terapias alternativas, que utilizam fitote-rápicos, produtos homeopáticos e outros. Entre os medicamentos li-cenciados, no Brasil, nos últimos três anos, pelo Ministério da Saúde estão os agentes anti-hipertensivos representando o maior número de inovações no tratamento da hipertensão (Camargo; Zanini; Ciola-San-chez, 1991; Ciola-Sanchez, 1993).
O captopril (Figura 1), inibidor da enzima conversora de angiotensina (ECA), é um fármaco bastante empregado na terapêutica em esquemas de monoterapia ou em associações para o tratamento de pacientes com hipertensão arterial. Também é utilizado na insuficiência cardíaca, infarto do miocárdio e nefropatia diabética (Korolkovas, 2006).
a moderada, é de 25 mg, duas vezes ao dia, podendo ser aumentada, conforme a resposta clínica, para 50 mg, 2 ou 3 vezes ao dia. Essa dosa-gem deve ser reduzida em casos de insuficiência renal. A dose máxima diária é de 450mg. O captopril está disponível no mercado em compri-midos de 12,5, 25 e 50mg. É também encontrado em associação com o diurético hidroclorotiazida (50mg de captopril + 25mg de hidroclorotiazi-da) (Larini, 2008).
Esse fármaco apresenta elevada susceptibilidade à degradação oxi-dativa. Temperatura e umidade elevadas promovem a sua degradação, com consequente formação de seu produto de degradação, o dissulfe-to de captopril, em um complexo mecanismo, envolvendo a função tiol, onde ½ mol de O2 é suficiente para degradar 2 mols de captopril (Brasil, CFF, 2008) (Figura 2).
Figura 1: Estrutura molecular do captopril.
Em relação ao mecanismo de ação, o captopril suprime o sistema re-nina-angiotensina, agindo como inibidor reversível da enzima conversora de angiotensina (ECA), que hidrolisa a angiotensina I em angiotensina II, diminuindo a pressão arterial pela diminuição da resistência vascular periférica (Brasil, CFF, 2008).
A dose recomendada em adultos, no tratamento da hipertensão leve
O captopril, veiculado em forma farmacêutica sólida, apresenta considerável estabilidade. Porém, quando misturado a excipientes que liberam umidade e/ou armazenado sob circunstâncias de umidade e temperatura elevadas, pode ocorrer a sua degradação. Por isso, exis-te a necessidade de utilização de barreiras efetivas contra oxigênio e umidade na embalagem primária, para permitir um prazo de validade adequado em condições ambientais de elevado calor e umidade (Mar-catto, 2005).
Nos casos em que produtos lançados no mercado apresentam pro-blemas de não conformidade pós-comercialização, como o caso do teor de dissulfeto de captopril acima do especificado pelos compêndios ofi-ciais, as vigilâncias sanitárias (nas esferas municipal, estadual e fede-ral) intervêm através de uma interdição cautelar, principal ferramenta de controle sobre a qualidade dos medicamentos comercializados no Brasil. Esse controle pode ocorrer de duas maneiras distintas, uma pelo Progra-ma Nacional de Verificação da Qualidade de Medicamentos (Proveme) e a outra, através de denúncia de irregularidades (Brasil, Provene, 2008).
A interdição cautelar representa a interrupção por 90 dias de um determinado lote de medicamento no que se refere a sua co-mercialização, distribuição ou venda. Quando o laboratório creden-ciado pela Anvisa realiza as análises, são recolhidas três amostras do medicamento, uma delas vai para a análise, a outra fica no local onde foi coletado o produto, e a última fica com a empresa denun-ciada (Brasil, Provene, 2008).
Nesses 90 dias, a empresa responsável pela produção do medi-camento pode solicitar a análise de contraprova, que consiste em uma nova análise do medicamento feita com uma das três amostras reco-lhidas inicialmente, para conferir o desvio de qualidade apresentado (Brasil, Provene, 2008).
Durante a interdição cautelar, os medicamentos devem ser mantidos em área isolada e impossibilitados de comercialização. O
Figura 2: Degradação do captopril: a = captopril; b = dissulfeto de captopril.

42 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 40-46
estabelecimento comercial e o próprio consumidor devem aguardar as orientações da vigilância sanitária quanto ao futuro uso do me-dicamento (Brasil, Provene, 2008). A Anvisa faz o lançamento em rede de uma resolução (RE) dissertando acerca da interdição do produto e da empresa.
De acordo com a Figura 3, pode-se verificar o número de inci-dências de interdição cautelar sobre o captopril e a relação com os demais produtos que receberam a mesma notificação entre os anos de 2005 e 2008.
Logo, faz-se necessário o estudo sobre o produto de degradação dissulfeto de captopril, já que este é um fator importante e está dire-tamente relacionado com a qualidade e estabilidade do medicamento produzido, armazenado e comercializado.
Com isso, este estudo pretende determinar e avaliar o teor do produto de degradação do dissulfeto de captopril em comprimidos de captopril 25mg produzidos no Laboratório Farmacêutico da Marinha (LFM) no ano de 2008 e confrontar os resultados obtidos com dois ou mais produtos comumente encontrados no mercado.
METODOLOGIAPara desenvolvimento desse estudo foram coletados, no
LFM, os dados referentes ao período de produção entre janeiro e junho de 2008, que compreendem os lotes 0801003, 0801004, 0801005, 0802014, 0802015 e 0802016. Como houve poucos lo-tes produzidos ao longo desse período, foram utilizados todos os resultados e, por isso, não houve necessidade da utilização de uma técnica de coleta estatística.
No caso dos produtos coletados no mercado, não foi feita nenhu-ma metodologia de escolha de estabelecimento, nem de fornecedor. Isso ocorreu para simular as mesmas condições de um usuário do medicamento e, também, para que o estudo não sofresse influência pela marca ou nome da empresa. Para fins de estudo, não revelare-mos os nomes dos produtos, somente serão intitulados de Laborató-
rio A e Laboratório B.A avaliação da qualidade desses comprimidos de captopril
25mg foi realizada frente a uma pesquisa experimental na qual fo-ram executados os testes físicos de friabilidade, dureza e desinte-gração e os testes físico-químicos de dissolução e teor do princípio ativo e seu produto de degradação, dissulfeto de captopril, confor-me descrito na Farmacopéia Brasileira (2002). Porém, serão so-mente discutidos neste trabalho os resultados do teor do princípio ativo e do produto de degradação, foco principal do estudo.
A metodologia utilizada para a deter-minação do teor do princípio ativo e do produto de degradação foi a cromatogra-fia líquida de alta eficiência (Clae), provi-da de coluna RP – 18, com diâmetro in-terno de 4,6mm e 25cm de comprimento, com carga de hidrocarboneto de aproxi-madamente 15% e 5 µm de tamanho de partícula (Merck). A fase móvel foi obtida de uma mistura filtrada e desaerada de 550ml de metanol Clae, 450ml de água e 0,50ml de ácido fosfórico.
Utilizou-se soluções de padrões de captopril United States Pharmacopeia (2005) e de dissulfeto de captopril (USP), nas concentrações de 1,0mg/ml e 0,03mg/ml (3%), respectivamente. Esses padrões foram dissolvidos com a fase móvel.
As amostras foram preparadas em duplicatas, onde foram pulverizados cerca de 20 comprimidos, pesando-se o equivalente a cerca de 2 pesos
médios (aproximadamente 50mg de captopril). Essa massa foi transferida, quantitativamente, para balão volumétrico de 50ml, diluída com a fase móvel e sonicada por 15 minutos. As amos-tras foram filtradas através de membranas de 0,45µm.
Injetou-se, separadamente, cerca de 20µl da solução padrão e da solução de amostra no aparelho, sendo cinco injeções para o padrão e duas injeções de cada amostra. Registraram-se os croma-togramas e as áreas dos picos foram medidas. Os valores obtidos foram transportados para uma planilha Excel e os resultados para o teor de Captopril e dissulfeto de captopril, nos comprimidos, fo-ram calculados a partir das respostas obtidas com as soluções do padrão e da amostra.
A Farmacopéia Brasileira (2002), estabelece como especifica-ções um teor de captopril entre 90% a 110% da quantidade declarada (25mg/comprimido) e limite máximo de 3,0% do produto de degrada-ção dissulfeto de captopril.
RESULTADOS E DISCUSSÃOConsideração inicial
A atenção deste estudo concentra-se nos parâmetros de teor do ativo e no teor do produto de degradação. Logo, cabe ressaltar que os outros parâmetros (dissolução, dureza, umidade, desinte-gração etc.) encontram-se dentro dos valores permitidos, conforme as Tabelas 1 e 2.
Figura 3: Comparação entre o número de interdições cautelares do captopril por ano com outros produtos.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 40-46 - 43
Tabela 1: Resultados obtidos dos lotes do LFM frente aos testes aplicados
TESTE ESPECIFICAÇÃORESULTADOS
0801003 0801004 0801005 0802014 0802015 0802016
Aspecto Passa no teste Passa no teste Passa no teste Passa no teste Passa no teste Passa no teste Passa no teste
Identificaçãofármaco: captopril
CLAE: de acordocom o padrão
Corresp. Corresp. Corresp. Corresp. Corresp. Corresp
Peso médio (mg) 125,0 ± 7,5% (115,6 a 134,3)
124,0 124,1 128,4 124,6 126,9 126,1
Dureza Mínimo 4,0 Kp Corresp. Corresp. Corresp. Corresp. Corresp. Corresp.
Desintegração Máximo 30minutos (H2O 37ºC)
Corresp. Corresp. Corresp. Corresp. Corresp. Corresp.
FriabilidadeMáximo 1,5% em 5 minutos
Corresp. Corresp. Corresp. Corresp. Corresp. Corresp.
Água Máximo 7,0 (KF) (informativo)
6,8% 6,8% 6,2% 5,7% 6,6% 6,8%
DissoluçãoMínimo 80% m 20 minutos
100,0% 105,8% 102,3% 102,8% 103,4% 104,9%
Limite de dissulfeto de captopril Máximo 3,0% 0,3% 0,2% 0,8% 1,7% 1,6% 1,5%
Uniformidade dedoses unitárias
85,0% a 115,0% (variação de peso)
90,9% a103,6%
92,6% a102,1%
88,7% a98,1%
97,4% a102,2%
96,6% a 102,9%
93,8% a99,8%
Doseamento90,0% a 110,0% do valor declarado
96,9% 97,4% 94,6% 99,7% 100,1% 97,6%
22,5 a 27,5mg/com 24,2 mg/com 24,4mg/com 23,7mg/com 24,9mg/com 25,0 mg/com 24,4mg/com
TESTE ESPECIFICAÇÃORESULTADO
Lab. A Lab. B
Aspecto Passa no teste Passa no teste Passa no teste
Identificação fármaco: captopril HPLC: de acordo com o padrão Corresponde Corresponde
Peso médio 100,0mg ± 7,5% (92,5 a 107,5mg) 102,3mg 101,5mg
Dureza Mínimo 4,0 Kp Corresponde Corresponde
Desintegração Máximo 30 minutos (H20 37ºC) - -
Friabilidade Máximo 1,5% em 5 minutos Corresponde Corresponde
Água Máximo 7,0% (KF) (Informativo) 6,3% 6,2%
Dissolução Mínimo 80% em 20 minutos - -
Limite de dissulfeto de captopril Máximo 3,0% 2,89% 0,32%
Uniformidade de doses unitárias 85,0% a 115,0% (variação de peso) 95,0 a 98,6% 97,3 a 99,9%
Doseamento90,0% a 110,0% do valor declarado 97,2% 98,8%
22,5 - 27,5mg/com 24,3mg/com 24,7mg/com
Fonte: Divisão de Controle da Qualidade, LFM, 2008.
Tabela 2: Resultados obtidos dos Laboratório A e B frente aos testes aplicados
Fonte: Divisão de Controle da Qualidade, LFM, 2008.
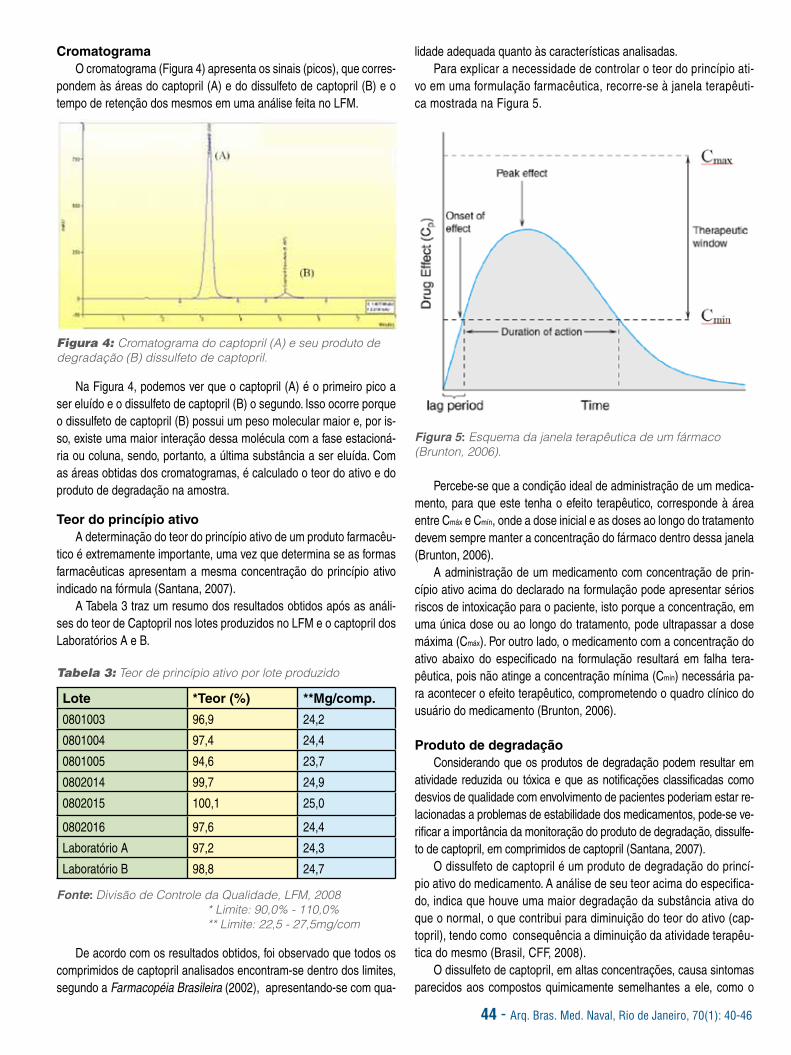
44 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 40-46
CromatogramaO cromatograma (Figura 4) apresenta os sinais (picos), que corres-
pondem às áreas do captopril (A) e do dissulfeto de captopril (B) e o tempo de retenção dos mesmos em uma análise feita no LFM.
Figura 4: Cromatograma do captopril (A) e seu produto de degradação (B) dissulfeto de captopril.
Na Figura 4, podemos ver que o captopril (A) é o primeiro pico a ser eluído e o dissulfeto de captopril (B) o segundo. Isso ocorre porque o dissulfeto de captopril (B) possui um peso molecular maior e, por is-so, existe uma maior interação dessa molécula com a fase estacioná-ria ou coluna, sendo, portanto, a última substância a ser eluída. Com as áreas obtidas dos cromatogramas, é calculado o teor do ativo e do produto de degradação na amostra.
Teor do princípio ativoA determinação do teor do princípio ativo de um produto farmacêu-
tico é extremamente importante, uma vez que determina se as formas farmacêuticas apresentam a mesma concentração do princípio ativo indicado na fórmula (Santana, 2007).
A Tabela 3 traz um resumo dos resultados obtidos após as análi-ses do teor de Captopril nos lotes produzidos no LFM e o captopril dos Laboratórios A e B.
Tabela 3: Teor de princípio ativo por lote produzido
Lote *Teor (%) **Mg/comp.
0801003 96,9 24,2
0801004 97,4 24,4
0801005 94,6 23,7
0802014 99,7 24,9
0802015 100,1 25,0
0802016 97,6 24,4
Laboratório A 97,2 24,3
Laboratório B 98,8 24,7
Fonte: Divisão de Controle da Qualidade, LFM, 2008* Limite: 90,0% - 110,0% ** Limite: 22,5 - 27,5mg/com
De acordo com os resultados obtidos, foi observado que todos os comprimidos de captopril analisados encontram-se dentro dos limites, segundo a Farmacopéia Brasileira (2002), apresentando-se com qua-
lidade adequada quanto às características analisadas.Para explicar a necessidade de controlar o teor do princípio ati-
vo em uma formulação farmacêutica, recorre-se à janela terapêuti-ca mostrada na Figura 5.
Figura 5: Esquema da janela terapêutica de um fármaco (Brunton, 2006).
Percebe-se que a condição ideal de administração de um medica-mento, para que este tenha o efeito terapêutico, corresponde à área entre Cmáx e Cmín, onde a dose inicial e as doses ao longo do tratamento devem sempre manter a concentração do fármaco dentro dessa janela (Brunton, 2006).
A administração de um medicamento com concentração de prin-cípio ativo acima do declarado na formulação pode apresentar sérios riscos de intoxicação para o paciente, isto porque a concentração, em uma única dose ou ao longo do tratamento, pode ultrapassar a dose máxima (Cmáx). Por outro lado, o medicamento com a concentração do ativo abaixo do especificado na formulação resultará em falha tera-pêutica, pois não atinge a concentração mínima (Cmín) necessária pa-ra acontecer o efeito terapêutico, comprometendo o quadro clínico do usuário do medicamento (Brunton, 2006).
Produto de degradaçãoConsiderando que os produtos de degradação podem resultar em
atividade reduzida ou tóxica e que as notificações classificadas como desvios de qualidade com envolvimento de pacientes poderiam estar re-lacionadas a problemas de estabilidade dos medicamentos, pode-se ve-rificar a importância da monitoração do produto de degradação, dissulfe-to de captopril, em comprimidos de captopril (Santana, 2007).
O dissulfeto de captopril é um produto de degradação do princí-pio ativo do medicamento. A análise de seu teor acima do especifica-do, indica que houve uma maior degradação da substância ativa do que o normal, o que contribui para diminuição do teor do ativo (cap-topril), tendo como consequência a diminuição da atividade terapêu-tica do mesmo (Brasil, CFF, 2008).
O dissulfeto de captopril, em altas concentrações, causa sintomas parecidos aos compostos quimicamente semelhantes a ele, como o

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 40-46 - 45
dissulfeto de carbono, sendo os sintomas mais comuns: náuseas, ton-turas e mal-estar. Por causa disso, deve-se fazer o controle desse com-posto nos comprimidos de captopril (Brasil, CFF, 2008).
A Tabela 4 mostra os resultados obtidos durante o período de acompanhamento dos lotes produzidos no LFM, Laboratório A e Laboratório B.
Tabela 4: Teor de dissulfeto de captopril
Lote *Dissulfeto (%)
0801003 0,3
0801004 0,2
0801005 0,8
0802014 1,7
0802015 1,6
0802016 1,5
Laboratório A 2,89
Laboratório B 0,32
Fonte: Divisão de Controle da Qualidade, LFM, 2008* Limite: 3,0%
De acordo com os lotes analisados, pode-se verificar que ne-nhum deles ultrapassou o valor máximo especificado (3,0%), Farma-copéia Brasileira (2002). Vale destacar que entre os lotes produzidos no LFM, o lote 0801004 apresentou o menor resultado, 0,2%, e o lote 08020014 apresentou o maior valor entre todos, 1,7%. Em uma aná-lise geral, o Laboratório A foi o que apresentou o maior valor entre todos, chegando a um nível crítico de valor, 2,89%. Esse fato pode ser visto melhor na Figura 6.
Figura 6: Resultados do teor de dissulfeto de captopril nos lotes do LFM, Laboratório A e Laboratório B.
A prática corrente, quando encontra-se um resultado elevado ou fora de especificação, preconiza o procedimento de rever toda a técni-ca empregada na análise. Porém, como as análises foram realizadas ao mesmo tempo para todos os lotes, pode-se inferir que o resultado é o correto.
De acordo com a Figura 6, verificou-se que os lotes 0802014, 08020015 e 08020016 apresentam um valor de dissulfeto em torno da metade do valor máximo permitido. Nesses casos, é aconselhável que o laboratório produtor faça um estudo de acompanhamento mais detalhado para esses lotes, em relação ao de controle do dissulfeto, ao longo do prazo de validade desses lotes, a fim de evitar possíveis transtornos, conforme preconizado na Resolução RE nº 01, de 29 de julho de 2005, (Brasil, Anvisa, 2005).
Ao se fazer um levantamento sobre esses três lotes, verificou-se que foram colocados em estudos de estabilidade, pois eles en-contravam-se em processo de validação, apesar de a legislação preconizar somente a necessidade de análise para um desses lo-tes, já que a produção anual do captopril 25mg do LFM, gira em torno de mais de 15 lotes/ano (Brasil, Anvisa, 2005).
CONCLUSÃODe acordo com os resultados obtidos, conclui-se que o produto
captopril produzido no LFM, apresentou os resultados dentro dos pa-drões de qualidade exigidos pela Farmacopéia Brasileira.
Ao se fazer uma avaliação do produto de degradação no captopril 25mg produzido no LFM e compará-lo com os resultados de dois pro-dutos existentes no mercado, verificou-se que o LFM encontra-se no mesmo patamar de qualidade que os lotes dos produtos comercializa-dos no mercado, no que tange à qualidade do captopril em relação a tal produto de degradação.
Durante o estudo constatou-se que é extremamente importante fa-zer o controle da matéria-prima, desde a aquisição, armazenagem até sua utilização, com relação ao teor de dissulfeto de captopril, a fim de se evitar possíveis transtornos durante o prazo de validade do produto. Tendo como exemplo o Laboratório A, que apresentou um valor de pro-duto de degradação muito próximo do limite máximo permitido. Assim, estima-se a possibilidade de futuros problemas, pois o seu prazo de validade ainda perdurará por mais um ano.
A análise dos estudos de acompanhamento dos lotes produzidos no LFM é de extrema importância para as boas práticas de fabrica-ção, pois assegura uma análise da qualidade dos produtos desde a sua produção até o término do prazo de validade, podendo-se tomar medidas de precaução, caso seja necessário, se o produto apresentar algum desvio de qualidade durante estes estudos.
A avaliação da qualidade de produtos farmacêuticos, disponíveis no mercado, é uma iniciativa importante, principalmente para as ações dos órgãos de vigilância sanitária na ocorrência de suspeita ou denún-cia de medicamentos adulterados, falsificados, com falha terapêutica e com alterações no aspecto e nas propriedades físico-químicas.
AGRADECIMENTOSÀ Escola de Saúde, ao diretor do LFM, ao responsável técnico (RT)
pela orientação, à Divisão de Controle da Qualidade, à Divisão de Pes-quisa e a todos do LFM pela ajuda e colaboração para o desenvolvi-mento deste trabalho.
REFERÊNCIAS1. Azevedo RCP. Estudo da liberação in vitro de Captopril cápsulas
magistrais por Cromatografia Líquida de Alta Eficiência. 2007. Disser-tação (Mestrado em Ciências Farmacêuticas) – Universidade Federal de Alfenas, Minas Gerais.
2. Brasil. Agência Nacional de Vigilância Sanitária. Proveme. Brasí-lia. [Acesso em: 19 jun. 2008]. Disponível em: <http:// www.anvisa.gov.br/Inspeção/ Fiscalização>
3. Brasil. Agência Nacional de Vigilância Sanitária. Resolução RDC 210 de 04 de agosto de 2003. Regulamento técnico das boas práticas para a fabricação de medicamentos. Diário da República Federativa do Brasil. Brasília: 2003.

46 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 40-46
4. Brasil. Agência Nacional de Vigilância Sanitária. Resolução RE nº 1 de 29 de julho de 2005. Guia para a realização de estudos de estabilidade. Diário da República Federativa do Brasil. Brasília; 2005.
5. Brunton LL, Lazo JS, Parker KL. In: Goodman, Gilman. As ba-ses farmacológicas da terapêutica. 11. ed. Rio de Janeiro: McGra-wHill ; 2006. p.17.
6. Camargo EA, Zanini AC, Ciola-Sanchez L. Avaliação qualitativa no uso de medicamentos. Semina. 1991; 2(2):70-83.
7. Ciola-Sanchez L. Consumo, custos e utilidade clínica: a avalia-ção do uso de medicamentos na região de Emília Romagna. Rev Bras Med. 1993;50(4):297-313.
8. Farmacopéia Brasileira. 4. ed. São Paulo: Atheneu; 2002. pt. 2, p. 181.
9. Larini L. Fármacos e Medicamentos. Porto Alegre: Artmed, 2008. p.167-168.
10. Marcatto AP., et al. Análise de cápsulas de Captopril manipu-ladas em farmácias. Rev Ci Farm Basic e Aplic. 2005;26(3): 221-25.
11. Palmeira Filho PL, Pan SSK. Cadeia farmacêutica no Brasil: avaliação preliminar e perspectivas. BNDES Setorial. 2003;18:3-22.
12. Santana G., et al. Avaliação da qualidade do AAS 100mg frente ao teor do produto de degradação ácido salicílico. Rev Control. Conta-minação. 2007; 9(99):33-8.
13. Thomaz S. Manipulação magistral no Brasil: cinco séculos de futuro. Intern. J Pharm Comp. 2001; 3(1):10-16.
14. US Pharmacopeia National Formulary. 29. ed . lWebcom Limi-ted; 2005. p. 366-7.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53 - 47
ASSESSMENT STUDY OF THE DEGRADATION PRODUCT CAPTOPRIL DISULFIDE IN 25MG CAPTOPRIL TABLETS
AUTHORS:1ºT (S) ROBSON MARQUES GOUVÊABachelor’s Degree in Industrial Pharmacy from UFF.Specialization in Industrial Pharmacy from UFF.Assistant at the Development Division of LFM. CC (S) MARCO ANTONIO ARRUDABachelor’s Degree in Industrial Pharmacy from UFF.Extended Training in Industrial Pharmacy at LFM.Chief of the Research Division at LFM.
CC (S) RUBEN DOS SANTOSBachelor’s Degree in Industrial Pharmacy from UFF.Extended Training in Industrial Pharmacy at LFM.Master’s Degree in Sciences from Fiocruz.Technician Responsible for LFM.
ARMANDO LUCAS CHEREM DA CUNHA, M.D.Bachelor’s Degree in Chemistry from UFRJ.Master’s Degree in Sciences from UFRJ.Chemist of LFM.
ABSTRACTThe highly competitive pharmaceutical industry calls for a widespread pursuit for total quality assurance. Therefore, sound and detailed
knowledge of each phase of a product’s final assessment procedure has become essential before a given product is launched into the market. Good Production Practices (GPPs) are key for the assessment of captopril tablets and its degradation product, captopril disulfide.
The technique employed in this type of assessment is equally important to verify compliance with the quantitative determination of the active principle, thus preventing the public embarrassment of a pharmaceutical laboratory if a product’s active principle is found to be at a higher or lower concentration level than that established by sanitary surveillance officials. Such situation would lead to the product being withdrawn from the market by means of an interim interdict issued by sanitary officials. Product withdrawal processes can wear out a company’s image and damage consumer relations.
Assessing the degradation product of the 25mg captopril tablets produced by the Pharmaceutical Laboratory of the Brazilian Navy (Laboratório Farmacêutico da Marinha - LFM) and comparing findings against the existing results for two similar products available in the market will allow for the assessment of the LFM’s current Quality Control processes.
Keywords: captopril; captopril disulfide.
INTRODUCTIONPromoting rational drug use has been one of the World Health
Organization (WHO) major directives regarding the design of national drug policies. In order to reach this aim, the active and conscientious efforts of all those responsible for drug prescription and dispensing (physicians, dentists and pharmacists) is just as important and strategic as is clear public communication of accurate information about drugs (Azevedo, 2007).
Providing pharmacists with knowledge and guidance brings about significantly improved levels of assistance that these professionals can supply to drug users, thus leading to subsequent increase in the population’s life quality conditions. Such chain of awareness is
able to raise public healthcare standards – the ultimate objective of all healthcare professionals. This chain of integrated and multi-professional actions aims to eventually promote man’s healthy life (Azevedo, 2007).
Throughout man’s history, pharmacists have played a major social function, especially in Brazil, where in old times pharmacies constituted highly important centers of culture dissemination. The so-called small-scale “manipulation pharmacies” have been operating for centuries, while the pharmaceutical industry as it is known today is barely over a hundred years old. Industrialized, large-scale drug manipulation, however, has gradually but consistently reduced small-scale drug manipulation (Thomaz, 2001).

48 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53
Regarding its mechanism of action, captopril suppresses the renin-angiotensin system (RAS), acting as a reversible inhibitor of the angiotensin converting enzyme (ACE), which hydrolyzes the angiotensin I in the angiotensin II, thus lowering the arterial pressure by decreasing peripheral vascular resistance (Brazil, CFF, 2008).
The recommended adult dosage for mild hypertension is 25 mg twice a day, which may be increased to 50mg twice or three times a day depending on the patient’s response. This dosage should be reduced in cases of renal insufficiency. The maximum daily dosage is 450mg. Captopril is available in 12.5, 25 and 50mg tablets and can also be found in association with the diuretic hydrochlorothiazide (50mg captopril + 25mg hydrochlorothiazide) (Larini, 2008).
This pharmaceutical product is highly susceptible to oxidative degradation. High temperatures and humidity levels lead to its degradation product, captopril disulfide, by means of a complex mechanism that involves the thiol function where ½mol O2 is enough to degrade 2 mols of captopril (Brazil, CFF,
2008) (Figure 2).
Figure 2: Degradation of captopril: a = captopril; b = captopril disulfide.
Captopril is highly stable as a solid pharmaceutical product. Nevertheless, when mixed to a high humidity excipient and/or stored under high temperature and humidity conditions, captopril can undergo degradation. That explains the need for effective anti-oxygen and humidity contact packaging solutions, so that the product validity time is preserved even under high heat and humidity environmental conditions (Marcatto, 2005).
Non-conformity problems identified at the post-sales phase of product marketing, like higher captopril disulfide content than that established by official directives, call for the intervention of the sanitary surveillance officials (at municipal, state and federal levels) by means of an interim interdict, their major control tool for pharmaceutical drugs traded in Brazil. Such intervention may unfold through either one of two distinct paths: through the National Drug Quality Control Program (Programa Nacional de Verificação da Qualidade de Medicamentos - Proveme) or through a non-compliance indictment (Brazil, Provene, 2008).
The interim interdict stands for a 90-day interruption of a product supply, distribution or sale. When the laboratory accredited with Anvisa conducts the assessment analyses, three samples of the drug are collected: one undergoes the analyses, the second one is kept where the product was collected, and the third one remains with the pharmaceutical laboratory being indicted (Brazil, Provene, 2008).
The winds of change blew hard in the 1940s and 50s with the worldwide expansion of the pharmaceutical industry. Local small-scale “manipulation pharmacies” were not able to cater for the demand for drugs to fight the outbreak of epidemics and the Brazilian government passed policies to attract foreign capital and expertise. Foreign laboratories settled in and introduced new technologies for large-scale production of higher quality and longer validity time drugs (Thomaz, 2001).
The Brazilian National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária –Anvisa) was established in 1999 and became responsible for developing a baseline framework that aimed at raising national production sanitary standards and at implementing Good Production Practices (GPPs). Its Resolution Act RDC no. 210/2003 revolutionized the Brazilian pharmaceutical industry and pharmaceutical corporations had to develop a new stance face to the new industry scenario, which meant adopting new procedures, raising professional standards and implementing responsible drug production. All these changes shaped a new Brazilian pharmaceutical market (Palmeira Filho, 2003).
The pharmaceutical market comprises a number of products of various formulations which share one single active principle or associat ions of var ious pr inciples. There are also alternative therapies that use phytotherapic and homeopathic products, among others. In the past three years, the Brazilian Ministry of Health has licensed a number of drugs, especially a large number of innovative anti-hypertension products (Camargo; Zanini; Ciola-Sanchez, 1991; Ciola-Sanchez, 1993).
Captopril (Figure 1), an angiotensin converting enzyme (ACE) inhibitor, is widely used in monotherapy schemes or in association with other drugs to control arterial blood pressure. It is also prescribed for cardiac insufficiency, strokes and diabetic nephropathy (Korolkovas, 2006).
Figure 1: Captopril’s molecular structure

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53 - 49
Within these 90 days, the company responsible for the production of the drug may request a counterproof analysis, which consists of a new analysis of the drug conducted with one of the three samples initially collected to verify quality non-compliance conditions (Brazil, Provene, 2008).
Throughout the interim interdict, the drugs must be kept in an isolated place and cannot be traded. The trading businesses (wholesalers and retailers) and the drug consumer must await the assessment of the sanitary surveillance officials regarding the future destination of the product (Brazil, Provene, 2008). Anvisa will issue a network communication through a Resolution Act (RE, in Brazilian Portuguese) discussing the interim interdict of the product and of the pharmaceutical company.
Figure 3 shows the number of captopril interim interdicts and how they compare against other products that have been granted the same type of interdict between 2005 and 2008.
Figure 3: Contrast between the number of captopril interim interdicts against other products – per year.
That explains the need for a degradation product (captopril disulfide) assessment study, once this is a key factor that is directly related to the quality and stability of the produced, stored and traded product.
This study, therefore, aims to assess the degradation product (captopril disulfide) content in 25mg captopril tablets produced by the Pharmaceutical Laboratory of the Brazilian Navy (LFM) in the year 2008 and contrast its findings with two or more similar products available in the pharmaceutical market.
METHODOLOGYIn order to develop this assessment study, the LFM collected
the data that referred to the production process between January and June 2008, that is, batches no. 0801003, 0801004, 0801005, 0802014, 0802015 and 0802016. As few batches were produced within this period of time, all the findings were assessed and therefore, a statistical data collection method was not necessary.
Regarding the sample products collected in the market, the
trading businesses and the product suppliers were selected randomly in order to simulate the same conditions of a product user and also to prevent any influence regarding the product or pharmaceutical laboratory brand name. In order to safeguard anonymity, this study will not reveal the product names; they will be referred to as Laboratory A and Laboratory B.
The quality assessment of 25mg captopril tablets was conducted by an experimental research that comprised friability, hardness and disintegration physical tests, as well as dissolution and active principle and degradation product (captopril disulfide) content physical-chemical tests, as described in Farmacopéia Brasileira (2002). However, this study will only discuss the findings for active principle and degradation product content, the main object of this study.
The methodology used for determining the active principle and degradation product content was high-performance liquid
chromatography (HPLC), on RP – 18 column, with an internal 4.6mm diameter and 25cm in length, wherein an approximate carbon charge of 15% and 5 µm particle size (Merck) was used. The mobile phase was obtained from a filtered and de-aired mixture of 550ml methanol (HPLC grade), 450ml water and 0.5ml phosphoric acid.
Captopril United States Pharmacopeia (2005) and captopril disulfide (USP) standard solutions were used at 1.0mg/ml and 0.03mg/ml (3%) concentrations, respectively. These solutions were dissolved in the mobile phase.
The samples were prepared in duplicates where about 20 tablets weighing the equivalent to two average weights (approximately 50mg captopril) were pulverized. This mass was
then quantitatively transferred to a 50mg volumetric balloon, diluted in the mobile phase and sonicated for 15 minutes. The samples were then filtered through 0.45µm membranes.
Approximately 20µl of the standard solution and of the sample solution were then injected into the equipment separately - five injections of the standard solution and two injections of each sample solution. Chromatograms were recorded and the peak areas were measured. The values were entered into an Excel spreadsheet and the results for captopril and captopril disulfide content in the tablets were calculated based on the responses of the standard and sample solutions.
The Farmacopéia Brasileira (2002), establishes a captopril content between 90% and 110% of the stated value (25mg/tablet) and a top limit of 3.0% of the degradation product – captopril disulfide.
DISCUSSION
Preliminary Considerations
This study is centered on the parameters for active principle and degradation product content. It is worth noting that other parameters (dissolution, hardness, humidity, disintegration, etc.) were found to be within the established values, as shown in Tables 1 and 2.

50 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53
Table 1: Findings of the tests conducted with LFM batches
Source: Quality Control Division, LFM, 2008.
Table 2: Findings of tests conducted by Laboratory A and B
TEST TYPE SPECIFICATIONFINDINGS
Lab. A Lab. B
Aspect Passes the test Passed Passed
Pharmaceutical identification: captopril HPLC: compliance with standard Complied Complied
Average weight (mg) 100.0 mg ± 7.5% (92.5 a 107.5 mg) 102.3 mg 101.5 mg
Hardness Minimum 4.0 Kp Complied Compplied
Disintegration Maximum 30 mins (H20 37ºC) - -
Friability Maximum 1.5% in 5 mins Complied Complied
Water Maximum 7.0% (KF) (Informative standard) 6.3% 6.2%
Dissolution Minimum 80% in 20 mins - -
Captopril disulfide limit Maximum 3.0% 2.89% 0.32%
Uniformity of unitary dosage 85.0% to 115.0% (weight variation) 95.0 to 98.6% 97.3 to 99.9%
Dosage90.0% to 110.0% of stated value 97.2% 98.8%
22.5 - 27.5mg/tablet 24.3mg/tablet 24.7mg/tablet
Source: Quality Control Division, LFM, 2008.
TEST TYPE SPECIFICATIONFINDINGS
0801003 0801004 0801005 0802014 0802015 0802016
Aspect Passes the test Passed Passed Passed Passed Passed Passed
Pharmaceutical identification: captopril HPLC: compliance with standard Complied Complied Complied Complied Complied Complied
Average weight (mg) 125.0 ± 7.5% (115.6 to 134.3) 124.0 124.1 128.4 124.6 126.9 126.1
Hardness Minimum 4.0 Kp Complied Complied Complied Complied Complied Complied
Disintegration Maximum 30 mins
(H2O 37ºC) Complied Complied Complied Complied Complied Complied
Friability Maximum 1.5% in
5 mins Complied Complied Complied Complied Complied Complied
Water Maximum 7.0 (KF)(informative standard)
6.8% 6.8% 6.2% 5.7% 6.6% 6.8%
Dissolution Minimum 80% in 20 Mins 100.0% 105.8% 102.3% 102.8% 103.4% 104.9%
Captopril disulfide limit Maximum 3.0% 0.3% 0.2% 0.8% 1.7% 1.6% 1.5%
Uniformity of unitary dosage 85.0% to 115.0%(weight variation)
90.9% a 103.6%
92.6% a 102.1%
88.7% a 98.1%
97.4% a 102.2%
96.6% a 102.9%
93.8% a 99.8%
Dosage
90.0% to 110.0% of stated value 96.9% 97.4% 94.6% 99.7% 100.1% 97.6%
22.5 to 27.5 mg/com 24.2mg/com
24.4mg/com
23.7mg/com
24.9mg/com
25.0mg/com
24.4mg/com

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53 - 51
ChromatogramChromatogram (Figure 4) shows the signs (peaks) that correspond
to captopril (A) areas and captopril disulfide (B) areas, as well as their respective retention times as per an analysis conducted at LFM.
Figure 4: Chromatogram for captopril (A) and its degradation product (B) –captopril disulfide.
Figure 4 shows that captopril (A) is the first eluted peak, followed by captopril disulfide (B). This occurs because captopril disulfide (B) has greater molecular weight and therefore, this molecule interacts more with the stationary or column phase and is the last substance to be eluated. Active principle content and the degradation product content of the sample can be calculated based on the areas obtained from the chromatograms.
Active principle contentThe quantitative determination of the active principle of a
pharmaceutical product is of utmost importance, once this subsequently determines the pharmaceutical applications of the same active principle concentration as discussed in the product formula (Santana, 2007).
Table 3 summarizes the findings of captopril quantitative determination analyses conducted in the batches produced by LFM and by Laboratories A and B.
Table 3: Active principle determination per batch produced
Batch *Content (%) **Mg/tablet
0801003 96.9 24.2
0801004 97.4 24.4
0801005 94.6 23.7
0802014 99.7 24.9
0802015 100.1 25.0
0802016 97.6 24.4
Laboratory A 97.2 24.3
Laboratory B 98.8 24.7
Source: Quality Control Division, LFM, 2008.* Limit value: 90.0% - 110.0% ** Limit value: 22.5 – 27.5 mg/com
The findings show that all the captopril tablets that were analyzed were found to be within the limit values established by Farmacopéia Brasileira (2002), and there was quality compliance with all the assessed product features.
Figure 5 shows the therapeutic window used to justify the need of quantitative determination of active principle in a pharmaceutical product.
Figure 5: Therapeutic window of a pharmaceutical product (Brunton, 2006).
This figure makes it clear that the ideal drug dispensing conditions – to foster the aimed therapeutic effect – corresponds to the area comprised by Cmax and Cmin, wherein the initial dosage and the subsequent doses throughout the prescribed treatment must always keep the drug concentration range within this window (Brunton, 2006).
Dispensing a drug whose active principle concentration level is above the ones discussed and recommended in the drug formula may pose intoxication risks to the patient, as the concentration dispensed either through a single dosage or throughout the treatment may go beyond the maximum recommended dosage (Cmax). On the other hand, dispensing lower active principle concentration levels will lead to therapeutic failure, as the minimum recommended concentration (Cmin) may not yield the aimed response, thus causing adverse impacts upon the user’s clinical conditions (Brunton, 2006).
Degradation productThe fact that degradation products may result in reduced or toxic
drug effects and that the notifications defined as quality non-compliance may be related to drug stability problems evidences the importance of assessing and monitoring the degradation product, captopril disulfide, in captopril tablets (Santana, 2007).
Captopril disulfide is a degradation product of the active principle of captopril. Higher active principle content than that desired shows that there was a higher than usual degradation of the drug’s active principle. This contributes to reduced active principle content (captopril), which in turn leads to a lesser therapeutic effect of such principle (Brazil, CFF, 2008).
Higher captopril disulfide concentration has similar symptoms to those of chemically similar compounds, like carbon disulfide. The most common symptoms are nausea, dizziness and distress. That is why this compound must be assessed in captopril tablets (Brazil, CFF, 2008).
Table 4 shows the findings of the assessment of the batches produced by LFM, Laboratory A and Laboratory B.

52 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53
Table 4: Captopril disulfide content
Batch *Disulfide (%)
0801003 0.3
0801004 0.2
0801005 0.8
0802014 1.7
0802015 1.6
0802016 1.5
Laboratory A 2.89
Laboratory B 0.32
Source: Quality Control Division, LFM, 2008.* Limit value: 3.0%
None of the assessed batches was beyond the maximum limit value (3.0%), Farmacopéia Brasileira (2002). It is worth noting that among the batches produced by LFM, batch no. 0801004 showed the lowest percentage of disulfide – 0.2%, and batch no. 08020014 the highest – 1.7%. Overall, Laboratory A showed the highest percentage of all and reached the critical limit level – 2.89%. These findings are more clearly expressed in Figure 6.
Figure 6 : Findings of captopril disulfide content in the batches produced by LFM, Laboratory A and Laboratory B.
Whenever higher value or non-compliant values are found, the current practice advises reviewing all the methodology employed in the assessment procedures. Nevertheless, as all the batches were analyzed at the same time, it can be inferred that the findings reveal correct values.
Figure 6 shows that batches no. 0802014, 08020015 and 08020016 have a disulfide content value of about half the maximum allowed value. In cases like this, it is advisable that the laboratory that manufactured the product conduct a more detailed disulfide content monitoring study for as long as the validity time of the referred batches, in order to avoid future problems as advised by Resolution Act RE no. 1 of July 29, 2005. (Brasil, Anvisa, 2005).
When these three batches were assessed, it came to our notice that they were then the object of stability studies as they were undergoing the process of validation. The current legislation, however, advises for the analysis of one of such batches, since LFM’s annual 25mg captopril production is a little over 15 batches/year (Brasil, Anvisa, 2005).
CONCLUSIONAccording to our findings, it can be concluded that the captopril
produced by LFM complies with the quality control standards established by Farmacopéia Brasileira.
By assessing the degradation product in 25mg captopril produced by LFM and comparing the findings with two other products available in the market we conclude that LFM has the same levels of quality compliance as the batches of products available in the market regarding the quality standards of captopril and its degradation product.
This study has evidenced the utmost importance of assessing and monitoring the quality of the raw materials used in the pharmaceutical industry, starting off with their acquisition and moving on to storage and product final use, as far as the quantitative determination of captopril disulfide content is concerned. Such assessment aims to avoid future problems and public embarrassment of a pharmaceutical company regarding the validity time of a product. This was further evidenced by the findings regarding Laboratory A, which showed a degradation product value very close to maximum limit value. Such precautionary assessment can prevent the emergence of future problems as it may extend the validity time of the product for one more year.
The assessment study with the batches produced by LFM is also highly important regarding Good Production Practices (GPP), as it assures the assessment of quality compliance as of production start-up through the limit date of the validity time. It also allows for precautionary assessment and subsequent action, if necessary, in case any trait of non-compliance is detected during the studies.
In addition to the stated above, quality assessment of the pharmaceutical products available in the market is a strategically valuable tool for sanitary surveillance agencies whenever they are faced with suspicion or indictment of adulterated, therapeutically defective or somehow altered (regarding their aspect or physical-chemical properties) pharmaceutical products.
ACKNOWLEDGEMENTSWe would like to thank the Escola de Saúde, the LFM Director, the
technician in charge of the study guidance, the Quality Control Division, the R&D Department, and all the staff of LFM for their invaluable support and collaboration throughout the development of this study.
REFERENCES1. Azevedo RCP. Estudo da liberação in vitro de Captopril cápsulas
magistrais por Cromatografia Líquida de Alta Eficiência. 2007. Dissertação (Mestrado em Ciências Farmacêuticas) – Universidade Federal de Alfenas, Minas Gerais.
2. Brasil. Agência Nacional de Vigilância Sanitária. Proveme. Brasília. [Accessed on: 19 jun. 2008]. Available at: <http:// www.anvisa.gov.br/Inspeção/ Fiscalização>
3. Brasil. Agência Nacional de Vigilância Sanitária. Resolução RDC 210 de 04 de agosto de 2003. Regulamento técnico das boas práticas para a fabricação de medicamentos. Diário da República Federativa do Brasil. Brasília: 2003.
4. Brasil. Agência Nacional de Vigilância Sanitária. Resolução RE nº 1 de 29 de julho de 2005. Guia para a realização de estudos de estabilidade. Diário da República Federativa do Brasil. Brasília; 2005.
5. Brunton LL, Lazo JS, Parker KL. In: Goodman, Gilman .As bases

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 47-53 - 53
farmacológicas da terapêutica. 11. ed. Rio de Janeiro: McGrawHill ; 2006. p.17.
6. Camargo EA, Zanini AC, Ciola-Sanchez L. Avaliação qualitativa no uso de medicamentos. Semina. 1991; 2(2):70-83.
7. Ciola-Sanchez L. Consumo, custos e utilidade clínica: a avaliação do uso de medicamentos na região de Emília Romagna. Rev Bras Med. 1993;50(4):297-313.
8. Farmacopéia Brasileira. 4. ed. São Paulo: Atheneu; 2002. pt. 2, p. 181.
9. Larini L. Fármacos e Medicamentos. Porto Alegre: Artmed, 2008. p.167-168.
10. Marcatto AP., et al. Análise de cápsulas de Captopril manipuladas em farmácias. Rev Ci Farm Basic e Aplic. 2005;26(3): 221-25.
11. Palmeira Filho PL, Pan SSK. Cadeia farmacêutica no Brasil: avaliação preliminar e perspectivas. BNDES Setorial. 2003;18:3-22.
12. Santana G., et al. Avaliação da qualidade do AAS 100mg frente ao teor do produto de degradação ácido salicílico. Rev Control. Contaminação. 2007; 9(99):33-8.
13. Thomaz S. Manipulação magistral no Brasil: cinco séculos de futuro. Intern. J Pharm Comp. 2001; 3(1):10-16.
14. US Pharmacopeia National Formulary. 29. ed . lWebcom Limited; 2005. p. 366-7.
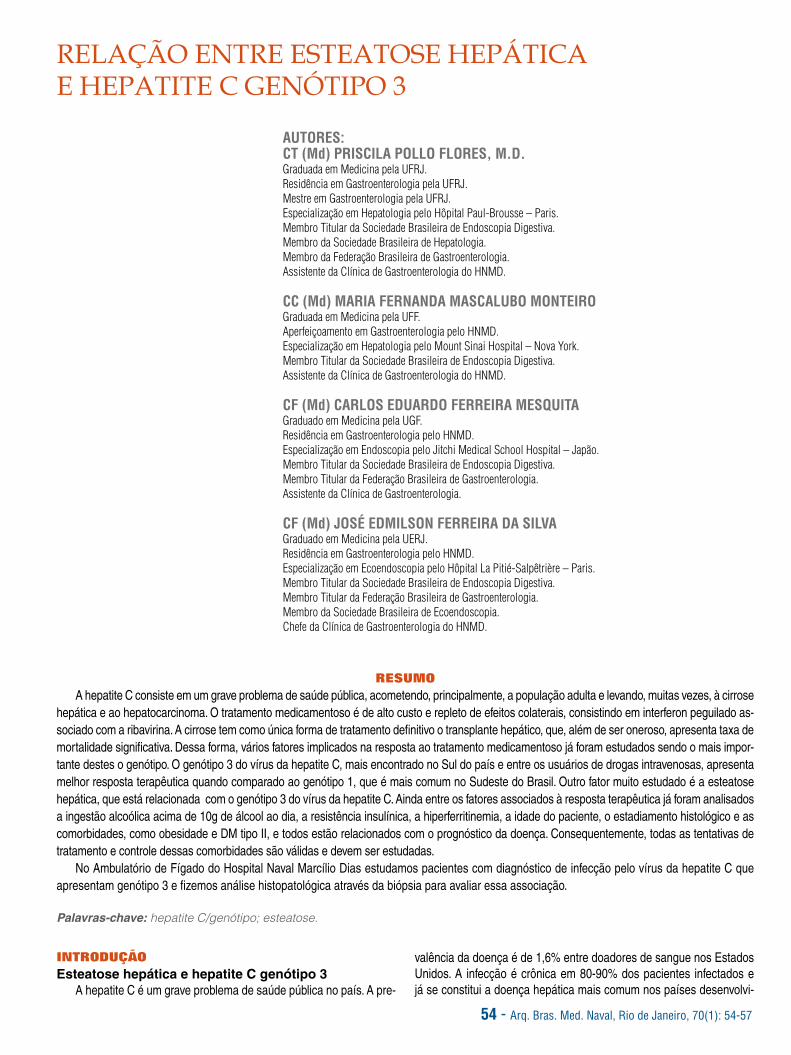
54 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 54-57
RELAÇÃO ENTRE ESTEATOSE HEPÁTICA E HEPATITE C GENÓTIPO 3
AUTORES:CT (Md) PRISCILA POLLO FLORES, M.D. Graduada em Medicina pela UFRJ.Residência em Gastroenterologia pela UFRJ.Mestre em Gastroenterologia pela UFRJ.Especialização em Hepatologia pelo Hôpital Paul-Brousse – Paris.Membro Titular da Sociedade Brasileira de Endoscopia Digestiva.Membro da Sociedade Brasileira de Hepatologia.Membro da Federação Brasileira de Gastroenterologia.Assistente da Clínica de Gastroenterologia do HNMD.
CC (Md) MARIA FERNANDA MASCALUBO MONTEIRO Graduada em Medicina pela UFF.Aperfeiçoamento em Gastroenterologia pelo HNMD.Especialização em Hepatologia pelo Mount Sinai Hospital – Nova York.Membro Titular da Sociedade Brasileira de Endoscopia Digestiva.Assistente da Clínica de Gastroenterologia do HNMD.
CF (Md) CARLOS EDUARDO FERREIRA MESQUITA Graduado em Medicina pela UGF.Residência em Gastroenterologia pelo HNMD.Especialização em Endoscopia pelo Jitchi Medical School Hospital – Japão.Membro Titular da Sociedade Brasileira de Endoscopia Digestiva.Membro Titular da Federação Brasileira de Gastroenterologia.Assistente da Clínica de Gastroenterologia.
CF (Md) JOSÉ EDMILSON FERREIRA DA SILVA Graduado em Medicina pela UERJ.Residência em Gastroenterologia pelo HNMD.Especialização em Ecoendoscopia pelo Hôpital La Pitié-Salpêtrière – Paris.Membro Titular da Sociedade Brasileira de Endoscopia Digestiva.Membro Titular da Federação Brasileira de Gastroenterologia.Membro da Sociedade Brasileira de Ecoendoscopia.Chefe da Clínica de Gastroenterologia do HNMD.
RESUMOA hepatite C consiste em um grave problema de saúde pública, acometendo, principalmente, a população adulta e levando, muitas vezes, à cirrose
hepática e ao hepatocarcinoma. O tratamento medicamentoso é de alto custo e repleto de efeitos colaterais, consistindo em interferon peguilado as-sociado com a ribavirina. A cirrose tem como única forma de tratamento definitivo o transplante hepático, que, além de ser oneroso, apresenta taxa de mortalidade significativa. Dessa forma, vários fatores implicados na resposta ao tratamento medicamentoso já foram estudados sendo o mais impor-tante destes o genótipo. O genótipo 3 do vírus da hepatite C, mais encontrado no Sul do país e entre os usuários de drogas intravenosas, apresenta melhor resposta terapêutica quando comparado ao genótipo 1, que é mais comum no Sudeste do Brasil. Outro fator muito estudado é a esteatose hepática, que está relacionada com o genótipo 3 do vírus da hepatite C. Ainda entre os fatores associados à resposta terapêutica já foram analisados a ingestão alcoólica acima de 10g de álcool ao dia, a resistência insulínica, a hiperferritinemia, a idade do paciente, o estadiamento histológico e as comorbidades, como obesidade e DM tipo II, e todos estão relacionados com o prognóstico da doença. Consequentemente, todas as tentativas de tratamento e controle dessas comorbidades são válidas e devem ser estudadas.
No Ambulatório de Fígado do Hospital Naval Marcílio Dias estudamos pacientes com diagnóstico de infecção pelo vírus da hepatite C que apresentam genótipo 3 e fizemos análise histopatológica através da biópsia para avaliar essa associação.
Palavras-chave: hepatite C/genótipo; esteatose.
INTRODUÇÃOEsteatose hepática e hepatite C genótipo 3
A hepatite C é um grave problema de saúde pública no país. A pre-
valência da doença é de 1,6% entre doadores de sangue nos Estados Unidos. A infecção é crônica em 80-90% dos pacientes infectados e já se constitui a doença hepática mais comum nos países desenvolvi-

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 54-57 - 55
dos. Essa infecção é também a maior causa de transplantes hepáticos nessas regiões. A transmissão ocorre através de transfusões sanguí-neas, uso de drogas intravenosas e em pacientes em hemodiálise. A infecção leva à cirrose hepática em 20-30% dos casos num período de 20-30 anos. A apresentação crônica geralmente é assintomática enquanto não ocorre cirrose. A queixa de fadiga muitas vezes está pre-sente, mas compreende um sintoma muito inespecífico. As alterações laboratoriais, por sua vez, também são inespecíficas, pois o aumento das aminotransferases pode não ocorrer em um terço dos casos. Há fatores do hospedeiro e virais relacionados com a evolução da doença. Existem fatores do hospedeiro como idade, etnia, uso de álcool e este-roides que estão relacionados com a evolução da doença, assim como entre os fatores virais, a infecção, por mais de uma quasiespécie, piora o prognóstico. Existem seis genótipos diferentes identificados além de subtipos. As quasiespécies surgem principalmente com o tratamento do vírus. A identificação do genótipo é importante pois modifica o tem-po de tratamento. A evolução da fibrose para cirrose não parece estar relacionada com a quasiespécie ou o genótipo através dos estudos. Os genótipos presentes no Brasil são, principalmente, os tipos 1, 2 e 3. O genótipo 3 é mais prevalente no Sul do Brasil e, principalmente, entre usuários de drogas intravenosas. No Sudeste, os genótipos mais comuns são o 1a e 1b, relacionados com pior resposta ao tratamento com interferon peguilado associado com ribavirina. Os fatores prediti-vos de resposta ao tratamento são vários e fundamentais, visto que nos permitem entender melhor os não respondedores e respondedo-res parciais, além de possibilitar uma nova perspectiva de tratamento e retratamento. O mais importante fator isolado implicado na resposta ao tratamento é o genótipo do paciente, mas a idade < 40 anos, a carga vi-ral mais baixa, a ferritina normal, a gama-glutamil transpeptidase mais baixa e a ausência de cirrose são outros fatores associados com bom prognóstico. Outro fator muito estudado é a presença de esteatose e, mais atualmente, de esteatohepatite. A presença de esteatose, resis-tência insulínica, síndrome plurimetabólica e mesmo o diabetes melli-tus tipo II está associada com pior resposta ao tratamento, pior evolu-ção clínica e mais fibrose à biópsia. Na hepatite C existe associação já comprovada com maior prevalência de DM tipo II e esteatose hepática. A presença de esteatose, no caso do genótipo 1, está associada com o distúrbio metabólico per se, enquanto no genótipo 3 está associada com fatores virais, que, quando tratados, são corrigidos e a esteatose tende a desaparecer.
A esteatose hepática é muito prevalente e consiste na maior causa de consulta ao hepatologista nos dias atuais. A sua presença é fator de prog-nóstico ruim tanto para evolução da doença como para a resposta ao tra-tamento. No entanto, a associação com o genótipo 3 na biópsia hepática é descrita na literatura como frequente. Essa associação é relacionada com a cinética viral e uma vez tratada a hepatite C com sucesso, a esteatose desaparece com tratamento antiviral. Essa observação já não é encontra-da no genótipo 1, no qual a esteatose não resolve com tratamento antiviral, mas sim com tratamento que visa ao desarranjo metabólico.
Objetivos primários
1) Identificar, na nossa casuística, a prevalência de genótipo 3.2) Correlacionar a presença de esteatose na biópsia hepática com
o genótipo 3.
Objetivos secundários1) Caracterizar os parâmetros clínicos, evolutivos e laboratoriais dos
pacientes com genótipo 3 acompanhados no Ambulatório de Hepatolo-gia do Hospital Naval Marcílio Dias.
PACIENTES E MÉTODOSForam estudados 287 pacientes do Ambulatório de Hepatologia do
Hospital Naval Marcílio Dias, sendo 14 pacientes portadores de genótipo 3.Desenho do estudo: retrospectivo transversal.Os prontuários foram avaliados e todos os dados foram lançados no
banco de dados do Excel. Esses dados são aqueles referentes a epide-miologia, dados demográficos, resultado de carga viral pelo método PCR, análise histopatológica pela classificação de Metavir e resposta terapêuti-ca. A resposta terapêutica foi considerada quando houve negativação da carga viral pelo método PCR (Polymerase Chain Reaction) no terceiro mês de tratamento (12 semanas) ou queda de 2 log ou mais nesse período e negativação no sexto mês de tratamento. A resposta terapêutica sustenta-da foi caracterizada quando, depois de seis meses do final do tratamento, a carga viral pelo método PCR persistia negativa.
A análise foi feita através de tabelas 2 X 2 e teste do qui-quadrado para variáveis categóricas e adotado o valor de p < 0,05 como estatisti-camente significativo.
RESULTADOS1) Idade: conforme o gráfico apresentado, observa-se que a maio-
ria dos pacientes encontra-se na faixa etária acima dos 50 anos
2) Sexo: a metade dos pacientes estudados é feminina e a outra metade, masculina.
3) Cirrose: dez pacientes não apresentavam cirrose à biópsia he-pática mas quatro pacientes apresentavam esse achado à biópsia.

56 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 54-57
4) Carga viral: a maior parte desses pacientes apresentava carga viral reduzida, abaixo de 300 mil.
5) Aminotransferases: os valores de aminotransferases foram ele-vados em metade dos casos.
6) Biópsia hepática: foi realizada em 57% dos pacientes.
7) Resultados histopatológicos: aproximadamente, metade dos pa-cientes apresentava biópsia hepática, e os achados mais comuns fo-ram fibrose e inflamação, sendo a esteatose encontrada apenas em 20% dos casos.
8) Resposta ao tratamento: os pacientes tratados tiveram res-posta em apenas 6%, enquanto 20% não obtiveram nenhuma res-posta. Alguns ainda estão em tratamento e em outros foi necessária a suspensão devido a efeitos colaterais graves como plaquetopenia e neutropenia.
Resultados Coinfectados – 0%. Transplante – 0%. Sem tratamento – 9/14. Interferon + Ribavirina – 3/14. Interferon + Ribavirina/Interferon peguilado + Ribavirina – 1/14. Ribavirina + Peguilado – 1/14.
DISCUSSÃOA hepatite C genótipo 3 apresenta certas particularidades já es-
tabelecidas, como maior presença de esteatose hepática à biópsia hepática, que está relacionada com a cinética viral e não com as condições individuais. Da mesma forma, o prognóstico e a resposta ao tratamento padrão costumam ser melhores do que no genótipo 1, que é muito mais comum. Por outro lado, sabemos que esse genóti-po é menos comum, apresentando uma distribuição geográfica bem conhecida, mais frequente no Sul do país e também entre usuários de drogas venosas. Os valores da alanina aminotransferase (ALT) estavam elevados em metade dos pacientes e hoje em consonância com estudos recentes, sabemos que cerca de um terço dos pacien-tes com hepatite C apresentam ALT normal. O achado de fibrose he-pática à biópsia hepática foi, surpreendentemente, mais comum do que aquele descrito na literatura bem como a resposta ao tratamento foi menor na nossa amostragem. Na tentativa de conhecer e justificar esses achados discrepantes podemos sugerir o tempo de doença dos pacientes em questão, que foi superior ao encontrado em outros estudos. Poderíamos fazer alusão também à idade dos pacientes, já que a grande maioria se encontrava além da sexta década de vida. Um ponto importante a ser considerado consiste no fato de que utili-zamos apenas interferon convencional nesses pacientes nessa épo-ca, o que, certamente, interfere no resultado, uma vez que o interfe-ron peguilado ainda apresenta melhor resultado.
CONCLUSÃOEmbora a nossa amostragem tenha sido pequena em relação ao
grupo de pacientes com genótipo 3, podemos observar que a percen-tagem e o número de pacientes com esteatose na biópsia hepática fo-ram menores do que o descrito na literatura, bem como a percentagem de fibrose encontrada no estudo foi maior do que aquela descrita nos estudos recentes. Em relação ao tratamento com interferon e ribaviri-na, os pacientes estudados também tiveram resposta menor do que a descrita na literatura.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 54-57 - 57
REFERÊNCIAS1. Lim YS, Kim WR. The global impact of hepatic fibrosis and end-
stage liver disease. Clin Liver Dis. 2008; 12(4):733.2. Manns MP, Wedemeyer H, Cornberg M (2006). Treating viral he-
patitis C: efficacy, side effects, and complications.Gut. 55(9): 1350-9.3. Pawlotsky JM (2003). Diagnostic testing in hepatitis C virus in-
fection: viral kinetics and genomics. Semin Liver Dis. 23 Suppl 1: 3-11.4. Bacon BR. Treatment of patients with hepatitis C and normal se-
rum aminotransferase levels. Hepatology. 2002;36(5 Suppl 1): S179-S184.
5. Berg T, von Wagner M, Nasser S, et al. Extended treatment dura-tion for hepatitis C virus type 1: comparing 48 versus 72 weeks of pegin-terferon-alfa-2a plus ribavirin. Gastroenterology. 2006;130(4):1086-97.
6. Dalgard O, Bjoro K, Hellum KB et al. Treatment with pegylated interferon and ribavarin in HCV infection with genotype 2 or 3 for 14 weeks: a pilot study. Hepatology. 2004;40(6):1260-5.
7. Dalgard O, Bjoro K, Ring-Larsen H, et al. Pegylated interferon alfa and ribavirin for 14 versus 24 weeks in patients with hepatitis C virus genotype 2 or 3 and rapid virological response. Hepatology. 2008;47(1):35-42.
8. Di Bisceglie AM, Shiffman ML, Everson GT, et al. Prolonged an-tiviral therapy with peginterferon to prevent complications of advanced liver disease associated with hepatitis c: results of the hepatitis c an-
tiviral long-term treatment against cirrhosis (HALTC) Trial. Hepatology. 2007;46(4):80.
9. Jacobson IM, Gonzalez SA, Ahmed F, et al. A randomized trial of pegylated interferon alpha-2b plus ribavirin in the retreatment of chronic hepatitis C. Am J Gastroenterol. 2005;100(11):2453-62.
10. Mangia A, Santoro R, Minerva N, et al. Peginterferon alfa-2b and ribavirin for 12 vs. 24 weeks in HCV genotype 2 or 3. N Engl J Med. 2005;352(25):2609-17.
11. Marcellin P, Freilich B, Andreone P, et al. HCV-RNA sta-tus at week 12 of treatment with peginterferon alfa-2a/RBV pre-dicts SVR in patients with prior non-response to pegylated interfe-ron alfa-2b/RBV: Results from repeat study. Journal of Hepatology. 2008;48:S301.
12. Shiffman ML, Di Bisceglie AM, Lindsay KL, et al. Peginterferon alfa-2a and ribavirin in patients with chronic hepatitis C who have failed prior treatment. Gastroenterology. 2004;126(4):1015-23.
13. Shiffman ML, Suter F, Bacon BR, et al. Peginterferon alfa-2a and ribavirin for 16 or 24 weeks in HCV genotype 2 or 3. N Engl J Med. 2007;357(2):124-34.
14. Lange C, Sarrazin C, Acute and cronic hepatitis C: diagnostics tests. In: Hepatology: a clinical textbook. 2009. p.171-82.
15. Cornberg M, Michael P. Manns and Wedemeyer H Standards of care. In: Hepatology: a clinical textbook. 2009. p. 183-210

58 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 58-61
THE ASSOCIATION BETWEEN HEPATIC STEATOSIS AND HEPATITIS C VIRUS GENOTYPE 3
AUTHORS:CT (Md) PRISCILA POLLO FLORES, M.D. Bachelor’s Degree in Medicine from UFRJ.Medical Resident Training in Gastroenterology at UFRJ.Master’s Degree in Gastroenterology from UFRJ.Specialization in Hepatology from the Hôpital Paul-Brousse – Paris.Active Member of the Brazilian Society of Digestive Endoscopy.Member of the Brazilian Society of Hepatology.Member of the Brazilian Federation of Gastroenterology.Physician Assistant at the Gastroenterology Clinic of HNMD.
CC (Md) MARIA FERNANDA MASCALUBO MONTEIRO Bachelor’s Degree in Medicine from UFF.Extended Training in Gastroenterology at HNMD.Specialization in Hepatology from the Mount Sinai Hospital – New York.Active Member of the Brazilian Society of Digestive Endoscopy.Physician Assistant at the Gastroenterology Clinic of HNMD.
CF (Md) CARLOS EDUARDO FERREIRA MESQUITA Bachelor’s Degree in Medicine from UGF.Medical Resident Training in Gastroenterology at HNMD.Specialization in Endoscopy from the Jitchi Medical School Hospital – Japan.Active Member of the Brazilian Society of Digestive Endoscopy.Active Member of the Brazilian Federation of Gastroenterology.Physician Assistant at the Gastroenterology Clinic.
CF (Md) JOSÉ EDMILSON FERREIRA DA SILVA Bachelor’s Degree in Medicine from UERJ.Medical Resident Training in Gastroenterology at HNMD.Specialization in Echoendoscopy from the Hôpital La Pitié-Salpêtrière – Paris.Active Member of the Brazilian Society of Digestive Endoscopy.Active Member of the Brazilian Federation of Gastroenterology.Member of the Brazilian Society of Echoendoscopy.Chief of the Gastroenterology Clinic at HNMD.
ABSTRACTType C hepatitis is a serious public health problem that affects mainly the adult population. It can evolve into hepatic cirrhosis and hepatocellular
carcinoma. The medical treatment is highly costly and leads to a considerable number of side effects, derived from the best available therapy - pegylated interferon associated with ribavirine. The only definitive treatment of cirrhosis is liver transplantation, which is extremely expensive and has significant mortality rate. Therefore, various factors implied in medication treatment response have been studied, and genotype has been pointed as the major factor. Genotype 3 of Type C hepatitis, more commonly found in the Southern parts of Brazil and in intravenous drug users, has shown a more therapeutic response when compared against genotype 1, which more commonly occurs in Southeastern Brazil. Another much studied factor is hepatic steatosis, which is associated with genotype 3 of the type C hepatitis virus. Still among already investigated therapeutic response-associated factors are daily alcoholic intake higher than 10g, insulin resistance, hyperferritinemia, the patient’s age, histologic assessment and comorbidities like obesity and DM (diabetes mellitus) type II. Consequently, all attempts to treat and control these comorbidities are valid and must be investigated.
We have studied type C hepatitis genotype 3 virus patients at the Hepatic Ward of Hospital Naval Marcílio Dias and conducted their histopathologic analysis in order to assess this association.
Keywords: type C hepatitis/genotype; steatosis.
INTRODUCTIONHepatic steatosis and type C hepatitis genotype 3
Type C hepatitis is a serious public health problem in Brazil. In the US,
the disease is identified in 1.6% of all blood donors and it develops into a chronic infection in 80-90% of all infected patients, thus constituting the most common hepatic disease in developed countries. This infection is also the

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 58-61 - 59
major cause for hepatic transplants in these countries. Transmission occurs through blood transfusion, use of intravenous drugs and in patients under hemodyalysis. This infection develops into hepatic cirrhosis in 20-30% of all cases within 20-30 years. Chronic manifestation is generally asymptomatic until cirrhosis does not develop. Patients complain about fatigue often times, but in a rather non-specific manner. Laboratory test alterations are also non-specific, as the increase of aminotransferasis may not occur in one-third of all the cases. Some host-patient related and virus-related features can be associated with the disease development. Host-patient related factors such as age, ethnics and alcohol and steroid consumption are associated with the disease development. Likewise, virus-related factors, and infection, a quasi-species, so as to speak, makes prognostics worse. There are six different identified genotypes in addition to the subtypes. Quasi-species emerge mainly once the virus is treated. Identifying the genotype is essential once it affects the treatment length. Studies have shown that the evolution of fibrosis into cirrhosis does not seem to be associated with the quasi-species or the genotype. The genotypes that occur in Brazil are mainly types 1, 2 and 3. Genotype 3 prevails in Southern Brazil and mainly amongst intravenous drug users, while in the Southeast the most common genotypes are 1a and 1b, related to lower response to pegylated interferon associated with ribavirine. Predictable response factors are various and of fundamental importance, for they allow us to better understand those that do not respond and those that respond partially, and so prescribe better directive treatment and retreatment. The major response-associated isolated factor is the patient’s genotype, while being under 40 years of age, bearing a lower viral load, having normal ferritin levels, lower gama-glutamil transferasis (GGT) and the lack of cirrhosis are other factors associated with good prognostics. Another widely studied factor is the presence of steatosis and more recently, of steatohepatitis. Steatosis, insulin resistance, plurimetabolic syndrome and even diabetes mellitus type II, are associated with the worst response to treatment, worse clinical evolution and added fibrosis to the biopsy. In the case of type C hepatitis, it has been proven a higher level of association with DM type II and hepatic steatosis. The latter, regarding genotype 1, is associated with the metabolic condition per se, while in genotype 3, it is associated with viral factors that, when treated, are corrected and steatosis tends to disappear.
Hepatic steatosis is prevalent and stands for the major cause of visits to hepatologists nowadays. Its presence is a bad prognostics factor, both for the disease evolution and for the response to treatment. Nevertheless, the association with genotype 3 in hepatic biopsy is described by the literature as being frequent. Such association is related to the viral kinetics, and once type C hepatitis is successfully treated, steatosis disappears with antivirus treatment. The latter result does not apply, however, to genotype 1, in which steatosis cannot be cured through antivirus treatment, but rather through metabolic disarrangement treatment.
Primary objectives1) Identify, within our casuistic scope, the prevalence of genotype 3.2) Correlate the presence of steatosis in hepatic biopsy with genotype 3.
Secondary objectives1) Characterize the clinical, evolutionary and laboratorial parameters
for genotype 3 patients that have been assessed at the Hepatic Ward of Hospital Naval Marcílio Dias.
PATIENTS AND METHODSStudy sample: 287 patients at the Hepatic Ward of Hospital Naval
Marcílio Dias, 14 of which were genotype 3 patients.Study design: retrospective transversal analysis.Patient records were assessed and all data were uploaded into
an Excel database. Data refer to epidemiology, demographics, and viral load results as per PCR (Polymerase Chain Reaction) method, histopathologic analysis according to Metavir classification and therapeutic response. Therapeutic response referred to negative viral load as per PCR method in the third month of treatment (12 weeks) or an equal to or higher than 2 log decrease within this period, and negative load in the sixth month of treatment. Sustained therapeutic response was characterized when, six months after the treatment was completed, the viral load as per PCR method remained negative.
The analysis was conducted through 2 X 2 tables and chi-square test for categorical variables, in compliance with the adopted value of p < 0.05 taken as statistically significant.
RESULTS1) Age: as shown in the graph below, most patients belong to the
above 50 years of age group.
2) Gender: half the assessed patients are female, and the other half are male.
3) Cirrhosis: the hepatic cirrhosis analysis revealed that ten patients did not have cirrhosis, while four patients did.

60 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 58-61
4) Viral load: most of the assessed patients had a lower viral load, below 300 thousand.
5) Aminotransferasis: aminotransferasis amounts increased in about half the cases.
6) Hepatic biopsy: conducted in 57% of the patients.
7) Histopathologic results: approximately half the patients showed hepatic biopsy, and the most common findings were fibrosis and inflammation, while steatosis was found in only 20% of the cases.
8) Response to treatment: the patients that were treated showed a mere 6% response, while 20% had no response. Some patients are still undergoing treatment, while for others treatment has been suspended because of serious side effects like plaquetopeny and neutropeny.
Results Co-infected patients – 0%. Transplants – 0%. Not undergoing any treatment – 9/14. Interferon + Ribavirine – 3/14. Interferon + Ribavirine/Pegylated interferon + Ribavirine – 1/14. Ribavirina + Pegylated – 1/14.
DISCUSSIONThe hepatitis C virus genotype 3 has some peculiarities that
have already been established as, for instance, the higher presence of hepatic steatosis to hepatic biopsy, which is associated with viral kinetics and not with individual conditions. Equally, the prognosis and response to standard treatment are usually better in genotype 3 than in genotype 1, which is much more common. On the other hand, we know that genotype 3 is less common, showing a well known geographic distribution, more commonly found in the Southern parts of Brazil and among intravenous drug users. The alanina aminotransferase (ALT) values were higher in half of the patients and, today, based on recent studies, we know that approximately one-third of the patients with hepatitis C show normal ALT level. Hepatic fibrosis added to hepatic biopsy was, surprisingly, more common than that described by the literature. It was also found lesser response to treatment in our sampling. A possible reason for these differing findings may arise from the length of the disease, which was longer than the cases observed in the other studies. We could also point out the age of the patients; almost all were 60 years old or older. An important point to be considered is the fact that they were only treated with standard interferon at that time. This treatment interferes with the result, once the pegylated interferon still shows a more optimistic prognosis.
CONCLUSIONAlthough our sampling was rather small given the group of genotype 3
patients, our study shows that the percentage and the number of patients that had steatosis in the hepatic biopsy was below what is expressed in the literature. The percentage of fibrosis revealed by this study was above that described in recent studies. In what regards the treatment with interferon and ribavirine, the assessed patients also showed a lower response than that discussed in the literature.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 58-61 - 61
REFERENCES1. Lim YS, Kim WR. The global impact of hepatic fibrosis and end-
stage liver disease. Clin Liver Dis. 2008;12(4):733.2. Manns MP, Wedemeyer H, Cornberg M (2006). Treating
viral hepatitis C: efficacy, side effects, and complications. Gut. 55(9): 1350-9.
3. Pawlotsky JM (2003). Diagnostic testing in hepatitis C virus infection: viral kinetics and genomics. Semin Liver Dis. 23 Suppl 1: 3-11.
4. Bacon BR. Treatment of patients with hepatitis C and normal serum aminotransferase levels. Hepatology. 2002;36(5 Suppl 1): S179-S184.
5. Berg T, von Wagner M, Nasser S, et al. Extended treatment duration for hepatitis C virus type 1: comparing 48 versus 72 weeks of peginterferon-alfa-2a plus ribavirin. Gastroenterology. 2006;130(4):1086-97.
6. Dalgard O, Bjoro K, Hellum KB et al. Treatment with pegylated interferon and ribavarin in HCV infection with genotype 2 or 3 for 14 weeks: a pilot study. Hepatology. 2004;40(6):1260-5.
7. Dalgard O, Bjoro K, Ring-Larsen H, et al. Pegylated interferon alfa and ribavirin for 14 versus 24 weeks in patients with hepatitis C virus genotype 2 or 3 and rapid virological response. Hepatology. 2008;47(1): 35-42.
8. Di Bisceglie AM, Shiffman ML, Everson GT, et al. Prolonged antiviral therapy with peginterferon to prevent complications of
advanced liver disease associated with hepatitis c: results of the hepatitis c antiviral long-term treatment against cirrhosis (HALTC) Trial. Hepatology. 2007; 46(4) :80.
9. Jacobson IM, Gonzalez SA, Ahmed F, et al. A randomized trial of pegylated interferon alpha-2b plus ribavirin in the retreatment of chronic hepatitis C. Am J Gastroenterol. 2005;100(11): 2453-62.
10. Mangia A, Santoro R, Minerva N, et al. Peginterferon alfa-2b and ribavirin for 12 vs. 24 weeks in HCV genotype 2 or 3. N Engl J Med. 2005; 352 (25): 2609-17.
11. Marcellin P, Freilich B, Andreone P, et al. HCV-RNA status at week 12 of treatment with peginterferon alfa-2a/RBV predicts SVR in patients with prior non-response to pegylated interferon alfa-2b/RBV: Results from repeat study. Journal of Hepatology. 2008; 48: S301.
12. Shiffman ML, Di Bisceglie AM, Lindsay KL, et al. Peginterferon alfa-2a and ribavirin in patients with chronic hepatitis C who have failed prior treatment. Gastroenterology. 2004; 126(4): 1015-23.
13. Shiffman ML, Suter F, Bacon BR, et al. Peginterferon alfa-2a and ribavirin for 16 or 24 weeks in HCV genotype 2 or 3. N Engl J Med. 2007; 357(2): 124-34.
14. Lange C, Sarrazin C, Acute and cronic hepatitis C: diagnostics tests. In: Hepatology: a clinical textbook. 2009. p.171-82.
15. Cornberg M, Michael P. Manns and Wedemeyer H Standards of care. In: Hepatology: a clinical textbook. 2009. p. 183-210

62 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 62-68
TRATAMENTO CIRÚRGICO DAS COMPLICAÇÕES MECÂNICAS DO INFARTO AGUDO DO MIOCÁRDIO
AUTORES:CMG (Md-RM1) HERMES DE SOUZA FELIPPEGraduado em Medicina pela Santa Casa de Misericórdia de Vitória.Residência em Cirurgia Cardíaca pelo Incor.Especialista em Cirurgia Cardíaca pela Sociedade Brasileira de Cirurgia Cardiovascular.Chefe da Clínica de Cirurgia Cardíaca do HNMD.
CT (Md) MARCOS FLORIPES DA SILVAGraduação em Medicina pela Faculdade de Medicina de Valença.Residência em Cirurgia Geral pelo HNMD.Residência em Cirurgia Torácica pelo HNMD.Especialista em Cirurgia Cardíaca pelo Incor.Assistente da Clínica de Cirurgia Cardíaca do HNMD.
EDUARDO SÉRGIO BASTOS, M.D., Ph.D.Graduação em Medicina pela Universidade Federal de Sergipe.Residência em Cirurgia Cardíaca pelo Hospital dos Servidores do Estado do Rio de Janeiro.Mestrado em Cirurgia Cardíaca pela UFRJ.Doutorado em Cirurgia Cardíaca pela UFRJ.Professor Associado de Cirurgia Cardíaca da Faculdade de Medicina da UFRJ.Membro Titular da Sociedade Brasileira de Cirurgia Cardiovascular.Cirurgião Cardíaco do HNMD.
RESUMOApós o advento das terapias com trombolíticos e da angioplastia de resgate, para o tratamento do Infarto Agudo do Miocárdio, tem-se observado uma
redução das complicações de origem mecânica, embora ainda participe com um importante percentual na taxa de mortalidade. Neste estudo revisional, os autores descrevem suas formas de apresentação, taxas de ocorrência e as principais técnicas cirúrgicas empregadas para correções dessas complicações.
Palavras-chave: infarto agudo do miocárdio/complicações; aneurisma cardíaco/complicações; ruptura cardíaca pós infarto/complicações.
INTRODUÇÃOApesar do desenvolvimento e aperfeiçoamento de métodos propedêu-
ticos mais eficazes, a incidência de complicações e da mortalidade do infar-to agudo do miocárdio (IAM) ainda permanece consideravelmente elevada.
Terapêuticas que visam à reperfusão precoce no IAM têm reduzido as complicações, a área de necrose e mortalidade relacionadas ao infarto; o controle do remodelamento ventricular vem promovendo melhora na quali-dade de vida. Apesar de todos os recursos disponíveis, alguns casos ainda respondem mal à terapêutica instituída podendo apresentar complicações graves como: ruptura da parede livre do ventrículo esquerdo, ruptura ou disfunção de músculo papilar com insuficiência mitral aguda, ruptura do septo interventricular, aneurismas e pseudoaneurismas ventriculares, cho-que cardiogênico, complicações elétricas e insuficiência cardíaca. Tratare-mos neste artigo das complicações mecânicas do IAM.
Diante de tais consequências são necessárias intervenções, mui-tas vezes emergenciais, visando restabelecer a dinâmica funcional ventricular para manter o equilíbrio hemodinâmico.
DESENVOLVIMENTOCIV pós IAM
A Comunicação Intraventricular pós IAM (CIV pós IAM) é uma com-plicação extremamente grave, com altos índices de morbimortalidade. Um terço dos pacientes que falecem em decorrência de complicações
agudas do infarto apresenta ruptura de parede ventricular. A maioria das rupturas ocorre na parede livre do ventrículo esquerdo e apenas 15 a 20% ocorrem no septo interventricular (Janardhana, 2004).
A primeira descrição da ruptura do septo interventricular em conse- quência de um infarto agudo do miocárdio foi relatada por Latham, em 1845, e o diagnóstico em vida foi feito pela primeira vez em 1923 por Brunn (Kirklin, 1993); em 1934, Sagar (Balkanay, 2005), correlacionou a compli-cação com a doença coronariana.
A comunicação interventricular pós-infarto agudo do miocárdio (CIV pós IAM) incide aproximadamente em 1 a 3% de todos os infartos do mio-cárdio (Villavicencio, 2002) e ocorre entre o 1º e o 19º dia do IAM, mais fre-quentemente entre o 3º ± 4º dia (David, 1995). Com a implementação da terapêutica trombolítica essa incidência tem reduzido para 0,2% como de-monstrado no estudo GUSTO-I (Global Utilization of Streptokinase and TPA for Occludede Coronary Arteries) com ocorrência mais precoce, a maioria das vezes nas primeiras 24h (Elsner, 1998).
A mortalidade da CIV pós IAM é de aproximadamente 24% nas pri-meiras 24h, 60% na primeira semana e apenas 10% sobrevivem aos primeiros três meses (Marti, 2004).
Em 2000, Crenshaw e colaboradores publicaram uma análise revi-sional de 84 pacientes portadores de CIV pós IAM alocados no estudo GUSTO-I (Crenshaw, 2000) em que foram observados 41.021 pacien-tes portadores de IAM submetidos à trombólise. A CIV pós IAM, con-

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 62-68 - 63
firmada, ocorreu em 0,2% dos pacientes, sendo 94% destes diagnos-ticados na primeira semana.
A mortalidade é influenciada principalmente pelo tamanho do infar-to, localização da CIV e da precocidade do aparecimento do defeito (Ro-bert, 2003). Vários preditores foram apontados como fatores de risco para a ocorrência da CIV: hipertensão, idade avançada, sexo feminino e ausência de IAM ou angina prévia. Pacientes portadores de angina ou história prévia de IAM desenvolvem mais colaterais e estão mais sujeitos ao precondi-cionamento, o que explicaria a menor incidência da CIV pós IAM nestes pacientes (Birnbaum, 2002).
Do ponto de vista de sua localização, a maioria dos casos envolve a região ântero-apical (60%) e o restante, a região póstero-septal. A oclusão da artéria interventricular anterior está relacionada com a ori-gem das CIV ântero-apicais, e os defeitos póstero-basais com a oclu-são da coronária direita ou da artéria circunflexa, quando dominante.
Cummings et al. (1989) avaliaram 42 pacientes consecutivos porta-dores de CIV pós IAM e seus achados são semelhantes aos resultados de vários outros autores: 57% apresentavam IAM anterior, 33% inferior e 10% considerados combinados.
O comprometimento coronariano pode ser de um único vaso, ocor-rendo na maioria das vezes quando há pobre circulação colateral (Fi-gura 1). No estudo GUSTO-I a oclusão total de uma artéria estava pre-sente em 57% dos pacientes portadores de CIV pós IAM e apenas em 18% dos pacientes com IAM sem CIV (Crenshaw, 2000).
O tratamento dessa complicação é eminentemente cirúrgico. Me-didas clínicas devem ser inicialmente adotadas, como a instalação do balão intra-aórtico (BIA), suporte pressórico com drogas inotrópicas, otimização hemodinâmica e encaminhamento à cirurgia. A cirurgia de-ve ser realizada tão logo possível e preferencialmente com recurso do ecocardiograma transesofágico peroperatório.
A utilização do BIA em pacientes com sinais de baixo débito ou evidência de deterioração do quadro clínico é recomendada pela maio-ria dos autores, tendo sido relatada mortalidade de até 66,6% nos pa-cientes operados em vigência de choque cardiogênico (Dallan, 1989).
A necessidade do estudo cinecoronariográfico nos pacientes gra-ves em choque cardiogênico pode ser questionada. Alguns autores acreditam que pacientes portadores de CIV pós IAM em choque car-diogênico não necessitam de cineangiocardiografia (Skillington, 1990). Muehrcke et al. em 1992 afirmam que a revascularização do miocárdio durante a correção da CIV não interfere com a mortalidade imediata (Muehrcke, 1992), entretanto, de forma diferente, existem estudos con-flitantes sobre o prognóstico a longo prazo (Komeda, 1990; Labrousse, 2002). Evidências recomendam a realização de cinecoronariografia e, se necessário, revascularização do miocárdio nos pacientes encami-nhados à cirurgia, portadores da CIV pós-infarto (Robert, 2003).
A primeira cirurgia realizada para correção do defeito septal pós-infarto foi creditada a Cooley em 1957 e a primeira correção com so-brevida a Payne na Mayo Clinic em 1963 (Robert, 2003).
A partir da década de 70, por causa dos avanços da cirurgia cardí-aca e dos métodos de diagnóstico, a fisiopatologia dessa complicação tornou-se mais compreensível, proporcionando assim, o desenvolvi-mento e aprimoramento de várias técnicas para sua correção.
A mortalidade é significativamente menor nos pacientes submeti-dos ao tratamento cirúrgico quando comparados ao tratamento clínico, respectivamente 47% e 94% (Crenshaw, 2000).
A cirurgia visa essencialmente à correção da comunicação com utili-zação de patches (Dacron®, pericárdio autólogo, pericárdio bovino, polite-trafluoroetileno – PTFE) (David, 1995; Piwnica, 1987; Janardhana, 2004), o restabelecimento ou manutenção da geometria ventricular, e a revascu-larização do miocárdio quando indicada.
Procurando desenvolver princípios cirúrgicos básicos para a corre-ção da CIV pós IAM, Daggett (Daggett, 1982) em 1970 descreveu os princípios, que na época, nortearam a cirurgia e que consistia em re-tardar a correção para além da 6ª semana do surgimento da CIV, épo-ca em que era realizada a infartectomia e reconstrução das paredes.
Com a avaliação dos resultados observou-se que muitos pacientes não suportavam este tempo de espera, razão da redução inicial para três semanas (Piwnica, 1987) neste prazo. Essa conduta também permitiu que o tempo fosse o encarregado da seleção natural, e isso despertou a necessidade de novas mudanças na conduta, culminando com a re-comendação atual que preconiza a intervenção imediata, por mostrar melhores resultados e postergar a cirurgia excepcionalmente apenas em casos selecionados ou em pacientes portadores de defeitos de pequena magnitude com reduzido comprometimento funcional.
A maior dificuldade na correção da CIV na fase aguda deve-se à friabilidade do tecido muscular adjacente ao defeito, consequente à necrose e à isquemia da região com extensão imprevisível, dentro do conceito evolutivo da doença.
O septo apresenta-se delgado, necrosado, com fragmentos de músculos nas bordas da ruptura secundários à desintegração regional (Figura 2). A CIV varia em tamanho, de milímetros a vários centímetros, na forma e localização, podendo não ser única e, se múltiplas, não se desenvolverem a um só tempo (Kirklin, 1993). O exame ecocardiográ-fico seriado é capaz de demonstrar alterações no diâmetro e fluxos através da comunicação.
Figura 1: Paciente feminina, 73 anos, com lesão única em descendente anterior e CIV pós IAM.
Figura 2: Necrose de septo com uma CIV recente.

64 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 62-68
O orifício comunicante pode se apresentar no mesmo nível em relação ao endocárdio do septo do Ventrículo Esquerdo (VE) e Ventrículo Direito (VD), isto é, retilíneo, chamadas de CIV pós IAM simples, ou ainda, com trajetos sinuosos através do tecido necrótico do septo interventricular, cha-madas nesses casos de CIV pós IAM complexas (Jimenez, 2001). Apro-ximadamente 70% das CIV inferiores apresentam-se de forma complexa com trajeto serpiginoso através do miocárdio necrosado (Robert, 2003).
O procedimento operatório tradicional consistia na maioria das ve-zes da infartectomia e reconstrução do septo e ou parede ventricular com um ou mais patches (Daggett, 1982). Esta técnica apresentou um elevado índice de mortalidade operatória, variando de 35 a 50%.
A correção da CIV crônica infere a mesma abordagem acrescida da facilidade de se deparar com as bordas da CIV mais delimitadas e mais fibróticas, oferecendo mais consistência e firmeza às suturas. O mais pro-vável é que pacientes que evoluem nessa condição apresentem uma CIV pequena com shunt E-D menor que 1:1,5 com pouca repercussão clínica.
Em 1989 no Brasil, Da Silva et al. (Piwnica, 1987), emprega-ram uma técnica para correção da CIV em que nenhuma parte do septo ou músculo infartado era ressecada. A técnica consiste de uma incisão na zona de infarto introduzindo um patch de Dacron® na cavidade ventricular cobrindo a zona de infarto adjacente à CIV (Figuras 3 e 4). A parede ventricular é suturada utilizando-se um segundo patch para reforço e hemostasia. Esta técnica foi utilizada em sete pacientes com apenas um óbito, ocorrido em um pacien-te terminal. Dois pacientes evoluíram com pequenas CIV residuais sem repercussão clínica.
Em 1990, Komeda e colaboradores, registraram a técnica co-mo método de exclusão da área infartada (Komeda, 1990) difun-dida em 1995 por David et al. (David, 1995) com a utilização de um patch de pericárdio bovino excluindo da mesma forma a CIV e o tecido infartado. Consiste em alocar o patch sobre a área infar-tada incluindo a CIV suturando-o no endocárdio sadio em torno do orifício estendendo-se lateral e anteriormente, exteriorizando o retalho, através da ventriculotomia.
Figura 3: IAM ântero-septal com abordagem da CIV via ventriculotomia através da zona de infarto.
Quando o comprometimento for mais apical ou exigir utilização de um grande retalho, este deve ser posicionado procurando refazer a for-ma geométrica do VE. A manutenção da forma geométrica de maneira a preservar o cone apical funcional confere maior eficiência contrátil ao VE (Vera, 2001).
A abordagem da CIV através da zona de infarto atualmente é a
mais utilizada. Outras vias incluem a atrial direita (Varvarigos, 2005) para casos selecionados de pequenas CIV tardias septo-basais e utilização de umbrellas através de procedimento endovascular. Fe-chamento de CIV pequenas e apicais em alguns casos pode ser re-alizado por plicatura direta das paredes ventriculares englobando o defeito sem o emprego da circulação extra-corpórea (CEC).
Ruptura da parede livre do ventrículoA ruptura da parede livre do ventrículo é uma das complicações
mais catastróficas do infarto do miocárdio. Sua incidência ocorre apro-ximadamente em 7% dos pacientes que falecem em decorrência de um infarto agudo do miocárdio (Becker, 1996). Predomina nas primei-ras 24 horas do evento e diminui progressivamente, tornando-se pouco frequente após o quinto dia (Cordero, 2006).
A manifestação clínica predominante é de tamponamento cardíaco agudo com instalação de um hemopericárdio levando a um colapso cardio-circulatório e morte. O diagnóstico na maioria das vezes é realizado post-mortem e em raras ocasiões a intervenção cirúrgica torna-se possível.
Cordero e colaboradores (2006), relataram um caso em que a ruptura ocorreu imediatamente após o procedimento de angioplastia realizada no quinto dia do IAM de parede inferior, inferindo a reperfu-são como causa, uma vez que a maioria dos casos de ruptura pode ser devida à reperfusão tardia.
O tratamento clínico de suporte emergencial deve ser instituído e imediatamente conduzir à cirurgia. A pericardiocentese de alívio é um procedimento paliativo de salvamento e o tratamento cirúrgico deve ser considerado emergencialmente e visa principalmente corri-gir a laceração da parede com pontos aproximando as bordas da feri-da apoiadas em tiras de Teflon® uma vez que a região torna-se friável pela necrose e quase sempre circundada por uma área de sufusão hemorrágica ou hematoma.
Quando a ruptura ocorrer em pacientes previamente estudados, procedimentos complementares, como revascularização do miocárdio ou correção de outros defeitos quando associados devem ser realiza-dos visando facilitar a recuperação do paciente.
Ruptura ou disfunção do músculo papilarA maioria das rupturas de músculos papilares é decorrente de
um IAM ou trauma. A ruptura espontânea é rara e ocorre mais em pa-cientes com hipertrofia de ventrículo esquerdo e hipertensos (Vera,
Figura 4: Exclusão da CIV com pericárdio bovino e aspecto final da sutura da parede ventricular com pontos apoiados em duas tiras de Teflon®.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 62-68 - 65
2001). Atribui-se a hipertrofia a uma menor concentração de capila-res e maior grau de fibrose no miocárdio hipertrófico (Roberts, 1941), ou ainda ao aumento da massa miocárdica como causa de maior resistência à perfusão (Arosemana, 1967). Barbour et al. (1986) le-vantaram a hipótese de que a ruptura seria secundária à necrose transitória em artéria não visualizada através da cinecoronariografia responsável pela irrigação do músculo papilar.
O músculo papilar posteromedial é afetado com mais frequência. A sua ruptura produz um prolapso de ambas as cúspides da valva mitral com importante insuficiência. Apenas 25% dos pacientes sobrevivem além das primeiras 24h (Vera, 2001).
O quadro clínico depende da importância da insuficiência mitral, que quase sempre é grave, representado clinicamente por edema pulmonar e hipotensão arterial. O surgimento de um sopro, geral-mente entre o 3º e o 10º dia do IAM, faz-se suspeitar de uma com-plicação mecânica, e entre elas a disfunção ou ruptura do músculo papilar. A ruptura de músculo papilar evolui com rápida deterioração do quadro clínico, e medidas de suporte hemodinâmico devem ser prontamente utilizadas de modo a conduzir o paciente o mais breve possível à cirurgia.
A isquemia do músculo papilar que redunda em uma insufici-ência valvar também apresenta uma significativa morbimortalidade diretamente proporcional ao grau da insuficiência e velocidade de sua instalação.
O exame ecocardiográfico é considerado o “padrão ouro” para ava-liação estrutural da valva. Define o diagnóstico, diferencia a disfunção da ruptura e identifica a coexistência de outras complicações. Além disso, fornece informações com razoável acurácia para nortear a pro-babilidade de uma valvuloplastia ou troca valvar.
Novas tecnologias, como a ressonância magnética, podem ser aplicadas nessa investigação e alguns serviços a têm associado como método de investigação (D’Ancona, 2007) com detalhamento cada vez mais progressivo do funcionamento do aparelho valvar e ventricular.
Pacientes em vigência de monitorização hemodinâmica podem se beneficiar da análise gasométrica do sangue colhido nas cavidades ventriculares. A ausência de um salto oximétrico ao nível do ventrículo direito exclui uma CIV e uma onda “v” elevada nos remete ao diagnós-tico de insuficiência mitral aguda.
A base do tratamento de ambas complicações consiste em trata-mento da insuficiência valvar, revascularização do miocárdio e corre-ção das patologias associadas quando coexistirem. Os determinantes que envolvem a escolha da técnica a ser empregada dependem da experiência do grupo cirúrgico, da acurácia do diagnóstico e das con-dições clínicas apresentadas pelo paciente.
A mortalidade cirúrgica oscila entre 19 a 85% e é maior quando estão associadas outras morbidades como: ruptura de septo, choque cardiogênico e aneurisma (Mesa, 1998).
Aneurisma do ventrículo esquerdoO aneurisma do ventrículo esquerdo (VE) normalmente ocor-
re após um infarto do miocárdio que compromete uma grande massa muscular. A parede comprometida se distende durante a sístole, não acompanha morfologicamente a dinâmica contrátil dos músculos normais, se adelgaça, e passa a não suportar a
tensão intracavitária se distendendo progressivamente duran-te a sístole produzindo um movimento paradoxal, referenciado também como discinético.
O aneurisma de VE ocorre em aproximadamente 7,6% dos pacien-tes portadores de doença coronariana (Cho, 2006), quatro vezes mais na parede anterior e em 12 a 15% dos pacientes que sobrevivem ao IAM (Abrams, 1963).
Dependendo da magnitude do aneurisma, as manifestações mais comuns são: insuficiência cardíaca, embolias e angina. São essas mani-festações que norteiam o tipo de tratamento. As arritmias refratárias ao tratamento clínico ou ablativos constituem outras complicações que po-dem ser abordadas cirurgicamente.
A confirmação diagnóstica é obtida principalmente no estudo he-modinâmico, e a ventriculografia tem sido o método ideal para a sua detecção, seguidos pelo estudo ecocardiográfico (Figura 5). A car-diorressonância magnética tem surgido como um método não inva-sivo muito promissor. Nesses estudos a detecção de elementos da parede ventricular, os movimentos das cavidades permitem identifi-car e diferenciar os aneurismas verdadeiros dos pseudoaneurismas. A presença de gordura adjacente à área discinética exclui, por exem-plo, um possível pseudoaneurisma (Duvenoy, 1992).
O tratamento cirúrgico do aneurisma teve início com Bailey e Likoff (1995), que realizaram a primeira aneurismectomia sem circulação extracorpórea (CEC) utilizando-se um clampeamento e sutura na sua base, excluindo a zona dilatada. Em 1958 Cooley et al. realizaram a primeira correção utilizando a CEC. A técnica consistia de uma sutura longitudinal na base do aneurisma e permaneceu por vários anos co-mo a técnica padrão.
Com o advento de meios mais eficientes de diagnósticos e melhor compreensão da fisiopatologia dessa doença, Jatene (1985) introduziu o conceito da reconstrução geométrica do VE. Posteriormente surgi-ram variantes técnicas que consistiam basicamente na aneurismecto-mia e reconstrução ventricular utilizando-se patches e/ou reduzindo a zona fibrótica com suturas circulares procurando reorganizar a cavida-de de modo a mimetizar as condições normais e ideais de contratilida-de (Jatene, 1985).
Parolari et al. (2007), compararam os resultados do tratamento dos aneurismas utilizando a técnica clássica idealizada com Cooley e a reconstrução geométrica do ventrículo através de um estudo de me-tanálise. Dos 18 grupos analisados, em 11 deles, quando a reconstru-
Figura 5: Aspecto cineangiográfico e cirúrgico de um aneurisma verdadeiro do VE.

66 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 62-68
ção geométrica foi adotada, houve significativa redução da mortalida-de hospitalar. Nos demais grupos não houve diferenças claras entre o reparo linear e a reconstrução geométrica (Figura 6).
PseudoaneurismasA formação do pseudoaneurisma pós-infarto do miocárdio tem si-
do atribuída na maioria das vezes a uma ruptura do miocárdio conti-da por aderências pericárdicas ou epicárdicas (Hung, 1998). A ruptura miocárdica pode estar ainda tamponada por trombos, aderências peri-cárdicas locais preexistentes ou processos inflamatórios secundários que se desenvolvem quando a ruptura inicialmente é pequena (Milgar-ter, 1987). Além do infarto, os pseudoaneurismas podem ocorrer após correção de um aneurisma verdadeiro, após procedimentos valvares, displasias miocárdicas, traumas ou endocardites.
O pericárdio, o coágulo ou ambos organizados, tamponam a ruptura, se organizam e formam um tecido de contenção fibrótico que se expande progressivamente. Tais aneurismas se diferenciam dos verdadeiros por não apresentarem as três camadas da parede muscular e um colo estreito (Cho, 2006).
Usualmente localizam-se na parede inferior ou posterolateral do ventrículo esquerdo (Hung, 1998) pós-infarto do miocárdio, ou outras localizações, tais como: parede atrial (Jutrin, 1979), linhas de suturas, subaórticos ou no sulco atrioventricular após procedi-mentos valvares e localizações adversas pós-traumas.
As manifestações clínicas são semelhantes às dos aneurismas verdadeiros. O surgimento de uma deformidade na silhueta cardí-aca, identificada ao raio X simples de tórax, semanas ou meses após um infarto do miocárdio, chama a atenção para um possível pseudoaneurisma. A presença de um pseudoaneurisma implica em um risco adicional de ruptura espontânea (Antman, 2005) e junta-mente com a patologia de base associada à insuficiência cardíaca são as principais causas de morte (Davidson, 1977; March, 1989; Yeo, 1998).
O exame ecocardiográfico, ressonância magnética ou a ventricu-lografia realizada durante o estudo hemodinâmico são exames que facilmente identificam essa complicação. Usualmente apresentam uma cavidade sacular comunicando-se com a cavidade verdadeira através de um colo estreito, é comum a presença de trombos no seu interior, um fluxo turbilhonar entre as cavidades, descontinuidade das camadas da parede ventricular na base do aneurisma e movimento sistólico paradoxal (Hung, 1998). Gatewood et al. (1980), correlacio-naram a relação entre o diâmetro do colo do aneurisma e o diâmetro máximo interno da cavidade e propuseram que nos pseudoaneuris-mas essa relação deva restar abaixo de 0,5 e nos aneurismas verda-
deiros, entre 0,9 a 1,0 (Figura 5).O tratamento de escolha dos pseudoaneu-
rismas é cirúrgico, e consiste em sua ressecção, reconstrução da parede ventricular e revascula-rização do miocárdio se necessário e reconstru-ção da parede ventricular. A tática cirúrgica pa-ra abordagem dos pseudoaneurismas deve ser cuidadosa devido à fragilidade da estrutura en-volvida na sua formação. Uma vez isolado, o pro-cedimento se assemelha aos utilizados para o tratamento dos aneurismas verdadeiros.
Outras complicaçõesAs dissecções intramiocárdicas entre ventrículos e átrios são
complicações mecânicas raras que surgem geralmente pós-necroses posteroinferiores (Jiménez, 2001). Geralmente um trajeto serpiginoso iniciando-se no ventrículo esquerdo progride através do septo inter-ventricular culminando com trombose ou comunicação com outra ca-vidade.
Apesar das terapias de reperfusão precoce no IAM terem redu-zido substancialmente a mortalidade, a incidência da insuficiência cardíaca tem aumentado (Dor, 2004). Klein (1967) demonstrou que o remodelamento ventricular ocorre irreversivelmente quando há necrose de 20% ou mais de músculo cardíaco.
V. Dor (2004) demonstrou através de estudos com a RM que, após a reperfusão, a região epicárdica do músculo pode ser sal-va e permanecer uma zona endocárdica com necrose, que pode ser bem delimitada através da cardiorressonância com o uso do contraste gadolinium. Essa área assinérgica pode se tornar dis-cinética ou acinética, e para fins prognósticos é mais importante nós quantificarmos o percentual dessa área do que propriamente o tipo de movimento.
A parede muscular, normal inicialmente, se remodela com hiper-trofia e finalmente dilatação, induzidas por um complexo de causas mecânicas, inflamatórias e neurohormonais desencadeados pelos me-canismos compensadores (Packer, 1992). Na série analisada por Dor, quando havia um comprometimento de 50% ou mais da circunferência ventricular, invariavelmente desenvolvia insuficiência cardíaca, poden-do ocorrer em semanas ou anos, de maneira progressiva.
A cirurgia proposta por Dor para correção de áreas discinéticas também se aplica para correção de áreas acinéticas responsáveis pela insuficiência cardíaca. Implica em reduzir a cavidade ventricular com exclusão da área acinética mantendo um volume diastólico final ade-quado, aproximadamente 50 a 60 ml/m2. A revascularização do miocár-dio deve ser realizada sempre que houver isquemia residual. A insu-ficiência mitral quando existente é corrigida e o anel mitral reduzido a 30 mm ou menos do seu diâmetro. Todos os pacientes são submetidos à terapêutica clínica com associações de diuréticos, vasodilatadores, betabloqueadores e inibidores da enzima conversora da angiotensina (ECA). Mais de 80% dos pacientes apresentam um remodelamento reverso com melhora da classe funcional e da fração de ejeção com expectativa de vida em 5 anos de 80%.
Entretanto pacientes com comprometimento hemodinâmico, em classe funcional IV, com fração de ejeção (FE) < 20%, volume diastóli-co final do ventrículo esquerdo (VDFVE) > 100ml/m2, hipertensão pul-
Figura 6: Correção linear de um aneurisma apical após trombectomia.
Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 62-68 - 67
monar devem receber suporte hemodinâmico com BIA ou assistência mecânica, e se possível referendado para transplante cardíaco.
Reyes e colaboradores (2007), reportaram a utilização de dispo-sitivos para assistência mecânica ventricular em 53 pacientes como ponte para o transplante cardíaco, resultando em 23 transplantes, e destes, em cinco a indicação foi falência miocárdica pós-infarto agudo do miocárdio.
O transplante cardíaco é a opção terapêutica mais efetiva para pa-cientes portadores de insuficiência cardíaca terminal. A despeito da escassez de doadores, o choque cardiogênico pós IAM, em casos se-lecionados, pode requerer a assistência mecânica circulatória como ponte para o transplante ou para recuperação miocárdica. A generali-zação da utilização desses dispositivos dependerá do estabelecimento apropriado das indicações, da melhora da relação custo/benefício e redução das taxas de complicações (Bueno, 2006).
CONCLUSÃOConcluímos que a rotura da parede livre do VE, ainda constitui
a mais grave complicação do IAM, e responsável por 16 a 21% dos óbitos em Unidades Coronarianas, sendo a segunda causa mortis mais frequente, superada apenas pelo Choque Cardiogênico. Entre as demais complicações destaca-se a Comunicação Interventricular e a Insuficiência Mitral Aguda, também com índices elevados de mor-talidade e que encontram na precocidade do tratamento cirúrgico seu melhor prognóstico.
REFERÊNCIAS1. Janardhana D, Muralidharan KV, Balasubramanian P, Penumatsa
S, Ponraj PR. Post infarction ventricular septal rupture: repair by endo-ventricular patch platy with infarct exclusion – Vijaya Heart Fundation Technique. Ind J Thorac Cardiovasc Surg. 2004; 20: 168-72.
2. Latham PM. Lectures on Subjects Connected With Clinical Me-dicine Comprising Disease of Heart. London: Longman Rees, Vol 2. p.168-85.
3. Kirklin JW, Barratt-Boyes BG, (Eds.) Cardiac surgery: postinfarc-tion ventricular septal defect. New York: Churchill Livingstone; 1993: 403-13.
4. Balkanay B, Eren E, Keles C, Toker ME, Guler M. Double-Patch repair of postinfarction ventricular septal defect. Tex Heart Inst J. 2005; 32: 43-6.
5. Villavicencio M, Garayar B, Irarrázavel MJ, et al. Cirurgía coroná-ria en el infarto de miocárdio de menos de 24 horas de evolución. Rev Esp Cardiol. 2002; 55(2): 135.
6. David TE, Dale L, Sun Z. Post infarction ventricular septal rupture: repair by endocardial patch with infarct exclusion. J Thorac Cardiovasc Surg. 1995; 110: 1315-22.
7. Elsner M, Zeiher AM. Perforation and rupture of coronary arte-ries. Herz 1998; 23: 311.
8. Marti V, Castaño C, Guiteras P, et al. Perforación coronária com-plicada com tamponamiento cardíaco sellada mediante coils metálicos. Rev Esp Cardiol. 2004; 57(10): 990.
9. Crenshaw BS, Granger CB, Birnbaum Y, et al. Risk factors, an-giographic patterns, and outcomes in patients with ventricular sep-tal defect complicating acute myocardial infarction. Circulation. 2000; 101: 27-32.
10. Robert C. King, MD, Edward D. Verrier, MD. Advanced Therapy in Cardiac Surgery in Postinfarction Ventricular Septal Defect Repair. London: BC Decker : Atheneu; 2003. Chapter 9, p. 83-7.
11. Birnbaum Y, Fishbein MC, Blanche C, Siegel RJ. Ventricular septal rupture after acute myocardial infarction. N Engl J Med. 2002; 347: 1426-32.
12. Cummings RG, Califf R, Jones RN, Reimer KA, Kong Y-H, Lowe JE. Correlates of survival in patients with postinfarction ventricular sep-tal defect. Ann Thorac Surg. 989; 47: 824–30.
13. Dallan LA, Oliveira AS, Ramires JAF, Sabino Neto A, Verginelli G, Jatene AD. Tratamento cirúrgico da comunicação interventricular pós-infarto agudo do miocárdio: conduta atual. Rev Bras Cir Cardio-vasc. 1989; 4: 64-74.
14. Skillington PD, Lamb RD, Monro JL, et al. Surgical treatment of infarct related ventricular septal defects: improved early results combi-ned with analysis of late functional status. J Thorac Cardiovasc Surg 1990; 99: 798-808.
15. Muehrcke DD, Daggett WM, Buckley MJ, et al. Postinfarct ventri-cular septal defect repair: effect of coronary artery bypass grafting. Ann Thorac Surg.1992; 54: 876–83.
16. Komeda M, Fremes SE, David TE. Surgical repair of postinfarc-tion ventricular septal defect. Circulation. 1990; 82 Suppl IV: IV243–7.
17. Labrousse L, Choukroun JM, Chevalier F, et al. Surgery for post-infarction ventricular septal defect (VSD): risk factors for hospital death and long-term results. Eur J Cardiothorac Surg. 2002; 21: 725–32.
18. Piwnica A, Menasche P, Beaufils P, et al. Long-term results of emergency surgery for postinfarction ventricular septal defect. Ann Tho-rac Surg. 1987; 44: 274–6.
19. Daggett WM. Surgical technique for early repair of posterior ventricular septal rupture. J Thorac Cardiovasc Surg. 1982; 84: 306-12.
20. Jiménez J, Almeria C, Zamorano JL, et al. Disección intramio-cárdica postinfarto de la parede posterior del ventrículo izquierdo con comunicación con el seno coronário. Rev Esp Cardiol. 2001; 54: 247.
21. Vera TR, Albertí JFF, Palomeque CF, et al. Rotura espontánea de musculo papilar con coronárias angiograficamente normales. Rev Esp Cardiol. 2001; 54: 1010-12.
22. Varvarigos N, Koletsis E, Zafiropoulos A, et al. A case of left ventricular pseudoaneurysm with long survival and congestive heart failure as first presentation . Case report and review of the literature. Med Sci Monit. 2005; 11 (11): csa69-73.
23. Becker RC, Gore JM, Lambrew C, et al: A composite view of cardiac rupture in the Unite States National Registry of Myocardial In-farction. J Am Coll Cardiol.1996; 27:1 321-26.
24. Cordero A, Artaiz M, Calabuig J. Rotura de la parede libre del ventriculo izquierdo tras reperfusión coronária percutánea de un infarto de miocárdio evolucionado. Rev Esp Cardiol. 2006; 59 (1): 82-3.
25. Roberts JT, Wearn Jt. Quantitative changes in the capillary mus-cle relationship in human hearts during normal growth and hypertrophy. Am Heart J. 1941; 21: 617-33.
26. Arosemana E, Moller JH, Edwards JE. Scarring of the papilla-ry muscles in left ventricular hypertrophy. Am Heart J. 1967;74:446-52.
27. Barbour DJ, Roberts WC. Rupture of left ventricular papillary muscle during acute myocardial infarction: analysis of 22 necropsy pa-tients. J Am Coll Cardiol. 1986; 8: 558-65.
28. D`Ancona G, Mamone G, et al. Ischemic mitral valve regurgita-

68 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 62-68
tion: the new challenge for magnetic resonance imaging. Eur J Cardio-thorac Surg. 2007; 32: 475-80.
29. Mesa JM, Aroca A, Ramirez U, et al. Cirurgia de las compli-caciones mecanicas del infarto agudo de miocárdio. Rev Esp Cardiol. 1998; 51(3): 71-9.
30. Cho MN, Metha SK, Matulevicius S, et al. Differentiating true versus pseudo left ventricular aneurysm: a case report and review of diagnostic strategies. Cardiol Review. 2006; 14: e27-e30.
31. Abrams DL, Edelist A, Luria MH, et al. Ventricular aneurysm: a reappraisal on a study of 65 consecutive autopsied cases. Circulation. 1963; 27: 164.
32. Duvenoy O, Wikstrom G, Mannting, et al. Pre- and postoperative CT and RM in pseudoaneurysms of the heart. J Comp Assist Tomogr. 1992; 16: 401-9.
33. Likoff W, Bailey CP. Ventriculoplasty: excision myocardial aneu-rysm: report of a successful case. JAMA .1955; 158: 915-20.
34. Jatene AD. Left ventricular aneurysmectomy: resection or re-construction. J Thorac Cardiovasc Surg. 1985; 89: 331.
35. Parolari A, Nliato M, Loardi C, et al. Surgery of left aneurysm: a meta-analysis of early outcomes following different reconstruction tech-niques. Ann Thorac Surg. 2007; 83: 2009-16.
36. Hung MJ, Wang CH, Cherng WJ. Unruptured left ventricular pseudoaneurysm following myocardial infarction. Heart .1998; 80: 94-7.
37. Milgarter E, Uretzky G, Levy P, et al: Pseudoaneurysm of the left ventricle. Thorac Cardiovasc Surg.1987; 35: 20-5.
38. Jutrin I, DiSegni E, Krabel G. False aneurysm of the right atrium. Chest. 1979; 75: 629.
39. Antman EM. ST-elevation myocardial infarction. In: Zipes ,et al.
(Eds). Braunwalds Heart Disease: a textbook of cardiovascular medici-ne. 7. ed. Philadelphia: Elsevier Saunders; 2005. p.1167-1226.
40. Davidson KH, Parisi AF, Harrington JJ, et al. Pseudoaneurysm of the left ventricule: an unusual echocardiographic presentation: re-view of the literature. Ann Intern Med .1977; 86: 430.
41. March KL, Sawada SG, Tarver RD, et al: Current concepts of left ventricular pseudoaneurysm: pathophysiology, therapy and diagnostic imaging methods. Clin Cardiol. 1989; 12: 531-40.
42. Yeo TG, Malouf JF, Oh JK, et al. Clinical profile and outcome in 52 patients with cardiac pseudoaneurysm. Ann Intern Med. 1998; 128: 299-305.
43. Gatewood RP, Nanda NC. Differentiation of left ventricular pseu-doaneurysm from true aneurysm with two dimensional echocardiogra-phy. Am J Cardiol. 1980; 46: 869-78.
44. Dor V, Sabatier M, Montiglio F, et al. Endoventricular patch re-construction of ischemic failing ventricle: a single center with 20 years experience. Advantages of magnetic resonance imaging assessment. Heart Failure Review. 2004; 9: 269-86.
45. Klein MD, Herman MV, Gorlin R. A hemodynamic study of left ventricular aneurysm. Circulation. 1967; 35: 614-30.
46. Packer M. The neurohormonal hypothesis: a theory to explain the mechanism of disease progression in heart failure. J Am Coll Car-diol. 1992; 20: 248-54.
47. Reyes G, Yáñez JF, Abella HR, et al: Asistencia ventricular me-cánica como puente al trasplante. Rev Esp Cardiol. 2007; 60 (1): 72-5.
48. Bueno MG, Cubero JS, Rivera LAP. Asistencia mecánica circu-latoria y trasplante cardíaco. Indicaciones y situación en España.Rev Esp Cardiol. 2006; 6 Supl.: 82F-94F.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75 - 69
ABSTRACTIt has been observed that the rate of mechanical complications has decreased after the advent of the thrombolytic therapies and the rescue
angioplasty for treating acute myocardial infarcion. However, they still still have a significant mortality rate. In this retrospective study, the authors describe their forms of presentation, rates of occurrence and the main surgical techniques employed to correct these complications.
Keywords: acute myocardial infarction/complications; acute myocardial infarction/surgical treatment.
SURGICAL TREATMENT OF MECHANICAL COMPLICATIONS OF ACUTE MYOCARDIAL INFARTION
AUTHORS:CMG (Md-RM1) HERMES DE SOUZA FELIPPEBachelor’s Degree in Medicine from the Santa Casa de Misericórdia de Vitória.Medical Residency Training in Cardiac Surgery at Incor.Specialist in Cardiac Surgery from the Brazilian Society of Cardiovascular Surgery.Chief of the Cardiac Surgery Clinic at HNMD.
CT (Md) MARCOS FLORIPES DA SILVABachelor’s Degree in Medicine from the Faculdade de Medicina de Valença.Medical Residency Training in General Surgery at HNMD.Medical Residency Training in Thoracic Surgery at HNMD.Specialist in Cardiac Surgery from Incor.Assistant Doctor at the Cardiac Surgery Clinic of HNMD.
EDUARDO SÉRGIO BASTOS, M.D., Ph.D.Bachelor’s Degree in Medicine from the Universidade Federal de Sergipe.Medical Residency Training in Cardiac Surgery at the Hospital dos Servidores do Estado do Rio de Janeiro.Master’s Degree in Cardiac Surgery from UFRJ.Doctor’s Degree in Cardiac Surgery from UFRJ.Associate Professor of Cardiac Surgery at the School of Medicine of UFRJ.Active Member of the Brazilian Society of Cardiovascular Surgery. Cardiac Surgeon at HNMD.
INTRODUCTIONDespite the development and improvement of more effective
propaedeutic methods, the incidence of complications and mortality associated with Acute Myocardial Infarction (AMI) is still considerably high.
Early reperfusion therapies in the AMI have reduced complications, the area of necrosis and mortality related to infarction. The control of ventricular remodeling has improved patients’ quality of life. Despite all the available resources, some patients still have an adverse reaction to the therapy employed and can have severe complications, such as: left ventricular free wall rupture, papillary muscle rupture or dysfunction with severe mitral regurgitation, ventricular septal defect, ventricular pseudoaneurysms and aneurysms, cardiogenic shock, electrical complications and heart failure. In this article we will discuss the mechanical complications of AMI.
Due to these complications emergency interventions are needed to reestablish ventricular functional dynamics in order to maintain hemodynamic balance.
DEVELOPMENTVSD post-AMI
A Ventricular Septal Defect after an AMI (VSD post-AMI) is an extremely severe complication with high morbidity and mortality rates. One third of the patients who die due to infarction complications
have ventricular wall rupture. The majority of the ruptures occur in the left ventricular free wall, and only 15 to 20% are located in the interventricular septum (Janardhana, 2004).
The first description of a ventricular septal defect after an acute myocardial infarction was reported by Latham in 1845. The diagnosis during life was first made by Brunn in 1923 (Kirklin, 1993). In 1934, Sagar associated this complication with coronary diseases (Balkanay, 2005).
The incidence of ventricular septal defect after an acute myocardial infarction varies from 1 to 3 % of all myocardial infarctions (Villavicencio, 2002). It occurs between the first and the nineteenth day following an AMI, more frequently between the third and the forth days (David, 1995). The GUSTO-1 (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) study showed that with the use of thrombolytic therapies this incidence has reduced to 0.2%. It further showed that the defect occurs mostly during the first 24 hours (Elsner, 1998).
The rate of mortality for VSD post-AMI is about 24% in the first 24 hours, 60% in the first week, and only 10% of the patients survive the first three months (Marti, 2004).
In 2000, Crenshaw and coworkers published a retrospective analysis of 84 patients with VSD post-AMI included in the GUSTO-I study (Crenshaw, 2000). The study observed 41,021 patients with AMI submitted to thrombolysis. A confirmed VSD post-AMI occurred in 0.2% of the patients; 94% of the cases were diagnosed in the first week.

70 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75
Figure 1: A 73 year-old female patient with a single lesion in the anterior descending artery and VSD post-AMI.
Mortality is mainly influenced by infarction size, VSD location and early diagnosis of the defect (Robert, 2003). Various predictors have been suggested as risk factors for VSD, including: hypertension, old people, women and absence of AMI or previous angina. Patients with angina or previous history of AMI have more side effects and are more susceptible to preconditioning, which could explain the lower rate of septal rupture in these patients (Birnbaum, 2002).
From the standpoint of its location, the majority of the cases involve the anteroapical region (60%) and the others, the postero-septal region. The occlusion of the anterior interventricular artery is related to the origin of the antero-apical VSD, and the postero-basal defects are related to the occlusion of the right coronary or the circumflex artery when dominant.
Cummings et al. (1989) have evaluated 42 consecutive patients with VSD post-AMI. Their findings agree with the results found by several other authors: 57% of the patients presented with anterior AMI, 33% with inferior AMI and 10% were considered a combination of both.
It can be a single-vessel coronary disease, mostly occurring in patients with poor collateral circulation (Figure 1). In the GUSTO-I study, the total occlusion of an artery was present in 57% of the patients with VSD post-AMI, and in only 18% of the ones with AMI without VSD (Crenshaw, 2000).
This complication is basically treated by a surgical procedure. Clinical measures should be initially adopted as, for example, the insertion of an intra-aortic balloon pump (IABP), pressure support with inotropic drugs, hemodynamic optimization and referring the patient to surgery. The surgery should be performed as soon as possible and the use of a preoperative trans-esophageal echocardiogram should be considered.
The majority of the authors recommend the use of IABP in patients with low cardiac output signs or in the event of patient’s clinical deterioration. The mortality rate of patients who undergo surgery while in cardiogenic shock is up to 66.6% (Dallan, 1989).
There is not a consensus of the need of performing a coronary angiography study in severe patients in cardiogenic shock. Some authors believe that patients with VSD post-AMI in cardiogenic shock do not need to undergo an angiography (Skillington, 1990). In accordance with Muehrcke et al. (1992), a myocardial revascularization during a VSD repair surgery does not affect immediate mortality rate (Muehrcke, 1992). On the other hand, however, there are conflicting studies concerning the long-range prognosis (Komeda, 1990; Labrousse, 2002). Coronary angiography and, if necessary, myocardial revascularization is recommended for patients with VSD post-infarction scheduled for surgery (Robert, 2003).
The first surgery to repair a post-infarction septal defect was conducted by Cooley in 1957, and the first one in which the patient survived was performed by Payne at the Mayo Clinic in 1963 (Robert, 2003).
Since the 1970s, the advances in cardiac surgery and in diagnostic methods have made it possible to better understand the pathophysiology of this complication. Thus, various techniques for its repair have been developed and improved.
Mortality rate is significantly lower in patients submitted to surgical treatment when compared to clinical treatment, 47% and 94% (Crenshaw, 2000), respectively.
The surgery aims essentially the repair of a ventricular septal defect by using patches (Dacron®, autologous pericardium, bovine pericardium, polytetra-fluoroethylene – PTFE) (David, 1995; Piwnica, 1987; Janardhana, 2004) as well as the reestablishment or maintainance
of ventricular geometry and myocardial revascularization if indicated.In 1970, in an attempt to develop the basic surgical principles for
the repair of VSD after an AMI, in 1970, Daggett (1982) described the guidelines for this type of surgery at that time. It consisted in delaying the repair beyond six weeks from the time the patient experiences VSD. At that time, infarctectomy and ventricular wall restoration were performed.
Since the results showed that many patients did not survive the waiting time, this period of time was initially reduced to three weeks (Piwnica, 1987). But even so time remained an important factor in the natural selection. It was agreed that changes needed to be made. These changes led to the current recommendation which advocates the immediate intervention for better results. Surgery should only be postponed in selected cases of patients with small defects, with reduced functional impairment.
The major problem of the VSD repair in the acute stage is the friability of the muscular tissue adjacent to the damaged area, resulting from the necrosis and the ischemia of the region with unpredictable extension, within the concept of the disease evolution.
It is a thin and necrotic septum, with muscle fragments in the margins of the defect, secondary to regional disintegration (Figure 2). The VSD ranges in size from millimeters to several centimeters, as well as in form and location. There could be one defect or multiple defects, which could not develop at the same time (Kirklin, 1993). The echocardiography test can detect any diameter and flow alterations through the defect.
Figure 2 : Septal necrosis with a recent VSD.
The septal rupture can be at the same level in relation to both the Left Ventricle (LV) and Right Ventricle (RV) septal endocardium, i.e., rectilinearly, and in this case, it is known as a simple VSD post-AMI, or whether with a tortuous course meandering through the necrotic septal tissue of the inter-ventricular septum, known as a complex VSD post-AMI. 20 About 70% of the inferior VSDs are of the complex type, with a

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75 - 71
Figure 3: Antero-septal AMI with a VSD approach via ventriculostomy through the infarcted area.
tortuous course through the necrotic myocardium Robert, 2003).The conventional surgical procedure consisted mostly in
infarctectomy and septal and/or ventricular wall repair with one or more patches (Daggett, 1982). The operative mortality rate was high, ranging from 35 to 50%.
The repair of a chronic VSD infers the same approach, but in this case the margins of the VSD are more delimited and fibrotic, enabling more consistency and stability to the sutures. Patients with this condition would most probably show a small VSD with L-R shunt lower than 1:1.5 with little clinical repercussion.
In 1989 in Brazil, Da Silva et al. (Piwnica, 1987) employed a technique to repair VSD in which no part of the infarcted septum or muscle was excised. This technique involves making an incision in the infarcted area, inserting a Dacron® patch in the ventricular cavity, covering the infarcted area adjacent to the VSD (Figures 3 and 4). The ventricular wall suture is reinforced with a second patch and hemostasis is accomplished. Seven patients were submitted to this technique and only one terminal patient died. Two patients had small residual VSDs without clinical repercussion.
In 1990, Komeda et al. registered the technique, which they called the “infarct exclusion method” (Komeda, 1990). In 1995, David et al. (1995) spread the technique with the use of a bovine pericardium patch, excluding in the same way the VSD and the infarcted tissue. The method consisted in placing the patch on the infarcted area, including the VSD, suturing it into the healthy endocardium across the defect, extending to the lateral and anterior aspects, holding up the flap, through ventriculostomy.
Figure 4: Exclusion of VSD with bovine pericardium and suture final aspect of the ventricular wall with stitches over two strips of Teflon®.
If the defect is more apical or the procedure demands a large flap, it should be placed in a manner to geometrically reshape the LV. In maintaining its geometric shape, the functional apical cone is preserved, bringing more contractile efficacy to the LV (Vera, 2001).
Currently, the most common approach for VSD is through the infarcted area. Other approaches include the right atrial (Varvarigos, 2005) which is used in selected cases of small tardive basal VSDs and the use of umbrellas through an endovascular procedure. In some cases, the small and apical VSDs can be closed by the direct plication of the ventricular walls, comprising the defect without the use of extracorporeal circulation (ECC).
Ventricular free wall ruptureThe ventricular free wall rupture is one of the most catastrophic
complications of myocardial infarction. The incidence rate of this complication is about 7% of all patients who die due to an acute myocardial infarction (Becker, 1996). It occurs mostly within the first 24 hours after the event and progressively decreases, becoming less frequent after the fifth day (Cordero, 2006).
The most common clinical manifestation is an acute cardiac tamponade with hemopericardium, leading to cardiocirculatory collapse and death. Most of the times the diagnosis is made post-mortem, and in rare situations surgical intervention can be performed.
Cordero et al. (2006) reported a case in which the rupture occurred immediately after the angioplasty procedure performed in the fifth day of an inferior wall AMI. They inferred that it was caused by reperfusion, once the majority of the ruptures that occur are due to late reperfusion.
Emergency Clinical treatment should be performed and the patient should be immediately submitted to surgery. Pericardiocentesis is a palliative procedure to provide relief of symptoms, and surgical treatment should be considered as an emergency procedure, aiming mainly to repair wall laceration, using stitches to approximate the wound margins on strips of Teflon®, once the region became friable due to necrosis and almost always it is surrounded by hemorrhagic suffusion or hematoma.
When the defect occurs in patients previously studied, supplementary procedures, such as myocardial revascularization or other defect repair, when coexisting, should be performed to facilitate patient’s recovery.
Papillary muscle rupture or dysfunctionMost of the papillary muscle ruptures occur due to AMI or trauma.
A spontaneous rupture is rare and occurs mostly in patients with left ventricular hypertrophy or those who are hypertensive (Vera, 2001). It is believed that hypertrophy – due to a lower concentration of capillaries and a higher level of fibrosis in the hypertrophic myocardium (Roberts, 1941) or even due to an increase of myocardial mass – causes more resistance to perfusion (Arosemana, 1967). Barbour et al. (1986) raised the hypothesis that the rupture would be secondary to the transitory necrosis in an artery not identified by the coronary angiography, responsible for the irrigation of the papillary muscle.
The posteromedial papillary muscle is most frequently affected. Its rupture causes a displacement of both mitral valve cusps with significant insufficiency. Only 25% of the patients survive after the first 24 hours (Vera, 2001).

72 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75
Figure 6: Linear repair of an apical aneurysm after thrombectomy.
Figure 5: Cineangiographic and surgical aspect of a true LV aneurysm.
Patients’ clinical status depends on the significance of mitral regurgitation, which in most of the times is severe, clinically represented by pulmonary edema and arterial hypotension. A heart murmur, usually diagnosed three to ten days after an AMI, suggests a mechanical complication, such as the papillary muscle rupture or dysfunction. The papillary muscle rupture evolves with a rapid deterioration of the patient’s condition, and hemodynamic measures should be promptly taken in order to submit the patient as soon as possible to surgery.
The papillary muscle ischemia which leads to valve regurgitation results also in a significant morbidity and mortality rate directly proportional to the degree of the insufficiency and the rate of its onset.
The echocardiography test is considered the ‘golden standard’ for structural assessment of the valve. It defines the diagnosis, differentiates dysfunction from rupture and identifies the coexistence of other complications. It further provides reasonably accurate information about the procedure to be performed: a valvuloplasty or a valve replacement.
New technologies, such as the Magnetic Resonance (MR), can help this investigation and some services have associated it to an investigation method (D’Ancona, 2007) with increasingly progressive details of the functioning of the ventricular and valve apparatus.
Patients undergoing hemodynamic monitoring can benefit from the gasometric analysis of the blood collected in the ventricular cavities. The absence of oxymetry pulse at the level of the right ventricle exclude a VSD, and a high ‘v’ wave leads us to the diagnosis of acute mitral regurgitation.
The treatment of both complications consists basically of valve regurgitation treatment, myocardium revascularization and repair of related pathologies, when coexisting. The type of technique to be performed depends on the experience of the surgical team, the accuracy of the diagnosis and the patient’s clinical status.
The operative mortality rate ranges from 19 to 85%, and in association with other morbidities, such as septal defect, cardiogenic shock and aneurysm, it increases (Mesa, 1998).
Left ventricular aneurysm The Left Ventricular (LV) aneurysm usually occurs
after a myocardium infarction that affects a large muscle mass. The affected wall expands during systole. It does not morphologically follow the contraction dynamics of the normal muscles, becomes thinner and does not sustain the progressively expanding intracavitary pressure, producing a paradoxal movement, also Known as dyskinetic movement.
The LV aneurysm occurs in approximately 7.6% of the patients with coronary disease (Cho, 2006). It occurs four times more in the anterior wall and in 12 to 15% of the patients who survive an AMI (Abrams, 1963).
Depending on the severity of the aneurysm, the most common manifestations are as follows: heart failure, embolisms and angina. They are taken into account before choosing the treatment. Other complications that may require a surgical approach are refractory arrhythmias due to clinical or ablative treatments.
The diagnosis is usually confirmed by the hemodynamic study.
Ventriculography has been suggested to be the ideal method for the detection of an aneurysm, followed by the echocardiographic study (Figure 5). The cardiac magnetic resonance has been considered to be a promising non-invasive method. The detection of elements of the ventricular wall and cavity movements through these studies make it possible to identify and differentiate true aneurysms from pseudoaneurysms. The presence of fat adjacent to the dyskinetic area excludes, for example, a possible pseudoaneurysm (Duvenoy, 1992).
The first surgical treatment of aneurysms was reported by Bailey and Likoff (1995). They performed the first aneurysmectomy without extracorporeal circulation (ECC), using clamp and suture at its base, excluding the dilated area. Cooley et al. performed the first repair method via ECC in 1958. The technique consisted in a longitudinal suture in the base of the aneurysm. This has been considered the standard technique for several years.
With the advent of more effective diagnosis methods and better understanding of the pathophysiology of this disease, Jatene (1985) introduced the concept of LV geometry restoration. Since then, several techniques have been developed, consisting basically of aneurysmectomy and ventricular restoration by using patches and/or reducing the fibrotic area with circular sutures in order to remodel the cavity so as to reproduce the normal and ideal contractility conditions (Jatene, 1985).
Parolari et al. (2007) compared the results of the treatment of aneurysm using the classical technique developed with Cooley and the ventricular geometry restoration by a meta-analysis study. Eleven of the 18 groups analyzed showed significant reduction of in-hospital mortality rate when the geometric restoration procedure was adopted. No clear differences were seen between the linear repair and the geometric restoration in the other groups (Figure 6).

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75 - 73
PseudoaneurysmsThe formation of a pseudoaneurysm after a myocardium infarction
has been mostly attributed to a myocardial defect contained by pericardial or epicardial adhesions (Hung, 1998). A myocardial defect can further occurs due to thrombi, preexisting local pericardial adhesions or secondary inflammatory processes developed when the defect is still small (Milgarter, 1987). In addition to infarction, pseudoaneurysms can occur after a true aneurysm repair, after valve procedures, myocardial dysplasias, traumas or endocarditis.
The pericardium, the clot or a combination of both occlude the defect, organize themselves and form a fibrotic containment tissue which expands in a progressive manner. These aneurysms differ from the true ones due to the lack of the three muscle wall layers and a narrow neck (Cho, 2006).
Pseudoaneurysms are usually located in the inferior or posterolateral wall of the left ventricle (Hung, 1998) after a myocardial infarction, or in other locations – such as in the atrial wall (Jutrin, 1979) suture lines, below the aortic valve or in the atrioventricular sulcus after valve procedures – and in post-trauma adverse locations.
Their clinical manifestations are similar to those of the true aneurysms. An abnormal cardiac silhouette, identified by a simple thorax X-ray, weeks or months after a myocardial infarction, suggests a probable pseudoaneurysm. A pseudoaneurysm involves an additional risk of spontaneous rupture (Antman, 2005) which together with the basic pathology associated to heart failure are the main causes of death (Davidson, 1977; March, 1989; Yeo, 1998).
This complication can be easily detected by an echocardiography, a magnetic resonance or a ventriculography performed during the hemodynamic study. Pseudoaneurysms usually have a saccular cavity which communicates with the true cavity through a narrow neck. The presence of thrombi, a turbulent flow between the cavities and discontinuity of the ventricular wall layers in the base of the aneurysm, as well as a paradoxal systolic movement are common (Hung, 1998). Gatewood et al. (1980) correlated the relationship between the diameter of the neck of the aneurysm and the maximum internal diameter of the cavity and suggested the following values: less than 0.5 in the pseudoaneurysms, and between 0.9 and 1.0 in the true aneurysms (Figure 5).
Surgery is the first choice treatment of pseudoaneurysms. It consists of its resection, restoration of the ventricular wall and myocardial revascularization if necessary. Particular attention should be paid to the surgical tactics adopted in the treatment of pseudoaneurysms due to the fragility of the structure involved in its formation. Once isolated, the procedure is similar to those used to treat true aneurysms.
Other complicationsIntramyocardial dissections between ventricles and atriums are not
frequent mechanical complications, which usually occur after postero-inferior necroses (Jiménez, 2001). In general, a tortuous course, beginning in the left ventricle extends through the inter-ventricular septum, culminating in thrombosis or communication with other cavity.
Despite the fact that early reperfusion therapies in AMI have reduced significantly mortality, the incidence of heart failure has
increased (Dor, 2004). Klein (1967) demonstrated that when at least 20% of the heart muscle necroses, the ventricular remodeling is irreversible.
V. Dor (2004) has demonstrated through MR studies that, after reperfusion, the muscle epicardial region can be saved and can remain an endocardial area with necrosis, which can be well-defined through cardiovascular magnetic resonance by using a gadolinium contrast agent. This asynergic area can become a dyscinetic or an akinetic area. For prognostic purposes, it is more important to quantify the percentage of this area than to specify the type of movement itself.
The initially normal muscle wall is remodeled with hypertrophy and finally dilatation, induced by a series of mechanical, inflammatory and neuro-hormonal causes resulting from compensatory mechanisms (Packer, 1992). The series analyzed by Dor has showed that heart failure invariably occurs when at least 50% of the ventricular circumference are affected. It can occur in weeks or years, in a progressive manner.
The surgery developed by Dor to repair dyscinetic areas is also applied to repair akinetic areas responsible for heart failure. It involves the reduction of the ventricular cavity with the exclusion of the akinetic area and maintenance of an adequate final diastolic volume, about 50 to 60ml/m2. Myocardial revascularization should be always performed if a residual ischemia occurs. Mitral regurgitation, if occurs, is repaired and the mitral ring is reduced up to 30 mm of its diameter. All patients are submitted to clinical therapies combined with diuretics, vasodilators, beta blockers and ACE inhibitors. More than 80% of the patients show a reverse remodeling with improvement in functional class and in ejection fraction, with expected survive rate of 80% in 5 years.
However, patients with hemodynamic instability, in Functional Class IV, with EF < 20%, LVFDV > 100ml/m2, and pulmonary hypertension should receive hemodynamic support with IABP or mechanical assistance and, if possible, referred to heart transplant.
Reyes et al. (2007) reported the use of devices for ventricular mechanical assistance in 53 patients as a bridge for heart transplant, resulting in 23 transplants, of which five were performed due to myocardial failure after an acute infarction.
Heart transplant is the more effective therapeutic technique for patients with terminal heart failure. Despite the scarce number of potential donors, cardiogenic shock after AMI can request, in selected cases, a circulatory mechanical assistance as a bridge for the transplant or for myocardial recovery. The generalization of the use of these devices will depend on the appropriate indications for their use, the best balance between cost and benefit, as well as the decrease of complication rates (Bueno, 2006).
CONCLUSIONWe conclude that the left ventricular free wall rupture is still
the most severe complication of AMI, responsible for 16 to 21% of in-hospital coronary deaths. It is the second most frequent cause of death surpassed only by cardiogenic shock. Among other complications, we highlight septal defect and acute mitral regurgitation, which also show high rates of mortality. An early surgery is the approach with the best prognosis.
74 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75
REFERENCES1. Janardhana D, Muralidharan KV, Balasubramanian P, Penumatsa
S, Ponraj PR. Post infarction ventricular septal rupture: repair by endoventricular patch platy with infarct exclusion – Vijaya Heart Fundation Technique. Ind J Thorac Cardiovasc Surg. 2004; 20: 168-72.
2. Latham PM. Lectures on Subjects Connected With Clinical Medicine Comprising Disease of Heart. London: Longman Rees, Vol 2. p.168-85.
3. Kirklin JW, Barratt-Boyes BG, (Eds.) Cardiac surgery: postinfarction ventricular septal defect. New York: Churchill Livingstone;1993: 403-13.
4. Balkanay B, Eren E, Keles C, Toker ME, Guler M. Double-Patch repair of postinfarction ventricular septal defect. Tex Heart Inst J. 2005; 32: 43-6.
5. Villavicencio M, Garayar B, Irarrázavel MJ, et al. Cirurgía coronária en el infarto de miocárdio de menos de 24 horas de evolución. Rev Esp Cardiol. 2002; 55(2): 135.
6. David TE, Dale L, Sun Z. Post infarction ventricular septal rupture: repair by endocardial patch with infarct exclusion. J Thorac Cardiovasc Surg. 1995; 110: 1315-22.
7. Elsner M, Zeiher AM. Perforation and rupture of coronary arteries. Herz 1998; 23: 311.
8. Marti V, Castaño C, Guiteras P, et al. Perforación coronária complicada com tamponamiento cardíaco sellada mediante coils metálicos. Rev Esp Cardiol. 2004; 57(10): 990.
9. Crenshaw BS, Granger CB, Birnbaum Y, et al. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. Circulation. 2000; 101: 27-32.
10. Robert C. King, MD, Edward D. Verrier, MD. Advanced Therapy in Cardiac Surgery in Postinfarction Ventricular Septal Defect Repair. London: BC Decker : Atheneu; 2003. Chapter 9, p. 83-7.
11. Birnbaum Y, Fishbein MC, Blanche C, Siegel RJ. Ventricular septal rupture after acute myocardial infarction. N Engl J Med. 2002; 347: 1426-32.
12. Cummings RG, Califf R, Jones RN, Reimer KA, Kong Y-H, Lowe JE. Correlates of survival in patients with postinfarction ventricular septal defect. Ann Thorac Surg. 1989; 47: 824–30.
13. Dallan LA, Oliveira AS, Ramires JAF, Sabino Neto A, Verginelli G, Jatene AD. Tratamento cirúrgico da comunicação interventricular pós-infarto agudo do miocárdio: conduta atual. Rev Bras Cir Cardiovasc. 1989; 4: 64-74.
14. Skillington PD, Lamb RD, Monro JL, et al. Surgical treatment of infarct related ventricular septal defects: improved early results combined with analysis of late functional status. J Thorac Cardiovasc Surg 1990; 99: 798-808.
15. Muehrcke DD, Daggett WM, Buckley MJ, et al. Postinfarct ventricular septal defect repair: effect of coronary artery bypass grafting. Ann Thorac Surg.1992; 54: 876–83.
16. Komeda M, Fremes SE, David TE. Surgical repair of postinfarction ventricular septal defect. Circulation. 1990; 82 Suppl IV: IV243–7.
17. Labrousse L, Choukroun JM, Chevalier F, et al. Surgery for post-infarction ventricular septal defect (VSD): risk factors for hospital death and long-term results. Eur J Cardiothorac Surg. 2002; 21: 725–32.
18. Piwnica A, Menasche P, Beaufils P, et al. Long-term results
of emergency surgery for postinfarction ventricular septal defect. Ann Thorac Surg. 1987;4 4: 274–6.
19. Daggett WM. Surgical technique for early repair of posterior ventricular septal rupture. J Thorac Cardiovasc Surg. 1982; 84: 306-12.
20. Jiménez J, Almeria C, Zamorano JL, et al. Disección intramiocárdica postinfarto de la parede posterior del ventrículo izquierdo con comunicación con el seno coronário. Rev Esp Cardiol. 2001; 54: 247.
21. Vera TR, Albertí JFF, Palomeque CF, et al. Rotura espontánea de musculo papilar con coronárias angiograficamente normales. Rev Esp Cardiol. 2001; 54: 1010-12.
22. Varvarigos N, Koletsis E, Zafiropoulos A, et al. A case of left ventricular pseudoaneurysm with long survival and congestive heart failure as first presentation . Case report and review of the literature. Med Sci Monit. 2005; 11(11): csa69-73.
23. Becker RC, Gore JM, Lambrew C, et al: A composite view of cardiac rupture in the Unite States National Registry of Myocardial Infarction. J Am Coll Cardiol.1996; 27: 1321-26.
24. Cordero A, Artaiz M, Calabuig J. Rotura de la parede libre del ventriculo izquierdo tras reperfusión coronária percutánea de un infarto de miocárdio evolucionado. Rev Esp Cardiol. 2006; 59(1): 82-3.
25. Roberts JT, Wearn Jt. Quantitative changes in the capillary muscle relationship in human hearts during normal growth and hypertrophy. Am Heart J. 1941; 21: 617-33.
26. Arosemana E, Moller JH, Edwards JE. Scarring of the papillary muscles in left ventricular hypertrophy. Am Heart J. 1967; 74: 446-52.
27. Barbour DJ, Roberts WC. Rupture of left ventricular papillary muscle during acute myocardial infarction: analysis of 22 necropsy patients. J Am Coll Cardiol. 1986; 8: 558-65.
28. D`Ancona G, Mamone G, et al. Ischemic mitral valve regurgitation: the new challenge for magnetic resonance imaging. Eur J Cardiothorac Surg. 2007; 32: 475-80.
29. Mesa JM, Aroca A, Ramirez U, et al. Cirurgia de las complicaciones mecanicas del infarto agudo de miocárdio. Rev Esp Cardiol. 1998; 51(3): 71-9.
30. Cho MN, Metha SK, Matulevicius S, et al. Differentiating true versus pseudo left ventricular aneurysm: a case report and review of diagnostic strategies. Cardiol Review. 2006; 14: e27-e30.
31. Abrams DL, Edelist A, Luria MH, et al. Ventricular aneurysm: a reappraisal on a study of 65 consecutive autopsied cases. Circulation. 1963; 27: 164.
32. Duvenoy O, Wikstrom G, Mannting, et al. Pre- and postoperative CT and RM in pseudoaneurysms of the heart. J Comp Assist Tomogr. 1992; 16: 401-9.
33. Likoff W, Bailey CP. Ventriculoplasty: excision myocardial aneurysm: report of a successful case. JAMA .1955; 158: 915-20.
34. Jatene AD. Left ventricular aneurysmectomy: resection or reconstruction. J Thorac Cardiovasc Surg. 1985; 89: 331.
35. Parolari A, Nliato M, Loardi C, et al. Surgery of left aneurysm: a meta-analysis of early outcomes following different reconstruction techniques. Ann Thorac Surg. 2007; 83: 2009-16.
36. Hung MJ, Wang CH, Cherng WJ. Unruptured left ventricular pseudoaneurysm following myocardial infarction. Heart .1998; 80: 94-7.
37. Milgarter E, Uretzky G, Levy P, et al: Pseudoaneurysm of the left ventricle. Thorac Cardiovasc Surg.1987; 35: 20-5.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 69-75 - 75
38. Jutrin I, DiSegni E, Krabel G. False aneurysm of the right atrium. Chest. 1979; 75: 629.
39. Antman EM. ST-elevation myocardial infarction. In: Zipes ,et al.( Eds). Braunwalds Heart Disease: a textbook of cardiovascular medicine. 7. ed. Philadelphia: Elsevier Saunders; 2005. p.1167-1226.
40. Davidson KH, Parisi AF, Harrington JJ, et al. Pseudoaneurysm of the left ventricule: an unusual echocardiographic presentation: review of the literature. Ann Intern Med .1977; 86: 430.
41. March KL, Sawada SG, Tarver RD, et al: Current concepts of left ventricular pseudoaneurysm: pathophysiology, therapy and diagnostic imaging methods. Clin Cardiol. 1989; 12: 531-40.
42. Yeo TG, Malouf JF, Oh JK, et al. Clinical profile and outcome in 52 patients with cardiac pseudoaneurysm. Ann Intern Med. 1998; 128: 299-305.
43. Gatewood RP, Nanda NC. Differentiation of left ventricular pseudoaneurysm from true aneurysm with two dimensional
echocardiography. Am J Cardiol. 1980; 46: 869-78.44. Dor V, Sabatier M, Montiglio F, et al. Endoventricular patch
reconstruction of ischemic failing ventricle: a single center with 20 years experience. Advantages of magnetic resonance imaging assessment. Heart Failure Review. 2004; 9: 269-86.
45. Klein MD, Herman MV, Gorlin R. A hemodynamic study of left ventricular aneurysm. Circulation. 1967; 35: 614-30.
46. Packer M. The neurohormonal hypothesis: a theory to explain the mechanism of disease progression in heart failure. J Am Coll Cardiol. 1992; 20: 248-54.
47. Reyes G, Yáñez JF, Abella HR, et al: Asistencia ventricular mecánica como puente al trasplante. Rev Esp Cardiol. 2007; 60(1): 72-5.
48. Bueno MG, Cubero JS, Rivera LAP. Asistencia mecánica circulatoria y trasplante cardíaco. Indicaciones y situación en España.Rev Esp Cardiol. 2006; 6 Supl.: 82F-94F.

76 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 76-78
MICOBACTERIOSE CUTÂNEA ATÍPICA, PÓS-MESOTERAPIA: INFECÇÃO POR Mycobacterium arupense
AUTORES:1ºT (S-RM2) FERNANDA MENDES PEREIRA MÜLLER, M.D. Graduação em Farmácia e Bioquímica pela Universidade Federal de Juiz de Fora.Mestrado em Ciências Biológicas – Microbiologia pela Universidade Federal de Minas Gerais.Assistente do Serviço de Análises Clínicas do HNBra.
MARIA LETÍCIA DOS SANTOS CABRAL Graduação em Medicina pela Faculdade de Ciências Médicas de Minas Gerais.Residência em Clínica Médica pelo Hospital Socor.Residência em Dermatologia. Especialização em Clínica Médica, pela Sociedade Brasileira de Clínica Médica.Especialização em Dermatologia pela Sociedade Brasileira de Dermatologia.Membro Titular da Sociedade Brasileira de Dermatologia.Assistente da Clínica de Dermatologia do HNBra.
CF (Md) LÁSARO PEREIRA DE MELO Graduação em Medicina pela Universidade de Brasília.Residência em Cirurgia Geral pelo Hospital das Forças Armadas e Hospital Regional de Taguatinga.Especialização em Cirurgia Geral pelo Colégio Brasileiro de Cirurgiões.Especializaçõ em Medicina Legal pela Associação Brasileira de Medicina Legal.Membro Titular do Colégio Brasileiro de Cirurgiões.Fellow do International College of Surgeons.Membro Associado da Sociedade Brasileira de Cirurgia Bariátrica e Metabólica.Membro da Associação Brasileira de Medicina Legal.Encarregado da Divisão de Cirurgia Geral do HNBra.
RESUMO Os autores relatam o primeiro caso, no Brasil, de micobacteriose cutânea atípica por Mycobacterium arupense, após mesoterapia para lipodistrofia
regional. Ressaltam ainda a importância do diagnóstico de micobacterioses atípicas após procedimentos cirúrgicos e o sucesso da terapia combinada.
Palavras-chave: Mycobacterium arupense; mesoterapia; micobacteriose cutânea.
INTRODUÇÃO
As micobacterioses cutâneas atípicas são doenças causa-
das por micobactérias “não tuberculosas”. O diagnóstico etioló-
gico é realizado pela análise microbiológica de tecidos e secre-
ções, demonstrando a presença do microrganismo. A pesquisa
de BAAR, pelo método de Ziehl-Neelsen, em secreção e/ou ma-
terial de biópsia pode fornecer subsídios importantes para dire-
cionar o diagnóstico.
A mesoterapia é uma técnica de origem francesa que consiste na
injeção intradérmica de substâncias medicamentosas com o propósi-
to de tratar várias afecções, principalmente, na área de dermatologia.
Nos últimos anos essa técnica tem sido associada ao aumento da
incidência de casos de infecções cutâneas.
Os raros relatos na literatura sobre micobacteriose cutânea atípica
e o primeiro isolamento da espécie Mycobacterium arupense, no Bra-
sil, motivaram a divulgação do caso.
RELATO DO CASO
Trata-se de paciente do sexo feminino, leucoderma, 26 anos,
natural e procedente de Brasília (DF), solteira, militar, que procurou
o serviço de dermatologia do Hospital Naval de Brasília, queixando-
se de furunculose na região das coxas, com três meses de evolu-
ção. Informa que as lesões iniciaram-se duas semanas após uma
sessão de mesoterapia, em uma clínica clandestina, na cidade do
Guará (DF).
Ao exame dermatológico, notavam-se nódulos endurecidos na
face lateral das coxas, de cor violácea, quentes, dolorosos, alguns
flutuantes, outros ulcerados com drenagem de secreção serosa
nos prováveis sítios de injeção. Na região abdominal havia três nó-
dulos endurecidos, indolores e sem flutuações. Não apresentava
linfoadenomegalias.
Foram realizadas aspirações por agulha nas lesões que apresenta-
vam flutuação, para coleta de material, sendo realizado exame direto e

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 76-78 - 77
Figura 1: Bacilos álcool-ácido resistentes, pela coloração de Ziehl-Neelsen.
Figura 2: Colônias não pigmentadas isoladas da secreção das lesões, sugerindo o diagnóstico de micobactéria atípica.
cultura dessas secreções. Ao exame
direto pelo método de Ziehl-Neelsen,
foram visualizados bacilos álcool-áci-
do resistentes (Figura 1). A cultura foi
realizada por meio de semeadura do
material em meio de Löwenstein-Jen-
sen e incubada em aerobiose à tem-
peratura de 37ºC. Após dez dias, foi
observado o crescimento de colônias
não pigmentadas, caracterizando e
confirmando a presença de micobac-
téria atípica (Figura 2). Posteriormente, o microrganismo foi identificado,
por método molecular, no Centro de Referência Professor Hélio Fraga,
no Rio de Janeiro, como Mycobacterium arupense.
Os exames complementares – hemograma completo, glicemia, função hepática, lipidograma e função renal – estavam dentro dos limi-tes da normalidade e a sorologia para HIV foi negativa.
Foi instituído, inicialmente, o tratamento medicamentoso, de acor-do com a Nota Técnica nº 2/Devep/SVS/MS (Brasil, MS) com clarito-micina e etambutol, durante seis meses e amicacina, por três meses.
Figura 4: Aspecto das lesões, em coxa direita, após desbridamento.
Figura 5: Aspecto das lesões, em parede abdominal, após desbridamento.
A conduta operatória consistiu em desbridamentos amplos das le-sões, em centro cirúrgico (Figuras 3, 4 e 5). A biópsia do material des-bridado revelou infiltrado granulomatoso na derme profunda e subcu-tâneo, com numerosos neutrófilos e necrose tecidual.
Um ano após o início da afecção, a paciente apresentava lesões cicatrizadas (Figura 6) com queixas relativas somente ao aspecto estético resultante.
Figura 3: Aspecto das lesões, em coxa esquerda, após desbridamento.
DISCUSSÃOA mesoterapia ou intradermoterapia é um método terapêutico
francês que consiste na injeção via intradérmica e subcutânea de pe-quenas quantidades de substâncias ou combinação de substâncias farmacológicas no local da afecção, sendo de uso exclusivo médico
Figura 6: Lesões na coxa direita, cicatrizadas.
78 - Arq. Bras. Med. Naval, Rio de Janeiro, 70(1): 76-78
(Del Solar, 2005; Kede, 2003; Reis, 1993). As indicações para meso-terapia vêm crescendo, ao longo dos anos, como por exemplo, nas afecções osteoarticulares, alopecias, estrias, fotoenvelhecimento cutâneo e lipodistrofias regionais (celulite) (Kede, 2003; Reis, 1993).
As complicações pós-mesoterapia começaram a ser descritas na década de 80 e as micobacterioses atípicas, atualmente, são as prin-cipais responsáveis pelas complicações infecciosas, mesmo que o seu isolamento não seja conseguido em todos os casos (Reis, 1993). Em uma pesquisa retrospectiva na França, revelou-se que 15% dos casos de micobacterioses cutâneas atípicas, foram contraídas por meio da meso-terapia (Ssouza, 2001). Esse excelente método terapêutico, em mãos de pessoas inexperientes ou sem qualificação, vem causando prejuízos aos pacientes, que frequentam clínicas que oferecem tratamentos estéticos, muitas vezes realizados por profissionais não habilitados.
De acordo com Barreto, as espécies predominantes de micobacté-rias “não tuberculosas” no Brasil, são M. avium-intracellulare, M. kan-sasii e M. fortuitum (Barreto, 2000).
Recentemente foram relatadas infecções por micobactérias atípi-cas relacionadas com procedimentos cirúrgicos laparoscópicos, ar-troscópicos e procedimentos estéticos, como colocação de próteses mamárias e lipoaspirações, sendo identificados, principalmente, M. abscessus, M. fortuitum e M. chelonae (Brasil, MS; Brasil, SES-MG).
Relatos de isolamento de micobactéria atípica após procedimento estético – mesoterapia – não é novo: M. fortuitum, no Distrito Federal (Reis, 1993) M. fortuitum, na Bahia (Souza, 2001) M. chelonae, no Peru (Del Solar, 2005) e M. absessus, M. peregrinum, M. simiae, M. cosmeti-cum, na Venezuela (Rivera-Olivero, 2006). Entretanto, esse é o primei-ro caso de infecção por M. arupense relatado no Brasil (Barreto, 2000; Brasil, SES-DF) e não há, até o momento, relato em literatura desse tipo de infecção relacionado à mesoterapia.
M. arupense foi isolada pela primeira vez, em material coletado de pacientes, por Cloud et al., em 2006, nos Estados Unidos (Cloud, 2006). O nome “arupense” vem do Instituto ARUP – para Patologia Clínica e Experimental, localizado em Salt Lake City, EUA, onde a linhagem foi descrita (Cloud, 2006). Os achados fenotípicos situam, sem sombra de dúvida, o M. arupense dentro do complexo do M. terrae (Cloud, 2006; Tortoli, 2006). Essa micobactéria foi isolada também de material coletado de pacientes no Japão, sugerindo sua importância clínica (Masaki, 2006) e em roedores e animais insetívoros na África (Durnez, 2008).
O tratamento para a micobacteriose atípica ainda não é padro-nizado no Brasil, sendo realizado baseado em relatos de literatura e informes técnicos de instituições de vigilância sanitária governamen-tais (Brasil, MS; Brasil, SES-MG; Del Solar, 2005; Reis, 1993; Rivera-Olivero, 2006; Souza, 2001). Existem casos relatados de resistência ao tratamento antimicrobiano (Caminero, 2001; Del Solar, 2005).
No caso apresentado, foram utilizados além da antibioticoterapia, o desbridamento cirúrgico de todo o tecido afetado. Acreditamos que es-sa combinação terapêutica encurtou o tempo da doença em atividade, bem como a comorbidade. O tratamento para micobacteriose atípica é sempre difícil e desafiador, principalmente frente a uma espécie nova.
CONCLUSÃOAs infecções por micobactérias atípicas relacionadas a procedimen-
tos invasivos, especificamente a mesoterapia, têm sido descritas há mais de 20 anos. O diagnóstico deve ser precoce, permitindo o imediato início
do tratamento, assegurando bom resultado. Não há esquema específico para o tratamento da infecção por M. arupense, sendo uma opção aque-les já existentes para outros microorganismos do gênero.
BIBLIOGRAFIA1. Abreu D. Clínica de estética clandestina pode ter infecta-
do cliente com bactéria rara. Correio Web. 2008. [Acesso em 21 fev.2008]. Disponível em: http://noticias.correioweb.com.br/materias.php?id=2733209&sub=Distrito%20Federal
2. Barreto AMW, Campos CED. Micobactérias não tuberculosas no Brasil. Bol Pneum Sanit. 2000; 8(1): 23-32.
3. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Nota Técnica nº 2/DEVEP/SVS/MS [Acesso em 21set. 2008]. Disponível em:http://portal.saude.gov.br/portal/saude/visualizar_texto.cfm?idtxt=25831
4. Brasil.Secretaria de Estado de Saúde do Distrito Federal. Subse-cretaria de Vigilância em Saúde. Gerência de investigação e prevenção das infecções e eventos adversos em serviços de saúde – GEPEAS. Nota Técnica. [Acesso em 21 fev.2008]. Disponível em: http://www.sau-de.df.gov.br/003/00301015.asp?ttCD_CHAVE=58669
5. Brasil.Secretaria de Estado de Saúde de Minas Gerais. Subsecre-taria de Vigilância em Saúde. Superintendência de Vigilância Sanitária. Gerência de Vigilância em Estabelecimentos de Saúde. Alerta Técnico.[Acesso em 22 set. 2008]. Disponível em: http://www.saude.mg.gov.br/publicacoes/estatistica-e-informacao-em-saude/alertas-tecnicos/Aler-ta%20Tecnico%20da%20VISA%20-%20BH%20e%20SES.pdf
6. Caminero Luna JA. Micobactérias atípicas. BSCP Can Ped. 2001; 25(2): 237-48.
7. Cloud JL, et al. Mycobacterium arupense sp. nov., a non-chromo-genic bacterium isolated from clinical specimens. Int J Syst Evol Micro-biol. 2006; 56: 1413-18.
8. Del Solar M, et al. Infección cutânea por micobacterias atípicas de crecimiento rápido (MACR) debido a mesoterapia cosmética. Reporte de casos y revisión de la literatura. Folia Dermatol Peru. 2005; 16 (3):127-35.
9. Durnez L, et al. First detection of mycobateria in african rodents and insectivores, using stratifield poll screening. Appl Environ Microbiol. 2008; 74(3): 768-73.
10. Kede MPV, Sabotovich O. Dermatologia Estética. São Paulo: Atheneu; 2003.
11. Masaki T, et al. Mycobacterium kumamotonense Sp. Nov. Recovered from clinical specimen and the first isolation report of mycobacterium arupen-se in japan: novel slowly growing, nonchromogenic clinical isolates related to mycobacterium terrae complex. Microbiol Immunol. 2006; 50 (11): 889-97.
12. Reis, CMS, Wen L, Vieira FD, Lemos CMF. Complicações cutâ-neas da mesoterapia: infecção por mycobacterium fortuitum (duas ob-servações). An Bras Dermatol. 1993; 68: 277-80.
13. Rivera-Olivero IA, Guevara A, Escalona A, Oliver M,et al. Infec-ciones en tejidos blandos por micobacterias no tuberculosas secun-darias a mesoterapia: cuánto vale la belleza? Enferm Infecc Microbiol Clin. 2006; 24(5): 302-6.
14. Souza ACGO, Pereira CP, Guimarães NS, Rego VR, Paixão AP, Barbosa Jr AA. Micobacteriose cutânea atípica pós-mesoterapia. An Bras Dermatol. 2001; 76 (6): 711-15.
15. Tortoli E. The new mycobacteria: an update. FEMS Immunol Med Microbiol. 2006;48:159-78.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 79-81 - 79
ATYPICAL CUTANEOUS MYCOBACTERIOSIS POST-MESOTHERAPY: INFECTION CAUSED BY Mycobacterium arupense
AUTHORS:1ºT (S-RM2) FERNANDA MENDES PEREIRA MÜLLER, M.D. Bachelor’s Degree in Pharmacy and Biochemistry from the Universidade Federal de Juiz de Fora.Master’s Degree in Biological Sciences – Microbiology from the Universidade Federal de Minas Gerais.Clinical Analysis Service Assistant at HNBra.
MARIA LETÍCIA DOS SANTOS CABRAL Bachelor’s Degree in Medicine from the Faculdade de Ciências Médicas de Minas Gerais.Medical Residency Training in General Practice at the Hospital Socor.Medical Residency Training in Dermatology.Specialization in General Practice from the Brazilian Society of General Practice.Specialization in Dermatology from the Brazilian Society of Dermatology.Active Member of the Brazilian Society of Dermatology.Physician Assistant at the Dermatology Clinic of HNBra.
CF (Md) LÁSARO PEREIRA DE MELO Bachelor’s Degree in Medicine from the Universidade de Brasília.Medical Residency Training in General Surgery from the Hospital das Forças Armadas and the Hospital Regional de Taguatinga.Specialization in General Surgery from the Brazilian College of Surgeons.Specialization in Medical Jurisprudence from the Brazilian Medico-Legal Association.Active Member of the Brazilian College of Surgeons.Fellow of the International College of Surgeons.Associated Member of the Brazilian Society of Bariatric and Metabolic Surgery.Member of the Brazilian Medico-Legal Association.Chief of the General Surgery Division at HNBra.
ABSTRACT The authors report the first case of atypical cutaneous mycobacteriosis in Brazil caused by Mycobacterium arupense, after mesotherapy for regional
lypodistrophy. They also emphasize the importance of post-surgery diagnosis of atypical mycobacteriosis and discuss successful combined therapies.
Keywords: Mycobacterium arupense; mesotherapy; cutaneous mycobacteriosis.
INTRODUCTION
Atypical cutaneous mycobacteriosis is caused by non-tuberculous
mycobacteria. Etiologic diagnosis is conducted by means of microbiological
analysis of tissues and secretions, which evidences the presence of the
bacteria. The Ziehl-Neelsen acid-fast staining technique is an effective
method that provides relevant data for detection and diagnosis of alcohol
acid-resistant bacilli (AARB) in secretion and/or biopsy samples.
Mesotherapy is a procedure originated in France. It employs
intradermal injections of specific medication that aim to treat a spectrum
of medical conditions, especially those related to dermatology.
Nevertheless, this technique has lately been associated with an
increasing number of cutaneous infections.
This case report was motivated by the scarce number of publications
about atypical cutaneous mycobacteriosis and by the first isolation
report of Mycobacterium arupense in Brazil.
CASE REPORT
The patient is a 26 year-old single female military officer with
leucoderma. She is from and resides in Brasilia (Federal District) and
came to the Hospital Naval de Brasília complaining of a 3-month history
of furunculosis in the thighs. The lesions appeared after a mesotherapy
session in a clandestine clinic in the suburb town of Guará (Federal District).
The dermatological exam revealed the presence of violetish,
hardened, painful and warm-to-the-touch nodules on the side face of
the thighs. Some were fluctuating nodules, while others were ulcerated
nodules with serum secretion in what had probably been the sites of
the injections. On the abdomen, there were three hardened yet painless
and non-fluctuating nodules. There were no limphadenomegalies.
In order to collect samples of secretion for direct analysis and culture
analysis, needle aspiration was carried out into the fluctuating nodules.
The direct analysis employing Ziehl-Neelsen technique showed alcohol

80 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 79-81
Figure 1: Alcohol acid-resistant bacilli, as per Ziehl-Neelsen staining.
Figure 2: Non-pigmented colonies isolated from the secretion of the lesions, suggesting the diagnosis of atypical mycobacteria.
acid-resistant bacilli (Figure 1). The culture
analysis was conducted through inoculation
in Löwenstein-Jensen medium and incubated
in aerobiosis at a temperature of 37ºC. Ten
days later it was observed the growth of
non-pigmented colonies, thus characterizing
and confirming the presence of atypical
mycobacteria (Figure 2). This microorganism
was later identified by molecular method at
the Centro de Referência Professor Hélio
Fraga, in Rio de Janeiro, as Mycobacterium arupense. The results of the supplementary tests – complete hemogram,
glycemia, hepatic function, lipidogram and renal function – were all within normal range, and HIV serology was negative.
Drug treatment was then prescribed as noted down on the Technical Record (Nota Técnica nº 2/Devep/SVS/MS) (Brasil, MS) - claritomicine and ethambutol for six months, and amicacine for three months.
The lesions were also treated with a surgical procedure – ample debridement – at a surgery unit (Figures 3, 4 and 5). The biopsy of the debrided material samples revealed granulomatous infiltrate in deep skin and subcutaneous tissue, with a number of neutrophils and tissue necrosis.
One year after the dermal problems had started, the patient’s lesions were all healed (Figure 6) and the patient’s only complaints were about the resulting aesthetic aspect.
DISCUSSIONMesotherapy or intradermotherapy is a French therapeutic method
that employs intradermal and subcutaneous injection of small amounts of pharmaceutical substances or a combination of such substances into the affected sites, exclusively for medical purposes (Del Solar, 2005; Kede, 2003; Reis, 1993). The prescription for mesotherapy has increased in the past years to include, for instance, osteoarticulatory
Figure 5: Aspect of the lesions on the abdominal wall after debridement.
Figure 4: Aspect of the lesions on the right thigh after debridement.
Figure 6: Healed lesions on the right thigh.
Figure 3: Aspect of the lesions on the left thigh after debridement.

Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1): 79-81 - 81
conditions, alopecy, stretch marks, skin photoaging and regional lypodistrophy (cellulitis) (Kede, 2003; Reis, 1993).
Post-mesotherapy complications were first reported in the 1980s, and atypical mycobacteriosis currently stands for the major cause of infectious complications, even though isolation has not been achieved in all the reported cases (Reis, 1993). A retrospective study conducted in France found out that 15% of all atypical cutaneous mycobacterioses developed after mesotherapy (Souza, 2001). This excellent therapeutic method, however, when conducted by inexperienced or unqualified personnel, has caused serious damage to patients that resort to aesthetic treatment in clinics that often employ non-certified personnel.
According to Barreto (2000), the predominating types of non-tuberculous mycobacteria in Brazil are M. avium-intracellulare, M. kansasii and M. fortuitum.
There have been recent reports of infections caused by atypical mycobacteria related to laparoscopic, arthroscopic and aesthetic surgical procedures, like breast prosthesis and lipoaspiration, among which predominate M. abscessus, M. fortuitum and M. Chelonae (Brasil, MS; Brasil, SES-MG).
Reports of isolating atypical mycobacteria after aesthetic procedures - mesotherapy – are not new: M. fortuitum, in the Federal District of Brazil (Reis, 1993) M. fortuitum, in the Brazilian state of Bahia (Souza, 2001), M. chelonae in Peru (Del Solar, 2005), and M. absessus, M. peregrinum, M. simiae, M. cosmeticum in Venezuela (Rivera-Olivero, 2006). Nevertheless, this is the first case of infection by M. arupense reported in Brazil (Barreto, 2000; Brasil, SES-DF), and there has been no literature report so far about this type of infection related to mesotherapy.
M. arupense was first isolated in samples colleted from patients by Cloud et al., in 2006 in the United States (Cloud, 2006). The name “arupense” comes from the ARUP Institute for Clinical and Experimental Pathology, in Salt Lake City, USA, where this cellular microorganism lineage was first described (Cloud, 2006). Phenotypic findings undoubtedly place M. arupense within the M. terrae complex (Clud, 2006; Tortoli, 2006). This mycobacterium was also isolated in samples collected from patients in Japan - which evidences its clinical importance (Masaki, 2006), and from rodents and insectivorous animals in Africa (Durnez, 2008).
There is no standard treatment for atypical mycobacteriosis in Brazil, so what is usually prescribed is based on the existing literature and technical reports issued by government sanitary surveillance organizations (Brasil, MS; Brasil, SES-MG; Del Solar, 2005; Reis, 1993; Rivera-Olivero, 2006; Souza, 2001). There are reported cases of resistance to antimicrobial treatment (Caminero, 2001; Del Solar, 2005). In the herein reported case, besides antibiotic therapy, surgical debridement of all the affected tissue was also conducted, and we believe that this combined therapy has shortened the microorganisms’ activity time as well as comorbidity. Atypical mycobacteriosis treatment is generally difficult and challenging, especially when faced with a new species.
CONCLUSIONAtypical mycobacterial infections that are related to invasive procedures
– more specifically mesotherapy - have been reported for over 20 years. Early diagnosis enables immediate treatment and yields effective results. There is yet no specific or standard treatment for infection by M. arupense, and alternatives include existing treatment for similar types of microorganisms.
BIBLIOGRAPHY1. Abreu D. Clínica de estética clandestina pode ter infectado cliente com
bactéria rara. Correio Web. 2008. [Accessed on: 21 fev.2008]. Available at: http://noticias.correioweb.com.br/materias.php?id=2733209&sub=Distrito%20Federal
2. Barreto AMW, Campos CED. Micobactérias não tuberculosas no Brasil. Bol Pneum Sanit. 2000; 8(1): 23-32.
3. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Nota Técnica nº 2/DEVEP/SVS/MS [Accessed on 21set. 2008]. Available at: http://portal.saude.gov.br/portal/saude/visualizar_texto.cfm?idtxt=25831
4. Brasil.Secretaria de Estado de Saúde do Distrito Federal. Subsecretaria de Vigilância em Saúde. Gerência de investigação e prevenção das infecções e eventos adversos em serviços de saúde – GEPEAS. Nota Técnica. [Accessed on: 21 fev.2008]. Available at: http://www.saude.df.gov.br/003/00301015.asp?ttCD_CHAVE=58669
5. Brasil.Secretaria de Estado de Saúde de Minas Gerais. Subsecretaria de Vigilância em Saúde. Superintendência de Vigilância Sanitária. Gerência de Vigilância em Estabelecimentos de Saúde. Alerta Técnico.[Accessed on: 22 set. 2008]. Available at: http://www.saude.mg.gov.br/publicacoes/estatistica-e-informacao-em-saude/alertas-tecnicos/Alerta%20Tecnico%20da%20VISA%20-%20BH%20e%20SES.pdf
6. Caminero Luna JA. Micobactérias atípicas. BSCP Can Ped. 2001; 25(2): 237-48.
7. Cloud JL, et al. Mycobacterium arupense sp. nov., a non-chromogenic bacterium isolated from clinical specimens. Int J Syst Evol Microbiol. 2006; 56: 1413-18.
8. Del Solar M, et al. Infección cutânea por micobacterias atípicas de crecimiento rápido (MACR) debido a mesoterapia cosmética. Reporte de casos y revisión de la literatura. Folia Dermatol Peru. 2005; 16 (3): 127-35.
9. Durnez L, et al. First detection of mycobateria in african rodents and insectivores, using stratifield poll screening. Appl Environ Microbiol. 2008; 74(3): 768-73.
10. Kede MPV, Sabotovich O. Dermatologia Estética. São Paulo: Atheneu; 2003.
11. Masaki T, et al. Mycobacterium kumamotonense Sp. Nov. Recovered from clinical specimen and the first isolation report of mycobacterium arupense in japan: novel slowly growing, nonchromogenic clinical isolates related to mycobacterium terrae complex. Microbiol Immunol. 2006; 50 (11): 889-97.
12. Reis, CMS, Wen L, Vieira FD, Lemos CMF. Complicações cutâneas da mesoterapia: infecção por mycobacterium fortuitum (duas observações). An Bras Dermatol. 1993; 68: 277-80.
13. Rivera-Olivero IA, Guevara A, Escalona A, Oliver M,et al. Infecciones en tejidos blandos por micobacterias no tuberculosas secundarias a mesoterapia: cuánto vale la belleza? Enferm Infecc Microbiol Clin. 2006;24(5):302-6.
14. Souza ACGO, Pereira CP, Guimarães NS, Rego VR, Paixão AP, Barbosa Jr AA. Micobacteriose cutânea atípica pós-mesoterapia. An Bras Dermatol. 2001; 76 (6): 711-15.
15. Tortoli E. The new mycobacteria: an update. FEMS Immunol Med Microbiol. 2006; 48: 159-78.
82 - Arq. Bras. Med. Naval, Rio de Janeiro, 70 (1)
Os artigos científicos deverão ser inéditos e os autores de-vem encaminhá-lo para: [email protected].
Sugerimos que os autores sigam as seguintes regras para envio:
a) folha de rosto, com:
- o título do artigo;
- identificação e qualificação dos autores (todos terão a denominação “autores”, sendo descritos em ordem de participação/importância) constando: nome com-pleto, formação e qualificação profissional e/ou aca-dêmica (currículo resumido incluindo a entidade que titulou);
- endereço: e-mail dos autores para possível contato;
b) a estrutura de apresentação do artigo deverá conter: tí-tulo do artigo, resumo e palavras-chave em português e in-glês (title, abstract, key words), introdução, desenvolvimen-to, conclusão e referências;
c) a bibliografia completa deverá ser apresentada em ordem alfabética no fim do texto, de acordo com as normas de Vancouver. No decorrer do texto segue o exemplo: souzA et al., 2003; Souza, Medeiros e Bote-lho, 2008;
d) o artigo deverá ser digitado no sistema Word, formato A4, fonte Times New Roman, corpo 12 para o texto e me-nor para citações de mais de três linhas, notas de rodapé, paginação e legendas dos gráficos, tabelas e/ou ilustra-ções. As folhas devem apresentar margens esquerda e superior de 3 cm; direita e inferior de 2 cm; entrelinhas simples; alinhamento justificado;
e) cada artigo deverá ter no mínimo oito páginas e no má-ximo 12 páginas, sendo considerada cada página de 72 toques x 30 linhas;
f) cada artigo deverá estar perfeitamente revisado;
g) encaminhar as referências bibliográficas para o e-mail da revista ([email protected]) com o prazo mínimo de 30 dias de antecedência para normalização.
The scientific articles shall be unpublished and the author(s) shall send them to: [email protected]
We suggest that the authors observe the following guide-lines for sending articles:
a) cover sheet containing:
- the title of the article.
- the name and title of the author(s) (all of them shall be re-ferred to as ‘authors’, being described in their order of par-ticipation/importance), containing the following: full name, educational and professional and/or academic qualification (that would be the summarized curriculum vitae, includ-ing the name of the academic institution where the author earned his/her degree).
- the mailing address: e-mail of the author(s) for pos-sible contact;
b) the presentation structure of the article shall contain the following: title of the article, abstract and keywords in Portu-guese and English (title, abstract, keywords), introduction, development, conclusion and references;
c) the complete bibliography should be presented in alpha-betical order at the end of the text, in accordance with the Vancouver guidelines. Please use the following example as a guide along the text: Souza et al., 2003; Souza, Medeiros and Botelho, 2008;
d) the article should be typed in a MS Word document, A4 format size, in Times New Roman typeface, 12-point font size for the text and a smaller font size for quotations with more than three lines, as well as for footnotes, pagination and legends for the charts, tables and/or illustrations. The page setup should be the following: indentation – left and upper edges = 3 cm, right and lower edges = 2 cm; line spacing = single; alignment = justified;
e) each article should be at least eight pages long and should have the maximum of 12 pages, considering that each page has 72 strokes x 30 lines;
f) each article should be carefully reviewed;
g) send the bibliographical references to the e-mail of the magazine ([email protected]) within at least thirty days for normalization.
Normas para Publicação Guidelines for Publication

Dr. JOAQUIM CÂNDIDO SOARES DE MEIRELLESCirurgião-Mor da Armada Imperial
Patrono do Corpo de Saúde da Marinha

DIRETORIA DE SAÚDE DA MARINHA