

Apresentação do PowerPoint - EPI uff | Portal de...
25
AULA 1 – turma 214 – 1sem2017 Site: www.epi.uff.br Epidemiologia Analítica
Transcript of Apresentação do PowerPoint - EPI uff | Portal de...

Como o conhecimento médico é construído?
Pneumonia
Quais as questões clínicas frente a um paciente?
1. Causa, fatores de risco associados
2. Diagnóstico
3. Tratamento
4. Prognóstico
5. Prevenção

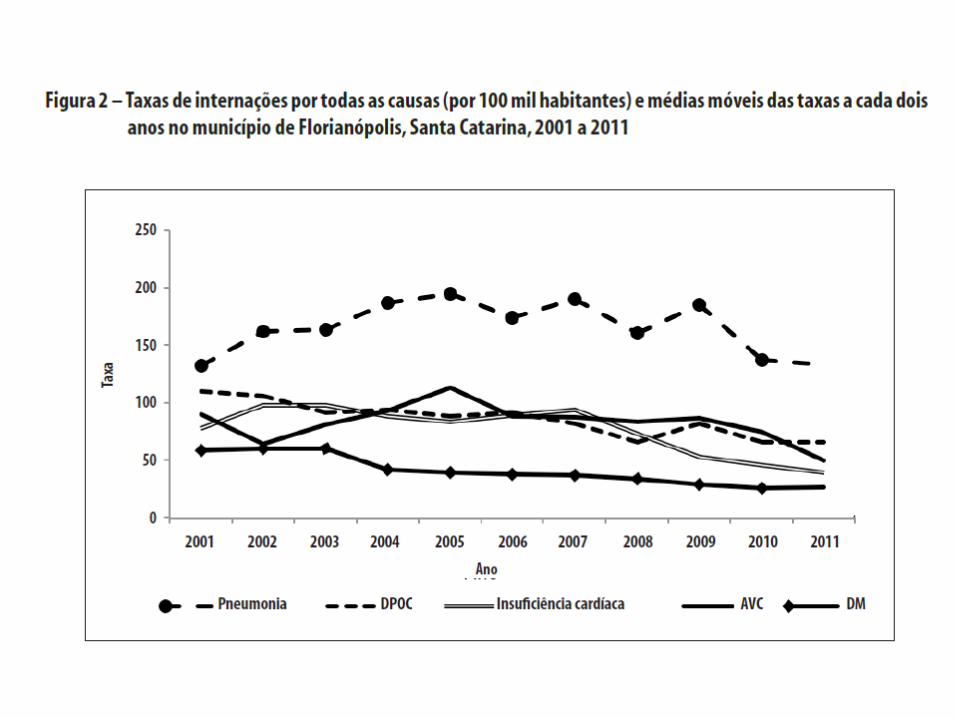
Epidemiologia descritiva • As doenças do aparelho respiratório são a principal causa de hospitalizações no
Brasil, excluídas as relacionadas ao parto, gravidez e puerpério.
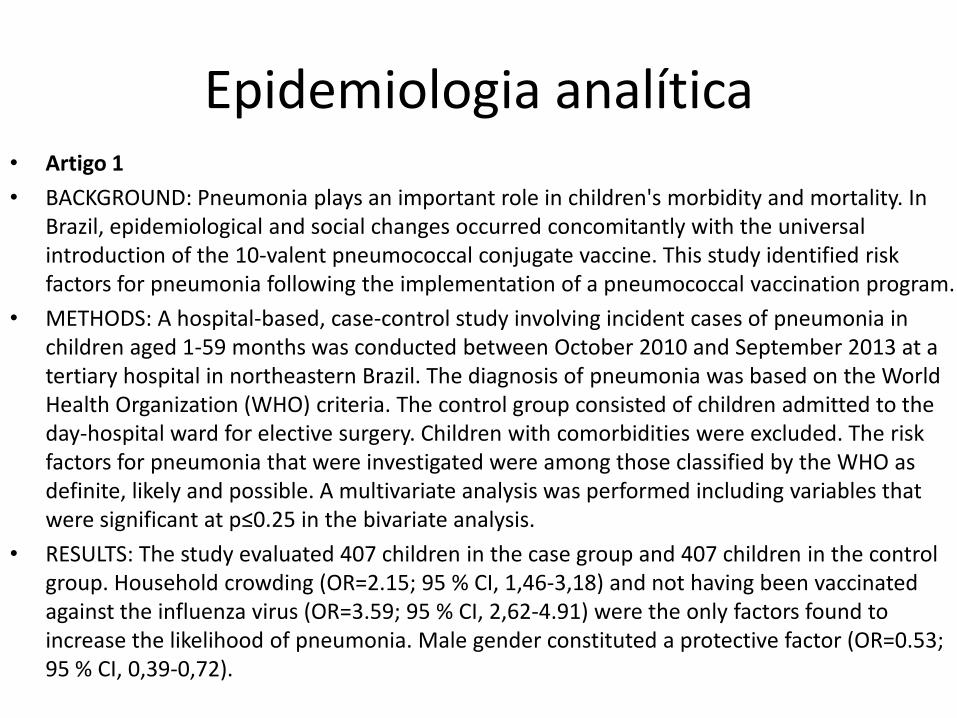
Epidemiologia analítica • Artigo 1
• BACKGROUND: Pneumonia plays an important role in children's morbidity and mortality. In Brazil, epidemiological and social changes occurred concomitantly with the universal introduction of the 10-valent pneumococcal conjugate vaccine. This study identified risk factors for pneumonia following the implementation of a pneumococcal vaccination program.
• METHODS: A hospital-based, case-control study involving incident cases of pneumonia in children aged 1-59 months was conducted between October 2010 and September 2013 at a tertiary hospital in northeastern Brazil. The diagnosis of pneumonia was based on the World Health Organization (WHO) criteria. The control group consisted of children admitted to the day-hospital ward for elective surgery. Children with comorbidities were excluded. The risk factors for pneumonia that were investigated were among those classified by the WHO as definite, likely and possible. A multivariate analysis was performed including variables that were significant at p≤0.25 in the bivariate analysis.
• RESULTS: The study evaluated 407 children in the case group and 407 children in the control group. Household crowding (OR=2.15; 95 % CI, 1,46-3,18) and not having been vaccinated against the influenza virus (OR=3.59; 95 % CI, 2,62-4.91) were the only factors found to increase the likelihood of pneumonia. Male gender constituted a protective factor (OR=0.53; 95 % CI, 0,39-0,72).

P Population/
patient
=
I Intervenção
ou exposição
=
C Comparator/
control
=
O Outcome
(Desfecho)
=
Fonseca Lima EJ, Mello MJ, Albuquerque MF, Lopes MI, Serra GH, Lima DE, Correia JB. Risk factors for community-acquired pneumonia in children under five years of age in
the post-pneumococcal conjugate vaccine era in Brazil: a case control study. BMC Pediatr. 2016;16(1):157
QUESTÃO CLÍNICA: DESENHO DE ESTUDO:
Epidemiologia analítica • Artigo 2
• Em países em desenvolvimento, a pneumonia é a principal causa de adoecimento e morte na infância, principalmente em grupos vulneráveis. O objetivo deste estudo foi analisar os fatores associados à pneumonia em crianças Yanomami internadas por condições sensíveis à atenção primária (ICSAP). As internações foram divididas em dois grupos: i) pneumonias e ii) demais causas, de acordo com a lista brasileira de ICSAP. Foram estimadas taxas ajustadas de ICSAP e utilizou-se a regressão logística não condicional para analisar fatores associados. Mais de 90% dos registros foram considerados ICSAP. A taxa padronizada de ICSAP foi 18,6/1.000. As chances de internação por pneumonia foram 2,7 (IC: 1,3- 5,4) vezes maiores em crianças de 0,1 a 5,9 meses; 1,9 (IC: 1,1-3,3) vezes maiores nas crianças que tiveram a duração da hospitalização variando de 8 a 14 dias; e 3,0 (IC: 1,2-7,5) vezes maiores nas crianças com diagnóstico secundário de desnutrição. O excesso de internações evitáveis é um forte indício da baixa qualidade das ações em terras indígenas e do limitado acesso à atenção primária.

Caldart RV, Marrero L, Basta PC, Orellana JD. Fatores associados à pneumonia em crianças Yanomami internadas por condições sensíveis à atenção primária na região
norte do Brasil. Cien Saude Colet. 2016;21(5):1597-606.
P Population/
patient
=
I Intervenção
ou exposição
=
C Comparator/
control
=
O Outcome
(Desfecho)
=
QUESTÃO CLÍNICA: DESENHO DE ESTUDO:
Epidemiologia analítica • Artigo 3
• Introdução: Community-acquired bacterial pneumonia (CABP) is a leading cause of morbidity and
mortality, and treatment recommendations, each with specific limitations, vary globally. We aimed to
compare the efficacy and safety of solithromycin, a novel macrolide, with moxifloxacin for treatment of
CABP.
• Métodos: We did this global, double-blind, double-dummy, randomised, active-controlled, non-inferiority
trial at 114 centres in North America, Latin America, Europe, and South Africa. Patients (≥18 years) with
clinically and radiographically confirmed pneumonia of Pneumonia Outcomes Research Team (PORT) risk
class II, III, or IV were randomly assigned (1:1), via an internet-based central block randomisation
procedure (block size of four), to receive either oral solithromycin (800 mg on day 1, 400 mg on days 2-5,
placebo on days 6-7) or oral moxifloxacin (400 mg on days 1-7). Randomisation was stratified by
geographical region, PORT risk class (II vs III or IV), and medical history of asthma or chronic obstructive
pulmonary disease. The study sponsor, investigators, staff, and patients were masked to group allocation.
The primary outcome was early clinical response, defined as an improvement in at least two of four
symptoms (cough, chest pain, sputum production, dyspnoea) with no worsening in any symptom at 72 h
after the first dose of study drug, with a 10% non-inferiority margin. The primary analysis was by intention
to treat. This trial is registered with ClinicalTrials.gov, number NCT-01756339.
• Resultados: Between Jan 3, 2013, and Sept 24, 2014, we randomly assigned 860 patients to receive
solithromycin (n=426) or moxifloxacin (n=434). Patients were followed up to days 28-35 after first dose.
Solithromycin was non-inferior to moxifloxacin in achievement of early clinical response: 333 (78·2%)
patients had an early clinical response in the solithromycin group versus 338 (77·9%) patients in the
moxifloxacin group (difference 0·29, 95% CI -5·5 to 6·1). Both drugs had a similar safety profile. 43
(10%) of 155 treatment-emergent adverse events in the solithromycin group and 54 (13%) of 154 such
events in the moxifloxacin group were deemed to be related to study druG.

Barrera CM, Mykietiuk A, Metev H , et al. Efficacy and safety of oral solithromycin versus oral moxifloxacin for treatment of community-acquired bacterial pneumonia: a global, double-blind, multicentre, randomised, active-controlled, non-inferiority trial (SOLITAIRE-ORAL). Lancet Infect Dis. 2016;16(4):421-30.
P Population/
patient
=
I Intervenção
ou exposição
=
C Comparator/
control
=
O Outcome
(Desfecho)
=
QUESTÃO CLÍNICA: DESENHO DE ESTUDO:

Epidemiologia analítica
• Artigo 4
• BACKGROUND: There are few data on long-term survival of Brazilian children with vertically acquired HIV infection. We assessed survival, mortality risk factors and response to antiretroviral therapy (ART). We compared children with early and late access to care.
• METHODS: We used Kaplan-Meier survival curves with Log-rank tests to compare survival time and mortality rates of 245 HIV vertically infected children admitted for care during 2002-2014.
• RESULTS: Total follow-up sum was 1584.4 person-years. Overall survival was 83.9%. Median age at start of ART was 51.6 (18.0-94.2) months, and median age at death was 8.2 (1.7-10.1) years (mortality rate: 1.7/100 person-years). Pneumonia and sepsis were the main causes of death. Male gender, viral load (VL) ≥100,000 copies, severe immunosuppression, moderate/severe symptoms and history of opportunistic infection were associated with higher mortality in bivariate analysis. Only severe symptoms remained associated in multivariate analysis (P = 0.03). There was no difference in mortality in early compared to late access group. Overall, 217 patients received ART; 192 had a recent VL, of which 116 (59.8%) had ≤400 copies. Variables associated with therapeutic failure were as follows: VL ≥100,000 copies, less immune suppression, age <12 months at admission and age <3 years at ART start.

Lorenzo CR, Netto EM, Patrício FR, Brites C. Survival Estimates
and Mortality Risk Factors in a Cohort of HIV Vertically Infected Individuals in Salvador, Brazil. Pediatr Infect Dis J. 2017;36(3):e62-e68.
P Population/
patient
=
I Intervenção
ou exposição
=
C Comparator/
control
=
O Outcome
(Desfecho)
=
QUESTÃO CLÍNICA: DESENHO DE ESTUDO:

Epidemiologia analítica • Artigo 5
• BACKGROUND: The relationship between pneumococcal conjugate vaccine-induced antibody responses
and protection against community-acquired pneumonia (CAP) and acute otitis media (AOM) is unclear.
This study assessed the impact of the ten-valent pneumococcal nontypable Haemophilus
influenzae protein D conjugate vaccine (PHiD-CV) on these end points. The primary objective was to
demonstrate vaccine efficacy (VE) against bacterial CAP (B-CAP: radiologically confirmed CAP with
alveolar consolidation/pleural effusion on chest X-ray, or non-alveolar infiltrates and C-reactive protein ≥
40 µg/ml); METHODS AND FINDINGS: This phase III double-blind randomized controlled study was
conducted between 28 June 2007 and 28 July 2011 in Argentine, Panamanian, and Colombian populations
with good access to health care. Approximately 24,000 infants received PHiD-CV or hepatitis
control vaccine (hepatitis B for primary vaccination, hepatitis A at booster) at 2, 4, 6, and 15-18 mo of
age. Interim analysis of the primary end point was planned when 535 first B-CAP episodes, occurring ≥2
wk after dose 3, were identified in the per-protocol cohort. After a mean follow-up of 23 mo (PHiD-CV, n
= 10,295; control, n = 10,201), per-protocol VE was 22.0% (95% CI: 7.7, 34.2; one-sided p = 0.002)
against B-CAP (conclusive for primary objective) and 25.7% (95% CI: 8.4%, 39.6%) against World
Health Organization-defined consolidated CAP. Intent-to-treat VE was 18.2% (95% CI: 5.5%, 29.1%)
against B-CAP and 23.4% (95% CI: 8.8%, 35.7%) against consolidated CAP. End-of-study per-protocol
analyses were performed after a mean follow-up of 28-30 mo for CAP and invasive pneumococcal disease
(IPD) (PHiD-CV, n = 10,211; control, n = 10,140) and AOM (n = 3,010 and 2,979, respectively). Per-
protocol VE was 16.1% (95% CI: -1.1%, 30.4%; one-sided p = 0.032) against clinically confirmed AOM,
67.1% (95% CI: 17.0%, 86.9%) against vaccine serotype clinically confirmed AOM, 100% (95% CI:
74.3%, 100%) against vaccine serotype IPD, and 65.0% (95% CI: 11.1%, 86.2%) against any IPD..
Serious adverse events were reported for 21.5% (95% CI: 20.7%, 22.2%) and 22.6% (95% CI: 21.9%,
23.4%) of PHiD-CV and control recipients, respectively. There were 19 deaths (n = 11,798; 0.16%) in
the PHiD-CV group and 26 deaths (n = 11,799; 0.22%) in the control group.

Tregnaghi MW, Sáez-Llorens X, López P, et al. Efficacy of Pneumococcal Nontypable Haemophilusinfluenzae Protein D Conjugate Vaccine (PHiD-
CV) in Young Latin American Children: A Double-Blind Randomized Controlled Trial. PLoS Med. 2014; 11(6): e1001657.
P Population/
patient
=
I Intervenção
ou exposição
=
C Comparator/
control
=
O Outcome
(Desfecho)
=
QUESTÃO CLÍNICA: DESENHO DE ESTUDO:

Epidemiologia analítica
• Artigo 6
• Despite emerging evidences on the clinical usefulness of lung ultrasound (LUS), international guidelines still do not recommend the use of sonography for the diagnosis of pneumonia.
• OBJECTIVE: Our study assesses the accuracy of LUS for the diagnosis of lungconsolidations when compared to chest computed tomography (CT).
• METHODS: This was a prospective study on an emergency department population complaining of respiratory symptoms of unexplained origin. All patients who had a chest CT scan performed for clinical reasons were consecutively recruited. LUS was targeted to evaluate lung consolidations with the morphologic characteristics of pneumonia, and then compared to CT.
• RESULTS: We analyzed 285 patients. CT was + for at least one consolidation in 87 patients. LUS was feasible in all patients and in 81 showed at least one consolidation, with sensitivity 82.8% (95% CI 73.2%-90%) and specificity 95.5% (95% CI 91.5%-97.9%). In a subgroup of 190 patients who underwent also chest radiography (CXR), the sensitivity of LUS (81.4%, 95% CI 70.7%-89.7%) was significantly superior to CXR (64.3%, 95% CI 51.9%-75.4%) (P<.05), whereas specificity remained similar (94.2%, 95% CI 88.4%-97.6% vs. 90%, 95% CI 83.2%-94.7%).

Nazerian P, Volpicelli G, Vanni S et al. Accuracy of lung ultrasound for the diagnosis of consolidations when compared to chest computedtomography. Am J
Emerg Med. 2015;33(5):620-5.
QUESTÃO CLÍNICA:

Epidemiologia Analítica
Objetivo da disciplina
• Estudar os diferentes tipos de estudos epidemiológicos;
• Aprender a interpretar os resultados dos estudos;
• Criar consciência crítica sobre a qualidade dos artigos;
• Entender o conceito de evidência científica

Livro texto
• Fletcher, Robert H; Fletcher, Suzanne W; Fletcher, Grant S. Epidemiologia clínica. Elementos essenciais. 5. ed. Porto Alegre: Artmed. 2014.

Tópico Questão clínica
Frequência (cap 2) Com que frequência (Incidência vs. Prevalência) a doença ocorre? (EPI2)
Estudos de Risco (cap 5 e 6)
5. Da exposição à doença
6. Da doença à exposição
Causalidade (cap 12)
Quais os fatores associados à ocorrência da doença? Quais os fatores que aumentam/diminuem o risco de um evento? Qual a força desta associação? Qual a significância? (EPI1) Esta associação é causal?
Prognóstico/sobrevida (cap 7) Quais os fatores associados à evolução da doença? Quanto tempo leva para um evento ocorrer? (Sobrevida)
Capítulos do livro texto Epidemiologia clínica. Elementos essenciais.

Capítulos do livro texto Epidemiologia clínica. Elementos essenciais
Tópico Questão clínica
Tratamento (cap 9) A intervenção altera o curso da doença? Qual a eficácia do tratamento?
Prevenção (cap 10) A intervenção evita a ocorrência de doença? Qual a eficácia da prevenção?
Diagnóstico (cap 8) O paciente tem ou não a doença? Qual a acurácia do teste diagnóstico usado?
Síntese da evidência (cap 13) Como identificar a melhor evidência sobre as questões acima? Qual a qualidade da evidência?

Cronograma 1 sem 2017
EPI3 – turma A EPI3 – turma B EPI3 – turma C
1 07/03 Apresentação
O que é epidemiologia analítica?
Apresentação
O que é epidemiologia analítica?
Apresentação
O que é epidemiologia analítica?
2 14/03 Busca bibliográfica e conceito de
evidência
Medidas de associação e teste de
significância
Estudos de prevalência e associação:
Transversais
3 21/03 Medidas de associação e teste de
significância
Estudos de prevalência e associação:
Transversais
Busca bibliográfica e conceito de
evidência
4 28/03 Estudos de prevalência e associação:
Transversais
Busca bibliográfica e conceito de
evidência
Medidas de associação e teste de
significância
5 04/04 Estudos de risco: Coorte
Validade interna e externa
Estudos de risco: Caso-controle
6 11/04 Estudos de risco: Caso-controle
Estudos de risco: Coorte
Validade interna e externa
7 18/04 Validade interna e externa
Estudos de risco: Caso-controle
Estudos de risco: Coorte
8 25/04 Avaliação 1

EPI3 – turma A EPI3 – turma B EPI3 – turma C
9 02/05 Estudos de intervenção
10 09/05 Estudos de intervenção - Artigo
Trabalho p entrega
11 16/05 Estudos de teste diagnóstico Sobrevida
Revisão sistemática
12 23/05 Sobrevida
Revisão sistemática Estudos de teste diagnóstico
13 30/05 Revisão sistemática
Estudos de teste diagnóstico Sobrevida
14 06/06 Artigo de meta-análise de estudos
observacionais
Artigo de meta-análise de ECR Artigo de meta-análise de teste
diagnóstico
15 13/06 Artigo de meta-análise de teste
diagnóstico
Artigo de meta-análise de estudos
observacionais
Artigo de meta-análise de ECR
20/06 Conferência curricular
16 27/06
escolha
do
artigo*
Artigo de meta-análise de ECR Artigo de meta-análise de teste
diagnóstico
Artigo de meta-análise de estudos
observacionais
17 04/07 Preparo do trabalho final presencial
18 11/07 Entrega trabalho final + 2 chamada da AVA1
19 18/07 V.S.

Avaliação da disciplina
• Aulas – exercícios e/ou análise de artigos
• Avaliação escrita (conceitos iniciais)
• Trabalhos com artigos
• Média final = Avaliação I (peso 2) + Avaliação II (peso 2) + média das atividades em sala de aula (peso1)/5
• Faltas – 25% - máximo 4 faltas


















