Br. J. Anaesth.-1998-Greer-384-5.pdf

of 2
-
Upload
rita-guerrero -
Category
Documents
-
view
212 -
download
0
Transcript of Br. J. Anaesth.-1998-Greer-384-5.pdf
-
7/26/2019 Br. J. Anaesth.-1998-Greer-384-5.pdf
1/2
British Journal of Anaesthesia1998; 80: 384385
Neuromuscular monitoring by intensive care nurses: comparison of
acceleromyography and tactile assessment
R. GREER, N. J. N. HARPERANDA. J. PEARSON
Summary
We have compared tactile assessment of thetrain-of-four (TOF) count and TOF ratio bynursing staff, with measurements made by anew aceleromyographic monitor, the TOF-Watch. We assessed neuromuscular block in 30sedated intensive care patients receiving acontinuous infusion of atracurium. Five nursesmade a tactile assessment of neuromuscularblock in each patient within a 5-min period. Eachassessment was paired with a blinded TOF-Watch measurement. The nurses were accuratein assessing twitch count in 55% of measure-ments and they tended to overestimate thedegree of block using tactile assessment of TOFratio. (Br. J. Anaesth. 1998; 80:384385)
Keywords: intensive care; monitoring, neuromuscular func-tion; neuromuscular block, measurement of response;
equipment, acceleromyograph
The use of neuromuscular blocking drugs in theintensive care unit is commonplace. It is important tomonitor neuromuscular function in the critically illbecause the action of these drugs varies widely in thispopulation.1Tactile assessment of the train-of-four(TOF) is used commonly in anaesthetic practice toassess the degree of block, but there are fewpublished data on tactile assessment of neuromuscu-lar block in the intensive care unit. The majority ofroutine monitoring of vital signs in the intensive careunit is performed by nurses. Our aim was to compare
the accuracy of nurse assessment of TOF responseswith acceleromyography, which is a reproduciblemethod of measurement.
Acceleromyography uses the principle that accel-eration of a contracting muscle is proportional to theforce of contraction (Newtons second law). In a pre-vious study it was demonstrated that a similar accel-eromyography device gave results comparable withthose of a standard mechanometric device (Myo-graph 2000) but there was greater variation inresponses to acceleromyography.2The TOF-Watch(Organon teknika) is an electromyographic device. Itcomprises a standard nerve stimulator and a small
piezoelectric acceleration transducer that is attachedto the thumb. The TOF-Watch enumerates the TOFratio and TOF count on a liquid crystal display.
Methods and results
We investigated 30 stable, sedated adult patientsreceiving an infusion of atracurium in our intensive
care unit. ECG-type electrodes were placed over theulnar nerve of both wrists. The TOF-Watch was usedto obtain acceleromyographic measurements ofneuromuscular block at one thumb (adductor polli-cis). The stimulating leads of the TOF-Watch werethen disconnected and reconnected to similar elec-
trodes on the contralateral wrist when tactile assess-ment was made. In this way the same nerve stimulatorwas used for tactile and acceleromyographic measure-ments at different wrists. We used two wrists to avoiddisplacement of the sensitive acceleration transducerbetween measurements: a small change in positioncould have affected the results. The same stimulatingcurrent was used at both wrists (60 mA). We ensuredthat the electrode position was identical at both wristsand we assigned at random the dominant andnon-dominant hands for measurement. The nursecaring for the patient (nurse A) made a tactile TOFassessment and then a TOF-Watch measurement.
Four subsequent assessments were made by fourdifferent nurses who were blinded to the TOF-Watchresult. At the same time as each tactile assessment,nurse A made a TOF-Watch measurement on thepatients other hand. Each of the four nurses stated thenumber of twitches she could feel in response to aTOF stimulus and if four were palpable she declared aTOF ratio. One minute elapsed between measure-ments. In this way we obtained five pairs of data foreach patient. The nurses were given standard instruc-tions in the simple theory and relevance of neuromus-cular function; however, they were not given practicalexperience in the technique before commencement of
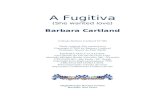
the study.The nurses estimated correctly the twitch count in80 assessments (54%); they overestimated the count in38 assessments (25.3%) and underestimated it in 31(20.6%). Seventeen percent of assessments were inac-curate by two twitches (fig. 1). A Bland and Altmanplot3demonstrated that nurses tended to overestimatethe TOF ratio by a small amount. There was alsogreater variability among the nursing assessment of theTOF ratio than among the TOF-Watch measure-ments. No learning effect could be demonstrated bycomparing the assessments of the first 10 patients andthe last 10.
SHORT COMMUNICATION
R. GREER, MB, BCH, BAO, DGM, N. J. N. HARPER, FRCA, A. J.PEARSON, Intensive Care Unit, Manchester Royal Infirmary,Manchester M13 9WL. Accepted for publication: October 14,1997.
Correspondence to N. J. N. H.
-
7/26/2019 Br. J. Anaesth.-1998-Greer-384-5.pdf
2/2
Neuromuscular monitoring by intensive care nurses 385
Comment
The use of neuromuscular blocking drugs in theintensive care unit is common. However, monitoringof neuromuscular function in the intensive care unitis not performed routinely. It is important to assessthe degree of block in critically ill patients becausethe action of these drugs varies widely in this popu-
lation. Changes in the pharmacokinetics and phar-macodynamics of neuromuscular blocking drugsmay occur and these patients may demonstrateincreased or decreased sensitivity to these agents.Differing degrees of block are required depending onthe clinical indication for the use of neuromuscularblocking agents in the intensive care unit.
Acceleromyography has been described as amethod of measurement of neuromuscular blockduring anaesthesia.4Acceleromyographic and mech-anomyographic measurements of TOF responsescompare well during stable neuromuscular block.Our study of tactile assessment of TOF count found
that the nurses were inaccurate in 45% of measure-ments and the degree of inaccuracy was two twitches
or more in 17% of cases. Underestimation of twitchcount leads to overestimation of the level of block,which may mislead doctors and nurses into reducingthe rate of infusion of atracurium. A patient in whoma deep level of block is required to avoid an increasein intracranial pressure or to improve thoraciccompliance may be put at risk by this course of
events.Measurement of TOF ratio is an important
method of assessing recovery from neuromuscularblock. It has been shown that tactile assessment ofTOF ratio by medical staff is inaccurate at low levelsof block.5Our results demonstrated that nursing stafftended to overestimate TOF ratio. There was alsogreater variability in the assessments by the nursingstaff. Full recovery from neuromuscular block isimportant when it is necessary to make neurologicalor respiratory assessments after a period of block.Underestimation of the degree of block may lead toinaccurate patient assessment and inappropriate
changes in therapy.We suggest that acceleromyography is a useful toolin the intensive care unit. In particular, theTOF-Watch appears to be an appropriate neuromus-cular monitor in this setting. The accuracy of tactileassessment of TOF twitch count and TOF ratio bynursing staff may not be a sufficient basis on which tomake decisions on clinical management in the inten-sive care unit.
References
1. Harper NJN. Neuromuscular blocking drugs: practical
aspects of research in the intensive care unit. Intensive CareMedicine1993; 19: S8085.
2. Harper NJN, Martlew R, Strang T, Wallace M. Monitoring
neuromuscular bock by acceleromyography: comparison ofthe Mini-Accelerograph with the Myograph 2000. British
Journal of Anaesthesia1994; 72: 411414.
3. Bland JM, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurement.
Lancet1986; 1: 307310.
4. Viby-Mogensen J, Jensen E, Werner M, Kirkegaad NielsenH. Measurement of acceleration: an new method of monitor-
ing neuromuscular function. Acta Anaesthesiologica Scandi-navica1988; 32: 4548.
5. Viby Mogensen J, Jensen NH, Engbaek J, Ording H,
Skovgaard LT, Chraemmer-Jorgensen B. Tactile and visual
evaluation of the response to train-of-four nerve stimulation.Anesthesiology1985; 63: 440443.
Figure 1 Degree of inaccuracy with which ICU nurses estimatedthe number of train-of-four responses. A degree of inaccuracy of1, for example, indicates that the nurses were able to feel onefewer response than the number measured by the TOF-Watch.