HIDROCEFALIA CONSEQÜENTE À VARÍOLA INCIDINDO NO PERÍODO FETAL


Camilla A. F. Yamada Oncologista Clínica
Centro Oncológico Bp a Beneficência Portuguesa de São Paulo

Introdução • Complicação rara nos tumores sólidos diagnosticada em
aproximadamente 5% J Neurooncol. 1990;9(3):225.
Neurol Clin. 2003;21(1):25
• Em necrópsias a incidência é muito maior (20%)
Adv Neurol. 1978;19:579
• Coexistência com metastáses cerebrais: em 50-80% das
séries Neurology. 2010;74(18):1449
Breast J. 2012 May;18(3):233-41. Epub 2012 Apr 5 J Thorac Oncol. 2012;7(2):382
Neuro Oncol. 2008 Apr;10(2):199-207. Epub 2008 Feb 2

Introdução • Sem tratamento – sobrevida de 4-6 semanas
Semin Oncol 2009;36(4 Suppl. 2):S46–54.
• Com Tratamento: SM 3-6 meses • Mama 7-12 meses
J Neurooncol 1997;35(1):55–64 Arch Neurol 1994;51(5):457–61
• Melanoma/ pulmão 4 meses Int J Oncol 1996;9(3):505–10.
J Thorac Oncol 2013;8(5):599–605 Lung cancer 2015;89(3):255–61


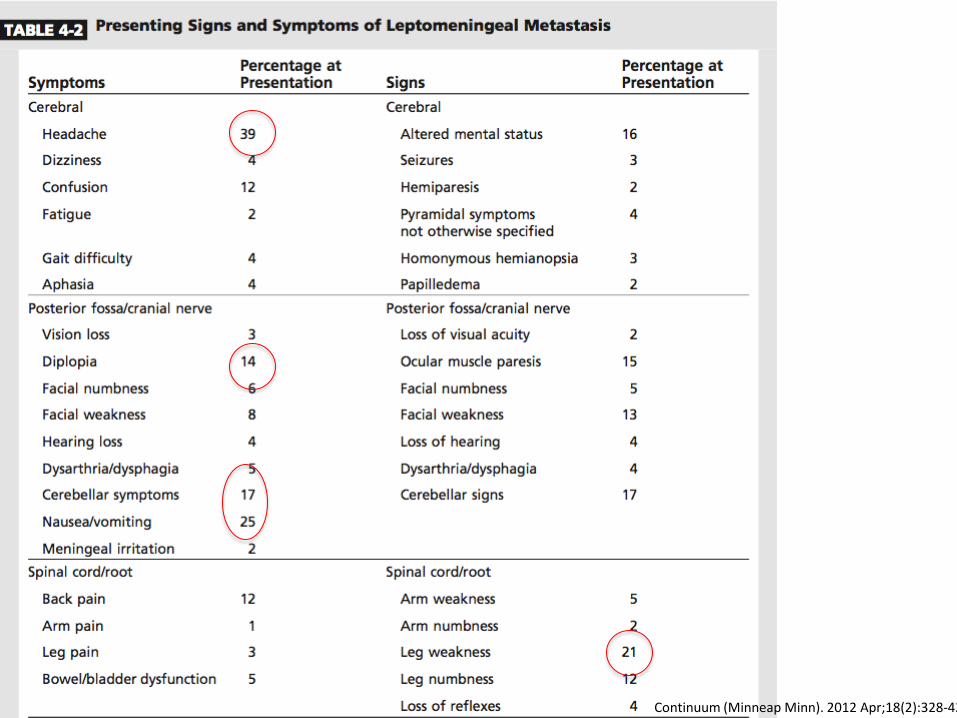
Carcinomatose meningea
Tumores sólidos
Linfomatose meníngea ou meningite linfomatosa
Tumores hematológicos
Gliomatose leptomeníngea
Tumores primários de SNC

Continuum (Minneap Minn). 2012 Apr;18(2):328-42
Título Texto
Continuum (Minneap Minn). 2012 Apr;18(2):328-42

Tratamento • Objetivo
• Estabilizar ou melhorar quadro neurológico
• Prolongar sobrevida • Paliar sintomas
• Estratificação risco • Performance Status • Status neurológico • Extensão doença
oncológica sistêmica e possibilidades terapêuticas
• Extensão doença em SNC


Cirurgia • Colocação de cateter
intraventricular com reservatório para quimioterapia (Ommaya)
• Complicações (9,3% - 10/107) • Infecção (2) • Posicionamento incorreto
(5) • Hemorragia intracraniana
(3) – 2 óbitos Neurosurgery 2000; 47:49-54
• Preferência à punção lombar • Menor variabilidade entre
os pacientes • Potencialmente menor
neurotoxicidade • Melhor distribuição das
drogas • Melhor farmacocinética • Mais confortável
Clin Pharnacokinet 2005;44(1):1-31
Cirurgia
• Derivação ventriculo peritoneal • Indicado para hidrocefalia ou outros sintomas
decorrentes do aumento da pressão intracraniana • Após uso de corticóide altas doses

Radioterapia
• Reservada para tratamento na doença sintomática, principalmente quando doença bulky • Whole Brain – 30-36Gy / 5 x 4Gy (pior PS)
• Obstrução do fluxo liquórico – reestabelece em
30-50% Arch Neurol 1998;55(4):506–12.
Curr Oncol Rep 2003;5(1):24Y28
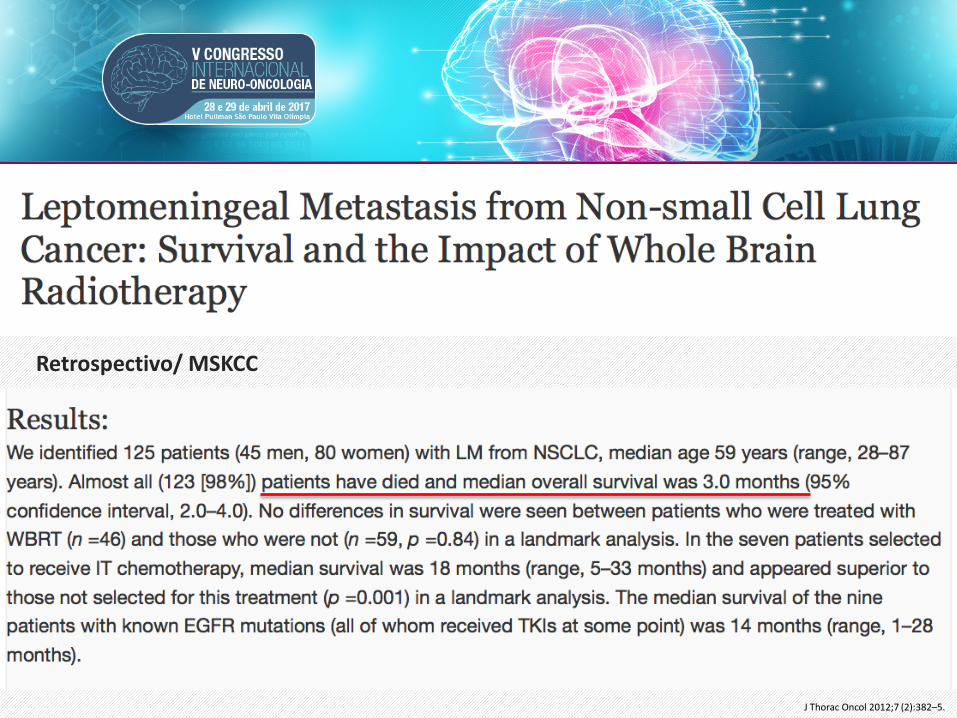
J Thorac Oncol 2012;7 (2):382–5.
Retrospectivo/ MSKCC

Tratamento Intratecal

Quimioterapia Intratecal
• Avaliação fluxo liquórico • Distribuição homogênea da droga –
efetividade e toxicidade • 2/3 dos pacientes podem ter alteração fluxo
liquórico sem evidência de hidrocefalia ou alteração exames de imagem
Am J Med. 1982;73(5):641
Neurology. 1991;41(11):1765. Cancer. 1995;75(12):2919

Quimioterapia Intratecal • Técnica
• Cuidado minimizar mudanças volume LCR
• Remover 15-20mL LCR pré infusão droga
• Sensação pressão retrorbital ou frontal – reposição fluidos, paciente posição supina
• Infusão medicação lenta 2-3 min

Metotrexato
• Mais comumente utilizado • Indução:
• 10-12mg 2x/semana x 4
• Consolidação • 1x/semana x 4 – 8
semanas
NEUROLOGY 1994;44:1463-1469
• Manutenção:
• 1x a a cada 2 semanas x4
• 1x por mês por 2-4 meses
• Solução 4mg/mL em
solução salina 0,9%
Metotrexato • Maior atividade em tumores de mama e
hematológicos • Negativação LCR em 20-60% dos casos • Quando indicado – RT concomitante aumento do risco
de neurotoxicidade • Sobrevida adicional 6 meses respondedores vs 1,8
meses NEUROLOGY 1994;44:1463-1469
J Neurooncol. 1988;6(2):107

Toxicidades
• Mielossupressão: principalmente Irenal; efeito terceiro espaço, alteração fluxo liquórico • Redução risco:
leucovorin 10mg 2x/dia D1-D3
• Neurológicas: • Meningite asséptica: 10%
pacientes. Sintomas após 4 horas da infusão
Blood. 1975;45(2):189
• Leucoencefalopatia – Tardia; >6meses, dose>140mg MTX IT
J Neurol Neurosurg Psychiatry. 1988;51(10):1277
• Encefalopatia aguda • Mielopatia transversa
Singapore Med J. 2007 Feb;48(2):e46-9

Citarabina Lipossomal (DepoCyt®)
• Tumores sólidos e hematológicos
• 50mg IT a cada 2 semanas, sem diluição
• Mantém concentração terapêutica no LCR por mais tempo
• Dados não demonstraram inferioridade administração lombar vs intraventricular
• Maior risco de meningite asséptica – profilaxia com dexametasona 4mg BID 5 dias
Cancer. 2010;116(8):194

Clin Cancer Res. 1999;5(11):3394

The DepoCyt group experienced a greater median time to neurological progression (58 versus 30 days; log-rank P 0.007) and longer neoplastic meningitis-specific survival (log-rank P 0.074; median meningitis-specific survival, 343 versus 98 days). Factors predictive of longer progres- sion-free survival included absence of visible central nervous system disease on neuroimaging studies (P < 0.001), longer pretreatment duration of CSF disease (P < 0.001), history of intraparenchymal tumor (P < 0.001), and treatment with DepoCyt (P 0.002). The frequency and grade of adverse events were comparable between treatment arms. In pa- tients with solid tumor neoplastic meningitis, DepoCyt pro- duced a response rate comparable to that of methotrexate and significantly increased the time to neurological progres- sion while offering the benefit of a less demanding dose schedule.

Breast Cancer Res Treat. 2013 May;139(1):13-22.
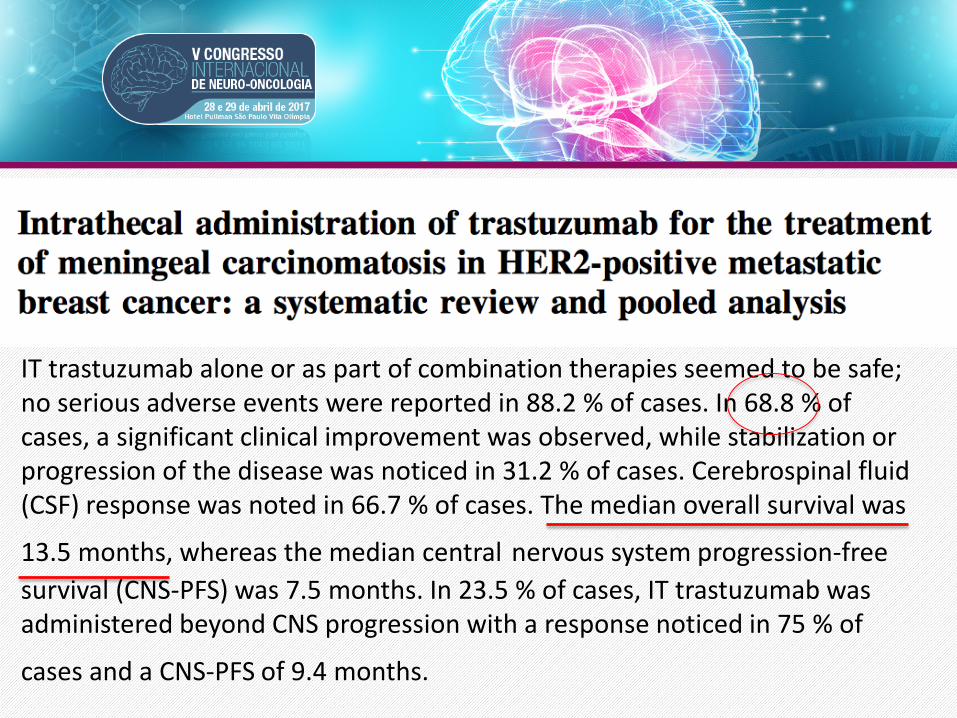
IT trastuzumab alone or as part of combination therapies seemed to be safe; no serious adverse events were reported in 88.2 % of cases. In 68.8 % of cases, a significant clinical improvement was observed, while stabilization or progression of the disease was noticed in 31.2 % of cases. Cerebrospinal fluid (CSF) response was noted in 66.7 % of cases. The median overall survival was
13.5 months, whereas the median central nervous system progression-free survival (CNS-PFS) was 7.5 months. In 23.5 % of cases, IT trastuzumab was administered beyond CNS progression with a response noticed in 75 % of
cases and a CNS-PFS of 9.4 months.

Tratamento Sistêmico

Tratamento Sistêmico
• Atingir concentrações terapêuticas no LCR • Vantagens:
• Não necessita de acesso ventricular • Obstrução fluxo liquórico pode ser tratada • Maior disponibilidade de drogas • Distribuição mais uniforme, com tratamento
da doença bulky


To assess the benefit of intraventricular chemotherapy, patients with leptomeningeal metastasis (LM) from breast cancer were randomised to treatment including intraventricular (IT) chemotherapy (n = 17) or to non-intrathecal (non-IT) treatment (n = 18). Appropriate systemic therapy and involved field radiation therapy (RT) were given in both arms. Intention-to-treat analysis showed neurological improvement or stabilisation in 59% of the IT and in 67% of the non-IT group, with median time to progression of 23 weeks (IT) and 24 weeks (non-IT). Median survival of IT patients was 18.3 weeks and 30.3 weeks for non-IT patients (difference 12.9 weeks; 95% Confidence Interval (CI) −5.5 to +34.3 weeks; P = 0.32). Neurological complications of treatment occurred in 47% (IT) vs 6% (non-IT) (P = 0.0072). In conclusion, standard systemic chemotherapy with involved field RT for LM from breast cancer is feasible. Addition of intraventricular chemotherapy does not lead to survival benefit or improved neurological response, and is associated with an increased risk of neurotoxicity.
Eur J Cancer. 2004;40(18):2726

• QT + IT vs QT • N= 35 pacientes • Melhora neurológica ou
estabilização 59% vs 67% • Tempo médio progressão
23 vs 24 semanas • SM 18,3 vs 30,4 semanas
(p=0,32) Eur J Cancer. 2004;40(18):2726

Tratamento Sistêmico
• Altas doses MTX / Citarabina EV
• Resgate em tumores hematológicos • Papel limitado nos tumores sólidos • Necessário internação (hidratação,
alcalinização urinária, PH urinário de 6/6h, resgate com leucovorin após 24h do MTX mantido 6/6h, dosagem sérica MTX)
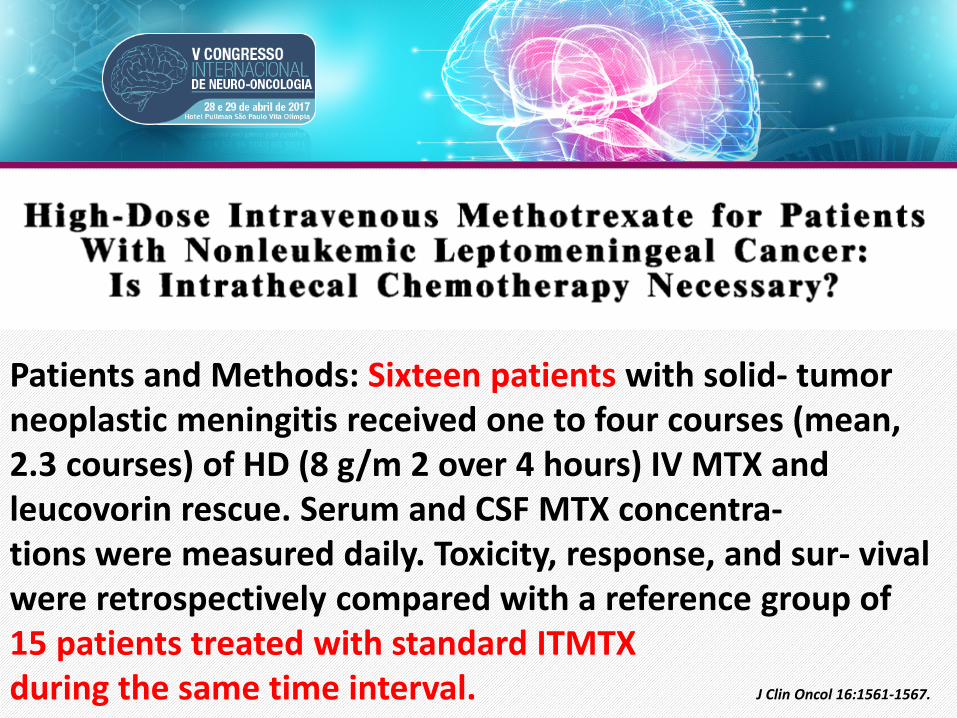
Patients and Methods: Sixteen patients with solid- tumor neoplastic meningitis received one to four courses (mean, 2.3 courses) of HD (8 g/m 2 over 4 hours) IV MTX and leucovorin rescue. Serum and CSF MTX concentra- tions were measured daily. Toxicity, response, and sur- vival were retrospectively compared with a reference group of 15 patients treated with standard ITMTX during the same time interval. J Clin Oncol 16:1561-1567.

Tratamento Sistêmico
• Terapia Alvo – TKI EGFR (Epidermal growth factor receptor) • Erlotinibe, gefitinibe, afatinibe • Adenocarcinoma pulmão com mutação
EGFR (Éxons 18,19 e 21) – em torno 15% dos pacientes
• Mutação adquirida Éxon 20 T790M- osimertinibe

Lung Cancer. 2009;65(1):80
Six patients were alive >6 months, and 2 additional patients were alive 2.5+ and 4.4+ months with clinical improvement. Two patients showed responses to higher than standard dose of gefitinib. The median overall survival was not reached. In conclusion, EGFR TKIs are effective in the treatment of LM from NSCLC when patients were selected properly.

Neuro Oncol 2011;13:1364- 1369
• 1500 mg semanal




Tratamento Sistêmico
• Terapia Alvo – inibidores ALK (Anaplastic lymphoma kinase) • Crizotinibe, ceritinibe, alectinibe • Adenocarcinoma pulmão com rearranjo ALK
em torno 4% dos pacientes

J Clin Oncol. 2015;33(17):1881

Lancet Oncol. 2014;15(10):1119


Relato de caso…. Molecular analyses revealed a V600E BRAF-mutated melanoma. Treatment ensued with whole brain radiotherapy (10 4 Gy), oral lomustine (110 mg/m2), and intrathecal (lumbar) DepoCyte (50 mg once every 14 days). Dur- ing therapy, all CSF samples taken biweekly contained Melan A-positive melanoma cells (Fig 1D) and showed unchanged, elevated cell count (10 to 53/ L), protein (623 to 873 mg/L), and lactate levels (3.3 to 3.7 mmol/L) We initiated second-line therapy with vemurafenib (960 mg twice per day) and stopped all other therapies. Twelve weeks after starting vemurafenib, the patient showed a complete resolution of all clinical symptoms,

Ann Oncol. 2015 Jan;26(1):113-9

Clin Breast Cancer. 2017 Feb;17(1):23-28

The HR -HER2- subgroup had the worst median survival from the time of LM diagnosis of 2.5 months (95% CI, 2.0-3.1) compared with the other subtypes: HR+HER2- , 3.9 months (95% CI, 3.0-5.7), and HR-/+ HER2+ 5.2 months (95% CI, 3.2-7.8) We dichotomized the cohort and examined the median survivals for HER2+ patients. In an exploratory analysis, the median survival was 3.3 months (95% CI, 2.4-5.0) before the year 2005 and 7.0 months (95% CI, 3.7-12.2) thereafter.



Conclusões • Carcinomatose meningea ainda é uma das
complicações nos tumores sólidos de pior prognóstico
• Aumento da incidência talvez pela maior sobrevida dos pacientes, métodos de imagem mais avançados
• Subdiagnosticada
Conclusões
• Melhores evidências • RT doença bulky/ obstrução fluxo liquórico • QT IT com MTX/ Citarabina lipossomal • Otimização tratamento sistêmico
• Perspectivas com novos tratamentos
sistêmicos alvo específicos com penetração em SNC