Do Ripen Em

of 4
Transcript of Do Ripen Em
-
7/31/2019 Do Ripen Em
1/4
V o l . 3 6 S u p p . 3 a u g u S t 2 0 0 7
the d-zone
a monthly supplement toDrug Therapy Topicspublished by the UWDrug Information Center
written by Doug Black, Pharm.D.
Associate Professor, Pharmacy PracticeUW School of Pharmacy &UW Medicine Infectious Disease Service,
also published online athttp://uw.prnrx.org/therapyTopics.asp
Copyright 2007
by the University of Washington
No material may be reproduced in wholeor in part without written permission
from the author.
Black D. Doripenem, the next carbapenem.The D-Zone 2007; 36(Suppl 3) : S9-S12.
A T imely D iscuss ion of conTemporAry An T ib ioT ic & infecT ious D iseAse Top ics
Cms: hi if hisy
Bacterial resistance continues to increase at an alarming rate. The rapid rise to promi-nence o vancomycin-resistant Enterococcus(VRE), penicillin-nonsusceptible Streptococcuspneumoniae(PNSP), and community-acquired methicillin-resistant Staphylococcus aureus(CA-MRSA) has helped uel the recent development o new agents or Gram-positiveinections, such as daptomycin. However, there is also a need or innovative tools tocombat highly resistant Gram-negative pathogens such asAcinetobacter, Enterobacter, andPseudomonas aeruginosa.
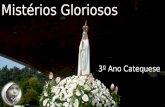
Until the discovery o thienamycin (the rst carbapenem) in the mid-1970s, -lactamdevelopment consisted o dozens o chemical modications to the classical penicillin(penam) and cephalosporin (cephem) nuclei. The carbapenem class can be consid-ered a hybrid o those two nuclei (see Figure 1). Thienamycin, produced by the soilorganism Streptomyces cattleya,was immediately recognized or its exceptionally broadspectrum o activity and resistance to destruction by bacterial -lactamases. Imipenem,the more stable N-ormimidoyl derivative o thienamycin, was unortunately subject torapid conversion in vivo to a nephrotoxic metabolite by mammalian dihydropeptidase I(DHP-1), located in renal proximal tubule cells. However, coadministration o imipenemwith the DHP-1 inhibitor cilastatin prevented this conversion and resulted in a sae andeective product or human use.1
Imipenem received Food and Drug Administration (FDA) approval in 1985.Meropenem, the next carbapenem, was approved in 1996. Advantages o meropeneminclude stability to metabolism by DHP-1 (because o the 1- methyl substituent on thecarbapenem nucleus), slightly greater potency against Gram-negative pathogens thanimipenem (at the expense o decreased Gram-positive activity), and less risk o neurotox-icity.2 Ertapenem, the third carbapenem (approved by the FDA in 2001), has a hal-lieo nearly our hours. This allows or once-daily dosing, which is arguably the drugs besteature. The antibacterial spectrum o ertapenem is limited; notable deciencies includeP. aeruginosa,Acinetobacter, and Enterococcus.3
Recently, the Clinical Laboratory Standards Institute (CLSI) incorporated the carbap-enem class o drugs into a larger grouping known simply as the penems, consisting otwo subclasses, penems and carbapenems (see Figure 2).
Doripenem (S-4661), initially under development in the United States by PeninsulaPharmaceuticals, is now part o Johnson & Johnsons (J&J) Anti-inective Researchand Development portolio ollowing the companys acquisition o Peninsula in 2005.Doripenem is licensed rom Shionogi & Co., Ltd., which launched doripenem in Japanin September, 2005. In June o this year, J&J announced the submission o a New DrugApplication (NDA) to the US FDA or treatment o nosocomial pneumonia. The noso-comial pneumonia indication has been granted ast-track status by the FDA. An NDAor the treatment o complicated intraabdominal inection and complicated urinary tractinection was previously submitted by J&J in December o 2006. Pending regulatoryapproval, the drug will be marketed in the US by Ortho-McNeil, Inc. Doripenem is themajor ocus o this months D-Zone.
Dg bak, pha.D.
th dzDoripenem, the next carbapenemStudy of the Month
I t ft admizd, ppctiv, dubl-
blid, placb-ctlld tial vacmyci vs.
mtidazl t tatmt Clostridium
dicile-aciatd diaa, vacmyci
appa upi v dia.
Zar FA, Bakkanagari SR, Mri KM, a.
A cmpai vacmyci ad mtidazl
t tatmt Clostridium dicile-
aciatd diaa, tatifd by dia
vity. Cli Ict Di 45 3: 302-7, 2007.
Review of the Month
Wagl ad cllagu mpaiz t
imptac cidig pamackitic
ad pamacdyamic picipl w
cig atibitic upi.
Wagnnr FM, Winr W, Nabr KG.
Pamackitic caactitic atimicbial
ad ptimal tatmt upi. Cli
Pamackit 46 4: 291-305, 2007.
Quote of the Month
Iv lad tat ppl will gt watyu aid, ppl will gt wat yu did,
but ppl will v gt w yu
mad tm l.
-Maya Aglu
-
7/31/2019 Do Ripen Em
2/4
Vo l. 3 6 S upp. 3 th e d- Zo N e
Mchism f ci
Doripenem exerts its bactericidal eect by binding to certainpenicillin-binding proteins (PBPs), membrane-associated bacte-rial enzymes involved in peptidoglycan (cell wall) synthesis. Likeother carbapenems, doripenem has the highest binding afnity
or PBP 2.4 Drug binding to PBP 2 produces cell lysis withoutprior flamentation, in contrast to drugs that bind primarily toPBP 3 (such as third-generation cephalosporins). Preerentialbinding to PBP 2 thus results in a smaller increase in cell mass,and consequently less endotoxin release, beore cell death.5
aimici civiy f dim
Pooled MIC90 carbapenem susceptibility data is summarizedin Table 1, adapted rom Zhanel et al.5 Doripenem is similarto imipenem in potency against most common Gram-positiveaerobic organisms, including penicillin-nonsusceptible strainsoS. pneumoniae. No carbapenem demonstrates useul activityagainst E. faecium or MRSA. The activity o doripenem againstGram-negative aerobic organisms is generally equivalent tomeropenem; potency against P. aeruginosa is slightly superior tothe other carbapenems, whereas the activity o doripenem against
Acinetobacteris comparable. Extended-spectrum -lactamase(ESBL) production has little impact on the activity o doripenemagainst Escherichia coliand Klebsiella pneumoniae. Antianaerobicactivity is similar to the other carbapenems.
phmckiics d hmcdymics
Single-dose carbapenem pharmacokinetic parameters appearin Table 2, adapted rom Zhanel et al.5 All currently marketedcarbapenems are or parenteral administration only. The
drugs penetrate most body fuids and tissues well. The highprotein binding o ertapenem results in a prolonged elimina-tion hal-lie that allows or once-daily dosing. Doripenem,imipenem, and meropenem are mainly eliminated in the urineas unchanged drug; 80% o ertapenem appears in the urine,hal as parent compound and hal as the open -lactam ringdegradation product o DHP metabolism. All our drugsrequire some degree o dosage adjustment in renal insuciency.
Fi 1. T cmity t pam, cpm, ad pm9
(rePrInTeD WITh PerMIssIon)
Fi 2. T pm ad cabapm9
(rePrInTeD WITh PerMIssIon)
Ertapenem, imipenem, and meropenem exhibit time-dependentpharmacodynamics; or optimum bactericidal activity, drugconcentrations should exceed the MIC or at least 40% o thedosage interval. Unlike other -lactams, these three carba-
penems also exhibit a postantibiotic eect (PAE) against bothGram-positive and Gram-negative bacteria.5 There arecurrently no published data describing the pharmacodynamicbehavior o doripenem.
Mchisms f sisc
Production o -lactamase is a common bacterial deensemechanism, with over 400 dierent -lactamases describedso ar. However, -lactamases with the ability to hydrolyzecarbapenems (carbapenemases) are relatively rare. -lactamasesare classied into our molecular classes based on amino acidhomology (Ambler class A through D) or unctionally accord-ing to their substrate spectrum and sensitivity to -lactamaseinhibitors (Bush classication scheme). Doripenem, like othercarbapenems, is generally stable toward hydrolysis by Amblerclass A, C, and D enzymes (serine -lactamases), includingESBLs and inducible AmpC -lactamases. However, classA enzymes o Bush group 2 (NMC, IMI, SME, and KPCenzymes) include carbapenems in their substrate prole. Theseenzymes have appeared sporadically in clinical isolates oEnterobacter cloacae, Serratia marcescens, and Klebsiellaspp. sincetheir original discovery in the mid-1980s. The genes encodingthe NMC, IMI, and SME enzymes tend to be located on thebacterial chromosome, whereas the KPC enzymes are encodedon transerable plasmids.6
Doripenem, the next carbapenem (continued)
Pm
Cabapm
-
7/31/2019 Do Ripen Em
3/4
th e d- Zo N e AuGuS t 0 0 7
S n f b a c k n t d Z n a r v i a m a i a b a c k @ . w as i n g n .
encoded enzymes romAeromonasspp., Bacillus cereus, andStenotrophomonas maltophilia. Recently, there has been a signi-cant increase in the detection and spread o readily transerablemetallo--lactamases (VIM, IMP, GIM, and SIM enzymes).
Imipenem resistance in P. aeruginosa results rom loss o theOprD porin (the aqueous channel in the cell membranethrough which the drug gains access to the interior) coupledwith activity o AmpC -lactamase.5 In act, porin loss is themost common mechanism associated with imipenem resistancein P. aeruginosa. Doripenem (and meropenem) appear toadditionally require the expression o drug efux pumps orresistance to be conerred, which may help explain the superiorantipseudomonal activity o these two carbapenems.
Ciic is
There are currently no clinical trials o doripenem publishedin the medical literature. A study comparing doripenem to
meropenem or the treatment o complicated intraabdominalinection was summarized at the 46th annual InterscienceConerence on Antimicrobial Agents and Chemotherapy(ICAAC) meeting in San Francisco in 2006. Using a prospec-tive, multicenter, double-blind, double-dummy study design,486 patients diagnosed with complicated intraabdominalinection were randomized to treatment with doripenem (500mg IV q8h over 60 minutes) or meropenem (1 gm IV q8hover 35 minutes). Ater nine or more doses o intravenousstudy drug, patients could be switched to oral therapy(amoxicillin/clavulanic acid 875/125 mg PO bid) i speciccriteria were met; total study duration was 514 days. In the
microbiologically evaluable patients (baseline pathogen isolatedrom an abdominal culture) at the test-o-cure (TOC) visit(2842 days ater the last dose o study drug), the clinical curerate was 83.3% or doripenem versus 83.0% or meropenem.Microbiologic eradication rates in the treatment arms at theTOC visit were also comparable.8
advs ffcs
Inormation about adverse eects o doripenem is limited. Inthe intraabdominal inection trial summarized above, the mostcommon adverse eects in doripenem-treated patients werenausea (9.5%, vs. 9.4% with meropenem), diarrhea (7.4%, vs.7.7% with meropenem), anemia (7.0%, vs. 3.9% with merope-
nem), and vomiting (6.6%, vs. 6.9% with meropenem).8
-lactam antibiotics in high doses have been associated withseizures, possibly due to inhibition o gamma-aminobutyricacid (GABA) receptor binding.9 Carbapenem anity or theGABAAreceptor correlates with the relative basicity o theR-2 side chain (see Figure 2): the more basic the side chain,the more neurotoxic the drug. Based on this observation, therelative neuroexcitatory potential o the three antipseudomonalcarbapenems would be imipenem > meropenem > doripenem.Although conrmatory human data are lacking, doripenemproduced no proconvulsive activity in rats ollowing intrave-nous or intracerebroventricular administration.10
t 1. In vitro cm civiy (MIC90)5
DorIPeneM erTAPeneM IMIPeneM MeroPeneM
graM-poSItIVe aerobeS
Enterococcus aecalis 8 16 4 16
Enterococcus aecium >16 >16 >8 >16
Listeria monocytogenes nA 0.5 0.12 0.12
Streptococcus agalactiae 0.016 0.06 0.016 0.06
Streptococcus pneumoniae (PSSP) 0.008 0.015 0.008 0.008
Streptococcus pneumoniae (PISP) 0.25 1 0.12 0.5
Streptococcus pneumoniae (PNSP) 1 2 1 1
Streptococcus pyogenes 0.008 0.008 0.008 0.008
Staphylococcus aureus (MSSA) 0.06 0.25 0.5 0.12
Staphylococcus aureus (MRSA) 16 >32 32 32
graM-negatIVe aerobeS
Acinetobacterspp. 1 >8 0.25 1
Citrobacter reundii 0.03 0.015 1 0.03
Enterobacter cloacae 0.06 0.06 2 0.06
Escherichia coli 0.03 0.06 0.5 0.03
Escherichia coli(ESBL-producing) 0.06 0.25 0.5 0.06
Haemophilus infuenzae 0.5 0.12 4 0.25
Klebsiella oxytoca 0.06 0.015 0.5 0.03Klebsiella pneumoniae 0.06 0.06 1 0.03
Klebsiella pneumoniae (ESBL-producing) 0.12 0.5 1 0.12
Moraxella catarrhalis 0.03 0.008 0.12 0.008
Morganella morganii 0.5 0.03 4 0.12
Neisseria gonorrhoeae nA 0.03 0.016 nA
Proteus mirabilis 0.25 0.06 2 0.06
Proteus vulgaris 0.5 0.25 4 0.12
Pseudomonas aeruginosa 8 >8 >8 16
Salmonella spp. 0.06 0.06 0.5 0.03
Serratia marcescens 0.25 0.12 2 0.06
Shigella spp. 0.06 0.06 0.5 0.03
Stenotrophomonas maltophilia >16 >8 >8 >16
anaerobeS
Bacteroides ragilis 1 0.5 0.5 0.5Clostridium dicile 2 4 4 4
Clostridium perringens nA 0.06 0.12 0.06
Fusobacterium spp. 1 1 1 0.12
Peptostreptococcus spp. nA 0.12 0.06 0.12
Prevotella spp. 0.25 4 0.5 0.25
gloSSarY:
nA =information not available
S. pneumoniae: PSSP = penicillin-susceptible, PISP = intermediate-susceptible, PNSP = non-susceptible
S. aureus: MSSA = methicillin-susceptible, MRSA = methicillin-resistant
esBL = extended-spectrum -lactamase
Queenan et al. investigated the ability o imipenem, merope-
nem, and doripenem (along with ceoxitin and cetazidime)to induce AmpC expression in various Enterobacteriaceae andP. aeruginosa. Ceoxitin was the strongest inducer, ollowed byimipenem. Doripenem and meropenem were similar in theirinduction proles and at least two-old less than imipenem.Cetazidime, as expected, was weakest.7
Doripenem and other carbapenems are naturally susceptibleto hydrolysis by Ambler class B enzymes, also known asBush group 3 enzymes or zinc metallo--lactamases. Theseenzymes possess broad substrate specicity and resistanceto commercially available -lactamase inhibitors. The rstmetallo--lactamases widely studied were chromosomally
Doripenem, the next carbapenem (continued)
-
7/31/2019 Do Ripen Em
4/4
Vo l. 3 6 S upp. 3 th e d- Zo N e
D icis
No drug interactions in humans involving doripenem havebeen reported. Meropenem reduces plasma concentrationso valproic acid, apparently by enhancing glucuronidation;this interaction has also been reported with imipenem andertapenem.11 Doripenem has been shown to decrease valproic
acid concentrations in animals.12
oh ms
Biapenem and panipenem have been marketed in Asia but arenot undergoing development or other markets. Tebipenem, anorally active carbapenem, is currently in phase II study in Japan.
Faropenem medoxomil is an orally active penem (see Figure 2).The bioavailability o the original sodium salt was 2030%,but ormulation as an ester boosts oral bioavailability to7080%. Other eatures o aropenem medoxomil includereliable -lactamase stability (including ESBLs and AmpC-lactamases), low induction potential, and a marked PAE
against S. pneumoniaeand other organisms. The drug, whichlacks antipseudomonal activity, has an attractive antibacterialspectrum or ambulatory patients.13
These eatures suggest a role or aropenem medoxomil asswitch therapy or step-down therapy. However, in late2006 the FDA issued a non-approvable letter to Replidyne, thecompany developing aropenem medoxomil or use in the US,recommending urther clinical study.
Ccsi
Doripenem is a new, well-tolerated parenteral carbapenem thatcombines the Gram-positive activity o imipenem with theGram-negative activity o meropenem. The drug lacks activityagainst pathogens that are typically carbapenem-resistant.Whether the improved antipseudomonal potency o doripenemoers clinical benet is not known. Data concerning cross-resistance between doripenem and the other carbapenems ornonermenting Gram-negative bacilli such asAcinetobacterwillbe helpul. Pricing inormation is not yet available.
rfcs
Barza M. Imipenem: rst o a new class o beta-lactam antibiotics.Ann Intern Med. Oct 1985;103(4):552560.
Hurst M, Lamb HM. Meropenem: a review o its use in patients inintensive care. Drugs. 2000;59(3):653680.
Odenholt I. Ertapenem: a new carbapenem. Expert Opin InvestigDrugs. Jun 2001;10(6):11571166.
Davies TA, Shang W, Bush K, et al. Binding o doripenem andcomparators to penicillin-binding proteins in Escherichia coli andPseudomonas aeruginosa [abstract no. C1-0039]. Paper presentedat: 46th Interscience Conerence on Antimicrobial Agents andChemotherapy; Sept 2730, 2006; San Francisco, CA.
Zhanel GG, Wiebe R, Dilay L, et a l. Comparative review o thecarbapenems. Drugs. 2007;67(7):10271052.
Queenan AM, Bush K. Carbapenemases: the versatile beta-lac-tamases. Clin Microbiol Rev. Jul 2007;20(3):440458.
Queenan AM, Shang W, Flamm RK, et al. Eect o doripenem onAmpC induction in Enterobacteriaceae and Pseudomonas aeruginosa[abstract no. C1-0040]. Paper presented at: 46th InterscienceConerence on Antimicrobial Agents and Chemotherapy; Sept2730, 2006; San Francisco, CA.
1.
2.
3.
4.
5.
6.
7.
t 2. Sids cm hmckiics5
D gm Cmax g/ml AUC mg/L t1/2 Vd L/kg % pti bud% xctd i uia ucagd dug
DorIpeneM 0.5 20.2 44.1 0.93 nA 8.9 75
ertapeneM* 1 154.9 22.0 572.1 68.6 3.8 8.2 1.5 9295 44
IMIpeneM 0.5 3035 42.2 1 0.230.31 20 6070
MeropeneM 1 5060 66.977.5 1 0.230.35 2 70
*valu cpdig t dug a i pat
nA = t availabl
Malaaia O, Umeh O, Jiang J. Doripenem versus meropenem orthe treatment o complicated intra-abdominal inections [abstractno. L-1564b]. Paper presented at: 46th Interscience Conerence on
Antimicrobial Agents and Chemotherapy; Sept 2730, 2006; SanFrancisco, CA.
Dalho A, Janjic N, Echols R. Redening penems. BiochemPharmacol. Mar 30 2006;71(7):10851095.
Horiuchi M, Kimura M, Tokumura M, et al. Absence oconvulsive liability o doripenem, a new carbapenem antibiotic,in comparison with beta-lactam antibiotics. Toxicology. May 12006;222(12):114124.
Spriet I, Goyens J, Meersseman W, et al. Interaction bet weenvalproate and meropenem: a retrospective study. Ann Pharmacother.
Jul 2007;41(7):11301136.
Nakajima Y, Mizobuchi M, Nakamura M, et al. Mechanismo the drug interaction between valproic acid and carbap-enem antibiotics in monkeys and rats. Drug Metab Dispos. Dec2004;32(12):13831391.
Hamilton-Miller JM. Chemical and microbiologic aspects openems, a distinct class o beta-lactams: ocus on aropenem.
Pharmacotherapy. Nov 2003;23(11):14971507.
8.
9.
10.
11.
12.
13.
Doripenem, the next carbapenem (continued)











![O papel do alfabetismo em saúde no controle do diabetes em … · 2017-11-09 · O papel do alfabetismo em saúde no controle do diabetes em idosos. [Tese]. São Paulo: Faculdade](https://static.fdocumentos.com/doc/165x107/5f38f9b781548324c379568c/o-papel-do-alfabetismo-em-sade-no-controle-do-diabetes-em-2017-11-09-o-papel.jpg)