Eduardo M. Rego Faculdade de Medicina de Ribeirão Preto - USP · identificação da PML/RARA !! IF...
94
Eduardo M. Rego Faculdade de Medicina de Ribeirão Preto - USP
Transcript of Eduardo M. Rego Faculdade de Medicina de Ribeirão Preto - USP · identificação da PML/RARA !! IF...
Eduardo M. Rego
Faculdade de Medicina de Ribeirão Preto - USP
!! Grupo de doenças caracterizado pela expansão clonal de células miéloides imaturas na medula óssea, sangue, ou outros tecidos
!! São doenças genéticas, na maioria das vezes de caráter esporádico, associadas à anormalidades citogenéticas (40-50%) e/ou gênicas (50-60%)
Vardiman JW, et al. Blood. 2009;114(5):937.
!! Percentagem de blastos na M.O. ou sangue ! 20% "! Mieloblastos "! Monoblastos + Promonócitos "! Megacarioblastos
!! Sarcoma granulocítico (a menos que haja história prévia de MDS/NMP ou NMP)
!! Demonstração de anormalidades citogéneticas específicas
!! Quando os precursores eritróides ! 50% + mieloblastos ! 20% das células não eritróides
Vardiman JW, et al. Blood. 2009;114(5):937.
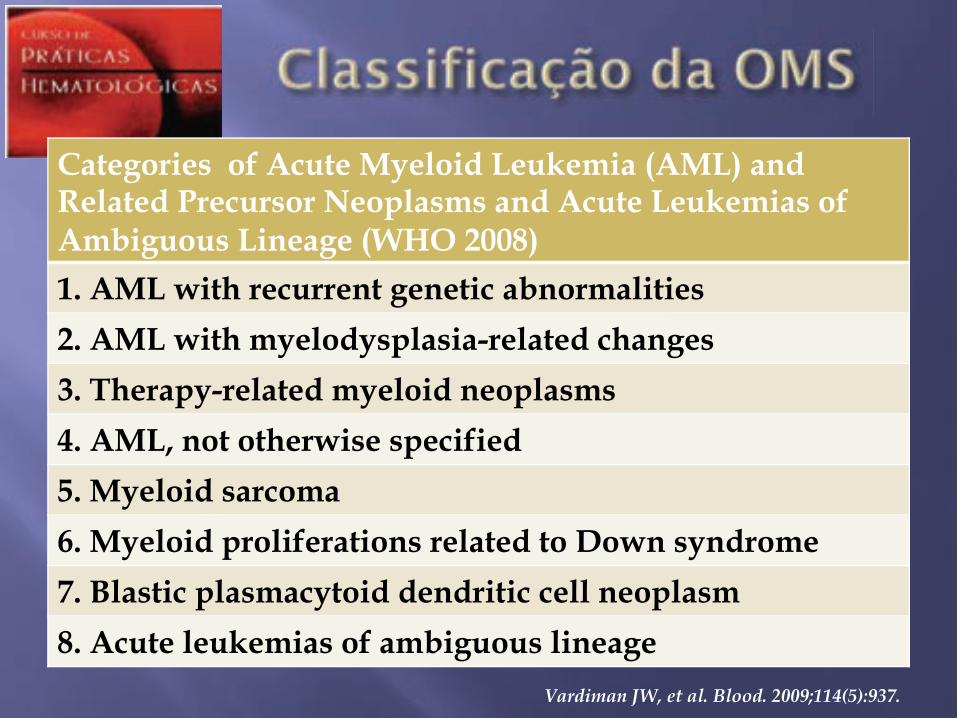
Categories of Acute Myeloid Leukemia (AML) and Related Precursor Neoplasms and Acute Leukemias of Ambiguous Lineage (WHO 2008)
1. AML with recurrent genetic abnormalities
2. AML with myelodysplasia-related changes
3. Therapy-related myeloid neoplasms
4. AML, not otherwise specified
5. Myeloid sarcoma
6. Myeloid proliferations related to Down syndrome
7. Blastic plasmacytoid dendritic cell neoplasm
8. Acute leukemias of ambiguous lineage Vardiman JW, et al. Blood. 2009;114(5):937.
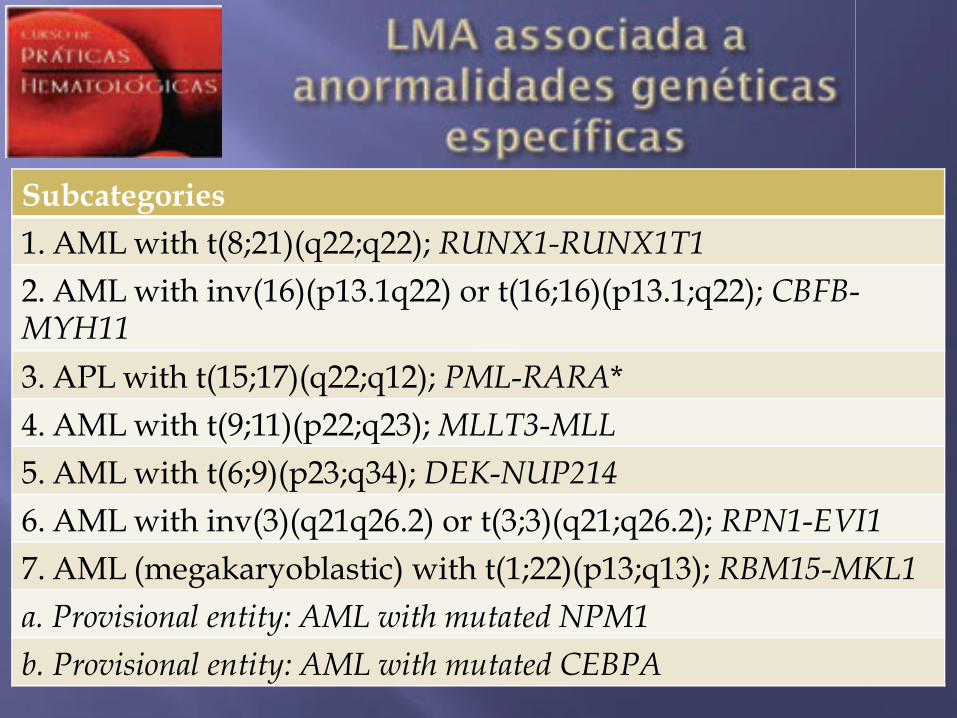
Subcategories
1. AML with t(8;21)(q22;q22); RUNX1-RUNX1T1 2. AML with inv(16)(p13.1q22) or t(16;16)(p13.1;q22); CBFB-MYH11 3. APL with t(15;17)(q22;q12); PML-RARA* 4. AML with t(9;11)(p22;q23); MLLT3-MLL 5. AML with t(6;9)(p23;q34); DEK-NUP214 6. AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); RPN1-EVI1 7. AML (megakaryoblastic) with t(1;22)(p13;q13); RBM15-MKL1 a. Provisional entity: AML with mutated NPM1 b. Provisional entity: AML with mutated CEBPA
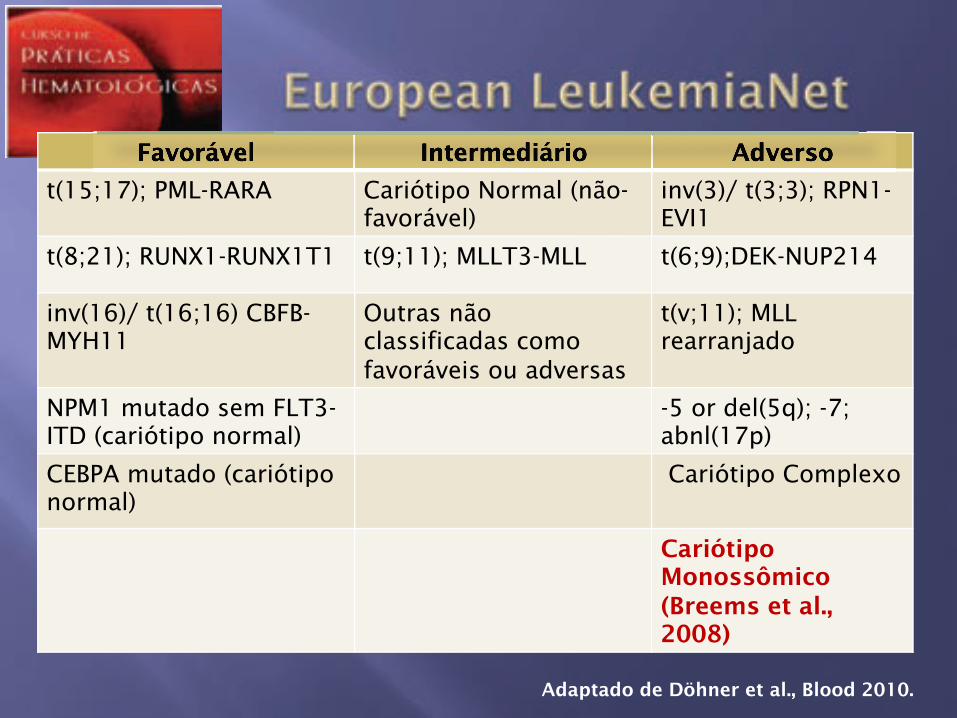
Favorável Intermediário Adverso
t(15;17); PML-RARA
Cariótipo Normal (não-favorável)
inv(3)/ t(3;3); RPN1-EVI1
t(8;21); RUNX1-RUNX1T1 t(9;11); MLLT3-MLL t(6;9);DEK-NUP214
inv(16)/ t(16;16) CBFB-MYH11
Outras não classificadas como favoráveis ou adversas
t(v;11); MLL rearranjado
NPM1 mutado sem FLT3-ITD (cariótipo normal)
-5 or del(5q); -7; abnl(17p)
CEBPA mutado (cariótipo normal)
Cariótipo Complexo
Cariótipo Monossômico (Breems et al., 2008)
Adaptado de Döhner et al., Blood 2010.
Favorável Intermediário Adverso
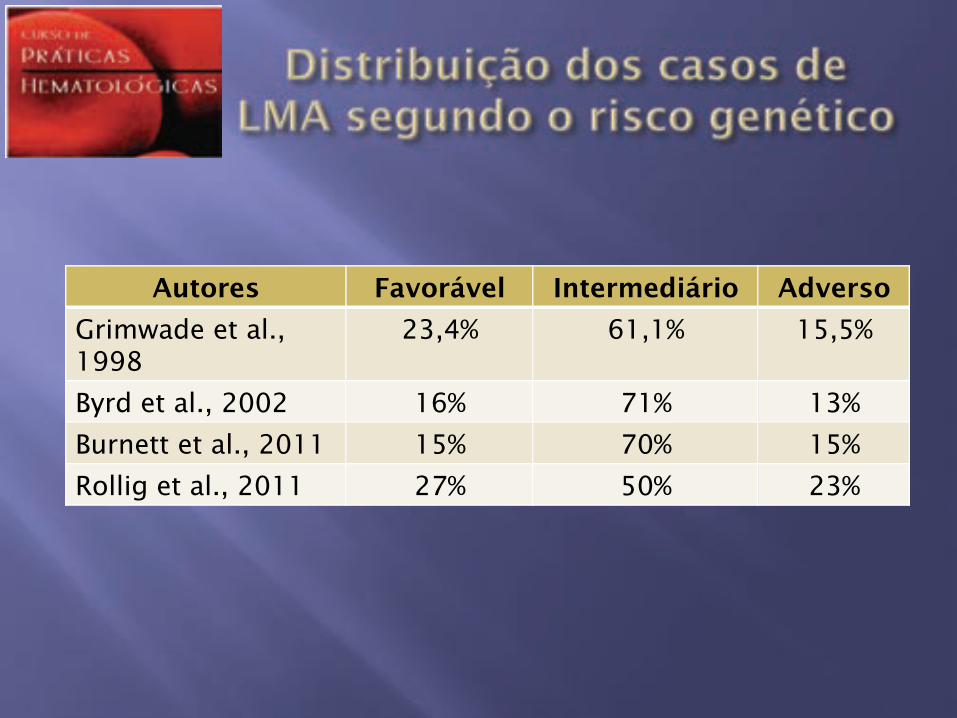
Autores Favorável Intermediário Adverso
Grimwade et al., 1998
23,4% 61,1% 15,5%
Byrd et al., 2002 16% 71% 13%
Burnett et al., 2011 15% 70% 15%
Rollig et al., 2011 27% 50% 23%
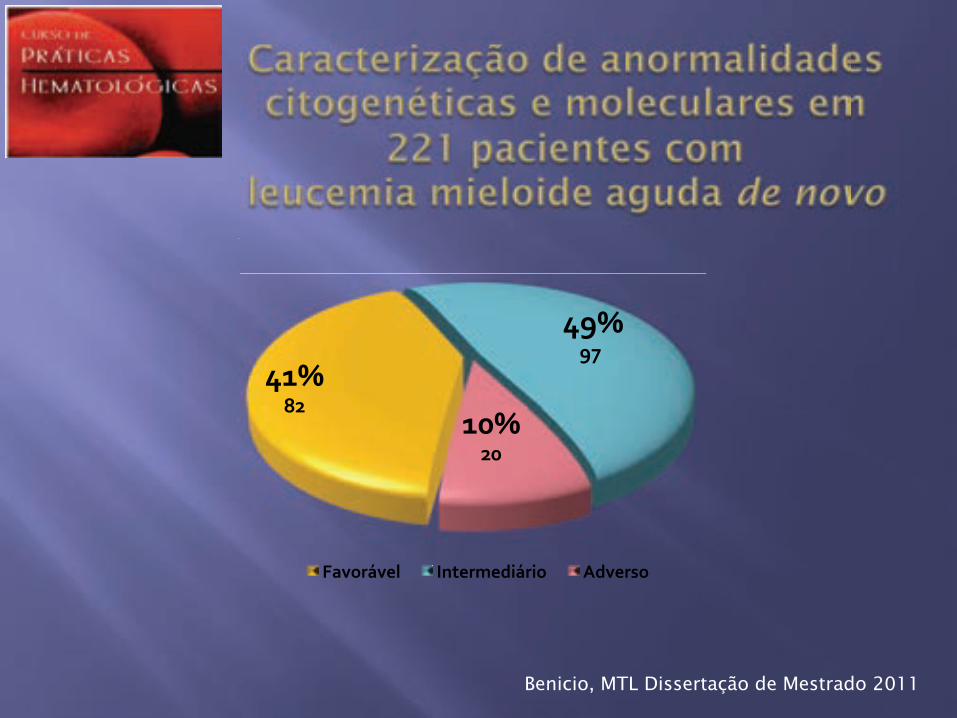
!"#$%&$
$!'#$'($
")#$&)$
*+,-./,01$ 2340.5067/.7-$ 86,0.9-$
Benicio, MTL Dissertação de Mestrado 2011
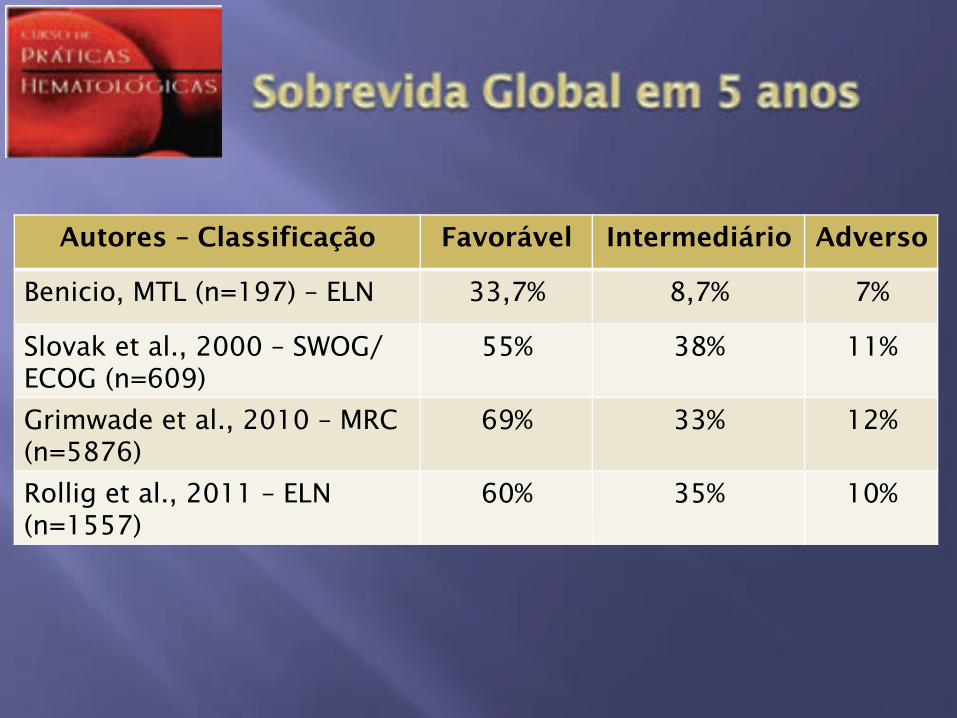
Autores – Classificação Favorável Intermediário Adverso
Benicio, MTL (n=197) – ELN 33,7% 8,7% 7%
Slovak et al., 2000 – SWOG/ECOG (n=609)
55% 38% 11%
Grimwade et al., 2010 – MRC (n=5876)
69% 33% 12%
Rollig et al., 2011 – ELN (n=1557)
60% 35% 10%
“ It is important to consider diagnostic suspicion of APL as a medical emergency (uncommon in AML) that requires several specific and simultaneous actions, including immediate commencement of ATRA therapy, prompt genetic diagnosis and measures to counteract the coagulopathy”.
Sanz et al. Blood 2009;113:1875-1891

!! Características imunofenotípicas sugestivas de LPA: "! Perda da expressão do CD34 e do HLA-DR
"! Elevado Side Scatter (SSC)
"! Expressão homogênea do CD33
"! Expressão heterogênea do CD13
"! Expressão muito frequente das moléculas de adesão CD11a/CD18
"! Ausência ou baixa expressão CD11b e CD11c
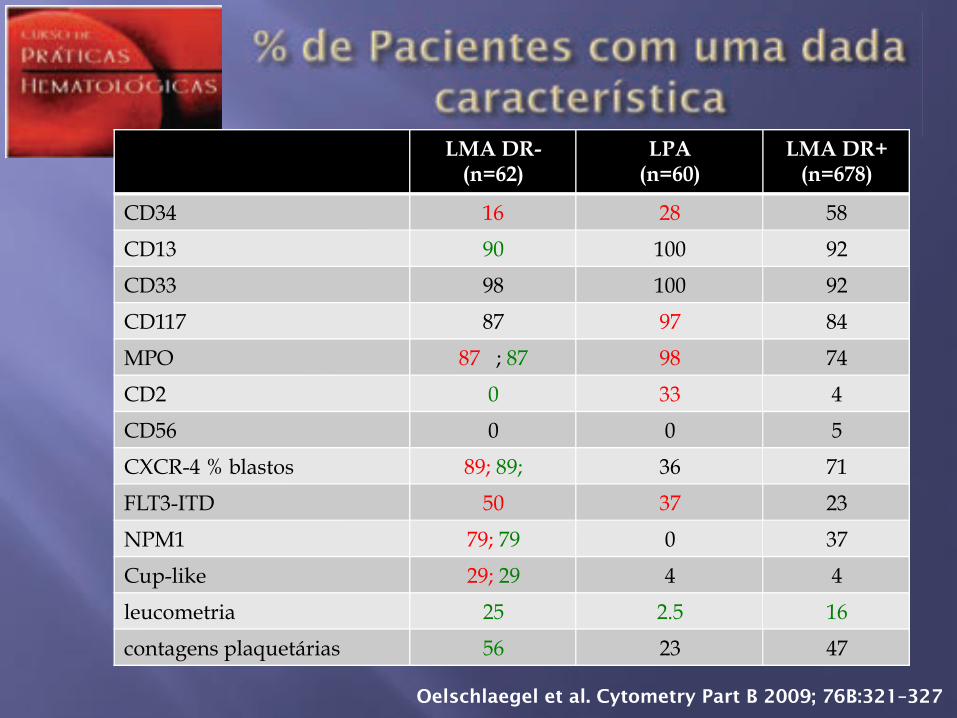
LMA DR- (n=62)
LPA (n=60)
LMA DR+ (n=678)
CD34 16 28 58
CD13 90 100 92
CD33 98 100 92
CD117 87 97 84
MPO 87 ; 87 98 74
CD2 0 33 4
CD56 0 0 5
CXCR-4 % blastos 89; 89; 36 71
FLT3-ITD 50 37 23
NPM1 79; 79 0 37
Cup-like 29; 29 4 4
leucometria 25 2.5 16
contagens plaquetárias 56 23 47
Oelschlaegel et al. Cytometry Part B 2009; 76B:321–327
!! Embora a morfologia e a imunofenotipagem sejam úteis na suspeita do diagnóstico da leucemia promielocítica aguda a confirmação genética é obrigatória.
!! Esta pode ser feita: "! Citogenética clássica
"! RT-PCR
"! FISH
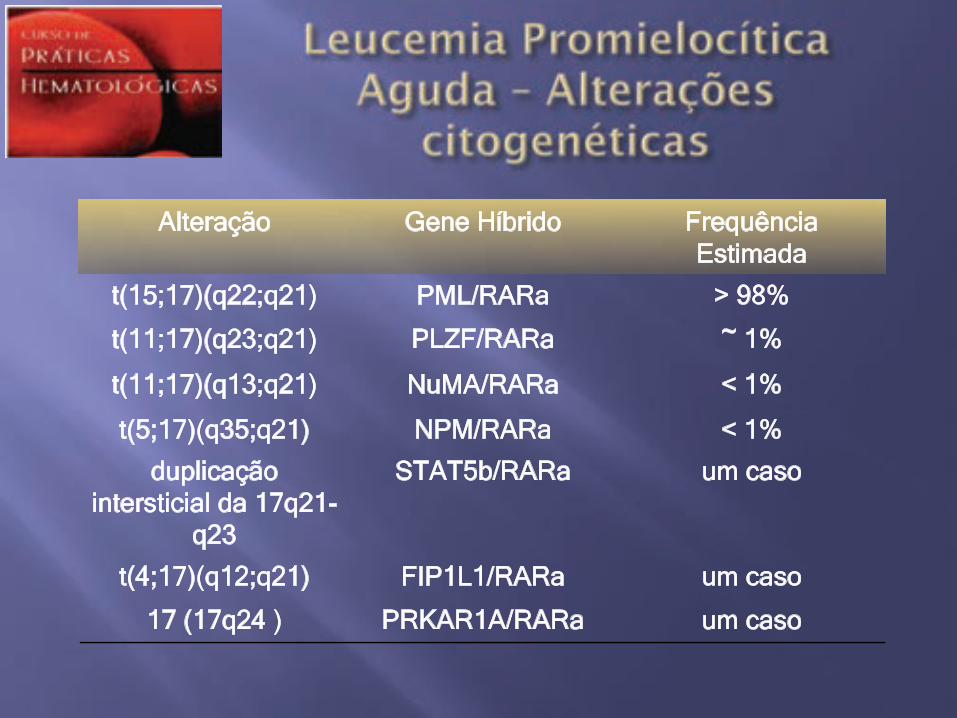
Alteração Gene Híbrido Frequência Estimada
t(15;17)(q22;q21) PML/RARa > 98%
t(11;17)(q23;q21) PLZF/RARa ~ 1%
t(11;17)(q13;q21) NuMA/RARa < 1%
t(5;17)(q35;q21) NPM/RARa < 1%
duplicação intersticial da 17q21-
q23
STAT5b/RARa um caso
t(4;17)(q12;q21) FIP1L1/RARa um caso
17 (17q24 ) PRKAR1A/RARa um caso
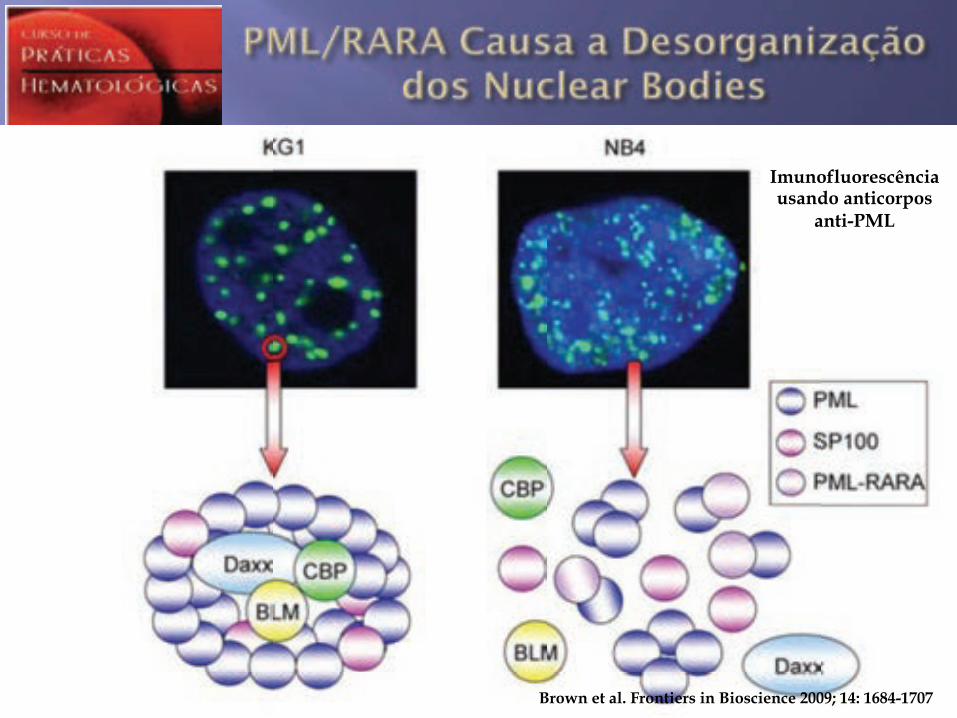
Brown et al. Frontiers in Bioscience 2009; 14: 1684-1707
Imunofluorescência usando anticorpos
anti-PML
!! Dimov et al. analizaram 199 casos de LPA e 150 casos de LMA e compararam a imunofluorescência com anti-PML com citogenética, FISH e RT-PCR para identificação da PML/RARA
!! IF c/ anti-PML foi + 182 dos 184 aspirados de M.O. e 32 dos 33 esfregaços de sangue de pacientes com LPA
!! A sensibilidade e a especificidade foram de 98.9% e 98.7%, respectivamente
Dimov et al. Cancer 2010;116:369–76 Falini et al. Blood. 1997;90: 4046-4053.
!! Consórcio Internacional para Tratamento da Leucemia Promielocítica Aguda (IC-APL) "! Protocolo adaptado aos recursos disponíveis
!! Daunorubicina como antracíclico !! ATRA
"! Multicêntrico, internacional e baseado no conceito de rede (networking) !! Base de dados usando ferramentas via internet !! Reuniões/Discussões de casos via internet
"! Diagnóstico rápido (IF com anti-PML) "! Consolidação adaptado ao risco (PETHEMA) "! Biobanco
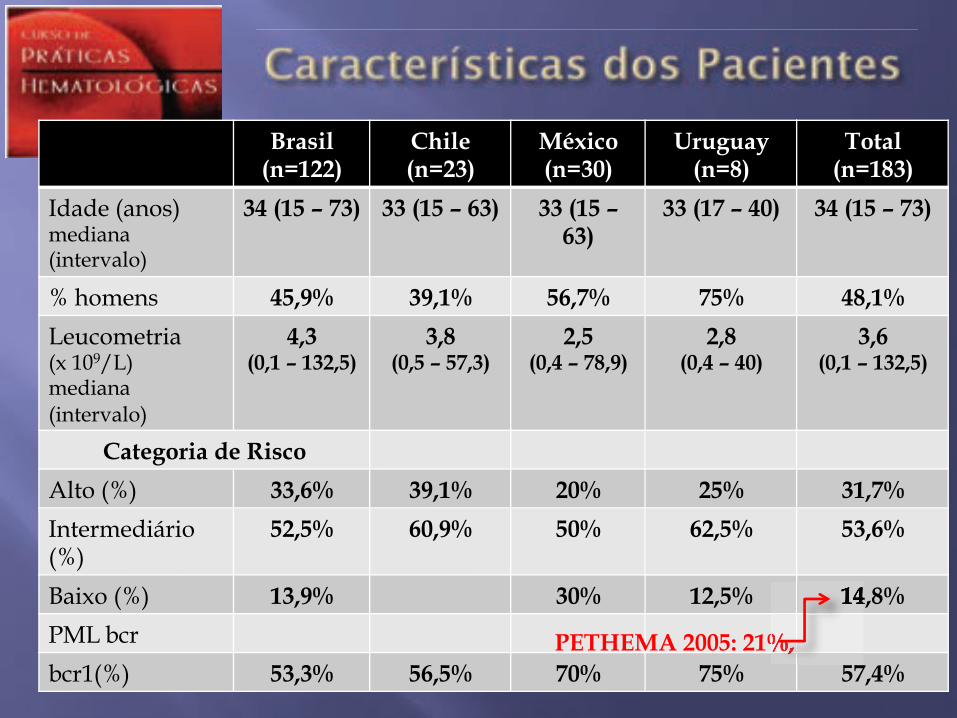
Brasil (n=122)
Chile (n=23)
México (n=30)
Uruguay (n=8)
Total (n=183)
Idade (anos) mediana (intervalo)
34 (15 – 73) 33 (15 – 63) 33 (15 – 63)
33 (17 – 40) 34 (15 – 73)
% homens 45,9% 39,1% 56,7% 75% 48,1%
Leucometria (x 109/L) mediana (intervalo)
4,3 (0,1 – 132,5)
3,8 (0,5 – 57,3)
2,5 (0,4 – 78,9)
2,8 (0,4 – 40)
3,6 (0,1 – 132,5)
Categoria de Risco
Alto (%) 33,6% 39,1% 20% 25% 31,7%
Intermediário (%)
52,5% 60,9% 50% 62,5% 53,6%
Baixo (%) 13,9% 30% 12,5% 14,8%
PML bcr
bcr1(%) 53,3% 56,5% 70% 75% 57,4% PETHEMA 2005: 21%,
14,8%
PETHEMA 2005: 21%, PETHEMA 2005: 21%, PETHEMA 2005: 21%, PETHEMA 2005: 21%, PETHEMA 2005: 21%, PETHEMA 2005: 21%, PETHEMA 2005: 21%,
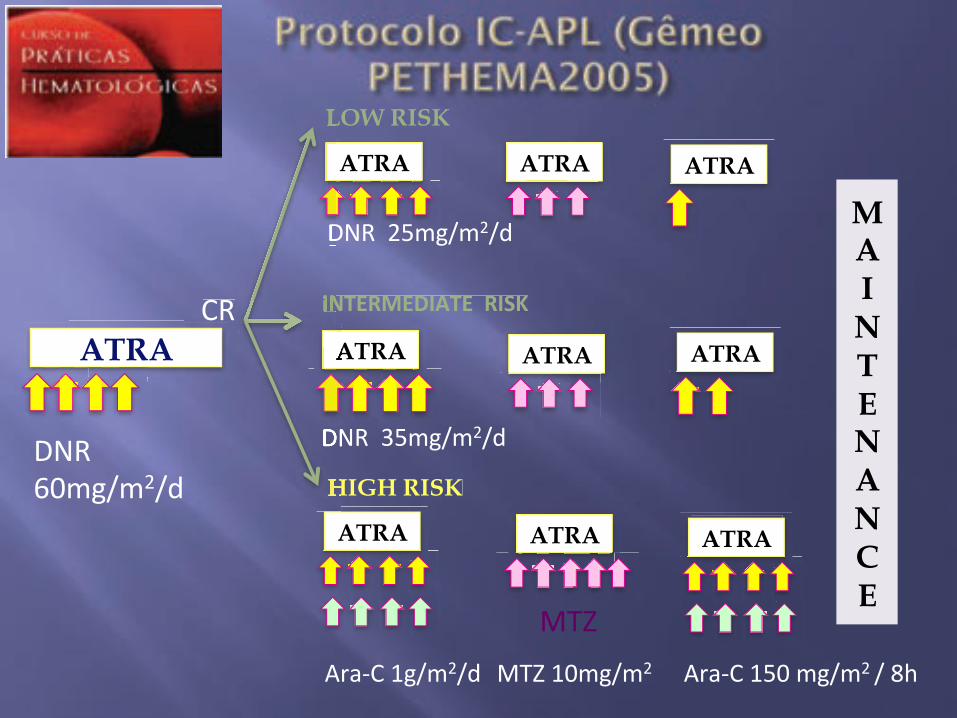
ATRA !"#
ATRA
ATRA
ATRA
$%"##&'()*(+*,#
-./0!#1)*(+*,#
LOW RISK
!"#$%&$'!(#$))%!*+)
HIGH RISK
ATRA
ATRA
ATRA ATRA
234#-./0!#15'#()*(+#*#67#
ATRA
$%"##+5()*(+*,#
$%"##85()*(+*,#
ATRA
M A I N T E N A N C E
LOW RISK LOW RISK
!"#$%&$'!(#$))%!*+)
$%"##+5()*($%"##+5()*(
!"#$%&$'!(#$))%!*+)
ATRA
HIGH RISK
$%"##85()*(
234#1'()*(+#
!! ATRA 45 mg/m2/d x 15dias a cada 3 meses
!! Metotrexate 15 mg/m2/d (1x/sem)
!! 6-mercaptopurina 50 mg/m2/d
!! Duração de 2 anos
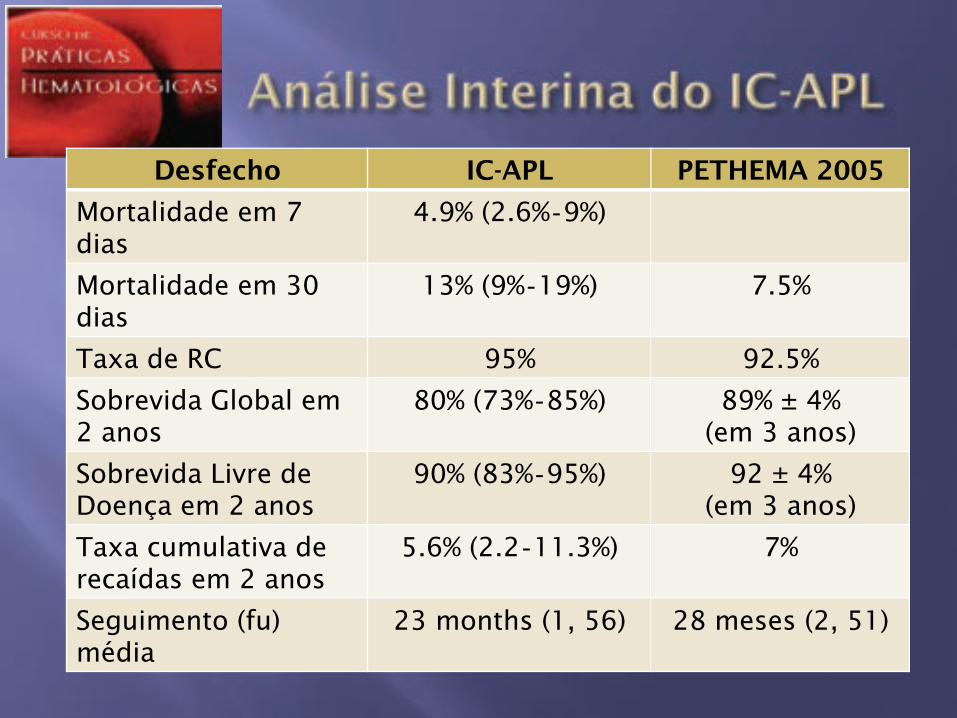
Desfecho IC-APL PETHEMA 2005
Mortalidade em 7 dias
4.9% (2.6% 9%)
Mortalidade em 30 dias
13% (9% 19%) 7.5%
Taxa de RC 95% 92.5%
Sobrevida Global em 2 anos
80% (73% 85%) 89% ± 4% (em 3 anos)
Sobrevida Livre de Doença em 2 anos
90% (83% 95%) 92 ± 4% (em 3 anos)
Taxa cumulativa de recaídas em 2 anos
5.6% (2.2 11.3%) 7%
Seguimento (fu) média
23 months (1, 56) 28 meses (2, 51)
!! M.D. Anderson !! Duas coortes:
"! n=47; ATRA (45 mg/m2/d) e ATO (0.15 mg/kg/d começando no D10 do ATRA). Pacientes de alto risco recebiam tb Gentuzimab (GO) 9 mg/m2 no 10 dia da indução)
"! n=45; ATRA + ATO concomitantes a partir do D1
!! Consolidação 4 ciclos de ATO, 1x/dia por 5d/sem por 4 semanas em meses alternados + ATRA quinze dias sim, quinze não, por um total de 28 semanas após CR.
Ravandi et al. 15th EHA meeting Abstract 0545
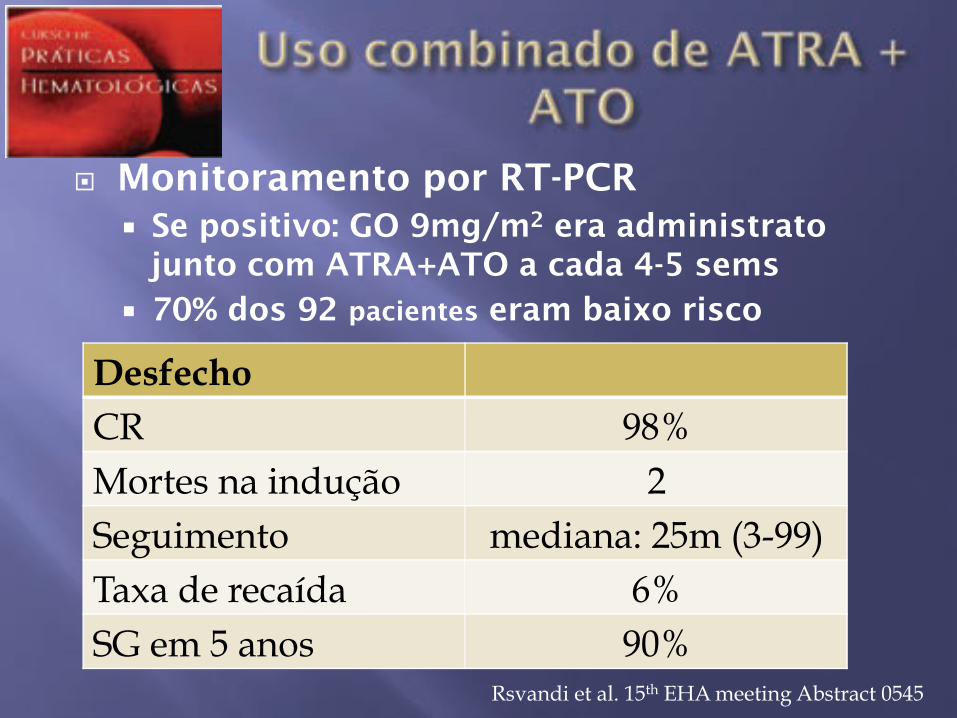
!! Monitoramento por RT-PCR "! Se positivo: GO 9mg/m2 era administrato
junto com ATRA+ATO a cada 4-5 sems "! 70% dos 92 pacientes eram baixo risco
Desfecho CR 98% Mortes na indução 2 Seguimento mediana: 25m (3-99) Taxa de recaída 6% SG em 5 anos 90%
Rsvandi et al. 15th EHA meeting Abstract 0545
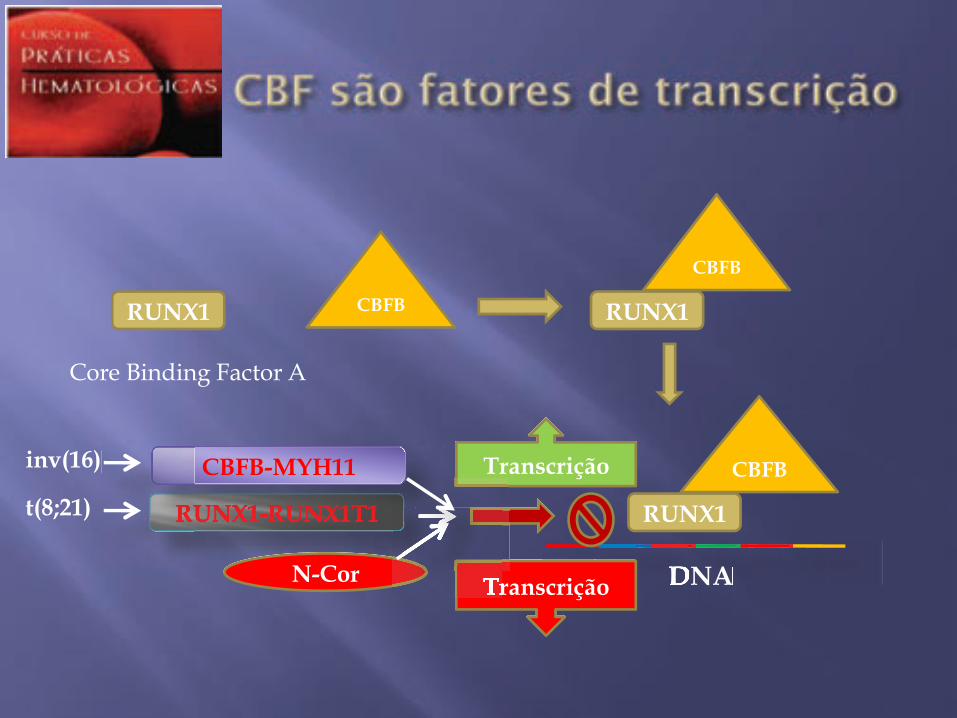
RUNX1
Core Binding Factor A
CBFB RUNX1
CBFB
RUNX1
CBFB
DNA
Transcrição
DNA
RUNX1-RUNX1T1
N-Cor Transcrição Transcrição
RUNX1-RUNX1T1
CBFB-MYH11
t(8;21)
inv(16) Transcriçãoinv(16)
RUNX1-RUNX1T1RUNX1-RUNX1T1RUNX1-RUNX1T1
"! ~5% das LMAs e 10% das “LMA c/maturação (M2)
"! Predomina em jovens "! Sarcomas granulocíticos são
comuns "! A detecção do gene de fusão
RUNX1-RUNX1T1 (AML1/ETO) é diagnóstica mesmo se <20% de blastos na M.O.
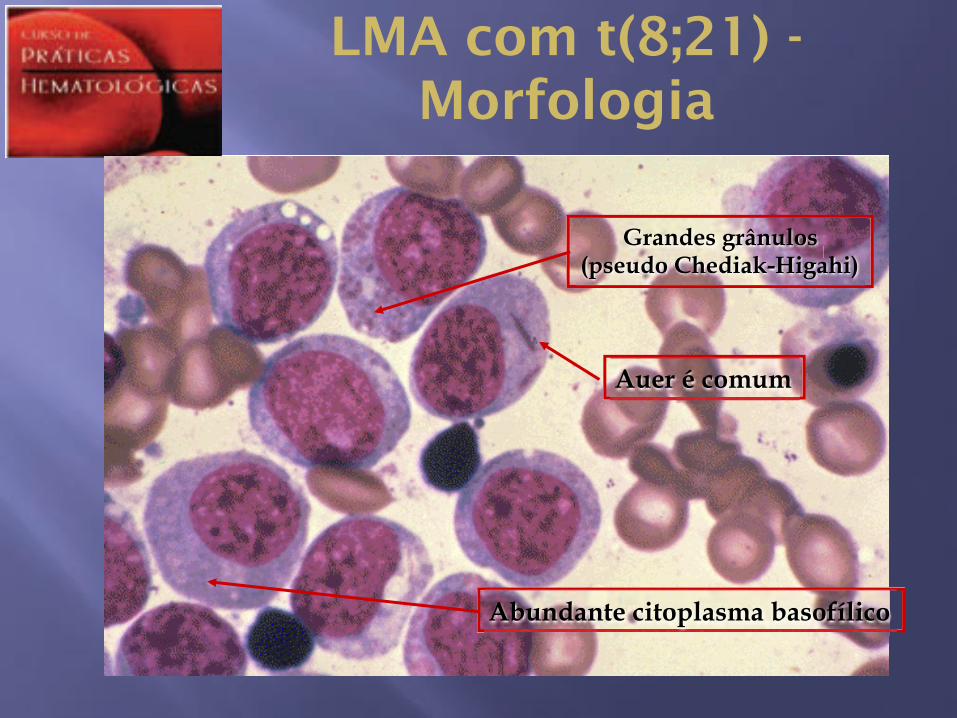
Abundante citoplasma basofílico
Grandes grânulos (pseudo Chediak-Higahi)
Auer é comum
LMA com t(8;21) - Morfologia
"! Eosinófilos morfologicamente normais podem estar aumentados em número [" inv(16)]
"! Menos frequentemente: excesso de mastócitos e/ou basófilos
"! Componente monocítico ausente ou escasso
LMA com t(8;21) - Morfologia
"! Alta intensidade de expressão do CD34
"! HLA-DR+, MPO+, CD13+
"! CD33+ - fraca intensidade
"! Diferenciação granulocítica: CD15;CD65
"! As vezes há assincronia CD34/CD15
!! Citogenética clássica ou FISH
!! RT-PCR
!! 70% dos pacientes possuem anormalidades adicionais
!! Mutações do Kit + em 20-25% dos casos
"! 5 - 8% das LMAs e 10% das “LMA c/maturação (M2)
"! Predomina em jovens
"! Sarcomas granulocíticos são comuns
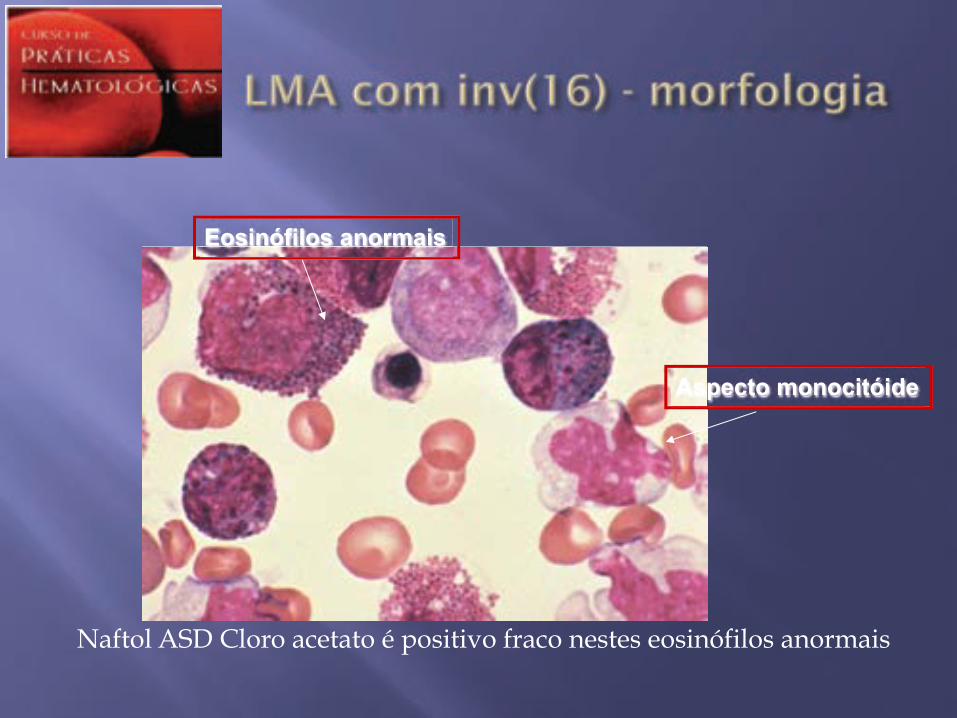
Aspecto monocitóide
Eosinófilos anormais
Naftol ASD Cloro acetato é positivo fraco nestes eosinófilos anormais
"! Várias subpopulações de blastos
"! Diferenciacão granulocítica e monocítica
"! Co-expressão do CD2 é comum
"! Identificação por FISH ou RT-PCR
"! 40% de anormalidades citogenéticas adicionais (destaca-se +22)
"! Mutações do Kit + em 30% dos casos
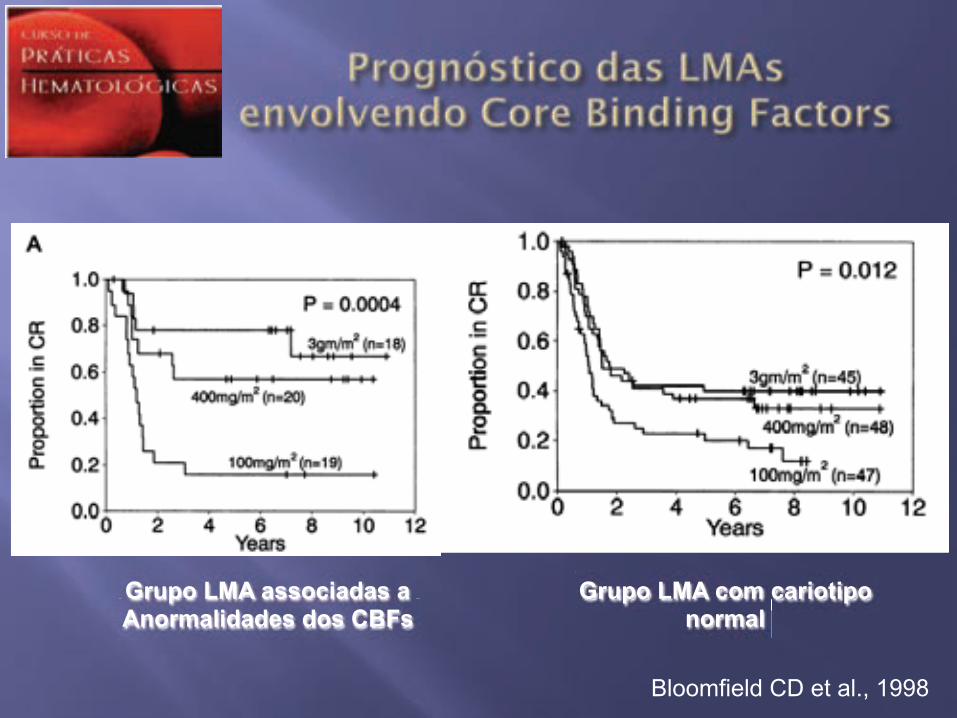
Grupo LMA associadas a Anormalidades dos CBFs
Grupo LMA com cariotipo normal
Bloomfield CD et al., 1998
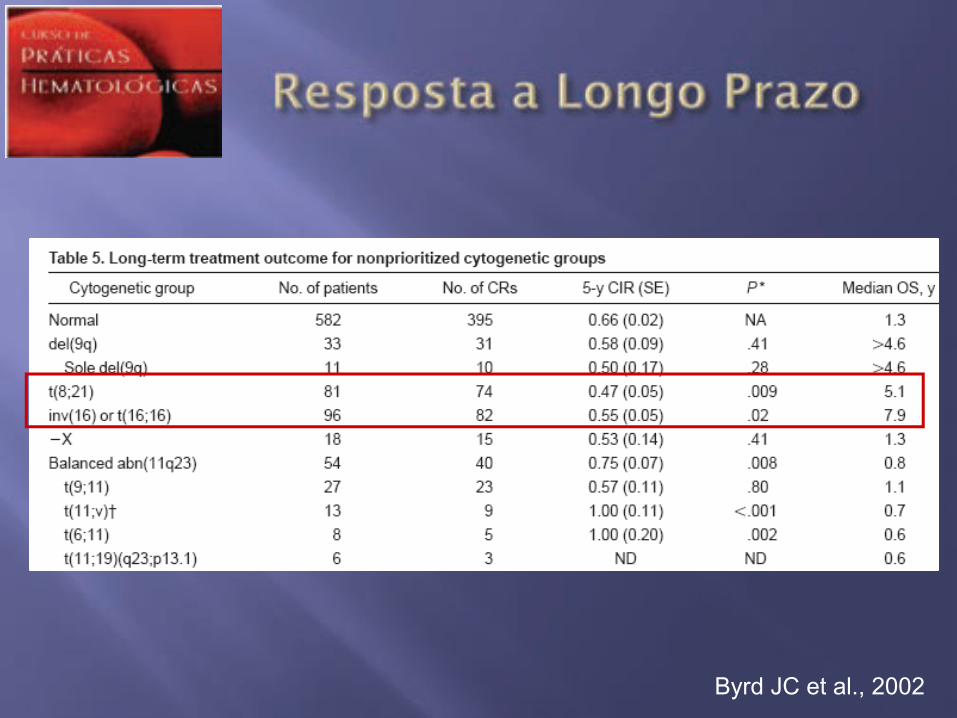
Byrd JC et al., 2002
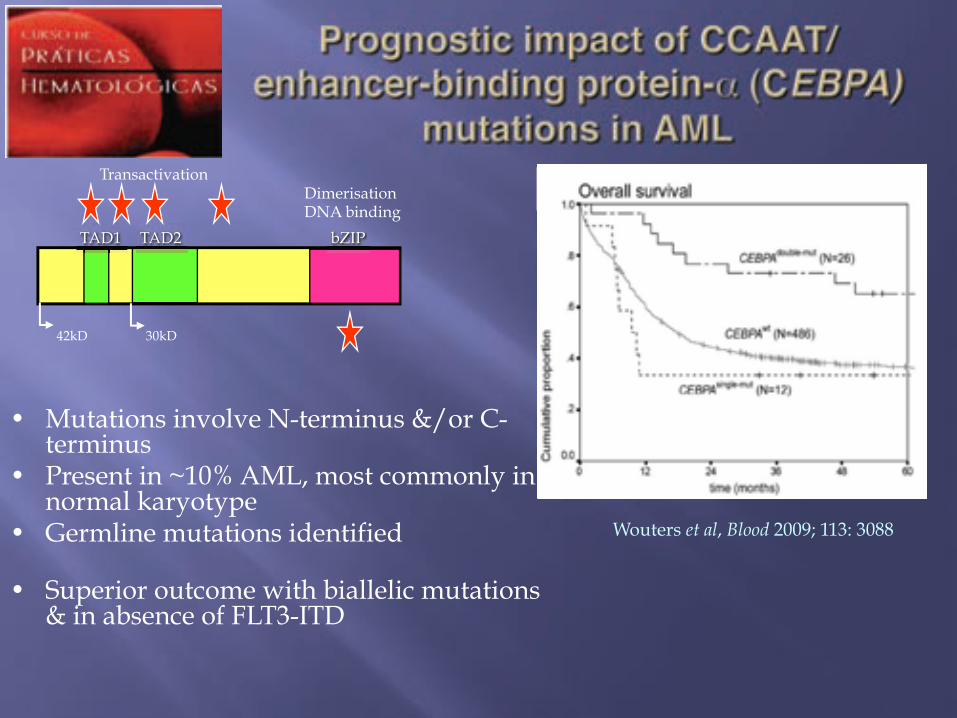
Wouters et al, Blood 2009; 113: 3088
•! Mutations involve N-terminus &/or C-terminus
•! Present in ~10% AML, most commonly in normal karyotype
•! Germline mutations identified
•! Superior outcome with biallelic mutations & in absence of FLT3-ITD
TAD1 TAD2 bZIP
42kD 30kD
Dimerisation DNA binding
Transactivation
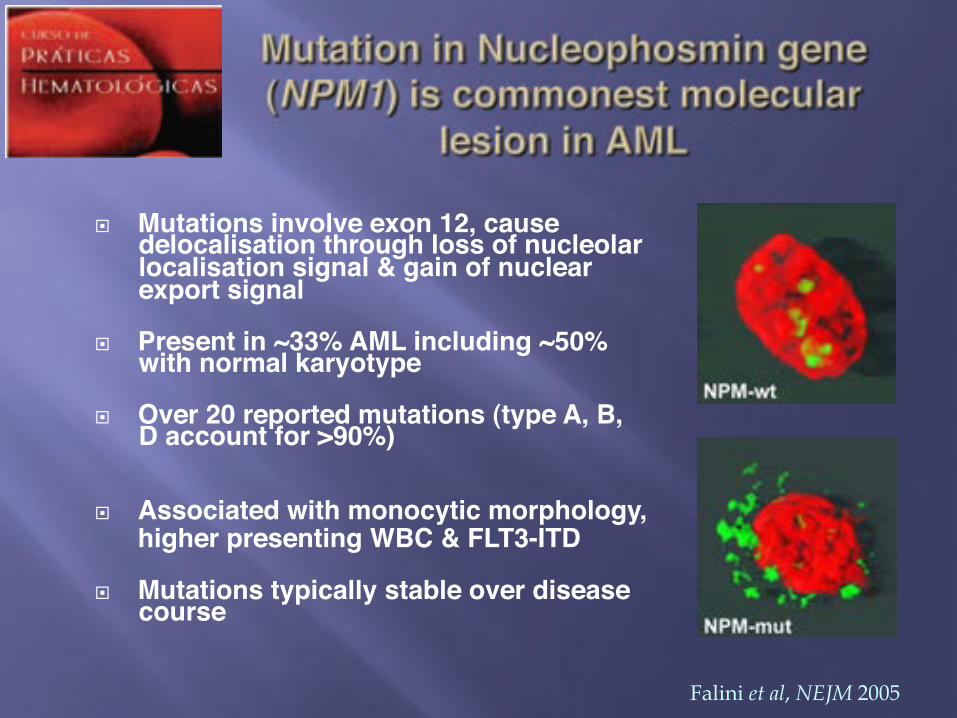
!! Mutations involve exon 12, cause delocalisation through loss of nucleolar localisation signal & gain of nuclear export signal ! ! !!
!! Present in ~33% AML including ~50% with normal karyotype ! !! ! ! !
!! Over 20 reported mutations (type A, B, D account for >90%) ! !! ! ! ! !! ! ! !
!! Associated with monocytic morphology, !!higher presenting WBC & FLT3-ITD
! ! ! !!! Mutations typically stable over disease
course!
Falini et al, NEJM 2005
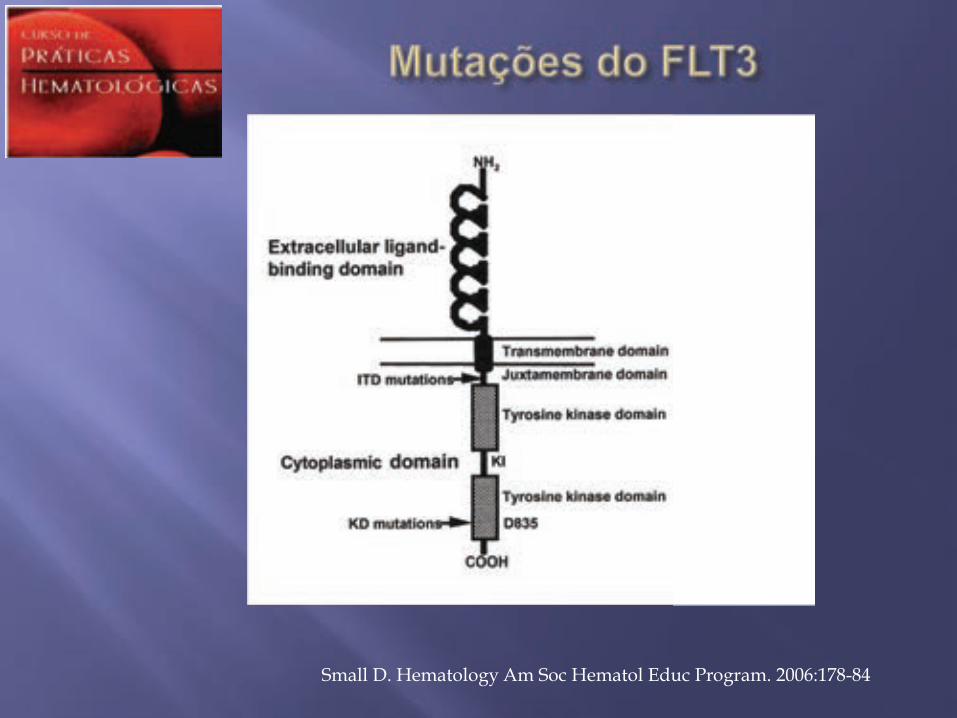
Small D. Hematology Am Soc Hematol Educ Program. 2006:178-84

#! Ocorrem em aproximadamente 20-25% das LMAs
#! Predominam nos pacientes com cariótipo normal
#! Envolvem duas regiões: o domínio justamembrana e o domínio catalítico
#! As primeiras são muito mais comuns e são internal tandem duplications (ITD)
#! As mutações do domínio tirosina quinase (TKD) são do tipo ponto
#! As mutações FLT3-ITD estão associadas a pior evolução dos pacientes
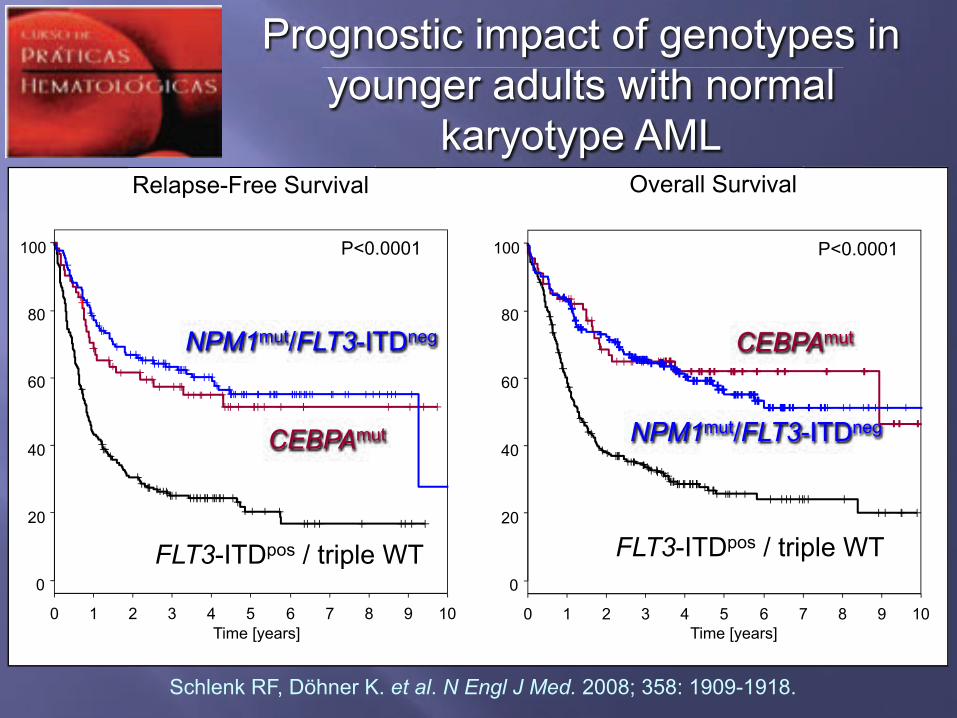
Prognostic impact of genotypes in younger adults with normal
karyotype AML Relapse-Free Survival Overall Survival
P<0.0001 P<0.0001
FLT3-ITDpos / triple WT
CEBPAmut
NPM1mut/FLT3-ITDneg CEBPAmut
NPM1mut/FLT3-ITDneg
Time [years] Time [years] 0 1 2 3 4 5 6 7 8 9 10
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
0
20
40
60
80
100
FLT3-ITDpos / triple WT
Schlenk RF, Döhner K. et al. N Engl J Med. 2008; 358: 1909-1918.
!! Objetivo: Integrar todos os fatores associados ao prognóstico de pacientes com LMA com cariótipo normal num sistema de pontos único
!! Casuística: 275 pacientes com LMA com cariótipo normal do estudo AML SHG Hannover 0199 e 0295. A validação externa foi feita em 131 pacientes do HOVON/SAKK
Damm et al. Blood. 2011;117(17):4561-4568
!! Foram avaliadas mutações/polimorfismos nos genes NPM1, FLT3, CEBPA, MLL, NRAS, IDH1/2, e WT1. Quantificação dos transcritos: BAALC, ERG, EVI1, ID1, MN1, PRAME e WT1.
!! O peso dos fatores seguiram o seguinte critério: "! RR < 1,2 – fator excluído "! RR ! 1,2 e " 1,7 – peso 1 "! RR > 1,7 e < 2,7 – peso 2 "! RR ! 2,7 – peso 3
Ganser et al. Damm et al. Blood. 2011;117(17):4561-4568
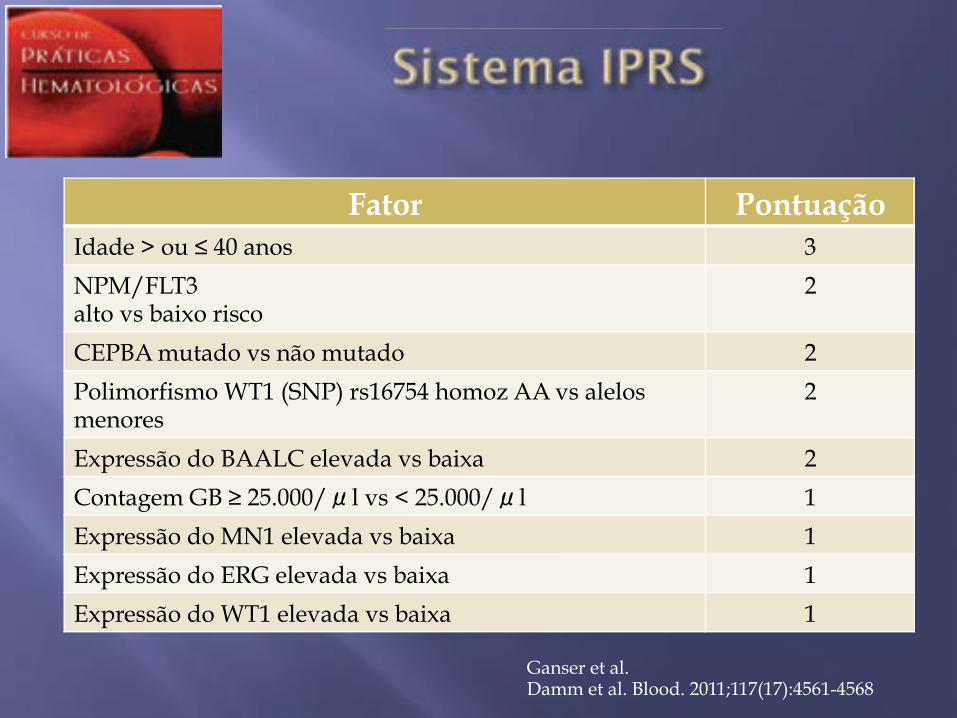
Fator Pontuação Idade > ou ! 40 anos 3
NPM/FLT3 alto vs baixo risco
2
CEPBA mutado vs não mutado 2
Polimorfismo WT1 (SNP) rs16754 homoz AA vs alelos menores
2
Expressão do BAALC elevada vs baixa 2
Contagem GB " 25.000/ l vs < 25.000/ l 1
Expressão do MN1 elevada vs baixa 1
Expressão do ERG elevada vs baixa 1
Expressão do WT1 elevada vs baixa 1
Ganser et al. Damm et al. Blood. 2011;117(17):4561-4568
!! Baixo risco: 0 a 7
!! Intermediário: 8 a 10
!! Alto risco: 11 a 15
Ganser et al. Damm et al. Blood. 2011;117(17):4561-4568
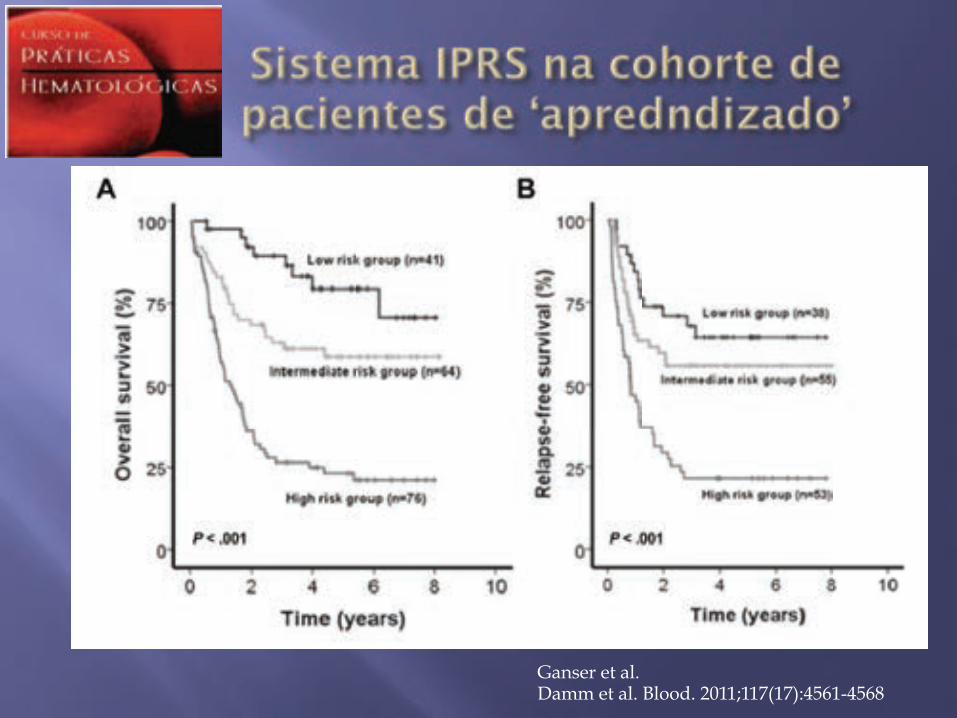
Ganser et al. Damm et al. Blood. 2011;117(17):4561-4568
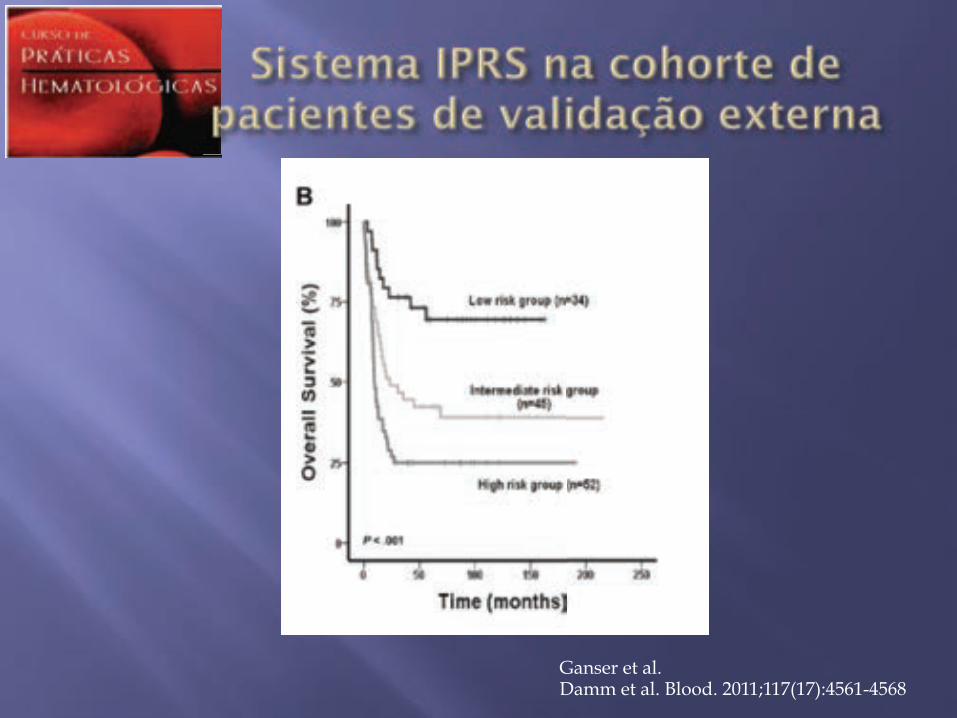
Ganser et al. Damm et al. Blood. 2011;117(17):4561-4568
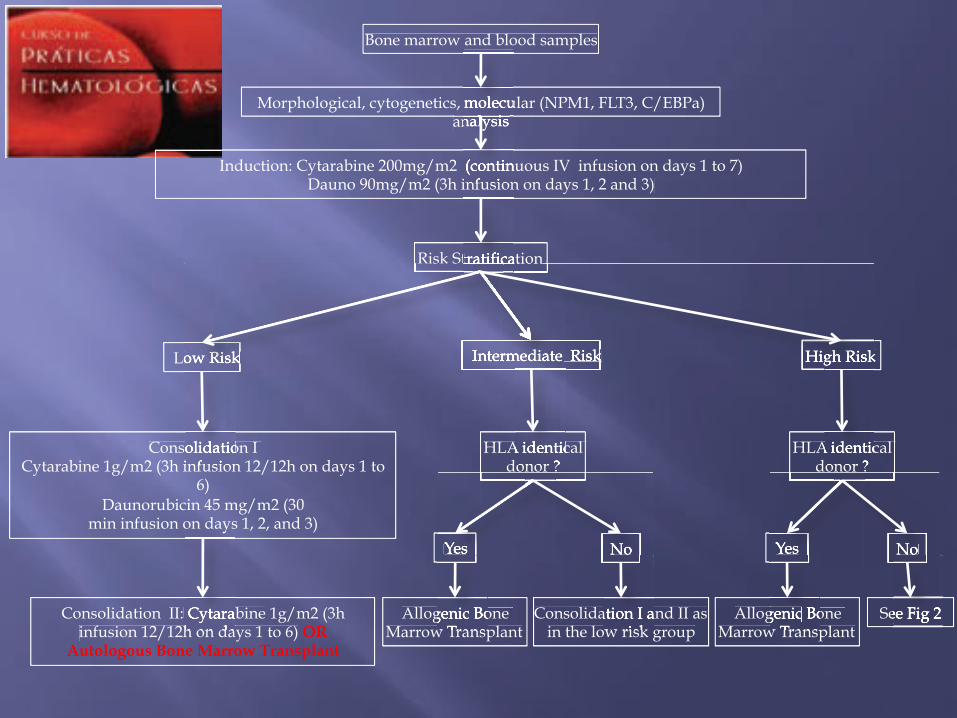
Bone marrow and blood samples
Morphological, cytogenetics, molecular (NPM1, FLT3, C/EBPa) analysis
Induction: Cytarabine 200mg/m2 (continuous IV infusion on days 1 to 7) Dauno 90mg/m2 (3h infusion on days 1, 2 and 3)
Risk Stratification
Low Risk
Consolidation I Cytarabine 1g/m2 (3h infusion 12/12h on days 1 to
6) Daunorubicin 45 mg/m2 (30
min infusion on days 1, 2, and 3)
Consolidation II: Cytarabine 1g/m2 (3h infusion 12/12h on days 1 to 6) OR
Autologous Bone Marrow Transplant
Intermediate Risk
HLA identical donor ?
HLA identical donor ?
Yes
Allogenic Bone Marrow Transplant
No
Consolidation I and II as in the low risk group
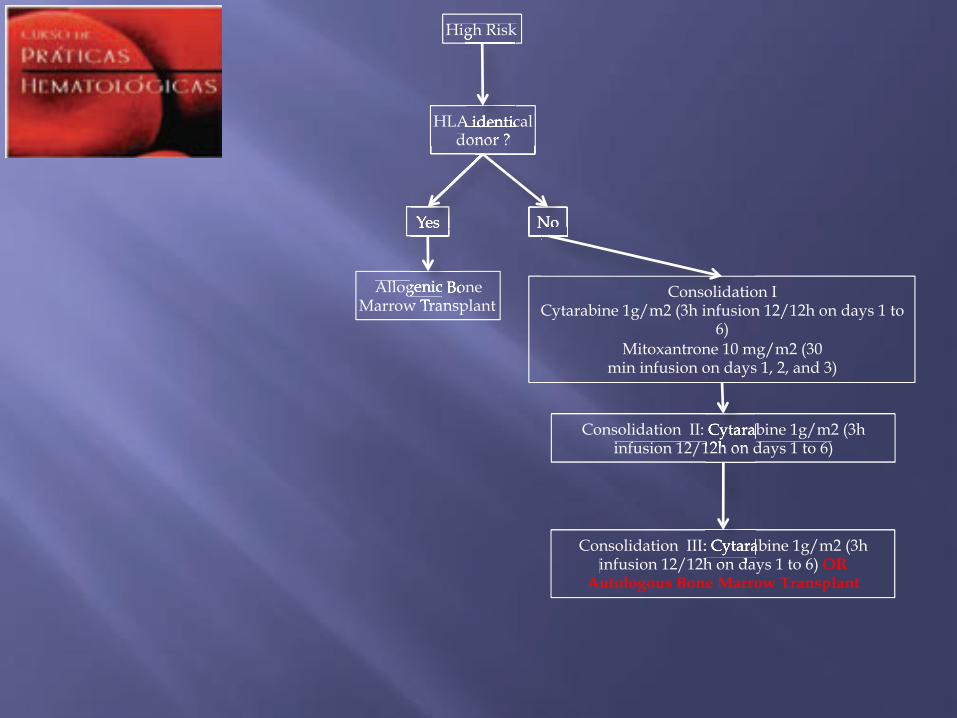
High Risk
Yes
Allogenic Bone Marrow Transplant
No
See Fig 2
Bone marrow and blood samples
, molecular (NPM1, FLT3, C/analysis
200mg/m2 (continuous IV infusion on days 1 to 7) 90mg/m2 (3h infusion on days 1, 2 and 3)
, molecular (NPM1, FLT3, C/analysis analysis
90mg/m2 (3h infusion on days 1, 2 and 3)
Risk Stratification Risk Stratification
Low Risk Low Risk Intermediate Risk
Risk Stratification
Intermediate Risk
Risk Stratification
Intermediate Risk Intermediate Risk High Risk
Risk Stratification Risk Stratification
Intermediate Risk Intermediate Risk
Consolidation I 1g/m2 (3h infusion 12/12h on days 1 to
min infusion on days 1, 2, and 3)
Cytarabineinfusion 12/12h on days 1 to 6)
HLA identical donor ?
Yes No
Allogenic Bone Marrow Transplant
Consolidation I and II as in the low risk group
HLA identical donor ?
High Risk High Risk
Yes No
Allogenic Bone Marrow Transplant
See Fig 2
HLA identical donor ?
High Risk
Yes
Allogenic Bone Marrow Transplant
No
HLA identical donor ?
High Risk
Yes No
Allogenic Bone Marrow Transplant
No
Consolidation I Cytarabine 1g/m2 (3h infusion 12/12h on days 1 to
6) Mitoxantrone 10 mg/m2 (30
min infusion on days 1, 2, and 3)
Consolidation II: Cytarabine 1g/m2 (3h infusion 12/12h on days 1 to 6)
Consolidation III: Cytarabine 1g/m2 (3h infusion 12/12h on days 1 to 6) OR
Autologous Bone Marrow Transplant
min infusion on days 1, 2, and 3)
Cytarabineinfusion 12/12h on days 1 to 6)infusion 12/12h on days 1 to 6)
Consolidation III: Cytarabineinfusion 12/12h on days 1 to 6)
History in March 2001 "! 36-year-old male, medical oncologist "! Complaining of acute pain in the
right lower abdominal quadrant "! Physical exam suggestive of acute
abdomen. Absence of palpable masses or adenopathy
"! Initial diagnosis based on history + physical exam: acute appendicitis
Authors: Evandro Fagundes and Henrique Bittencourt, UFMG
Hemoglobin: 15.8g/dl Hematocrit: 48% MCV: 89 fl WBC: 7.9 x 109/L Neutrophils: 56% Lymphocytes: 35% Monocytes: 4% Eosinophils: 5% Platelets: 280.0 x 109/L
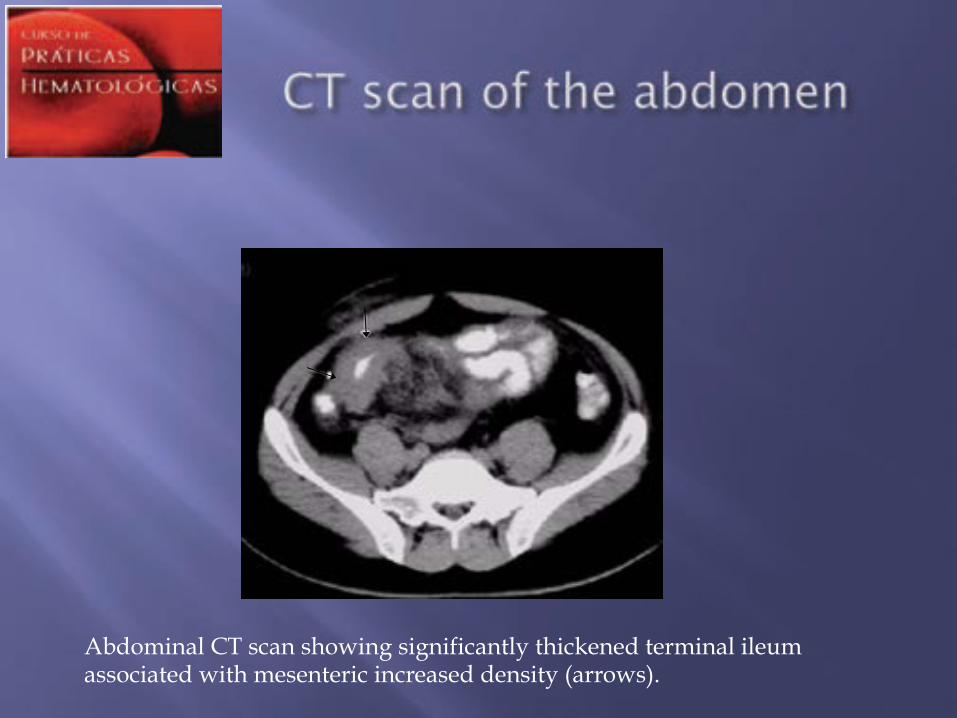
Abdominal CT scan showing significantly thickened terminal ileum associated with mesenteric increased density (arrows).
!! Surgical Diagnosis: Tumoral abdominal mass
!! Histological Diagnosis: Large Cell Lymphoma
Antigens Values CD 20: Negative CD43: Positive CD 5: Negative Myeloperoxidase: Positive AEI/AE3 (citoceratina): Negative Ki67: Positive 50% Conclusion: Acute myeloid leukemia infiltrate
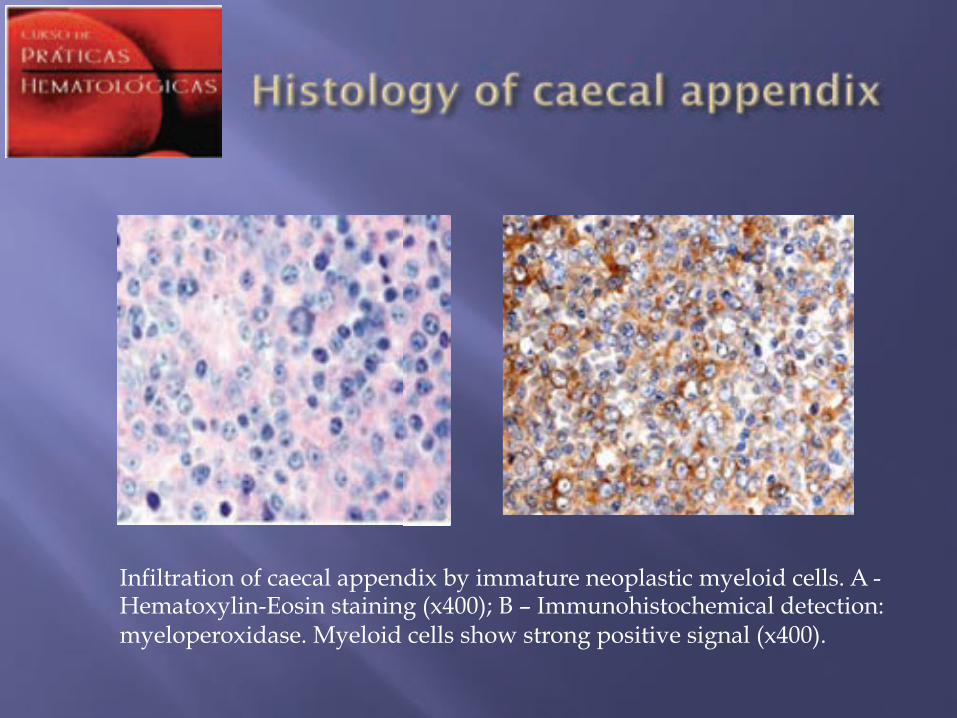
Infiltration of caecal appendix by immature neoplastic myeloid cells. A - Hematoxylin-Eosin staining (x400); B – Immunohistochemical detection: myeloperoxidase. Myeloid cells show strong positive signal (x400).
Difuse infiltration by blastic cells with fine cytoplasmatic granules. There are also admixed eosinophilic myelocytes, characteristic of this tumor type. Diagnosis: Granulocytic Sarcoma
!! Normal cellularity !! Erythroid Cells: 37% !! Myeloid Cells: 51% ( Blasts: 10,8%) !! Lymphocytes: 12% !! S o m e n e u t r o p h i l s s h o w e d
hypogranulation. There were some eosinophils with abnormal granules. Megakaryocytes were observed in number apparently normal
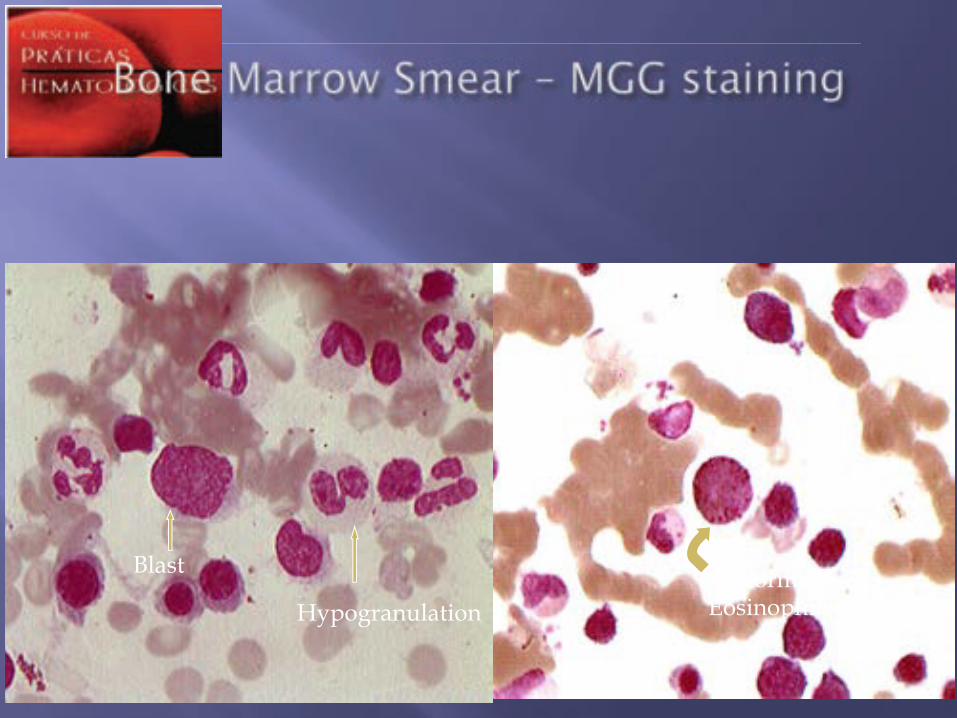
Hypogranulation
Blast Abnormal Eosinophil
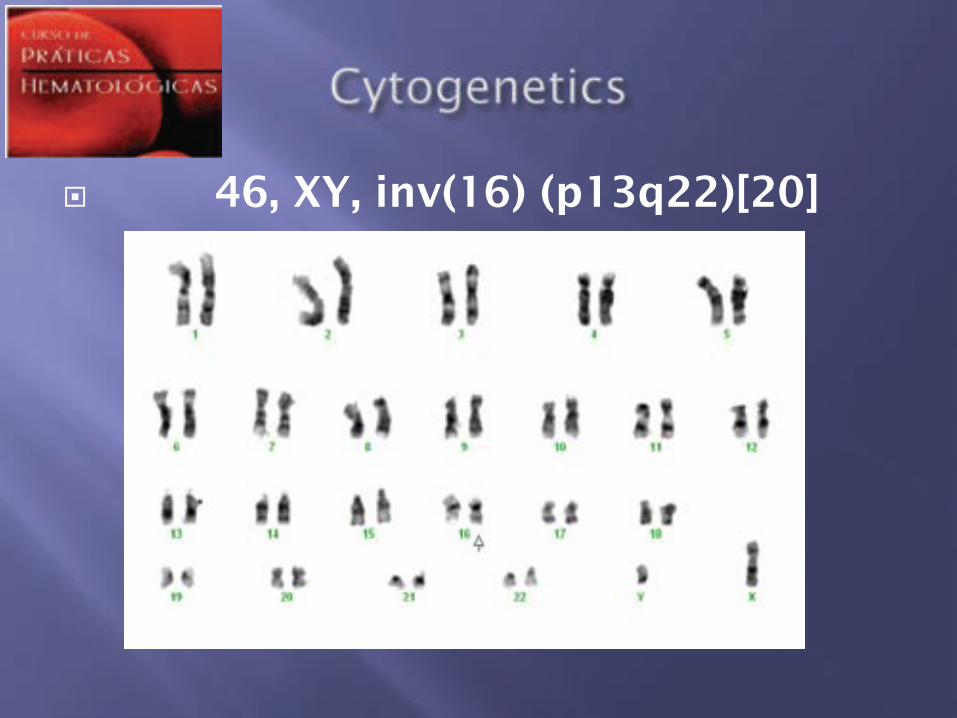
!! 46, XY, inv(16) (p13q22)[20]
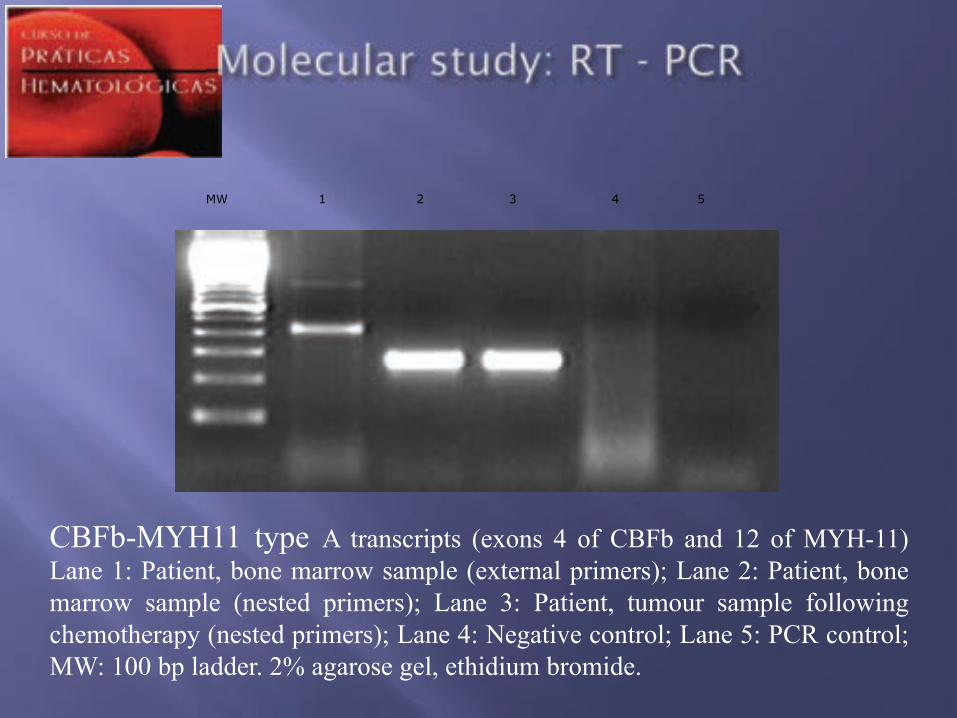
MW 1 2 3 4 5
CBFb-MYH11 type A transcripts (exons 4 of CBFb and 12 of MYH-11) Lane 1: Patient, bone marrow sample (external primers); Lane 2: Patient, bone marrow sample (nested primers); Lane 3: Patient, tumour sample following chemotherapy (nested primers); Lane 4: Negative control; Lane 5: PCR control; MW: 100 bp ladder. 2% agarose gel, ethidium bromide.
"!Acute Myeloid Leukemia with inv16
"! Induction: one course of ara-C + dauno 60mg/m2
"! Post-remission therapy:
1st course: HidAC (3g/m2 x 6) + Dauno
2nd course: Ara-C +Dauno+VP16
3rd course: HidAC (3g/m2 x 6) +Dauno
"! Palpable RLQ mass
"!Abdominal CT – Residual mass
"! Bone marrow – cytologic remission
"! Biopsy of residual mass: Fibrosis
"!Molecular biology of bone marrow: negative for CBFb-MYH11.
"!Molecular biology of residual mass: positive for CBFb-MYH11.

"!Therapeutic decision: Autologous HSCT (no HLA match sibling available)
"! Follow up – stable residual mass. "!Overall survival 6y "! LFS from CR1 5y10m "! Survival after SCT 4y11m.
!! Granulocytic Sarcoma (GS) is a rare manifestation of AML. It may be a forerunner of AML in non-leukemic patients.
!! GS has been associated with many chromosome abnormalities, including CBF leukemias.
!! GS is more freqüent with t(8;21) than Inv(16).
!! The Inv (16) seems to be associated with small intestine involvement.
!! Patients with SG should be treated as patients with AML.
!! The presence of Inv(16) confers favorable prognosis for AML patients.
!! The treatment is based on repetitive cycles of HiDAC, althought autologous stem cell transplantation may be have a role.
!! Xavier SG, Fagundes EM, Hassan R et al. Granulocytic
Sarcoma of the small intestine with CBF!/MYH11 fusion gene: report of aleukemic case and review of the literature. Leuk Res 2003; 27: 1063-66.
!! Pileri SA, Ascani S, Campidelli C et al. Myeloid Sarcoma clinico-pathologic, phenotypic and cytogenetics analysis of 92 adult patients. Leukemia 2007; 21: 340 – 350.
!! Byrd JC, Ruppert AS, Mrózek K et al. Repetitive cycles of high-dose cytarabine benefit patients with acute myeloid leukemia and inv (16)(p13:q22) or t(16;16)(p13:q22): results from CALGB 8461. J Clin Oncol 2004; 22: 1087-94.
!! Slovak M, Kopecky KJ, Cassileth PA et al. Karyotypic analysis predict outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southewest Oncology Group/ Eastern Cooperative Oncology Group Study. Blood 2000; 96: 4075-83.
: !! Evandro Fagundes and Henrique Bittencourt
attending physicians
!! Sandra Xavier M.D. for providing the CT scan,
cytogenetic and RT-PCR figures. !! Lúcia Porto M.D. for providing the photographs of
bone marrow smears.
!! MTFA, female, 52 y, teacher
!! Fatigue and loss of weight (3kg) in the last 3 months
!! Evaluated by her GP who detected anemia and prescribed the transfusion (2 units RBCs)
!! Previously healthy
!! No significant past or familiar history, except smoking (1 pkg/d for the last 20 years)
!! Pale 2/4+, without fever or jaundice !! Absence of lymphnode enlargements or
masses !! No mucocutaneous findings, !! BP: 120 x 70 mmHg, Cardiac rate: 108, no
murmurs !! Chest auscultation: normal breath sounds !! Abdomen: splenomegaly (4cm below the
costal margin) without hepatomegaly !! No neurological abnormalities
!! CBC "! Hb: 8.8 g/dL "! RBCs: 3.13 x 106/mm3 "! Ht: 26% "! VCM: 84fl "! HCM: 28pg "! RDW: 14.5 "! Leukocytes: 3,500/mm3
!! Neutrophils: 2,400 !! Lymphocytes: 800 !! Monocytes: 200 !! Basophils: 100
"! Platelets: 15,000/mm3
"! Reticulocytes: 0.1%
•! Citoquímica •! MPO negativa •! Esterase não específica não realizada

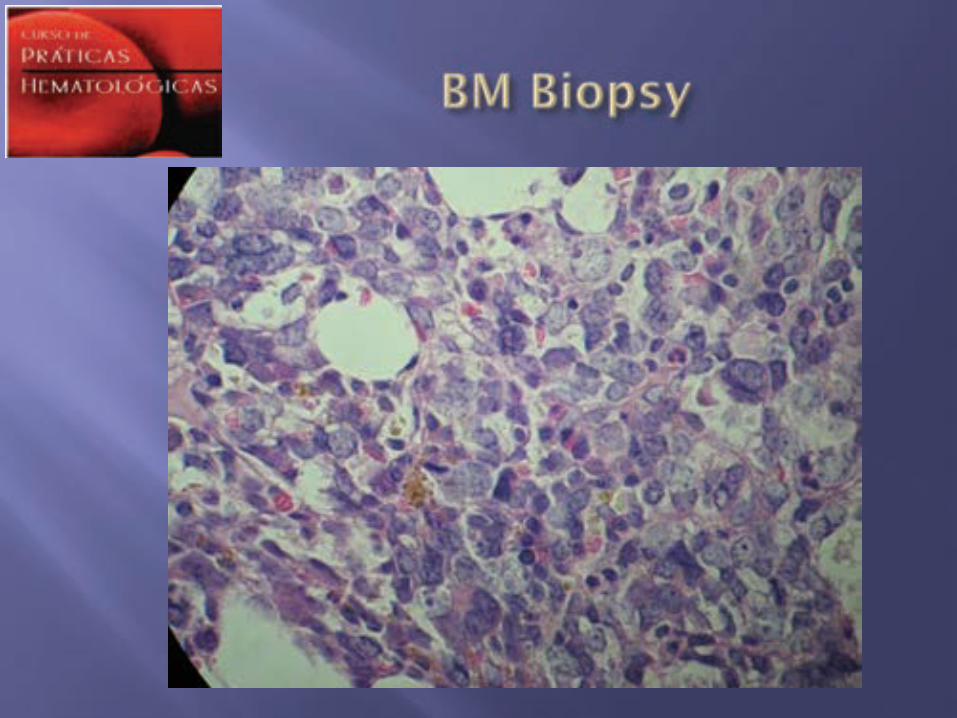
Several attempts of BM aspiration were unsuccessful (dry tap)
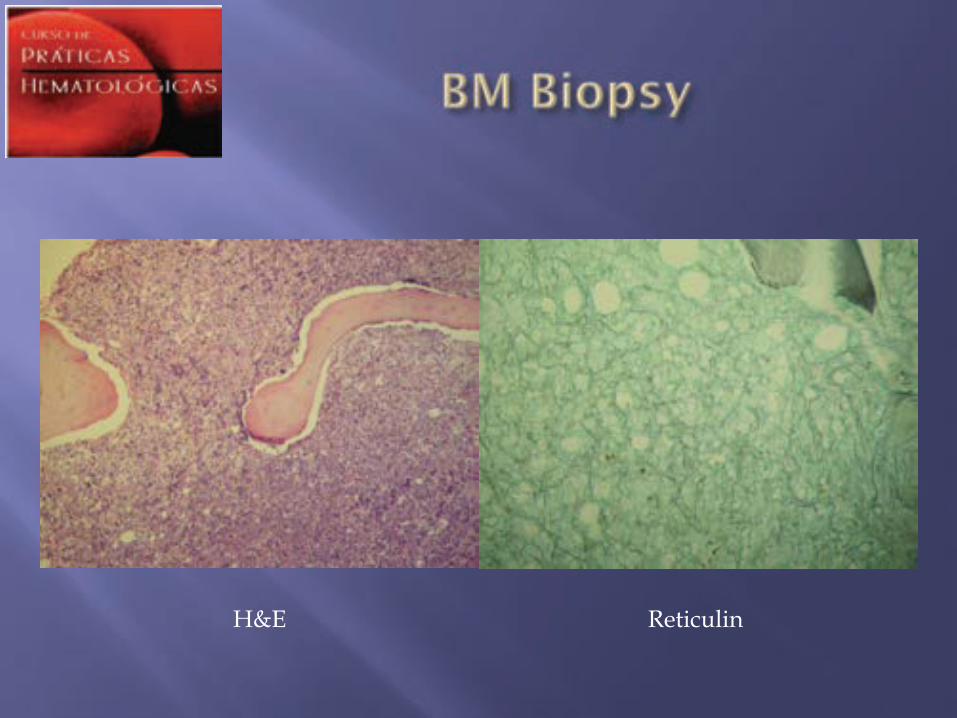
H&E Reticulin
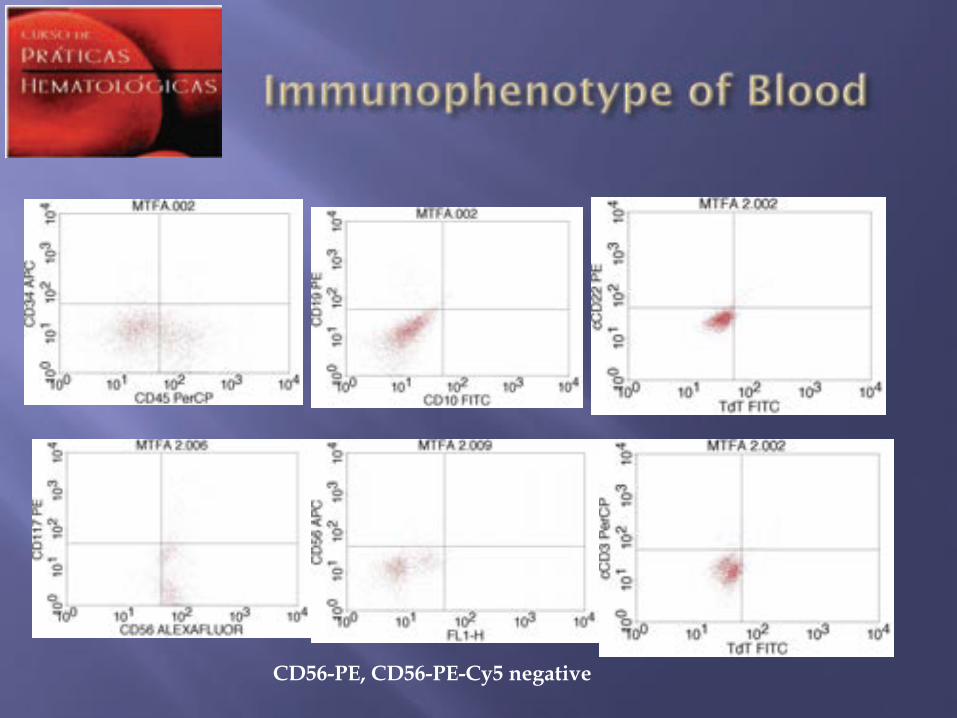
CD56-PE, CD56-PE-Cy5 negative
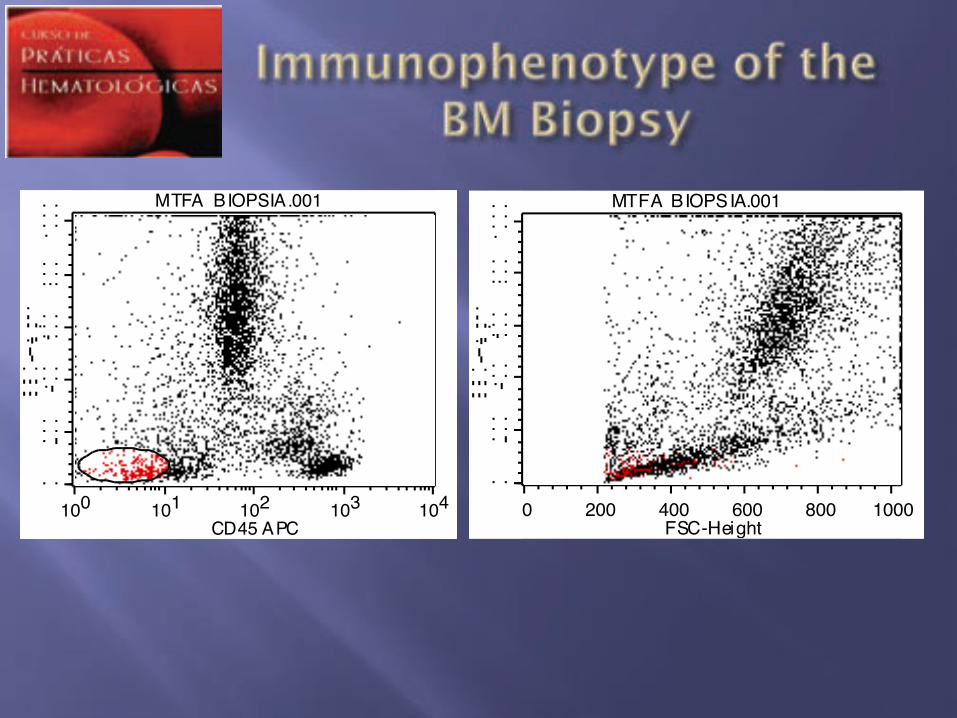
0 200 400 600 800 1000FSC-Height
MTFA BIOPSIA.001
100 101 102 103 104CD45 APC
MTFA BIOPSIA.001
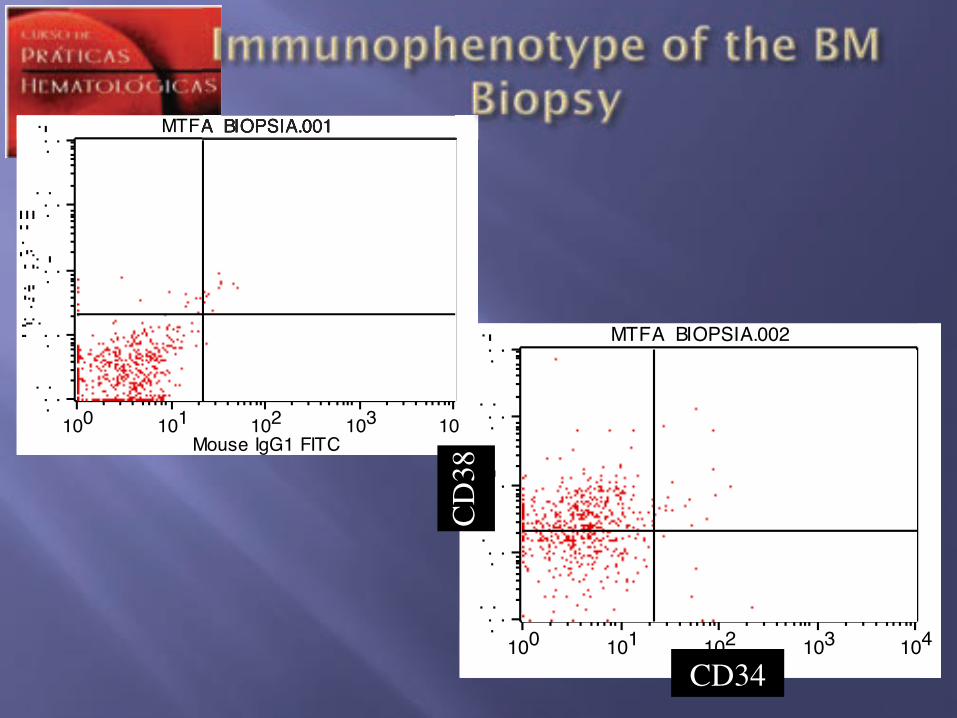
100 101 102 103 104Mouse IgG1 FITC
MTFA BIOPSIA.001
100 101 102 103 104CD34 FITC
MTFA BIOPSIA.002
CD38!
CD34!
MTFA BIOPSIA.001
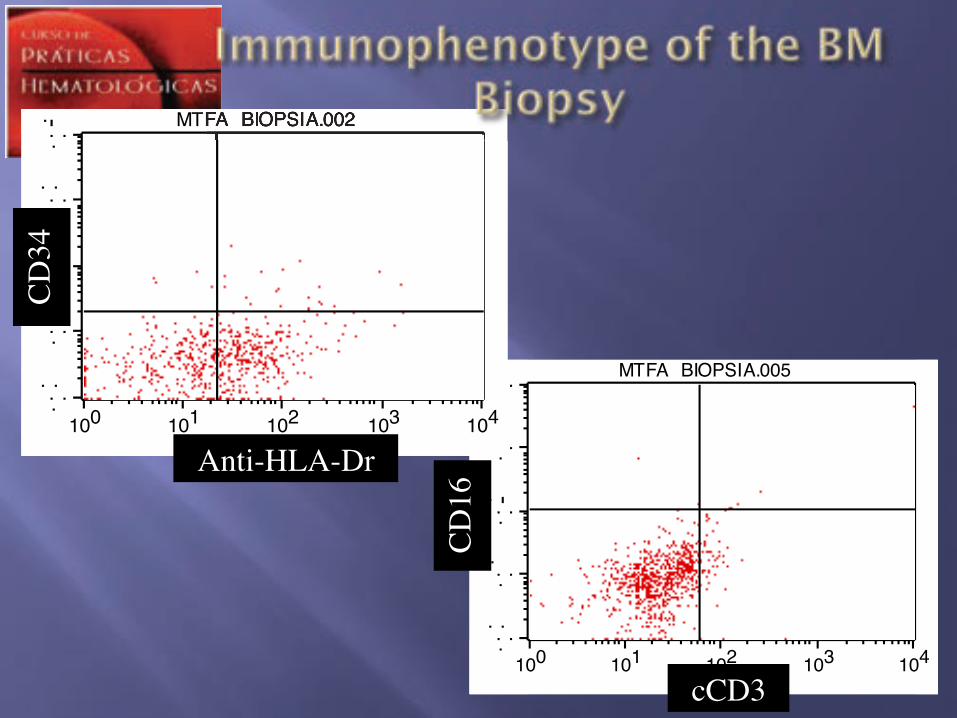
100 101 102 103 104cCD3 FITC
MTFA BIOPSIA.005
cCD3!
CD16!
100 101 102 103 104Anti -HLA-DR PerCP
MTFA BIOPSIA.002
Anti-HLA-Dr!
CD34!
MTFA BIOPSIA.002
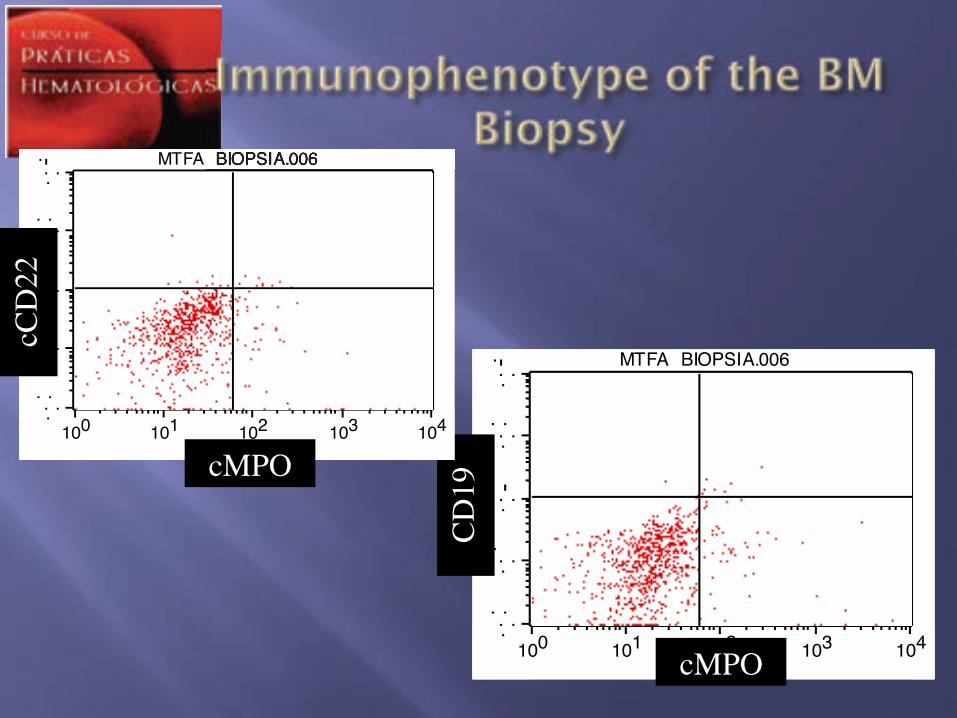
100 101 102 103 104cMPO FITC
MTFA BIOPSIA.006
cMPO!
CD19!
100 101 102 103 104cMPO FITC
MTFA BIOPSIA.006
cMPO!
cCD22!
MTFA BIOPSIA.006
!! Non hematological malignancies (MPO positive?)
!! AML, NOS "! With minimal differentiation
!! Acute panmyelosis with mielofibrosis
!! Blastic plasmocytoid dendritic cell neoplasm
!! Multiple myeloma
!! Acute undifferentiated leukemia
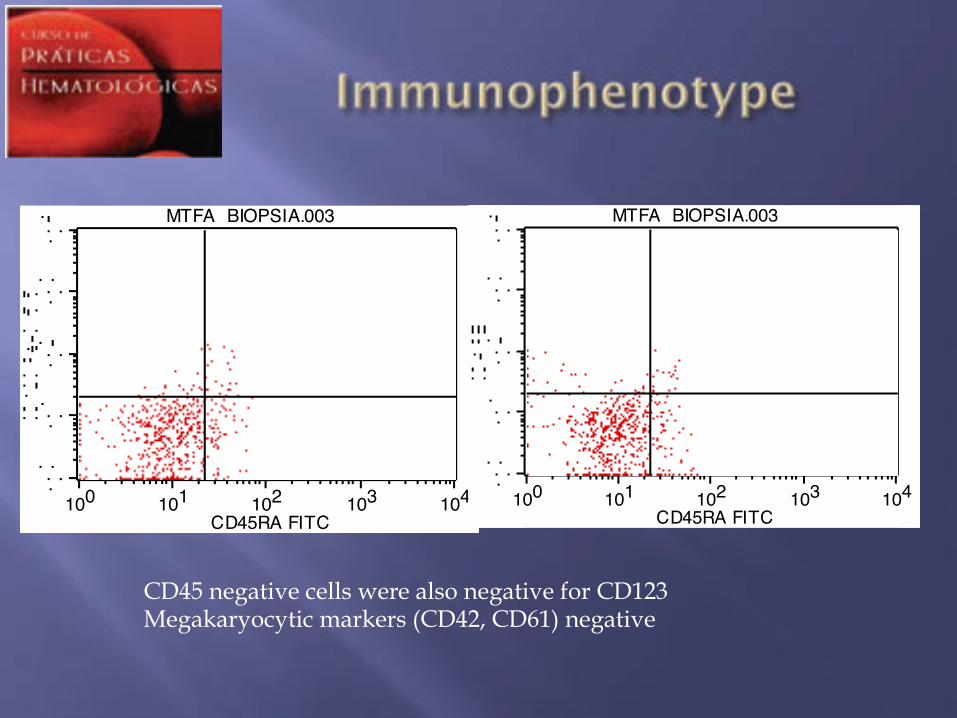
CD45 negative cells were also negative for CD123 Megakaryocytic markers (CD42, CD61) negative
100 101 102 103 104CD45RA FITC
MTFA BIOPSIA.003
100 101 102 103 104CD45RA FITC
MTFA BIOPSIA.003
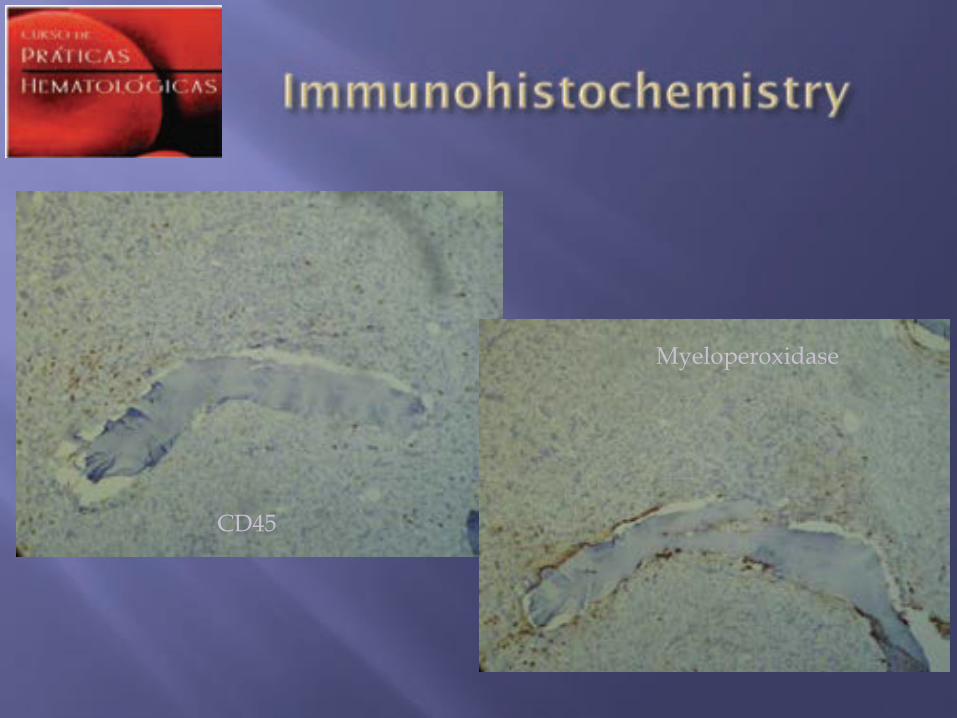
CD45
Myeloperoxidase
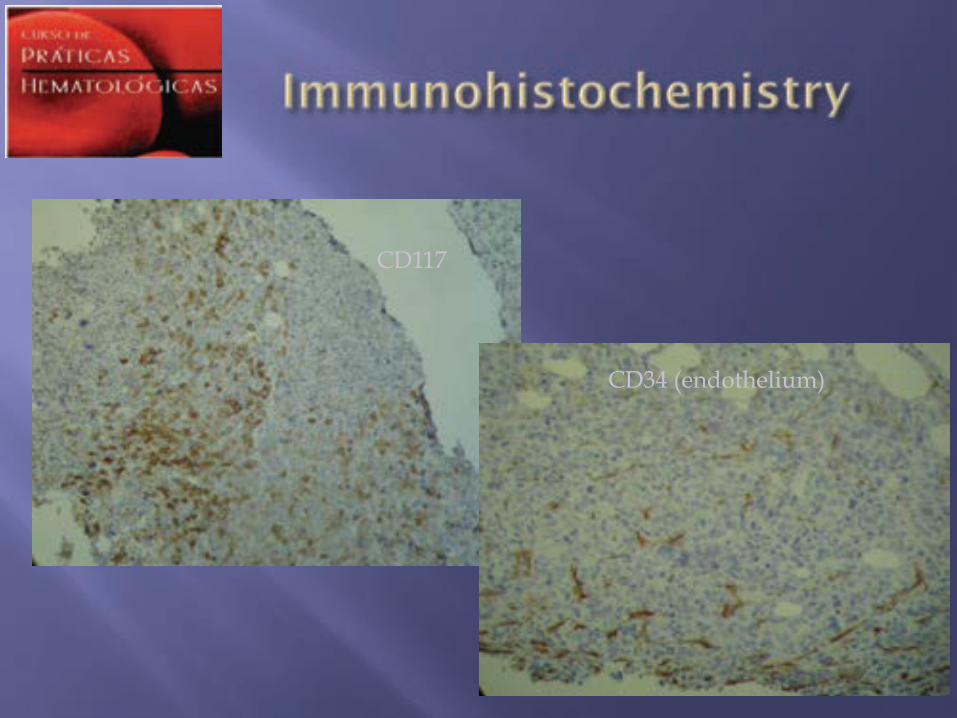
CD117
CD34 (endothelium)
!! 44~45,XX,t(2;11)(p21;q12),t(3;15)(q12;q15),inv(3)(q21q26),t(4;7)(q21;q21),+mar[12]/46,XX[8]. #
Cortesia: Fábio Morato
!! Patient received one course of anthracycline and citarabine as cytoreduction, before the definitive diagnosis and one course of induction
!! The D30 BM aspirate after induction showed that patient was in remission