FIRST‐LINE RIBOCICLIB + LETROZOLE IN …gbcc2016.gbcc.kr/GBCC2017_upload/PFile_02_22_OP 2_Yoon Sim...
15
FIRST‐LINE RIBOCICLIB + LETROZOLE IN POSTMENOPAUSAL ASIAN WOMEN WITH HR+, HER2– ADVANCED BREAST CANCER: A SUBGROUP ANALYSIS OF MONALEESA‐2 Yoon‐Sim Yap, 1 Chiun‐Sheng Huang, 2 Tae‐Yong Kim, 3 Kyung Hae Jung, 4 Keun Seok Lee, 5 Joohyuk Sohn, 6 Jee Hyun Kim, 7 Yu Han, 8 Michelle Miller, 8 Sunil Verma 9 1 Department of Medical Oncology, National Cancer Center Singapore, Singapore; 2 Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan; 3 Department of Internal Medicine, Seoul National University Hospital, Seoul, Republic of Korea; 4 Department of Oncology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Republic of Korea; 5 Research Institute and Hospital, National Cancer Center, Goyang‐si, Republic of Korea; 6 Department of Surgery, Severance Hospital of Yonsei University, Seoul, Republic of Korea; 7 Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Republic of Korea; 8 Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA; 9 Department of Oncology, Tom Baker Cancer Centre, Calgary, Canada Abstract #ABS‐0114 Presented on Friday April 21, 2017 (Invited Oral Presentation)
Transcript of FIRST‐LINE RIBOCICLIB + LETROZOLE IN …gbcc2016.gbcc.kr/GBCC2017_upload/PFile_02_22_OP 2_Yoon Sim...

FIRST‐LINE RIBOCICLIB + LETROZOLE IN POSTMENOPAUSAL ASIAN WOMEN WITH HR+, HER2– ADVANCED BREAST CANCER:A SUBGROUP ANALYSIS OF MONALEESA‐2
Yoon‐Sim Yap,1 Chiun‐Sheng Huang,2 Tae‐Yong Kim,3 Kyung Hae Jung,4 Keun Seok Lee,5Joohyuk Sohn,6 Jee Hyun Kim,7 Yu Han,8 Michelle Miller,8 Sunil Verma9
1Department of Medical Oncology, National Cancer Center Singapore, Singapore; 2Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan; 3Department of Internal Medicine, Seoul National University Hospital, Seoul, Republic of Korea; 4Department of Oncology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Republic of Korea; 5Research Institute and Hospital,National Cancer Center, Goyang‐si, Republic of Korea; 6Department of Surgery, Severance Hospital of Yonsei University, Seoul, Republic of Korea; 7Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Republic of Korea; 8Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA; 9Department of Oncology, Tom Baker Cancer Centre, Calgary, Canada
Abstract #ABS‐0114 Presented on Friday April 21, 2017 (Invited Oral Presentation)

Disclosure SlideYoon‐Sim Yap Advisory board/consultant (Novartis); honoraria (Novartis); fees for advisory board meetings (Pfizer)
Chiun‐Sheng Huang Institute remuneration (Novartis)
Tae‐Yong Kim Kyung Hae Jung Keun Seok Lee Joohyuk Sohn Jee Hyun Kim
Nothing to declare
Yu Han Employment (Novartis)
Michelle Miller Employment (Novartis); stock ownership (Novartis)
Sunil Verma Advisory board (Amgen, AstraZeneca, Lilly, Novartis, Pfizer, Roche)
• Study sponsored by Novartis Pharmaceuticals Corporation

• 23% of breast cancers worldwide are diagnosed in Asia1 and advanced breast cancer is a significant health burden in Asian countries
• Endocrine therapy is the preferred first‐line treatment forHR+, HER2– advanced breast cancer
• Endocrine resistance and eventual disease progression occur in most patients2–4
• An increase of cyclin D–CDK4/6 pathway activation is associated with endocrine resistance5,6
• Ribociclib (LEE011) is an orally bioavailable, selective CDK4/6 inhibitor that demonstrated preliminary clinical activity in advanced solid tumors7
• The efficacy and safety of ribociclib in combination with endocrine therapy was demonstrated in the randomized, placebo‐controlled Phase III MONALEESA‐2 study8
CDK, cyclin‐dependent kinase; HER2–, human epidermal growth factor receptor 2‐negative; HR+, hormone receptor‐positive. 1. Youlden DR, et al. Cancer Biol Med 2014;11:101–115; 2. Cardoso F, et al. Ann Oncol 2014;25:1871–1888; 3. Rugo HS, et al. J Clin Oncol 2016;34:3069–3103;
4. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer, version 2.2016; 5. Hosford SR & Miller TW. Pharmgenomics Pers Med 2014;7:203–215;6. Thangavel C, et al. Endocr Relat Cancer 2011;18:333–345; 7. Infante JR, et al. Clin Cancer Res 2016;22:5696–5705; 8. Hortobagyi GN, et al. N Engl J Med 2016;375:1738–1748.
Introduction
E2FRbRb
P
Genetranscription
CDK4/6Cyclin D
ER/PgR
Wnt/β-cateninSTATs
MAPKsPl3K/mTOR
NF-kBp21p16
p53
E2FComplexed, inactive E2F
(tumor suppressor)
G2
M
G1
SG0 Restriction
point
Ribociclib

• Postmenopausal women with HR+, HER2– ABC
• No prior systemic therapy for advanced disease
• N=668
Randomization (1:1)
Stratified by the presence/absence of liver and/or lung
metastases
Ribociclib (600 mg/day)3‐weeks‐on/1‐week‐off
+Letrozole (2.5 mg/day)
n=334
Placebo3‐weeks‐on/1‐week‐off
+Letrozole (2.5 mg/day)
n=334
Primary endpoint• PFS (locally assessed per RECIST v1.1)
Secondary endpoints• Overall survival (key)• Overall response rate• Clinical benefit rate• Safety & tolerability (per CTCAE v4.03)
MONALEESA‐2 Study Design
• Tumor assessments were performed every 8 weeks for the first 18 months, then every 12 weeks thereafter• Supportive PFS analyses were conducted in pre‐specified patient subgroups, including in
Asian patients (as defined by geographic region or by race)
ABC, advanced breast cancer; CTCAE, Common Terminology Criteria for Adverse Events; HR+, hormone receptor‐positive; HER2–, human epidermal growth factor receptor 2‐negative; PFS, progression‐free survival; RECIST, Response Evaluation Criteria In Solid Tumors.

Prob
ability of P
FS (%
)
0
20
40
60
80
100
0 4 8 12 16 20 24 Time (months)
R + Ln=334
P + Ln=334
Median PFS, months (95% CI) NR (19.3–NR) 14.7 (13.0–16.5)
HR (95% CI) 0.556 (0.429–0.720)One‐sided p value 0.00000329
• PFS results by independent central review: HR 0.592 (95% CI: 0.412–0.852; p=0.002)• Treatment benefit was consistent across patient subgroups and for secondary endpoints analyzed
CI, confidence interval; HR, hazard ratio; L, letrozole; NR, not reached; P, placebo; PFS, progression‐free survival; R, ribociclib.
MONALEESA‐2 Primary Endpoint:Progression‐free Survival in the Full Population

68 patients treated in Asian countries 51 Asian patients (by race)*
Singapore13%
Republic of Korea13%
Lebanon22%
Turkey18%
Other 4%Taiwan 28%
Thailand 6%Europe 2%
North America12%
Asia82%
Approximately two‐thirds of patients treated in Asian countries were Asian (by race)
Most Asian patients (by race) were treated in countries in Asia
*Race was self‐reported at screening.
MONALEESA‐2 Asian Subgroups

Asian region (n=68) Non‐Asian region (n=600)Ribociclib + Letrozole
n=35Placebo + Letrozole
n=33Ribociclib + Letrozole
n=299Placebo + Letrozole
n=301Median age, years (range) 61 (46–74) 62 (49–77) 62 (23–91) 63 (29–88)Median weight, kg (range) 59 (35–83) 61 (42–108) 71 (46–154) 70 (42–126)ECOG performance status, n (%)0 22 (63) 26 (79) 183 (61) 176 (59)1 13 (37) 7 (21) 116 (39) 125 (42)
Disease‐free interval, n (%)De novo 14 (40) 17 (52) 100 (33) 96 (32)Non de novo 21 (60) 16 (49) 199 (67) 205 (68)*≤12 months 0 1 (3) 4 (1) 9 (3)>12–≤24 months 1 (3) 1 (3) 13 (4) 14 (5)>24 months 20 (57) 14 (42) 182 (61) 181 (60)
Metastatic sites, n (%)Bone 22 (63) 22 (67) 224 (75) 222 (74)Visceral‡ 25 (71) 21 (64) 172 (58) 175 (58)
Number of metastatic sites, n (%)<3 22 (63) 27 (82) 198 (66) 194 (64)≥3 13 (37) 6 (18) 101 (34) 107 (36)
Neutrophils (absolute) hypo, n (%) §Grade 1/2 2 (6) 0 10 (3) 15 (5)Grade 3/4 0 0 0 0
ECOG, Eastern Cooperative Oncology Group.*One patient with non de novo disease had an unknown disease‐free interval; ‡includes liver, lung, and other visceral sites; § based on safety population.
Patient Characteristics at Baseline

Patient DispositionAsian region (n=68) Non‐Asian region (n=600)
Ribociclib + Letrozolen=35
Placebo + Letrozolen=33
Ribociclib + Letrozolen=299
Placebo + Letrozolen=301
Treatment ongoing, n (%)* 26 (74) 12 (36) 169 (57) 142 (47)
Treatment discontinued, n (%) 9 (26) 21 (64) 130 (44) 159 (53)
Reason for treatment discontinuation, n (%)
Disease progression 7 (20) 20 (61) 80 (27) 126 (42)
Adverse event 1 (3) 0 24 (8) 7 (2)
Physician decision 1 (3) 0 9 (3) 13 (4)
Protocol deviation 0 0 3 (1) 1 (<1)
Patient decision 0 1 (3) 12 (4) 12 (4)
Death 0 0 2 (1) 0
*Treatment ongoing at data cut‐off: January 29, 2016.

Primary Endpoint: Progression‐free Survival
Prob
ability of P
FS (%
)
201816141210864200
20
40
60
80
100
Time (months)
Asian region (n=68)
R + L (n=35) P + L (n=33)Median PFS, months (95% CI)
NR (14.9–NR)
11.0 (9.1–16.4)
HR (95% CI) 0.298 (0.134–0.662)
Non‐Asian region (n=600)
24221616121086420 18140
20
40
60
80
100
Prob
ability of P
FS (%
)
Time (months)
R + L (n=299) P + L (n=301)Median PFS, months (95% CI)
NR (19.3–NR)
15.2 (13.4–19.2)
HR (95% CI) 0.602 (0.457–0.792)
• PFS benefit with ribociclib + letrozole was also observed in Asian patients (by race): HR 0.387 (95% CI 0.166–0.906)
CI, confidence interval; HR, hazard ratio; L, letrozole; NR, not reached; P, placebo; PFS, progression‐free survival; R, ribociclib.
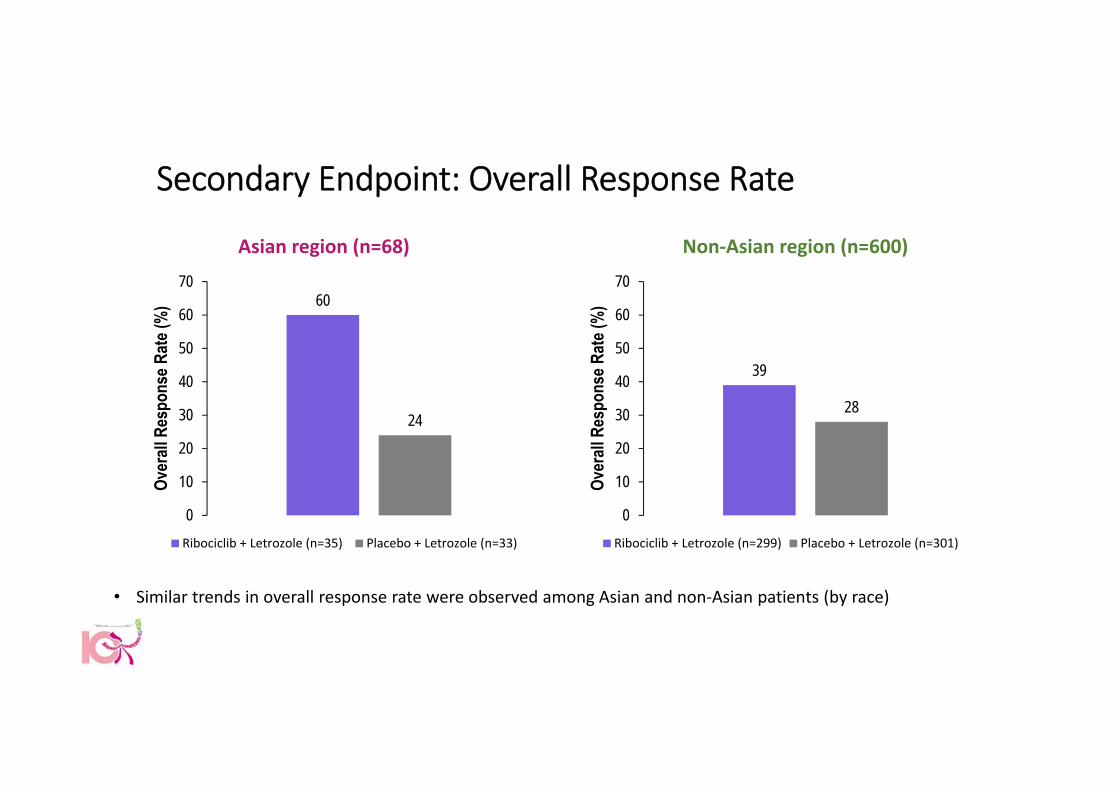
Secondary Endpoint: Overall Response Rate
Asian region (n=68) Non‐Asian region (n=600)
60%
24%
39%
28%
• Similar trends in overall response rate were observed among Asian and non‐Asian patients (by race)
60
24
0
10
20
30
40
50
60
70
Over
all R
espo
nse R
ate (
%)
Ribociclib + Letrozole (n=35) Placebo + Letrozole (n=33)
39
28
0
10
20
30
40
50
60
70
Over
all R
espo
nse R
ate (
%)
Ribociclib + Letrozole (n=299) Placebo + Letrozole (n=301)

Safety: All‐grade Adverse Events (≥20% of Patients)Asian region (n=68) Non‐Asian region (n=596)
All‐grade adverse events, n (%) Ribociclib + Letrozolen=35
Placebo + Letrozolen=33
Ribociclib + Letrozolen=299
Placebo + Letrozolen=297*
HematologicNeutropenia‡ 32 (91) 2 (6) 216 (72) 15 (5)Leukopenia§ 11 (31) 1 (3) 99 (33) 12 (4)Anemia 8 (23) 0 55 (18) 15 (5)
Non‐hematologicNausea 16 (46) 4 (12) 156 (52) 90 (30)Cough 10 (29) 7 (21) 55 (18) 52 (18)Rash|| 9 (26) 0 58 (19) 27 (9)Alopecia 8 (23) 5 (15) 103 (34) 46 (16)Upper respiratory tract infection 8 (23) 6 (18) 27 (9) 29 (10)Diarrhea 7 (20) 2 (6) 110 (37) 71 (24)
• All‐grade liver enzyme elevations were reported in 11% vs 3% of patients treated in Asian countries (ribociclib vs placebo arm)• No Asian patients in the ribociclib arm had QTcF prolongation >480 msec, or a >60 msec increase from baseline• A similar safety profile was observed among Asian patients (by race)
QTcF, QT corrected with Fridericia’s formula.All‐grade adverse events reported in ≥20% of patients treated in Asia in the ribociclib + letrozole arm are presented.
*4 patients in the placebo + letrozole arm did not receive study treatment; ‡neutropenia also includes ‘neutrophil count decreased’ and ‘granulocytopenia’; §leukopenia also includes ‘white blood cell count decreased’; ||rash also includes ‘maculopapular rash’.
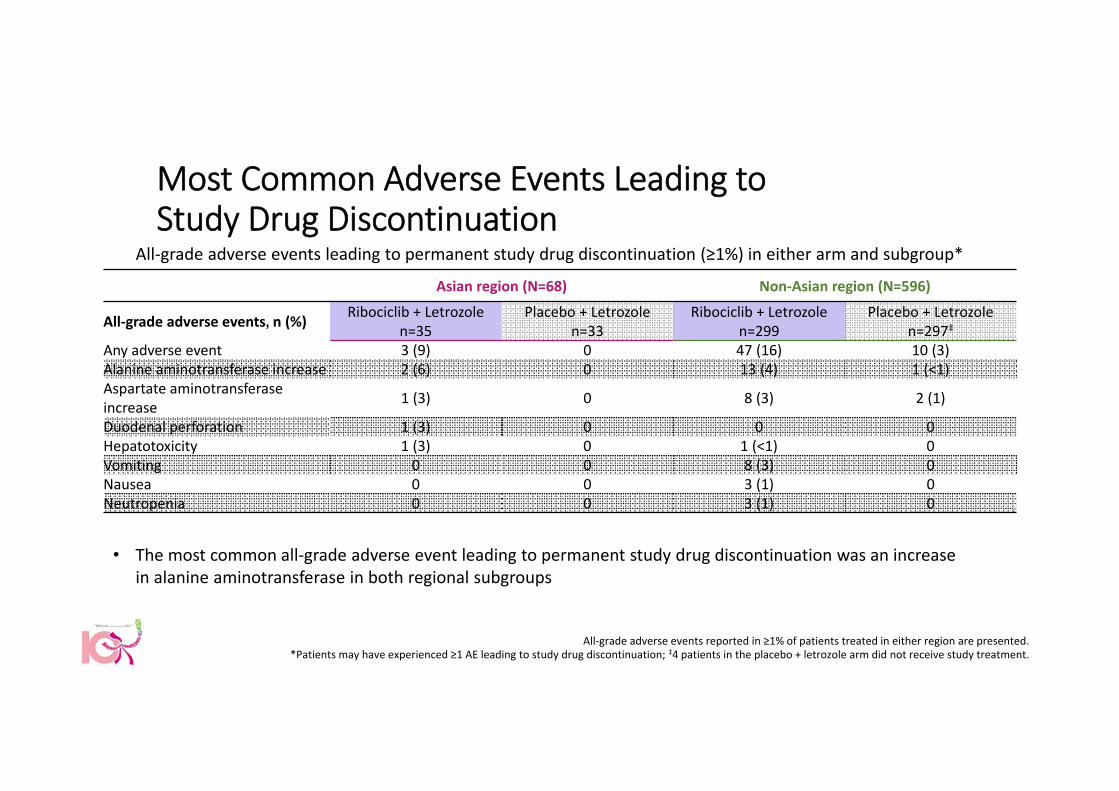
Most Common Adverse Events Leading to Study Drug Discontinuation
Asian region (N=68) Non‐Asian region (N=596)
All‐grade adverse events, n (%) Ribociclib + Letrozolen=35
Placebo + Letrozolen=33
Ribociclib + Letrozolen=299
Placebo + Letrozolen=297‡
Any adverse event 3 (9) 0 47 (16) 10 (3)Alanine aminotransferase increase 2 (6) 0 13 (4) 1 (<1)Aspartate aminotransferase increase 1 (3) 0 8 (3) 2 (1)
Duodenal perforation 1 (3) 0 0 0Hepatotoxicity 1 (3) 0 1 (<1) 0Vomiting 0 0 8 (3) 0Nausea 0 0 3 (1) 0Neutropenia 0 0 3 (1) 0
All‐grade adverse events leading to permanent study drug discontinuation (≥1%) in either arm and subgroup*
All‐grade adverse events reported in ≥1% of patients treated in either region are presented.*Patients may have experienced ≥1 AE leading to study drug discontinuation; ‡4 patients in the placebo + letrozole arm did not receive study treatment.
• The most common all‐grade adverse event leading to permanent study drug discontinuation was an increase in alanine aminotransferase in both regional subgroups

Treatment Exposure and Dose ModificationsAsian region (n=68)
Ribociclib/placebo Letrozole
Ribociclib + Letrozole n=35
Placebo + Letrozole n=33
Ribociclib + Letrozole n=35
Placebo + Letrozole n=33
Median duration of exposure, months (range) 12.6 (0–21) 11.6 (2–17) 13.5 (2–21) 11.6 (2–17)
Dose interruptions due to AEs, n (%) 26 (74) 2 (6) 1 (3) 1 (3)Dose reductions due to AEs, n (%) 21 (60) 0 – –Median relative dose intensity, % 87 100 100 100
Non‐Asian region (n=596)
Ribociclib/placebo Letrozole
Ribociclib + Letrozolen=299
Placebo + Letrozolen=297
Ribociclib + Letrozolen=299
Placebo + Letrozolen=297
Median duration of exposure, months (range) 12.1 (0–23) 12.6 (0–22) 12.9 (0–23) 12.6 (0–22)
Dose interruptions due to AEs, n (%) 201 (67) 42 (14) 45 (15) 13 (4)Dose reductions due to AEs, n (%) 148 (50) 14 (5) – –Median relative dose intensity, % 88 100 100 100
AE, adverse event.

Conclusions• First‐line ribociclib + letrozole significantly prolonged PFS compared with letrozole
alone in postmenopausal women with HR+, HER2– advanced breast cancer• Hazard ratio 0.556 (95% CI 0.429–0.720); p=0.00000329
• Clinically meaningful PFS benefit with ribociclib + letrozole was maintained in Asian patients• Hazard ratio: 0.298 (95% CI 0.134–0.662) in patients treated in Asian countries• Hazard ratio: 0.387 (95% CI 0.166–0.906) in Asian patients (by race)
• Combined ribociclib + letrozole treatment was well tolerated in Asian patients, with a similar safety profile as observed in the full population
• Neutropenia was the most common hematologic all‐grade adverse event and nausea was the most common non‐hematologic all‐grade adverse event in both populations
CI, confidence interval; HR+, hormone receptor‐positive; HER2–, human epidermal growth factor receptor 2‐negative; PFS, progression‐free survival.

Acknowledgments
Patients and their families who participated in MONALEESA‐2
Members of the Study Steering Committee, all investigators, research coordinators, and site staff
Members of the Data Monitoring Committee
This study was sponsored by Novartis Pharmaceuticals Corporation, who provided financial support for medical editorial assistance from ArticulateScience Ltd.
Ribociclib was discovered by Novartis Institutes for BioMedical Research in collaboration with Astex Pharmaceuticals
Countries with active centers Asian countries with active centers
Germany HungaryIrelandIsraelItalyLebanonNetherlandsNorwayRepublic of KoreaRussian Federation
ArgentinaAustraliaAustriaBelgiumBrazilCanadaCzech RepublicDenmarkFinlandFrance
SingaporeSouth AfricaSpainSwedenTaiwanThailandTurkeyUnited KingdomUSA