High-ResolutionArrayCGHandGeneExpressionPro lingof ... · Alveolar Soft Part Sarcoma Shamini...
11
Human Cancer Biology High-Resolution Array CGH and Gene Expression Profiling of Alveolar Soft Part Sarcoma Shamini Selvarajah 1,2 , Saumyadipta Pyne 2 , Eleanor Chen 1 , Ramakrishna Sompallae 4 , Azra H. Ligon 1,2 , Gunnlaugur P. Nielsen 3 , Glenn Dranoff 2 , Edward Stack 2 , Massimo Loda 1,2 , and Richard Flavin 1,2,5 Abstract Purpose: Alveolar soft part sarcoma (ASPS) is a soft tissue sarcoma with poor prognosis, and little molecular evidence exists for its origin, initiation, and progression. The aim of this study was to elucidate candidate molecular pathways involved in tumor pathogenesis. Experimental Design: We employed high-throughput array comparative genomic hybridization (aCGH) and cDNA-Mediated Annealing, Selection, Ligation, and Extension Assay to profile the genomic and expression signatures of primary and metastatic ASPS from 17 tumors derived from 11 patients. We used an integrative bioinformatics approach to elucidate the molecular pathways associated with ASPS pro- gression. FISH was performed to validate the presence of the t(X;17)(p11.2;q25) ASPL–TFE3 fusion and, hence, confirm the aCGH observations. Results: FISH analysis identified the ASPL–TFE3 fusion in all cases. aCGH revealed a higher number of numerical aberrations in metastatic tumors relative to primaries, but failed to identify consistent alterations in either group. Gene expression analysis highlighted 1,063 genes that were differentially expressed between the two groups. Gene set enrichment analysis identified 16 enriched gene sets (P < 0.1) associated with differentially expressed genes. Notable among these were several stem cell gene expression signatures and pathways related to differentiation. In particular, the paired box transcription factor PAX6 was upregulated in the primary tumors, along with several genes whose mouse orthologs have previously been implicated in Pax6 DNA binding during neural stem cell differentiation. Conclusion: In addition to suggesting a tentative neural line of differentiation for ASPS, these results implicate transcriptional deregulation from fusion genes in the pathogenesis of ASPS. Clin Cancer Res; 20(6); 1521–30. Ó2014 AACR. Introduction Alveolar soft-part sarcoma (ASPS) is a rare mesenchymal tumor of uncertain histogenesis. The tumor occurs primar- ily in adolescent and young adults with a female predilec- tion, and accounts for 0.4% to 1% of all soft tissue sarcomas (1). Commonly, the tumor involves the deep soft tissues of the extremities, buttocks, abdominal, or thoracic wall in adults, and the head and neck region in children. ASPS has also been reported in tissues where skeletal muscle is not usually found, such as the stomach, pituitary gland, sacral bone, breast, lung, retroperitoneum, and female genital tract (1–3). ASPS is a malignant tumor with a slow, indolent clinical course, with survival rates of 77% at 2 years, 60% at 5 years, 35% at 10 years, and only 15% at 20 years (1). It is not particularly responsive to adjuvant chemotherapy, although there may be some role for adjuvant radiotherapy in reducing the risk of local recurrence (1). Vascular inva- sion is common with subsequent hematogenous metastases to lung and brain, and although prolonged survival is possible in such patients, the longer-term disease-specific mortality is high. Although tumor size has been correlated to the survival in the past (4), no specific clinical or histo- pathologic features exist currently that are reliably predic- tive of disease course in ASPS. Since its description by Christopherson in 1952, the histogenesis of ASPS has remained controversial. Histolog- ically, ASPS exhibits variable architecture ranging from alveolar to solid patterns composed of nonspecific, uniform round cells with central nuclei, diastase periodic acid Schiff (DPAS)–positive granular cytoplasmic crystals, and charac- teristic rectangular/rhomboid cytoplasmic crystals seen Authors' Affiliations: 1 Department of Pathology, Brigham and Women's Hospital, Harvard Medical School; 2 Center for Molecular Oncologic Pathol- ogy, Dana-Farber Cancer Institute; 3 Massachusetts General Hospital, Boston, Massachusetts; 4 Carver College of Medicine, University of Iowa, Iowa City, Iowa; and 5 Department of Pathology, St. James's Hospital, Dublin, Ireland Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). M. Loda and R. Flavin share senior authorship of this article. Corresponding Author: Richard Flavin, St. James's Hospital, James's Street, Dublin 8, Ireland. Phone: 353-01-416-2992; Fax: 353-01-410-3514; E-mail: fl[email protected] doi: 10.1158/1078-0432.CCR-13-2090 Ó2014 American Association for Cancer Research. Clinical Cancer Research www.aacrjournals.org 1521 on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090
Transcript of High-ResolutionArrayCGHandGeneExpressionPro lingof ... · Alveolar Soft Part Sarcoma Shamini...

Human Cancer Biology
High-Resolution Array CGH and Gene Expression Profiling ofAlveolar Soft Part Sarcoma
Shamini Selvarajah1,2, Saumyadipta Pyne2, Eleanor Chen1, Ramakrishna Sompallae4, Azra H. Ligon1,2,Gunnlaugur P. Nielsen3, Glenn Dranoff2, Edward Stack2, Massimo Loda1,2, and Richard Flavin1,2,5
AbstractPurpose: Alveolar soft part sarcoma (ASPS) is a soft tissue sarcoma with poor prognosis, and little
molecular evidence exists for its origin, initiation, and progression. The aim of this study was to elucidate
candidate molecular pathways involved in tumor pathogenesis.
Experimental Design: We employed high-throughput array comparative genomic hybridization
(aCGH) and cDNA-Mediated Annealing, Selection, Ligation, and Extension Assay to profile the genomic
and expression signatures of primary andmetastatic ASPS from17 tumors derived from11patients.Weused
an integrative bioinformatics approach to elucidate the molecular pathways associated with ASPS pro-
gression. FISH was performed to validate the presence of the t(X;17)(p11.2;q25) ASPL–TFE3 fusion and,
hence, confirm the aCGH observations.
Results: FISH analysis identified the ASPL–TFE3 fusion in all cases. aCGH revealed a higher number of
numerical aberrations inmetastatic tumors relative to primaries, but failed to identify consistent alterations
in either group. Gene expression analysis highlighted 1,063 genes thatwere differentially expressed between
the two groups. Gene set enrichment analysis identified 16 enriched gene sets (P < 0.1) associated with
differentially expressed genes. Notable among these were several stem cell gene expression signatures and
pathways related to differentiation. In particular, the paired box transcription factor PAX6was upregulated
in the primary tumors, along with several genes whosemouse orthologs have previously been implicated in
Pax6 DNA binding during neural stem cell differentiation.
Conclusion: In addition to suggesting a tentative neural line of differentiation for ASPS, these results
implicate transcriptional deregulation from fusion genes in thepathogenesis of ASPS.ClinCancer Res; 20(6);
1521–30. �2014 AACR.
IntroductionAlveolar soft-part sarcoma (ASPS) is a rare mesenchymal
tumor of uncertain histogenesis. The tumor occurs primar-ily in adolescent and young adults with a female predilec-tion, and accounts for 0.4% to 1%of all soft tissue sarcomas(1). Commonly, the tumor involves the deep soft tissues ofthe extremities, buttocks, abdominal, or thoracic wall inadults, and the head and neck region in children. ASPS has
also been reported in tissues where skeletal muscle is notusually found, such as the stomach, pituitary gland, sacralbone, breast, lung, retroperitoneum, and female genitaltract (1–3). ASPS is amalignant tumorwith a slow, indolentclinical course, with survival rates of 77% at 2 years, 60% at5 years, 35% at 10 years, and only 15% at 20 years (1). It isnot particularly responsive to adjuvant chemotherapy,although there may be some role for adjuvant radiotherapyin reducing the risk of local recurrence (1). Vascular inva-sion is commonwith subsequent hematogenousmetastasesto lung and brain, and although prolonged survival ispossible in such patients, the longer-term disease-specificmortality is high. Although tumor size has been correlatedto the survival in the past (4), no specific clinical or histo-pathologic features exist currently that are reliably predic-tive of disease course in ASPS.
Since its description by Christopherson in 1952, thehistogenesis of ASPS has remained controversial. Histolog-ically, ASPS exhibits variable architecture ranging fromalveolar to solid patterns composed of nonspecific, uniformround cells with central nuclei, diastase periodic acid Schiff(DPAS)–positive granular cytoplasmic crystals, and charac-teristic rectangular/rhomboid cytoplasmic crystals seen
Authors' Affiliations: 1Department of Pathology, Brigham and Women'sHospital, HarvardMedical School; 2Center forMolecularOncologic Pathol-ogy, Dana-Farber Cancer Institute; 3Massachusetts General Hospital,Boston, Massachusetts; 4Carver College of Medicine, University of Iowa,Iowa City, Iowa; and 5Department of Pathology, St. James's Hospital,Dublin, Ireland
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
M. Loda and R. Flavin share senior authorship of this article.
Corresponding Author: Richard Flavin, St. James's Hospital, James'sStreet, Dublin 8, Ireland. Phone: 353-01-416-2992; Fax: 353-01-410-3514;E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-13-2090
�2014 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 1521
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

with the electronmicroscope. On the basis of the morphol-ogy, this entity has been designated in the past as bothmalignant organoid granular cell myoblastoma and malig-nant nonchromaffin paraganglioma, inferring myogenicand neurogenic differentiation, respectively.
The current singular definingmolecular feature of ASPS isthe nonreciprocal translocation t(X;17)(p11;q25), result-ing in the fusion of the nuclear transcription factor geneTFE3 to the ASPL gene (5). Although this translocation isnot specific to ASPS (occurring in a subset of renal cellcarcinoma, RCC; ref. 6), it is consistently and uniformlypresent in all ASPS cases. In this study, we employed high-throughput technology to profile the genomic and geneexpression signatures of primary and metastatic ASPS.Moreover, we used an integrative bioinformatics approachto elucidate the molecular pathways associated with theprogression of ASPS.
Materials and MethodsCase selection
Paraffin blocks from surgical specimens covering a 13-year period (1994–2007) were obtained from the archivesof Massachusetts General Hospital, Brigham and Women’sHospital, and Boston Children’s Hospital (Boston, MA), inaccordance with the regulations for excess tissue use stip-ulated by the institutional review board at each hospital.Altogether, 17 tumors from 11 patients were used for thisstudy. Archival material corresponding to both the primarytumor sites as well as from metastases or re-excisions wasavailable for four of the cases. All cases were fixed in 10%
neutral-buffered formalin and routinely embedded inparaffin. Pertinent clinical data are summarized in Table1. Diagnosis was confirmed by retrospective review ofhematoxylin and eosin (H&E)–stained sections by studypathologist E. Chen.WorldHealthOrganization diagnosticcriteria were used for assigning histopathology diagnoses(7). Where necessary, periodic acid–Schiff (PAS) staining,TFE3 immunohistochemistry, and electron microscopywere utilized as ancillary aids to diagnosis (Fig. 1).
ImmunohistochemistryWe used the P-16 polyclonal antibody to TFE3 (Santa
Cruz# sc-5958; Santa Cruz Biotechnology), which bindsto the C-terminal portion of the TFE3 protein downstreamof the region encoded by exon 6 to help confirm thediagnosis of ASPS (6). Representative 5-mm formalin-fixed,paraffin-embedded (FFPE) sections from each case weremounted onto positively charged slides and, subsequently,processed for immunohistochemical (IHC) staining using astandard protocol. Briefly, the sections were deparaffinizedin xylene, rehydrated using graded ethanol concentrations,and then subjected to antigen retrieval by boiling in citratebuffer at pH 6.0 for 10 minutes. Following quenching withperoxidase and blocking with avidin, sections were incu-bated overnight with a 1:500 dilution of the polyclonalantibody toTFE3 in PBS.Detectionof antibody bindingwasachieved using a biotinylated secondary antibody andhorseradish peroxidase–conjugated streptavidin (Dako)and 3,3,5,50-diaminobenzidine as chromogen.
FISHLoci corresponding to the TFE3 and ASPL genes were
visualized by dual color, single fusion FISH design. Fluo-rescent probes were generated by nick translation of bacte-rial artificial chromosome (BAC) clones RP11-634L102(labeled SpectrumOrange) and CTD-2311N12 (Spectrum-Green) BACs (obtained from CHORI; www.chori.org),which map to 17q25 and Xp11.2, respectively. RP11-634L102 includes almost the entire ASPL gene, whereasthe latter includes the entire TFE3 locus (SupplementaryFig. S1).
Four-micrometer FFPE sections were mounted on stan-dard glass slides and baked at 60�C overnight. Followingdeparaffinization in xylene, the sections were dehydrated inethanol and air dried. The sections were subsequentlytreated in 1 mol/L sodium isothiocyanate in 2� sodiumchloride–sodium citrate (SSC) for 20 minutes at 75�C, andrinsed in 2� SSC for 5minutes at room temperature, beforedigestion in 0.25mg/mL proteinase K (Roche) in 2� SSC at45�C for 20minutes. The slides were rinsed in 2� SSC, thendehydrated in ethanol series, and air dried. The probe andtarget DNA (tissue sections) were codenatured at 80�C for10minutes (Hybrite; AbbottMolecular Inc.) and allowed tohybridize for 16 hours at 37�C. Post-hybridization washeswere carried out in 2� SSC at 70�C for 10 minutes, then atroom temperature for 5minutes. The sectionswere counter-stained with 40,6-diamidino-2-phenylindole (DAPI; AbbottMolecular Inc.), and signals were visualized on anOlympus
Translational RelevanceIn this article, we provide one of the largest high-
resolution oligonucleotide aCGH and expression anal-yses of primary andmetastatic alveolar soft part sarcoma(ASPS) samples to elucidate candidate molecular path-ways involved in tumor pathogenesis. We also usedan integrative bioinformatic approach to elucidate themolecular pathways associated with the ASPS progres-sion. We report numerous gene sets that were differen-tially expressed between primary andmetastatic tumors.Notable among these were several stem cell gene expres-sion signatures and pathways related to differentiation,including the paired box transcription factor PAX6. Inaddition to suggesting a tentative neural line of differ-entiation forASPS, these results implicate transcriptionalderegulation from fusion genes in the ASPS pathogen-esis, rather than extensive chromosomal instability. Inthis regard, an improved understanding of the aberranttranscriptional mechanisms in ASPS pathogenesis canlead to the identification of key genes in pathwaysthat can represent potential therapeutic targets and/orpotential markers for sensitivity to specific anticancertreatments.
Selvarajah et al.
Clin Cancer Res; 20(6) March 15, 2014 Clinical Cancer Research1522
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

Tab
le1.
Sum
maryof
clinical
features
intheASPSstud
yco
hort
Patient/site
Age/se
xOutco
me
Surviva
ldTreatmen
tDiagno
sis
FISHa
ACGH
alterations
1MT(lu
ng)
30F
Dea
d84
Sys
temic
chem
othe
rapy
TFE3þ
NA
Non
eob
served
2MT(lu
ng)
36M
Awd
132
Clinical
trial:Gleev
ecEM,D
PASþ
46%
;multip
lefusion
sign
als
Loss
of1ch
rX;b
reak
point
atXp11
.2(gainto
pter);
loss
at17
q25
;los
sof
8p,1
7p;los
sof
chr1
(slig
htsh
ift);ch
r12ga
in3M
T(adrena
l)41
FDea
d72
Non
eEM
22%
NA
4MT(lu
ng)
27M
Lost
tofu
72Sys
temic
chem
othe
rapy
TFE3þ
20%
Loss
of1ch
rX;b
reak
point
atXp11
.2(gainto
pter);
copy
loss
of19
qan
d22
q5M
T(pan
crea
s)47
MAwd
156
Non
eTF
E3þ
72%
Loss
of1ch
rX;b
reak
point
atXp11
.2(gainto
pter);
loss
of17
q25
ban
d;loss
of1p
and18
p6P
(thigh)
b29
MDea
d60
Non
eEM
17%
Loss
of1ch
rX;b
reak
point
atXp11
.2(gainto
pter);
noad
dition
alalteratio
ns6M
T1(colon
)bNon
eTF
E3þ
66%
Loss
of1ch
rX;b
reak
point
atXp11
.2(gainto
pter);
noad
dition
alalteratio
ns6M
T2(abdom
en)b
TFE3þ
20%
Loss
of1ch
rX;b
reak
point
atXp11
.2no
tiden
tified
;no
addition
alalteratio
ns7P
(retro-orbita
l)b27
MAwd
60Non
eMorpho
logy
cNA
NA
7MT(brain)b
Non
eTF
E3þ
NA
One
copy
loss
of10
qan
d22
q;BRUNOL4
loss
(18q
12.2);
break
point
atXp11
.2(gainto
pter)
8MT(brain)
28M
Dea
d16
Sys
temic
chem
othe
rapy
Morpho
logy
cNA
NA
9P(th
igh)
b28
FDea
d36
Non
eEM
80%
Multip
lealteratio
ns9M
T(brain)b
Rad
iotherap
yMorpho
logy
c48
%Non
eob
served
10P(bac
k)20
MNed
24Non
eDPASþ
80%
One
copy
loss
of21
q;los
sof
1ch
rX;b
reak
point
atXp11
.2(gainto
pter)
11MT1
(intestine)
b27
FAwd
168
Intestinal
chem
othe
rapy
EM
56%
Break
point
atXp11
.2no
tiden
tified
;multip
lealteratio
ns11
MT2
(femur)b
Rad
iotherap
yMorpho
logy
cNA
NA
12P(buttock
)26
FAwd
72Non
eEM
46%
Break
point
atXp11
.2;n
oad
dition
alalteratio
ns13
P(nec
k)47
FAwd
96Non
eEM
35%
;multip
lefusion
sign
als
11alteratio
ns;b
reak
pointat
Xp11
.2but
loss
from
TFE3to
pteran
dbreak
point
isdow
nstrea
mof
TFE3
Abbreviations
:Awd,a
livewith
dise
ase;
chr,ch
romos
omeF;
EM,e
lectronmicrosc
opy;
F,female;
fu,follow
up;M
,male;
MT,
metas
tase
s;NA,n
otav
ailable;N
ed,n
oev
iden
ceof
disea
se;P
,prim
ary.
aPerce
ntag
eof
tumor
nuclei
with
fusion
.bPairedsa
mples.
cSim
ilarto
prim
arytumor.
dIn
mon
ths.
Molecular Profiling of Alveolar Soft Part Sarcoma
www.aacrjournals.org Clin Cancer Res; 20(6) March 15, 2014 1523
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

BX51 fluorescence microscope (Olympus). Individualimages were captured using an Applied Imaging systemrunning CytoVision Genus version 3.9 (Applied Imaging).
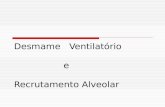
Tumor regions were identified on each section by pathol-ogists (E. Chen and R. Flavin) from corresponding H&Esections of the FFPEblock. Analysiswas limited to the intact,nontruncated andnonoverlapping tumor cell nuclei. A totalof 50 nuclei per section were sampled from two separateregions, and FISH signals were scored for the number ofTFE3 (green), ASPL (red), and fusion signals in each nucle-us. Signals were deemed to be fused when the red and greensignals were separated by less than three signal diameters.The FISH criteria used to evaluate theASPL–TFE3 rearrange-ment were as follows: (i) in female patients, visualization oftwo green TFE3 (another normal Xp11 signal) and one redASPL separate signals in addition to a fusion signal; (ii) inmale patients, visualization of one green and one red ASPLsignal in addition to a fusion signal (Fig. 1 and Supple-mentary Fig. S1).
Oligonucleotide human genome 500k aCGHNormal female genomic DNA was obtained from Pro-
mega. Genomic DNA was extracted from 15 samples ofASPS tumors (5 primary and 10 metastases) using theQIAampDNAFFPETissue Kit (Qiagen). TheGenomicDNAULS labeling kit for FFPE Samples (Agilent) was used tochemically label 1 mg of genomic DNAwith either ULS-Cy5(tumor) or ULS-Cy3 dye (normal/reference DNA), accord-ing to the manufacturer’s protocol (Agilent Technologies,Inc.). An equimolar mixture of labeled normal and tumorDNA was applied to the Agilent Human Genome CGH
2�400k Microarray, which features 411,056 in situ synthe-sized 60-mer oligonucleotide probes that span coding andnoncoding sequences with an average spatial resolution of5.3 kb. Hybridization was carried out at 65�C for 40 hours,in a rotating oven at 20 rpm. The arrays were washedaccording to themanufacturer’s protocol, and then scannedusing an Agilent DNA microarray scanner. CGH Analyticssoftware version 3.4 (Agilent Technologies) was used toanalyze the aCGH data.
Thedataquality of eachmicroarraywas assessedusing theQuality Metrics report generated by the Agilent CGH ana-lytics software (v.3.4). Copy-number aberrations weredetected using the aberration detection method (ADM-1)algorithm, based on computing significance scores for allgenomic intervals. Aberrations were assigned as either gain(ratio � 0.5), loss (�–1.0), or amplification (�2.0). Acontiguous change of imbalance level within a chromo-some was considered to be indicative of an unbalancedtranslocation event. For this study, the threshold was opti-mized to a value of 6.0 to reduce inherent sample noisecontribution in the analysis, without negating true consis-tent imbalances along each chromosome. Only aberrationsspanning a minimum of 10 consecutive oligonucleotideprobes were marked as significant, so that only imbalancesspanning greater than approximately 50 kb will be includ-ed. Further details about these principles are available at theAgilent website (www.agilent.com/chem/goCGH). Arraydata have been published in compliance with MIAME 2.0guidelines and deposited in the publicly available NationalCenter for Biotechnology Information Gene ExpressionOmnibus (NCBI GEO) database (GSE49327).
A B
C D
Figure 1. Case of ASPS. A,H&E (�10) of tumor highlightingthe alveolar to solid pattern.B, positive nuclear TFE3immunohistochemistry (�40). Cand D, interphase FISH with BAC-based probes harboring TFE3 andASPL on amale patient with ASPS.
Selvarajah et al.
Clin Cancer Res; 20(6) March 15, 2014 Clinical Cancer Research1524
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

cDNA-mediated annealing, selection, ligation, andextension assayThirteen cases were amenable to global gene expression
analysis (five primary tumors and eight metastases). Twosamples were matched primary and metastatic tumors; twowere paired cases of metastatic lesions from different sites.For each sample, H&E sectionswere viewed by a pathologist(R. Flavin) to ensure at least 80% tumor content. Fiveconsecutive 20-mm sections were collected for analysis.Total RNA was extracted, cleaned up, and eluted using theRNeasy MiniKit and RNeasy MinElute Cleanup Kit, respec-tively (Qiagen), according to the manufacturer’s protocol.The total RNA yield per sample ranged from 191 ng to 2 mg.cDNA-mediated annealing, selection, ligation, and exten-sion (DASL) expression assay (Illumina) was performedas per manufacturer’s instructions on a panel comprising24,526 probes for a total of 18,631 genes (Human Ref-8Expression; BeadChip).Data were quantile normalized and a two-sample t test
was used to detect differential expression of every geneacross five primary and eight metastatic sarcomas usingBroad Institute’s GenePattern platform. We obtained genesets representing key biologic processes from GO, diseasepathways from Molecular Signature Database (MSigDB),and gene expression signatures from the literature fromGenesigDB were used for gene set enrichment analysis. Theenrichment of each gene set among the top differentiallyexpressed genes was tested with two-sided hypergeometrictest in R. Finally, we used the Ingenuity Pathway Analysistool to construct a network of direct and indirect interac-tions among the differentially expressed genes that containPAX6-specific putative regulatory binding sites in theirpromoter regions.
Clinicopathologic correlationWe examined whether the presence of simple or complex
chromosomal abnormalities was associated with clinico-pathologic features of the ASPS samples (simple chromo-somal abnormalities was defined as the presence of two orless gross abnormalities, including the breakpoint atXp11.2). Two by two group comparison was performedusing the Fischer exact test. In addition, we examinedwhether the presence of simple or complex chromosomalabnormalities was associatedwith patient survival. Kaplan–Meier survival analysis was performed using the log-ranktest. Statistical analysis was performed with both Analyse-ItSoftware Ltd. and MedCalc Software Ltd.
ResultsDifferential gene expression analysis and pathwayanalysisOn the basis of the t test for differential gene expression
across primary and metastatic sarcomas, 1,063 genes werefound to be significant at the nominal P value level of 0.05,of which 323 genes with a t test score greater than 3 weremost differentially expressed; the full set of data maybedownloaded fromNCBIGEO(GSE49327). Among these
top differentially expressed genes, 207 were upregulated inprimary and 116 in metastases. The differential expressionheat map is shown in Fig. 2. Gene set enrichment analysisidentified 16 gene sets as enriched (P < 0.1), both amonggenes that are upregulated in primary and metastatic sar-comas (Supplementary Fig. S2). We observed that severalstem cell gene expression signatures andpathways related todifferentiation are enriched among the top differentiallyexpressed genes (Fig. 3 and Supplementary Fig. S2). Inparticular, we noted distinct upregulation of the paired boxtranscription factor PAX6 and PAX6 target genes in primarysarcomas (Figs. 3 and4). Interestingly, oneof the targets, theLIM/homeobox protein Lhx6, is an important transcriptionregulator that is known to control differentiation anddevelopment of neural cells (8). By observing the knowndirect and indirect interactions among the differentiallyexpressed genes that have putative binding sites in theirpromoters, we noted interesting subnetworks of hub nodesand GeneGO processes. Moreover, indirect connectionsbetween TFE3 and PAX6 via genes involved in the TGF-bsignaling pathway could be inferred (SupplementaryFig. S3).
Oligonucleotide human genome 500k aCGHGenomic aberrations in ASPS were analyzed using the
Agilent 2� 500k high-resolution aCGH platform with
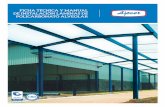
Figure 2. Top 323 differentially expressed genes. The heat map depictsthe expression of genes with a t test score greater than 3. Each rowrepresents a gene. The samples (in columns) are grouped as five primary(green labels) and eight metastatic (gold labels) sarcomas. Red and blueentries in the heat map indicate high and low gene expressions,respectively. The black horizontal line separates the genes upregulated inprimary sarcomas (above the line) from those upregulated in metastases.
Molecular Profiling of Alveolar Soft Part Sarcoma
www.aacrjournals.org Clin Cancer Res; 20(6) March 15, 2014 1525
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

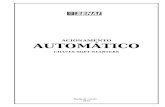
protocols optimized for FFPE tumor material (9). Asexpected from the unbalanced rearrangement involving theX chromosome, the most frequent genomic aberrationdetected was a large segmental gain on Xp, with the break-point localizing at TFE3 and extending telomeric to it (10 of14 cases; Table 1 andFig. 5).Genomic loss at 17q25was alsoobserved frequently, although the amplitude of the alter-ation showed variation between samples. The only sharedalteration thatwas observed in twometastatic sampleswas a1 copy loss of chromosome 22. A few samples displayedmultiple aberrations, such as sample 2M, which is a met-astatic tumor sample from the lungs of a patient beingtreated with the kinase inhibitor Gleevec. This patient wasa male and, as expected, the chromosome X profile showeda relative loss from Xp11.2 to Xqter, and gain of sequencesfrom Xp11.2 to Xpter that one would expect in a fusion-positive sample.We alsoobservedmultiple fusion signals inaddition to numerous whole chromosomal as well aswhole-arm imbalances in this sample, such as loss of 8pand17p and gainof entire chromosomes 12 and14. Sample14P, which is a primary tumor excised from the neck of afemale patient, showed an atypical genomic profile forchromosome X. Instead of showing the characteristic gain
from the TFE3 locus to pter, we actually observed theopposite, which was a large segmental loss of the p-armfrom TFE3 to pter. Not only did this sample show multiplefusion signalswith FISHanalysis, but like sample 2, this alsohad a segmental loss on chromosome 17 from 17p12 topter, among numerous other alterations. Otherwise, we didnot observe any consistent genomic imbalances when com-paring primary and metastatic tumors, and no high-levelamplifications were found in any of the tumors.
FISHDual-color, single-fusion FISH was performed on 4-mm
tissue sections to validate the presence of the t(X;17)(p11.2;q25) ASPL–TFE3 fusion and, hence, to confirm the aCGHobservations. For each sample, a total of 50 interphasenuclei were analyzed using the RP11-634L102 (Spectru-mOrange) and CTD-2311N12 (SpectrumGreen) home-brew probes. A baseline for false-positive fusion signals of1% was established by probing synovial sarcoma, whichharbors a t(X;18) rearrangement. Of the 15 tumors ana-lyzed, two samples failed to show signals and showedperinuclear chromatin halos, consistent with severe degra-dation of DNA. The remaining 13 samples consistentlyexhibited the characteristic ASPL–TFE3 fusion (Fig. 1),according to the expected gender-specific pattern. It isnoteworthy, however, that the fusion was not uniformlypresent in all cells within the analyzed tissue regions; thevast majority of the samples contained less than 50%fusion-positive cells, with two samples exceeding 70%fusion-positive cells (Table 1). Genomic heterogeneity wasfurther indicated by the presence of additional fusion sig-nals in two of the samples (2M and 14P), as also observedon aCGH. In these sections, themajority of the cells showedthe characteristic pattern,with few interspersed populationsof cells that displayed two fusion signals, in addition toseparately localized red and green signals. No consistentdifferences were observed between the primary, recurrent,andmetastatic tumors with regard to the pattern or numberof fusion-positive nuclei.
Clinicopathologic featuresTherewas no statistically significant relationship between
the presence of simple or complex chromosomal abnor-malities and the clinicopathologic features of age, sex, site ofdisease, patient status, whether adjuvant therapy wasreceived, and type of therapy (Supplementary Table S1).Genomic imbalance did not exhibit a statistically significantrelationship with overall patient survival (P ¼ 0.13 by log-rank test).
DiscussionIn this study, we employed high-throughput approaches
to profile the genomic and expression signatures of primaryand metastatic ASPS. Moreover, we used an integrativebioinformatics approach to elucidate the molecular path-ways associated with the progression of ASPS. To our
Figure 3. Gene set enrichment analysis for all top differentially expressedgenes. Each column represents a gene set that is either a key biologicprocess/pathway/gene signature from the literature that is enrichedamong the top 323 differentially expressed genes. Each horizontalorange bar represents one of the top differentially expressed genesdepicted in the sorted order t test score. The black horizontal lineseparates the genes upregulated in primary sarcomas (above the line)from thoseupregulated inmetastases. The occurrenceof Pax6, as a stemcell transcription factor, is marked with a green arrow, and thedistribution of its targets among the differentially expressed genesaccording to mouse ChIP studies (32) is shown with green marks besidethe plot.
Selvarajah et al.
Clin Cancer Res; 20(6) March 15, 2014 Clinical Cancer Research1526
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

knowledge, this is the most comprehensive and largestcohort of ASPS cases analyzed to date.Gene expression profiling identified a number of key
gene sets in ASPS pathogenesis, a number of which werepreviously identified in three previous microarray studies,thereby providing cross-validation for our current analysis(10–12). These included the hypoxia, hypoxia-induciblefactor (HIF), and angiogenesis pathways, suggesting anactive role for these gene sets in ASPS pathogenesis andfurther supporting the rationale for the use of antiangio-genic inhibitors in therapeutic regimens for the disease.Interestingly, the study by Kobos and colleagues examinedthe functional properties of the ASPSCR1–TFE3 fusiononcoprotein, defined its target promoters on a genome-wide basis, and performed a high-throughput RNA inter-ference screen to identify which of its transcriptional targetscontribute to cancer cell proliferation (12). HIF1a wasobserved to be a shared target between both this study andour own analysis. Although HIF1a has a central role in theadaptation of tumor cells to hypoxia by activating thetranscription of targeting genes, its dysregulation is seen innumerous other types of neoplasias (13). Although this is acomprehensive study, the overall biologic questionaddressed is significantly different from the one beingaddressed in our study. Specifically, the study design byKobos and colleagues questions the mechanism by whichthe primary tumors arise, thus profiling the molecularsignature of the early events in ASPS oncogenesis. In con-
trast, our study specifically interrogates the molecularmechanisms in the critical events of metastasis.
Recurrent regions of copy-number abnormalities in thegenomic DNA of tumors can identify genes that drivedisease pathogenesis. In this study, we therefore focusedon identifying recurrent regions of gain or loss in primaryand metastatic samples using a unique high-throughputapproach. Until now, there has only been one metaphaseCGH study on ASPS, which revealed gains of 1q, 8q, and16q, including the gain of Xp11�pter (14). In this study,high-resolution aCGH revealed a higher number of numer-ical aberrations in metastatic tumors relative to primaries,but failed to identify any consistent alterations in eithergroup. Indeed, our analysis identified gains and losses notpreviously observed in ASPS, such as the imbalances seen insample 2M (Table 1). Multiple and complex abnormalitiesinvolving deletions, translocations, trisomy 12, and loss ofchromosome 17, obtained after chemotherapy, have beendescribed (15). Given that we sawmultiple fusion signals insample 2M, it is likely that this tumor exhibits aneuploidy asa result of increasing chromosomal instability during themetastatic process. The only shared alteration that wasobserved in two metastatic samples was a 1 copy loss ofchromosome 22. As expected from the unbalanced rear-rangement involving the X chromosome, themost frequentchromosomal aberration detected was a large segmentalgain on Xp, with the breakpoint localizing at the TFE3 geneand extending telomeric to it. Genomic loss at 17q25 was
Figure 4. Differential expression ofPax6 targets. The heat mapdepicts the top differentiallyexpressed genes (in rows) whosemouse orthologs show Pax6binding with DNA in ChIP studies(32) in the process of neural stemcell differentiation in thedeveloping mouse cerebral cortex.The samples (in columns) aregrouped as primary (green labels)and metastatic (gold labels)sarcomas. Red and bluerectangles indicate high and lowgene expressions, respectively.The expression of the paired boxtranscription factor Pax6 is shownin the topmost row.
Molecular Profiling of Alveolar Soft Part Sarcoma
www.aacrjournals.org Clin Cancer Res; 20(6) March 15, 2014 1527
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

also observed frequently, though the amplitude of thealteration showed variation between samples. This seemedto correlate with the percentage of fusion-positive cellsin the tumor samples (data not shown). As previouslyreported, this is the hallmark translocationof ASPS. Ladanyiand colleagues showed that this unbalanced translocationresults in the fusion of TFE3 on Xp11.2, a member of thebasic helix–loop–helix family of transcription factors, toASPL on 17q25. The resulting fusion gene encodes chimericASPL–TFE3 RNA transcripts. Two mutually exclusivetypes of fusion products, designated type 1 and type 2, areobserved (5). ASPL exons 1–7 are fused to TFE3 exon 6 intype 1 and exon 5 in type 2 transcripts (16). Interestingly,TFE3 is also found to be rearranged by specific reciprocaltranslocations involving Xp11.2 in a subset of pediatricRCCs, of which one variant translocation is a balancedt(X;17)(p11.2;q25), the breakpoints of which are cytoge-netically identical to the translocation that is characteristicof ASPS (6).
A remarkable observation was that the low prevalence ofthe t(X;17)(p11.2;q25) rearrangement in tumor sampleswas belied by the uniform nuclear staining that wasobserved with TFE3 IHC staining. Discrepancy may arisefrom the fact that we were comparing a quantitative (FISH)method with a semiquantitative (IHC) method. Although
the enumeration process in FISH is based on quantifyingdiscrete signals, interpretation of IHC staining is generallymade in a qualitative and subjective manner, where apositive result might refer to the presence of staining inany part of the studied tissue. Another reason for thisdiscrepancy stems from a limitation of detecting rearrange-ments in FFPE tissue sections. Part of the cell can be lostduring the sectioning process, leading to artificially inducedloss of a significant percentage of nuclei. This truncationeffect can generate a high false-negative rate of cells losingsignals due to section artifact when using a 5-mm section.Finally, it is noteworthy that the IHCand the FISHassays fora given tumor were not always performed on the same FFPEblocks. Specifically, the IHC assays were routinely per-formed on the samples as a part of the diagnostic workupand, in some cases, the particular blocks were not availablefor the retrospective FISH assays. Given the heterogeneousnature of the sarcomas, a part of the discrepancy may beattributable to the variation in the tumor makeup.
Conflicting theories on the cellular origin of ASPS (i.e.,myogenic vs. neurogenic) have been proposed in the liter-ature, with the former hypothesis favored by some solelybased on the preferential involvement of skeletal muscle (2,3, 11, 17–23). Indeed, early studies using immunohis-tochemistry highlighted tumor positivity for myogenic
2M (Lung)
p22.32
–4 –2 +2 +4–1 +10 –4 –2 +2 +4–1 +10 –4 –2 +2 +4–1 +10 –4 –2 +2 +4–1 +10 –4 –2 +2 +4–1 +10 –4 –2 +2 +4–1 +10 –4 –2 +2 +4–1 +10
p22.2p22.12
p21.3
p21.1
p11.3
p11.22
q12q13.2
q21.1
q21.31q21.33q22.2
q23
q25q28.2q27.1q27.3
6M (Pancreas) 7P (Thigh) 7M (Colon) 8M (Brain2) 11P (Back) 13P (Buttock)
Figure 5. Composite analysis of the break at Xp11.23 and subsequent imbalance in three primary and four metastatic tumors. Blue horizontal line representsthe location of the break at TFE3. Aberrations above the ADM-1 threshold of 10.0 are represented by the colored regions deviating to the left (relative loss tocontrol) or right (relative gain to control). Imbalances in the primary and metastatic tumors are color coded as yellow and blue, respectively.
Selvarajah et al.
Clin Cancer Res; 20(6) March 15, 2014 Clinical Cancer Research1528
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

antibodies (including MyoD1, desmin, and sarcomericactin) in ASPS, which supported the hypothesis that ASPSis of muscular origin (19, 22). Moreover, recent geneexpression profiling studies have identified a number ofdifferentially expressed muscle-related transcripts inpatients with ASPS, adding further weight to the case fora muscle cell progenitor as origin of the disease (11, 21).However, many other IHC- and PCR-based studies havefailed to support these findings (2, 20, 23). In this study,several stem cell gene expression signatures and pathwaysrelated to differentiation are enriched among the top dif-ferentially expressed genes. Furthermore, we noted distinctupregulation of the paired box transcription factor PAX6 inprimary sarcomas, along with several genes whose mouseorthologs have previously been implicated in Pax6 DNAbinding during neural stem cell differentiation (Figs. 3and 4). PAX6 has important functions in the developmentof the eye, nose, pancreas, and central nervous system.Interestingly, PAX6 is necessary and sufficient for humanneuroectoderm specification through repression of plurip-otent genes and activation of neural genes (24). Further-more, one of the PAX6 targets, the LIM/homeobox proteinLhx6, is an important transcription regulator that is knownto control the differentiation and development of neuralcells (8). Indeed, PAX6 as a putative tumor suppressor mayhave a role in the pathogenesis of many cancers (includingbreast, oral, lung, gastric, bladder, and brain) throughpromoter hypermethylation or through the sonic hedge-hog–GLI signaling pathway (25–31). It is noteworthy,however, that many of the translocation-associated sarco-mas use abberant transcription factors in their pathogene-sis, and tend to be difficult to classify in terms of their cell oforigin, even when dominant patterns are found in terms oflines of differentiation. The signature reported herein, how-ever, does bear a strong resemblance to the molecularmechanism observed in neural stem cells.
In conclusion, our findings seem to indicate that, inaddition to suggesting a tentative neural line of differenti-ation for ASPS, transcriptional deregulation from fusiongenes may have a critical role in the pathogenesis of ASPS,rather than extensive chromosomal instability.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: S. Selvarajah, E. Chen, M. Loda, R. FlavinDevelopment of methodology: S. Selvarajah, E. Chen, M. Loda, R. FlavinAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): S. Selvarajah, E. Chen, A.H. Ligon, G. Dranoff,E. Stack, M. Loda, R. FlavinAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): S. Selvarajah, S. Pyne, E. Chen, A.H.Ligon, G. Dranoff, M. Loda, R. FlavinWriting, review, and/or revisionof themanuscript: S. Selvarajah, S. Pyne,E. Chen, A.H. Ligon, G.P. Nielsen, G. Dranoff, E. Stack, M. Loda, R. FlavinAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): S. Selvarajah, E. Chen, R. Sompal-lae, E. StackStudy supervision: S. Selvarajah, R. Flavin
AcknowledgmentsThe authors thank Dr. Ewa T. Sicinska of Dana-Farber Cancer Institute
(Boston, MA) for her help in sample procurement.
Grant SupportFunding for this work was obtained from iCureASPS and a gift from
Nuclea Biomarkers to the Jimmy Fund and the Loda laboratory. This workwas also supported in part by the National Cancer Institute (RO1CA131945,PO1CA89021, and P50 CA90381) to M. Loda.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received July 29, 2013; revised December 3, 2013; accepted December 23,2013; published OnlineFirst February 3, 2014.
References1. Folpe AL, Deyrup AT. Alveolar soft-part sarcoma: a review and update.
J Clin Pathol 2006;59:1127–32.2. Gomez JA, Amin MB, Ro JY, Linden MD, Lee MW, Zarbo RJ. Immu-
nohistochemical profile of myogenin and MyoD1 does not supportskeletal muscle lineage in alveolar soft part sarcoma. Arch Pathol LabMed 1999;123:503–7.
3. Guillou L, Lamoureux E, Masse S, Costa J. Alveolar soft-part sarcomaof the uterine corpus: histological, immunocytochemical and ultra-structural study of a case. Virchows Arch A Pathol Anat Histopathol1991;418:467–71.
4. Evans HL. Alveolar soft-part sarcoma. A study of 13 typical examplesand one with a histologically atypical component. Cancer 1985;55:912–7.
5. Ladanyi M, LuiMY, Antonescu CR, Krause-BoehmA,Meindl A, ArganiP, et al. The der(17)t(X;17)(p11;q25) of human alveolar soft part sar-coma fuses theTFE3 transcription factor gene toASPL, anovel gene at17q25. Oncogene 2001;20:48–57.
6. Argani P, Antonescu CR, Illei PB, Lui MY, Timmons CF, Newbury R,et al. Primary renal neoplasms with the ASPL-TFE3 gene fusion ofalveolar soft part sarcoma: a distinctive tumor entity previously includ-ed among renal cell carcinomas of children and adolescents. Am JPathol 2001;159:179–92.
7. Fletcher CDM, Unni K, Mertens F. Pathology and genetics of tumoursof soft tissue and bone. World Health Organization classification oftumours. Lyon, France: IARC Press; 2002.
8. Flandin P, Zhao Y, Vogt D, Jeong J, Long J, Potter G, et al. Lhx6and Lhx8 coordinately induce neuronal expression of Shh thatcontrols the generation of interneuron progenitors. Neuron2011;70:939–50.
9. De Witte A, Lea-Chou E, Collins J. Copy number analysis of archivalFFPE tumor samples by Oligo Array CGH. Application note. SantaClara, CA: Agilent Technologies.
10. Lazar AJ, Das P, Tuvin D, Korchin B, Zhu Q, Jin Z, et al. Angiogenesis-promoting genepatterns in alveolar soft part sarcoma.ClinCancer Res2007;13:7314–21.
11. Stockwin LH, Vistica DT, Kenney S, Schrump DS, Butcher DO, RaffeldM, et al. Gene expression profiling of alveolar soft-part sarcoma(ASPS). BMC Cancer 2009;9:22.
12. KobosR, NagaiM, TsudaM,MerlMY, Saito T, La�eM , et al. Combiningintegrated genomics and functional genomics to dissect the biology ofa cancer-associated, berrant transcription factor, the ASPSCR1-TFE3fusion oncoprotein. J Pathol 2013;229:743–54.
13. Semenza GL. Targeting HIF-1 for cancer therapy. Nat Rev Cancer2003;3:721–32.
Molecular Profiling of Alveolar Soft Part Sarcoma
www.aacrjournals.org Clin Cancer Res; 20(6) March 15, 2014 1529
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

14. Kiuru-Kuhlefelt S, El-Rifai W, Sarlomo-Rikala M, Knuutila S, MiettinenM. DNA copy number changes in alveolar soft part sarcoma: acomparative genomic hybridization study. Mod Pathol 1998;11:227–31.
15. Craver RD, Heinrich SD, Correa H, Kao YS. Trisomy 8 in alveolar softpart sarcoma. Cancer Genet Cytogenet 1995;81:94–6.
16. Aulmann S, Longerich T, Schirmacher P, Mechtersheimer G, Penzel R.Detection of the ASPSCR1-TFE3 gene fusion in paraffin-embeddedalveolar soft part sarcomas. Histopathology 2007;50:881–6.
17. Cullinane C, Thorner PS, Greenberg ML, Kwan Y, Kumar M, Squire J.Molecular genetic, cytogenetic, and immunohistochemical character-ization of alveolar soft-part sarcoma. Implications for cell of origin.Cancer 1992;70:2444–50.
18. Foschini MP, Eusebi V. Alveolar soft-part sarcoma: a new type ofrhabdomyosarcoma? Semin Diagn Pathol 1994;11:58–68.
19. Hirose T, Kudo E, Hasegawa T, Abe J, Hizawa K. Cytoskeletal prop-erties of alveolar soft part sarcoma. Hum Pathol 1990;21:204–11.
20. Hoshino M, Ogose A, Kawashima H, Izumi T, Hotta T, Hatano H, et al.Molecular analyses of cell origin and detection of circulating tumorcells in the peripheral blood in alveolar soft part sarcoma. CancerGenet Cytogenet 2009;190:75–80.
21. Nakano H, Tateishi A, Imamura T, Miki H, Ohno T, Moue T, et al. RT-PCR suggests human skeletal muscle origin of alveolar soft-partsarcoma. Oncology 2000;58:319–23.
22. Rosai J, Dias P, Parham DM, Shapiro DN, Houghton P. MyoD1protein expression in alveolar soft part sarcoma as confirmatoryevidence of its skeletal muscle nature. Am J Surg Pathol 1991;15:974–81.
23. Wang NP, Bacchi CE, Jiang JJ, McNutt MA, Gown AM. Does alveolarsoft-part sarcoma exhibit skeletal muscle differentiation? An immu-nocytochemical andbiochemical studyofmyogenic regulatory proteinexpression. Mod Pathol 1996;9:496–506.
24. Zhang X, Huang CT, Chen J, Pankratz MT, Xi J, Li J, et al. Pax6 is ahuman neuroectoderm cell fate determinant. Cell Stem Cell 2010;7:90–100.
25. Agundez M, Grau L, Palou J, Algaba F, Villavicencio H, Sanchez-CarbayoM. Evaluation of themethylation status of tumour suppressorgenes for predicting bacillus Calmette-Guerin response in patientswith T1G3 high-risk bladder tumours. Eur Urol 2011;60:131–40.
26. Gasche JA, Hoffmann J, Boland CR, Goel A. Interleukin-6 promotestumorigenesis by altering DNA methylation in oral cancer cells. Int JCancer 2011;129:1053–63.
27. Lian ZQ, Wang Q, Li WP, Zhang AQ, Wu L. Screening of significantlyhypermethylated genes in breast cancer using microarray-basedmethylated-CpG island recovery assay and identification of theirexpression levels. Int J Oncol 2012;41:629–38.
28. Moelans CB, Verschuur-Maes AH, van Diest PJ. Frequent promoterhypermethylation of BRCA2, CDH13, MSH6, PAX5, PAX6 and WT1 inductal carcinoma in situ and invasive breast cancer. J Pathol2011;225:222–31.
29. Pesek M, Kopeckova M, Benesova L, Meszarosova A, Mukensnabl P,Bruha F, et al. Clinical significance of hypermethylation status inNSCLC: evaluation of a 30-gene panel in patients with advanceddisease. Anticancer Res 2011;31:4647–52.
30. Yao D, Shi J, Shi B, Wang N, Liu W, Zhang G, et al. Quantitativeassessment of gene methylation and their impact on clinical outcomein gastric cancer. Clin Chim Acta 2012;413:787–94.
31. Zong X, Yang H, Yu Y, Zou D, Ling Z, He X, et al. Possible role of Pax-6in promoting breast cancer cell proliferation and tumorigenesis. BMBRep 2011;44:595–600.
32. Sansom SN, Griffiths DS, Faedo A, Kleinjan DJ, Ruan Y, Smith J, et al.The level of the transcription factor Pax6 is essential for controlling thebalance between neural stem cell self-renewal and neurogenesis.PLoS Genet 2009;(6):e1000511.
Selvarajah et al.
Clin Cancer Res; 20(6) March 15, 2014 Clinical Cancer Research1530
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090

2014;20:1521-1530. Published OnlineFirst February 3, 2014.Clin Cancer Res Shamini Selvarajah, Saumyadipta Pyne, Eleanor Chen, et al. Alveolar Soft Part SarcomaHigh-Resolution Array CGH and Gene Expression Profiling of
Updated version
10.1158/1078-0432.CCR-13-2090doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/02/04/1078-0432.CCR-13-2090.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/6/1521.full#ref-list-1
This article cites 30 articles, 3 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/6/1521.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/6/1521To request permission to re-use all or part of this article, use this link
on July 14, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 3, 2014; DOI: 10.1158/1078-0432.CCR-13-2090