Síndroma X cardíaca

of 11
-
Upload
alexandre-cardoso -
Category
Documents
-
view
215 -
download
0
Transcript of Síndroma X cardíaca
-
8/8/2019 Sndroma X cardaca
1/11
Recebido para publicao: Outubro de 2008 Aceite para publicao: Junho de 2009 Received for publication: October 2008 Accepted for publication: June 2009
193
????????????????
Sndroma X cardaca,gradientes intraventriculares
e bloqueadores beta adrenrgicos [15]CARLOS COTRIM*,***; A NA G ALMEIDA**,***; M ANUEL CARRAGETA*,***.
*Servio de Cardiologia, do Hospital Garcia de Orta, Almada, Portugal**Servio de Cardiologia do Hospital de Santa Maria, Lisboa, Portugal
*** Faculdade de Medicina de Lisboa, Lisboa, Portugal
Rev Port Cardiol 2010; 29 (02): 193-203
RESUMO
Introduo : O desenvolvimento de gradi-entes intraventriculares (GIV) durante o
esforo ocorre raramente numa populaono seleccionada. Num jovem de 23 anos,atleta, com prova de esforo positiva, com
ecocardiograma transtorcico (ETT) normale coronrias angiograficamente normais
(sndroma X) efectumos ecocardiograma deesforo (EE) e detectmos GIV de 102
mmHg e movimento sistlico anterior davlvula mitral (SAM). Posteriormente
estudmos 91 doentes (dts), 44 mulheres,com 51,4 12,1 anos (20 a 75), com provasde esforo positivas para isqumia que pos-teriormente efectuaram cateterismo que re-
velou coronrias angiograficamente normais.Em 33 (36%) dts detectmos gradienteintraventricular com pico telesistlico -
86 34 mmHg (30 a 165) acompanhadopor SAM em 23 dts. Os 20 doentes aos
quais foi possvel repetir EE sob teraputicacom bloqueadores beta adenrgicos
constituem a populao do presente estudo.Destes 7 (33%), so mulheres com
50,7 13,4 anos (23 a 72).Objectivo: O objectivo do presente estudo
foi avaliar o efeito dos bloqueadoresbeta adrenrgicos na ocorrncia de GIV e
SAM da vlvula mitral em doentes comsndroma X cardaca.
ABSTRACT
Cardiac syndrome X, intraventriculargradients and blockers
Introduction: Development of intraventricu-lar gradients (IVG) on exertion seldomoccurs in an unselected population. Weperformed exercise stress echocardiography(SE) in a 23-year-old athlete with a positive
treadmill ECG and normal resting echocar-diogram, but without angiographicallydemonstrable coronary disease (cardiacsyndrome X), during which he developed anIVG of 102 mmHg and systolic anterior motion (SAM) of the mitral valve.Subsequently, we performed SE in 91patients, 44 of whom were women, meanage 51.412.1 years (20-72), under similar circumstances positive treadmill testingand no angiographically demonstrable
coronary disease. In 33 (36%) of these,SE disclosed IVG with a mean end-systolicpeak of 8634 mmHg (30-165), together with mitral valve SAM in 23. The 20patients who repeated SE under -blocker therapy constitute the study population.Seven (35%) of them were women, meanage 50.713.4 years (23 to 72).Objective: To assess the effect of -blockerson the occurrence of IVG and mitral valveSAM in patients with cardiac syndrome X.
Methods: We repeated SE in 20 of the 33
FEV 201007-AO-96
-
8/8/2019 Sndroma X cardaca
2/11
Recebido para publicao: ????????????? Aceite para publicao: ????????? Received for publication: ????????????? Accepted for publication: ?????????
194
Populao e mtodos : Repetimos EE em 20dos 33 doentes doentes que desenvolveram
GIV sob teraputica com bloqueador betaadrenrgico. O EE foi efectuado com avali-ao ecogrfica bidimensional e Doppler
pulsado, contnuo e codificado em cor antes, durante e depois do esforo.
Resultados: O GIV nos 20 dts estudados foi97 31 mmHg no 1 EE. No EE efectuado
sob teraputica com bloqueador betaadrenrgico verificou-se que no surgiu
GIV em 11 dts e que nos restantes 9 estediminuiu significativamente: 46 13
mmHg. A frequncia cardaca atingida no1 EE foi 161 17 e no EE com blo-
queador beta adrenrgico foi 143 12(p
-
8/8/2019 Sndroma X cardaca
3/11
ficamente normais detectmos, de modo ines-perado, um gradiente intraventricular de 102mmHg e movimento sistlico anterior davlvula mitral que no estava presente emrepouso (4). Um caso semelhante tinha sidopublicado previamente por Lau et al. (5) numdoente com angina, prova de esforo positivae coronrias angiograficamente normais. Estesautores demonstraram tambm a eficcia tera-putica dos bloqueadores no tratamentodeste doente.
OBJECTIVO
O objectivo do presente estudo foi avaliar o efeito dos bloqueadores na ocorrnciade GIV e SAM da vlvula mitral em doentescom angina, prova de esforo positiva paraisqumia e coronrias angiograficamentenormais.
POPULAO E MTODOS
PopulaoEstudmos previamente 91 doentes (dts),
44 mulheres, com 51,4 12,1 anos (20 a75), com provas de esforo positivas paraisqumia que posteriormente efectuaramcateterismo que revelou coronrias angio-graficamente normais. Em 33 (36%) dtsdetectmos gradiente intraventricular compico telesistlico - 86 34 mmHg (30 a 165) acompanhado por SAM em 23 dts (6). Os 20doentes aos quais foi possvel repetir EE sobteraputica com bloqueadores b constituema populao do presente estudo. Foramcritrios de excluso a presena de diabetesmellitus , hipertrofia ventricular esquerda,prolapso da vlvula mitral ou outra patologiavalvular e hipertenso arterial no contro-lada h pelo menos um ano. No momento darealizao do EE2 todos os doentes estavammedicados com bloqueadores beta adrenr-gicos mantendo-se inalterada a restanteteraputica. Os bloqueadores beta adrenr-
IVG of 102 mmHg and systolic anterior move-ment (SAM) of the mitral valve that was notpresent at rest (4). A similar case was reportedby Lau et al. (5) in a patient with angina, posi-tive exercise treadmill test and angiographi-cally normal coronary arteries. These authorsalso demonstrated the therapeutic efficacy of -blocker therapy in this patient.
OBJECTIVE
The aim of the present study was toassess the effect of -blockers on the occur-rence of IVG and mitral valve SAM inpatients with angina, positive exercise testfor ischemia and angiographically normalcoronary arteries.
METHODS
PopulationWe studied 91 patients, of whom 44 were
women, mean age 51.4 12.1 years (20-75),with positive treadmill testing for ischemiaand no angiographically demonstrable coro-nary disease. IVG were detected in 33(36%) of these patients, with a mean end-systolic peak of 86 34 mmHg (30-165),together with mitral valve SAM in 23 (6). The20 patients who repeated SE under -block-er therapy constitute the present study pop-ulation. Exclusion criteria were the pres-ence of diabetes, left ventricular (LV) hyper-trophy, mitral valve prolapse or other valvu-lar disease, and uncontrolled hypertensionfor at least a year. At the time of the secondSE assessment all patients were medicatedwith -blockers, other therapy remainingunchanged. In all cases, -blockers were takenat breakfast on the morning of the exam, andhad been prescribed by the patients gener-al practitioners: bisoprolol in nine, atenololin eight, metoprolol in two, and propranololin one. All patients gave their informed con-sent to participation in the study. 195
Carlos Cotrim, et alRev Port Cardiol 2010; 29: 193-203FEV 2010
07-AO-96
-
8/8/2019 Sndroma X cardaca
4/11
gicos foram sempre tomados ao pequeno al-moo da manh da realizao do EE, sendoprescritos pelos respectivos mdicos assis-tentes e eram: bisoprolol em 9 doentes, ate-nolol em 8 doentes, metoprolol em 2 doentese pro-pranolol em outro doente. Todos osdoentes deram consentimento informadopara a participao no estudo.
Ecocardiografia de esforoFoi efectuada uma avaliao ecocardio-
grfica completa que incluiu a medio dotrato de sada do ventrculo esquerdo e cl-culo do respectivo ndice (ITSVE), ndice demassa ventricular esquerda (IMVE), espes-sura relativa de parede (ERP), ndice devolume telediastlico do ventrculo esquerdo(IVOLTDVE). Foi tambm avaliada, comDoppler contnuo alinhado no tracto desada do ventrculo esquerdo no plano api-cal cinco cmaras, a velocidade mxima dofluxo para clculo do gradiente intraven-tricular. Os doentes efectuaram um primeiroecocardiograma de esforo sem bloqueado-res (EE1). Posteriormente os doentes fo-ram medicados com bloqueadores eefectuaram novamente ecocardiograma deesforo sob teraputica boqueadora (EE2)no decorrer do ano que se seguiu ao EE1. Aecocardiografia de esforo de acordo com ametodologia utilizada pelos autores (7) inclui aavaliao da contractilidade durante oesforo em tapete rolante, mas tambm aavaliao dos fluxos com Doppler pulsado econtnuo para deteco de GIV e Doppler codificado em cor. A motilidade da vlvulamitral tambm avaliada tendo em atenoparticularmente a ocorrncia de movimentosistlico anterior da vlvula mitral (SAM).Os estudos foram totalmente gravados emvdeo e parcialmente em disco ptico.Considerou-se gradiente intraventricular significativo o aumento de velocidade paramais de 2,5 m/s no final da sstole (picotelesistlico) tal como utilizado por outrosautores (8,9,10) . Os parmetros ecocardiogrfi-cos apresentados so a mdia de trs me-
Exercise stress echocardiographyA complete echocardiographic assess-
ment was performed, including measure-ment of the LV outflow tract and calcula-tion of the index, LV mass index, relativewall thickness, and LV end-diastolic vol-ume. Maximum flow velocity was alsoassessed by continuous wave Doppler inthe LV outflow tract in five-chamber apicalview to calculate the intraventricular gra-dient. The patients had previously under-gone exercise stress echocardiographywithout -blockers, and subsequentlyrepeated the exam under -blocker thera-py during the following year. The method-ology used (7) includes assessment of wallmotion during treadmill exercise, as wellas of flows by pulsed and continuous waveDoppler for detection of IVG and color Doppler. Mitral valve motion is alsoassessed, particularly for SAM. The examswere recorded on video in their entirety,with parts recorded on optical disk. A sig-nificant IVG was defined as an increase inflow velocity to more than 2.5 m/s at theend of systole (end-systolic peak), as usedby other authors (8-10). The echocardiograph-ic parameters presented are the mean of three measurements obtained on consecu-tive good-quality recordings.
Ergometric parametersThe following parameters were assessed
during SE: test duration (in seconds), sys-tolic blood pressure at rest and at peak exer-cise, heart rate at rest and at peak exercise,peak double product, and occurrence of ST-segment alterations ST depression of 1mm 80 ms after the J point. Occurrence of symptoms such as angina during the testsimilar to those that prompted the patientsoriginal assessment was also recorded.
Statistical analysisThe results are presented as means
standard deviation for continuous variables,and frequencies and percentages for cate-196
Rev Port CardiolVol. 29 Fevereiro 10 / February 10FEV 2010
07-AO-96
-
8/8/2019 Sndroma X cardaca
5/11
dies de registos consecutivos de boa qua-lidade.
Parmetros ergomtricosRelativamente s provas de esforo foram
avaliados os seguintes parmetros: Duraoda prova em segundos (DurPE), tensoarterial sistlica em repouso (TASr) e nopico (TASp) de esforo, frequncia cardacaem repouso (FCr) e frequncia cardaca nopico (FCp), o duplo produto no Pico(DPPico) e a ocorrncia de alteraes de ST-infradesnivelamento de ST maior ou igual a1mm 80 ms depois do ponto J altST. Foiainda avaliada a ocorrncia de sintomasdurante a prova semelhantes (angor) aos queoriginaram a avaliao clnica dos doentes(reproduo dos sintomas REPsint)
Anlise estatisticaOs resultados so apresentados como
media DP para as variveis contnuas, epercentagem de frequncia para as variveiscategricas. As variveis foram comparadasentre os dois momentos de avaliao sendoutilizado o test T de student para as variveiscontnuas e o teste McNemar paracomparao de amostras emparelhadas paradados qualitativos nominais.
RESULTADOS
Foram includos no estudo vinte doentes.Destes, 7 (33%) so mulheres com 50,7 13,4 anos (23 a 72). Seis doentes (30%) sofumadores, 8 doentes (40%) tinham hiperco-lesterolmia, 8 doentes (40%) estavam medi-cados com nitratos, 3 doentes (15%) estavammedicados com antagonistas de clcio, 5 doen-tes estavam medicados com bloqueadores (que foram suspensos dois dias antes darealizao do 1 ecocardiograma de esforo),3 doentes (15%) com antagonistas dos recepto-res da angiotensina II ou dos inibidores doIECA e dois doentes (10%) com diurticos.
Relativamente aos parmetros avaliados
gorical variables, comparison between thetwo assessments being performed using theStudents t test for continuous variables andthe McNemar test for paired samples for nominal qualitative data.
RESULTS
Of the 20 patients enrolled in the study,seven (33%) were women, mean age50.7 13.4 years (23-72). Six (30%) weresmokers, eight (40%) had hypercholes-terolemia, eight (40%) were taking nitrates,three (15%) calcium channel blockers, five(25%) -blockers (which were suspendedtwo days before the first SE), three (15%)angiotensin receptor blockers or angiotensin-converting enzyme inhibitors, and two(10%) diuretics.
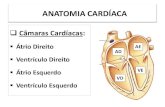
On the resting echocardiogram at thefirst assessment, LV outflow tract indexwas 10.30.8 mm/m 2, LV mass index was7512.5 g/m 2, relative wall thickness was0.370.07, and LV end-diastolic volumewas 429.5 ml/m 2. No wall motion abnor-malities were detected in any of the exams,with or without -blockers. IVG at peakexercise on the first assessment was 97 31mmHg. Fifteen patients (75%) showedimprovement in symptoms, with fewer episodes of angina and an increased levelof exercise required to trigger symptoms.The main results of the variables studiedare shown in Table I and Figure 1.
STUDY LIMITATIONS
The main limitations of the study are: 1)the small sample size; 2) the fact that bothpatients and investigators were aware of thetherapy in progress and that all tests under therapy were performed at the secondassessment, which may have influenced theresults, particularly treadmill test durationand how the patients rated their symptoms. 197
Carlos Cotrim, et alRev Port Cardiol 2010; 29: 193-203FEV 2010
07-AO-96
-
8/8/2019 Sndroma X cardaca
6/11
no ecocardiograma em repouso na data doprimeiro exame, o ITSVE foi 10,3 0,8mm/m2, o IMVE foi 75 12,5 g/m 2 , a ERPfoi 0,37 0,07, o IVOLTDVE foi 42 9,5ml/m2. No detectmos alteraes dacontractilidade segmentar em nenhum dosEE efectuados com e sem bloqueadores. OGIV no pico de esforo do EE1 foi 97 31mmHg. Quinze doentes (75%) tiverammelhoria dos seus sintomas anginosos comdiminuio do nmero de episdios deangor e aumento do nvel de esforo neces-srio para a sua ocorrncia. Os resultadosrelevantes das variveis estudadas soapresentados no Quadro I e na Figura 1.
However, this would not influence objectiveparameters such as the presence andseverity of IVG, or heart rate and bloodpressure; 3) -blocker therapy variedaccording to how it was prescribed by the
patients general practitioners; 4) it wouldalso have been interesting to compare theclinical (angina and exercise tolerance)and echocardiographic response of cardiacsyndrome X patients with IVG who are notunder -blocker therapy with that of thepresent study population, but this was notpossible due to the small number of patients who met the criteria.
198
Rev Port CardiolVol. 29 Fevereiro 10 / February 10FEV 2010
07-AO-96
Quadro I. Variveis avaliadas nos dois ecocardiogramas de esforo
Dur PE durao da prova de esforo; FCr frequncia cardaca em repouso; FCp frequncia cardaca no pico de esforo; TASr tenso arterial sistlica em repouso; TASp tenso arterial sistlica no pico de esforo; DPPico duplo produto no pico de esforo; REPsint reproduo dos sintomas durante o EE; GIV Pico gradiente intraventricular nopico de esforo; SAM movimento sistlico anterior da vlvula mitral; altST alteraes do segmento ST
EE1 EE2 p
Dur PE seg. 636 172 669 179 0,039
FCr 73 11 62 5 < 0,000
FCp 161 17 143 12 < 0,000
TASr mmHg 136 14 121 12 0,0001
TASp mmHg 175 22 154 17 < 0,000
DPPico 28424 5071 22101 3744 < 0,000
REPsint 14/20 (70%) 4/20(20%) 0,006
GIV Pico 20/20 (100%) 9/20 (45%) 0,001
SAM 16/20 (80%) 5/20 (25%) 0,001
altST 20/20 (100%) 6/20(30%) 0,000
Table I. Variables assessed in the two stress echocardiograms
DP: double product; HR: heart rate; IVG: intraventricular gradient; SAM: mitral valve systolic anterior motion; SBP: systolic blood pressure; SE: stress echocardiography
EE1 EE2 p
Test duration (sec) 636172 669179 0.039
Resting HR (bpm) 7311 625 < 0.000
Peak exercise HR (bpm) 16117 14312 < 0.000
Resting SBP (mmHg) 13614 12112 0.0001
Peak exercise SBP (mmHg) 17522 15417 < 0.000
Peak exercise DP 284245071 221013744 < 0.000
Symptoms during SE (n) 14/20 (70%) 4/20 (20%) 0.006
Peak IVG (n) 20/20 (100%) 9/20 (45%) 0.001
SAM (n) 16/20 (80%) 5/20 (25%) 0.001
ST-segment alterations (n) 20/20 (100%) 6/20 (30%) 0.000
-
8/8/2019 Sndroma X cardaca
7/11
Limitaes do estudoComo principais limitaes do estudo
salientamos: 1 - A pequena dimenso daamostra estudada. 2 - O facto de os doentese investigadores terem conhecimento dateraputica em curso e de todas as provassob teraputica terem sido efectuadas emsegundo lugar. Este facto pode ter influen-ciado os resultados nomeadamente a du-rao das provas de esforo e a valorizao
DISCUSSION AND CONCLUSIONS
Patients with angina, positive exercisetest and normal coronary arteries have longconstituted an important clinical problem (11-13),the clinical entity characterized by theseinitial studies now being known as cardiacsyndrome X (14).
Intraventricular gradients in a patientwith this syndrome were first described by 199
Carlos Cotrim, et alRev Port Cardiol 2010; 29: 193-203FEV 2010
07-AO-96
Figura 1. GIV detectado no pico de esforo sem e com teraputica com bloqueadores beta adrenrgicos.
Figure 1. IVG at peak exercise without and with -blockers. BBs: -blockers
IVG without BBs IVG with BBs
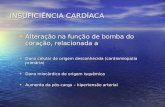
Figura 2. Caso ilustrativo de uma doente estudada antes (esquerda) e aps (direita) a teraputica com bloqueador beta adrenrgico.
Figure 2. Female patient assessed before (left) and after (right) -blocker therapy
-
8/8/2019 Sndroma X cardaca
8/11
que o doente faz dos seus sintomas. Salien-tamos, no entanto, que parmetros objecti-vos como presena e o valor do GIV ou afrequncia cardaca e a presso arterial noso influenciados por este facto. 3 - Ateraputica com bloqueadores era hetero-gnea o que se deve ao facto de ser pres-crita livremente pelos mdicos assistentesrespectivos. 4 - Seria interessante tambmsaber a resposta clnica (angina e tolernciaao esforo) e ecocardiogrfica, de doentescom sndroma X com GIV que no fizerambloquedores beta adrenrgicos e comparar estes resultados com os doentes do presenteestudo no entanto tal no foi possvelatendendo ao diminuto nmero de doentesque satisfizeram estas condies.
Discusso e conclusesOs doentes com angina, prova de esforo
positiva e coronrias normais constituem umproblema com grande relevncia clnicadesde h longa data (11,12,13) . Estes primeirosestudos caracterizaram a entidade clnica aque hoje denominamos sndroma X cardaco (14).
A ocorrncia de gradiente intraventri-cular num doente com a sndroma Xcardaca foi descrita pela primeira vez por Lau (5) que no s detectou o fenmeno numdoente com angina de esforo como utilizoubisoprolol no seu tratamento conseguindomelhoria clnica e demonstrando uma signi-ficativa diminuio do gradiente intraventri-cular. Posteriormente tambm ns demons-trmos a presena de GIV em doentes comangina e coronrias angiograficamentenormais (4,15) o que conduziu ao estudo de 91doentes com a sndroma X (6) dos quaisviramos a seleccionar os 20 do presenteestudo. Recentemente Bueno (16) demonstrou,num pequeno nmero de doentes, apresena de gradientes intraventricularesem doentes com Sndroma X embora algunsdoentes tivessem hipertenso arterial ehipertrofia ventricular esquerda que, por definio de Sndroma X, foram excludosno presente estudo.
Lau et al. (5), who detected the phenomenonin a patient with effort angina and treated itwith bisoprolol, resulting in clinicalimprovement and a significant reduction inthe IVG. Subsequently, we also demonstrat-ed the presence of IVG in patients withangina and angiographically normal coro-nary arteries (4, 15), which led to a study of 91syndrome X patients (6), from among whomwe selected the 20 patients of the presentstudy. Bueno et al. (16), in a small number of patients, demonstrated the presence of IVGin syndrome X patients, although some hadhypertension and left ventricular hypertro-phy, conditions which would have excludedthem from the present study, based on thedefinition of the syndrome.
-blockers are used to treat patients withangina and angiographically normal coro-nary arteries not only because of their anti-ischemic and antianginal properties, butalso because of their effect on heart rate.They are particularly efficacious in control-ling chest pain in patients with increasedsympathetic activity, as well as in those withno alterations in cardiac autonomic control.One study (17) has shown that acebutulolimproves exercise tolerance in syndrome Xpatients who show signs of increased sympa-thetic activity during exercise, and other investigators have reported similar results inpatients with inverted T waves on the ECGand signs of adrenergic hyperreactivity (18).Chronic -blocker therapy has been shownto improve exercise tolerance and left ven-tricular filling dynamics (19), while another study found a good correlation between con-trol of anginal symptoms and normalizationof sympathetic hyperactivity in patients withangina (20). In general, -blockers should befirst-line pharmacological treatment (21, 22) inthese patients, particularly when there isevidence of increased sympathetic tone,such as high heart rate or diminished HRvariability on 24-hour Holter monitoring, or a rapid increase in heart rate or blood pres-sure during exercise testing (23).200
Rev Port CardiolVol. 29 Fevereiro 10 / February 10FEV 2010
07-AO-96
-
8/8/2019 Sndroma X cardaca
9/11
Os bloqueadores tm sido utilizados nateraputica de doentes com angina e coro-nrias angiograficamente normais no sdevido ao seu efeito anti isqumico eantianginoso, mas tambm devido ao seuefeito sobre a frequncia cardaca. Osbloqueadores so particularmente eficazesno controlo da dor torcica em doentes comaumento da actividade simptica, noentanto tambm so eficazes em doentessem alteraes do controlo autonmicocardaco. Num estudo foi demonstrado que oacebutulol (17) melhora a tolerncia ao esforoem doentes com a sndroma X que tmsinais de aumento da actividade simpticadurante o esforo, tendo outros investiga-dores encontrado resultados semelhantesem doentes com ondas T invertidas noelectrocardiograma (18) e sinais de hiperacti-vidade adrenrgica. Foi demonstrado que ateraputica crnica com bloqueadores melhora a tolerncia ao esforo e o padrode enchimento do ventrculo esquerdo (19),tendo outro estudo verificado existir umaboa correlao entre o controlo da angina ea normalizao da hiperactividade simp-tica em doentes com angina (20). De um modogeral, os bloqueadores devem fazer parteda primeira linha na teraputica farmacol-gica (21,22) destes doentes sobretudo quandoexiste evidncia de um aumento do tnussimptico, como frequncia cardaca alta oudiminuio da variabilidade no Holter de 24horas ou um aumento muito rpido dafrequncia cardaca e da presso arterialdurante a prova de esforo (23).
A abordagem teraputica da sndroma X ainda actualmente um desafio para omdico e para o doente, o que compreens-vel se tivermos em conta a diversidade demecanismos que parecem estar envolvidosna sua fisiopatologia. A abordagem maisfrequente de informar o doente de que notem doena cardaca significativa tem sidoquestionada (24), sobretudo se tivermos emateno o facto de alguns subgrupos dedoentes com sndromes coronrias agudas
Management of syndrome X remains achallenge for the physician and the patient,which is understandable given the variety of mechanisms that appear to be involved in itspathophysiology. The usual approach of telling patients that they have no significantheart disease has been called into question (24),particularly in view of the fact that certainsubgroups of patients with cardiac syndromeX have significant event rates, and patientswith complete left bundle branch block alsohave worse prognosis. While the prognosisis good in most other patients (25), quality of life is significantly affected in many.
In our study we found that -blockersreduced heart rate, ST-segment depression,systolic blood pressure and hence peak dou-ble product, during exercise. The occur-rence of IVG and SAM on exertion alsodecreased significantly. These changes wereaccompanied by improvement in anginalsymptoms during follow-up and exercisetesting, as well as in functional capacity.
Improvement in symptoms with -block-er therapy in patients with documented IVGhas been demonstrated (26, 27, 5) ; these studiesalso clearly showed an association betweenreduced IVG and improvement of symptomsand functional capacity. Since -blockersare recommended in the treatment of syn-drome X patients, the results of this studysuggest that exercise stress echocardiogra-phy would help in selecting patients whodevelop IVG on exertion and who wouldrespond particularly well to these drugs.
201
Carlos Cotrim, et alRev Port Cardiol 2010; 29: 193-203FEV 2010
07-AO-96
-
8/8/2019 Sndroma X cardaca
10/11
poderem ter uma taxa de eventos signi-ficativa. Os doentes com bloqueio completode ramo esquerdo tm tambm um pior prognstico e embora o prognstico dosrestantes doentes seja bom (25), a qualidadede vida est seriamente alterada numgrande nmero de doentes.
No nosso estudo verificmos que autilizao dos bloqueadores diminui afrequncia cardaca, o infradesnivelamentode ST, a tenso arterial sistlica e por consequncia o duplo produto mximoatingido durante o esforo. Tambm os GIVe a ocorrncia de SAM durante o esforodiminuem de modo significativo. Estasalteraes so acompanhadas de melhoriado angor durante o seguimento e durante aprova de esforo e tambm de um aumentoda capacidade funcional.
A melhoria dos sintomas conseguida,com o tratamento com bloqueadores , emdoentes em que foi demonstrada a presenade GIV, tinha j sido demonstrada (26,27,5) . Nas
mesmas publicaes foi tambm evidente aassociao entre a diminuio do GIV e amelhoria dos sintomas e da capacidadefuncional. Sendo os bloqueadores , umadas armas teraputicas preconizadas, emdoentes com sndroma X cardaca, osresultados deste estudo sugerem-nos que autilizao da ecocardiografia de esforo,pode permitir seleccionar um subgrupo dedoentes que desenvolvem GIV durante oesforo e que respondem particularmentebem teraputica com estes frmacos.
Pedido de separatas:Address for reprints:
Carlos CotrimHospital Garcia de OrtaAvenida Torrado da Silva2805-267 Almada - [email protected] 00351 916 885 153
202
Rev Port CardiolVol. 29 Fevereiro 10 / February 10FEV 2010
07-AO-96
BIBLIOGRAFIA / REFERENCES
1. Scandura S, Arcidiacono S, Felis S, Barbagallo G, et al.Dynamic obstruction to left ventricular outflow during dobuta-mine stress echocardiography: The probable mechanisms andclinical implications. Cardiologia 1998;43:1201-1208.
2. Pellikka PA, Oh JK, Bailey KR, et al. Dynamic intraventric-ular obstruction during dobutamine stress echocardiography: anew observation. Circulation 1992;86:1429-32.
3. Peteiro J, Monserrat L, Castro Beiras. Labile subaortic
obstruction during exercise stress echocardiography. Am JCardiol 1999 Nov 1;84(9):1119-23,A10-1
4. Cotrim C, Joo I, Fazendas P, et al. Exercise induced ven-tricular gradient in a young patient with positive treadmill testand normal coronary arteries. Rev Port Cardiol 2002;21:331-5.
6. Lau TK, Navarijo J, Stainback RF. Pseudo-False-PositiveExercise Treadmill Testing Caused by Systolic Anterior Motionof the Anterior Mitral Valve Leaflet. Tex Heart Inst J2001;28:308-11.
7. Cotrim C, Almeida AG, Carrageta M. Exercise-inducedintra-ventricular gradients as a frequent potential cause of myocardial ischemia in cardiac syndrome X patients.Cardiovascular Ultrasound 2008;6:3
8. Cotrim C, Carrageta M. Ecocardiografia de sobrecarga Esforo. Rev Port Cardiol 2000;19 (3):345-350.
9. Bueno FC, Bailn IR, Salguero RL, et al. Obstruccindinmica intraventricuar izquierda inducida por esfuerzo. RevEsp Cardiol 2004:57(12):1179-87.
10. Lpez AJ, Evangelista MA, Armada RE, et al. Aparicinde gradiente dinmico intraventricular despus de la sustitu-icin valvular artica en pacientes com estenosis artica sev-
era. Rev Esp Cardiol 2002 ;55 :127-34.
11. Barletta G, del Bene MR, Gallini C, et al. The clinicalimpact of dynamic intraventricular obstruction during dobuta-mine stress echocardiography. Int J Cardiol 1999 ;70 :179-189.
12. Likoff W, Segal BL, Kasparian H. Paradox of normal selec-tive coronary angiograms in patients considered to haveunmistakable coronary heart disease. N Engl J Med1967;276:1063-1066.
13. Kemp HG, Elliot WC, Gorlin R. The anginal syndromewith normal coronary arteriography. Trans Assoc AmPhysicians 1967;80:59-70.
14. Kemp GH. Left ventricular function in patients with the
-
8/8/2019 Sndroma X cardaca
11/11
203
Carlos Cotrim, et alRev Port Cardiol 2010; 29: 193-203FEV 2010
07-AO-96anginal syndrome and normal coronary arteriograms. Am JCardiol 1973;32:375-376.
15. Kaplan MN. Syndromes X : two too many. J Am CollCardiol 1992;69;1643-1644.
16. Cotrim C, Loureiro MJ, Simes O, et al. Intraventricular gradient during effort in a professional soccer player. Clinical
significance. Rev Port Cardiol 2005;24(11):1395-1401.
17. Bueno FC, Doblas JJ, Garcia AM, et al. Effort angina, nor-mal coronary angiogram and dynamic left ventricular obstruc-tion. J Am Soc Echocardiogr 2007;20:415-420.
18. Romeo F, Gaspardone A, Ciavolleta M, et al. Verapamilversus acebutulol for syndrome X. Am J Cardiol 1988;62:312-313.
19. Montorsi F, Fabbiocchi, Loaldi L, et al. Coronary adrener-gic hyperreactivity in patients with syndrome X and abnormalelectrocardiogram at rest. Am J Cardiol 1988;62:312-313.
20. Fragasso G, Chierchia S, Pizzeti G, et al. Impaired left ven-tricular filling dynamics in patients with angina pectoris andangiographically normal coronary arteries: effect of beta-adrenergic blockade. Heart 1997;77:32-39.
21. Leonardo F, Fragasso G, Rosano GC, et al. Effect of atenolol on QT interval and dispersion in patients with syn-drome X. Am J Cardiol 1997;80:789-90.
22. Bugiardini R, Borghi A, Biagetti L, et al. Comparison of verapamil versus propranolol therapy in syndrome X. Am JCardiol. 1989;63:286-290.
23. Lanza GA, Colonna G, Pasceri V, et al. Atenolol versusamlodipine versus isosorbide-5-mononitrate on anginal symp-toms in syndrome X. Am J Cardiol. 1999;84:854-856.
24. Crea F, Lanza GA. Angina pectoris and normal coronaryarteries: cardiac syndrome X. Heart 2004;90;457-463.
25. Bugiardini R, Merz CB. Angina with normal coronaryarteries. A changing philosophy. JAMA 2005;293:477-484.
26. Kaski JC. Pathophysiology and management of patientswith chest pain and normal coronary arteriograms (cardiacsyndrome X). Circulation 2004;109:568-572.
27. Cabrera-Bueno F, Pinilla JMG, Doblas JJG, et al. Beta-blocker therapy for dynamic left ventricular outflow tractobstruction induced by exercise. Int J Cardiol, 2007;25:117(2):222-6.
28. Almeida S, Cotrim C, Brando L, et al. Exercise-inducedleft ventricular outflow tract obstruction. A potential cause of symptoms in the elderly. Rev Port Cardiol 2007;26(3):257-262.