artigoradioterapia1

of 7
-
Upload
gabriela-barboza -
Category
Documents
-
view
224 -
download
0
Transcript of artigoradioterapia1
-
7/30/2019 artigoradioterapia1
1/7
159
DOI: 10.1177/0022034509351251
Received July 17, 2008; Last revision April 15, 2009; AcceptedJuly 23, 2009
C.J. Soares 1*, C.G. Castro 1,N.A. Neiva 1, P.V. Soares 1,P.C.F. Santos-Filho1, L.Z. Naves1,
and P.N.R. Pereira2
1Biomechanics Group, School of Dentistry, FederalUniversity of Uberlndia, Dept. of Operative Dentistry andDental Materials, Av. Par 1720, Bloco 2B, Sala 2B-24,Campus Umuarama, Uberlndia, MG 38400-902, Brazil;and 2Department of Operative Dentistry, University of
North Carolina, Chapel Hill, NC, USA; *correspondingauthor, [email protected]
J Dent Res 89(2):159-164, 2010
ABSTRACTThe effect of gamma irradiation therapy on the ulti-
mate tensile strength (UTS) of enamel and dentin inrelation to prism orientation, dentin tubule orienta-tion, and location is unknown. It was hypothesizedthat tubule and prism orientation, location, and irra-diation have an effect on the UTS of dental struc-tures. Forty human third molars were used, half of which were subjected to 60 Gy of gamma irradiation,in daily increments of 2 Gy. The specimens wereevaluated by microtensile testing. Results showedthat irradiation treatment significantly decreased theUTS of coronal and radicular dentin and of enamel,regardless of tubule or prism orientation. With or without irradiation, enamel was significantly stronger
when tested parallel to its prismatic orientation.Coronal and radicular dentin of non-irradiated speci-mens presented significantly higher UTS when tested
perpendicularly to tubule orientation. However, whenthe teeth were irradiated, the influence of tubuleorientation disappeared, demonstrating that irradia-tion is more harmful to organic components.
KEY WORDS:ultimate tensile strength, irradia-tion, tubule orientation, prism orientation; dentin,enamel.
INTRODUCTION
Individuals diagnosed with head and neck cancer may be treated surgically(Hong et al ., 2001) by radiotherapy (Lyons, 2006; Lazarus et al ., 2007), bychemotherapy (Lyons, 2006; Lazarus et al ., 2007), or by a combination of these treatments. Despite the advantage of preserving tissue structure, radio-therapy causes adverse changes in the oral cavity (Spetch, 2002). Several
studies (Silverman, 1999; Craddock, 2006) have investigated the causesof radiation caries; however, little is known about the structural alterationsoccurring in the dentin and enamel after irradiation (Frnzel et al ., 2006).
Enamel is composed of 1-2% organic material and 3-4% water by weight,and 92-96% of inorganic matter organized in prisms, whose orientation deter-mines enamels anisotropic behavior and influences its mechanical properties(Urabe et al ., 2000; Giannini et al ., 2004). Dentin is a hydrated biologicalcomposite composed of 70% inorganic material, 18% organic matrix, and12% water (wt%), with various properties and structural components, depend-ing on location (Mjr, 1972), which confer directional properties (anisotropy)on the tissue and have profound effects on its tensile strength (Carvalho et al .,2001; Giannini et al ., 2004). It has been observed (Frnzel et al ., 2006) that,after irradiation, the mechanical properties of teeth are altered.
While several studies have measured the ultimate tensile strength (UTS) of root and coronal dentin or of enamel (Lertchirakarn et al ., 2001; Giannini et al .,2004; Miguez et al ., 2004), no systematic study has been carried out analyzing theeffect of gamma irradiation therapy on the UTS of enamel and dentin in relationto prism orientation, dentin tubule orientation, and location. The null hypothesisto be tested in this study is that gamma irradiation therapy has no effect on theUTS of dental tissues, despite tubule or prism orientation and dentin location.
MATERIALS & METHODSForty sound human third molars free of caries, from individuals 18 to 23 yrs old,were collected with informed donor consent. The teeth were obtained under a
protocol (248/05) analyzed and approved by the Ethical Committee of theFederal University of Uberlndia, MG, Brazil. They were stored in a solution of 0.2% thymol for no longer than 1 mo after extraction, then cleaned of grossdebris and placed in distilled water for 24 hrs before the beginning of the exper-iment. The teeth were divided into 2 groups: an irradiated group (Ir) (number of specimens, N = 15) and a non-irradiated group (NIr) (N = 15). The Ir groupreceived 60 Gy of gamma radiation in a 60Cobalt irradiation unit (TheratronPhoenix 60Cobalt Radiotherapy Treatment Unit - Theratronics International, Ltd.,Atomic Energy of Canada, Ltd., AECL Medical, Ottawa, ON, Canada), withexposure to daily increments of 2 Gy, 5 days a wk. The dose was defined on theradiotherapy unit panel that self-measures the radiation level emitted. Bothgroups of samples were stored in distilled water changed daily.
Effect of Gamma Irradiationon Ultimate Tensile Strength ofEnamel and Dentin
RESEARCH REPORTSBiomaterials & Bioengineering
-
7/30/2019 artigoradioterapia1
2/7
160 Soares et al. J Dent Res 89(2) 2010
The intact occlusal enamel surface was etched with 37% phosphoric acid (Dentsply Caulk, Milford, DE, USA) for 30 sec,rinsed, and bonded with Adper Single Bond 2 (3M-ESPE,St. Paul, MN, USA). A resin composite block (5 mm high) was
built up in 3 layers with TPH Spectrum resin composite(Dentsply Caulk), to form an extension of the crown to facilitatefurther slicing and testing (Giannini et al ., 2004). Each incre-ment was light-polymerized for 20 sec, and the specimens werestored in distilled water at 37C for 24 hrs. Roots and crowns
were then serially sectioned vertically in a buccal-lingual direc-tion (Fig. 1) to obtain several slices of approximately 1.0 mmthick by means of a low-speed diamond saw (Isomet, Buehler Ltd., Lake Bluff, IL, USA) under water cooling. Six slices 1.0 0.16 mm in thickness were obtained for each root and crown
portion and were further trimmed to an hourglass shape that produced a cross-sectional testing area of 1.0 0.1 mm 2. Thesamples of each tooth were randomly assigned to one of 6groups (number of slices per group = 20). The slices weretrimmed to an hourglass shape with a superfine diamond bur #1090 (KG Sorensen, Barueri, So Paulo, Brazil) under air-water irrigation, reducing enamel to a parallel positioning of
prisms (Fig. 1A), enamel transverse to the orientation of prisms(Fig. 1B), coronal dentin transverse to the orientation of tubules(Fig. 1C), coronal dentin parallel to the orientation of tubules(Fig. 1D), root dentin parallel to the orientation of tubules (Fig.1E), and coronal dentin transverse to the orientation of tubules(Fig. 1F).
Each specimen was fixed to the grips of a microtensile test-ing device with cyanoacrylate glue (Loctite Super Bonder,Henkel Loctite Corporation, Munich, Germany) and subjectedto tensile testing at 0.5 mm/min in a testing machine (EMIC2000 DL, So Jos dos Pinhais, PR, Brazil) until failure. After fracture, the specimen was removed from the testing apparatus,
and the cross-sectioned area at the site of fracture was measuredwith a digital caliper (S235, Sylvac, Crissier, Switzerland) to thenearest 0.01 mm. Mean tensile strength values were expressedin MPa, and data were analyzed by two-way ANOVA with ten-sile strength as the dependent variable, and radiotherapy andorientation of the dental structure as factors, followed by theTukey test (significance, p < 0.05).
The specimens were allowed to air-dry overnight, sputter-coated with gold (MED 010, Balzers, Balzers, Leichtenstein),and examined by scanning electron microscopy (LEO 435 VP,Carl Zeiss, Jena, Germany). Representative areas of tested siteswere photographed at 2500-3000X magnification.
RESULTSInfluence of Tubule and Prism Orientation andIrradiation on UTS of Enamel and DentinTwo-way ANOVA revealed that there were significant differ-ences between the UTS of the dental structures (p = 0.001) andthe irradiation (p = 0.003), but not for both factors (p = 0.154).The Table shows the means of UTS for all groups.
The direction of the tubules and prisms in the specimenstested, either parallel or perpendicular, was confirmed by low-magnification scanning electron microscopy. The presence of irradiation significantly decreased the UTS of coronal andradicular dentin and of enamel, regardless of tubule or prismorientation. Enamel was significantly stronger when tested par-allel to its prismatic orientation, regardless of the presence of irradiation. Non-irradiated dentin specimens, coronal and radic-ular, presented significantly higher UTS when tested perpen-dicularly to tubule orientation. When the dentin substrate wassubjected to irradiation, tubule orientation had no influence onUTS.
Appearance of Fracture SurfacesThe fractured site of non-irradiated enamel tested transverselyto its prismatic orientation showed a preferential plane of fracture (Fig. 2A), with less oblique fractures of the prisms.The fractured site of non-irradiated enamel tested parallel to its
prismatic orientation (Fig. 2B) presented a cone-shaped struc-tures. Since fracture did not occur in a single plane, these struc-tures appeared to be protruding from the surface. Fracturedirradiated enamel tested transversely to its prismatic orientationshowed predominantly oblique fracture orientation (Fig. 3A),tending to cross to the inter-prismatic region. The fracture of non-irradiated enamel tested transversely to its prismatic orien-tation presented a fractured surface with a melted appearance(Fig. 3A). The surfaces of irradiated samples stressed parallelto prisms showed more irregular surfaces involving greater interprismatic change (Fig. 3B), demonstrating alteration of interprismatic areas.
Non-irradiated crown dentin (Fig. 2C) fractured transverselyto tubules showed regular planes similar to non-irradiated rootdentin (Fig. 2E). In these samples, intertubular dentin wassmooth, showing collagen fibrils oriented transversely to thetubule direction (Figs. 2C, 2E). The plane of fracture passed
Figure 1.Schematic representation of specimen preparation.(A) Enamelparallel to the prism orientation. (B) Enamel stressed perpendicular toenamel prisms. (C) Coronal dentin stressed perpendicular to tubuleorientation. (D) Coronal dentin tested parallel to tubule orientation.(E) Orientation for testing radicular dentin parallel to the long axisof the tubules. (F) Radicular dentin stressed perpendicular to tubuleorientation.
-
7/30/2019 artigoradioterapia1
3/7
J Dent Res 89(2) 2010 Effect of Radiation on Tooth Structures 161
approximately through thecentral axis of tubules andtangentially through others(Figs. 2C, 2E). Crown den-tin fractured parallel totubule orientation (Fig. 2D)
was more irregular thanroot dentin (Fig. 2F), with peritubular dentin protrud-ing from the surface as adistinct structure (Fig. 2D).Samples of irradiatedcrown dentin fracturedtransversely to tubule ori-entation showed the same
plane of fracture, but withgreater micro-cracks pres-ent in peritubular dentin(Figs. 3C, 3E). Irradiateddentin fractured parallel totubule orientation showedmore inhomogeneous frac-ture planes (Figs. 3D, 3F),with great numbers of micro-cracks in peritubular dentin which was less dis-tinctly discerned (Fig. 3D).
DISCUSSIONThe null hypothesis wasrejected, since gammaradiation influenced theUTS of enamel in relationto prism and dentin tubuleorientation. Dentin pre-sented different character-istics after radiotherapytreatment when comparedwith non-irradiated den-tin, while the prism orien-tation maintained the in-fluence on UTS mean values inirradiated ena-mel. While the structured biological hard tis-sues presented anisotropic characteristics, other studies have
found that the UTS of dental structures varied widely accord-ing to intra-tooth location (Staninec et al ., 2002; Gianniniet al ., 2004). It has been observed (Giannini et al ., 2004) that
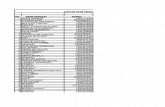
Table. Ultimate Tensile Strength of Human Dentin in Crownvs . Root and Enamel Influenced by Gamma Irradiation
Ultimate Tensile Strength Values (MPa)
Parallel Orientation Perpendicular Orientation
Tooth Structure Non-irradiated Irradiated Non-irradiated Irradiated
Enamel 40.1 12.4 Aa 29.4 7.9 Ba 17.6 5.7 Ab 10.9 3.9 Bb
Crown dentin 54.2 19.5Ab
39.8 13.4Ba
86.5 20.2Aa
51.3 16.9Ba
Root dentin 49.8 13.9 Ab 30.2 12.0 Ba 64.7 14.7 Aa 43.7 15.4 Ba
Values are adjusted means SD. Different superscript letters indicate a statistically significant difference by the Tukey test (p < 0.05). Capital lettersrepresent comparison of irradiation factors for each structural orientation. Lower-case letters represent structural orientation comparison (parallel operpendicular) for each tooth structure in the same irradiation pattern (non-irradiated or irradiated). Number of slices = 20 for all groups.
Figure 2.Fracture pattern in sites of non-irradiated samples of stressed perpendicular enamel(A). Enamel testedparallel to prism orientation(B). Coronal dentin stressed perpendicular to tubule orientation(C). Coronal dentintested parallel to tubule orientation(D). Radicular dentin tested perpendicular to tubule orientation(E). Radiculardentin tested parallel to tubule orientation(F). Original magnification: 2500-3000X.
-
7/30/2019 artigoradioterapia1
4/7
162 Soares et al. J Dent Res 89(2) 2010
when enamel was tested transversely to the orientation of prisms, fractures occurred preferentially along the interpris-matic substance, while, when it was tested parallel to its pris-matic orientation, fractures occurred obliquely to its longaxis, as occurred in the present study. These observationsclearly confirm the brittle and anisotropic behavior of enamel(Rasmussen et al ., 1976; Hassan et al ., 1981; Xu et al., 1998).The weaker interprismatic substance was aligned perpendicu-lar to the load, so the tension rapidly propagated across thespecimen, causing it to fail under a lower load. The enamelfailure occurred by separation of prisms along the interpris-matic substance; only a few prisms were obliquely cleaved(Giannini et al ., 2004). On enamel stressed parallel to its pris-matic orientation, the stress concentrated on the stronger
prismatic units, and the fracture required all prisms to becleaved before catastrophic failure occurred, resulting in
significantly higher UTS for enamel when tested under these conditions (Gianniniet al ., 2004).
Several factors mightinfluence the results of themicrotensile test. In this
study, all sample surfaceswere fixed with glue for thetesting (Soares et al ., 2008).We stored the samples inthymol, because it has beenshown (Giannini et al. , 2004)that this procedure does notaffect strength measure-ments. The cross-head speedwas defined at 0.5 mm/min,
because it is known to produce adequate stress/strain distribution during
load application. The proto-col used for radiation therapywas the same as that nor-mally used for the treatmentof patients with head andneck cancer; the incrementalfraction dose was importantto simulate the same dosethat patients receive daily.During radiation, teeth werestored in distilled water; stud-ies should be conducted toclarify the effects of storagemedia during this period.
Since the protein phase,which is concentrated inthe interprismatic region, ismore influenced by radio-therapy (Baker, 1982), theUTS was less in the perpen-dicular prismatic plane than
in the parallel plane. We identified a greater degree of irregu-larity in the fracture pattern of irradiated than non-irradi-ated enamel. This can possibly be explained by adisarrangement of the crystalline portion of enamel (Jansmaet al ., 1988), which represents the restructuring of the chemi-cal bonds into the mineral components that alter the crystal-line organization and alterations of protein interprismaticlinks (Baker, 1982), which resulted in higher prism cleavageindependent of stress orientation.
Previous results indicated that the UTS of dentin varies signifi-cantly and is dependent on intra-tooth location (Wang, 2005) anddepth (Konishi et al ., 2002; Giannini et al ., 2004). The presentstudy yielded higher UTS values when tensile force was directed
perpendicular to tubule orientation. It has been reported (Miguezet al ., 2004) that the majority of the fibrils run either perpen-dicular or oblique to the tubule direction, so tensile force applied to
Figure 3. Fracture pattern in sites of irradiated samples of stressed perpendicular enamel(A). Enamel testedparallel to prism orientation(B). Coronal dentin stressed perpendicular to tubule orientation(C). Coronal dentintested parallel to tubule orientation(D). Radicular dentin tested perpendicular to tubule orientation(E). Radiculardentin tested parallel to tubule orientation(F). Parallel and perpendicular fractured surface of enamel presentedplasticized and cone-shaped characteristics (A,B). At higher magnification, typical microcracks along intertu-bular dentin stressed parallel (D) and perpendicular (E) can be noted. Original magnification: 2500-3000X.
-
7/30/2019 artigoradioterapia1
5/7
J Dent Res 89(2) 2010 Effect of Radiation on Tooth Structures 163
collagen fibrils longitudinally results in higher UTS values than thatapplied perpendicularly. The results are consistent that fiber orienta-tions of crown and root dentin, which involve the tubules perpen-dicularly in the long axis. The mechanical properties of dentinare defined partly by its organic components (Inoue et al ., 2003;Miguez et al. , 2004), so when dentin is stressed perpendicular to tubule orientation, this substrate is really stressed parallel to
fiber orientation, which, since the fibers are stretched, results inincreased load to failure.In 1975, Walker affirmed that therapeutic irradiation did
not significantly affect the susceptibility of teeth to fracturein vivo but possibly may increase tooth fragility caused by pro-tein degradation. It was considered that there are two importantfactors that promote the destruction of enamel and dentin: radia-tion-associated destruction and radioxerostomia (Frnzel et al .,2006). The interaction of the organic matrix with apatite crystalsresults from the electrostatic binding of collagen carboxylate side-chains and surface mineral phosphate groups via calcium ions.The loss of acidic phosphate groups through the decarboxylationside-chain, promoted by radiation, precedes the formation of new
calcium ion bridge phosphate groups. Moreover, the mineral-organic interaction is reduced, and the development of carbondioxide may induce microcracks in the hydroxyapatite mineral,resulting in a roughened surface (Hubner et al ., 2005; Frnzelet al ., 2006).
While the mineral concentration is higher in peritubular dentin,the microcracks are concentrated in this area, reducing UTS valuesin coronal and root dentin. Additionally, the denaturation of theorganic matrix caused by radiolysis would reduce the physicalanchorage between enamel and dentin and the inner stability of dentin, since it contains collagen fibers as well (Pioch et al ., 1992).This tended to be more evident in this study, because, initially, theorientation of dentin tubules influenced UTS, but when the teethwere irradiated, the effects of tubule orientation on UTS disap-
peared, demonstrating that irradiation was more damaging toorganic components, mainly the collagen fibers.
Radioxerostomia also accompanies tooth destruction (Frnzelet al ., 2006). To avoid this, it is necessary that one use a methodthat can reduce tissue damage, such as a radio-protector (Heyet al., 2009). The irradiation effect on cross-linked collagen, andover the total integration or stability of collagen, in the testing of a new product that has been used to establish collagen structure(Salz et al., 2005; Bedran-Russo et al., 2007), should be tested inassociation with irradiation therapy. The stabilization of dentincollagen with biocompatible cross-linking agents may be of clini-cal importance to improve the UTS of dentin (Salz et al., 2005;Bedran-Russo et al ., 2007), and it is necessary to study differentmethods using chlorhexidine (Carrilho et al ., 2007) or other natu-ral cross-linking agents (Bedran-Russo et al ., 2007) and mecha-nisms to control the demineralization that occurs in enamel withthe use of fluoride solutions (Ccahuana-Vsquez et al ., 2007;Salar et al., 2007). Sealants applied to dentin and enamel(Gernhardt et al., 2007) should be tested during and betweenirradiation sessions, in an attempt to reduce this irradiation inter-ference and increase the quality of life of persons undergoingirradiation therapy for head and neck cancer. Within thelimitations of an in situ study, it can be concluded that irradiation
therapy significantly decreases the UTS of coronal and radicular dentin and enamel, regardless of tubule or prism orientation.However, this study also showed that the damage is potentiallygreatest for organic components.
ACKNOWLEDGMENTS
The authors are indebted to Dr. E.W. Kitajima (NAP/MEPA-ESALQ/USP) for SEM equipment support and to the Cancer Hospital of Uberlndia for irradiation equipment support. Thisstudy was supported by grants from FAPEMIG.
REFERENCES
Baker DG (1982). The radiobiological basis for tissue reactions in the oralcavity following therapeutic x-irradiation. A review. Arch Otolaryngol 108:21-24.
Bedran-Russo AK, Pereira PN, Duarte WR, Drummond JL, Yamauchi M(2007). Application of crosslinkers to dentin collagen enhances theultimate tensile strength. J Biomed Mater Res B Appl Biomater 80:268-272.
Carrilho MR, Carvalho RM, de Goes MF, de Hipolito V, Geraldeli S, TayFR, et al. (2007). Chlorhexidine preserves dentin bond in vitro . J Dent
Res 86:90-94.Carvalho RM, Fernandes CA, Villanueva R, Wang L, Pashley DH (2001).
Tensile strength of human dentin as a function of tubule orientation anddensity. J Adhes Dent 3:309-314.
Ccahuana-Vsquez RA, Tabchoury CP, Tenuta LM, Del Bel Cury AA, ValeGC, Cury JA (2007). Effect of frequency of sucrose exposure on dental
biofilm composition and enamel demineralization in the presence of fluoride. Caries Res 41:9-15.
Craddock HL (2006). Treatment and maintenance of a dentate patient withradiation caries. Dent Update 33:462-468.
Frnzel W, Gerlach R, Hein HJ, Schaller HG (2006). Effect of tumor thera- peutic irradiation on the mechanical properties of teeth tissue. Z Med Phys 16:148-154.
Gernhardt CR, Bekes K, Schaller HG (2007). Influence of three differentsealants on root dentin demineralization in situ. Am J Dent 20:390-393.
Giannini M, Soares CJ, de Carvalho RM (2004). Ultimate tensile strength of tooth structures. Dent Mater 20:322-329.
Hassan R, Caputo AA, Bunshah RF (1981). Fracture toughness of humanenamel. J Dent Res 60:820-827.
Hey J, Setz J, Gerlach R, Janich M, Sehlleier S, Schaller HG, et al. (2009).Parotid-gland-sparing 3D conformal radiotherapy in patients with bilat-eral radiotherapy of the head and neck regionresults in clinical prac-tice. Oral Oncol 45:e11-17.
Hong SX, Cha IH, Lee EW, Kim J (2001). Mandibular invasion of lower gingival carcinoma in the molar region: its clinical implications on thesurgical management. Int J Oral Maxillofac Surg 30:130-138.
Hubner W, Blume A, Pushnjakova R, Dekhtyar Y, Hein HJ (2005). Theinfluence of x-ray radiation on the mineral/organic matrix interaction of
bone tissue: an FT-IR microscopic investigation. Int J Artif Organs 28:66-73.
Inoue S, Pererira PNR, Kawamoto C, Nakajima M, Kenishi K, et al. (2003).Effect of depth and tubule direction on ultimate tensile strength of human coronal dentin. Dent Mater J 22:39-47.
Jansma J, Buskes JA, Vissink A, Mehta DM, sGravenmade EJ (1988). Theeffect of x-ray irradiation on the demineralization of bovine dentalenamel. A constant composition study. Caries Res 22:199-203.
Konishi N, Watanabe LG, Hilton JF, Marshall GW, Marshall SJ, Staninec M(2002). Dentin shear strength: effect of distance from the pulp. Dent
Mater 18:516-520.Lazarus C, Logemann JA, Pauloski BR, Rademaker AW, Helenowski IB,
Vonesh EF, et al. (2007). Effects of radiotherapy with or without che-motherapy on tongue strength and swallowing in patients with oralcancer. Head Neck 29:632-637.
-
7/30/2019 artigoradioterapia1
6/7
164 Soares et al. J Dent Res 89(2) 2010
Lertchirakarn V, Palamara JE, Messer HH (2001). Anisotropy of tensilestrength of root dentin. J Dent Res 80:453-456.
Lyons A (2006). Current concepts in the management of oral cancer. Dent Update 33:538-539, 542-545.
Miguez PA, Pereira PN, Atsawasuwan P, Yamauchi M (2004). Collagen cross-linking and ultimate tensile strength in dentin. J Dent Res 83:807-810.
Mjr IA (1972). Human coronal dentine: structure and reactions. Oral Surg Oral Med Oral Pathol 33:810-823.
Pioch T, Golfels D, Staehle HJ (1992). An experimental study of the stability
of irradiated teeth in the region of the dentinoenamel junction. Endod Dent Traumatol 8:241-244.
Rasmussen ST, Patchin RE, Scott DB, Heuer AH (1976). Fracture propertiesof human enamel and dentin. J Dent Res 55:154-164.
Salar DV, Garcia-Godoy F, Flaitz CM, Hicks MJ (2007). Potential inhibitionof demineralization in vitro by fluoride-releasing sealants. J Am Dent
Assoc 138:502-506.Salz U, Zimmermann J, Zeuner F, Moszner N (2005). Hydrolytic stability of
self-etching adhesive systems. J Adhes Dent 7:107-116.Silverman SJr (1999). Oral cancer. Complications of therapy. Oral Surg
Oral Med Oral Pathol Oral Radiol Endond 88:122-126.
Soares CJ, Soares PV, Santos-Filho PC, Armstrong SR (2008). Microtensilespecimen attachment and shapefinite element analysis. J Dent Res 87:89-93.
Spetch L (2002). Oral complications in the head and neck irradiated patient.Introduction and scope of the problem. Supp Care Dent 10:36-39.
Staninec M, Marshall GW, Hilton JF, Pashley DH, Gansky SA, MarshallSJ, et al. (2002). Ultimate tensile strength of dentin: evidence for adamage mechanics approach to dentin failure. J Biomed Mater Res 63:342-345.
Tronstad L (1973). Ultrastructural observation on human coronal dentin.Scand J Dent Res 81:101-111.
Urabe I, Nakajima M, Sano H, Tagami J (2000). Physical properties of thedentin-enamel junction region. Am J Dent 13:129-135.
Walker R (1975). Direct effect of radiation on the solubility of human teethin vitro [annotation]. J Dent Res 54:901.
Wang R (2005). Anisotropic fracture in bovine root and coronal dentin. Dent Mater 21:429-436.
Xu HHK, Smith DT, Jahanmir S, Romberg E, Kelly JR, Thompson VP, et al(1998). Indentation damage and mechanical properties of humanenamel and dentin. J Dent Res 77:472-480.
-
7/30/2019 artigoradioterapia1
7/7
Copyright of Journal of Dental Research is the property of Sage Publications Inc. and its content may not be
copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.