Aspectos Fisiopatológicos da Inflamação e o Planejamento ...
Contribuição dos novos conceitosFisiopatológicos no Tratamento da FA
Dra Martha Pinheiro (QuintaD`Or)

Fibrilação atrial
Arritmia sustentada mais comum na prática clínica;
Acomete 1-2% da população mundial
Doença multi-fatorial relacionada a patologias cardíacas e não cardíacas

World map showing the age-adjusted prevalence rates (per 100 000 population) of atrial
fibrillation in the 21 Global Burden of Disease regions, 2010.
Sumeet S. Chugh et al. Circulation. 2014;129:837-847
Copyright © American Heart Association, Inc. All rights reserved.

Year
Pro
ject
ed n
um
ber
of
pe
rso
ns
wit
h
AF
(mill
ion
s)
5.15.9
6.77.7
8.9
10.2
11.7
13.114.3
15.215.9
10.311.1
11.7 12.1
5.1 5.66.1 6.8
7.58.4
9.4
Miyasaka et.al Circulation 2006
Curva de prevalência da fibrilação atrial

Rohan S. Wijesurendra, and Barbara Casadei Cardiovasc Res 2015;cvr.cvv001
© The Author 2015. Published by Oxford University Press on behalf of the European Society of
Cardiology.
Efeitos sistêmicos da FA

Fatores de risco:
Clássicos:
•Envelhecimento
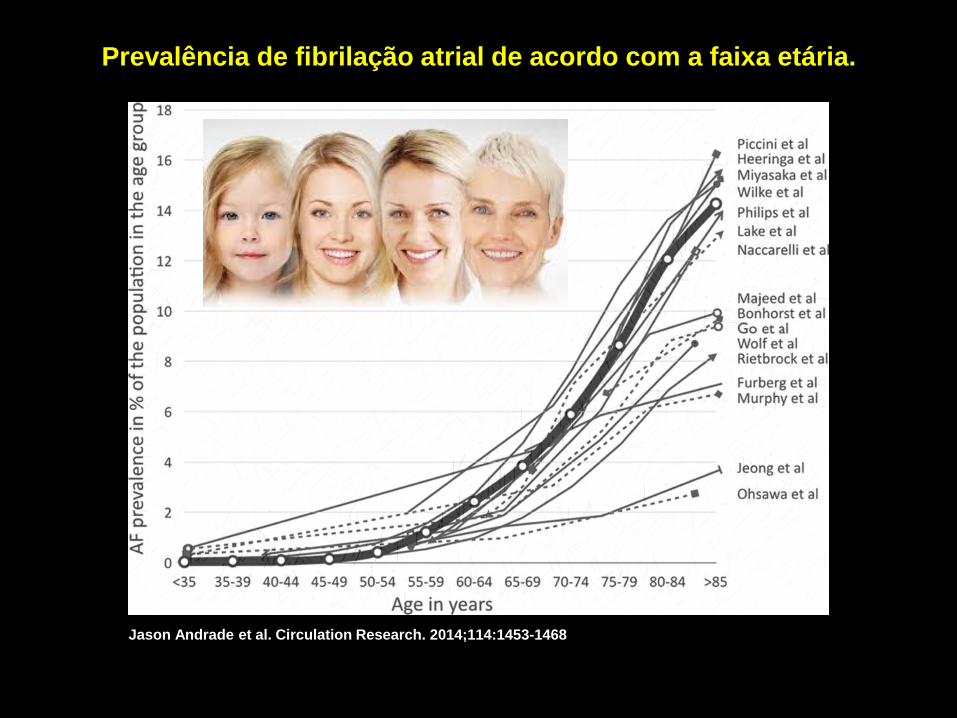
Prevalência de fibrilação atrial de acordo com a faixa etária.
Jason Andrade et al. Circulation Research. 2014;114:1453-1468
Copyright © American Heart Association, Inc. All rights reserved.

Fatores de risco:
Clássicos:
•Envelhecimento
•Gênero masculino
•HAS
•DM
•Doença valvar
•Insuficiência cardíaca
Fatores de risco:
Emergentes:
•Obesidade
•Síndrome da Apnéia Obstrutiva do Sono
•Estados inflamatórios sistêmicos
•Tabagismo
•Disfunção diastólica
•Variações genéticas

Fatores de risco:
Emergentes:
•Obesidade
•Síndrome da Apnéia Obstrutiva do Sono
•Estados inflamatórios sistêmicos
•Tabagismo
•Disfunção diastólica
•Variações genéticas

Risco de FA na Síndrome Metabólica
0
0,05
0,1
0,15
0,2
0,25
0 2 4 6 8 10 12 14 16 18 20
0 1 2 3 4 5
Chamberlain et al, ARIC Study, AHJ 2010
HR 1.67 CI (1.49-1.87)
HR (CI)
Metabolic Syndrome Component
Elevated waist circumference1.40
(1.23-1.59)
Elevated blood pressure1.95
(1.72-2.21)
Elevated triglycerides0.95
(0.84-1.09)
Low HDL cholesterol1.20
(1.06-1.37)
Impaired fasting glucose1.16
(1.03-1.31)

20%
30%
40%
50%
60%
70%
1982 1992 2002 2012 2022
USAEngland
France
Australia
KoreaPro
po
rtio
n o
verw
eigh
t
Years
Sassi et.al, OCED Publishing, 2014
Curva de evolução da obesidade

Evolução de indicadores na população de 20+ anos de idade, por sexo – Brasil
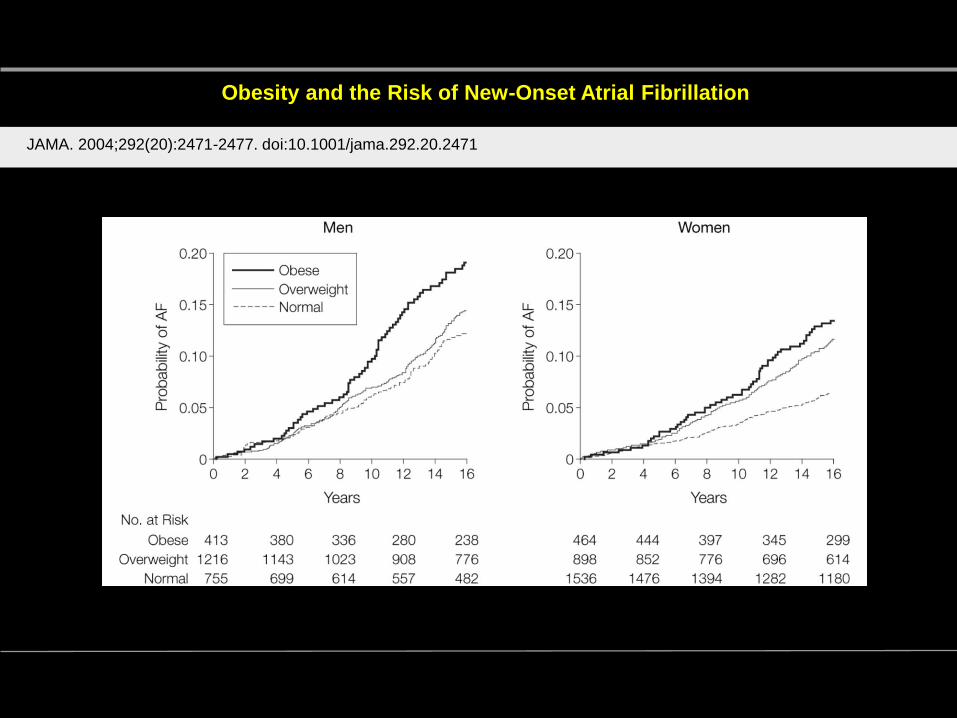
Obesity and the Risk of New-Onset Atrial Fibrillation
JAMA. 2004;292(20):2471-2477. doi:10.1001/jama.292.20.2471
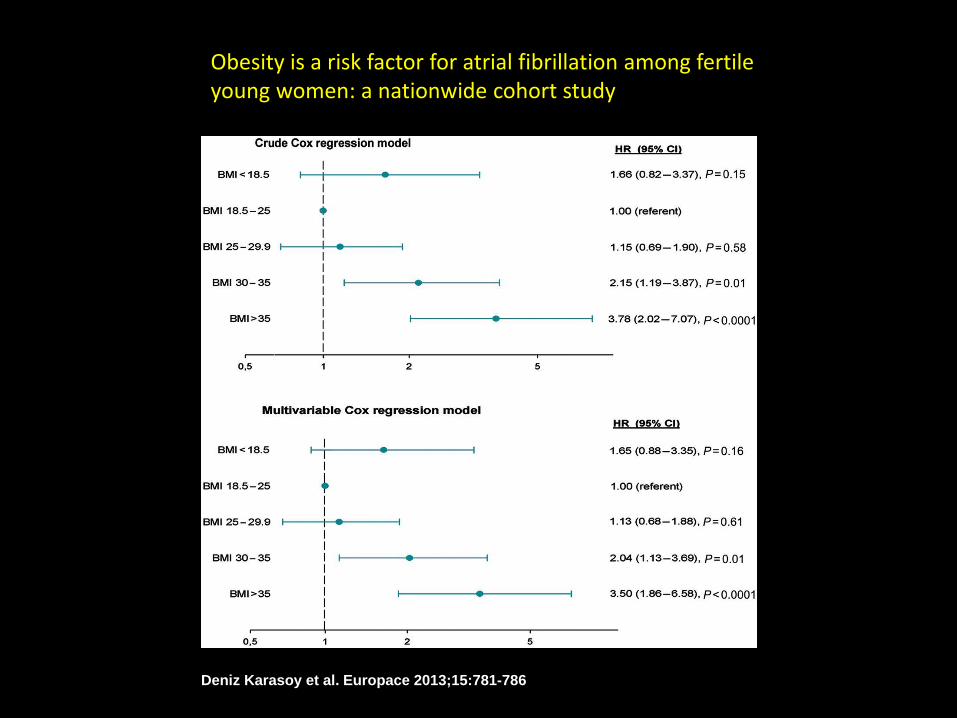
Deniz Karasoy et al. Europace 2013;15:781-786
Obesity is a risk factor for atrial fibrillation among fertile young women: a nationwide cohort study

Age- and sex-adjusted hazards of progression to permanent atrial fibrillation
stratified by body mass index categories and LA volume quartiles.
Teresa S.M. Tsang et al. Eur Heart J 2008;29:2227-2233
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2008. For permissions please email: [email protected]

Survival without conversion to permanent atrial fibrillation.
Teresa S.M. Tsang et al. Eur Heart J 2008;29:2227-2233

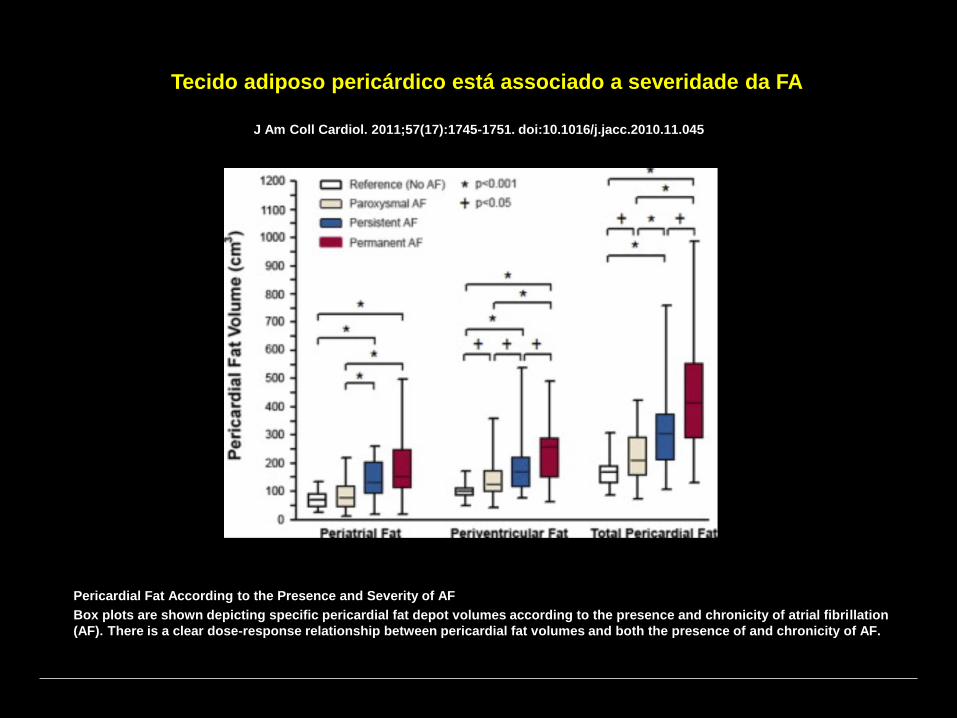
Pericardial Fat Is Associated With Atrial Fibrillation Severity and
Ablation OutcomeJ Am Coll Cardiol. 2011;57(17):1745-1751. doi:10.1016/j.jacc.2010.11.045
Volumetric MRI Assessment of Periatrial and Periventricular Fat
Example magnetic resonance imaging (MRI) slices depicting volumetric assessment of periatrial (A) and periventricular (B) fat
depots. Areas of pericardial fat are shaded in blue.
J Am Coll Cardiol. 2011;57(17):1745-1751. doi:10.1016/j.jacc.2010.11.045
Pericardial Fat According to the Presence and Severity of AF
Box plots are shown depicting specific pericardial fat depot volumes according to the presence and chronicity of atrial fibrillation
(AF). There is a clear dose-response relationship between pericardial fat volumes and both the presence of and chronicity of AF.
Tecido adiposo pericárdico está associado a severidade da FA

Mina K. Chung et al. Circulation. 2001;104:2886-2891
Copyright © American Heart Association, Inc. All rights reserved.
Inflamação e Fibrilação atrial
39
71
86
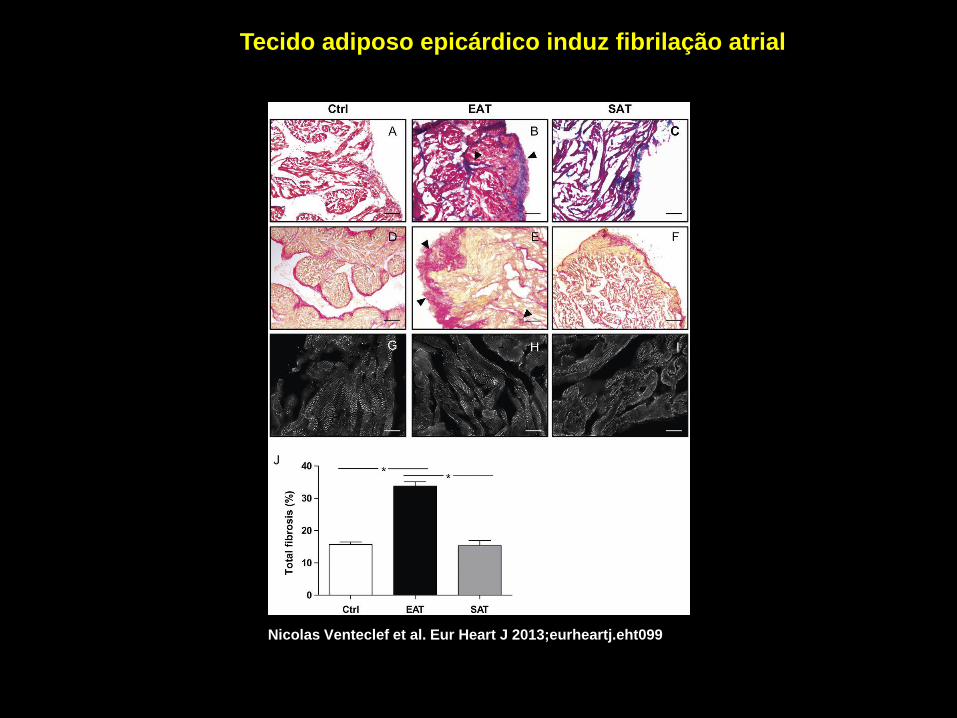
Nicolas Venteclef et al. Eur Heart J 2013;eurheartj.eht099
Tecido adiposo epicárdico induz fibrilação atrial

Jason Andrade et al. Circulation Research. 2014;114:1453-1468
Copyright © American Heart Association, Inc. All rights reserved.

Fibrose atrial e arritmogênese
Jason Andrade et al. Circulation Research. 2014;114:1453-1468
Copyright © American Heart Association, Inc. All rights reserved.
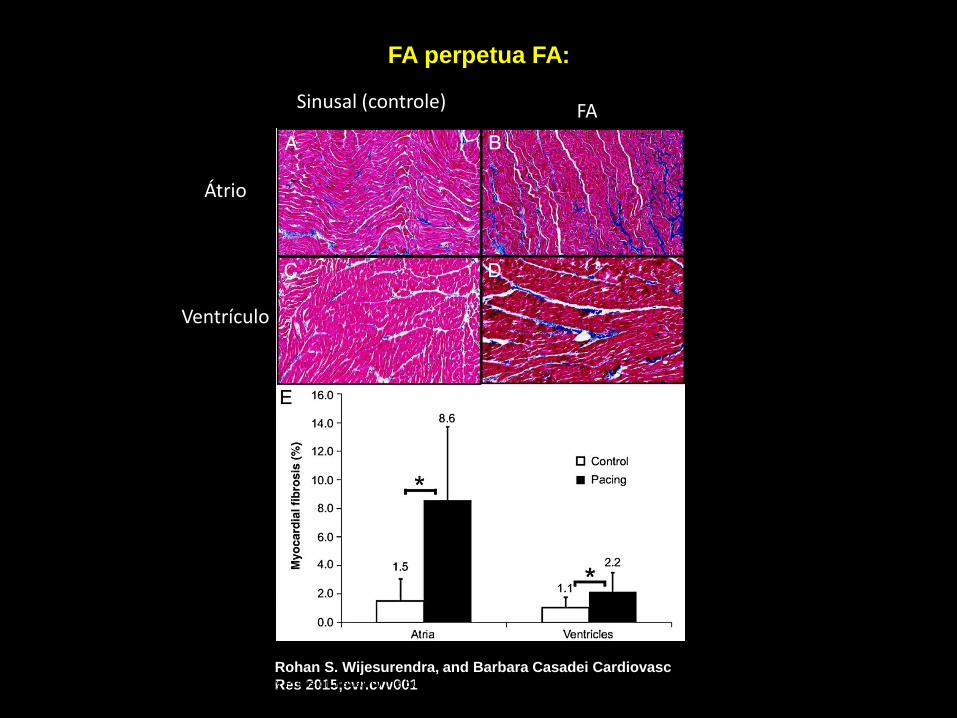
FA perpetua FA:
Rohan S. Wijesurendra, and Barbara Casadei Cardiovasc
Res 2015;cvr.cvv001© The Author 2015. Published by Oxford University Press on behalf of the European Society of
Cardiology.
Sinusal (controle) FA
Átrio
Ventrículo
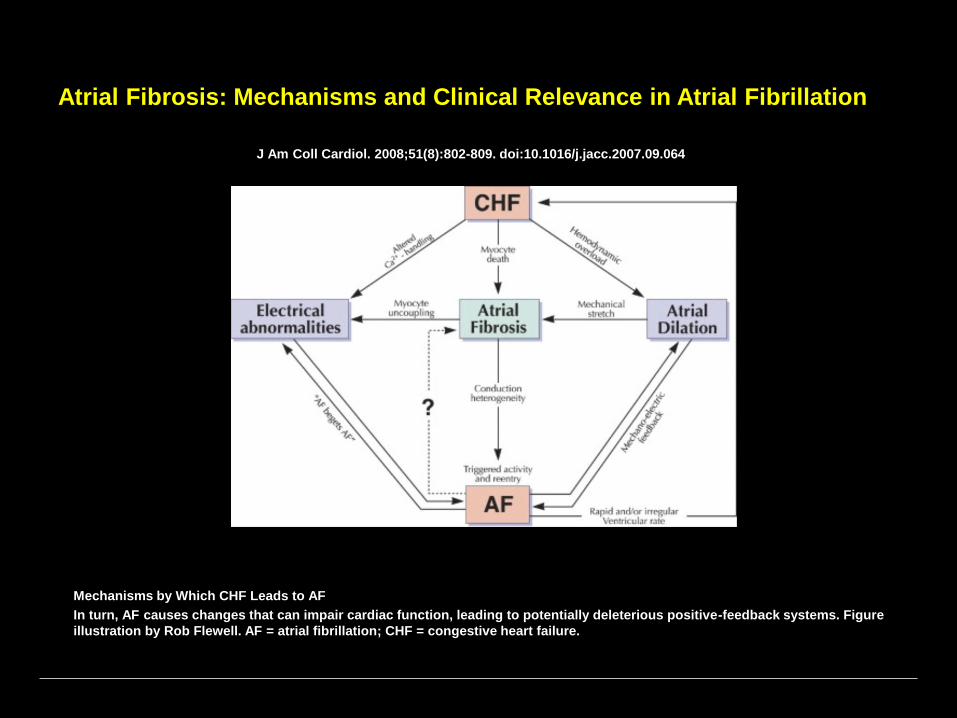
Atrial Fibrosis: Mechanisms and Clinical Relevance in Atrial Fibrillation
J Am Coll Cardiol. 2008;51(8):802-809. doi:10.1016/j.jacc.2007.09.064
Mechanisms by Which CHF Leads to AF
In turn, AF causes changes that can impair cardiac function, leading to potentially deleterious positive-feedback systems. Figure
illustration by Rob Flewell. AF = atrial fibrillation; CHF = congestive heart failure.

Rajeev K. Pathak; Melissa E. Middeldorp; Megan Meredith;Abhinav B. Mehta; Rajiv Mahajan; Walter P. Abhayaratna;
Dennis H. Lau; Prashanthan Sanders
Long-Term Effect of Goal Directed Weight Management in an Atrial Fibrillation Cohort:
A 5 Follow-Up StudY (LEGACY STUDY)
J Am Coll Cardiol. 2015;65(20):2159-2169. doi:10.1016/j.jacc.2015.03.002

J Am Coll Cardiol. 2015;65(20):2159-2169. doi:10.1016/j.jacc.2015.03.002
Long-Term Effect of Goal-Directed Weight Management in an Atrial
Fibrillation Cohort: A Long-Term Follow-Up Study (LEGACY)

Patients with BMI ≥ 27 N=825 Met Exclusion Criteria (N=293)
Terminal Cancer (N=10)Inflammatory Dx (N=20)Permanent AF (N=84)AV Node ablation (N=12)AF ablation (N=90)Severe Medical Illness (N=77)
<3%WL or WGN=117
3-9%WLN=103
Final Cohort N=355
Assessed for EligibilityN=1415
≥10%WLN=135
Weight Management

<3% Wt LossGroup 3N= 117
3-9% Wt LossGroup 2N = 103
>10% Wt LossGroup 1N = 135
P Value
Age (years) 6111 6311 6511 0.06
Male gender, n (%) 83 (71) 65 (63) 86 (64) 0.4
Non-Paroxysmal AF, n (%) 45 (56) 46 (45) 64 (47) 0.9
BMI 32.94.8 32.74.4 33.64.7 0.2
Hypertension 90 (78) 75 (73) 109 (81) 0.3
DM/IGT, n (%) 34 (29) 28 (27) 41 (30) 0.5
Hyperlipidemia, n (%) 56 (48) 45 (44) 66 (49) 0.7
CAD, n (%) 14 (12) 12 (12) 21 (16) 0.3
AHI>30, n (%) 61 (52) 52 (50) 69 (51) 0.1
Smoker, n (%) 47 (40) 41 (40) 50 (37) 0.9
ETOH (>30g/week), n (%) 34 (29) 35 (34) 42 (31) 0.7
Características basais
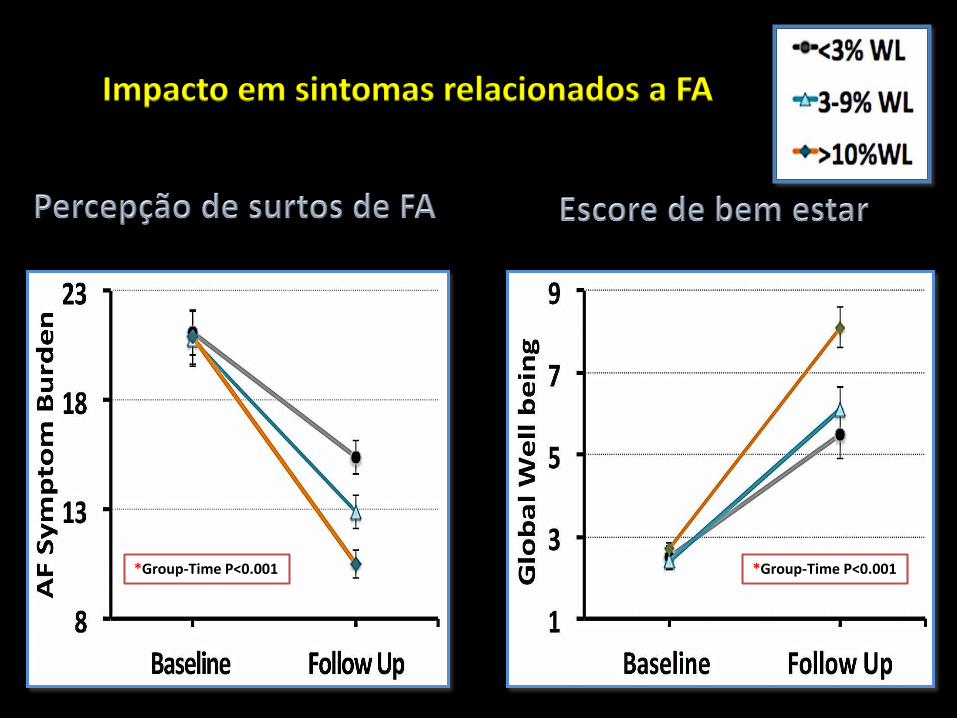
Impacto em sintomas relacionados a FA
*Group-Time P<0.001 *Group-Time P<0.001
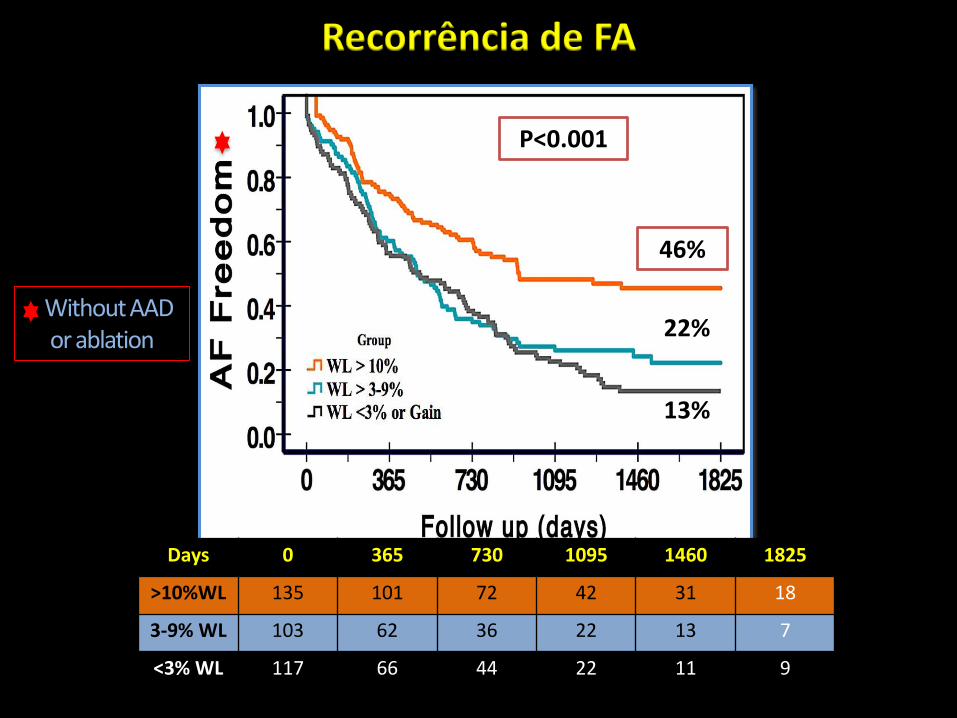
Recorrência de FA
Days 0 365 730 1095 1460 1825
>10%WL 135 101 72 42 31 18
3-9% WL 103 62 36 22 13 7
<3% WL 117 66 44 22 11 9
P<0.001
13%
22%Without AAD or ablation
46%46%
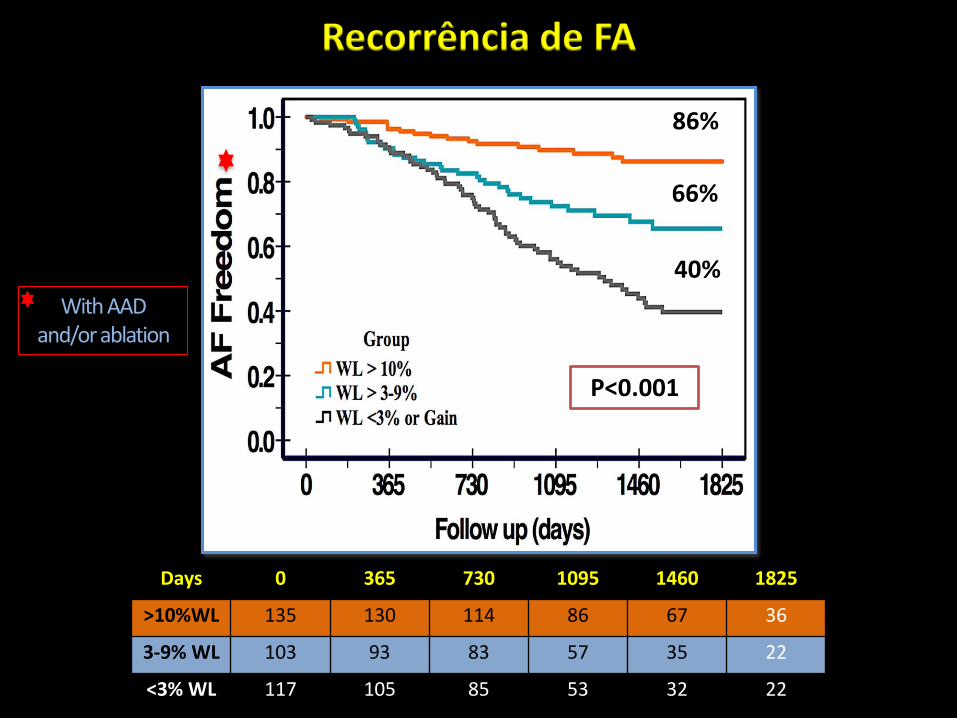
Days 0 365 730 1095 1460 1825
>10%WL 135 130 114 86 67 36
3-9% WL 103 93 83 57 35 22
<3% WL 117 105 85 53 32 22
P<0.001
86%
66%
40%
With AAD and/or ablation
Recorrência de FA

Impacto nos fatores de risco
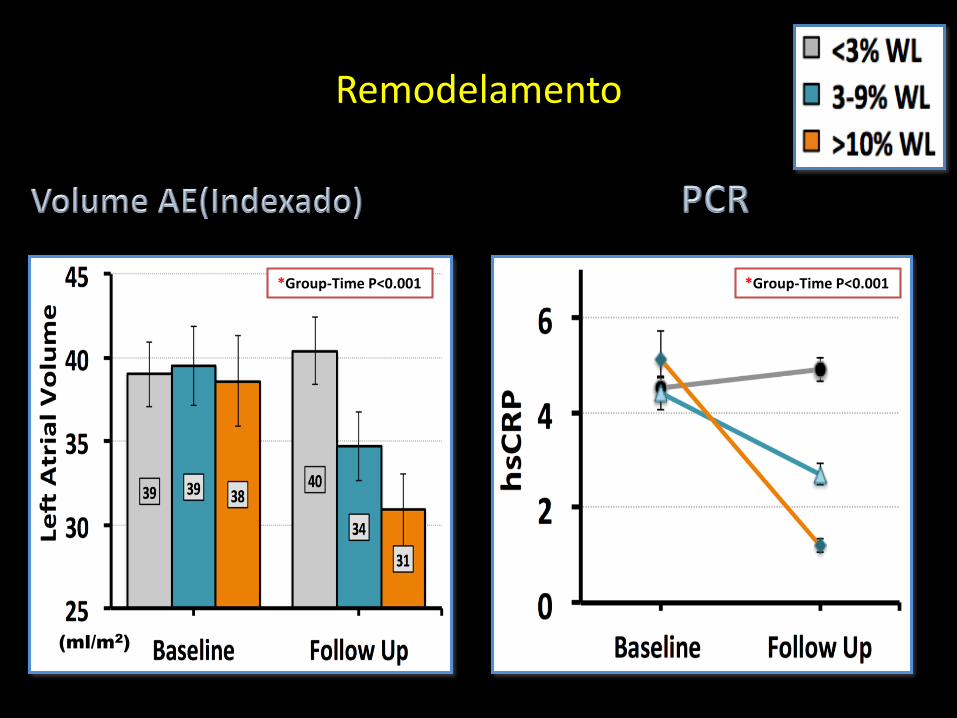
(ml/m2) (mg/L)
*Group-Time P<0.001 *Group-Time P<0.001
Remodelamento
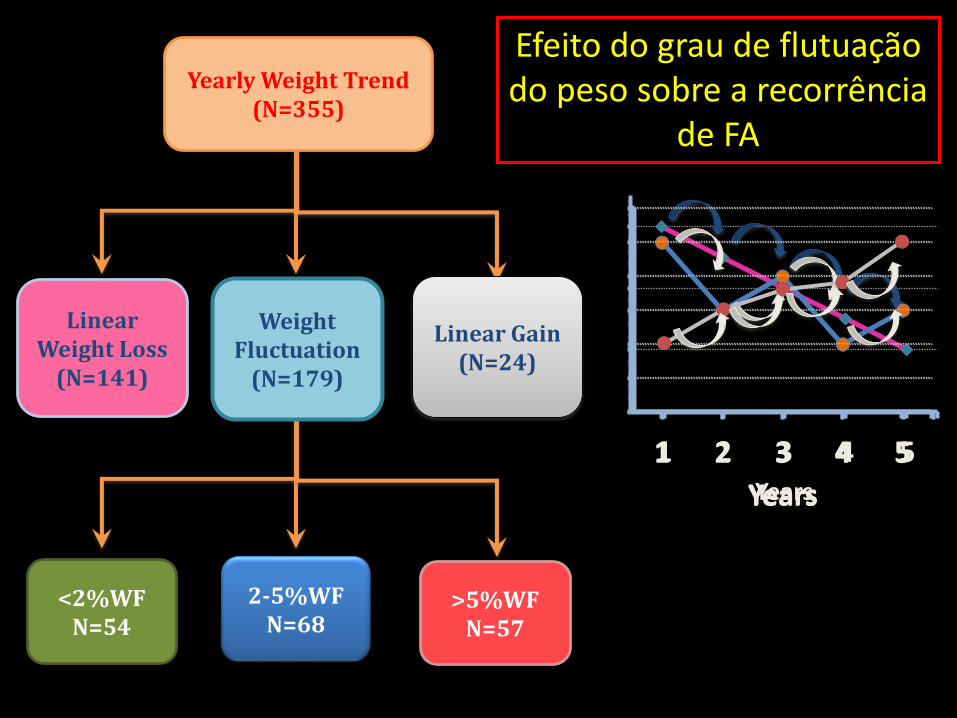
Yearly Weight Trend (N=355)
>5%WF N=57
2-5%WF N=68
<2%WF N=54
Linear Weight Loss
(N=141)
Weight Fluctuation
(N=179)
Linear Gain(N=24)
Efeito do grau de flutuação do peso sobre a recorrência
de FA
50
70
90
110
1 2 3 4 5Years
90
95
100
105
110
115
120
1 2 3 4 5
Years
80
85
90
95
100
105
110
1 2 3 4 5
Years
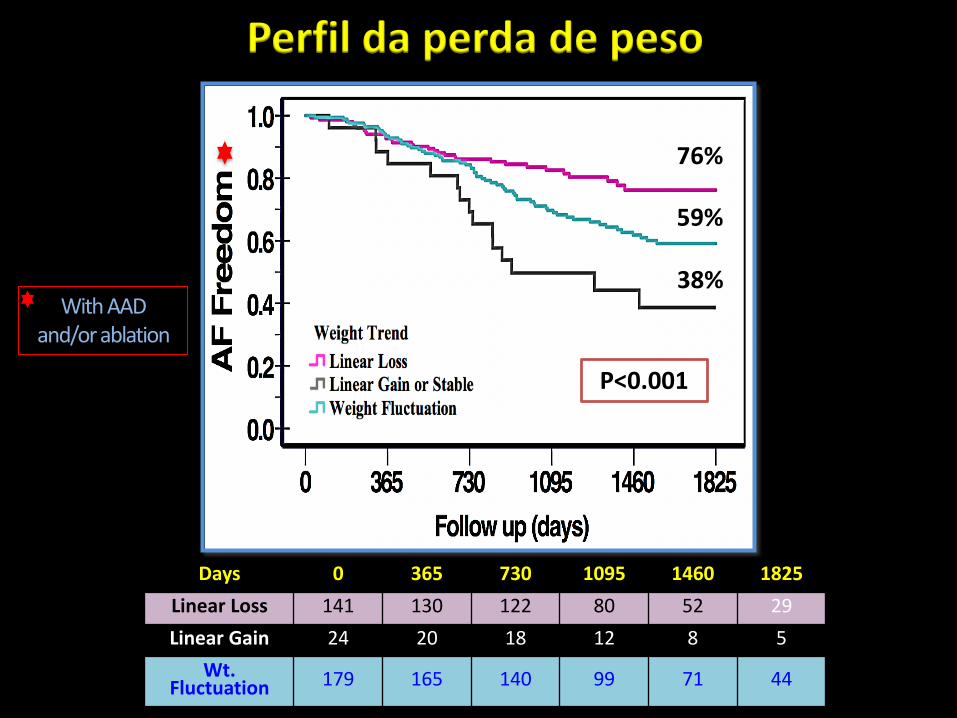
Perfil da perda de peso
P<0.001
Days 0 365 730 1095 1460 1825
Linear Loss 141 130 122 80 52 29
Linear Gain 24 20 18 12 8 5
Wt. Fluctuation 179 165 140 99 71 44
76%
59%
38%With AAD
and/or ablation
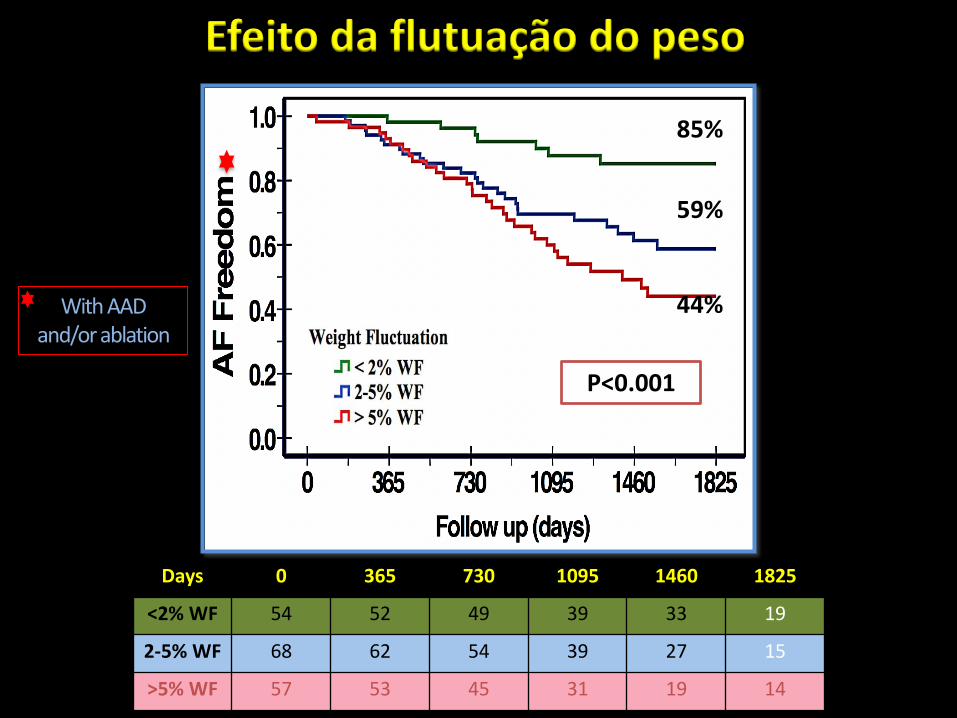
Efeito da flutuação do peso
Days 0 365 730 1095 1460 1825
<2% WF 54 52 49 39 33 19
2-5% WF 68 62 54 39 27 15
>5% WF 57 53 45 31 19 14
P<0.001
85%
59%
44%With AAD and/or ablation

Conclusões do Estudo Legacy
Perda sustentada de peso está associada com redução na taxa de eventos de FA e manutenção do ritmo sinusal;
Redução dos eventos é proporcional ao grau de perda de peso.
Flutuações de peso acima de 5% amortece o benefício conferido pela perda ponderal

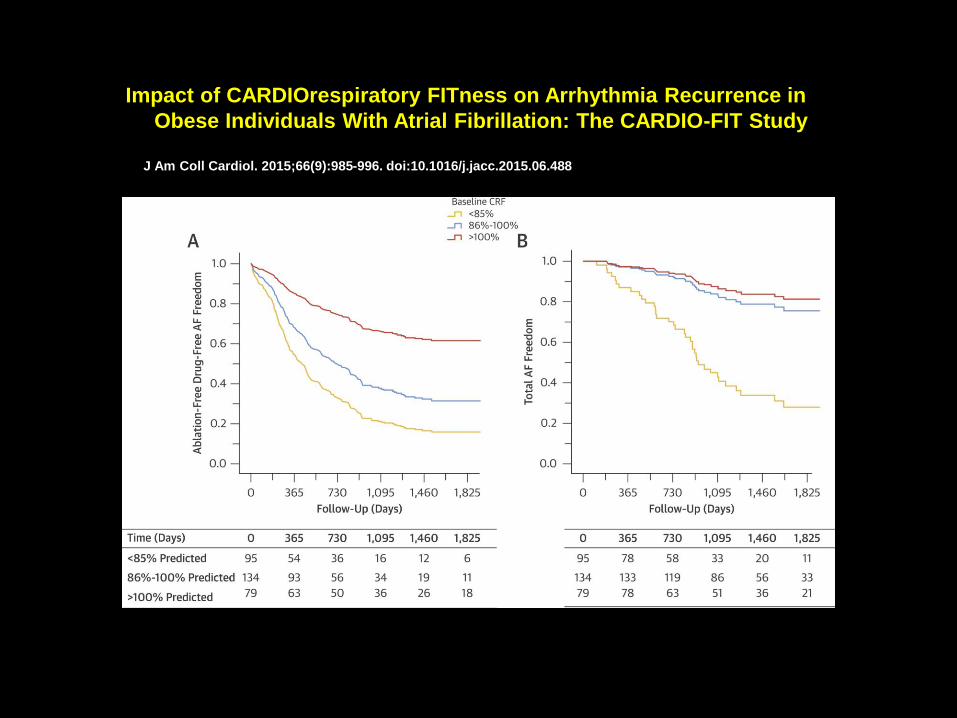
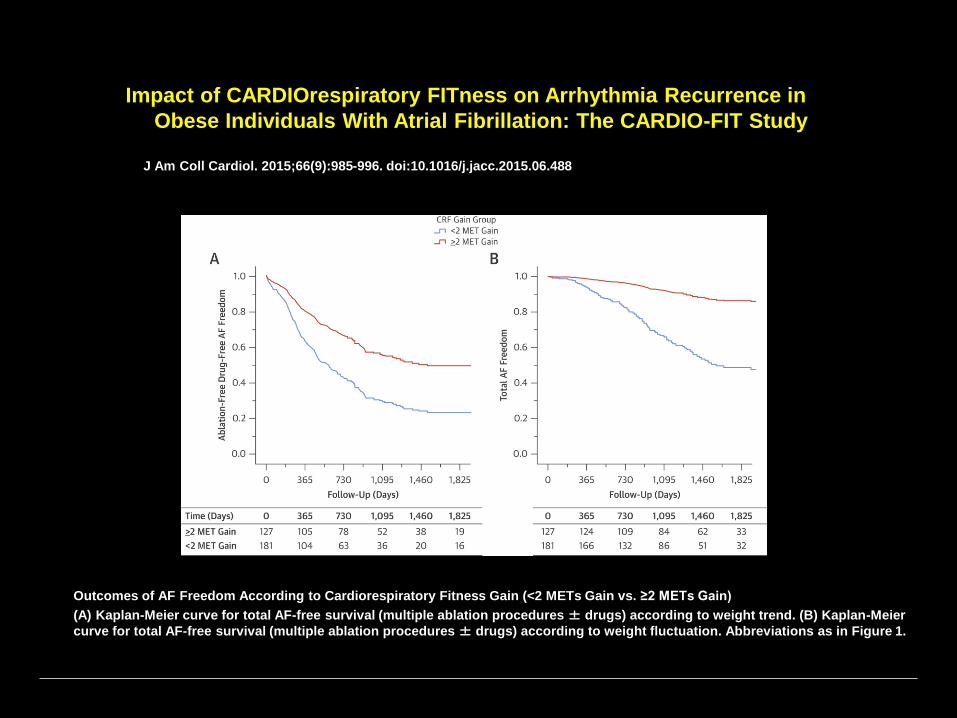
Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in
Obese Individuals With Atrial Fibrillation: The CARDIO-FIT Study
J Am Coll Cardiol. 2015;66(9):985-996. doi:10.1016/j.jacc.2015.06.488
Cardiorespiratory Fitness and AF Recurrence: CARDIO-FIT trial
AF = atrial fibrillation; BP = blood pressure; CARDIO-FIT = CARDIOrespiratory FITness; CRF = cardiorespiratory fitness; MET =
metabolic equivalent.

J Am Coll Cardiol. 2015;66(9):985-996. doi:10.1016/j.jacc.2015.06.488
Rajeev K. Pathak, MBBS∗; Adrian Elliott, PhD∗; Melissa E. Middeldorp∗; Megan Meredith∗; Abhinav B. Mehta, M Act St†; Rajiv Mahajan, MD, PhD∗; Jeroen M.L. Hendriks, PhD∗; Darragh Twomey, MBBS∗; Jonathan M. Kalman, MBBS, PhD‡; Walter P. Abhayaratna, MBBS, PhD§; Dennis H. Lau, MBBS, PhD∗; Prashanthan Sanders, MBBS, PhD∗
Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in Obese Individuals With Atrial Fibrillation

Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in
Obese Individuals With Atrial Fibrillation: The CARDIO-FIT Study
J Am Coll Cardiol. 2015;66(9):985-996. doi:10.1016/j.jacc.2015.06.488
Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in
Obese Individuals With Atrial Fibrillation: The CARDIO-FIT Study
J Am Coll Cardiol. 2015;66(9):985-996. doi:10.1016/j.jacc.2015.06.488
Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in
Obese Individuals With Atrial Fibrillation: The CARDIO-FIT Study
J Am Coll Cardiol. 2015;66(9):985-996. doi:10.1016/j.jacc.2015.06.488
Outcomes of AF Freedom According to Cardiorespiratory Fitness Gain (<2 METs Gain vs. ≥2 METs Gain)
(A) Kaplan-Meier curve for total AF-free survival (multiple ablation procedures ± drugs) according to weight trend. (B) Kaplan-Meier
curve for total AF-free survival (multiple ablation procedures ± drugs) according to weight fluctuation. Abbreviations as in Figure 1.

Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in
Obese Individuals With Atrial Fibrillation: The CARDIO-FIT Study
J Am Coll Cardiol. 2015;66(9):985-996. doi:10.1016/j.jacc.2015.06.488
Outcomes of AF Freedom According to Cardiorespiratory Fitness Gain (<2 METs Gain vs. ≥2 METs Gain) and Weight Loss (<10%
vs. ≥10% Weight Loss)
(A) Kaplan-Meier curve for total AF-free survival (multiple ablation procedures ± drugs) according to weight trend. (B) Kaplan-Meier
curve for total AF-free survival (multiple ablation procedures ± drugs) according to weight fluctuation. WL = weight loss; other
abbreviations as in Figure 1.
Conclusões do Estudo Cardio-Fit
Ganho no condicionamento cardiorrespiratório aumenta em cerca de 12% o benefício da perda de peso na manutenção do ritmo sinusal;

Apnéia do sono e Fibrilação atrial
Sleep-disordered breathing: a novel predictor of atrial fibrillation after coronary artery bypass surgery.Mooe T1, Gullsby S, Rabben T, Eriksson P
Coron Artery Dis. 1996 Jun;7(6):475-8
Sobrecarga hemodinâmica , ativação simpática e estresse hemodinâmico podem desencadear arritmias.
Risco de fibrilação atrial em pós-operatório de cirurgia cardíaca:
121 pacientes consecutivos submetidos a cirurgia de revascularização miocárdica;
Apnéia do sono aumenta 2 x o risco de FA no pós-operatório

Proportion and 95% CI of patients with OSA. Prevalence of OSA is significantly higher in patients
with AF than in patients without past or current AF in general cardiology practice (49% [95% CI 41%
to 57%] vs 32% [95% CI 27% to 37%], P=0.0004).
Apoor S. Gami et al. Circulation. 2004;110:364-367
Copyright © American Heart Association, Inc. All rights reserved.
Apnéia do sono e Fibrilação atrial

Atrial Fibrillation Promotion With Long-Term Repetitive Obstructive Sleep
Apnea in a Rat ModelJ Am Coll Cardiol. 2014;64(19):2013-2023. doi:10.1016/j.jacc.2014.05.077
AF Susceptibility Changes at Study End
Examples of atrial fibrillation (AF) induction attempts in (A) an open airway rat and (B) an OSA rat, respectively. (C) AF duration.
(D) AF inducibility. (E) AF inducibility during acute OSA. *p < 0.05 vs. sham. AF duration compared by using 1-way analysis of
variance; AF inducibility compared by using the Fisher exact test. EGM = electrogram; OSA = obstructive sleep apnea; SR = sinus
rhythm.
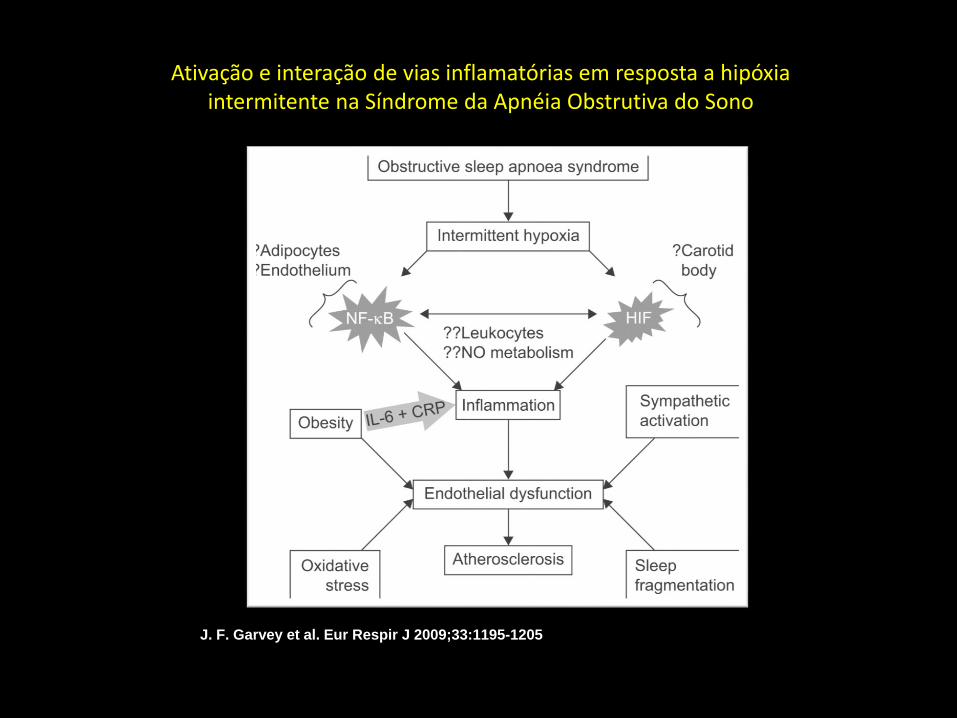
J. F. Garvey et al. Eur Respir J 2009;33:1195-1205
©2009 by European Respiratory Society
Ativação e interação de vias inflamatórias em resposta a hipóxia intermitente na Síndrome da Apnéia Obstrutiva do Sono

(A) Kaplan–Meier curves showing survival free of atrial fibrillation recurrence according to
dichotomized aponea/hypopnoea index (<15/≥15 events/h).
Andrea Mazza et al. Europace 2009;11:902-909
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2009. For permissions please email: [email protected]
SAOS e risco de recorrência de FA em indivíduos submetidos a cardioversão elétrica

Andrea Mazza et al. Europace 2009;11:902-909
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2009. For permissions please email: [email protected]
Inflamação e recorrência de FA em pacientes tratados com cardioversão elétrica

Andrea Mazza et al. Europace 2009;11:902-909
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2009. For permissions please email: [email protected]
(A) Kaplan–Meier curves showing survival free of atrial fibrillation recurrence according to
dichotomized aponea/hypopnoea index (<15/≥15 events/h).
Índice de apnéia/hipopnéia e níveis de PCR combinados e recorrência de FA em pacientes tratados com cardioversão

Freedom from arrhythmia recurrences after a single ablation procedure.
Maria Matiello et al. Europace 2010;12:1084-1089

Effect of Obstructive Sleep Apnea Treatment on Atrial Fibrillation Recurrence:
A Meta-Analysis
JACCCEP. 2015;1(1):41-51. doi:10.1016/j.jacep.2015.02.014
AF Recurrence in Users Versus Nonusers of CPAP in 2 Groups of Patients With OSA: PVI and Non-PVI Groups
PVI = pulmonary vein isolation;
Contribuição dos novos conceitosFisiopatológicos no Tratamento da FA
Conclusão:
•Influência da obesidade e Síndrome da Apnéia do Sono sobre o risco de desencadeamento e perpetuação de Fibrilação atrial;
•Necessidade de controle destes fatores de risco modificáveis para reduzir o risco de desencadeamento da FA e otimizar o efeito das estratégias de controle do ritmo cardíaco.
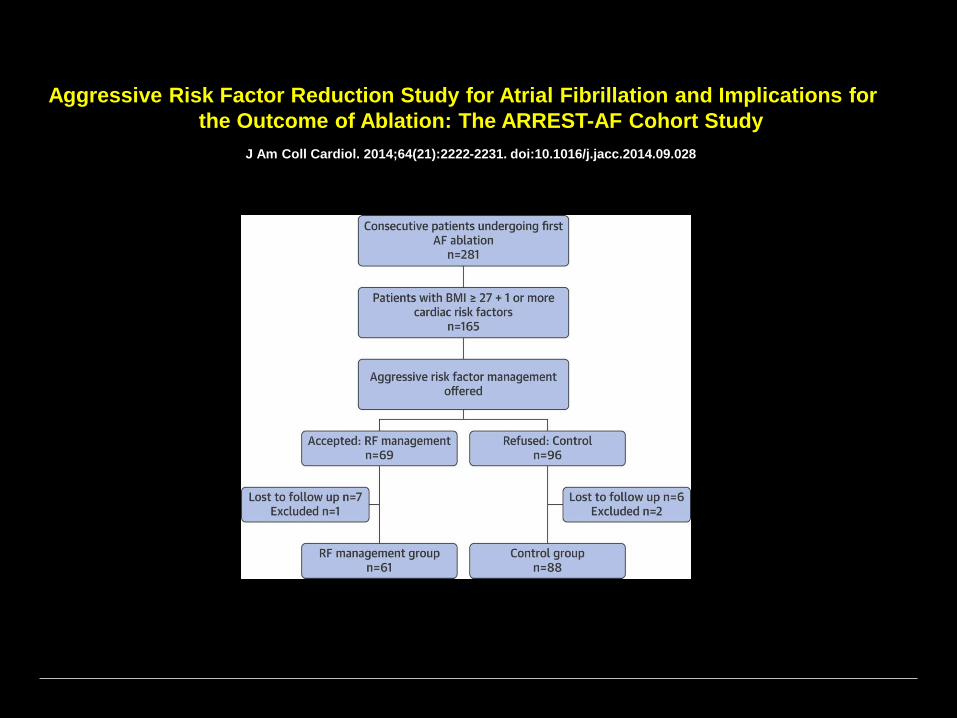
Aggressive Risk Factor Reduction Study for Atrial Fibrillation and Implications for
the Outcome of Ablation: The ARREST-AF Cohort Study
J Am Coll Cardiol. 2014;64(21):2222-2231. doi:10.1016/j.jacc.2014.09.028

Yohei Sotomi et al. Europace 2013;15:1581-1586
Incidence and risk factors for very late recurrence of atrial fibrillation after radiofrequency catheter ablation

Aggressive Risk Factor Reduction Study for Atrial Fibrillation and
Implications for the Outcome of Ablation: The ARREST-AF Cohort
Study
J Am Coll Cardiol. 2014;64(21):2222-2231. doi:10.1016/j.jacc.2014.09.028

Fibrotic Atrial Cardiomyopathy, Atrial Fibrillation, and Thromboembolism:
Mechanistic Links and Clinical Inferences
J Am Coll Cardiol. 2015;65(20):2239-2251. doi:10.1016/j.jacc.2015.03.557
3D Cardiac Magnetic Resonance Reconstructions of LA Fibrosis in the RAO and PA Projections
Reconstructions are according to the percent of fibrosis, as graded by the UTAH staging system. UTAH I: <5% fibrosis; II: 5% to
19% fibrosis; III: 20% to 35% fibrosis; and IV: >35% fibrosis. Green indicates LA fibrosis. Reprinted with permission from Akoum
et al. (96). 3D = 3-dimensional; LA = left atrium; PA = postero-anterior; RAO = right anterior oblique.
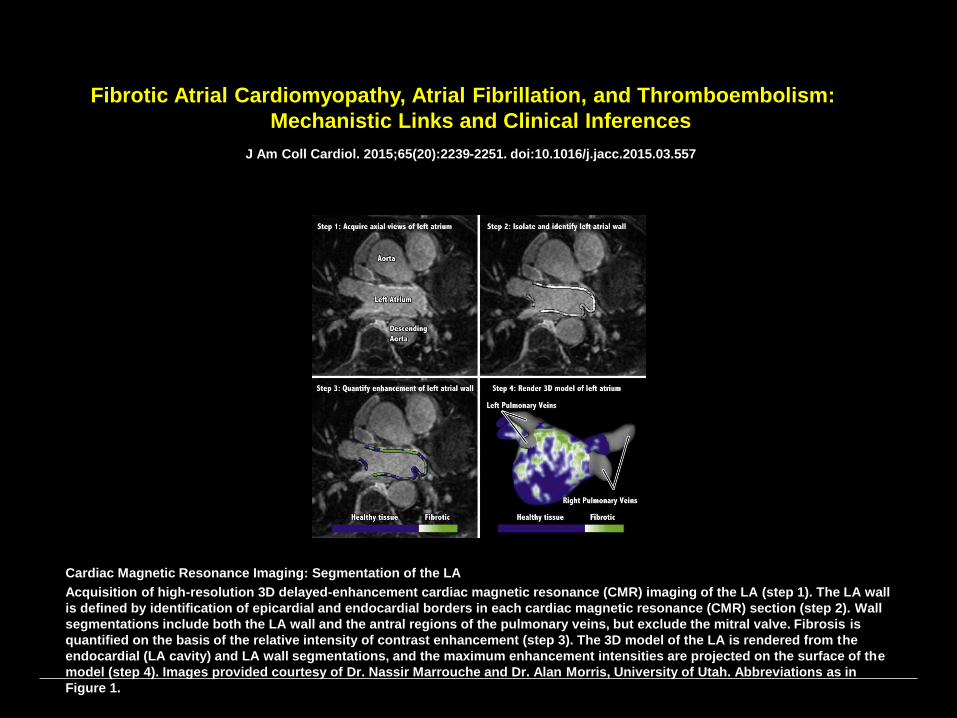
Fibrotic Atrial Cardiomyopathy, Atrial Fibrillation, and Thromboembolism:
Mechanistic Links and Clinical Inferences
J Am Coll Cardiol. 2015;65(20):2239-2251. doi:10.1016/j.jacc.2015.03.557
Cardiac Magnetic Resonance Imaging: Segmentation of the LA
Acquisition of high-resolution 3D delayed-enhancement cardiac magnetic resonance (CMR) imaging of the LA (step 1). The LA wall
is defined by identification of epicardial and endocardial borders in each cardiac magnetic resonance (CMR) section (step 2). Wall
segmentations include both the LA wall and the antral regions of the pulmonary veins, but exclude the mitral valve. Fibrosis is
quantified on the basis of the relative intensity of contrast enhancement (step 3). The 3D model of the LA is rendered from the
endocardial (LA cavity) and LA wall segmentations, and the maximum enhancement intensities are projected on the surface of the
model (step 4). Images provided courtesy of Dr. Nassir Marrouche and Dr. Alan Morris, University of Utah. Abbreviations as in
Figure 1.
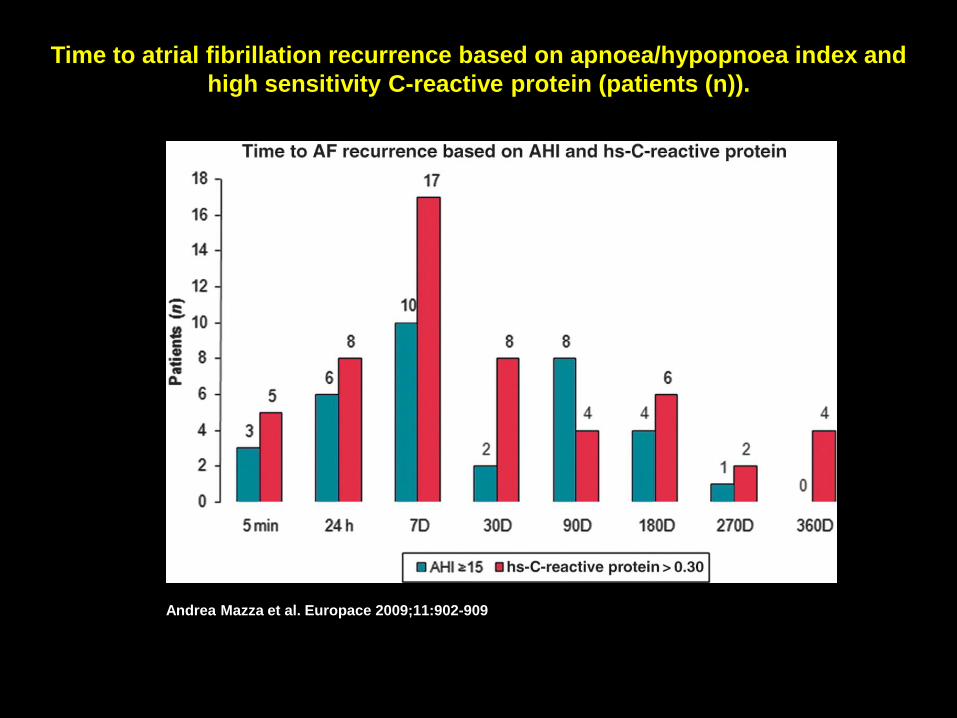
Time to atrial fibrillation recurrence based on apnoea/hypopnoea index and
high sensitivity C-reactive protein (patients (n)).
Andrea Mazza et al. Europace 2009;11:902-909
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author
2009. For permissions please email: [email protected]

Fibrotic Atrial Cardiomyopathy, Atrial Fibrillation, and Thromboembolism:
Mechanistic Links and Clinical Inferences
J Am Coll Cardiol. 2015;65(20):2239-2251. doi:10.1016/j.jacc.2015.03.557