Fisiologia do Sistema Digestório e aplicações clínicas Profa. Dra. Cristina Maria Henrique Pinto...
93
Fisiologia do Fisiologia do Sistema Sistema Digestório Digestório e aplicações e aplicações clínicas clínicas Profa. Dra. Cristina Maria Henrique Pinto Profa. Associada II do Depto. Ciências Fisiológicas CCB-UFSC Como citar este documento: PINTO, Cristina Maria Henrique. Fisiologia do Sistema Digestório relacionada à Clínica Médica. Disponível em: <http://www.cristina.prof.ufsc.br>. Acesso em: (coloque a data aqui)
-
Upload
caua-solomon -
Category
Documents
-
view
221 -
download
3
Transcript of Fisiologia do Sistema Digestório e aplicações clínicas Profa. Dra. Cristina Maria Henrique Pinto...

Fisiologia do Sistema Fisiologia do Sistema Digestório Digestório
e aplicações clínicase aplicações clínicas
Profa. Dra. Cristina Maria Henrique PintoProfa. Associada II do Depto. Ciências Fisiológicas
CCB-UFSC
Como citar este documento: PINTO, Cristina Maria Henrique. Fisiologia do Sistema Digestório relacionada à Clínica Médica. Disponível em:
<http://www.cristina.prof.ufsc.br>. Acesso em: (coloque a data aqui)

Esta apresentação foi utilizada em minhas aulas para a
graduação em Medicina (6ª fase) até o ano de 2007. Para
que este material não se perca, deixo aqui à disposição
daqueles que eventualmente tenham interesse porém, ele carece de revisão constante.
Bons estudos!

Profa. Dra. Cristina Maria Henrique PintoProfa. Associada II do Depto. Ciências Fisiológicas
CCB-UFSC
Esta aula e outros materiais relacionados estão disponíveis na página dedicada à
MED da 6ª fase em meu website:www.cristina.prof.ufsc.br
porém o acesso é restrito e exige os seguintes:
login : digfisiomed6 e senha: mercurio
Caso interesse o acesso à Med 2ª fase: login: fisiomed2 senha: saturno
Veja aqui a bibliografia básica

Caso interesse, consulte:Caso interesse, consulte:
Livro-texto:“Fisiologia Clínica do Sistema Digestório”
JOSE RAUL CISTERNAS & CARLOS ROBERTO
DOUGLAS, 2004. Ed. Tecmed
Recursos disponíveis on-line relacionados à Gastroenterologia

Motilidade (tipos, funções e regulação): Esofágica
Disfunções (GERD e acalasia) Gástrica (relaxamento receptivo, mistura e esvaziamento)
Disfunções (GERD)
Secreções gástricas Tipos de secreções (exócrinas e endócrinas ) Regulação das secreções Disfunções da secreção gástrica (úlceras pépticas)
Fisiologia do Sistema Digestório e aplicações clínicas relacionadas
ao esôfago e ao estômago

Fisiologia do Sistema Digestório e aplicações clínicas relacionadas
ao esôfago e ao estômago
Motilidade (tipos, funções e regulação): Esofágica
Disfunções (GERD e acalasia) Gástrica (relaxamento receptivo, mistura e esvaziamento)
Disfunções (GERD)
Secreções gástricas Tipos de secreções (exócrinas e endócrinas ) Regulação das secreções Disfunções da secreção gástrica (úlceras pépticas)

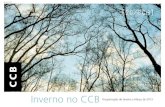
Motilidade esofágica: peristalse
esfíncter esofágico superior (EES)
esfíncter esofágico inferior (EEI)
esôfago diafragma
estômago
traquéia
Estímulos:
Deglutição
Presença de resíduo no esôfago
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

A deglutição desencadeia um movimento peristáltico (onda 1ária), que desloca-se desde o início do esôfago (1º terço, musculatura esquelética sob a coordenação de nervos cranianos)...
esfíncter esofágico superior (EES)
esfíncter esofágico inferior (EEI)
esôfago diafragma
estômago
traquéia
Motilidade esofágica: peristalse
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

esfíncter esofágico superior (EES)
esfíncter esofágico inferior (EEI)
esôfago diafragma
estômago
traquéia
... e propaga-se ao longo da musculatura lisa (3º terço de seu comprimento). O terço intermediário é constituído por fibras mistas (esqueléticas e lisas).
Motilidade esofágica: peristalse
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

esfíncter esofágico superior (EES)
esfíncter esofágico inferior (EEI)
esôfago diafragma
estômago
traquéia
Relaxamento do EEI: reflexo pela deglutição (movimento peristáltico desencadeado pela deglutição).
Resíduo no esôfago: ocorrência de ondas 2árias (reflexas).
Motilidade esofágica: peristalse
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill
esfíncter esofágico superior (EES)
esfíncter esofágico inferior (EEI)
esôfago diafragma
estômago
traquéia
Na porção intermediária e final da fase esofágica, a deglutição não envolve mais apenas o SNC, mas também o SNE para a propulsão do bolo alimentar e o relaxamento do EEI.
Motilidade esofágica: peristalse

Note that the cervical esophagus and the small part of the thoracic esophagus that includes the upper esophageal sphincter are composed of striated muscle. The lower two thirds of the esophagus, including the thoracic and abdominal parts containing the lower esophageal sphincter, are composed of smooth muscles. The diseases of the striated muscle include polymyositis and myasthenia gravis, whereas scleroderma and achalasia are diseases that involve the smooth muscle portion of the esophagus. (Source: AGA Gastroenterology Teaching Project, 2001, In myasthenia gravis, antibodies block, alter, or destroy the receptors for acetylcholine at the neuromuscular junction which prevents the muscle contraction from occurring. Polymyositis: inflamação da fibra muscular. Physiology of esophageal motility, Hiroshi Mashimo e Goyal, 2006, Motility online. http://www.nature.com/gimo/contents/pt1/full/gimo3.html
Características musculares do
esôfago
(perda da força muscular e atrofia ou por inflamação da
fibra muscular ou por bloqueio da junção meuro-muscular )
(doença auto-imune do tecido conjuntivo ou a alteração do
SNE)

Fase esofágica: podemos considerar a motilidade esofágica como sendo a continuação da deglutição: uma onda peristáltica começa logo abaixo do EES que desloca-se até o esfíncter esofágico inferior (EEI) relaxando-o e permitindo a entrada do bolo alimentar no estômago (relaxamento receptivo).
Veja aqui animação online
A motilidade esofágica se dá principalmente no momento da fase esofágica da deglutição
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

Motilidade esofágica durante a deglutição(veja vídeo online)
In normal subjects, swallowing is associated with opening of the upper and the lower esophageal sphincter and sequential peristaltic wave that pushes the tail of barium ahead of it. Normal esophageal clearing time is around 13 seconds.
“Physiology of oral cavity, pharynx and upper esophageal sphincter”, Massey, 2006 (GI motility online)página com índice dos vídeos: http://www.nature.com/gimo/videos/index.html página principal: http://www.nature.com/gimo/index.html

vista lateral indicando as regiões do esôfago
EEI ou complexo esfincteriano
inferior:EEI: esfíncter esofágico inferior
(“interno”) e hiato do diafragma
(componente “externo” do EEI)
O complexo esfincteriano inferior:
EEI esfíncter esofágico inferior
(“interno”):camada circular espessa,
especializada, 3-4cm, em contração tônica,
15-30 mmHg. Refluxo pode ocorrer caso
esta pressão seja inferior a 5 mmHg.
Relaxamento por inervação oxinitrérgica (NO) mas também
ATP e VIP.
Inervação: PS e SNE (vago, inibitório geralmente, inervação
colinérgica receptores nicotínicos).
Hiato do diafragma:contrai durante inspiração e contribui para o aumento do
tônus do EEI
“Barreira anti-refluxo”
O complexo esfincteriano inferior EEI
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

http://www.nature.com/gimo/contents/pt1/fig_tab/gimo14_F7.html
O complexo esfincteriano inferior:
EEI esfíncter esofágico inferior
(“interno”):camada circular espessa,
especializada, 3-4cm, em contração tônica,
15-30 mmHg. Refluxo pode ocorrer caso
esta pressão seja inferior a 5 mmHg.
Relaxamento por inervação oxinitrérgica (NO) mas também
VIP e ATP.
Inervação: PS e SNE (vago, inibitório geralmente, inervação
colinérgica receptores nicotínicos).
Hiato do diafragma:contrai durante inspiração e contribui para o aumento do
tônus do EEI
O complexo esfincteriano inferior EEI

DISFUNÇÕES MOTORAS DO ESÔFAGO
DOENÇAS DO REFLUXO GASTRO-ESOFÁGICO (GERD)
(Incompetência da barreira anti-refluxo da região esôfago-gástrica)
ACALASIA(Perda da capacidade de relaxamento do EEI)

A, B, esôfago normal comparado à esofagite erosiva.; A’, B’, visões endoscópicas
Doenças do refluxo gastroesofágico (GERD)A inflamação é resultante de contato prolongado da mucosa com o
conteúdo gástrico, podendo levar a lesões/úlceras de mucosa.
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

revisão: Boeckxstaens, 2005
Traçado manométrico de um exemplo típico de relaxamento do EEI (LOS) durante um episódio de refluxo e de relaxamento normal induzido por deglutição.
s/ deglutição c/ deglutição
Refluxo gastro-esofageano
TLOSR relaxamento transitório do EEI/LOS – reflexo vago-vagal
O TLOSR é fisiológico, ocorre periodicamente devido, por exemplo, à distensão gástrica (presença de ar ou alimento). Portanto, se a sua freqüência for baixa e se os mecanismos de depuração esofágica forem eficientes, não
provoca lesões de mucosa.
Pacientes com doenças do refluxo gastro-esofágico (GERD) podem apresentar tônus normal no EEI/LOS.
Uma possível causa da GERD: TLOSR (relaxamento transitório do EEI) – reflexo vago-vagal é mais freqüente, de maior duração e deflagrado quando ocorre distensão gástrica (presença de ar
ou alimento). Outra causa comum: hérnia de hiato

http://www.manualmerck.net/?url=/artigos/%3Fid%3D127%26cn%3D1084%26ss%3D
A hérnia do hiato é um protraimento anormal de uma porção do estômago para o interior do tórax através do diafragma.
Refluxo gastro-esofageano

Refluxo gastroesofágico(veja vídeo online)
Back flow of barium from the stomach into the esophagus.“Physiology of oral cavity, pharynx and upper esophageal sphincter”, Massey, 2006 (GI motility online)
página com índice dos vídeos: http://www.nature.com/gimo/videos/index.html página principal: http://www.nature.com/gimo/index.html

MÉTODOS DE AVALIAÇÃO DE DISFUNÇÕES MOTORAS DO ESÔFAGOEstudos manométricos(diagnósticos mais precisos)
Estudos manométricos avaliam as alterações de pressão que ocorremdurante a deglutição.Nesse teste são usados cateteres finos e flexíveis que passam através do nariz ou boca até o esôfago.O tubo possui uma série de sensores que permitem o registro da peristalse esofageana e graus de contração e relaxamento dos esfíncteres.http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

http://www.netanatomy.com/RA/ra_frame.htm
Métodos de avaliação de disfunções motoras do esôfagoVideofluoroscopia com visão normal da junção gastro-esofágica
extraído (enquanto disponível) de: http://www.netanatomy.com/nosubscription/notvalidip.htm

Métodos de avaliação de disfunções motoras do esôfagoVideofluoroscopia com visão normal da junção gastro-esofágica
extraído (enquanto disponível) de: http://www.netanatomy.com/nosubscription/notvalidip.htm

http://www.netanatomy.com/RA/ra_frame.htm
Métodos de avaliação de disfunções motoras do esôfagoVideofluoroscopia com visão normal da junção gastro-esofágica
extraído (enquanto disponível) de: http://www.netanatomy.com/nosubscription/notvalidip.htm

Métodos de avaliação de disfunções motoras do esôfagoVideofluoroscopia com visão normal da junção gastro-esofágica
extraído (enquanto disponível) de: http://www.netanatomy.com/nosubscription/notvalidip.htm

Hérnia de hiato(veja vídeo online)
Normally during a swallow, a portion of the stomach moves into the chest due to contraction of the esophageal longitudinal muscle. Failure of the portion of the gastric fundus to return to its intra-abdominal location is
indicative of hiatal hernia.“Physiology of oral cavity, pharynx and upper esophageal sphincter”, Massey, 2006 (GI motility online)
página com índice dos vídeos: http://www.nature.com/gimo/videos/index.html página principal: http://www.nature.com/gimo/index.html

Acalasia clássica(veja vídeo online)
In classic achalasia, the esophagus is dilated with poor contractions. The lower esophageal sphincter remains contracted producing a bird beak appearance. Achalasia must be differentiated from other cases of narrowing at the lower end of the esophagus, like carcinoma of the esophagogastric junction and peptic strictures with scleroderma.
“Physiology of oral cavity, pharynx and upper esophageal sphincter”, Massey, 2006 (GI motility online)página com índice dos vídeos: http://www.nature.com/gimo/videos/index.html página principal: http://www.nature.com/gimo/index.html

http://www.nature.com/gimo/contents/pt1/fig_tab/gimo20_F3.html
a; Classical achalasia, showing a dilated esophageal body bird beak-like narrowing of lower esophageal sphincter (see Video 1). b; Vigorous achalasia showing diffuse spasm-like contractions in the esophageal body with closed lower esophageal sphincter (see Video 2). c; Diffuse esophageal spasm shows typical corkscrew appearance of the lower part of the esophagus (see Video 3). d: Midesophageal propulsion diverticulum with esophageal motility disorder (see Video 5). e; Normal peristaltic sequence for comparison with slow esophageal transit (see Video 6). f; Hypotensive (incompetent) esophageal peristalsis with slow esophageal transit through the esophagus (see Video 7). g; Gastroesophageal reflux (see Video 8).
“Physiology of oral cavity, pharynx and upper esophageal sphincter”, Massey, 2006 (GI motility online)página com índice dos vídeos: http://www.nature.com/gimo/contents/pt1/fig_tab/gimo20_F3.html
página principal: http://www.nature.com/gimo/index.html
Veja outros vídeos
interessantes sobre
acalasia online

A, Achados anatômicos na acalasia; B, imagem endoscópica e C, imagem radiográfica (bário)
ACALÁSIA - esvaziamento esofágico deficientePode ocorrer por ausência de peristalse esofágica e tônus
acima do normal do EEI/LOS
Distensão gástrica
(TLOSR ) não provoca relaxamento
do EEI
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

http://www.gastroatlas.com/index.aspx
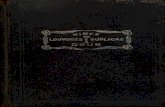
Lateral radiograph from a barium swallow in a patient with achalasia of the esophagus. There is lack of an opening of the gastroesophageal junction; however, the esophagus is not dilated. Irregular margins of the distal esophagus are the result of tertiary contractions. An air-fluid level is seen in the proximal esophagus. This case demonstrates that not all patients with achalasia of the esophagus have dilated, tortuous, and sigmoid esophagus.
Distensão gástrica
(TLOSR ) não provoca
o relaxamento
do EEI
ACALÁSIA - esvaziamento esofágico deficientePode ocorrer por ausência de abertura da junção gastro-
esofágica mas sem dilatação esofágica.

(A) Manometric tracing of swallow-induced peristalsis and lower oesophageal sphincter (LOS) relaxation in a healthy control subject. Note the absence of peristalsis and LOS relaxation in a tracing obtained from a patient with achalasia. (B) Representative tracings from muscle strips of the LOS of a control subject and a patient with achalasia. In control tissue, electrical field stimulation (EFS) results in frequency-dependent relaxations, mimicked by nitric oxide (NO). In contrast, EFS-induced relaxation is significantly impaired in achalasia, whereas the response to NO is similar to that in control tissue.
não relaxa com aestimulação
elétrica do nervo
mas relaxacom NO
tônus de repouso elevado
administração de NO na preparação
estimulações elétricas
Achados histológicos: diminuição significante do número de neurônios mioentéricos, especialmente dos nn.
inibidores oxinitrégicos (NO) no esôfago distal e no EEI. Possível causa: ganglionite mioentérica de origem auto-
imune ou vírus.
Registro normal de peristalse, relaxamento do EEI e experimentos com estimulação de tiras do EEI in vitro Registro de indivíduo com acalasia
revisão: Boeckxstaens, 2005 (Neurogastroenterology & Motility, Volume 17, Issue s1, Page 13-21, Jun 2005 )

Fisiologia do Sistema Digestório e aplicações clínicas relacionadas
ao esôfago e ao estômago Motilidade (tipos, funções e regulação):
Esofágica Disfunções (GERD e acalasia)
Gástrica (relaxamento receptivo, mistura e esvaziamento)
Disfunções (GERD)
Secreções gástricas Tipos de secreções (exócrinas e endócrinas ) Regulação das secreções Disfunções da secreção gástrica (úlceras pépticas)

Motilidade Gástricaas camadas musculares gástricas

Motilidade Gástrica
Período interdigestivo (jejum):complexo migratório mioelétrico
Período digestivo:recepção, mistura e esvazimento

Contractile activity in the stomach and small intestine of a fasting dog, showing the characteristic pattern of the migrating myoelectric complex. The ligament of Treitz marks the border between the duodenum and the jejunum. (From Itoh Z, Sekiguchi T: Scand J Gastroenterol Suppl 82:121, 1983.) Berne et al., 2004
Motilidade durante o jejum: complexo migratório mioelétrico (CMM, estômago Int. Grosso)

Motilidade Gástrica:
Período interdigestivo (jejum):complexo migratório mioelétrico
Período digestivo:recepção, mistura e esvazimento

O estômago pode ser dividido em:
Reservatório Reservatório gástrico gástrico
contraçõescontraçõestônicastônicas
BombaBomba gástrica gástricacontraçõescontrações
fásicasfásicas
BFundus
CorpusAntrum
Pylorus
A3 regiões anatômicas 2 regiões funcionais
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

BFundus
CorpusAntrum
Pylorus
A3 regiões anatômicas 2 regiões funcionais
O estômago como reservatório(relaxamento)
Reservatório gástrico
contraçõestônicas
Bomba gástricacontrações
fásicas
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Inhibitoryvagal fibre
Relaxation of gastric reservoir
ACH
Vaguscentre
NO + VIP (SNE)
1. Receptive relaxationMechanical
stimuli in the pharynx
O estômago como reservatórioRelaxamento gástrico é regulado principalmente por reflexos.
2. Adap tive relax ation
TensionreceptorsNutrients
CCK
3. Feedback relaxation
Nutrients
Distension
Três tipos de relaxamento podem ser observados:receptivo, adaptivo e relaxamento por feedback
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

esvaziamento gástrico: regulador do ritmo da digestão
bomba pilóricaB
Fundus
CorpusAntrum
Pylorus
A
Bomba gástricacontrações fásicas
Reservatório gástrico
contraçõestônicas
O estômago como reservatório
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Porque é importante entender como ocorre o esvazimento gástrico?
Há correlação direta entre a taxa de esvaziamento gástrico e
a ocorrência de úlceras duodenais:
de secreções basais de HCl durante a noite+
velocidade de esvaziamento gástrico=
maior ocorrência de úlceras duodenais

O transporte do conteúdo gástrico do reservatório para a região do antro (bomba antral) é causado por 2 mecanismos:
contrações tônicas e ondas peristálticas na região do corpo gástrico.
Tonic contraction
Peristaltic wave(Pump of the reservoir)Proximal antrum
Fluxo retrógrado do antro e fluxo para o reservatório
Pylorus
Accumulationof chyme
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

A função da bomba antral pode ser diferenciada em 3 fases: A: fase de propulsão, B: fase de esvaziamento, C: fase de retropulsão
A Fase de propulsão Contração do antro proximal (PA)
B Fase de esvaziamento Contração do antro medial (MA)
Propulsão do quimo para o antro proximal relaxado
+ contração duodenal
Fluxo transpilórico e retrógrado+ relaxamento duodenal
C Fase de retropulsão Contraçãodo antro terminal (TA)
Fluxo retrógrado em jato+ contração duodenal
PhasesA B C
10 sec
antroproximal
antro medial
antroterminal
Piloro
Duodeno
Pylorus
PA
fechado
aberto
MA
TA
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Líquidos e pequenas partículas saem do estômagomais rapidamente do que partículas grandes.
Essa discriminação é chamada de função de peneira
Fase de propulsão
Fluxo rápido de líquidos e de pequenas
partículas em suspensão e fluxo mais
lento para grandes partículas no antro
Antrum
Fase de esvaziamento
Esvaziamento de líquidos e pequenas partículas enquanto
grandes partículas são retidas no antro
terminal
Retropulsão de grandes partículas (moagem) e esvaziamento do antro
terminal
Fase de retropulsão
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Sólidos e líquidos do quimo gástrico sãoesvaziados com velocidades diferentes
fase de atraso
Tempo (min)
conteúdo viscoso
conteúdo líquido
Solids100
80
60
40
20
00 20 40 60 80 100 120
volu
me
Gás
tric
o (%
)
O esvaziamento de líquidos é exponencial. Já o esvaziamento de grandes particulas sólidas começa apenas após a trituração/moagem suficiente
(fase de atraso). Em seguida, o quimo viscoso é esvaziado de uma maneira quase linear.
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Videofluoroscopia de movimentos peristálticos durante o esvaziamento gástrico (bomba pilórica ou antral) de cão após a ingestão de substância não-calórica
(goma com viscosidade similar a catchup).
Esvaziamento gástrico(viscoso)
Videofluoroscopia de movimentos peristálticos durante o esvaziamento gástrico (bomba pilórica ou antral) de cão após a ingestão de salina.
Esvaziamento gástrico(líquido)
Repare na ocorrência de ondas segmentares no duodeno(não é possível ver sua luz) e na mistura que ocorre no antro
Videofluoroscopia de movimentos peristálticos durante o esvaziamento gástrico (bomba pilórica ou antral) de cão após a ingestão de gordura (ácido graxo de
cadeia longa)Esvaziamento gástrico (gordura) Reflexo enterogástrico (-)
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Esvaziamento gástrico: função de peneira
Fluxo rápido de líquidos e de pequenas partículas em
suspensão e fluxo mais lento para grandes partículas no antro
Esvaziamento de líquidos e pequenas partículas enquanto grandes partículas são retidas
no antro terminal
Retropulsão de grandes partículas (moagem) e esvaziamento do antro
terminal
Fase de propulsão
Antrum
Fase de esvaziamento Fase de retropulsão
Videofluoroscopia do esvaziamento gástrico de substâncias de diferentes tamanho (efeito de peneira) após ingestão de líquido
viscoso, não calórico e esferas sólidas em cão.
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Anastomose do jejuno no estômago: gastro-jejunostomia em Y de Roux
Videofluoroscopia do esvaziamento gástrico de salina após a anastomose do jejuno no estômago de cão (gastro-jejunostomia em Y de Roux)
repare a rapidez do esvaziamento, indicando a ausência do reflexo enterogástrico
Esvaziamento gástrico de salina no jejuno após Y de Roux
Videofluoroscopia do esvaziamento gástrico de gordura (ácido graxo de cadeia longa) após a anastomose do jejuno no estômago de cão
(gastro-jejunostomia em Y de Roux)
Repare a rapidez do esvaziamento, indicando a ausência do reflexo enterogástrico
Esvaziamento gástrico de gordura no jejuno após Y de Roux
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Diferença entre Roux em Y estômago-jejuno (demonstrado em cão) e o desvio de Fobi-Capella
Bypass proximal em Y de Roux
Gastroplastia com anel
Anastomose do jejuno no
estômago: gastro-jejunostomia em Y
de Roux em cão
Extraído, enquanto disponível, do seguinte website : http://www.wzw.tum.de/humanbiology/data/motility/34/?alt=english

Fisiologia do Sistema Digestório e aplicações clínicas relacionadas
ao esôfago e ao estômago Motilidade (tipos, funções e regulação):
Esofágica Disfunções (GERD e acalasia)
Gástrica (relaxamento receptivo, mistura e esvaziamento)
Disfunções (GERD)
Secreções gástricas Tipos de secreções (exócrinas e endócrinas ) Regulação das secreções Disfunções da secreção gástrica (úlceras pépticas)

Veja mais em: http://mcb.berkeley.edu/courses/mcb136/topic/Gastrointestinal/Secretion_in_GI-Tract/
SECREÇÕES GÁSTRICAS

Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill
Interações das secreções gástricas
mucous

A absorção da Vitamina B12
Revisão: Vitamin B12 (cobalamin) deficiency in elderly patients, Adrès et al, 2006
Veja a legenda desta Figura a seguir:

Fig. 1: Cobalamin metabolism and corresponding causes of deficiency. Causes of cobalamin deficiency are shown in blue. The metabolic pathway starts when (1) dietary cobalamin (Cbl), obtained through animal foods, enters the stomach bound to animal proteins (P). (2) Pepsin and hydrochloric acid (HCl) in the stomach sever the animal protein, releasing free cobalamin. Most of the free cobalamin is then bound to R-protein (R), which is released from the parietal and salivary cells. Intrinsic factor (IF) is also secreted in the stomach, but its binding to cobalamin is weak in the presence of gastric and salivary R-protein. (3) In the duodenum, dietary cobalamin bound to R-protein is joined by cobalamin–R-protein complexes that have been secreted in the bile. Pancreatic enzymes degrade both biliary and dietary cobalamin–R-protein complexes, releasing free cobalamin. (4) The cobalamin then binds with intrinsic factor. The cobalamin–intrinsic factor complex remains undisturbed until the distal 80 cm of the ileum, where (5) it attaches to mucosal cell receptors (cubilin) and the cobalamin is bound to transport proteins known as transcobalamin I, II and III (TCI, TCII and TCIII). Transcobalamin II, although it represents only a small fraction (about 10%) of the transcobalamins, is the most important because it is able to deliver cobalamin to all cells in the body. The cobalamin is subsequently transported systemically via the portal system. (6) Within each cell, the transcobalamin II–cobalamin complex is taken up by means of endocytosis and the cobalamin is liberated and then converted enzymatically into its 2 coenzyme forms, methylcobalamin and adenosylcobalamin (this process is shown in greater detail in Fig. 2). * Nitrous oxide, a general anesthetic, causes multiple defects in cobalamin use, most of which are intracellular and clinically relevant only in people who have low or borderline-low serum cobalamin levels.
Revisão: Vitamin B12 (cobalamin) deficiency in elderly patients, Adrès et al, 2006

Revisão: Vitamin B12 (cobalamin) deficiency in elderly patients, Adrès et al, 2006
A absorção da Vitamina B12

Revisão: Vitamin B12 (cobalamin) deficiency in elderly patients, Adrès et al, 2006
Alterações na absorção da Vitamina B12

Revisão: Vitamin B12 (cobalamin) deficiency in elderly patients, Adrès et al, 2006
Alterações na absorção da Vitamina B12

mucous
Interações das secreções gástricas
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

The protection provided to the mucosal surface of the stomach by the bicarbonate-containing mucus layer is known as the gastric mucosal barrier. In man, the mucus layer is about 0.2 mm thick. Buffering by the bicarbonate-rich secretions of the surface epithelial cells and the restraint to convective mixing caused by the high viscosity of the mucus layer allow the pH at the cell surface to remain near 7, whereas the pH in the gastric juice in the lumen is 1 to 2.
COX1: atividade ciclooxigenase da PGH2-sintase). Berne et al., 2004
secreção de muco e HCO3- pelas
células epiteliais e mucosas fluxo sangüíneo
camada mucosa (2mm)
Proteção mucosa
PGE2( prostaglandinas são citoprotetoras)
ACh(PS e SNE)

Mecanismos protetoresde defesa:
integridade da barreira mucosamuco e HCO3
-
(células mucosas epiteliais superficiais que possuem anidrase carbônica)
Mecanismos antioxidantes celulares(glutationa)
Fluxo sangüíneoFatores de crescimentohormônios: GH/IGF-1
PGE2
de reparação tecidual:restituição e replicação celular
(fatores de crescimento TGF, IGF-1 9GH)cicatrização (fibrinogênese)
A integridade do trato gastrointestinal superior depende do balanço entre fatores “hostis” e “protetores”
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

The protection provided to the mucosal surface of the stomach by the bicarbonate-containing mucus layer is known as the gastric mucosal barrier. In man, the mucus layer is about 0.2 mm thick. Buffering by the bicarbonate-rich secretions of the surface epithelial cells and the restraint to convective mixing caused by the high viscosity of the mucus layer allow the pH at the cell surface to remain near 7, whereas the pH in the gastric juice in the lumen is 1 to 2.
COX1: atividade ciclooxigenase da PGH2-sintase). Berne et al., 2004
secreção de muco e HCO3- pelas
células epiteliais e mucosas fluxo sangüíneo
camada mucosa (2mm)
Proteção mucosa
PGE2( prostaglandinas são citoprotetoras)
ACh(PS e SNE)
NSAIDs(drogas antiinflamatórias
não-esteróides)
inibição da COX 1
(constitucional)

prejuízo da defesa de mucosa
RESUMO DOS MECANISMOS PATOGÊNICOS DA ÚLCERA.destaque para os fatores que afetam a defesa de mucosa
(isolados ou em conjunto)
álcool (?)fumo
fatores genéticosestresse (?)
Summary of pathogenic mechanisms in ulcer disease. Several factors may alone or in combination cause peptic ulcer. Non-steroidal anti-inflammatory drugs and Helicobacter pylori impair mucosal defense. Exogenous factors, such as smoking, also impair mucosal defense. Genetic factors play a role in predisposing to ulcer disease. The role of stress in the genesis of ulcer remains controversial. http://www.gastroatlas.com/03/0307/0307002ALL.aspx (Não encontrado)

Lesões das mucosas gástrica e duodenal podem ocorrer quando efeitos deletérios do ácido gástrico superam as propriedades de defesa da mucosa.
Inibição de síntese endógena de prostaglandinas leva à diminuição do muco epitelial, da secreção de bicarbonato, do fluxo sangüíneo da mucosa, da proliferação epitelial e da
resistência da mucosa à injúria. Menor resistência da mucosa aumenta a incidência de danos por fatores endógenos tais como
o ácido, pepsina e sais biliares assim como fatores exógenos tais como NSAIDs (anti-inflamatórios não-esteródeis), etanol e outros agentes nocivos.
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

Helicobacter pylori
H. pylori is the etiologic factor in most patients with peptic ulcer disease and may predispose individuals to the development of gastric carcinoma. H. pylori colonizes in the human stomach. The method of H. pylori transmission is unclear, but seems to be person-to-person spread via a fecal-oral route. The prevalence of H. pylori in adults appears to be inversely related to the socioeconomic status. It is also thought that water is a reservoir for transmission of H. pylori.
The Nobel Prize in Physiology or Medicine for 2005:jointly to
Barry J. Marshall and J. Robin Warren(University of Western Australia Nedlands)
for their discovery of “The bacterium Helicobacter pylori
and its role in gastritis and peptic ulcer disease“
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

Helicobacter pylori and peptic ulcer disease. The assumption that H. pylori causes peptic ulcer disease is based on two lines of evidence. H. pylori has a higher prevalence in gastric and duodenal ulcer patients than in noninfected, healthy controls. Although H. pylori has a stronger association with duodenal ulcers than with gastric ulcers, H. pylori is the most common cause of gastric ulcers. Depending on the series, H. pylori has been associated from 50% to 80% of all gastric ulcers. NSAIDs–nonsteroidal anti-inflammatory drugs.
Extraído, enquanto disponível, de: http://www.gastroatlas.com/03/0306/0306001ALL.aspx
Infecção por H. pylori como provável causa de úlcera péptica
1ª evidência:
maior prevalência de H. pylori em
pacientes com úlceras gástricas e
duodenais do que em indivíduos não
infectados, controles saudáveis

Helicobacter pylori and peptic ulcer disease. The second major proof that H. pylori causes peptic ulcer disease is that when duodenal ulcers are healed by eradication of H. pylori (C), rates of recurrent ulcers are much lower than when ulcers are healed but H. pylori is not eradicated (A and B).
Infecção por H. pylori como provável causa de úlcera péptica
2ª evidência:
tratamento de úlcera duodenal que
erradica o H. pylori tem maior chance de
cura
1ª evidência:
maior prevalência de H. pylori em
pacientes com úlceras gástricas e
duodenais do que em indivíduos não
infectados, controles saudáveis
Extraído, enquanto disponível, de: http://www.gastroatlas.com/03/0306/0306001ALL.aspx

mucous
Interações das secreções gástricas
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

Secreção de pepsinogênio/pepsinafase gástrica e intestinal
Além de estímulos do SNE, estímulos hormonais: Gastrina, Secretina e CCK

Interações das secreções gástricas
mucous
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

(A) Drawing of a resting parietal cell with cytoplasm full of tubulovesicles and an internalized intracellular canaliculus. (B) An acid-secreting parietal cell. Tubulovesicles have fused with the membrane of the intracellular canaliculus, which is now open to the lumen of the gland and lined with abundant, long microvilli. (From Ito S: In Johnson RL, editor: Physiology of the
gastrointestinal tract, New York, 1981, Raven Press.)
Secreção ácida gástrica: a célula parietal
em “repouso” em atividade secretora

Mecanismos intracelulares de secreção ácida gástrica (célula parietal)

REGULAÇÃO DA SECREÇÃO ÁCIDA GÁSTRICA – receptores da cél. parietal
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

REGULAÇÃO DA SECREÇÃO ÁCIDA GÁSTRICA – receptores da cél. parietal
JEJUM(TÔNUS PS)
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

REGULAÇÃO DA SECREÇÃO ÁCIDA GÁSTRICA – receptores da cél. parietal
FASE CEFÁLICA(+ PS)
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

REGULAÇÃO DA SECREÇÃO ÁCIDA GÁSTRICA – receptores da cél. parietalFASE GÁSTRICA(fatores locais + PS)
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

Figure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003
tônus PS
SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
JEJUM(períodos
interdiges-tivos)

Figure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003
tônus PS
SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
JEJUM(períodos
interdiges-tivos)

SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
FASE
CEFÁLICA
tônus PSFigure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003

tônus PS
PS
SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
FASE
CEFÁLICA
Figure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003

PS
SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
FASE
GÁSTRICA
Figure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003

PS
SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
FASE
GÁSTRICA
Figure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003

PS
SECRETINApH do I.D.
SECREÇÃO ÁCIDA
GÁSTRICA: moduladores
FASE
INTESTINAL
Figure 1 Model for the regulation of gastric acid secretion. Shown are a parietal cell, an ECL cell, a D cell, and many of the important regulators of acid secretion. Parietal cells are stimulated by three main agonists: gastrin, histamine, and ACh. Gastrin binds to CCKB (gastrin/cholecystokinin-B)receptors on the parietal cell to evoke an increase in intracellular calcium; histamine binds to H2 receptors, which primarily signal through increased cAMP; ACh binds to M3 receptors to stimulate an increase in intracellular calcium. Parietal cell stimulation results in movement of H +/K+-ATPase pumps to the apical membrane to secrete acid. Histamine is released from ECL cells in response to gastrin stimulation as well as neuronal stimulation via PACAP ( pituitary adenylate cyclase-activating polypeptide). Somatostatin (Sst) released from D cells inhibits acid secretion by reducing ECL cell histamine release, blocking gastrin release, and directly inhibiting parietal cell acid secretion. Annual Review of Physiology March 2003, Vol. 65, pp. 383-400 Samuelson and Hinkle, 2003

REGULAÇÃO DA SECREÇÃO ÁCIDA GÁSTRICA – receptores da cél. parietal
Interesseno conhecimento
dos diferentes mecanismos reguladores
da secreção ácida gástrica: uso de drogas seletivas
para a reduçãodessa secreção
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

INIBIDORES DA SECREÇÃO ÁCIDA GÁSTRICA
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

INIBIDORES DA SECREÇÃO ÁCIDA GÁSTRICA
Olbe, Carlsson & Lindberg, 2003. Nature Reviews Drug Discovery 2, 132-139 (2003). Caso interesse, solicite uma cópia.http://www.nature.com/nrd/journal/v2/n2/index.html

mucous
Inibição das células parietais também inibe a secreção do FI (ex: atropina, vagotomia ou uso
de inibidor da secreção ácida por uso de inibidores de receptores
H2)
INIBIDORES DA SECREÇÃO ÁCIDA GÁSTRICA
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

mucousinibidores de bomba de próton inibem apenas a
secreção de ácido clorídrico
INIBIDORES DA SECREÇÃO ÁCIDA GÁSTRICA
Figura extraída de Vander, Sherman & Luciano, Human Physiology, Cap. 17, 2002, McGraw Hill

“Sem secreção de ácido, sem úlcera péptica” é um erro conceitual. A secreção excessiva de ácido é somente um dos fatores de patogênese da úlcera péptica. A diminuição da defesa de mucosa contra o ácido gástrico é outra causa importante. A integridade do TGI superior depende do balanço entre fatores “hostis” (como o ácido gástrico, H. pylori, anti-inflamatórios não-esteroidais e pepsina) e fatores de “proteção” (prostaglandinas, muco, bicarbonato e fluxo sangüíneo adequado) presentes na mucosa gastrointestinal.
A integridade do trato gastrointestinal superior depende do balanço entre fatores “hostis” e “protetores”
http://www.hopkins-gi.org/GDL_Disease.aspx?CurrentUDV=31&GDL_Disease_ID=197E00D5-029B-48B8-9A68-53077FCC9A0F&GDL_DC_ID=E25BDF77-223D-4B6F-9700-5BE41DBDE28B

Summary of pathogenic mechanisms in ulcer disease. Several factors may alone or in combination cause peptic ulcer. Non-steroidal anti-inflammatory drugs and Helicobacter pylori impair mucosal defense. Exogenous factors, such as smoking, also impair mucosal defense. Genetic factors play a role in predisposing to ulcer disease. The role of stress in the genesis of ulcer remains controversial.In Zollinger-Ellison (Z-E) syndrome (gastrinoma, raro) = acid and pepsin alone cause ulceration.
Extraído, enquanto disponível, de: http://www.gastroatlas.com/03/0307/0307002ALL.aspx
Resumo dos mecanismos patogênicos nas úlceras pépticasque podem ocorrer sozinhos ou combinados
úlcera
ácido e pepsinagastrinoma na síndrome
de Zollinger-Ellisonprejuízo
da defesa de mucosa
álcool (?)fumo
fatores genéticosestresse (?)

Veja mais a esse respeito na revisão abaixo (acesso pelo Portal CAPES/UFSC):
Reviews in Basic and Clinical Gastroenterology“
Control of Gastric Acid Secretion in Health and Disease
”Mitchell L. Schubert, , and David A. Peura‡
Gastroenterology, Volume 134, Issue 7, June 2008, Pages 1842-1860
(caso interesse, peça cópia à Profa. Cristina)

Profa. Dra. Cristina Maria Henrique PintoProfa. Associada II do Depto. Ciências Fisiológicas
CCB-UFSC
Fisiologia do Sistema Fisiologia do Sistema Digestório relacionada à Digestório relacionada à
Clínica MédicaClínica Médica
Veja as demais apresentações aquiVeja as demais apresentações aqui