IDENTIFICAÇÃO DE LESÕES PERIAPICAIS POR MEIO DE CINCO ...
33
PONTIFÍCIA UNIVERSIDADE CATÓLICA DE MINAS GERAIS Programa de Pós-graduação em Odontologia Eduardo Murad Villoria IDENTIFICAÇÃO DE LESÕES PERIAPICAIS POR MEIO DE CINCO MÉTODOS DE DIAGNÓSTICO POR IMAGEM Belo Horizonte 2013
Transcript of IDENTIFICAÇÃO DE LESÕES PERIAPICAIS POR MEIO DE CINCO ...

PONTIFÍCIA UNIVERSIDADE CATÓLICA DE MINAS GERAIS
Programa de Pós-graduação em Odontologia
Eduardo Murad Villoria
IDENTIFICAÇÃO DE LESÕES PERIAPICAIS POR MEIO DE CINCO
MÉTODOS DE DIAGNÓSTICO POR IMAGEM
Belo Horizonte
2013

Eduardo Murad Villoria
IDENTIFICAÇÃO DE LESÕES PERIAPICAIS POR MEIO DE CINCO
MÉTODOS DE DIAGNÓSTICO POR IMAGEM
Dissertação apresentada ao Programa de Pós-
graduação em Odontologia – Mestrado da
Pontifícia Universidade Católica de Minas
Gerais, como requisito parcial para obtenção
do título de Mestre em Odontologia, área de
concentração em Clínicas Odontológicas -
Ênfase: Radiologia Odontológica e
Imaginologia.
Orientador: Flávio Ricardo Manzi
Belo Horizonte
2013

FICHA CATALOGRÁFICA
Elaborada pela Biblioteca da Pontifícia Universidade Católica de Minas Gerais
Villoria, Eduardo Murad
V759i Identificação de lesões periapicais por meio de cinco métodos de
diagnóstico por imagem / Eduardo Murad Villoria. Belo Horizonte, 2011.
38f.: il.
Orientador: Flávio Ricardo Manzi
Dissertação (Mestrado) – Pontifícia Universidade Católica de Minas Gerais.
Programa de Pós-Graduação em Odontologia.
1. Doenças periapicais. 2. Dentes - Radiografia. 3. Radiografia dentária
digital. 4. Tomografia computadorizada de feixe cônico. I. Manzi, Flávio
Ricardo. II. Smith Neto, Perrin. III. Pontifícia Universidade Católica de Minas
Gerais. Programa de Pós-Graduação em Odontologia. IV. Título.
CDU: 616.314.18

Eduardo Murad Villoria
IDENTIFICAÇÃO DE LESÕES PERIAPICAIS POR MEIO DE CINCO MÉTODOS
DE DIAGNÓSTICO POR IMAGEM
Dissertação apresentada ao Programa de Pós-
graduação em Odontologia da Pontifícia
Universidade Católica de Minas Gerais, como
requisito parcial para obtenção do título de Mestre
em Odontologia. Área de Concentração: Clínicas
Odontológicas – Ênfase: Radiologia Odontológica e
Imaginologia.
COMPOSIÇÃO DA BANCA EXAMINADORA:
1- Prof. Dr. Antônio Paulino Ribeiro Sobrinho – UFMG
2- Profa. Dra. Helenice de Andrade Marigo Grandinetti – PUC Minas
3- Prof. Dr. Flávio Ricardo Manzi – PUC Minas
DATA DA APRESENTAÇÃO E DEFESA: 31 de maio de 2013
A dissertação, nesta identificada, foi aprovada pela Banca Examinadora
Belo Horizonte, 07 de agosto de 2013
Prof. Dr. Flávio Ricardo Manzi Prof. Dr. Martinho Campolina Rebello Horta
Orientador Coordenador do Programa de Pós-graduação
em Odontologia - Mestrado

AGRADECIMENTOS
Agradeço a todos que, de alguma forma, contribuíram para a realização deste
trabalho, especialmente:
À minha família, responsável por minha formação moral e intelectual, que
sempre teve toda dedicação e carinho para que eu chegasse até esta etapa da
minha vida.
Ao meu pai, German Eduardo Miguel Villoria, por todos os finais de semana
de praia com os amigos, pelos domingos de Maracanã, por sempre ter investido no
meu crescimento e por ser, além de pai, meu grande amigo.
À minha mãe, Maria Fernanda Guita Murad, e avós, Marilia Macedo Guita e
Clélia Maria Filonila Miranda de Miguel Villoria, por todo amor e atenção que
sempre dedicaram a mim e a minha irmã.
À minha irmã, Paula Murad Villoria, por ser minha grande amiga, estando ao
meu lado em todos os momentos da minha vida.
Aos meus amigos, pelo companheirismo e amizade, em especial ao meu
grande amigo, Daniel Marones, por ter me hospedado em sua casa mineira.
Ao meu grande amigo, John Monteiro Middleton, por ter me ajudado na
revisão textual deste trabalho.
À minha namorada, Julia Fernandes Travassos, por todos os momentos de
carinho e alegria que tornam minha vida mais feliz.
Aos meus amigos e professores, Kyria Spyro Spyrides e Spyro Nicolau
Spyrides, por quem tem carinho especial e devo grande parte do meu conhecimento
e crescimento como radiologista.
À minha amiga Juliana Noia, por ter sido uma grande professora nos meus
primeiros passos na Clínica Radiológica Spyro Spyrides.
Ao professor Alexandre M. Perez, por toda amizade e atenção que sempre
demonstrou em momentos importantes para meu crescimento profissional.
Ao professor Flávio Ricardo Manzi, pela amizade, conhecimento passado
em suas aulas e por ter aberto as portas de sua clínica para que fosse viável a
realização deste trabalho.
Aos meus colegas Luciano Andrei Francio e Christian Hellen Rodrigues
da Cunha, por toda a ajuda e companheirismo nesses dois anos de curso.

Aos meus colegas da Clínica Radiológica Spyro Spyrides e do Centro
Odontológico de Correas, especialmente ao Genival Marques e Juliano, que me
apoiaram nos momentos de ausência e viagens para Belo Horizonte.
A todos os colegas e professores do curso de mestrado em clínicas
odontológicas da Pontifícia Universidade Católica de Minas Gerais, por toda troca de
experiências, ajuda, amizade e pelo convívio leve e saudável que tivemos durante
esses dois anos.

RESUMO
O objetivo desta pesquisa foi avaliar cinco métodos de diagnóstico por imagem,
radiografia panorâmica digital, radiografia periapical convencional, radiografia
periapical digital por meio do sensor CCD (Charge Coupled Device) e PSP
(Photostimulable Phosphor Plates), além de tomografia computadorizada cone beam
(TCCB), na identificação de lesões periapicais associadas a dentes anteriores e
posteriores da arcada inferior. Para a realização da presente pesquisa, foram
selecionadas mandíbulas humanas secas, apresentando 10 raízes/alvéolos de
dentes anteriores e 20 raízes/alvéolos de dentes posteriores. Foram realizadas,
previamente, as radiografias panorâmicas digitais, periapicais convencionais e
digitais, e TCCB, com o intuito de descartar regiões que apresentassem lesões
periapicais ou condições semelhantes, formando também o grupo controle.
Posteriormente, foram produzidas lesões periapicais com brocas esféricas de
diferentes diâmetros, de maneira progressiva, permitindo que as lesões
apresentassem tamanhos diferentes. Os diferentes métodos de diagnóstico por
imagem foram realizados após cada fase e analisados por 2 radiologistas calibrados.
Por meio do teste de Kappa, verificou-se boa concordância na maioria das
avaliações intra e inter-examinador. Por meio dos gráficos de curva ROC e avaliação
da sensibilidade, especificidade e acurácia, verificou-se que a TCCB obteve os
melhores resultados na grande maioria das imagens, principalmente em lesões
produzidas com a broca 6, quando comparado com os outros métodos de imagem
utilizados. Com base nos dados obtidos, pode-se concluir que a TCCB é o método
de imagem mais confiável para o diagnóstico correto de lesões periapicais,
principalmente aquelas de menores dimensões.
Palavras chave: Lesão periapical. Radiografia convencional. Radiografia digital.
Tomografia computadorizada cone beam.

ABSTRACT
The aim of this study was to evaluate five methods of diagnostic imaging, digital
panoramic radiography, conventional periapical radiograph, digital periapical
radiograph CCD (Charge Coupled device) and phosphor plate (PSP), and cone
beam computed tomography (CBCT ) in identification of periapical lesions. Some
dried human mandibles were used in order to carry out this research, showing 10
anterior and 20 posterior roots/dental alveolus. Digital panoramic radiographs,
conventional and digital periapical and CBCT were performed prior to discard regions
that presented periapical lesions or similar conditions, also forming the control group.
Later periapical lesions were produced with carbide round bur of different diameters
in a progressive manner, allowing the lesions to present different sizes. The different
methods of diagnostic imaging were performed after each phase and analyzed by 2
calibrated radiologists. When using the Kappa test, good agreement in most
evaluations intra and inter-examiner was found. Through the ROC curve graphs and
evaluation of sensitivity, specificity and accuracy, it was found that the CBCT
achieved the best results in most images, especially in lesions produced with the
round bur size 6, when compared with other imaging methods used. Based on the
data, it can be concluded that CBCT imaging is the most reliable method for the
accurate diagnosis of periapical lesions, especially those of smaller dimension.
Keywords: Periapical lesion. Conventional radiograph. Digital radiograph. Cone beam
computed tomograph.

SUMÁRIO
1 INTRODUÇÃO ....................................................................................................... 15 2 OBJETIVO ............................................................................................................. 17 3 MATERIAL E MÉTODOS ...................................................................................... 18 3.1 Preparo da amostra ........................................................................................... 18 3.2 Aquisição das imagens ..................................................................................... 19 3.2.1 Radiografias Periapicais ................................................................................ 20 3.2.2 Radiografia Panorâmica Digital .................................................................... 21 3.2.3 Tomografia Computadorizada Cone Beam .................................................. 21 3.3 Avaliação das imagens ..................................................................................... 22 3.4 Testes estatísticos ............................................................................................ 24 4 ARTIGO ................................................................................................................. 26 5 CONSIDERAÇÕES FINAIS ................................................................................... 35 REFERÊNCIAS ......................................................................................................... 36

15
1 INTRODUÇÃO
As lesões periapicais são causadas, na maioria das vezes, por reações
inflamatórias decorrentes da necrose pulpar e contaminação bacteriana do canal
radicular. O diagnóstico correto dessas lesões é essencial para determinar a seleção
de um efetivo protocolo terapêutico para o controle da infecção endodôntica
(ESTRELA et al., 2008).
Desde a descoberta dos raios X por Röntgen, filmes fotográficos/radiográficos
têm sido utilizados como detectores de fótons de raios X na radiografia oral. A
interpretação dessas imagens radiográficas continua sendo a principal ferramenta
para o diagnóstico de anomalias ósseas em maxila e mandíbula. As radiografias
periapicais convencionais são as mais comumente utilizadas para avaliação da
região periapical (FRIEDLANDER et al., 2002; LOFTHAG-HANSEN et al., 2007;
CARVALHO et al., 2007; COSTA et al., 2009). Por sua vez, as radiografias
panorâmicas cada vez mais fazem parte do cotidiano do cirurgião dentista, estando
presentes não só nos grandes centros de diagnóstico por imagem, mas também em
muitos hospitais e faculdades do país.
As características radiográficas das lesões periapicais são, primeiramente, a
destruição da lâmina dura da região do ápice radicular e, seguida da extensão da
lesão e posterior destruição do osso trabecular, conferindo um aspecto radiolúcido à
imagem na região (BARBAT; MESSER, 1998). A sobreposição de estruturas ósseas,
no entanto, pode prejudicar a visualização da imagem radiolúcida periapical. Bender
e Seltzer demonstraram que lesões periapicais podem ser visualizadas
radiograficamente apenas quando a rarefação óssea atinge o osso cortical
vestibular, lingual ou ambos, sendo imperceptíveis quando confinadas apenas em
osso trabecular (BENDER; SELTZER, 1961).
As radiografias convencionais, tanto periapical quanto panorâmica, vêm
sendo substituídas pelo sistema digital, que também fornece imagem bidimensional
e sobreposição de estruturas adjacentes. Porém, a radiografia digital possui as
vantagens de uma imediata geração de imagens, redução de 50% na exposição à
radiação, eliminação do processamento químico (revelador e fixador), além de
permitir a manipulação da imagem (ampliação e alteração de brilho e contraste) e o
armazenamento e envio das mesmas para outros profissionais (PAURAZAS et al.,

16
2000; BARBAT; MESSER, 1998), aumentando a capacidade de visualização e
diagnóstico dos profissionais envolvidos.
Devido às limitações da imagem radiográfica no que concerne à característica
bidimensional da imagem e a sobreposição de estruturas adjacentes, Tachibana e
Matsumoto, em 1990, foram uns dos primeiros autores a pesquisar sobre o uso de
tomografias computadorizadas em endodontia, a fim de conseguir informações não
encontradas por meio dos exames radiográficos. Cabe salientar, todavia, que a
tomografia computadorizada possui desvantagens, como, por exemplo, altas doses
de radiação, alto custo do exame e o fato de que o uso do aparelho restringe-se a
centros especializados (PATEL et al., 2008; LOFTHAG-HANSEN et al., 2007).
Frente a isso, a TCCB foi desenvolvida para o mercado odontológico com o objetivo
de proporcionar a visualização das estruturas ósseas e dento-alveolares em três
dimensões, e suas relações com estruturas anatômicas, empregando menor dose de
radiação (JORGE et al., 2008). A dose de radiação proporcionada pela TCCB é
menor, principalmente quando o exame é realizado com campo de visão ou “Field of
View” (FOV) reduzido, já que a colimação do feixe limita a radiação para a região de
interesse, equivalendo à dose de duas radiografias periapicais. Para patogenias
endodônticas, dentre as quais se incluem as lesões periapicais, recomenda-se a
utilização do FOV limitado e voxel isotrópico de menor dimensão, pois promovem
melhor resolução da imagem para visualização de alterações no espaço do
ligamento periodontal que mede, aproximadamente, 200μm (SCARFE, 2011).
Existem, entretanto, alguns métodos de diagnóstico por imagem capazes de
identificar a presença de lesões periapicais de maneira precisa.

17
2 OBJETIVO
O presente trabalho de pesquisa teve como objetivo avaliar, e comparar, a
precisão na identificação de lesões periapicais, de diferentes tamanhos, nas
imagens de radiografias periapicais convencionais e digitais (CCD e PSP),
radiografias panorâmicas digitais, além de tomografia computadorizada cone beam.

18
3 MATERIAL E MÉTODOS
O presente trabalho foi aprovado pelo comitê de ética da PUC Minas (CAAE:
07790512.9.0000.5137).
3.1 Preparo da amostra
O grupo do experimento foi composto por 30 alvéolos (10 em dentes
anteriores e 20 em posteriores) selecionados a partir de mandíbulas secas
pertencentes ao laboratório de radiologia da PUC Minas.
Foram realizadas, previamente, as radiografias panorâmicas, periapicais
convencionais e digitais, e a tomografia computadorizada cone beam, com o intuito
de descartar regiões que apresentassem lesões periapicais ou condições
semelhantes, formando também o grupo controle.
As mandíbulas foram imersas por 90 minutos em recipiente contendo água e
detergente líquido, a fim de reduzir a tensão superficial do osso e aumentar a
absorção de água, facilitando a extração dos dentes presentes (PATEL et al., 2008).
Os dentes foram removidos e recolocados após cada preparo do alvéolo.
Foram produzidas artificialmente lesões periapicais de diferentes tamanhos,
em cada alvéolo, por meio de brocas carbide esféricas de aço para baixa rotação,
com haste longa, de números 6 (1,8 mm de diâmetro) e 10 (2,7mm de diâmetro). O
limite de penetração foi determinado pelo próprio tamanho da ponta ativa da broca
(ALMEIDA et al., 2001). Foi realizada mais uma perfuração rompendo a cortical
vestibular, o que acarretou em quatro fases distintas (Figuras 1 e 2). Após cada
preparo, as mandíbulas foram submetidas aos exames radiográficos e tomográficos.
Os diferentes tamanhos de lesões correspondem às seguintes fases:
a) fase inicial ou A (ausência de lesão);
b) fase B (lesão produzida com a broca 6);
c) fase C (lesão produzida com a broca 10);
d) fase D (lesão rompendo cortical vestibular).

19
Figura 1: Brocas carbide esféricas de aço, com haste longa, em baixa rotação
(A); Momento da produção da lesão periapical no alvéolo do dente 36 (B).
Fonte: Fotos do autor
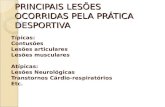
Figura 2: Alvéolo íntegro sem preparo (A); Setas indicando alvéolo após
produção da lesão periapical com a broca 6 (B), após produção da lesão
periapical com a broca 10 (C) e rompimento da cortical óssea vestibular (D).
Fonte: Fotos do autor
3.2 Aquisição das imagens
As mandíbulas foram submetidas aos seguintes métodos de diagnóstico por
imagem: radiografias periapicais convencionais, radiografias periapicais digitais
(CCD e PSP), radiografias panorâmicas digitais, além de tomografia
computadorizada cone beam. Todos estes exames foram realizados antes e após
cada preparo dos alvéolos.

20
3.2.1 Radiografias Periapicais
Para as radiografias periapicais, foi utilizado o aparelho radiográfico Kodak
2200 Intraoral X-Ray System® (Carestream Health, Inc.), operando com 60 Kv e 7
mA. No método convencional, foram utilizados filmes radiográficos Kodak Insight®
(Carestream Health, Inc.) tamanho 2, e os tempos de exposição foram de 0,3 e 0,36
segundos, para as regiões de dentes anteriores e posteriores, respectivamente. O
processamento dos filmes convencionais foi realizado logo após a exposição aos
raios X em processadora automática A/T2000 XR® (Air Techniques), num tempo
total, de seco a seco, de cinco minutos com as soluções reveladoras e fixadoras
Kodak Automixer® (Carestream Health, Inc.) novas. No método digital sistema CCD
foi utilizado o sensor digital Kodak RVG 5100® (Carestream Health, Inc.) tamanho 1,
com 14pl/mm de resolução espacial, e no método digital PSP, o sistema Scan-X Due
(Air Techniques), com 22 pl/mm de resolução espacial. Os tempos de exposição
foram de 0,15 e 0,18 segundos, para as regiões de dentes anteriores e posteriores,
respectivamente. O cilindro localizador foi posicionado sempre perpendicular ao
filme, sensor e placa de fósforo, e estes paralelos ao objeto (dente). As mandíbulas
ficaram estáveis com o auxílio de uma base de plástico suportada por um tripé
fotográfico, que permitiu manter uma distância padrão (40 cm) entre fonte de raios X
e filme, sensor e placa de fósforo. Para simular os tecidos moles do paciente, foi
utilizada uma placa de acrílico com 10 mm de espessura (Figura 3).
Figura 3: Mandíbula posicionada em cima de uma base de plástico. Cilindro localizador do aparelho periapical posicionado perpendicularmente ao sensor
CCD e dentes, e estes paralelos entre si. Presença da placa de acrílico para simular tecidos moles.
Fonte: Foto do autor

21
3.2.2 Radiografia Panorâmica Digital
As radiografias panorâmicas digitais foram realizadas por meio do aparelho
radiográfico Kodak 9000C 3D® (Carestream Health, Inc.), operando com 60 Kv, 2
mA e 14,1 segundos de exposição. Para auxiliar no posicionamento das mandíbulas,
e aquisição de imagens, uma base de plástico foi utilizada com o objetivo de
proporcionar a padronização do posicionamento das mandíbulas e permitir que
mesmas ficassem adequadamente posicionadas na camada de corte do aparelho.
Este dispositivo foi adaptado a um tripé fotográfico e, após o posicionamento da
mandíbula, foi preenchido com 750 ml de água, com o intuito de promover uma
atenuação dos feixes de raios X e simular a presença de tecido mole (Figura 4). Este
tipo de atenuação foi baseado no estudo realizado por Butterfield, Dagenais e Clokie
(1997).
3.2.3 Tomografia Computadorizada Cone Beam
Para as tomografias computadorizadas cone beam, foi utilizado o aparelho
Kodak 9000C 3D® (Carestream Health, Inc.), operando com 62 Kv, 10 mA e 10,8
segundos de exposição. O escaneamento foi realizado com 5,0 cm x 3,7cm de
colimação (FOV). O conjunto de dados foi exportado em formato DICOM, e o
tamanho do voxel isotrópico foi de 76 x 76 x 76 μm. A imagem volumétrica foi
analisada em cortes com 0,076mm de espessura. Para o posicionamento das
mandíbulas no aparelho, foi utilizado o mesmo suporte de plástico descrito
anteriormente e utilizado para a aquisição das imagens de radiografias panorâmicas
(Figura 4).

22
Figura 4: Aparelho Kodak 9000 3D (TCCB e Panorâmico). Mandíbula posicionada dentro de um recipiente com 750 ml de água para mimetizar
tecidos moles.
Fonte: Foto do autor
3.3 Avaliação das imagens
Dois cirurgiões dentistas especialistas em Radiologia odontológica e
Imaginologia analisaram separadamente todas as imagens radiográficas e
tomográficas de maneira independente. O estudo foi do tipo duplo-cego, ou seja, os
observadores não conheciam a condição de cada dente/alvéolo. Apenas o
pesquisador responsável pela realização dos preparos teve acesso a essas
informações.
Para interpretação das radiografias convencionais foi utilizado negatoscópio
de luz fria com máscaras de cartolina preta no tamanho das imagens, sendo
permitido o uso de lupas. A interpretação das imagens digitais e tomografia
computadorizada cone beam foi realizada diretamente no software KDIS - Kodak
Dental Imaging Software® (Carestream Health, Inc.), sendo permitido o uso de todos
os recursos disponíveis, os quais foram devidamente explicados aos observadores.
Foi utilizado computador com placa gráfica GeForce 9500 GT® (Nvidia Corporation)
e monitor LED LG Flatron E2241® (LG Electronics), com resolução de 1920x1080
pixels e os níveis de brilho e contraste do monitor fixados em sua configuração pré-
estabelecida. A presença de imagem radiolúcida associada ao ápice radicular, com a

23
descontinuidade da lâmina dura, foi indicativa da presença de lesão periapical
(Figuras 5 e 6).
Figura 5: Setas indicando lesão periapical na imagem digital do dente 36, por
meio do sensor CCD (A), e em incisivos inferiores, por meio do sistema PSP.
Radiografia panorâmica digital, demonstrando o painel de controle com
ferramentas para manipulação da imagem (C).
Fonte: Fotos do autor
Figura 6: Setas indicando lesão periapical, com rompimento da cortical óssea
vestibular, em plano axial (A) e corte oblíquo (B) de TCCB.
Fonte: Fotos do autor
Com a finalidade de oferecer as mesmas condições aos observadores, todos
utilizaram os mesmos recursos para avaliação das imagens, ou seja, o mesmo
negatoscópio, ambiente, computador e monitor.

24
As imagens radiográficas e tomográficas foram interpretadas de maneira
aleatória, devendo todos os observadores avaliar todas as imagens ao menos duas
vezes e em momentos distintos. Para evitar comprometimento em virtude de fadiga
visual, foi limitada a análise de 50 imagens por dia.
Os examinadores avaliaram cada tipo de imagem em dias alternados, para
que não houvesse comparação entre as técnicas empregadas. A avaliação foi
realizada atribuindo-se os seguintes escores: 1- lesão certamente ausente; 2 - lesão
provavelmente ausente; 3 - lesão provavelmente presente; 4 - lesão certamente
presente; 5 - impreciso.
3.4 Testes estatísticos
Os dados obtidos com as interpretações pelo método comparativo foram
submetidos a análises estatísticas, visando à determinação dos valores relativos à
reprodutibilidade, acurácia, sensibilidade e especificidade, para as modalidades de
aquisição de imagens radiográficas em estudo.
Wenzel (1998) explicou que a reprodutibilidade implica na precisão do
método, portanto, uma modalidade de aquisição de imagens é considerada precisa,
se os diagnósticos fornecidos com suas radiografias forem consistentes. A avaliação
da precisão investiga as variações inter e intra-examinador. Nesta pesquisa
experimental, foi executada a estatística Kappa de Cohen, com ponderação linear,
para as mensurações de concordância inter e intra-examinador.
Os valores verdadeiro negativo (correta identificação das imagens sem lesão -
especificidade), verdadeiro positivo (correta identificação das imagens com a
presença de lesões periapicais - sensibilidade), falso positivo, falso negativo e a
acurácia foram calculados por meio da análise da área sob a curva ROC (Receiver
Operating Characteristic) utilizando o software BioEstat 5.0 (Belém, Brasil) para cada
tipo de imagem.
As imagens radiográficas e tomográficas de cada modalidade de aquisição
(radiografia panorâmica digital, radiografias intra-oral convencional, CCD, PSP e
tomografia computadorizada cone beam) foram comparadas. Nos gráficos ROC, as
curvas são diferenciadas pelas áreas.
No gráfico ROC, o eixo das ordenadas representa a sensibilidade e o eixo das
abscissas, o inverso da especificidade. O cálculo do balanço entre os índices de

25
verdadeiro-positivos e falso-positivos é obtido pela determinação da área sob a
curva ROC, que representa uma expressão do poder discriminativo global que um
teste de diagnóstico possui e constitui uma boa medida sumária de exatidão
(HANLEY; MCNEIL, 1982; WENZEL; VERDONSCHOT, 1994). O valor mínimo da
área sob a curva ROC é de 0,50, sendo a representação gráfica de uma reta em 45º.
Isso acontece se as capacidades de previsão da modalidade não forem superiores
ao puro acaso, ou seja, quando o método não possui qualquer capacidade
discriminativa. Então, o índice de verdadeiro-positivos é igual ao índice de falso-
positivos. O valor máximo é igual a 1 nas situações em que se obtêm 100% de
verdadeiro-positivos e 0% de falso-positivos. O melhor desempenho é indicado por
uma curva que é mais elevada e voltada para a esquerda, no espaço ROC
(HANLEY; MCNEIL, 1982).
Foi realizado o teste Q de Cochran, com nível de significância de 5%.

26
4 ARTIGO
Identification of Periapical Lesions by Using Five Image Diagnosis
Methods.
O artigo será submetido ao Journal of Endodontics. (Qualis: A1)
Endereço eletrônico para acesso às normas do periódico:
http://www.jendodon.com

27
Abstract Introduction: The correct diagnosis of periapical lesions is crucial to determine the most
effective therapeutic protocol for control of endodontic infection. The objective of this study
was to assess and compare five image diagnosis methods used for identification of periapical
lesions, which artificially produced periapical lesions. Materials and Methods: Dried human
mandibles were selected, all presenting 10 roots/alveoli of anterior teeth and 20 roots/alveoli
of posterior teeth. Digital panoramic radiography, conventional and digital periapical
radiography (CCD and PSP), and cone beam computed tomography (CBCT) were previously
carried out to form the control group. Then, periapical lesions were progressively produced
with spherical drills of different diameters, thus creating lesions of different sizes (1.8 mm,
2.7 mm, and buccal cortical bone rupture). The different image diagnosis methods were
performed after each phase and analysed by two properly trained radiologists. Data were
assessed by using the Kappa test and ROC curve graphs. Significance level was set at 5%.
Results: Kappa test showed good intra- and inter-rater reliabilities regarding the evaluations.
ROC curve graphs showed that CBCT produced the best results in the majority of the images,
mainly in lesions produced with #6 drill. Conclusion: Based on the data obtained, one can
conclude that CBCT is the most reliable image diagnosis method for identification of small
periapical lesions.
Keywords Periapical lesion, conventional radiography, digital radiography, cone beam computed
tomography.
Introduction The interpretation of radiographic images continues to be the main tool for diagnosis
of osseous anomalies in the maxillo-mandibular complex. Conventional periapical
radiographs are the most commonly used for evaluation of the periapical region (1-4), but
superposition of bone structures can impair visualisation of the periapical radiolucent image,
mainly initial lesions.
Conventional radiographs, both periapical and panoramic, has been replaced by digital
systems as these have the advantage of immediately generating images, reducing radiation
exposure by 50%, eliminating chemical process, and allowing image to be manipulated,
stored and sent to other practitioners (5, 6), thus increasing the practitioner’s capacity to
visualise the image and find a diagnosis.
Tachibana & Matsumoto, in 1990, were the pioneers in the research on the use of
computed tomography in endodontics. However, this method has also disadvantages, such as
high radiation doses and high exam cost (2, 7). In view of this, CBCT was developed for the
dentistry market in order to provide visualisation of bone and alveolar structures in three
dimensions, as well as of their relationships with other anatomical structures, using a low
radiation dose (8). The radiation dose provided by CBCT is lower, mainly when the exam is
performed with a reduced field of view (FOV). To improve the visualisation of endodontic
diseases, such as periapical lesions, one recommends the use of limited FOV and small
isotropic voxel (9).
The objective of the present study was to assess and compare five image diagnosis
methods for identification of periapical lesions, which were simulated in several stages and/or
sizes.

28
Materials and Methods
Sample Preparation The present work was approved by the local ethics research committee at the
Pontifical Catholic University of the State of Minas Gerais. The experimental group consisted
of 30 roots/alveoli (10 anterior teeth and 20 posterior teeth) selected from dried human
mandibles. Digital panoramic radiography, conventional and digital periapical radiography
(CCD and PSP), and cone beam computed tomography were previously performed in order to
disregard regions presenting periapical lesions or similar conditions, which also formed the
control group. Mandibles were immersed in a recipient with water and liquid detergent for 90
minutes in order to facilitate the extraction of teeth (7). Teeth were then removed and integrity
of alveolar bone was checked.
Periapical lesions of different sizes were artificially produced in each alveolus by
means of spherical carbide burs, numbers 6 (1.8 mm diameter) and 10 (2.7 mm diameters), at
low rotation. Penetration limit was determined by the diameter of the head (10). Another
perforation was performed breaking the buccal cortical bone, resulting in four different phases
(Figure 1). After each preparation, the mandibles were submitted to radiographic and
tomographic examinations.
Figure 1. Healthy alveolus without preparation (A); Arrows indicating alveolus following production of
periapical lesion with #6 bur (B), following production of periapical lesion with #10 bur (C), and rupture of the
buccal cortical bone (D).
Image Acquisition and Evaluation To obtain the periapical radiographs, a Kodak 2200 Intraoral X-Ray System
®
(Carestream Health, Inc., Rochester, NY, USA) was used at 60 Kv and 7 mA. In the
conventional method, size #2 radiographic films (Kodak Insight®, Carestream Health, Inc.,
Rochester, NY, USA) were used in exposure times of 0.3 and 0.36 seconds in the anterior and
posterior tooth, respectively. With regard to the digital method, a size#1 CCD sensor (Kodak
RVG 5100®,
Carestream Health, Inc. Rochester, NY, USA) is used to allow a spatial
resolution of 14 lp/mm, whereas a ScanX Due digital system (Air Techniques) was used to
allow a spatial resolution of 22 lp/mm. Exposure times were set at 0.15 and 0.18 seconds for
anterior and posterior teeth, respectively. The parallelism technique was performed and the
mandibles were made stable with the aid of a plastic box supported by a camera tripod, thus
allowing a standard distance to be kept between X-ray source and sample surface. An acrylic
plate of 10 mm thickness was used to simulate the soft tissues (Figure 2).
Digital panoramic radiographs were taken by using the Kodak 9000C 3D® system
(Carestream Health, Inc., Rochester, NY, USA) operating at 60 Kv and 2 mA in an exposure

29
time of 14.1 seconds. A plastic box with rods was used for positioning of the mandibles and
image acquisition, which allowed stability of them for standardisation and their proper
positioning within the detail layer. Next, the plastic box was filled with water (750 ml) in
order to promote attenuation of X-ray beams and simulate the presence of soft tissue (11)
(Figure 2).
With regard to cone beam computed tomography, the Kodak 9000C 3D® system
(Carestream Health, Inc., Rochester, NY, USA) was used at 60 Kv and 10 mA in an exposure
time of 10.8 seconds. Scanning was performed with FOV of 5.0 cm x 3.7 cm and isotropic
voxel size of 76 μm. The mandibles were positioned by using the same plastic box for
acquisition of panoramic images.
Figure 2. Mandibles positioned within a plastic box supported by camera tripod. Acrylic plate of 10 mm
thickness was used to simulate soft tissues in the periapical radiography (A), and plastic box filled with 750 ml
of water to simulate soft tissues in the panoramic radiography and CBCT (B).
Two surgeon dentists expert in dental radiography and imaginology analysed all the
images separately and independently.
For interpretation of the conventional radiographs, a cold light negatoscope with a
black cardboard mask of the same size as the images was used. The use of magnifying glass
was also allowed. Digital and tomographic images were visualized by using the Kodak Dental
Imaging Software (Carestream Health, Inc., Rochester, NY, USA.)
The examiners evaluated each type of image in alternate days so that no comparison
could be made between the techniques used. The presence of radiolucent image related to root
apex, with discontinuity of lamina dura, was indicative of presence of periapical lesion.
Statistical Tests Intra- and inter-rater reliabilities were assessed by using Kappa coefficient. The area
under the ROC curve was calculated by using the BioEst 5.0 software (Belém, Brazil). The
values for true negative, true positive, false negative, false positive and accuracy were
calculated. Cochran’s Q test was performed at significance level of 5%.
Results By using the ROC analysis, one observed that the images of anterior teeth obtained the
from digital panoramic radiography and conventional film presented higher area values
indicating rupture of the buccal cortical bone and smaller area values indicating lesions
artificially produced with #6 burs. Digital panoramic radiography had 100% of true-positive
results for rupture lesions, but a low area value of 0.55 was observed for lesions artificially

30
produced with #6 burs, with low sensitivity and high specificity (high false negatives). In the
digital periapical radiography (CCD and PSP), the area values for lesions artificially produced
with #10 burs and rupture of the buccal cortical bone were found to be equal (0.95), that is,
high rate of true positives. With regard to the CBCT, area values were found to be high for all
lesion sizes (Table 1), which demonstrates high accuracy.
In the posterior teeth, small area values were observed in digital panoramic images and
conventional film in those cases of lesions artificially produced with #6 burs. However, one
can observe that the value of the area becomes higher as the size of the lesion increases.
CBCT had the same are value (0.85) for all lesion sizes (Table 1).
Table 1. Values of the ROC curve areas for lesion sizes in anterior and posterior teeth according to the different
image diagnosis methods used.
Image method Panoramic Film CCD PSP CBCT
#6 bur (a) 0.55* 0.65* 0.85 0.75 0.90
#10 bur (a) 0.85 0.8 0.95 0.95 0.95
Rupture (a) 1 0.95 0.95 0.95 0.95
#6 bur (p) 0.70* 0.65* 0.75 0.8 0.85
#10 bur (p) 0.85 0.8 0.75 0.8 0.85
Rupture (p) 0.95 0.9 0.8 0.85 0.85
(a) Anterior teeth; (p) posterior teeth
Areas followed by (*) show statistic differences compared to controls (Cochran’s Q at significance level of 5%)
With regard to the dental regions studied, the images obtained with conventional film
and digital panoramic radiography showed statistically significant difference compared to
controls (p < 0.05) for lesions artificially produced with #6 burs.
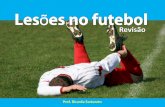
Because the ROC curve graphs regarding the different lesion sizes showed the worst
results for lesions artificially produced with #6 burs, the different image diagnosis methods
were compared to each other only for this case (Figure 2). ROC analysis of CBCT showed a
higher number of true-positive results in both anterior and posterior teeth. By comparing the
images from conventional and digital (CCD and PSP) intra-oral radiographs, it was found that
digital systems presented greater areas during evaluation. It is also observed that evaluation of
panoramic images had a curve excessively towards the left, but with low values (high false
negatives), similar to that of conventional intra-oral images.
Figure 3. ROC curves for analysis of the images obtained from digital panoramic radiographs (A), film (B),
CBCT (C) CCD (D) and PSP (E) for lesions artificially produced with #6 burs in anterior and posterior teeth.
Kappa coefficient was used to assess intra- and inter-rate reliabilities for lesions
artificially produced with #6 bur. Intra-rater reliability was found to be good in the majority of
Roc Curve (Anterior Teeth) Roc Curve (Posterior Teeth)
Specificity Specificity

31
image methods. Excellent reliability was also found in digital panoramic radiographs, digital
intra-oral radiographs (PSP), and CBCT for anterior teeth as well as in conventional intra-oral
radiographs, digital intra-oral radiographs (CCD), and CBCT for posterior teeth. Inter-rater
reliability was found to be good in the majority of the image methods, except the conventional
intra-oral images of posterior teeth, which presented excellent reliability (Table 2).
Table 2. Intra- (1-1) and (2-2) and inter-rate (1-2) reliabilities (weighted Kappa coefficient) of each image
diagnosis method for lesions artificially produced with #6 burs in anterior and posterior teeth.
Images 1-1* 2-2* 1-2* 1-1** 2-2** 1-2**
Panoramic 0.75 0.85 0.80 0.76 0.74 0.72
Film 0.75 0.70 0.75 0.90 0.71 0.85
CCD 0.78 0.79 0.75 0.70 0.84 0.61
PSP 0.84 0.70 0.77 0.75 0.72 0.71
CBCT 0.93 0.87 0.80 0.91 0.72 0.80
* Anterior teeth ** Posterior teeth
Discussion In the present study, CBCT always had high values of accuracy. The greatest
difference compared to the other methods was in relation to the lesions artificially produced
with #6 burs (1.8 mm), a finding similar to that reported by other authors (12, 13, 14).
The use of a device with reduced FOV and small voxel (76 μm) provides a better
image resolution for visualisation of the changes in the periodontal ligament space, which
measures approximately 200 μm, compared to other systems with larger voxel size and FOV
(9). In fact, an isotropic voxel of 76 μm provides a spatial resolution of 6.5 lp/mm, which is
inferior to that of the conventional film (approximately 20 lp/mm) and digital systems (8 to 20
lp/mm). However, the capacity of this technology to demonstrate geometrically precise 3D
images and to eliminate the superposition of anatomical structures enables the accurate
evaluation of important characteristics in the endodontic diagnosis (4, 9, 15, 16). One should
also consider the lowest radiation dose produced when FOV is reduced, since beam
collimation limits the radiation to the region of interest, which is equivalent to the dose of two
periapical radiographs (9, 17, 18).
In 1961, Bender and Seltzer demonstrated that periapical lesions can be
radiographically viewed only when the osseous rarefaction reaches the buccal or lingual
cortical bone, or both (19). In the present work, the accuracy regarding conventional and
digital periapical images of lesions produced with #6 and #10 burs was low for posterior
teeth, the same region studied by Bender and Seltzer. This can be explained by the fact that
the buccal cortical bone in this region is thicker. The lower sensitivity (0.2) observed in the
present study was verified in the conventional periapical image of lesions produced with #6
burs in the posterior teeth. Regardless of the region, the conventional intra-oral techniques
were found to be more accurate for diagnosis of greater lesion sizes compared to smaller ones,
mainly when cortical bone was involved (6, 16, 20, 21).
In the study in question, only lesions produced with #6 burs had images statistically
different from the controls (p < 0.05). Such lesions were not detected with these images,
which were performed by using both conventional intra-oral and digital panoramic methods in
anterior and posterior regions. Tanomaru-Filho et al. (2009) followed up the evolution of
periapical lesions induced by pulp exposure in dog teeth by using conventional periapical
radiography and histological analysis, and they concluded that radiographic exam was not
capable of diagnosing initial-stage lesions (21). In the present study, digital images produced
by means of CCD sensor were found to have the highest accuracy for lesions of 1.8 mm
diameter compared to conventional periapical radiography, a finding similar to that reported
by Tirrel et al. (22). According to Farrier et al. (2009), the PSP system produced images with

32
significantly high quality compared to those from CCD sensors, a result that was not found in
the present study (23). However, their study involved patients and there was difficulty in
positioning of CCD sensors properly, which might have been contributed to the worst results,
since other studies also compared CCD with PSP in dried mandibles and found acceptable
images in both systems (10).
The digital systems used were of high resolution, with CCD sensor having 14 lp/mm
and PSP system 22 lp/mm, thus enabling to distinguish details accurately but without
eliminating the superposition of osseous structures. Other authors found better results for the
conventional intra-oral method in relation to the PSP system regarding the diagnosis of small
periapical lesions, although the digital system had a spatial resolution of 6 pl/mm. This
resolution provides less detailed images than the digital system used in the present study, and
in addition their examiners had no previous experience with digital radiographs (1, 24),
differently from our work in which the examiners had knowledge on several digital image
manipulation tools. One should also consider the shorter exposure time in the digital systems
compared to that of conventional periapical technique, that is, less radiation is emitted to the
patient.
In the present study, the digital panoramic radiography had the smallest area (0.55),
and consequently the least accurate diagnosis of lesions produced with #6 burs in anterior
teeth, even with the availability of manipulation image tools. Estrela et al. (2009) found the
same negative result for incisors, but their study involved patients instead of dried mandibles
(25). Therefore, the poor sharpness in the image of anterior teeth may have occurred due to an
inclination of the osseous tables within the detail layer rather than to a superposition with the
cervical spine. On the other hand, lesions produced in posterior teeth using #6 burs showed a
higher area value (0.7) compared to anterior teeth, probably due to the better framing of the
posterior region within the detail layer (26). Nevertheless, panoramic image also showed
statistically significant difference in the region of posterior teeth compared to the controls as
panoramic radiographs of lesions produced with #10 burs and of those breaking the buccal
cortical bone were shown to be a reliable method in the diagnosis of periapical lesions.
Therefore, panoramic radiography continues to be an ideal method of initial evaluation.
The majority of the results obtained from Kappa’s coefficient demonstrated good
intra- and inter-rater reliabilities, thus showing that all the image diagnosis methods are
reproducible.
References 1. Friedlander LT, Love RM, Chandler NP. A comparison of phosphor-plate digital images
with conventional radiographs for the perceived clarity of fine endodontic files and periapical
lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93:321-7.
2. Lofthag-Hansen S, Huumonen S, Gröndahl K, Gröndahl HG. Limited cone-beam CT and
intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod. 2007;103:114-9.
3. Carvalho FB, Gonçalves M, Tanomaru-Filho M. Evaluation of chronic periapical lesions
by digital subtraction radiography by using Adobe Photoshop CS: a technical report. J Endod.
2007;33:493-7.
4. Costa CC, Netto CM, Koubik AC, Michelotto AL, et al. Aplicações clínicas da tomografia
computadorizada cone beam na Endodontia. J Health Sci Inst;2009:279-86.
5. Barbat J, Messer HH. Detectability of artificial periapical lesions using direct digital and
conventional radiography. J Endod. 1998;24:837-42.
6. Paurazas SB, Geist JR, Pink FE, et al. Comparison of diagnostic accuracy of digital
imaging by using CCD and CMOS-APS sensors with E-speed film in the detection of
periapical bony lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:356-62.

33
7. Patel S, Dawood A, Mannocci F, et al. Detection of periapical bone defects in human jaws
using cone beam computed tomography and intraoral radiography. Int Endod J.2009;42:507-
515.
8. Jorge EG, Tanomaru-Filho M, Gonçalves M, Tanomaru JM. Detection of periapical lesion
development by conventional radiography or computed tomography. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod. 2008;106:e56-61.
9. Scarfe WC. Use of cone-beam computed tomography in endodontics Joint Position
Statement of the American Association of Endodontists and the American Academy of Oral
and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod;2011:234-7.
10. de Almeida SM, Bóscolo FN, Haiter Neto F, dos Santos JC. [Assessment of 3
radiographic methods (conventional periapical, digital periapical, and panoramic) ni the
diagnosis of artificially produced periapical lesions]. Pesqui Odontol Bras. 2001;15:56-63.
11. Butterfield KJ, Dagenais M, Clokie C. Linear tomography's clinical accuracy and validity
for presurgical dental implant analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
1997;84:203-9.
12. Sogur E, Baksi BG, Gröndahl HG, et al. Detectability of chemically induced periapical
lesions by limited cone beam computed tomography, intra-oral digital and conventional film
radiography. Dentomaxillofac Radiol. 2009;38:458-64.
13. Soğur E, Gröndahl HG, Baksı BG, Mert A. Does a combination of two radiographs
increase accuracy in detecting acid-induced periapical lesions and does it approach the
accuracy of cone-beam computed tomography scanning? J Endod. 2012;38:131-6.
14. Tsai P, Torabinejad M, Rice D, Azevedo B. Accuracy of cone-beam computed
tomography and periapical radiography in detecting small periapical lesions. J Endod.
2012;38:965-70.
15. Cotti E. Advanced techniques for detecting lesions in bone. Dent Clin North Am.
2010;54:215-35.
16. Estrela C, Bueno MR, Azevedo BC, et al. A new periapical index based on cone beam
computed tomography. J Endod. 2008;34:1325-31.
17. Kamburoğlu K, Kiliç C, Ozen T, Horasan S. Accuracy of chemically created periapical
lesion measurements using limited cone beam computed tomography. Dentomaxillofac
Radiol. 2010;39:95-9.
18. Lennon S, Patel S, Foschi F, et al. Diagnostic accuracy of limited-volume cone-beam
computed tomography in the detection of periapical bone loss: 360° scans versus 180° scans.
Int Endod J. 2011;44:1118-27.
19. Bender IB, Seltzer S. Roentenographic and direct observation of experimental lesions in
bone I. J Am Dent Assoc 1961;62:152-60.
20. Petersson A, Axelsson S, Davidson T, et al. Radiological diagnosis of periapical bone
tissue lesions in endodontics: a systematic review. Int Endod J. 2012;45:783-801.
21. Tanomaru-Filho M, Jorge EG, Duarte MA, et al. Comparative radiographic and
histological analyses of periapical lesion development. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod. 2009;107:442-7.
22. Tirrel BC, Miles DA, Brown CE, Legan JJ, et al. Interpretation of chemically created
lesions using direct digital imaging. J Endod. 1998;22:74-8.
23. Farrier SL, Drage NA, Newcomb RG, et al. A comparative study of image quality and
radiation exposure for dental radiographs produced using a charge-coupled device and a
phosphor plate system. Int Endod J. 2009;42:900-7.
24. Wallace JA, Nair MK, Colaco MF, Kapa SF. A comparative evaluation of the diagnostic
efficacy of film and digital sensors for detection of simulated periapical lesions. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. 2001;92:93-7.

34
25. Estrela C, Bueno MR, Leles CR, et al. Accuracy of cone beam computed tomography and
panoramic and periapical radiography for detection of apical periodontitis. J Endod.
2008;34:273-9.
26. de Almeida SM, de Oliveira AE, Ferreira RI, Bóscolo FN. Image quality in digital
radiographic systems. Braz Dent J. 2003;14:136-41.

35
5 CONSIDERAÇÕES FINAIS
O presente trabalho concluiu, a partir dos dados obtidos, que a TCCB
apresentou elevados valores de acurácia no diagnóstico das lesões periapicais de
diferentes tamanhos, em ambas as regiões avaliadas (dentes anteriores e
posteriores), e demonstrou ser o método mais confiável para a visualização das
lesões periapicais iniciais.
Os métodos intra-orais digitais apresentaram imagens capazes de
diagnosticar lesões periapicais, com menor acurácia para as rarefações ósseas
menores, quando comparadas com TCCB, porém, sem diferença estatística com o
real.
As radiografias periapicais convencionais e as radiografias panorâmicas
digitais não proporcionaram imagem satisfatória para o diagnóstico das lesões com
1,8 mm de diâmetro.

36
REFERÊNCIAS
ALMEIDA, S.M. et al. Avaliação de três métodos radiográficos (periapical convencional, periapical digital e panorâmico) no diagnóstico de lesões apicais produzidas artificialmente. Pesquisa Odontológica Brasileira, São Paulo, v.15, n.1, p.56-63, Jan./Mar. 2001. ALMEIDA, S.M. et al. Image quality in digital radiographic systems. Brazilian Dental Journal, Ribeirão Preto, v.14, n.2, 136-141, Apr. 2003. BARBAT, J.; MESSER, H.H. Detectability of Artificial Periapical Lesions Using Direct Digital and Conventional Radiography. Journal of Endodontics, Baltimore, v. 24, n.12, p. 837-842, Dec. 1998. BENDER, I.B.; SELTZER, S. Roentenographic and direct observation of experimental lesions in bone: I. Journal of Endodontics, Baltimore, v.29, n.11, p. 702-706, Nov. 2009. BENDER, I.B.; SELTZER, S. Roentenographic and direct observation of experimental lesions in bone: II. Journal of Endodontics, Baltimore, v.29, n.11, p. 707-712, Nov. 2009. BUTTERFIELD, K.J.; DAGENAIS, M.; CLOKIE, C. Linear tomography´s clinical accuracy and validity for presurgical dental implant analysis. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, Saint Louis, v.84, n.2, p. 203-209, Aug. 1997. CARVALHO, F.; GOLÇALVES, M.; TANOMARU-FILHO, M. Evaluation of Chronic Periapical Lesions by Digital Subtraction Radiography by Using Adobe Photoshop CS: A Technical Report. Journal of Endodontics, Baltimore, v.33, n.4, p. 493-497, Apr. 2007. COSTA, C.C.A. et al. Aplicações clínicas da tomografia computadorizada cone beam na Endodontia. Revista do Instituto de Ciências da Saúde, São Paulo, v.25, n.3, p. 279-286, 2009. COTTI, E. Advanced Techniques for Detecting Lesions in Bone. Dental Clinics of North America, Philadelphia, v.54, p. 215-235, 2010. ESTRELA, C. et al. Accuracy of Cone Beam Computed Tomography and Panoramic and Periapical Radiography for Detection of Apical Periodontitis. Journal of Endodontics, Baltimore, v.34, n.3, p. 273-279, Mar. 2008. ESTRELA, C. et al. A new periapical index based on cone beam computed tomography. Journal of Endodontics, Baltimore, v.34, n.11, p. 1325-1331, Nov. 2008. FRIEDLANDER, L.T.; LOVE, R.M.; CHANDLER, N.P. A comparison of phosphor-plate digital images with conventional radiographs for the perceived clarity of fine

37
endodontic files and periapical lesions. Oral Surgery Oral Medicine Oral Pathology, Saint Louis, v.93, n.3, p. 321-327, Mar. 2002. FARRIER, S.L. et al. A comparative study of image quality and radiation exposure for dental radiographs produced using a charge-coupled device and a phosphor plate system. International Endodontic Journal, Oxford, v.42, n.10, p. 900-907, Oct. 2010. HANLEY, J.A.; MCNEIL, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology, Easton, v.143, n.1, p. 29-36, Apr. 1982. JORGE, E. et al. Detection of periapical lesion development by conventional radiography or computed tomography. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, Saint Louis, v.106, n.1, p. e56-e61, July 2008. KAMBUROGLU, K. et al. Accuracy of chemically created periapical lesion measurements using limited cone beam computed tomography. Dentomaxillofacial Radiology, Houndsmills, v.39, n.2, p. 95-99, Feb. 2010. LENNON, S. et al. Diagnostic accuracy of limited-volume cone-beam computed tomography in the detection of periapical bone loss: 360° scans versus 180° scans. International Endodontic Journal, Oxford, v.44, n.12, p. 1118-1127, Dec. 2011. LOFTHAG-HANSEN, S. et al. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, Saint Louis, v.103, n.1, p. 114-119, Jan. 2007. PATEL, S. et al. Detection of periapical bone defects in human jaws using cone beam computed tomography and intraoral radiography. International Endodontic Journal, Oxford, v.42, n.6, p. 507-515, June 2009. PAULA-SILVA, F.W.G. et al. accuracy of periapical radiography and cone-beam computed tomography scans in diagnosing apical periodontitis using histopathological findings as a gold standard. Journal of Endodontics, Baltimore, v.35, n.7, p. 1009-1012, July 2009. PAURAZAS, S.B. et al. Comparison of diagnostic accuracy of digital imaging by using CCD and CMOS-APS sensors with E-speed film in the detection of periapical bony lesions. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, Saint Louis, v.89, n.3, p. 356-362, Mar. 2000. PETERSSON, A. et al. Radiological diagnosis of periapical bone tissue lesions in endodontics: a systematic review. International Endodontic Journal, Oxford, v.45, n.9, p. 783-801, Sept. 2012. SCARFE, W.C. Use of cone-beam computed tomography in endodontics Joint Position Statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology. Oral Surgery Oral Medicine Oral

38
Pathology Oral Radiology and Endodontology, Saint Louis, v.111, n.2, p. 234-237, Feb. 2011. SOGUR, E. et al. Detectability of chemically induced periapical lesions by limited cone beam computed tomography, intra-oral digital and conventional film radiography. Dentomaxillofacial Radiology, Houndsmills, v.38, n.7, p. 458-464, Oct. 2009. SOGUR, E. et al. Does a combination of two radiographs increase accuracy in detecting acid-induced periapical lesions and does it approach the accuracy of cone-beam computed tomography scanning? Journal of Endodontics, Baltimore, v.38, n.2, p. 131-136, Feb. 2012. TANOMARU-FILHO, M. et al. Comparative radiographic and histological analyses of periapical lesion development. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, Saint Louis, v.107, n.3, p. 442-447, Mar. 2009. TIRREL, B.C. et al. Interpretation of chemically created lesions using direct digital imaging. Journal of Endodontics, Baltimore, v.22, n.2, p. 74-78, Feb. 1996. TSAI, P. et al. Accuracy of cone-beam computed tomography and periapical radiography in detecting small periapical lesions, Journal of Endodontics, Baltimore, v.38, n.7, p. 965-970, July 2012. WALLACE, J.A. et al. A comparative evaluation of the diagnostic efficacy of film and digital sensors for detection of simulated periapical lesions. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, Saint Louis, v.92, n.1, p. 93-97, July 2001. WENZEL, A.; VERDONSCHOT, E.H. Some considerations in the evaluation of diagnostic tests in dentistry. Dentomaxillofacial Radiology, Houndsmills, v.23, n.4, p. 179-182, Nov. 1994. WENZEL, A. Digital radiography and caries diagnosis. Dentomaxillofacial Radiology, Houndsmills, v.27, n.1, p. 3-11, Jan. 1998.