Abomen Aberto - VAC PAC

of 4
-
Upload
vitor-francisco -
Category
Documents
-
view
218 -
download
0
Transcript of Abomen Aberto - VAC PAC
-
8/14/2019 Abomen Aberto - VAC PAC
1/4
No such thing as an "open abdomen"
A term commonly used by surgeons for the treatment of major trauma casesand abdominal compartment syndrome is "open abdomen." (This term may alsobe used on someone with another type or surgery such as an aortic aneurysm
repair, but most commonly it refers to trauma.) This term means that thesurgeon operated on a patient's abdomen and did not sew them back shutbecause they already had IAH or ACS and needed to be decompressed, theyhad so much swelling in their abdomen that they could not tuck the guts back in,or they were afraid that if they did tuck the guts back in, the patient woulddevelop abdominal hypertension and possibly abdominal compartmentsyndrome. A common belief is that because the abdomen is left open, thepatient cannot develop IAH or ACS
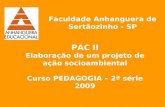
Figure 1: This patient has an IAP of 33 mm Hg he is suffering from organdysfunction due to abdominal compartment syndrome and needs a
decompressive laparotomy.[1]
Figure 2: This is the patient from figure 1 after his decompressive Laparotomy.Note how dramatically the swollen intestines have bulged out of the abdominalincision. You can imagine how this swelling led to a dramatic increase in theIAP when the abdominal wall confined it. Now that it has been decompressed,the patient's IAP has dropped to 15 mm Hg.
The result of a decompressive laparotomy, or of simply leaving the abdomen"open" after a surgical case is that the volume of space available for theabdomens contents is much larger probably half again as large. Once the
abdomen is opened, the patients intestines are not left out in the open airbecause this would result in them drying out and dying as well as becoming
-
8/14/2019 Abomen Aberto - VAC PAC
2/4
infected by the external environment. For this reason, every "open abdomen" isclosed with a dressing.
Dressing closures are done in a variety of ways: Bogota bag, Ioban dressing,Wittman patch, KCI Vac-pac, etc. One of the more common methods is using a
"Bogota bag" because it costs almost nothing.
Figure 4: A Bogota bag is simply a 3 liter IV plastic bag with 3 of the edges cutoff so it lies flat (Figures 3 & 4) It is put in a sterilizer in the operating room, thengiven to the surgeon who stitches it over the guts to the sides of the abdominalincision. This allows the clinician to be able to look through the clear window ofthe plastic bag and see if the guts are healthy. Sometimes they pack gauzeunder the bag to absorb fluid. The other methods are variations on the sametheme, some including suction that allows re-accumulated fluid to be suctionedout of the abdominal cavity.
-
8/14/2019 Abomen Aberto - VAC PAC
3/4
Figure 5: A commercially available temporary abdominal wall with Velcro toallow gradual wound tightening
Figures 6a & 6b: KCI Vac-Pac Sponge inserted over an internal dressing,with suction in center, then covered again with outer dressing. 6a is early in thecourse when abdomen is still widely open. 6b is later as the wound is partiallyclosed and the sponge is trimmed smaller.
-
8/14/2019 Abomen Aberto - VAC PAC
4/4
The point of all the above discussion is this: There is no such thing as an openabdomen after surgery. This would lead to desiccation (drying/mummification)and death of the bowel plus internal infection. ALL open abdomens are closedwith an airtight dressing for protection. The result is a closed abdomen that hasa larger volume that the previous abdomen so the internal pressure is reduced.
However, the same processes that led to the accumulation of fluid and increasein IAP in the first place are still present. If they continue and further edemadevelops, the pressure within the abdomen can easily begin rising again andACS can recur. This has been described in many reports. The largest series, byGracias demonstrated that of all patients who had their abdomen left open toprevent IAH / ACS and had a vacuum pack placed to suction out excess fluid,still developed ACS (defined as IAP > 25 mmHg plus organ dysfunction).[2] Themortality in those who developed ACS was 60% while it was only 7% in theothers.
The authors recommend that "treatment of IAH can be achieved by incising theexternal antimicrobial drape to allow for further expansion of the abdominal wall Prior to placement of a new sterile drape."[2]
Their conclusion: "Management of the open abdomen with the vacuum-packclosure technique does not obviate against the development of ACS. Ongoing vigilant monitoring of IAP is mandatory in this patient population torecognize IAH and treat it expediently."[2]
More recent data out of Colombia confirm Gracia's observations: In a series of79 open abdomens who were all serially monitored for IAP from the time ofsurgery through their ICU stay, Ordonez et al found recurrent abdominalcompartment syndrome occurring in 8.9% of their study population - all whorequired emergent reexploration and relief of the elevated pressure despitehaving an "open" dressing.[3] The subgroup of patients who developedrecurrent ACS suffered a 78% mortality while those who did not had a 20%mortality. Based on the enorous costs occuring when the patient is opened andthe ability to monitor and prevent ACS in many patients, these clinicians feelaggressive bladder pressure monitoring of all open abdomens and earlyintervention to reduce rising pressures is mandatory to avoid death and reducecosts.





![CT102 - keyautomation.it Unidade para um motor 230 Vac (120 Vac), para portão de correr ou portão basculante Centrala do silnika 230 Vac (120 Vac),QDS G]DMFHJRSU]HVXZQEUDP RJURG]HQLRZOXE](https://static.fdocumentos.com/doc/165x107/5c24810609d3f21f508c6e1b/ct102-unidade-para-um-motor-230-vac-120-vac-para-portao-de-correr-ou-portao.jpg)