DIRETRIZ CÂNCER DE TIREÓIDE
68
7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 1/68 Continue NCCN Clinical Practice Guidelines in Oncology™ Thyroid Carcinoma V.2.2007 www.nccn.org
Transcript of DIRETRIZ CÂNCER DE TIREÓIDE

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 1/68
Continue
NCCN Clinical Practice Guidelines in Oncology™
Thyroid
Carcinoma
V.2.2007
www.nccn.org

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 2/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
NCCN Thyroid Carcinoma Panel Members
Steven I. Sherman, MD/Chair The University of Texas M. D. AndersonCancer Center
Peter Angelos, MD, PhDRobert H. Lurie Comprehensive Cancer Center of Northwestern University
Douglas W. Ball, MDThe Sidney Kimmel ComprehensiveCancer Center at Johns Hopkins
David Byrd, MDFred Hutchinson Cancer ResearchCenter/Seattle Cancer Care Alliance
Orlo H. Clark, MDUCSF Comprehensive Cancer Center
Gilbert H. Daniels, MDDana-Farber/Brigham and Women’sCancer Center | Massachusetts GeneralHospital Cancer Center
Raza A. Dilawari, MD
St. Jude Children's ResearchHospital/Univeristy of TennesseeCancer Institute
Hormoz Ehya, MDFox Chase Cancer Center
ð
¶
†
¶
¶
ð
¶
¹
William B. Farrar, MDArthur G. James Cancer Hospital andRichard J. Solove Research Institute atThe Ohio State University
Robert F. Gagel, MDThe University of Texas M. D. Anderson
Cancer Center
Fouad Kandeel, MDCity of Hope
Richard T. Kloos, MDArthur G. James Cancer Hospital &Richard J. Solove Research Institute atThe Ohio State University
Peter Kopp, MDRobert H. Lurie Comprehensive Cancer Center of Northwestern University
Dominick M. Lamonica, MDRoswell Park Cancer Institute
Thom R. Loree, MD
Roswell Park Cancer Institute
William M. Lydiatt, MDUNMC Eppley Cancer Center at TheNebraska Medical Center
¶
ð Þ
ð
ð
ð
Þ
¶
¶
f
f
Judith McCaffrey, MDH. Lee Moffitt Cancer Center andResearch Institute at the University of South Florida
John A. Olson, Jr., MD, PhDDuke Comprehensive Cancer Center
John A. Ridge, MD, PhDFox Chase Cancer Center
Jatin P. Shah, MDMemorial Sloan-Kettering Cancer Center
James C. Sisson, MD
University of Michigan ComprehensiveCancer Center
R. Michael Tuttle, MDMemorial Sloan-Kettering Cancer Center
Marshall M. Urist, MD
z
f
University of Alabama at Birmingham
Comprehensive Cancer Center
¶
¶
¶
Þ
ð
¶
*
ð Endocrinology
Pathology
Nuclear MedicineOtolaryngology
¶ Surgery/Surgical oncology
Þ Internal medicine
*Writing Committee Member
† Medical Oncology
¹
f
z
Continue
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 3/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Table of Contents
Papillary Carcinoma
Medullary Carcinoma
NCCN Thyroid Carcinoma Panel MembersNodule Evaluation (THYR-1)
Follicular Carcinoma (FOLL-1)
Hürthle Cell Carcinoma ( -1)
Diagnosed by FNA (MEDU-1)
Germline mutation of RET proto-oncogene (MEDU-2)
Anaplastic Carcinoma (ANAP-1)
Guidelines Index
Print the Thyroid Carcinoma Guideline
·
·
·
·
FNA positive (PAP-1)
Incidental finding postlobectomy (PAP-2)
HÜRT
These guidelines are a statement of consensus of the authors regarding their views of currently accepted approaches to treatment. Any clinicianseeking to apply or consult these guidelines is expected to use independent medical judgment in the context of individual clinical circumstances todetermine any patient's care or treatment. The National Comprehensive Cancer Network makes no representations nor warranties of any kindwhatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way. These guidelines arecopyrighted by National Comprehensive Cancer Network. All rights reserved. These guidelines and the illustrations herein may not be reproduced inany form without the express written permission of NCCN. ©2007.
For help using thesedocuments, please click here
Staging
Manuscript
References
Clinical Trials:
Categories of Consensus:NCCN All recommendations are Category2A unless otherwise specified.
See
Thebelieves that the best managementfor any cancer patient is in a clinicaltrial. Participation in clinical trials isespecially encouraged.
NCCN
To find clinical trials online at NCCNmember institutions, click here:nccn.org/clinical_trials/physician.html
NCCN Categories of Consensus
Summary of Guidelines Updates
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 4/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 5/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Thyroid Carcinoma
Nodule Evaluation
WORKUPCLINICAL PRESENTATION
Clinically euthyroid:··
··
TSH measurementUltrasound of thyroid
and neck includingadjacent cervical lymphnodesFNA of noduleFNA of clinicallysuspicious lymphnodes
Follow-up as clinically indicated(Observe for criteria of increasedsuspicion - see above pathway)
Thyroidnodule with
unknownTSH
Nodules < 1 cm in diameter without enlarged cervicallymph nodes or suspicious findings by ultrasoundor nodules 1-4 cm with no suspicious criteria
·
·
Solitary nodule > 1 cm in diameter
Increased suspicion if anyof the following are present:
Age < 15 y or > 45 yMale sexNodule > 4 cm in diameter History of radiation exposureHistory of diseases associated with
thyroid cancer:HyperparathyroidismGardner’s syndromeFamilial adenomatous polyposisCarney complexCowden’s syndrome
Suspicious criteria by ultrasoundCentral hypervascularity
MicrocalcificationIncidentally identified focal PETpositive lesion in the thyroid
a
>
>
>
>
>
7
7
7
7
7
7
>
7
77
>
Pheochromocytoma
Irregular border
· Highly suspicious:Rapid nodule growth
b
>
>
>
>
>
>
>
Very firm noduleFixation to adjacentstructuresFamily history of thyroidcancer
Vocal cord paralysisEnlarged regional lymphnodesSymptoms of invasion intoneck structures
See FNAResults(THYR-2)
a
b
In selected cases, it may be reasonable to follow with serial ultrasounds.
Consider surgery after FNA.
Papillary carcinoma,finding postlobectomyfor benign disease
See Primary Treatment (PAP-2)
THYR-1
Thyroidnodule withlow TSH
See Primary Treatment (THYR-2)

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 6/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
c
d
e
This includes cytology suspicious for papillary carcinoma.If suspicious, perform serum calcitonin and CEA.
Consider trial of thyroxine therapy for small, clinically nonsuspicious, follicular neoplasm in a young female patient (category 3).
FNA RESULTS TREATMENT
Carcinoma
See pathway for carcinoma, above
Follicular neoplasm(suspicious/atypia)or presenting nodule
with low TSH
Benign(Hürthle cells in theabsence of neoplasm)
Insufficient
biopsy
Surgery e
·
·
ObserveIf nodule growth, repeat FNA or consider surgery
Repeat FNA, consider ultrasoundguidance and immediate cytologic reviewor consider surgery
Papillary c
Hürthle cell
See Primary Treatment (PAP-1)
See Primary Treatment (FOLL-1)
See Primary Treatment (HÜRT-1)
See Primary Treatment (MEDU-1)
See Primary Treatment (ANAP-1)Anaplastic
Hot
Cold Surgery
Thyroidscan
Follicular
Medullaryd
TSH high or normal
TSH lowEvaluate and treat for thyrotoxicosis as indicated(malignancy is rare)
Thyroidlymphoma See NCCN Non-Hodgkin’s Lymphoma Guideline
Back to ThyroidCarcinoma Table
of Contents
THYR-2
Pathology and
cytopathology slidesshould be reviewed at thetreating institution by apathologist with expertisein thyroid carcinoma.
Thyroid Carcinoma
Nodule Evaluation
See Primary Treatment (PAP-1)
Well-differentiated
Poorly-differentiated

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 7/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Thyroid Carcinoma
Papillary Carcinoma
PapillarycarcinomaFNApositive
·
·
·
·
·
Consider chest x-
rayThyroidultrasound, if notpreviously doneConsider lateralneck ultrasound(category 2B)CT/MRI for fixed or substernal lesions
(avoid iodinatedcontrast, unlessessential)Evaluate vocalcord mobility(category 2B)
Indications for totalthyroidectomy:(any present)
Ag
·····
··
·
Age < 15 y or > 45 yRadiation historyKnown distant metastasesBilateral nodularityExtrathyroidal extension
Tumor > 4 cm in diameter Cervical lymph nodemetastases
gressive variant
a
b
Indications for totalthyroidectomy
lobectomy:(all present)
or
····
·
··
Age 15 y - 45 yNo prior radiationNo distant metastasesNo cervical lymph nodemetastasesNo extrathyroidalextension
Tumor < 4 cm in diameter No aggressive variant
a
b
PREOPERATIVE ORINTRAOPERATIVEDECISION-MAKING CRITERIA
DIAGNOSTICPROCEDURES
FNAFINDING
Total thyroidectomyIf lymph node(s) palpable or biopsypositive:··
Central neck dissection (level VI)Lateral neck dissection (levels II-V,sparing spinal accessory nerve,internal jugular vein, and
sternocleidomastoid muscle)Consider preservation of the cervicalsensory nerves, when feasible
Totalthyroidectomy(most common)(category 2B)
or
Lobectomy +isthmusectomy(category 2B)
PRIMARY TREATMENT
··
·
·
·
Aggressive variantMacroscopic multifocaldiseasePositive isthmusmarginsCervical lymph nodemetastasesExtrathyroidal extension
b
·
·
NegativemarginsNo contralaterallesion
See PostsurgicalEvaluation (PAP-3)
See PostsurgicalEvaluation (PAP-3)
a
b
Age is an approximation and not an absolute determination.
Tall cell, columnar cell, insular, oxyphilic, or poorly differentiated features.
Completion of thyroidectomy
·
·
Consider thyroglobulinmeasurementSuppress TSHwith thyroxine
See Surveillanceand Maintenance(PAP-5)
PAP-1

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 8/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Completion of thyroidectomy
·
··
·
Clinically suspiciouslymph node,contralateral lesion,or pAggressive variantMacroscopicmultifocal disease
1 cm in diameter
erithyroidal nodeb
³
····
Negative marginsNo contralateral lesion< 1 cm in diameter No suspicious lymphnode
PRIMARY TREATMENT
···
> 4 cmPositive marginsExtra-thyroidalinvasion (T3 or T4)
Papillarycarcinomafound post-lobectomy for benign disease
·
·
Thyroid and neckultrasound, if notpreviously doneChest x-ray, if notrecently done
CLINICAL PRESENTATION
See PostsurgicalEvaluation(PAP-3)
PAP-2
bTall cell, columnar cell, insular, oxyphilic, or poorly differentiated features.
Thyroid Carcinoma
Papillary Carcinoma
Consider thyroglobulinmeasurement +antithyroglobulinantibodies
Completion of thyroidectomy (category 2B)
or
Thyroglobulin measurement+ antithyroglobulinantibodies
Consider thyroxinetherapy to keepTSH low/normal
See Surveillanceand Maintenance(PAP-5)
See PostsurgicalEvaluation(PAP-3)
Thyroxine therapyto keep TSHlow/normal
See Surveillanceand Maintenance(PAP-5)

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 9/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
TSH + thyroglobulinmeasurement +
antithyroglobulinantibodies (1-12 wkpostoperatively)
POSTSURGICAL EVALUATIONAFTER THYROIDECTOMY
No grossresidualdisease
in neck
Grossresidualdiseasein neck
SuppressTSH withthyroxine
SeeSurveillanceand
Maintenance(PAP-5)
Unresectable
Resectable Resect, if possible
No grossresidual disease
Gross residualdisease
Inadequateuptake
No scanperformed
RT
·
·
·
Radioiodinetreatment
Post-treatment
I scanRT
131
SeePostsurgicalTherapy(PAP-4)
·
·
TSH + thyroglobulinmeasurement +antithyroglobulinantibodies (1-12 wkpostoperatively)
Total bodyradioiodine scan(category 2B)
PAP-3
Adequateuptake
Thyroid Carcinoma
Papillary Carcinoma
·
·
·
·
< 1 cm confined toglandNo nodal metastasesNo distant metastasesNon-aggressivehistology
SeeSurveillanceandMaintenance(PAP-5)
·
·
·
·
1 cmor Nodal metastasesor Distant metastasesor Aggressive histology
³

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 10/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Adjuvant radioiodineablation (30-100 mCi)of thyroid bed(category 2B) andposttreatment scan
RadioiodinemCi
posttreatment scan
treatment(100-200 ) and
Suppress
TSH withthyroxine
POSTSURGICAL THERAPY
T4 (surgicallyevident extra-
thyroidalinvasion) andage > 45 y
All others
Consider RT
SeeSurveillance
andMaintenance(PAP-5)
1-12 wkpostthyroidectomy:No gross residualdisease in neckwith adequate TSHstimulation (thyroidwithdrawal or recombinant rhTSH
stimulation)
Suspected or provenradioiodine avidresidual tumor
c
d
Suspected or proven thyroidbed uptake
c
Thyroglobulin< 1 ng/mL andradioiodinescan negative
No radioiodinetreatment
c
dSuspicion based on pathology, postoperative thyroglobulin, and intraoperative findings.
All patients should be examined and palpable neck disease should be surgically resected before radioiodine treatment.
PAP-4
Thyroid Carcinoma
Papillary Carcinoma
Total bodyradioiodinescan(category 2B)
G id li I d

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 11/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
·
·
·
·
·
Physical examination, TSH and thyroglobulinmeasurement + antithyroglobulin antibodies at6 and 12 mo, then annually if disease-free
Consider additional nonradioiodine imaging(eg, FDG PET ± CT if Tg 10 ng/mL), if Iscans negative and stimulated Tg > 2-5 ng/mL
Periodic neck ultrasound
TSH stimulated thyroglobulin without
radioiodine scan at 12 mo in patientspreviously treated with RAI with recentnegative neck ultrasound and undetectableTSH suppressed thyroglobulin (anti-thyroglobulin antibody negative) and T1-2, N0-1, M0 at initial staging
If detectable thyroglobulin, distant metastasesor soft tissue invasion on initial staging,radioiodine scan every 12 mo until noradioactive iodine avid tumor is evident (either withdrawal of thyroid hormone or rhTSH)e
131³
SURVEILLANCE AND MAINTENANCE
Locoregional recurrence
Metastatic disease
·
·
Thyroglobulin > 10 ng mLthyroid hormone)
Scans (including PET)negative
/(off
Consider therapywith 100-150 mCi, posttreatment
I scan (category 3)
radioiodine
131
Surgery (preferred) if resectable
and/or Radioiodine treatment,if radioiodine scan positiveand/or RT, if radioiodine scan negative
See Treatment of Metastases(PAP-6)
RECURRENT DISEASE
eIf there is a high likelihood of therapy, thyroid hormone withdrawal suggested; if not, suggest using rhTSH.
PAP-5
Thyroid Carcinoma
Papillary Carcinoma
·
·
·
Stimulated Tg 1-10 ng/mLNon-resectable tumorsNon-radioiodine avid
Suppress TSH with thyroxine
Guidelines Index

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 12/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
TREATMENT OF METASTASES
Solitary CNS
Consider neurosurgical resection
Radioiodine treatment with rhTSH and steroidprophylaxis, if radioiodine scan positive
RT
and/or
and/or
Bone
·
·
·
Surgical palliation, if symptomatic or asymptomatic in weight-bearing extremities
Radioiodine treatment, if radioiodine scan positiveand/or
and/or RTConsider bisphosphonate therapyConsider embolization of metastases
Other
extracervical sites
Consider surgical resection of selected, enlarging,or symptomatic metastasesand/or Radioiodine if positive uptake, with considerationof dosimetry to maximize dosingand/or Clinical trials for non-radioiodine avid tumors ;systemic therapy if not in clinical trialor Best Supportive Care
f
Metastatic disease· Continue to suppress
TSH with thyroxine
PAP-6
Thyroid Carcinoma
Papillary Carcinoma
f Cytotoxic chemotherapy has shown to have minimal efficacy. There are agents in clinical trials investigating novel targeted therapies.
See Clinical trials available at the NCCN member institutions.
Guidelines IndexTh id C i

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 13/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Thyroid Carcinoma
Follicular Carcinoma
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Follicular carcinoma
Total thyroidectomy if invasivecancer, metastatic cancer, or patient decisionIf lymph node(s) positive:
Central neck dissection(level VI)Lateral neck dissection
(levels II–V, sparing spinalaccessory nerve, internal
jugular vein, andsternocleidomastoid muscle)Consider preservation of thecervical sensory nerves,when feasible
·
·
or
Lobectomy/isthmusectomy
PATHOLOGYFINDING
DIAGNOSTICPROCEDURES
PRIMARY TREATMENT
··
·
·
Chest x-rayConsider lateralneck ultrasound
(category 2B)CT/MRI for fixedor substernallesions (avoidiodinatedcontrast, unlessessential)Evaluate vocalcord mobility(category 2B)
See PostsurgicalEvaluation
(FOLL-2)
Minimallyinvasivecancer a
Follicular adenoma
Invasive cancer (extensivevascular invasion)
Consider completion of thyroidectomy
or
Observe
Observe
Completion of thyroidectomy
aMinimally invasive cancer is characterized as a well-defined tumor with microscopic capsular and/or a few foci of vascular invasion
and often requires examination of at least 10 histologic sections to demonstrate.
See PostsurgicalEvaluation(FOLL-2)
See PostsurgicalEvaluation(FOLL-2)
FOLL-1
Follicular neoplasm
See NoduleEvaluation (THYR-2)
Suppress TSHwith thyroxine
See Surveillanceand Maintenance(FOLL-4)
Guidelines IndexThyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 14/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Guidelines IndexThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
POSTSURGICAL EVALUATIONAFTER THYROIDECTOMY
No grossresidualdiseasein neck
Grossresidualdiseasein neck
SuppressTSH withthyroxine
SeeSurveillanceand
Maintenance(FOLL-4)
Unresectable
Resectable Resect, if possible
No grossresidual disease
Gross residualdisease
RT·
·
TSH + thyroglobulinmeasurement +antithyroglobulinantibodies (1-12 wkpostoperatively)
Total bodyradioiodine scan(category 2B)
FOLL-2
No scanperformed
·
·
·
Radioiodinetreatment
Post-treatmentI scan
RT
131
Thyroid Carcinoma
Follicular Carcinoma
Inadequateuptake
Adequateuptake
TSH + thyroglobulinmeasurement +antithyroglobulinantibodies (1-12 wkpostoperatively)
SeePostsurgicalTherapy(FOLL-3)
·
·
·
·
< 1 cm confined toglandNo nodal metastasesNo distant metastasesNon-aggressivehistology
SeeSurveillanceandMaintenance(FOLL-4)
·
·
·
·
1 cmor Nodal metastasesor Distant metastasesor Aggressive histology
³
Guidelines IndexThyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 15/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007
Gu de es deThyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
SuppressTSH withthyroxine
SeeSurveillanceandMaintenance(FOLL-4)
FOLL-3
Thyroid Carcinoma
Follicular Carcinoma
Adjuvant radioiodineablation (30-100 mCi)of thyroid bed(category 2B) andposttreatment scan
RadioiodinemCi
posttreatment scan
treatment(100-200 ) and
POSTSURGICAL THERAPY
1-12 wkpostthyroidectomy:No gross residualdisease in neckwith adequate TSHstimulation (thyroidwithdrawal or recombinant rhTSH
stimulation)
Suspected or provenradioiodine avidresidual tumor
b
c
Suspected or proven thyroidbed uptake
b
Thyroglobulin< 1 ng/mL andradioiodinescan negative
No radioiodinetreatment
Total bodyradioiodinescan(category 2B)
b
cSuspicion based on pathology, postoperative thyroglobulin, and intraoperative findings.
All patients should be examined and palpable neck disease should be surgically resected before radioiodine treatment.
Guidelines IndexThyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 16/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007Thyroid Carcinoma TOC
Staging, MS, References
SURVEILLANCE AND MAINTENANCE
Locoregional recurrence
Metastatic disease
Surgery (preferred) if resectable
and/or radioiodine treatment,if radioiodine scan positiveand/or RT, if radioiodine scan negative
See Treatment of Metastases (FOLL-5)
RECURRENT DISEASE
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
d
If there is a high likelihood of therapy, thyroid hormone withdrawal suggested; if not, suggest using rhTSH.
FOLL-4
Thyroid Carcinoma
Follicular Carcinoma
·
·
·
·
Physical examination, TSH and thyroglobulinmeasurement + antithyroglobulin antibodies at6 and 12 mo, then annually if disease-free
Consider additional nonradioiodine imaging(eg, FDG PET ± CT if Tg 10 ng/mL), if Iscans negative and stimulated Tg > 2-5 ng/mL
TSH stimulated thyroglobulin withoutradioiodine scan at 12 mo in patients
previously treated with RAI with recentnegative neck ultrasound and undetectableTSH suppressed thyroglobulin (anti-thyroglobulin antibody negative) and T1-2, N0-1, M0 at initial staging
If detectable thyroglobulin, distant metastasesor soft tissue invasion on initial staging,
radioiodine scan every 12 mo until noradioactive iodine avid tumor is evident (either withdrawal of thyroid hormone or rhTSH)d
131³
·
·
·
Stimulated Tg 1-10 ng/mLNon-resectable tumorsNon-radioiodine avid
Suppress TSH with thyroxine
·
·
Thyroglobulin > 10 ng mLthyroid hormone)
Scans (including PET)
negative
/(off
Consider therapywith 100-150 mCi, posttreatment
I scan (category 3)
radioiodine
131
®Guidelines IndexThyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 17/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007Thyroid Carcinoma TOC
Staging, MS, References
TREATMENT OF METASTASES
Solitary CNS
Consider neurosurgical resection
Radioiodine treatment with rhTSH and steroidprophylaxis, if radioiodine scan positive
RT
and/or
and/or
Bone
·
·
·
Surgical palliation, if symptomatic or asymptomaticin weight-bearing extremities
Radioiodine treatment, if radioiodine scan positiveand/or
and/or RTConsider bisphosphonate therapyConsider embolization of metastases
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Other extracervical sites
Consider surgical resection of selected, enlarging, or symptomatic metastasesand/or Radioiodine if positive uptake, with consideration of
dosimetry to maximize dosingand/or Clinical trials for non-radioiodine avid tumors;systemic therapy if not in clinical trialor Best Supportive Care
e
FOLL-5
Thyroid Carcinoma
Follicular Carcinoma
eCytotoxic chemotherapy has shown to have minimal efficacy. There are agents in clinical trials investigating novel targeted therapies.
See Clinical trials available at the NCCN member institutions.
Metastatic disease· Continue to suppress
TSH with thyroxine
NCCN®
Guidelines IndexThyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 18/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007Thyroid Carcinoma TOC
Staging, MS, References
y
Hürthle Cell Carcinoma
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Hürthle cellcarcinoma
Total thyroidectomy, if invasive cancer or patientdecisionIf lymph node(s) positive:
Central neck dissection(level VI)
Consider preservation of thecervical sensory nerves,when feasible
·
· Lateral neck dissection
(levels II–V, sparing spinalaccessory nerve, internal jugular vein, and sterno-cleidomastoid muscle)
or
Lobectomy/isthmusectomy
FNA FINDING DIAGNOSTICPROCEDURES
PRIMARY TREATMENT
·
·
·
·
Chest x-ray
voidiodinated contrastunless essential)Evaluate vocalcord mobility
(category 2B)
Consider lateralneck ultrasound
(category 2B)CT/MRI for fixedor substernallesions (a
Minimallyinvasivecancer a
Hürthleadenoma
Invasive cancer (extensivevascular invasion)
Stronglyconsider completion of thyroidectomy
or
Observe
Observe
Completion of thyroidectomy
Suppress TSHwith thyroxine
See SurveillanceandMaintenance(H RT-4)Ü
See PostsurgicalEvaluation(H RT-2)Ü
See PostsurgicalEvaluation(H RT-2)Ü
See PostsurgicalEvaluation(H RT-2)Ü
aMinimally invasive cancer is characterized as a well-defined tumor with microscopic capsular and/or a few foci of
vascular invasion and often requires examination of at least 10 histologic sections to demonstrate.
H RT-1Ü
H rthleneoplasm
ü See NoduleEvaluation (THYR-2)
NCCN® P ti G id li
Guidelines IndexTh id C i TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 19/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007Thyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
POSTSURGICAL EVALUATIONAFTER THYROIDECTOMY
Gross
residualdiseasein neck
SuppressTSH withthyroxine
SeeSurveillanceandMaintenance(H RT-4)Ü
Unresectable
Resectable Resect, if possible
No grossresidual disease
Gross residualdisease
·
·
TSH + thyroglobulinmeasurement +antithyroglobulinantibodies (1-12 wkpostoperatively)Total bodyradioiodine scan(category 2B)
H RT-2Ü
RT
No scanperformed
·
·
·
Radioiodinetreatment
Post-treatmentI scan
RT
131
No grossresidualdiseasein neck
y
Hürthle Cell Carcinoma
Inadequateuptake
Adequateuptake
TSH + thyroglobulinmeasurement +antithyroglobulin
antibodies (1-12 wkpostoperatively)
SeePostsurgicalTherapy(H RT-3)Ü
·
·
·
·
< 1 cm confined toglandNo nodal metastasesNo distant metastasesNon-aggressivehistology
·
·
·
·
1 cmor Nodal metastasesor Distant metastasesor Aggressive histology
³
SeeSurveillanceandMaintenance(H RT-4)Ü
NCCN® Practice G idelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 20/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN® Practice Guidelines
in Oncology – v.2.2007Thyroid Carcinoma TOC
Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
See
SurveillanceandMaintenance(H RT-4)Ü
SuppressTSH withthyroxine
T4 (surgicallyevident extra-thyroidalinvasion) andage > 45 y
All others
Consider RT
H RT-3Ü
Hürthle Cell Carcinoma
Adjuvant radioiodineablation (30-100 mCi)of thyroid bed(category 2B) andposttreatment scan
RadioiodinemCi
posttreatment scan
treatment(100-200 ) and
POSTSURGICAL THERAPY
1-12 wkpostthyroidectomy:No gross residualdisease in neckwith adequate TSHstimulation (thyroidwithdrawal or recombinant rhTSH
stimulation)
Suspected or provenradioiodine avidresidual tumor
b
c
Suspected or proven thyroidbed uptake
b
Thyroglobulin< 1 ng/mL andradioiodinescan negative
No radioiodinetreatment
Total bodyradioiodinescan(category 2B)
b
cSuspicion based on pathology, postoperative thyroglobulin, and intraoperative findings.
All patients should be examined and palpable neck disease should be surgically resected before radioiodine treatment.
NCCN® Practice Guidelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 21/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCNPractice Guidelinesin Oncology – v.2.2007
Thyroid Carcinoma TOCStaging, MS, References
SURVEILLANCE AND MAINTENANCE
Locoregional recurrence
Metastatic disease
Surgery (preferred) if resectableand/or
Radioiodine treatment, if radioiodine scan positiveand/or RT, if radioiodine scan negative
See Treatment of Metastases (H RT-5)Ü
RECURRENT DISEASE
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
d
If there is a high likelihood of therapy, thyroid hormone withdrawal suggested; if not, suggest using rhTSH.
H RT-4Ü
Hürthle Cell Carcinoma
·
·
·
·
·
Physical examination, TSH and thyroglobulinmeasurement + antithyroglobulin antibodies at6 and 12 mo, then annually if disease-free
Consider additional nonradioiodine imaging(eg, FDG PET ± CT if Tg 10 ng/mL), if Iscans negative and stimulated Tg > 2-5 ng/mL
Periodic neck ultrasound
TSH stimulated thyroglobulin without
radioiodine scan at 12 mo in patientspreviously treated with RAI with recentnegative neck ultrasound and undetectableTSH suppressed thyroglobulin (anti-thyroglobulin antibody negative) and T1-2, N0-1, M0 at initial staging
If detectable thyroglobulin, distant metastases
or soft tissue invasion on initial staging,radioiodine scan every 12 mo until noradioactive iodine avid tumor is evident (either withdrawal of thyroid hormone or rhTSH)d
131³
·
·
·
Stimulated Tg 1-10 ng/mLNon-resectable tumorsNon-radioiodine avid
Suppress TSH with thyroxine
·
·
Thyroglobulin > 10 ng mLthyroid hormone)
Scans (including PET)
negative
/(off
Consider therapywith 100-150 mCi, posttreatment
I scan (category 2B)
radioiodine
131
NCCN® Practice Guidelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 22/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCNPractice Guidelinesin Oncology – v.2.2007
Thyroid Carcinoma TOCStaging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
TREATMENT OF METASTASES
Solitary CNSConsider neurosurgical resection
RTand/or
Bone
·
·
·
Surgical resection, if symptomatic or asymptomatic in weight-bearing extremitiesand/or RTConsider bisphosphonate therapy
Consider embolization of metastases
Other
extracervical sites
Consider surgical resection of selected, enlarging,or symptomatic metastasesand/or Radioiodine if positive uptake, with considerationof dosimetry to maximize dosing
and/or Clinical trials for non-radioiodine avid tumors;systemic therapy if not in clinical trialor Best Supportive Care
e
H RT-5Ü
Hürthle Cell Carcinoma
eCytotoxic chemotherapy has shown to have minimal efficacy. There are agents in clinical trials investigating novel targeted
therapies. See Clinical trials available at the NCCN member institutions.
Metastatic disease· Continue to suppress
TSH with thyroxine
NCCN® Practice Guidelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 23/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCNPractice Guidelinesin Oncology – v.2.2007
y o d Ca c o a OCStaging, MS, ReferencesMedullary Carcinoma
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
MEDU-1
Medullarythyroidcarcinomaon FNA
···
··
··
·
Calcitonin levelCEAPheochromocytomascreeningSerum calciumScreen for RET proto-oncogene mutations(exons 10, 11, 13-16)
Consider neck ultrasoundEvaluate vocal cordmobility (category 2B)Contrast-enhanced CT of chest and mediastinum
ab
³ 1.0 cm in
diameter or bilateralthyroid disease
< 1.0 cm indiameter andunilateralthyroid disease
·
·
·
Total thyroidectomy withbilateral central (level VI)Consider ipsilateral modifiedradical neck dissection (levels
II–V). Consider contralateralneck dissection if diseasepresent in ipsilateral neck(levels II, III, IV or V)Consider adjuvant RT for T4disease
Total thyroidectomy plusbilateral central neckdissection (level VI)
CLINICALPRESENTATION
ADDITIONAL WORKUP PRIMARY TREATMENT
SeeManagement2-3 MonthsPostoperative
(MEDU-4)
See Additional Workupand Primary Treatment(MEDU-2)
Germline
mutation of RET proto-oncogene
a
bGermline mutation should prompt family testing of first-degree relatives and counseling.
If exons 10, 11, 13-16 negative, evaluate for exon 8.
NCCN® Practice Guidelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 24/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCNPractice Guidelinesin Oncology – v.2.2007
yStaging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
CLINICALPRESENTATION
ADDITIONAL WORKUP PRIMARY TREATMENT
Germlinemutation of RETproto-oncogene
MEN 2B(codon 883, 918, or 922 RET mutations)
MEN 2Aor Familial medullarythyroid carcinoma(codon 609, 611, 618,620, 630, 634, 768,790, 791, 804 or 891 RET mutations)
cc c c
··
·
Calcitonin levelCEA
Pheochromocytomascreeningd,e
··
····
Basal calcitonin levelCalcium stimulated calcitonin test if calcitoninundetectable (category 2B for use in timing of surgery)CEAPheochromocytoma screeningSerum calciumConsider neck ultrasound (category 2B)
d,e
c
d
e
Lethality of medullary thyroid carcinoma associated with codon 768, 790, 791, and 804 RET mutations may be lower than with other RET mutations. In patients withthese RET mutations, annual provocative (calcium) calcitonin testing may be performed, with total thyroidectomy and central node dissection deferred until testsbecome abnormal after the age of 5. Brandi ML, Gagel RF, Angeli A, et al. Consensus: Guidelines for diagnosis and therapy of MEN type 1 and type 2. J ClinEndocrinol Metab 2002;87(6)5658-71.Evidence of pheochromocytoma should be evaluated and treated appropriately before proceeding to the next step on the pathway.Screening for pheochromocytoma (MEN 2A and 2B) and hyperparathyroidism (MEN 2A) should be performed annually. For some RET mutations (codons 768, 790,
V804M, or 891) less frequent screening may be appropriate.
·
·
·
Total thyroidectomy during the firstyear of life or at diagnosis + bilateralcentral neck dissection (level VI)Consider more extensive nodedissection (levels II–V) if tumor(s)> 0.5 cm in diameter Consider adjuvant RT for T4 disease
See PrimaryTreatment(MEDU-3)
SeeManagement2-3 MonthsPostoperative(MEDU-4)
MEDU-2
Medullary Carcinoma
NCCN® Practice Guidelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 25/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN in Oncology – v.2.2007 Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Measureserum intactparathyroidhormone
Notsuppressed
Suppressed
Evaluate for other causesof hyper-calcemia
·
·
·
·
Total thyroidectomy by age 5 or when mutationidentifiedConsider bilateral central neck dissection (levelVI) if elevated calcitonin or CEA test or ultrasound identified thyroid or nodal abnormalityConsider more extensive lymph node dissection(levels II–V) if tumor(s) > 1.0 cm or central node(s)positiveConsider adjuvant RT for T4 disease in adults
c
·
·
·
·
·
Total thyroidectomy by age 5 or when mutationidentifiedConsider bilateral central neck dissection (levelVI) if elevated calcitonin or CEA test or ultrasoundidentified thyroid or nodal abnormalityConsider more extensive lymph node dissection(levels II–V) if tumor(s) > 1.0 cm or central node(s)positiveDuring primary operative procedure andparathyroid exploration:
If single adenoma, exciseIf multiglandular hyperplasia, leave, or autotransplant the equivalent mass of onenormal parathyroidConsider cryopreservation of parathyroid tissue
Consider adjuvant RT for T4 disease in adults
c
?
?
?
MEN 2Aor Familialmedullarythyroidcarcinoma
PRIMARY TREATMENT
SeeManagement2-3 MonthsPostoperative(MEDU-4)
CLINICALPRESENTATION
SeeManagement2-3 MonthsPostoperative(MEDU-4)
MEDU-3
cLethality of medullary thyroid carcinoma associated with codon 768, 790, 791, and 804 RET mutations may be lower than with other RET mutations.In patients with these RET mutations, annual provocative (calcium) calcitonin testing may be performed, with total thyroidectomy and central nodedissection deferred until tests become abnormal after the age of 5. Brandi ML, Gagel RF, Angeli A, et al. Consensus: Guidelines for diagnosis andtherapy of MEN type 1 and type 2. J Clin Endocrinol Metab 2002;87(6)5658-71.
Medullary Carcinoma
NCCN® Practice Guidelines
Guidelines IndexThyroid Carcinoma TOC
Thyroid Carcinoma
M d ll C i

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 26/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN in Oncology – v.2.2007 Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
·
·
BasalcalcitoninCEA
Elevatedor
positive
Normalor negative f
·
·
Consider additionalimagingContrast-enhanced CT or
MRI of the neck,chest, abdomenwith liver protocol
MANAGEMENT2-3 MONTHSPOSTOPERATIVE
SURVEILLANCE
Observe
Imagingpositive or symptomaticdisease
Imagingnegative andasymptomatic
See Recurrent or PersistentDisease (MEDU-5)
···
·
·
Annual serum calcitonin, CEAConsider neck ultrasoundAdditional studies or more frequenttesting if significantly risingcalcitonin or CEANo additional imaging required if calcitonin and CEA stable
For MEN 2B or 2A, annualscreenings for pheochromocytomaand hyperparathyroidism(MEN 2A)
Continueobservationor Consider cervicalreoperation, if
primary surgeryincomplete
Continue observation
·
·
·
Annual serumcalcitonin, CEAAdditional studies or more frequent testingif significantly risingcalcitonin or CEANo additional imagingrequired if calcitoninand CEA stable
See Recurrent or Persistent Disease(MEDU-5)
Imagingpositive
Imagingnegative
Imagingpositive
Imagingnegative
f The likelihood of significant residual disease with a negative basal calcitonin is very low.
See Recurrent or
Persistent Disease(MEDU-5)
MEDU-4
Medullary Carcinoma
NCCN® Practice Guidelines
i O l 2 2007
Guidelines IndexThyroid Carcinoma TOC
St i MS R f
Thyroid Carcinoma
M d ll C i

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 27/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN in Oncology – v.2.2007 Staging, MS, References
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Locoregional
Symptomatic,distant metastases
Asymptomatic,distant metastases
Surgical resection ±postoperative RTor RT, if symptomatic progressivedisease or unresectable
Consider palliative resection,ablation (eg, radiofrequency[RFA], embolization or other regional therapy) or other regional treatment
Disseminatedsymptomaticdisease
·
·
·
Clinical trial (preferred)or RT for focal symptomsor DTIC-based chemotherapyConsider bisphosphonatetherapy for bone metastasesBest Supportive Care
RECURRENT OR PERSISTENT DISEASE
Observeor Consider resection, if possible,or ablation (eg, RFA,embolization or other regionaltherapy) especially if progressive disease
MEDU-5
Medullary Carcinoma
NCCN® Practice Guidelines
i O l 2 2007
Guidelines IndexThyroid Carcinoma TOC
Staging MS References
Thyroid Carcinoma
Anaplastic Carcinoma

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 28/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN in Oncology – v.2.2007 Staging, MS, ReferencesAnaplastic Carcinoma
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged.
Anaplasticcarcinoma a
FNA OR COREBIOPSY FINDING
DIAGNOSTICPROCEDURES
PRIMARY TREATMENT
···
·
CBCSerum calciumHead, neck,chest, abdomen,pelvis CTTSH
Locally resectable(rarelyencountered)
Unresectable
local tumor
·
·
Total or near-totalthyroidectomySelective resection of involved local or regionalstructures and lymph nodes
·
·
·
Clinical trials preferredRT (consider hyperfractionation) +chemotherapyBest Supportive Care
ANAP-1
a An FNA diagnosis of anaplastic carcinoma should be confirmed by core biopsy.

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 29/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 30/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 31/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 32/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 33/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 34/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 35/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 36/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 37/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 38/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 39/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 40/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 41/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 42/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 43/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 44/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 45/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 46/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 47/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 48/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 49/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 50/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 51/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 52/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 53/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 54/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 55/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 56/68
Guidelines Index
Thyroid Carcinoma TOCStaging, MS, References
Practice Guidelinesin Oncology – v.2.2007 Thyroid Carcinoma
NCCN
®

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 57/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN. MS-28
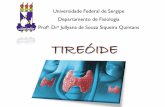
Tumor Size and Recurrence ( )
or Cancer Death ( )
Maximum Tumor Diameter (cm)Patients at Risk
P e r c e n t
R e c u r r e n c e o r C a n c e r
D e a t h
<1
30
25
20
15
10
5
0
1-1.9 2-2.9 3-3.9 4-4.9 5-5.9
106 281 320 174 98 135
Recurrence
R =0.672
Cancer Death
R =0.672
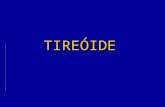
Recurrence ( ) and Cancer Deaths ( )
According to Age at Time of Diagnosis
Age at DiagnosisPatients at Risk
E v e n t s p e r D e c a d e ( % ) Recurrence
Cancer Death
0-9
60
50
40
30
20
10
0
10-19 20-29 30-39 40-49 50-59 60-69 70-91
11 95 440 363 224 118 60 40
Figure 1:
Relationship of cancer recurrence and mortality to patient age attime of diagnosis
(Reprinted and adapted from AM J Med, 97, Mazzaferri EL and
Jhiang SM, Long-term impact of initial surgical and medical therapy
on papillary and follicular thyroid cancer, pp 418-428, 1994, with
permission from Excerpta Medica Inc.).
Figure 2:
Relationship of cancer recurrence and mortality to tumor size
(Reprinted and adapted from AM J Med, 97, Mazzaferri EL and
Jhiang SM, Long-term impact of initial surgical and medical therapy
on papillary and follicular thyroid cancer, pp 418-428, 1994, with
permission from Excerpta Medica Inc.).
Guidelines Index
Thyroid Carcinoma TOCStaging, MS, References
Practice Guidelinesin Oncology – v.2.2007 Thyroid Carcinoma
NCCN
®

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 58/68
Version 2.2007, 04/20/07 © 2007 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN. MS-29
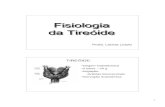
Table 2
Mutations of the RET Proto-oncogene Associated with MEN 2 and
Familial Medullary Thyroid Cancer (FMTC)
Affected Clinical Percentage of All
Codon/Exon Syndrome(s) MEN 2 Mutations
609/10 MEN 2A, FMTC 0 - 1%
611/10 MEN 2A, FMTC 2 - 3%
618/10 MEN 2A, FMTC 3 - 5%
620/10 MEN 2A, FMTC 6 - 8%
630/11 MEN 2A, FMTC 0 - 1%
634/11 MEN 2A 80-90%
635/11 MEN 2A Rare
637/11 MEN 2A Rare768/13 FMTC Rare
790/13 MEN 2A, FMTC Rare
791/13 FMTC Rare
804/13 MEN 2A, FMTC 0 - 1%
883/15 MEN 2B Rare
891/15 FMTC Rare
918/16 MEN 2B 3 - 5%922/16 MEN 2B Rare
With permission, from the , Volume
62:377-411 ©2000 by Annual Reviews
Annual Review of Physiology
www.AnnualReviews.org

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 59/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 60/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 61/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 62/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 63/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 64/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 65/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 66/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 67/68

7/30/2019 DIRETRIZ CÂNCER DE TIREÓIDE
http://slidepdf.com/reader/full/diretriz-cancer-de-tireoide 68/68