EPIDEMIOLOGIA DAS RECÍDAS - SBTMO · • Epidemiologia é o método usado para encontrar causas de...
38
EPIDEMIOLOGIA DAS RECAÍDAS Prof. Dr. Wellington Morais de Azevedo 2019
Transcript of EPIDEMIOLOGIA DAS RECÍDAS - SBTMO · • Epidemiologia é o método usado para encontrar causas de...

EPIDEMIOLOGIA DAS RECAÍDAS
Prof. Dr. Wellington Morais de Azevedo
2019

2
• Epidemiologia é o método usado para encontrar causas de
desfechos em eventos de saúde em populações. Pela
epidemiologia indivíduos são vistos coletivamente. Isso é o estudo
(científico, sistemático e derivado de dados) da distribuição
(frequencia, padrão) e determinantes (causas, fatores de risco) do
estado de saúde e eventos relacionados em uma população
específica. (Principles of Epidemiology, 3rd Edition).
• Epidemiologia Clinica: estuda a frequência e determinantes do
desenvolvimento de doenças, assim como as abordagens
diagnósticas e terapêuticas ao manejo clinico na prática clínica.

MM; 134
LNH; 51
LH; 46
LMA; 27
LLA; 25
SMD; 19
AAS; 11 OUTRAS; 9 LMMC; 3
211; 65%
89; 27%
19; 6% 6; 2%
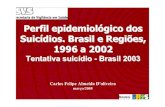
TRANSPLANTES REALIZADOS EM 2010 A 2018 (N = 325)
Autólogo Aparentado Não Aparentado Haplo

21; 44%
14; 29%
8; 17%
4; 8%
1; 2%
Recaída é a principal causa de Morte nos TCTH Alogênicos 2010 a 2018 (N114)
Recaida
MRT
GvHD
Infecção
Falha de pega

MRT
Óbito sem recaídaRecaída

INCIDÊNCIA DE RECAÍDA
RecaídaÓbito sem recaída

SOBREVIDA GLOBAL

SOBREVIDA LIVRE DE RECAÍDA

SOBREVIDA APÓS RECAÍDA
Mediana = 40 dias

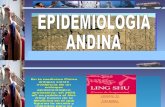
3 Year Outcomes after Allogeneic HCT for HematologicMalignancy
80
70
60
50
40
30
20
10
0
1980-89
(N=11,104)
1990-99
(N=47,781)
2000-09
(N=64,148)
2010-16
(N=57,936)
TRM Relapse Treatment Failure (TRM+Relapse)
10

Relapse is the Single Most Common Causes of
Death after Transplants done in 2014-2015
80%
70%
60%
50%
40%
30%
20%
10%
0%
Autotransplants HLA-identical sibs Unrelated donor
Relapse GVHDInfection Organ failureOther
11

Probability of Relapse after 2,254 HCTs for Early Leukemia

Median Age of HCT Recipients
60
50
40
30
20
10
0
Allo
1980-89 1990-99 2000-09
Auto
2010-16
13

Changes in Disease Indications - Allotransplants
1980-89 1990-99 2000-09 2010-16
60%
AML MDS ALL CML Lymphoma Myeloma
50%
40%
30%
20%
10%
0%
14

Changes in Conditioning Regimen Intensity - Allotransplants
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
1980-89 1990-99 2010-16
Myeloablative
2000-09
Less Intensive
15

Allogeneic HCT for Hematologic Malignancy, 2010-2016(N=40,109)
Cu
mu
lative
Incid
en
ce
,%
Years
40
100
80
60
0 2 5431
Relapse
NRM20
0
16

Allogeneic HCT for Leukemia / MDS, 2010-2016
Years
100
0
20
40
60
80
0 2 5431
Relapse
NRM
Years
100
0
20
40
60
80
0 2 5431
Relapse
NRM
CR1 or Early MDS More Advanced

5-Year outcomes after HCT for AML
80
70
60
50
40
30
20
10
0
1980-89 1990-99 2000-09 2010-16
TRM Relapse Treatment Failure (TRM+Relapse)
18

Outcomes after HCT for AMLin CR1, Age 20-45, MyeloablativeConditioning
80
70
60
50
40
30
20
10
0
1980-89 1990-99 2000-09 2010-16
TRM Relapse Treatment Failure (TRM+Relapse)
19

20
• Em 2019 as recaídas ainda constituem a principal causa
de falha dos transplantes de medula óssea, autólogos e
alogênicos
• Nós não somos muito bons em prever quais pacientes
vão recair
• O efeito GVL/GVT e a intensificação de doses tem sido
explorados mas sua importância varia de doença para
doença, dentre outros fatores
• Não é razoável esperar resultados diferentes dos atuais
enquanto continuarmos a fazer as mesmas coisas

Mudança de dogma do TMO
“HLA matching” como uma condição “sine qua non” (1970-1990)
Incompatibilitdades não são mais uma barrreira (1990-presente)
O futuro : Explorar “mismatches” para melhorar os resultados ?
“Imunoterapia”

Do Patients Destined to Relapse in the 1st Year after AlloHCT Year Look Different Pretransplant from Those Who Will Survive Relapse-free >1 Year?
Characteristic Relapse <1 year after HCT Alive, Relapse-free > 1 year
Age
<20 years
20-39 years
40-59 years
60+ years
10%
17%
38%
35%
13%
20%
37%
30%
Non-Caucasian 15% 13%
PreHCT Performance
Score <80
15% 10%
HCT-Comorbidity Index >2 48% 42%
Prior Malignancy 5% 4%
Prior Autotransplant 4% 3% 26

Do Patients Destined to Relapse in the 1st Year after AlloHCT Year Look Different Pretransplant from Those Who Will Survive Relapse-free >1 Year?
Characteristic Relapse <1 year after HCT Alive, Relapse-free > 1 year
Disease
AML
ALL
CML
MDS
Lymphoma
Myeloma
52%
15%
4%
15%
12%
1%
47%
21%
4%
16%
11%
1%
Disease stage
Early
Intermediate
Advanced
46%
23%
31%
62%
20%
18%
23

Do Patients Destined to Relapse in the 1st Year after AlloHCT Year Look Different Pretransplant from Those Who Will Survive Relapse-free >1 Year?
Characteristic Relapse <1 year after HCT Alive, Relapse-free > 1 year
AML Cytogenetic Risk
Good
Intermediate
Poor
4%
62%
34%
8%
71%
21%
ALL Cytogenetic Risk
Good
Intermediate
Poor
35%
45%
20%
35%
48%
17%
MDS Cytogenetic Risk
Good
Intermediate
Poor
31%
19%
49%
52%
20%
28%24

Do Patients Destined to Relapse in the 1st Year after AlloHCT Year Look Different Pretransplant from Those Who Will Survive Relapse-free >1 Year?
Molecular mutations Relapse <1 year after HCT Alive, Relapse-free > 1 year
AML
CEBPA
NPM1
FLT3-ITD
c-KIT
8%
24%
28%
5%
9%
26%
23%
6%
ALL
BCR/ABL 36% 40%
25

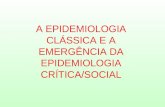
Relapse and Survival by FLT3 Mutation Status
(Doel et al, Cancer, 2016)
Relapse Survival

TP53 mutated MDS: Poor prognosis due to early relapse
(Lindsley, et al, NEJM 2017)
MDS
No
TP53 mutation
TP53 mutationMedian OS = 8
months
TP53 mutation
Survival
No TP53
mutation
TP53 mutation
No TP53
mutation
p < 0.0001
p < 0.0001
Relapse

TP53 mutation : Myeloablative conditioning does not
improve outcome
28

RAS pathway mutation: Myeloablative conditioning improves
survival and reduces relapse
29

Pro
bab
tili
0.0
0.2
0.4
0.6
1.0
0.8
y
0 1 2 3 4 5 6 7 8
Yearspost-SCT
JAK2 and RAS pathway mutations in patients without
TP53 mutations (Lindsley, et al, NEJM 2017)
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5 6 7 8
Pro
bab
ility
JAK2 V617F
Poor prognosis driven by
NRMNRM
p < 0.001
Relapse
p < 0.001
RAS pathway
Poor prognosis driven by
relapse
NoTP53mutation
Age ?40 Age <40
p <0.0001
RAS pathwaymutation*
Median OS = 11months
NoRASpathway
mutation
JAK2 V617FMedian OS= 6months
No RASpathway or JAK2mutationMedian OS= 2.3 years
P =0.004
P =0.001
*RAS pathway: NRAS, KRAS, CBL, PTPN11, NF1, RIT1, KIT,FLT3


Does Dose-Intensification Matter? Allotransplants for
DLBCL (Bacher, et al. Blood 2016)
0.0
0.5
1.0
1.5
2.0
2.5
Relapse TRM Treatment Failure Mortality
Myeloablative (n=165)
RIC (n=143)
NST (n=88)
32

(A) Overall survival (OS) and incidence of relapse by treatment armand (B) relapse-free survival (RFS)..
Incidence of TRM by treatment arm
More GVHD in MAC arm
Impact of Conditioning Intensity on Transplant Outcome forAML/MDS (BMT CTN 0901, Scott, et al JCO 2017)

Very Late Relapses AfterAlloHCT
34
Total
Relapses
>5 years >10
years
>15
years
AML 7574 209 46 19
ALL 4603 30 9 7
CML 3646 311 78 24
MDS 768 28 8 1
NHL 1201 30 6 2
Myeloma 1191 29 6 2

RECAÍDA ? QUAL RECAÍDA ?
35

EVOLUÇÃO CLONAL CONTINUA APÓS O TMO
Quek, Blood Adv, 2016
Cristopher, N Engl J Med, 2018

Recaída pós transplante: modalidades
Zeiser and Vago, Blood , 2019

Recaída pós transplante: modalidades• Perda do haplótipo HLA
Genomico, irreversívelPrincipalmente após Haplo (25-30%) > não relacionado > cordãoTerapia: no DLIs, “doador Haplo alternativo”, BiTEs? CAR-T cells?
• "Downregulation" de moléculas HLA class IITranscripcional, reversível(epigenética) Todos os tipos de transplantes (40%)Terapia: indução de liberação de IFN-γ (GVHD?)
• "Upregulation" de "T cell inhibitory ligands"Transcripicional, reversível (epigenética)Todos os tipos de transplantes (20%? Difícil de abordar, padrões complexos de combinações complexos)Terapia: Bloqueadores de checkpoint
A biologia das recaídas devem informar abordagens pela “medicina de precisão”