1_1 epidemiologia

of 16
-
Upload
raul-gascuena -
Category
Documents
-
view
233 -
download
0
Transcript of 1_1 epidemiologia
-
7/27/2019 1_1 epidemiologia
1/16
1.1: Global Burden of Cardiovascular Disease 1.1.1
The rst stage, pestilence and amine , is characterized by thepredominance o malnutrition and in ectious disease and by thein requency o CVD as a cause o death. Tuberculosis, dysentery,cholera, and infuenza are o ten atal, resulting in a mean li eexpectancy o about 30 years. CVD, which accounts or
-
7/27/2019 1_1 epidemiologia
2/16
1.1.2 Chapter 1: General Principles
deaths exceeds that o stroke by a ratio o 2:1 to 3:1. Duringthis period, average li e expectancy surpasses age 50. Roughly35% o the worlds population alls into this category.
In the age o delayed degenerative diseases , CVD and cancerremain the major causes o morbidity and mortality, with CVD
accounting or 40% o all deaths. However, reductions in risk be-haviors and actors such as smoking cessation programs and e -
ective blood pressure control make even greater contributions tothe decline in age-adjusted rates o death. Further, these reduc-tions are aided by improvements in acute hospital managementand technological advances, such as the availability o bypasssurgery. CHD, stroke, and congestive heart ailure are the primary
orms o CVD. About 15% o the worlds population is now inthe age o delayed degenerative diseases or is exiting this age andmoving into the th stage o the epidemiologic transition.
Per capita income and li e expectancy increase during the age o receding pandemics as the emergence o public health systems,cleaner water supplies, and improved nutrition combine to drivedown deaths rom in ectious disease and malnutrition. Thechange most characteristic o this phase is a precipitous declinein in ant and child mortality accompanied by a substantial in-
crease in li e expectancy. Deaths due to CVD (rheumatic valvulardisease, hypertension, and stroke) increase to between 10%and 35% o all deaths. Almost 40% o the worlds population iscurrently in this stage.
The age o degenerative and man-made diseases is distin-guished by mortality rom noncommunicable diseasesprimar-ily CVDsurpassing mortality rom malnutrition and in ectiousdiseases. Caloric intake, particularly rom animal at, increases.CHD and stroke are prevalent, and between 35% and 65%o all deaths can be traced to CVD. Typically, the rate o CHD
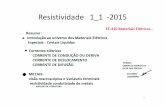
Table 1Stages o the Epidemiological Transition and Its Global Status, by Region
CVD = cardiovascular disease.Reproduced with permission rom Gaziano TA, Gaziano JM. Global burden o cardiovascular disease. In: Bonow RO, Mann DL, Zipes DP, Libby P.Braunwalds Heart Disease: A Textbook o Cardiovascular Medicine. 9th ed. Philadelphia: Saunders; 2011.
Stages of the Epidemiological Transition and Its Global Status, by Region
Pestilenceand famine
Recedingpandemics
Degenerativeand man-madediseases
Delayeddegenerativediseases
Predominance of malnutrition andinfectious diseases
Improved nutrition andpublic health leads toincrease in chronicdiseases, hypertension
Increased fat andcaloric intake,widespread tobaccouse, chronic diseasedeaths exceedmortality frominfections andmalnutrition
CVD and cancer areleading causes of morbidity andmortality, preventionand treatment avoidsdeath and delaysonset; age-adjustedCVD declines
35
50
60
>70
Rheumatic heartdisease,cardiomyopathy dueto infection andmalnutrition
Rheumatic valvulardisease, ischemicheart disease (IHD),hemorrhagic stroke
IHD, stroke (ischemicand hemorrhagic)
IHD, stroke (ischemicand hemorrhagic),congestive heartfailure
-
7/27/2019 1_1 epidemiologia
3/16
1.1: Global Burden of Cardiovascular Disease 1.1.3
Troubling trends in certain risk behaviors and risk actors mayoreshadow a new phase o the epidemiologic transition,
the age o inactivity and obesity .2 In the industrialized world,physical activity continues to decline while total caloric intakeincreases. Rates o type 2 diabetes mellitus, hypertension, andlipid abnormalities are on the rise, trends that are particularlyevident in children. I these trends continue, age-adjusted CVDmortality rates, which have declined over the past several de-cades in developed countries, could level or even increase in thecoming years.
Current Worldwide Variations inBurden o Cardiovascular Disease
An epidemiologic transition much like the one that occurred inthe developed countries is occurring throughout the world, butunique regional eatures have modi ed aspects o the transi-tion in various parts o the world. The rate o transition varieswidely, leading to large discrepancies in disease burden. In termso economic development, the world can be divided into twobroad categories: 1) high-income countries and 2) low- andmiddle-income countries, which can be urther subdivided intosix distinct economic/geographic regions. Currently, 85% o the
worlds population lives in low- and middle-income countries,and it is these countries that are driving the rates o change inthe global burden o CVD.
High-Income Countries Nearly 1 billion people live in the high-income countries, whereCHD is the dominant orm o CVD, with rates that tend to betwo- to ve- old higher than stroke rates. The rates o CVD inCanada, New Zealand, Australia, and Western Europe tend tobe similar to those in the United States; however, among thecountries o Western Europe, the absolute rates vary three- old,with a clear north/south gradient. The highest CVD death rates
are in the northern countries, such as Finland, Ireland, and Scot-land, with the lowest CVD rates in the Mediterranean countrieso France, Spain, and Italy.
Japan is unique among the high-income countries: Stroke ratesincreased dramatically, but CHD rates did not rise as sharply overthe last century. This di erence may stem in part rom genetic
actors, but it is more likely that the sh- and plant-based,low- at diet and resulting low cholesterol levels have played alarger role. Importantly, Japanese dietary habits are undergoing
substantial changes refected in an increase in cholesterol levels.
Low- and Middle-Income Countries The World Bank groups the low- and middle-income countries(gross national income per capita less than US $12,195) into sixgeographic regions, as ollows:
1. East Asia and the Paci c,
2. Eastern Europe and Central Asia,
3. Latin America and the Caribbean,
4. Middle East and North A rica,
5. South Asia, and
6. Sub-Saharan A rica.
Although communicable diseases continue to be a major causeo death, CVD has emerged as a signi cant health concern inthe low- and middle-income countries. In most, an urban/ruralgradient has emerged or CHD, stroke, and hypertension, withhigher rates in urban centers.
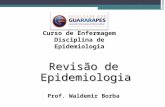
Figure 2Major Causes o Death in Personso All Ages orLow- and Middle-Income Regions
Reproduced with permission rom Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ, eds. Global Burdeno Disease and Risk Factors. New York: TheWorld Bank and Ox ord University Press; 2006.
60
Cardiovascular DiseasesRespiratory Infections
Malignant NeoplasmsChronic Lung Diseases
InjuriesHIV/AIDS
Major Causes of Death in Persons of All Agesfor Low- and Middle-Income Regions
50
40
30
10
0
20
Europe &Central Asia
Middle East &North Africa
East Asia &Pacic
Latin America &Caribbean
South Asia Sub-SaharanAfrica
P e r c e n
t o
f T o
t a l D e a
t h s
-
7/27/2019 1_1 epidemiologia
4/16
1.1.4 Chapter 1: General Principles
While CVD rates are rapidly rising, vast di erences exist amongthe regions ( Figure 2 ) and countries, and even within the coun-tries themselves. Many actors contribute to this heterogeneity.First, the regions are in various stages o the epidemiologicaltransition. Second, vast di erences in li estyle and behavioralrisk actors exist. Third, racial and ethnic di erences may leadto altered susceptibilities to various orms o CVD. In addition,it should be noted that or most countries in these regions,accurate country-wide data on cause-speci c mortality are notcomplete, as death certi cate completion is not routine, andmost countries do not have a centralized registry or deaths.
East Asia and Pacific RegionThe East Asia and Paci c region, home to nearly 2 billionpeople, appears to be straddling the second and third phaseso the epidemiological transition, with China, Indonesia, and SriLankas large combined population driving most o the trends.Overall, CVD is a major cause o death in China, but, like Japan,stroke (particularly hemorrhagic) causes more deaths than CHD,in a ratio o about 3:1. However, age-adjusted CHD mortalityincreased 40% rom 1984 to 1999, suggesting urther epide-miologic transition.
China also appears to have a geographic gradient like that oWestern Europe with higher CVD rates in northern China thanin southern China by a actor o six. Other countries, such asVietnam and Cambodia, are just emerging rom the pestilenceand amine transition.
Eastern Europe and Central AsiaThe Eastern Europe and Central Asia region is rmly in the peako the third phase, with the highest death rates (58%) due toCVD in the world, nearly double the rate o some high-incomecountries. More troubling is that nearly 35% o the deaths romCHD occur among working-age adults, which is three times therate o the United States.
In Russia, increased CVD rates have contributed to alling li eexpectancy, particularly or men, whose li e expectancy hasdropped rom age 71.6 years in 1986 to 59 years today. In Po-land, by contrast, the age-adjusted mortality rate decreased byapproximately 30% or men during the 1990s and slightly moreamong women. Slovenia, Hungary, the Czech Republic, andSlovakia have had similar declines.
Latin America and the CaribbeanIn general, Latin America appears to be in the third phase othe epidemiological transition, although as in other low- andmiddle-income regions, there is vast regional heterogeneity, withsome areas in the second phase o the transition and some inthe ourth. Today, approximately 28% o all deaths in this regionare attributable to CVD, with CHD rates higher than strokerates. Like Eastern Europe, some countriesMexico, Costa Rica,and Venezuelacontinued an overall increase in age-adjustedCHD mortality o 310% between 1970 and 2002, while in oth-ers-Argentina, Brazil, Chile, and Columbia-rates appear to havedeclined by as much as 2% per year over the same time period.
Middle East and North AfricaThe Middle East and North A rica region appears to be enteringthe third phase o the epidemiological transition, with increas-ing li e expectancy overall and CVD death rates just belowdeveloped nations. CHD is responsible or 17% o all deaths,and stroke or 7%. The traditional high- ber diet, low in at andcholesterol, has changed rapidly. Over the past ew decades,daily at consumption has increased in most o these countries,ranging rom a 13.6% increase in Sudan to a 143.3% increasein Saudi Arabia. Over 75% o Egyptians are overweight orobese, and the rate is 67% in Iraq and Jordan. Nearly 60% oSyrians and Iraqis report that they are physically inactive (50%. This is somewhatunexpected because stroke tends to be a more dominant actorearly in the epidemiological transition. This nding may refectinaccuracies in cause-speci c mortality estimates or possibly anunderlying genetic component.
It has been suggested that Indians have exaggerated insulininsensitivity in response to the Western li estyle pattern that maydi erentially increase rates o CHD over stroke. The South Asiaregion has the highest overall prevalence o diabetes in the low-income regions, with rates as high as 14% in urban centers. Incertain rural areas, the prevalence o CVD and its risk actors areapproaching urban rates. Nonetheless, rheumatic heart diseasecontinues to be a major cause o morbidity and mortality.
Sub-Saharan AfricaFor the most part, Sub-Saharan A rica remains in the rst phase othe epidemiological transition with CVD rates one-quarter o thosein developed nations. This area remains the only region where CVDis not the leading cause o death. Li e expectancy has decreasedby an average o 5 years since the early 1990s, largely because ohuman immunode ciency virus (HIV)/acquired immunode ciencysyndrome (AIDS) and other chronic diseases, according to theWorld Bank; li e expectancies are the lowest in the world. Still, CVDaccounts or 46% o noncommunicable deaths, and is the leading
cause o death among adults over the age o 35.As more HIV/AIDS patients receive antiretroviral treatment, man-aging CVD risk actors such as dyslipidemia in this populationrequires more attention. However, hypertension continues to bethe major public health concern and has resulted in stroke beingthe dominant orm o CVD. Rheumatic heart disease is still aprominent challenge.
-
7/27/2019 1_1 epidemiologia
5/16
1.1: Global Burden of Cardiovascular Disease 1.1.5
Global Trends in Cardiovascular Disease
In 1990, CVD accounted or 28% o the worlds 50.4 milliondeaths and 9.7% o the 1.4 billion lost DALYs, and by 2001,CVD was responsible or 29% o all deaths and 14% o the 1.5billion lost DALYs. By 2030, when the population is expected toreach 8.2 billion, 33% o all deaths will be the result o CVD. Othese, 14.9% o deaths in men and 13.1% o deaths in womenwill be due to CHD. Stroke will be responsible or 10.4% o allmale deaths and 11.8% o all emale deaths.
In the high-income countries, population growth will be ueledby emigration rom the low- and middle-income countries, butthe populations o high-income countries will shrink as a pro-portion o the worlds population. The modest decline in CVDdeath rates that began in the high-income countries in the latterthird o the 20th century will continue, but the rate o declineappears to be slowing. However, these countries are expected tosee an increase in the prevalence o CVD, as well as the absolutenumber o deaths, as the population ages.
Signi cant portions o the population living in low- and middle-income countries have entered the third phase o the epide-miological transition, and some are entering the ourth stage.Changing demographics play a signi cant role in uture predic-tions or CVD throughout the world. For example, between1990 and 2001, the population o Eastern Europe and CentralAsia grew by 1 million people per year, whereas South Asiaadded 25 million people each year.
CVD rates will also have an economic impact. Even assuming noincrease in CVD risk actors, most countries, but especially Indiaand South A rica, will see a large number o people betweenthe ages o 35 and 64 die o CVD over the next 30 years, aswell as an increasing level o morbidity among middle-agedpeople related to heart disease and stroke. In China, it is esti-mated that there will be 9 million deaths rom CVD in 2030up
rom 2.4 million in 2002with one-hal occurring in individualsbetween 35 and 64 years old.
Risk Factors
As indicated earlier, the global variation in CVD rates is relatedto temporal and regional variations in known risk behaviorsand actors. Ecological analyses o major CVD risk actors andmortality demonstrate high correlations between expected andobserved mortality rates or the three main risk actorssmok-ing, serum cholesterol, and hypertensionand suggest thatmany o the regional variations are based on di erences inconventional risk actors.
HypertensionElevated blood pressure is an early indicator o the epidemiologicaltransition. Worldwide, approximately 54% o strokes and 47%o cases o ischemic heart disease are attributable to suboptimal(>115 mm Hg systolic) blood pressure, which is believed to account
or more than 7 million deaths annually. Remarkably, nearly one-hal o this burden occurs among those with systolic blood pressure
-
7/27/2019 1_1 epidemiologia
6/16
1.1.6 Chapter 1: General Principles
current recommendation). In contrast, in countries like China,physical activity is still integral to everyday li e. Approximately90% o the urban population walks or rides a bicycle to work,shopping, or school daily.
Diabetes As a consequence o , or in addition to, increasing body massindex and decreasing levels o physical activity, worldwide rateso diabetes, predominantly type 2 diabetes, are on the rise. In2003, 194 million adults, or 5% o the worlds population, haddiabetes. By 2025, this number is predicted to increase 72% to333 million. By 2025, the number o people with type 2 diabe-tes is projected to double in three o the six low- and middle-income regions: Middle East and North A rica, South Asia, andSub-Saharan A rica. There appear to be clear genetic suscepti-
bilities to diabetes mellitus o various racial and ethnic groups.For example, migration studies suggest that South Asians andIndians tend to be at higher risk than those o European extrac-tion.
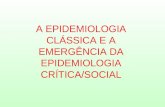
Obesity Although clearly associated with increased risk o CVD ( Figures
3, 4a, b ),4 much o the risk posed by obesity may be mediatedby other CVD risk actors, including hypertension, diabetes mel-litus, and lipid pro le imbalances. In the mid-1980s, the WorldHealth Organizations (WHOs) MONICA Project sampled 48populations or CV risk actors. In all but one male population(China), and in most o the emale populations, between 50%and 75% o adults ages 35-64 years were overweight or obese.
Figure 3Ischemic Heart Disease and Stroke Mortality Versus BMI in the Range 15-50 kg/m 2 (excluding the frst 5 years o ollow-up)
Relative risks at ages 3589 years, adjusted or age at risk, sex, smoking, and study, were multiplied by a common actor (i.e., foated) to make theweighted average match the Prospective Studies Collaboration mortality rate at ages 3579 years. Floated mortality rates shown above each square andnumbers o deaths below. Area o square is inversely proportional to the variance o the log risk. Boundaries o body mass index (BMI) groups are indicatedby tick marks. 95% con dence intervals (CIs) or foated rates refect uncertainty in the log risk or each single rate.
Reproduced with permission rom Whitlock G, Lewington S, Sherliker P, et al., on behal o the Prospective Studies Collaboration. Body-mass index and cause-specifc mortality in 900 000 adults: collaborative analyses o 57 prospective studies. Lancet 2009;373:1083-96.
Ischemic Heart Disease and Stroke Mortality Versus BMI in the Range 15-50 kg/m 2
(excluding the rst 5 years of follow-up)
Y e a r l y
D e a
t h s p e r
1 , 0
0 0 ( 9 5 %
C I )
Baseline BMI (kg/m 2 )
8
4
2
1
0.50 15 20 25 30 35 40 50
Number at Risk 64652 247268 92895 16726 3664 3278179450 195615 41714 7562
37
46
100
646
286
12696
1626
3074
4929
4497
2289675
220
504
837142015071040
417
1.3
1.21.2
1.2
1.3
1.7
2.0
2.2
2.6
2.9
8.3
7.8
6.6
5.8
5.1
4.1
3.5
3.0
2.72.6 Stroke
IschemicHeart Disease
-
7/27/2019 1_1 epidemiologia
7/16
1.1: Global Burden of Cardiovascular Disease 1.1.7
In addition, the prevalence o extreme obesity (body mass index[BMI] >40 kg/m2) more than tripled, increasing rom 1.3% to4.9%.
In many o the low- and middle-income countries, obesityappears to coexist with undernutrition and malnutrition. Obesityis increasing throughout the world, particularly in developingcountries, where the trajectories are steeper than those experi-enced by the developed countries. According to the latest WHOdata, this is equivalent to about 1.3 billion overweight adults inthe world. A survey undertaken in 1998 ound that as many as58% o A rican women living in South A rica may be overweightor obese.
Diet Total caloric intake per capita increases as countries develop.With regard to CVD, a key element o dietary change is anincrease in intake o saturated animal ats and hydrogenatedvegetable ats, which contain atherogenic trans atty acids,along with a decrease in intake o plant-based oods and anincrease in simple carbohydrates.
Fat contributes
-
7/27/2019 1_1 epidemiologia
8/16
1.1.8 Chapter 1: General Principles
percentage o calories derived rom saturated at decreasedrom 13% to 11%.
Scope o InterventionsThe large reductions in age-adjusted CVD mortality rates thathave occurred in high-income countries result rom three com-plementary types o interventions. One strategy targets thosewith acute or established CVD. A second entails risk assessmentand targeting those at high risk due to multiple risk actors orintervention be ore their rst CVD event. The third strategy usesmass education or policy interventions directed at the entirepopulation to reduce the overall level o risk actors.
This section highlights the variety o cost-e ective interven-
tions. Much work remains undone in developing countries todetermine the best strategies given limited resources, but iimplemented, these interventions could go a long way towardreducing the burden. Table 2 lists the cost-e ectiveness ratios
or many o the high-yield interventions that could be or havebeen adopted in developing regions.
Those at highest risk are those su ering an MI or stroke; asmany as one-hal die be ore they ever receive medical atten-tion. For those who do make it to a hospital, standard medicaltherapies were examined in a cost-e ectiveness analysis. 5 Fourincremental strategies were evaluated or the treatment o MIand compared to a strategy o no treatment as a base case orthe six World Bank low- and middle-income regions. The ourstrategies compared were: 1) aspirin; 2) aspirin and atenolol; 3)
M a
l e s
( % )
Prevalence in Males
Baseline BMI (kg/m 2 )
C80
60
40
20
00 15 25 35 50
37.0
46.4
56.9
40.4
31.0
21.1
17.6
10.3
5.8
1.81.8
61.6
11.4
32.932.8
48.2
59.3
69.2
73.2 71.7
66.5
5.8
2.8 2.9
Diabetes
Smoking
Drinking
F e m a
l e s
( % )
Prevalence in Females
Baseline BMI (kg/m 2 )
D80
60
40
20
00 15 25 35 50
Diabetes
Smoking
Drinking
Vascular Risk Factors Versus BMI at Baselinein the Range 15-50 kg/m 2 (2 of 2)
Males
Females
Figure 4bVascular Risk Factors Versus BMI at Baseline in the Range 1550 kg/m 2 (2 o 2)
Adjusted or baseline age, baseline smoking status (apart rom the smoking ndings), and study. Numerical values are shown or 2022.5 kg/m 2, or
3032.5 kg/m2,
and or the extreme body mass index (BMI) groups. Boundaries o BMI groups are indicated by tick marks. 95% con dence intervals (CIs)are not shown, but most are narrower than the heights o the plotted symbols.
(C) Prevalence in males or alcohol drinking (168,283), cigarette smoking (334,496), and diabetes (378,854).
(D) Prevalences in emales or alcohol drinking (129,301), cigarette smoking (226,307), and diabetes (319,401).
Reproduced with permission rom Whitlock G, Lewington S, Sherliker P, et al., on behal o the Prospective Studies Collaboration. Body-mass index andcause-speci c mortality in 900 000 adults: collaborative analyses o 57 prospective studies. Lancet 2009;373:1083-96.
-
7/27/2019 1_1 epidemiologia
9/16
1.1: Global Burden of Cardiovascular Disease 1.1.9
aspirin, atenolol, and streptokinase; and 4) aspirin, atenolol, andtissue plasminogen activator (t-PA).
The incremental cost per Quality o Adjusted Li e Years (QALY)gained or both the aspirin and beta-blocker interventions wasunder $25 or all six regions. Costs per QALY gained or strepto-kinase were between $630 and $730 across the regions. Incre-mental cost-e ectiveness ratios or t-PA were around $16,000/ QALY gained, compared with streptokinase. Minor variationsoccurred between regions due to small di erences in ollow-upcare based on regional costs.
Secondary prevention strategies are equally cost-e ective in de-veloping countries. Studies show that a combination o aspirin,an angiotensin-converting enzyme inhibitor, a beta-blocker, anda statin or secondary prevention can lead to acceptable cost-e ectiveness ratios in all developing regions. 5 Use o currentlyavailable generic agents, even in the absence o the so-calledpolypill, could be highly cost-e ective, on the order o $300-$400 per person per QALY gained. 6
Primary prevention is paramount or the large number o indi-viduals who are at high risk or CVD. Given limited resources,
nding low-cost prevention strategies is a top priority. Usingprediction rules or risk scores to identi y those at higher riskin order to target speci c behavioral or drug interventions is awell-established primary prevention strategy and has proven tobe cost-e ective in developing countries. 6, 7 Most have included
age, sex, hypertension, smoking status, diabetes mellitus, andlipid values, while others have also included amily history. 8, 9
Recently, many investigators have examined whether additionallaboratory-based risk actors can add to predictive discrimina-tion o the risk actors used in the Framingham Heart Study riskscore (Figures 5a, b ). The recent analyses in the ARIC (Athero-sclerosis Risk in Communities) study, 10 and the FraminghamO spring Study,11, 12 suggested that little additional in ormationwas gained when other blood-based novel risk actors wereadded to the traditional risk actors.
Although the Reynolds Risk Score or women, 13 which addedamily history, high-sensitivity C-reactive protein (hs-CRP),
and glycated hemoglobin levels, only had a marginally higherC-statistic (0.808) than the Framingham covariates (0.791), itcorrectly reclassi ed many individuals at intermediate risk(Figure 6 ). Some women deemed low risk by the Framinghamrisk score were reclassi ed as intermediate or high risk accordingto the Reynolds Risk Score and, thus, would have been eligible
or more aggressive management. Also, some women whowere initially high risk according to Framingham were reclassi-
ed as lower risk and, thus, would not have needed treatment.
More attention is now ocused on developing risk scores thatwould be easier to use in clinical practice without loss o predic-tive discrimination in resource-poor countries. In high-incomecountries, a prediction rule that requires a lab test is an incon-
Table 2Cost-E ectiveness or a Selection o CHDInterventions in Developing Regions
ASA = aspirin; BB = beta-blocker; SK = streptokinase;ACEI = angiotensin-converting enzyme inhibitor;tPA = tissue plasminogen activator.
*Across six World Bank regions.
CHD = coronary heart disease.
Range includes di erent estimates o cost ointerventions, as well as blood pressure reduction(
-
7/27/2019 1_1 epidemiologia
10/16
1.1.10 Chapter 1: General Principles
venience; in low-income countries, with limited testing acilities,it may be too expensive or widespread screening or precludeits use altogether. In response to this real concern, the WHOrecently released risk-prediction charts or the di erent regionso the world with and without cholesterol. 14, 15
A study based on the US National Health and Nutrition Exami-nation Survey (NHANES) ollow-up cohort demonstrated that anon-lab-based risk tool that uses in ormation obtained in a sin-gle encounter (age, systolic blood pressure, BMI, diabetes status,and smoking status) can predict CVD outcomes as well as onethat requires lab testing with C-statistics o 0.79 or men and0.83 or women that were no di erent rom the Framingham-based risk tool. 16 The association between BMI and cholesterolhas been con rmed by large cohorts. 4
Further, the results o the goodness-o - t tests suggest that thenon-laboratory-based model is well-calibrated across a widerange o absolute risk levels and without changes in classi ca-
tion o risk. A risk score based on the US NHANES ollow-upcohort can be used to predict CVD events in regions wherecholesterol testing is not available ( Figures 7a, b ).
Education and public policy interventions that have reducedsmoking rates, lowered mean blood pressure levels, andimproved lipid pro les have contributed to the reduction inCHD rates. 17 Education and policy e orts directed at tobaccoconsumption have contributed substantially to the reductions inCVD. In addition, salt and cholesterol reduction has been evalu-ated as a cost-e ective strategy to reduce stroke and MI in low-and middle-income countries by investigators at the WHO. 18 Community interventions have reduced levels o multiple risk
actors and, in some cases, CHD mortality.
Tobacco Tobacco control can be conceptualized in terms o strategiesthat reduce the supply o , or demand or, tobacco. Most publichealth and clinical strategies to date ocus on reducing demand
Figure 5a Assessing 10-Year Coronary Heart Disease Risk in Men (1 o 2)
Adapted with permission rom Wilson PW, DAgostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction o coronary heart disease using risk actor categories. Circulation 1998;97:1837-47.
Assessing 10-Year Coronary Heart Disease Risk in Men (1 of 2)Age
Years
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
LDL Pts
-1
0
1
2
3
4
5
6
7
Chol Pts
[-1]
[0]
[1]
[2]
[3]
[4]
[5]
[6]
[7]
Step 1
Cholesterol
(mg/dl)
-
7/27/2019 1_1 epidemiologia
11/16
1.1: Global Burden of Cardiovascular Disease 1.1.11
through economic disincentives (taxes), health promotion (me-dia and packaging e orts), restricted access (to advertising andtobacco), or clinical assistance or cessation. The WHO e ort tocatalyze the creation o a global treaty against tobacco use wasa key milestone. In May 2003, the WHO World Health Assemblyunanimously adopted the WHO Framework Convention in To-bacco Control (FCTC), the rst global tobacco treaty. The FCTChad been rati ed by 164 countries as o April 2009, making itone o the most widely embraced treaties in the United Nations.The FCTC has spurred e orts or tobacco control across theglobe by providing both rich and poor nations with a common
ramework o evidence-based legislation and implementationstrategies known to reduce tobacco use.
Jha and colleagues presented a landmark analysis in 2006 otobacco control cost-e ectiveness 19. They calculated the reduc-tions in uture tobacco deaths due to a range o tax, treatment,and nonprice interventions among smokers alive in 2000. They
ound that a 33% price increase would result in a reduction o
between 19.7 and 56.8 million (5.4-15.9% o total) deaths insmokers rom the developing world who were alive in 2000. 19
Calculations show that nicotine replacement therapy (NRT)could reduce the number o deaths by between 2.9 and 14.3million (0.8-4.0%) in the 2000 cohort. 19 A range o nonpriceinterventions such as advertising bans, health warnings, andsmoke- ree laws would reduce deaths by between 5.7 and 28.6million (1.6-7.9% o total) in that cohort. 19 These reductionswould translate into developing world cost-e ectiveness valueso between $3 and $42 per QALY saved or tax increases (notincluding tax revenue), $55 to $761 per QALY or NRT, and $54to $674 per QALY or nonprice measures. 19
Salt and Lipid Reductions The population-based intervention that is most touted as an e -
ective means to lower blood pressure is reduction o salt intake.Average consumption o salt in the United States is 10.4 g/day,
Figure 5b Assessing 10-Year Coronary Heart Disease Risk in Women (2 o 2)
Adapted with permission rom Wilson PW, DAgostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction o coronary heart disease using risk actor categories. Circulation 1998;97:1837-47.
Assessing 10-Year Coronary Heart Disease Risk in Women (2 of 2)Age
Years
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
LDL Pts
--9
-4
0
3
6
7
8
8
8
Chol Pts
[-9]
[-4]
[0]
[3]
[6]
[7]
[8]
[8]
[8]
Step 1
Cholesterol
(mg/dl)
-
7/27/2019 1_1 epidemiologia
12/16
1.1.12 Chapter 1: General Principles
o which 75% comes rom processed oods. In the United States,reducing salt intake by 3 g/day (1100 mg/day o sodium) wouldreduce systolic blood pressure by 3.6-5.61 mm Hg or hyperten-sives, and in all other patients, the e ect was 1.8-3.51 mm Hg. 20
Meta-analyses o randomized controlled trials examining thelong-term e ects o salt reduction in people with and without
hypertension have shown that reductions in salt intake canreduce absolute systolic blood pressure by a small but importantamount. 21 E ect o salt reduction on blood pressure reduc-tion was ound to be linear over the range o 0-3 g/day, or anapproximate 1:1 ratio in reduction in salt intake (grams/day)and decrease in mean systolic blood pressure (mm Hg). Reduc-ing population-wide salt consumption by only 15%throughmass media campaigns and re ormulation o ood products byindustrywould avert up to over 8.5 million deaths in 23 high-burden countries over a 10-year period. 21 The cost-e ectivenessanalyses on salt reduction as a result o public education are
quite avorable. 22, 23 The intervention ranges rom being cost-saving to $200 per DALY averted.
The results o a campaign or reducing saturated at and replacingit with polyunsaturated at is also likely to be cost-e ective. In thebase case, a 3% decline in cholesterol and $6 per capita educa-tion costs were assumed. This resulted in a cost as low as $1,800/
DALY averted in the South Asia region and up to $4,000/DALYaverted in the Middle East and North A rica region. However, ithe cost or the education plan were halved, the ratio would beapproximately $900/DALY and would be cost-saving i the reduc-tion could be achieved or under $0.50 per capita, which may bepossible in areas with much less expensive access to media.
Community Interventions In the 1970s and 1980s, a series o population-based communi-ty intervention studies were conducted to reduce risk actors orchronic disease and have been reviewed elsewhere. 24 These o-cused on either changes in health behaviors or risk actors such
Figure 6Reclassifcation o Risk Using the Reynolds Risk Score or a Representative Population o 100,000 Intermediate-Risk US
Women Without DiabetesReproduced with permission rom Ridker PM, Buring JE, Ri ai N, Cook NR. Development and validation o improved algorithms or the assessment o global cardiovascular risk in women: the Reynolds Risk Score. JAMA 2007;297:611-9.
Reclassi cation of Risk Using the Reynolds Risk Score for a RepresentativePopulation of 100,000 Intermediate-Risk US Women Without Diabetes
100,000 WomenWith Intermediate CVD Risk
10-Year CVD Risk Stratication Using Adult Treatment Panel III Covariates 45
80%
5% to
-
7/27/2019 1_1 epidemiologia
13/16
1.1: Global Burden of Cardiovascular Disease 1.1.13
as tobacco use, bodyweight, cholesterol, and blood pressure, aswell as a reduction in CVD morbidity and mortality. In general,they included a combination o communitywide actions, as wellas those ocused on individuals identi ed as high risk.
One o the earliest and most o ten cited community interven-tions is the North Karelia project, which began in 1972. Thecommunity-based interventions included health education,
screening, a hypertension control program, and treatment. Overthe rst 5 years o the study, reductions in risk actors as wellas a decline in CHD mortality o 2.9%/year versus a 1%/yeardecline in the remainder o Finland. During the next 10 years,declines were greater in the rest o Finland. Over 25 years o
ollow-up, a large decline in CHD occurred in both the NorthKarelia region (73%) and the remainder o Finland (63%). 25
While the overall di erence in the decline in CHD deaths wasnot signi cantly greater in the study area o North Karelia, thereduction in male tobacco-related cancers was signi cant. Asimilar study in the Stan ord, CA, area showed reductions in risk
actorscholesterol (2%), blood pressure (4%), and smokingrates (13%) when compared to sites without the interventionbut no impact on disease endpoints.
Later, community interventions in high-income countries showedmixed results, with some showing improvements in risk actorsbeyond the secular decline that was occurring throughout mosto the developed economies, and others with no additional
decline. However, a meta-analysis o the randomized multiple riskactor interventions showed net signi cant decreases in systolic
blood pressure (-4.2 mm Hg), smoking prevalence (-4.2%),and cholesterol (-0.14 mmol/L). 26 The declines in total and CHDmortality o 3% and 4% were not signi cant. The limitation to allo the projects includes the challenge o detecting small changesthat on a population level may be signi cant. It is possible that a10% reduction in mortality could have been missed. 26
Several community intervention studies have been conductedin developing countries, including China, Mauritius, and SouthA rica. The Tianjin Project showed reductions in hypertension and
Figure 7aRisk Prediction Chart or Cardiovascular Disease Using NonlaboratoryBased Measures (1 o 2)
Reproduced with permission rom Gaziano TA, Young CR, Fitzmaurice G, Atwood S, Gaziano JM. Laboratory-based versus non-laboratory-based method or assessment o cardiovascular disease risk: the NHANES I Follow-up Study cohort. Lancet 2008;371:923-31.
Risk Prediction Chart for Cardiovascular Disease Using NonlaboratoryBased Measures (1 of 2)Women
Age65-74
Age55-64
Age45-54
Age35-44
No DiabetesNon Smoker Smoker
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40
171-180
161-170
151-160
141-150
131-140
121-130111-120
171-180
161-170
151-160
141-150
131-140
121-130
111-120
171-180
161-170
151-160
141-150
131-140
121-130
111-120
171-180
161-170
151-160
141-150
131-140
121-130
111-120
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40
BMI (kg/m2) BMI (kg/m2)
DiabetesNon Smoker Smoker
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40171-180161-170151-160141-150131-140
121-130111-120
171-180161-170151-160141-150131-140121-130111-120
171-180161-170151-160141-150131-140121-130111-120
171-180161-170151-160141-150131-140121-130111-120
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40BMI (kg/m2) BMI (kg/m2)
S y s
t o l i c B l o o
d P r e s s u r e
( m m
H g
)
S y s
t o l i c B l o o
d P r e s s u r e
( m m
H g
)
How to use the ChartChoose the section with the sex, diabetes and smoking status; Find the cell that matches the patients risk factor pro le using the age, BMI, and blood pressure; Refer to physician thosewith excessive blood pressure (>180 mm Hg)
5 yearcardiovascular risk(fatal and non-fatal)
Low
< 5%5-10%
Moderate10-20%
High20-30%>30%
-
7/27/2019 1_1 epidemiologia
14/16
1.1.14 Chapter 1: General Principles
obesity. 27 The Mauritius Project, among other interventions, result-ed in a government-led program that changed the prime cookingoil rom a predominantly saturated at palm oil, to a soybean oilhigh in unsaturated atty acids. Overall total cholesterol levels ell14% during the 5-year study period rom 1987 to 1992. Changesin other risk actors were mixed, with declines in blood pressureand smoking rates and increases in obesity and diabetes. 28
The Coronary Risk Factor Study in South A rica compared acontrol community to two communities receiving two di erentlevels o intensity o interventions. The interventions includedmass media messages, group-sponsored educational sessions,and blood pressure screening and ollow-up with the health sec-tor when appropriated. Both high- and low-intensity interven-tions showed improvements in blood pressure, smoking rates,and high-density lipoprotein (HDL) to total cholesterol ratio overthe control community, but with little di erence between thetwo intervention communities. 29
One other signi cant reduction o CHD came not through aconcerted community intervention but through changes in scalpolicy. In Poland, reductions in subsidies or animal products suchas butter and lard led to a switch rom saturated to polyunsatu-rated ats, mainly grape seed- and soya bean-based oils. A decreasein CHD mortality o >25% between 1991 and 2002 could not beexplained by increased ruit consumption or declines in smoking.
Key Points CVD accounts or approximately 30% o deaths worldwide.
However, there is great variation in regional CVD mortalityrates.
Countries have gone through phases o the epidemiologictransition that are characterized by di erent li eexpectancies, di erent rates o CVD mortality, and di erentlevels o CVD risk actors.
Figure 7bRisk Prediction Chart or Cardiovascular Disease Using NonlaboratoryBased Measures (2 o 2)
Reproduced with permission rom Gaziano TA, Young CR, Fitzmaurice G, Atwood S, Gaziano JM. Laboratory-based versus non-laboratory-based method or assessment o cardiovascular disease risk: the NHANES I Follow-up Study cohort. Lancet 2008;371:923-31.
Risk Prediction Chart for Cardiovascular Disease Using NonlaboratoryBased Measures (2 of 2)Men
Age65-74
Age55-64
Age45-54
Age35-44
No DiabetesNon Smoker Smoker
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40
171-180
161-170
151-160
141-150
131-140
121-130111-120
171-180
161-170
151-160
141-150
131-140
121-130
111-120
171-180
161-170
151-160
141-150
131-140
121-130
111-120
171-180
161-170
151-160
141-150
131-140
121-130
111-120
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40
BMI (kg/m2) BMI (kg/m2)
DiabetesNon Smoker Smoker
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40171-180161-170151-160141-150131-140
121-130111-120
171-180161-170151-160141-150131-140121-130111-120
171-180161-170151-160141-150131-140121-130111-120
171-180161-170151-160141-150131-140121-130111-120
15-20 20-25 25-30 30-40 15-20 20-25 25-30 30-40BMI (kg/m2) BMI (kg/m2)
S y s
t o l i c B l o o
d P r e s s u r e
( m m
H g
)
S y s
t o l i c B l o o
d P r e s s u r e
( m m
H g
)
How to use the ChartChoose the section with the sex, diabetes and smoking status; Find the cell that matches the patients risk factor pro le using the age, BMI, and blood pressure; Refer to physician thosewith excessive blood pressure (>180 mm Hg)
5 yearcardiovascular risk(fatal and non-fatal)
Low< 5%5-10%
Moderate10-20%
High20-30%>30%
-
7/27/2019 1_1 epidemiologia
15/16
1.1: Global Burden of Cardiovascular Disease 1.1.15
The age o degenerative and man-made diseases isdistinguished by mortality rom noncommunicable diseases,primarily CVD-surpassing mortality rom malnutrition andin ectious diseases.
There is a continuous relationship between blood pressure,cholesterol levels, BMI, physical activity, and risk or CVDdespite arbitrary numeric thresholds used in guidelines.
Patients may have CVD events despite some individual riskactors being in the normal range, due to the overallcombined high risk rom all risk actors.
Three complementary types o interventions have occurredin high-income countries to result in large reductions inage-adjusted CVD mortality rates:
1. Targeting patients with acute or established CVD,
2. Risk assessment and identi ying those at high risk due tomultiple risk actors or intervention be ore their rst CVD
event, and
3. Mass education or policy interventions directed at the entirepopulation to reduce the overall level o risk actors.
Primary prevention is paramount or the large number oindividuals who are at high risk or CVD. A cost-e ectiveprimary prevention strategy includes use o prediction rulesor risk scores to identi y those at higher risk in order totarget speci c behavioral or drug interventions. Risk scorestypically include age, sex, hypertension, smoking status,diabetes mellitus, and lipid values. Some also include amilyhistory. Some risk scores do not require laboratory testing.
Education and public policy interventions that have reducedsmoking rates, lowered mean blood pressure levels, andimproved lipid pro les, have contributed to the reduction inCHD rates.
Re erences
1. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ, eds.Global Burden o Disease and Risk Factors. New York: The World Bank and Ox ord University Press; 2006: 552.
2. Gaziano JM. Fi th phase o the epidemiologic transition: the age o obesity and inactivity. JAMA 2010;303:275-6.
3. Lawes CM, Hoorn SV, Rodgers A. Global burden o blood-pressure-related disease, 2001. Lancet 2008;371:1513-8.
4. Whitlock G, Lewington S, Sherliker P, et al., on behal o the Pro- spective Studies Collaboration. Body-mass index and cause-specifc mortality in 900,000 adults: collaborative analyses o 57 prospec-tive studies. Lancet 2009;373:1083-96.
5. Gaziano TA. Cardiovascular disease in the developing world and itscost-e ective management. Circulation 2005;112:3547-53.
6. Gaziano TA, Opie LH, Weinstein MC. Cardiovascular disease prevention with a multidrug regimen in the developing world: acost-e ectiveness analysis. Lancet 2006;368:679-86.
7. Gaziano TA, Steyn K, Cohen DJ, Weinstein MC, Opie LH. Cost-e -ectiveness analysis o hypertension guidelines in South A rica: ab-
solute risk versus blood pressure level. Circulation 2005;112:3569-76.
8. Ferrario M, Chiodini P, Chambless LE, et al. Prediction o coro-nary events in a low incidence population. Assessing accuracy o the CUORE Cohort Study prediction equation. Int J Epidemiol 2005;34:413-21.
9. Wilson PW, DAgostino RB, Levy D, Belanger AM, Silbershatz H,Kannel WB. Prediction o coronary heart disease using risk actor categories. Circulation 1998;97:1837-47.
10. Folsom AR, Chambless LE, Ballantyne CM, et al. An assessment o incremental coronary risk prediction using C-reactive protein and other novel risk markers: The Atherosclerosis Risk in CommunitiesStudy. Arch Intern Med 2006;166:1368-73.
11. Wang TJ, Gona P, Larson MG, et al. Multiple biomarkers or the prediction o frst Major cardiovascular events and death. N Engl J Med 2006;355:2631-9.
12. Ware JH. The limitations o risk actors as prognostic tools. N Engl J Med 2006;355:2615-7.
13. Ridker PM, Buring JE, Ri ai N, Cook NR. Development and validation o improved algorithms or the assessment o global cardiovascular risk in women: the Reynolds Risk Score. JAMA2007;297:611-9.
-
7/27/2019 1_1 epidemiologia
16/16
14. Lindholm LH, Mendis S. Prevention o cardiovascular disease indeveloping countries. Lancet 2007;370:720-2.
15. Mendis S, Lindholm LH, Mancia G, et al. World Health Organiza-tion (WHO) and International Society o Hypertension (ISH) risk
prediction charts: assessment o cardiovascular risk or preventionand control o cardiovascular disease in low and middle-incomecountries. J Hypertens 2007;25:1578-82.
16. Gaziano TA, Young CR, Fitzmaurice G, Atwood S, Gaziano JM.Laboratory-based versus non-laboratory-based method or assess-ment o cardiovascular disease risk: the NHANES I Follow-up Study cohort. Lancet 2008;371:923-31.
17. Ford ES, Ajani UA, Cro t JB, et al. Explaining the Decrease inU.S. Deaths rom Coronary Disease, 1980-2000. N Engl J Med 2007;356:2388-98.
18. Asaria P, Chisholm D, Mathers C, et al. Population-wide interven-tions to prevent chronic diseases. Lancet 2007;370:2044-53.
19. Jha P, Chaloupka FJ, Moore J, et al. Tobacco Addiction. In: JamisonDT, Breman JG, Measham AR, et al. Disease Control Priorities inDeveloping Countries. 2nd ed. New York: Ox ord University Press;2006.
20. Bibbins-Domingo K, Chertow GM, Coxson PG, et al. Projected e ect o dietary salt reductions on uture cardiovascular disease. N Engl J Med 2010;362:590-9.
21. Asaria P, Chisholm D, Mathers C, Ezzati M, Beaglehole R. Chronic disease prevention: health e ects and fnancial costs o strate-
gies to reduce salt intake and control tobacco use. Lancet 2007;370:2044-53.
22. Jamison D, Breman JG, Measham AR, et al. Disease Control Priori-ties in Developing Countries. 2nd ed. New York: Ox ord University Press; 2006.
23. Gaziano TA, Galea G, Reddy KS. Scaling up interventions or chronic disease prevention: the evidence. Lancet 2007;370:1939-46.
24. Puska P, Vartiainen E, Tuomilehto J, Salomaa V, Nissinen A.Changes in premature deaths in Finland: success ul long-term
prevention o cardiovascular diseases. Bull World Health Organ,1998;76:419-25.
25. Ebrahim S, Smith GD. Systematic review o randomised controlled trials o multiple risk actor interventions or preventing coronary heart disease. BMJ 1997;314:1666-74.
26. Yu Z, Nissinen A, Vartiainen E, Song G, Guo Z, Tian H. Changes incardiovascular risk actors in di erent socioeconomic groups: seven
year trends in a Chinese urban population. J Epidemiol Community Health 2000; 54: 692-6.
27. Uusitalo U, Feskens EJ, Tuomilehto J, et al. Fall in total cholesterol concentration over fve years in association with changes in atty acid composition o cooking oil in Mauritius: cross sectional survey.BMJ 1996;313:1044-6.
28. Rossouw JE, Jooste PL, Chalton DO, et al. Community-based in-tervention: the Coronary Risk Factor Study (CORIS). Int J Epidemiol
1993;22:428-38.